
Submitted:
22 October 2024
Posted:
24 October 2024
You are already at the latest version
Abstract
Background: Decision, whether to de-label patient with suspected BL hypersensitivity, is based on the risk stratification. The aim of the study was to prepare a characteristic of diagnostic risk groups and to create a model enabling the identification of the low-risk diagnostic group. Methods: We analyzed medical records of patients hospitalized due to suspected hypersensitivity to BL antibiotics. Based on the history data, patients were divided into three diagnostic risk groups, using the criteria proposed by Shenoy et al. Univariate and multivariate analysis model were used to create a diagnostic tool. Results: Among 263 patients referred for BL hypersensitivity diagnosis, 88 (33.5%) were qualified to group I, 129 (49%) to group II, and 46 (17.5%) to group III. There were significant differences between diagnostic risk groups regarding history of hypersensitivity to penicillins (p<0.001), cephalosporins (p<0.001), >1 BL (p<0.05), several episodes of BL hypersensitivity (p<0.001), medical intervention (p<0.001), documented hypersensitivity (p<0.001), time from drug intake to symptoms (p<0.001), time from hypersensitivity to diagnosis (p<0.001). 81 patients (30.8%) were de-labeled: 52 (59.8%) in group I, 27 (20.9%) in group II and 2 (4.3%) in group III. In univariate analysis, model of the low diagnostic risk group applied to the de-labeled part showed 90% specificity and 21.93% sensitivity. NPV and PPV were estimated at 72.04% and 49.53%, respectively. Multivariate model had high specificity but low sensitivity; its NPV was 76% with 68% PPV. Conclusions: The tool enabling the identification of low diagnostic risk patients based on anamnesis is not sensitive enough, to de-label patients on its basis.
Keywords:
beta-lactam
; hypersensitivity
; de-labeling
; risk stratification
1. Introduction
Beta-lactam (BL) antibiotics are one of the most common causes of drug hypersensitivity [1,2,3]. Approximately 6%-10% of the population reports an "allergy" to penicillin’s (PN), including 15% of hospitalized patients, but allergy work-up excludes hypersensitivity in about 95% of them [4,5,6,7,8]. Actual hypersensitivity to cephalosporins (CF) is estimated at <2% [2], to carbapenems 0.3%-3.7% [9], while to monobactams is unknown. Hypersensitivity in the BL group may involve a BL ring, a single BL antibiotic or antibiotics with a similar or identical structure of R1 side chain, less often R2 [10,11,12,13]. Anaphylaxis after BL administration is rare, with a frequency of 46.9 per 10,000 for penicillins and 6.1 per 10,000 for cephalosporins in the general population. At the same time, penicillins are the most common cause of drug-induced anaphylaxis [14].
The diagnosis of "allergy" to BL antibiotics without verification, is associated with a longer hospital stay, more frequent use of fluoroquinolones, vancomycin and clindamycin, higher rates of Clostridium difficile, methicillin-resistant Staphylococcus aureus (MRSA) and vancomycin-resistant enterococci (VRE) infections compared to patients without the "allergy" label [15,16]. "Allergy" to BL antibiotics history is associated not only with negative consequences for the patient, but also for the health care system by increasing the cost of treatment [17,18,19]. Avoidance of BL antibiotics in patients reporting an „allergy” result in a higher risk of treatment failure [20].
De-labeling involves removing the "allergy" label reported by the patient. There are several de-labeling strategies:
- based only on the medical history, if anamnesis clearly indicates symptoms other than hypersensitivity (e.g., isolated, uncharacteristic gastrointestinal symptoms, headaches, hypersensitivity to BL antibiotics in the family),
- diagnosis based on skin tests with determinants, followed by provocation with a single dose of the drug or in divided doses,
The choice of de-labeling method is based on the risk stratification. The main goal of risk stratification is to select a group of high-risk patients who require access to specialized diagnostics first. At the same time, due to the rare actual hypersensitivity reactions to BL antibiotics, it is important to select a low-risk group in which de-labeling can be safely performed. Previous European Academy of Allergy and Clinical Immunology (EAACI) recommendations suggested a full allergy work-up in patients with suspected BL antibiotic hypersensitivity, without assessing the severity of the reaction [23,24,25]. Current EAACI position paper recommends risk stratification, assessing time and severity of the hypersensitivity reaction. Despite proposed high and low-risk groups, diagnosis without skin testing is recommended only in a narrow group of patients, which includes pediatric patients with benign maculopapular exanthema (MPE) and patients with palmar exfoliative exanthema [26]. In the last decade many papers on risk stratification in BL hypersensitivity were published, regarding mainly penicillins [27,28,29,30,31]. In contrast, recent United States guidelines suggested several important changes in the recommendations for BL hypersensitivity diagnosis, including direct de-labeling patients with nonspecific symptoms of penicillin hypersensitivity, direct provocation with CF with a different R1 side chain in patients with non-anaphylactic hypersensitivity to CF and anaphylactic hypersensitivity to PN. In patients with a history of unverified non-anaphylactic PN/CF allergy, the use of CF/PN without prior skin testing is suggested. [4]. Both in the United States and Europe, the number of patients reporting hypersensitivity to BL antibiotics (mainly penicillins) far exceeds the number of specialists who could verify the "allergy" label [32]. The purpose of this study was to analyze the group of patients reporting hypersensitivity to BL antibiotics and to create a model identifying low-risk patients based on anamnesis.
2. Materials and Methods
2.1. Study Design
We conducted a retrospective, single-center, observational study based on medical records analysis. We analyzed medical records of patients hospitalized at the Department of Allergology and Clinical Immunology between January 2018 to June 2022, due to suspected hypersensitivity to BL antibiotics. Among patients with reported hypersensitivity to various drugs, we selected a group of patients referred for diagnosis of antibiotics hypersensitivity. Then we excluded patients with suspected hypersensitivity to antibiotics other than BL. The final analysis included only patients reporting hypersensitivity to at least one BL antibiotic.
Based on the history data, patients were divided into three diagnostic risk groups, using the criteria proposed by Shenoy et al. [33]. Low risk (group I) included: isolated reactions that are unlikely allergic (eg, gastrointestinal symptoms, headaches), pruritus without rash, remote (>10 y) unknown reactions without features of IgE, family history of penicillin allergy. Moderate risk group (group II) included: urticaria or other pruritic rashes, reactions with features of IgE but not anaphylaxis. High risk group (group III) included: anaphylactic symptoms, positive skin testing, recurrent reactions, reactions to multiple β-lactam antibiotics. The criteria were applied to patients reporting hypersensitivity to either to penicillins or to cephalosporins, or to both. For the purpose of the study, hypersensitivity to cephalosporins was divided into three groups according to the R1 side chain structure based on Romano et al [34].
2.2. Statistical Analysis
For quantitative traits, due to the non-normal distribution in at least one group, the non-parametric Kruskall-Wallis (KW) test was used. For qualitative variables, statistical analysis was performed using a non-parametric test of independence x2. Linear model with a logit binding function was used to evaluate the model for membership in the low-risk group (group I). Results are presented as odds ratio with 95% confidence interval. Multivariate modeling was performed using a stepwise backward method, manually including age and gender as potential clinically relevant confounding variables in the model. Calculations were performed using the R language in the RStudio software. A p<0.05 was considered statistically significant.
3. Results
Between January 2018 and June 2022 there were 1,957 patients referred to the department due to the drug hypersensitivity diagnosis. Among them, 391 patients were hospitalized due to antibiotic hypersensitivity diagnosis. From this group we excluded 128 patients hospitalized due to the diagnosis of hypersensitivity to antibiotics other than BL. Final analysis included 263 patients classified into three groups. The low-risk group consisted of 88 (33.46%) patients, moderate risk of 129 (49.05%) patients (group II), while the remaining 46 (17.49%) patients were classified to the high diagnostic risk group (group III).
3.1. General Characteristic of the Diagnostic Risk Groups
Gender, the prevalence of seasonal and perennial rhinitis, asthma and smoking did not differ significantly between the diagnostic risk groups. Detailed data are shown in Table 1.

Table 1.
General characteristics of patients in diagnostic risk groups.
| General characteristics | I n=88 (33,46%) |
II n=129 (49,05%) |
III n=46 (17,49%) |
p value |
|---|---|---|---|---|
| Gender [F] | 76 (86,4) | 106 (82,2) | 34 (73,9) | ns |
| SAR | 12 (13,6) | 20 (15,5) | 6 (13) | ns |
| PAR | 5 (5,7) | 10 (7,8) | 3 (6,5) | - |
| Asthma | 10 (11,4) | 11 (8,5) | 5 (10,9) | ns |
| Smoking | 15 (16,1) | 24 (18) | 10 (21,7) | ns |
F – indicates female, ns – non-significant, PAR – perennial allergic rhinitis, SAR- seasonal allergic rhinitis.
3.2. Anamnestic Data
The frequency of reported hypersensitivity incidents to penicillins and to aminopenicillins significantly decreased as the diagnostic risk increased, (p <0.001). Reported hypersensitivity to all cephalosporins and cephalosporins with the methoxyimine side chain (group A) were significantly more common, along with increasing diagnostic risk (p<0.001). There were no significant differences between groups in the frequency of reporting hypersensitivity to non-BL antibiotics and other drugs. In the low-risk group (group I), patients were significantly more likely not to remember the time between taking the drugs and the onset of hypersensitivity symptoms (p<0.01) and to report several episodes of hypersensitivity to the BL antibiotic (p<0.01), compared to the moderate- and high-risk groups. Short time from BL ingestion to the reported onset of hypersensitivity symptoms, the need for medical intervention and documented anaphylaxis, occurred significantly more often in the high-risk group (group III). Due to too small numbers in the groups, the calculation of statistical significance was not possible in all the data. Detailed characteristics are shown in Table 2 A-B.
| 2 A | I n=88 (33,46%) |
II n=129 (49,05%) |
III n=46 (17,49%) |
p value - testχ 2 |
|---|---|---|---|---|
| PN hypersensitivity (n=198, 75.29%) | 77 (87,5) | 102 (79,1) | 19 (41,3) | p < 0,001 |
|
3 (3,4) | 2 (1,6) | 0 (0) | - |
|
1 (1,1) | 0 (0) | 1 (2,2) | - |
|
2 (2,3) | 1 (0,8) | 0 (0) | - |
|
62 (70,5) | 90 (69,8) | 18 (39,1) | p < 0,001 |
|
15 (17) | 18 (14) | 3 (6,5) | - |
| CF hypersensitivity (n=105, 39.92%) | 28 (31,8) | 47 (36,4) | 30 (65,2) | p < 0,001 |
ceftriaxone (n=5) cefixime (n=1) |
23 (26,1) | 38 (29,5) | 22 (47,8) | p < 0,001 |
cefaclor (n=4) cephalexine (n=3) |
5 (5,7) | 6 (4,7) | 1 (2,2) | - |
cefamandole (n=1) |
1 (1,1) | 4 (3,1) | 7 (15,2) | - |
|
2 (2,3) | 1 (0,8) | 0 (0) | - |
| Hypersensitivity to >1 BL antibiotic (n=62, 23.57%) | 24 (27,3) | 34 (26,3) | 4 (8,7) | p <0,05 |
| Hypersensitivity to non-BL antibiotics (n=80, 30.42%) | 27 (30,7) | 42 (32,6) | 11 (23,9) | ns |
|
11 (12,5) | 22 (17,1) | 6 (13) | ns |
|
3 (3,4) | 3 (2,3) | 0 (0) | - |
|
3 (3,4) | 5 (3,9) | 2 (4,3) | - |
|
7 (8) 0 (0) |
6 (4,7) 1 (0,8) |
3 (6,5) 0 (0) |
- - |
|
9 (10,2) | 11 (8,5) | 4 (8,7) | ns |
|
4 (4,5) | 5 (3,9) | 1 (2,2) | - |
| 2 B |
I n=88 (33,46%) |
II n=129 (49,05%) |
III n=46 (17,49%) |
p value - test 2 |
| Hypersensitivity to other drugs (n=107, 40,68%) |
39 (44,3) | 52 (40,3) | 16 (34,8) | ns |
|
28 (31,8) | 37 (28,7) | 10 (21,7) | ns |
|
3 (3,4) | 5 (3,9) | 3 (6,5%) | - |
|
1 (1,1) | 2 (1,6) | 1 (2,2) | - |
|
3 (3,4) | 1 (0,8) | 2 (4,3) | - |
|
1 (1,1) | 1 (0,8) | 0 (0) | - |
| Time from BL antibiotic intake to onset of symptoms | ||||
|
11 (12,5) | 46 (35,7) | 40 (87) | p < 0,001 |
|
15 (17) | 33(25,6) | 2 (4,3) | - |
|
21 (23,9) | 8 (6,2) | 0 (0) | - |
|
36 (40,9) | 38 (29,5) | 4 (8,7) | p <0,001 |
| >1 episode of hypersensitivity to BL antibiotic (n=72, 27.38%) | 33 (37,5) | 32 (24,8) | 7 (15,2) | p < 0,001 |
| Medical intervention (n=156, 59,32%) |
25 (28,7) | 85 (66,4) | 46 (100) | p < 0,001 |
| Documented anaphylactic reaction (n=76, 28.9%) | 2 (2,3) | 34 (26,4) | 40 (87) | p < 0,001 |
| Time from hypersensitivity episode to diagnosis | ||||
|
4 (4,5) | 10 (7,8) | 7 (15,2) | ns |
|
12 (13,6) | 20 (15,5) | 19 (41,3) | p < 0,001 |
|
19 (21,6) | 52 (40,3) | 12 (26,1) | p < 0,05 |
|
13 (14,8) | 13 (10,1) | 3 (6,5) | - |
|
15 (17) | 12 (9,3) | 2 (4,3) | - |
|
23 (26,1) | 22 (17,1) | 2 (4,3) | - |
BL indicates beta-lactam, CF - cephalosporins, LA - local anesthetics, non-BL - non-beta-lactam, ns – non-significant, NSAID - non-steroidal anti-inflammatory drugs, PN – penicillins.
3.3. De-Labeling in the Risk Groups
After full diagnostic work-up including skin tests and drug provocation, de-labeling was performed in 81 patients (30.8%): 52 patients (59.8%) in the group I, 27 patients (20.9%) in the group II, and 2 patients (4.3%) in the group III (p<0.001).
3.4. Analysis of a Low-Risk Group Hypersensitivity to Beta-Lactam Antibiotics
3.4.1. Univariate Analysis of a Low-Risk Group
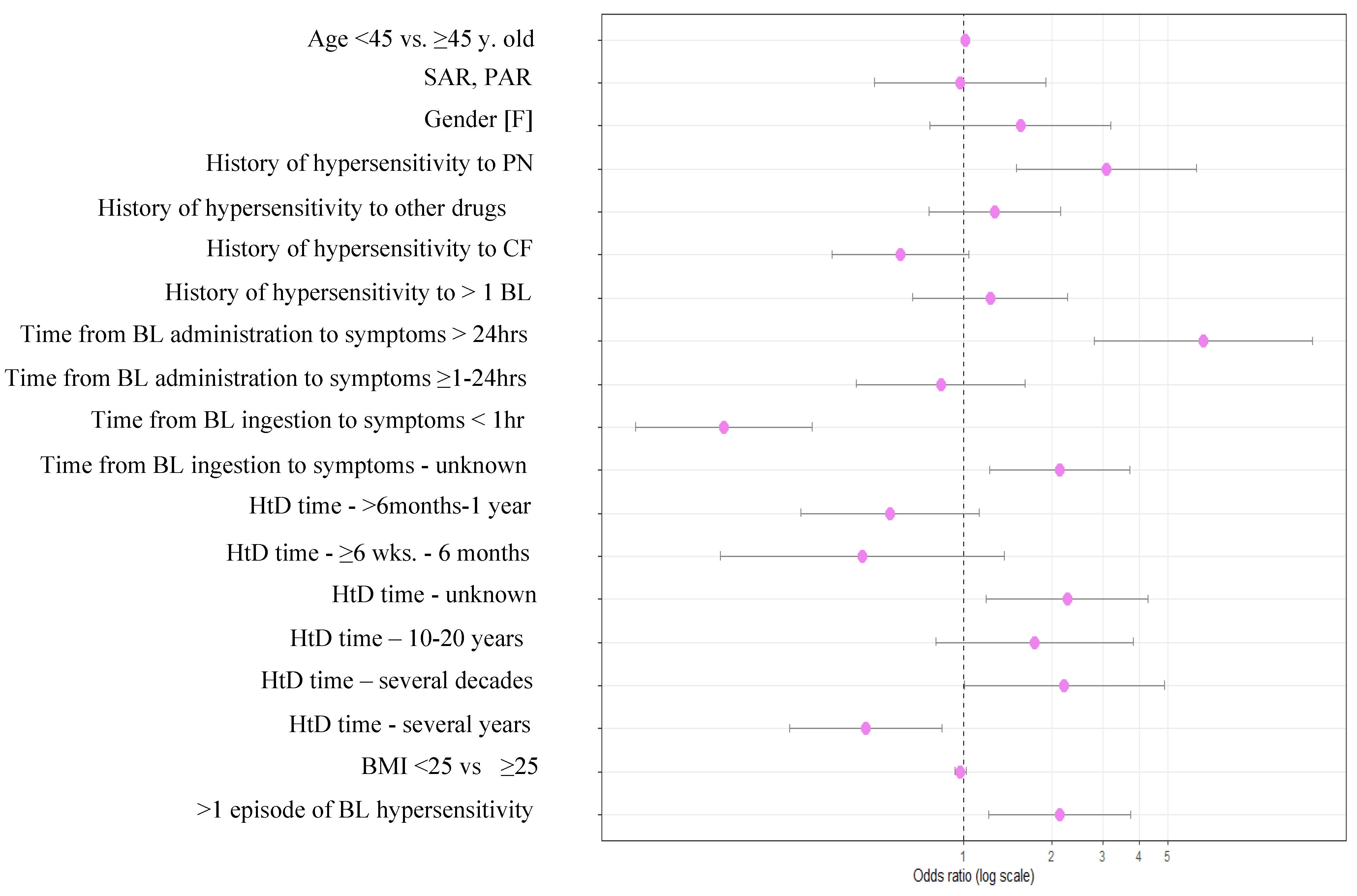
An increased chance of being assigned to a low-risk group (group I) was observed among patients who declared hypersensitivity to more than one BL antibiotic. The chance of being assign to the group I increased threefold in patients who reported hypersensitivity to penicillins on admission. A declared time from BL antibiotic ingestion to symptom onset of less than 1h strongly decreased the chance of being in the group I, while time longer than 24h increased the chance of being assigned to the I group. The chance of being assigned to the group I was increased by declaring an unknown time to symptoms and indicating the occurrence of more than one hypersensitivity episode. Patients diagnosed several years apart from the hypersensitivity episode were less likely to be assigned to the group I, while those whose time to reaction was several decades or unknown were assigned to the group I twice as often. Detailed data are shown in Table 3 and Figure 1. Model applied to the de-labeled part of the low-risk group in comparison to the rest of the group showed 90% specificity and 21.93% sensitivity. NPV and PPV were estimated at 72.04% and 49.53%, respectively.
Figure 1.
Forest plot of the univariate analysis of the low diagnostic risk group. BL – indicates beta-lactams, CF - cephalosporins, HtD time - time from hypersensitivity episode to allergologic diagnosis, PAR - year-round allergic rhinitis, PN - penicillins, SAR - seasonal allergic rhinitis.
Figure 1.
Forest plot of the univariate analysis of the low diagnostic risk group. BL – indicates beta-lactams, CF - cephalosporins, HtD time - time from hypersensitivity episode to allergologic diagnosis, PAR - year-round allergic rhinitis, PN - penicillins, SAR - seasonal allergic rhinitis.
3.4.2. Multivariate Analysis of a Low-Risk Diagnostic Group
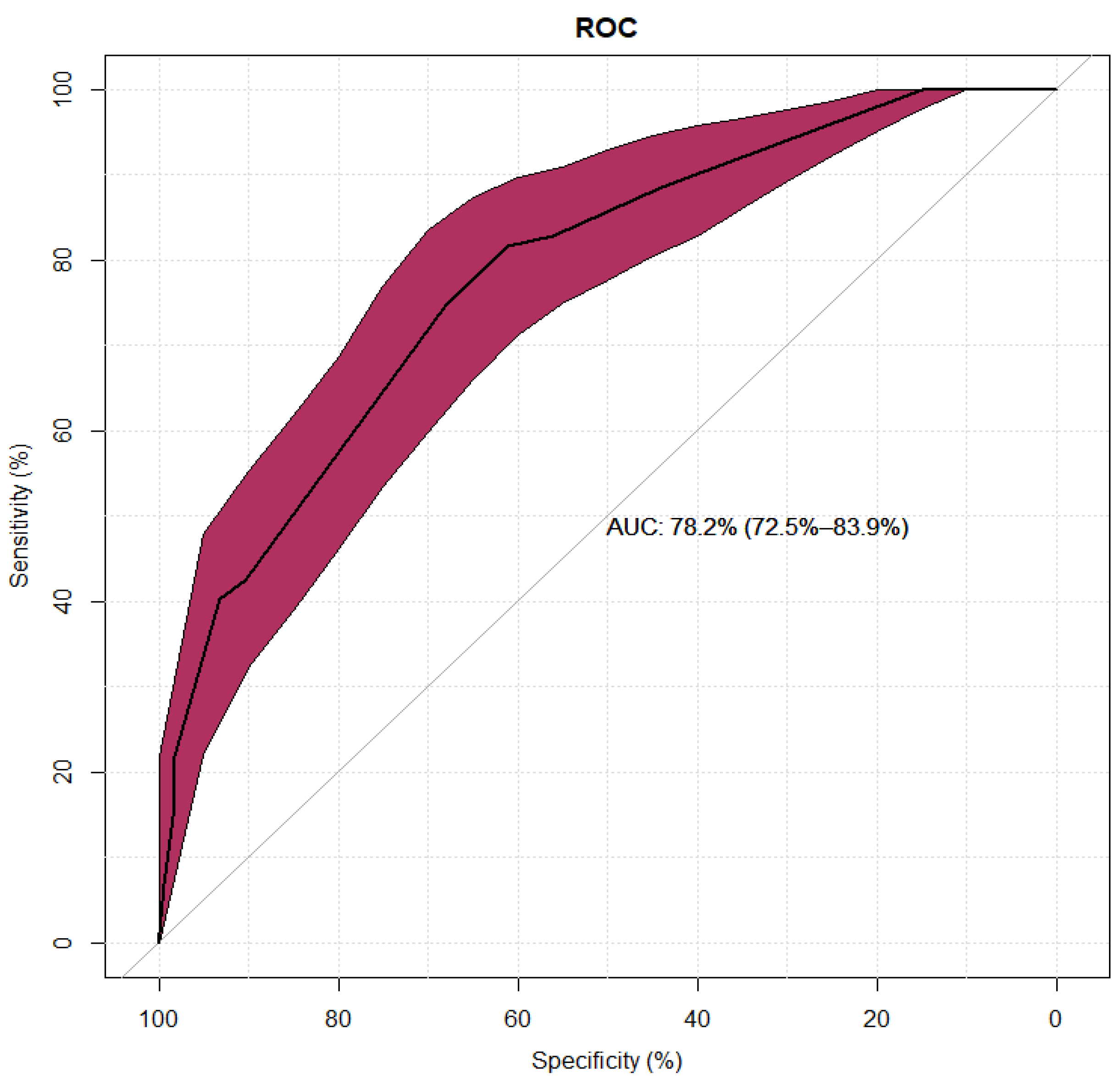
In a multivariate model, diagnostic time of several years since reported hypersensitivity to diagnosis significantly reduced chance of belonging to group I. More than one episode of hypersensitivity to BL characterized more often patients with low diagnostic risk, as did prolonged drug reaction time (>24h). A short reaction time occurs more often in the moderate and high-risk groups. Detailed results are shown in Table 4 and Figure 2. The model had high specificity but low sensitivity; its negative predictive value was 76% with 68% positive predictive value (Figure 3).
Table 4.
Multivariate logistic regression model of the low diagnostic risk group presented as odds ratio (OR) with 95% confidence interval.
Table 4.
Multivariate logistic regression model of the low diagnostic risk group presented as odds ratio (OR) with 95% confidence interval.
| Multivariate model | ||||
| Variable | p | OR | 95% CI | |
| HtD time- several years | < 0,01 | 0,26 | 0,13 | 0,54 |
| >1 episode of hypersensitivity to BL antibiotic | 0,02 | 2,20 | 1,15 | 4,23 |
| Time from BL antibiotic administration to symptoms <1hr | < 0,01 | 0,18 | 0,09 | 0,37 |
| Time from BL antibiotic administration to onset of symptoms >24hrs. | < 0,01 | 4,71 | 1,80 | 12,32 |
BL – indiciates beta-lactam, HtD time - time from hypersensitivity episode to allergologic diagnosis.
Figure 2.
Forest plot of the multivariate logistic regression model of the low diagnostic risk group. BL – indicates beta-lactam, HtD time - time from hypersensitivity episode to allergologic diagnosis
Figure 2.
Forest plot of the multivariate logistic regression model of the low diagnostic risk group. BL – indicates beta-lactam, HtD time - time from hypersensitivity episode to allergologic diagnosis
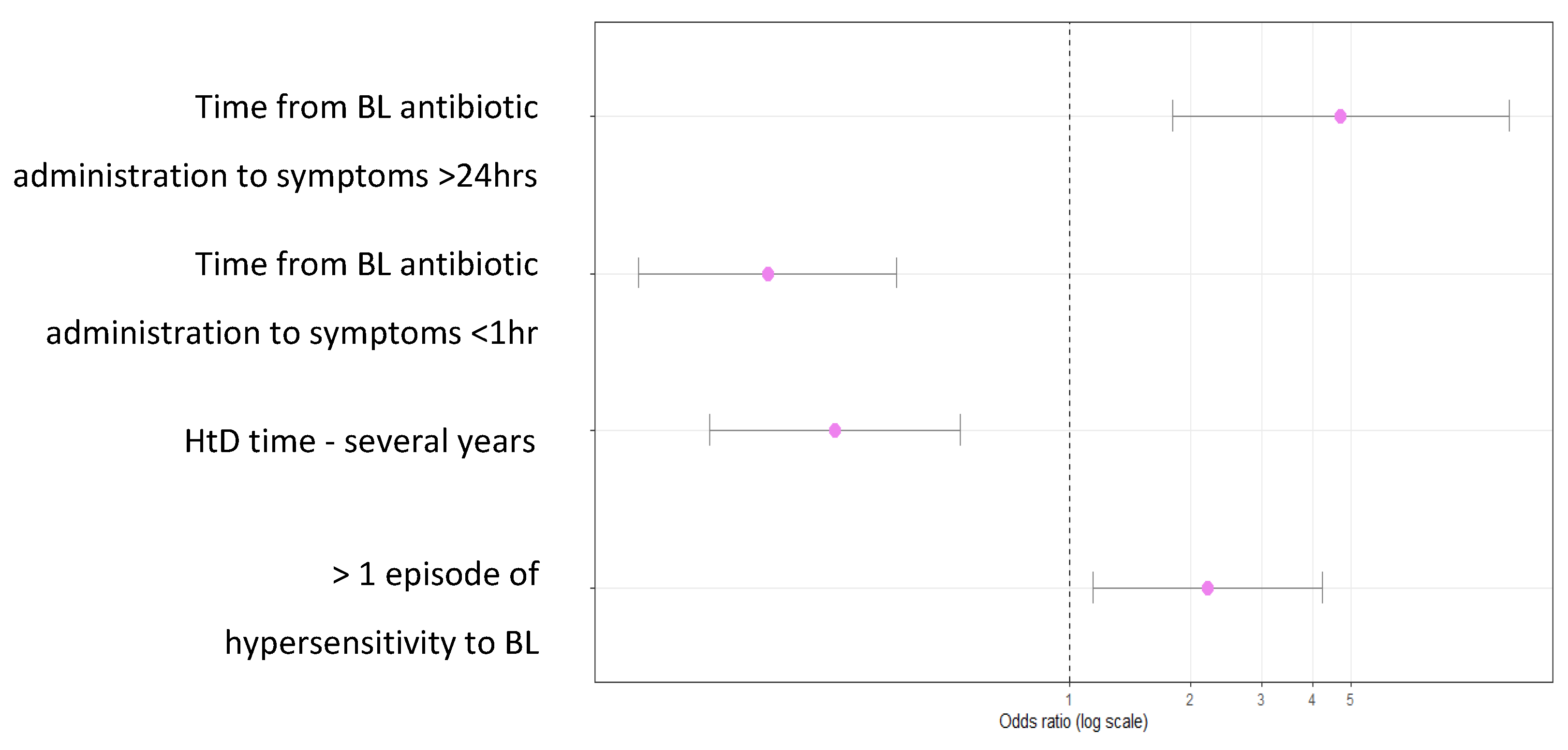
Figure 3.
Sensitivity and specificity for the multivariate logistic regression model of the low diagnostic risk group shown as a ROC (Receiver Operating Characteristic) curve. BL – indicates beta-lactam, HtD time - time from hypersensitivity episode to allergologic diagnosis.
Figure 3.
Sensitivity and specificity for the multivariate logistic regression model of the low diagnostic risk group shown as a ROC (Receiver Operating Characteristic) curve. BL – indicates beta-lactam, HtD time - time from hypersensitivity episode to allergologic diagnosis.
4. Discussion
Inglis et al. analyzed 5023 electronic databases with reported penicillin ADRs (adverse drug reaction). Among them, penicillin allergy was diagnosed in 4773 (95%) and intolerance in 250 (5%). The most reported drug was "penicillin," "penicillins" or "BL antibiotic" - in 3992 patients (79.5%), and among them amoxicillin was the most common 866 (17.2%). Among 4979 patients, about half of them – 2549 (50.7%) were classified as low risk, 1378 (27.4%) as high risk, while in 1052 (20.9%) the risk could not be assessed [35]. In a retrospective study by Albin et al. rash and unknown/undocumented hypersensitivity reaction to penicillins accounted more than half (57.2%) of the hypersensitivity symptoms reported by patients, urticaria 18.9%, angioedema 11.8%, and anaphylaxis 6.8%. At the same time, among patients reporting anaphylaxis, 92.4% had no medical records confirming the reaction [36]. Vyles et al. analyzed pediatric group of 500 patients, among them 380 (76%) children had symptoms of low-risk hypersensitivity to penicillins. The most reported symptoms were rash 466 (92.8%) and pruritus 203 (40.6%) patients. Among 120 children with at least one high-risk symptom, the most common manifestation of hypersensitivity was angioedema – 50 (10%) [37]. A similar study was conducted in pediatric group admitted to the emergency department due to hypersensitivity to cephalosporins. In 75 of 128 patients (58.6%), only low-risk symptoms were described, most common symptoms were skin rash and pruritus (73%) appearing at least 6 hours after taking the drug. In the high-risk group, the most common symptom was also a rash, but appearing within 6 hours of BL antibiotic administration [38].
A study by Touati et al. conducted between 1992 and 2018 at the Department of Allergology at the Montpellier Clinical Hospital included 476 patients who reported DHR (drug hypersensitivity reaction) after cephalosporin use. Among them, 83 patients reported anaphylactic shock, 85 reported anaphylaxis, and 308 reported "other" reactions, which included urticaria, angioedema, MPE, and severe cutaneous adverse reaction (SCAR) [39]. Anaphylaxis after cephalosporin administration is rare. In analysis by Macy et al. anaphylaxis was reported in 5 out of 901908 oral administrations of cephalosporins and in 8 out of 487630 parenteral administrations of cephalosporins [40].
In our study, as in the study cited above, patients reporting hypersensitivity to penicillins, mainly aminopenicillins, mostly belonged to the low-risk group, as well as patients who could not identify the specific "penicillin" causing the hypersensitivity. Over the past few decades, the use of parenteral penicillin’s significantly decreased, therefore the incidence of severe hypersensitivity, including anaphylaxis is rare [41]. On the contrary to the studies cited above, patients with a history of hypersensitivity to cephalosporins, including group A cephalosporins, were significantly more likely to be in the high-risk group. In our study, data regarding group A are similar with the results of a multicenter, retrospective, cohort study by Yang et al. In their study group I of cephalosporins (ceftriaxone, cefuroxime, cefepime, cefotacsime, ceftyzoxime) were the most common cause of anaphylaxis induced by cephalosporin administration [42]. In our study, patients reporting hypersensitivity to group C cephalosporins, mainly cefazolin, were mostly in the high-risk group. Similar observations were made by Bogas et al. in a study that examined a group of 184 patients, among whom 76 (41.3%) had confirmed hypersensitivity. Hypersensitivity was confirmed in all patients reporting anaphylactic shock and the majority reporting anaphylaxis, while in the group with mild reactions, all of the patients reporting skin rush and pruritus, were de-labeled [43].
In our analysis, patients who reported hypersensitivity to more than one BL antibiotic were significantly more often assigned in the low-risk group. This may be due to the simultaneously use of several antibiotics by patient during infection and the inability to determine which drug caused the reaction. This may be similar regarding non-BL antibiotics and other drugs (most often NSAIDs), although our analysis did not find significant differences between studied groups. Hypersensitivity to drugs from unrelated groups is a rare phenomenon [44,45].
A systematic review by Jagpal et al. revealed inaccuracies in the nomenclature and diagnosis of multiple drug intolerance syndrome (MDIS), multiple drug allergy syndrome (MDAS) and multiple drug hypersensitivity syndrome (MDHS) [44]. Blumenthal et al. described MDAS as a hypersensitivity reaction with a probable immune mechanism involved, to at least two drugs from different, unrelated groups. The incidence of MDAS was estimated at about 1%, while MDIS was estimated at about 6%. In contrast, Voelker et al. identified multidrug hypersensitivity as a risk factor for IgE mediated penicillin drug allergy in a pediatric population (OR =2.19, 95% CI 1.3-3.6, p=0.0019) [46]. The diagnosis of multidrug hypersensitivity, without verification, can be fatal for the patients, as in a situation requiring immediate intervention those patients may be left without antimicrobial treatment options.
In our study, patients reporting several episodes of hypersensitivity to BL were significantly more often assigned to low diagnostic risk group. In the high diagnostic risk group, only 15% reported more than one reaction after administration of BL antibiotic. Probably due to the fear of re-taking a drug that previously caused a hypersensitivity reaction and an unequivocal relationship between the drug and hypersensitivity symptoms, usually with a severe course. Study by Park et al. concluded that previous administration of any BL antibiotic significantly increased the risk of anaphylaxis in patients reporting hypersensitivity to cephalosporins (p=0.01), but not to penicillins (p=0.23). Interestingly, in multivariate regression, there was no statistical significance between re-exposure to BL antibiotic and increased risk of BL-induced anaphylaxis [47].
4.1. Characteristics of the Low Diagnostic Risk Group
A diagnostic tool based on anamnesis could help to identify a low-risk patients, who could be safely de-labeled. Complete work-up including skin and provocation tests would not be necessary in the abovementioned group. This would reduce the wait time for diagnosis in priority to high-risk patients.
Australian researchers presented a simple tool "PEN-FAST," which has been validated both internally and by researchers from the United States and Europe [30], [48]. In a multivariate analysis involving 622 subjects, four factors associated with penicillin hypersensitivity were summarized. They created mnemonic "PEN-FAST" in which "PEN" indicates penicillin hypersensitivity (2 points), "F" - time since the reaction within five years (2 points), "A" - anaphylaxis/angioedema (2 points), "S" - SCAR (2 points), and "T" - need for therapeutic intervention (1 point). Respondents with less than three points were classified as a low-risk patients. In internal validation, the tool’s sensitivity was estimated at 71%, specificity 79%, PPV 25%, and NPV 96% [30]. External validation in a group of 995 subjects from three centers showed a sensitivity of 70.4%-87.5%, and NPV of 84.9%-98.4% [49].
We attempted to create a model based on anamnesis alone, which would characterize low-risk patients using a multivariate logistic regression. In the univariate model, penicillin hypersensitivity, time from drug intake to symptoms >24 hours/unknown, long duration or unknown time from hypersensitivity episode to diagnosis, more than one episode of hypersensitivity to BL antibiotics were significant predictors of being assign to the low diagnostic risk group. Regarding the de-labeled group, the specificity of the tool was estimated at 90%, sensitivity 21.93%, NPV 72.04%, PPV 49.53%. In the multivariate model, the time from drug intake to symptom onset of more than 24 hours and more than one episode of hypersensitivity to BL antibiotics increased the chance of being in the low-risk group by several times. The NPV was 76% and the PPV was 68%.
Similar observations were described by Chiriac et al. in a study consisting of two parts, a retrospective analysis, based on which a predictive model was created, and a prospective study, in which prepared model was validated. Using logistic regression, sensitivity for the retrospective and prospective models was estimated at 51% and 60%, respectively, specificity at 75% and 80%, PPV at 40% and 57%, and NPV at 83% and 82%. The decision tree model presented high specificity, but low sensitivity <45%. Both methods were unable to accurately predict the occurrence of BL hypersensitivity to antibiotics [50].
In a multicenter Australian study, Stevenson et al. presented eight low-risk models. In the most precise model, which included isolated skin rash and a time from hypersensitivity reaction longer than one year, the sensitivity was 80.6%, specificity was 60.8%, and NPV was 94.7% [51].
Siew et al. identified a cohort of low-risk patients who could not remember the name of the BL antibiotic causing the hypersensitivity reaction, reported a history of no anaphylaxis, and had a hypersensitivity reaction at least one year before diagnosis. In this group, the medical history data had a comparable negative predictive value for the occurrence of type I hypersensitivity to BL antibiotics (98.4%), as negative skin test results (98.9%) [52].
The algorithm based on anamnesis proposed by Soria et al. showed high sensitivity (92.7%) with low specificity (35.8%) and NPV of 96.3% [53].
Devchand et al. developed a validated tool that can be used by non-allergist physicians to make further diagnostic decisions based on risk stratification. The tool takes into account data from the patient’s history and laboratory test results [31,54,55].
In a recently published study, Dunham et al. presented a digital tool designed to simplify decision-making for physicians from other specialties, in patients with a history of BL antibiotic hypersensitivity. The tool encourages appropriate antibiotic selection in groups at low and moderate risk groups, and to be extra cautious in high-risk groups [56].
Telemedicine is also usable in the risk stratification of BL antibiotic hypersensitivity. It does not completely replace diagnostics, but by identifying low-risk patients who can be safely de-labeled without an in-person visit, it can reduce waiting times to see a specialist and costs to the healthcare system [57,58].
Limitations of our analysis include its retrospective, single-center nature. Some complaints reported by patients, such as shortness of breath, are subjective are not verifiable, therefore those patients may have been misclassified into particular risk groups. Expanding the study with pediatric population would increase the value of this study. In conclusion, obtained data may improve the knowledge on risk stratification in patients hospitalized due to suspected BL hypersensitivity. Further research is needed to identify risk factors for BL antibiotic hypersensitivity and to enable the development of more precise, easily accessible diagnostic tools for removing the label of BL allergy. This would result in both health benefits for the patient and financial benefits for the healthcare system. The diagnostic tool based only on anamnesis, does not clearly identify low-risk patients, who could be safely de-labeled.
5. Conclusions
The tool enabling the identification of low diagnostic risk patients based on anamnesis is not sensitive enough, to de-label patients on its basis.
Author Contributions
Conceptualization, L.R, J.G; data curation, L.R. and J.G.; writing original draft preparation, L.R, B.R R. G, J.G.; writing—review and editing, L.R, B.R, R.G, J.G; supervision, J.G. All authors agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
Funding
The study was supported by grant PCN-2-091/N/0/K from the Medical University of Silesia, Katowice, Poland.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Patient consent was waived due to the retrospective nature of this study and the need for informed consent was waived. Patient confidentiality was maintained in the analysis, and the analysis was conducted using an anonymized dataset.
Data Availability Statement
All obtained and analyzed data are included in this article. Further enquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Doña, I.; Caubet, J.C.; Brockow, K.; Doyle, M.; Moreno, E.; Terreehorst, I.; Torres, M.J. An EAACI task force report: recognising the potential of the primary care physician in the diagnosis and management of drug hypersensitivity. Clin. Transl. Allergy 2018, 8, 16. [Google Scholar] [CrossRef] [PubMed]
- Zhou, L.; Dhopeshwarkar, N.; Blumenthal, K.G.; Goss, F.; Topaz, M.; Slight, S.P.; Bates, D.W. Drug allergies documented in electronic health records of a large healthcare system. Allergy 2016, 71, 1305–1313. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, K.G.; Peter, J.G.; Trubiano, J.A.; Phillips, E.J. Antibiotic allergy. Lancet 2019, 393, 183–198. [Google Scholar] [CrossRef] [PubMed]
- Khan, D.A.; Banerji, A.; Blumenthal, K.G.; Phillips, E.J.; Solensky, R.; White, A.A.; et al. Drug allergy: A 2022 practice parameter update. J. Allergy Clin. Immunol. 2022, 150, 1333–1393. [Google Scholar] [CrossRef]
- Trubiano, J.A.; Adkinson, N.F.; Phillips, E.J. Penicillin Allergy Is Not Necessarily Forever. JAMA 2017, 318, 201–220. [Google Scholar] [CrossRef]
- Sacco, K.A.; Bates, A.; Brigham, T.J.; Imam, J.S.; Burton, M.C. Clinical outcomes following inpatient penicillin allergy testing: A systematic review and meta-analysis. Allergy 2017, 72, 1288–1296. [Google Scholar] [CrossRef]
- West, R.M.; Smith, C.J.; Pavitt, S.H.; Butler, C.C.; Howard, P.; Bates, C.; et al. “Warning: allergic to penicillin”: association between penicillin allergy status in 2.3 million NHS general practice electronic health records, antibiotic prescribing and health outcomes. J. Antimicrob. Chemother. 2019, 74, 2075–2082. [Google Scholar] [CrossRef]
- Blumenthal, K.G.; Shenoy, E.S.; Varughese, C.A.; Hurwitz, S.; Hooper, D.C.; Banerji, A. Impact of a clinical guideline for prescribing antibiotics to inpatients reporting penicillin or cephalosporin allergy. Ann. Allergy Asthma Immunol. 2015, 115, 294–300.e2. [Google Scholar] [CrossRef]
- Lee, Y.; Bradley, N. Overview and Insights into Carbapenem Allergy. Pharm. 2019, 7, 110. [Google Scholar] [CrossRef]
- Trubiano, J.A.; Stone, C.A.; Grayson, M.L.; Urbancic, K.; Slavin, M.A.; Thursky, K.A.; et al. The Three C’s of Antibiotic Allergy – Classification, Cross-Reactivity and Collaboration. J. Allergy Clin. Immunol. Pract. 2017, 5, 1532. [Google Scholar] [CrossRef]
- Stone, C.A.; Trubiano, J.A.; Phillips, E.J. Testing Strategies and Predictors for Evaluating Immediate and Delayed Reactions to Cephalosporins. J. Allergy Clin. Immunol. Pract. 2021, 9, 435–444.e13. [Google Scholar] [CrossRef] [PubMed]
- Zagursky, R.J.; Pichichero, M.E. Cross-reactivity in β-Lactam Allergy. J. Allergy Clin. Immunol. Pract. 2018, 6, 72–81. [Google Scholar] [CrossRef] [PubMed]
- Romano, A.; Valluzzi, R.L.; Caruso, C.; Maggioletti, M.; Quaratino, D.; Gaeta, F. Cross-Reactivity and Tolerability of Cephalosporins in Patients with IgE-Mediated Hypersensitivity to Penicillins. J. Allergy Clin. Immunol. Pract. 2018, 6, 1662–1672. [Google Scholar] [CrossRef]
- Dhopeshwarkar, N.; Sheikh, A.; Doan, R.; Topaz, M.; Bates, D.W.; Blumenthal, K.G.; Zhou, L. Drug-Induced Anaphylaxis Documented in Electronic Health Records. J. Allergy Clin. Immunol. Pract. 2019, 7, 103–111. [Google Scholar] [CrossRef]
- Macy, E.; Contreras, R. Health care use and serious infection prevalence associated with penicillin “allergy” in hospitalized patients: A cohort study. J. Allergy Clin. Immunol. 2014, 133, 790–796. [Google Scholar] [CrossRef] [PubMed]
- Blumenthal, K.G.; Lu, N.; Zhang, Y.; Li, Y.; Walensky, R.P.; Choi, H.K. Risk of meticillin resistant Staphylococcus aureus and Clostridium difficile in patients with a documented penicillin allergy: population based matched cohort study. BMJ 2018, 361, k2400. [Google Scholar] [CrossRef]
- Huang, K.H.G.; Cluzet, V.; Hamilton, K.; Fadugba, O. The Impact of Reported Beta-Lactam Allergy in Hospitalized Patients With Hematologic Malignancies Requiring Antibiotics. Clin. Infect. Dis. 2018, 67, 27–33. [Google Scholar] [CrossRef]
- Li, M.; Krishna, M.T.; Razaq, S.; Pillay, D. A real-time prospective evaluation of clinical pharmaco-economic impact of diagnostic label of “penicillin allergy” in a UK teaching hospital. J. Clin. Pathol. 2014, 67, 1088–1092. [Google Scholar] [CrossRef]
- Picard, M.; Bégin, P.; Bouchard, H.; Cloutier, J.; Lacombe-Barrios, J.; Paradis, J.; Roches, A.D.; Laufer, B.; Paradis, L. Treatment of patients with a history of penicillin allergy in a large tertiary-care academic hospital. J. Allergy Clin. Immunol. Pract. 2013, 1, 252–257. [Google Scholar] [CrossRef]
- Jeffres, M.N.; Narayanan, P.P.; Shuster, J.E.; Schramm, G.E. Consequences of avoiding β-lactams in patients with β-lactam allergies. J. Allergy Clin. Immunol. 2016, 137, 1148–1153. [Google Scholar] [CrossRef]
- Stone, C.A.; Trubiano, J.; Coleman, D.T.; Rukasin, C.R.F.; Phillips, E.J. The challenge of de-labeling penicillin allergy. Allergy. 2020, 75, 273–288. [Google Scholar] [CrossRef] [PubMed]
- Wolfson, A.R.; Huebner, E.M.; Blumenthal, K.G. Acute care beta-lactam allergy pathways: approaches and outcomes. Ann. Allergy Asthma Immunol. 2019, 123, 16–34. [Google Scholar] [CrossRef]
- Torres, M.J.; Blanca, M.; Fernandez, J.; Romano, A.; Weck, A.; Aberer, W.; Brockow, K.; Pichler, W.J.; Demoly, P.; Enda, F.; et al. Diagnosis of immediate allergic reactions to beta-lactam antibiotics. Allergy 2003, 58, 961–972. [Google Scholar] [CrossRef] [PubMed]
- Romano, A.; Blanca, M.; Torres, M.J.; Bircher, A.; Aberer, W.; Brockow, K.; et al. ENDA; EAACI. Diagnosis of nonimmediate reactions to β-lactam antibiotics. Allergy 2004, 59, 1153–1160. [Google Scholar] [CrossRef] [PubMed]
- Demoly, P.; Adkinson, N.F.; Brockow, K.; Castells, M.; Chiriac, A.M.; Greenberger, P.A.; Khan, D.A.; Lang, D.M.; Park, H.; Pichler, W.; et al. International Consensus on drug allergy. Allergy 2014, 69, 420–437. [Google Scholar] [CrossRef]
- Romano, A.; Atanaskovic-Markovic, M.; Barbaud, A.; Bircher, A.J.; Brockow, K.; Caubet, J.C.; Celik, G.; Cernadas, J.; Chiriac, A.; Demoly, P.; et al. Towards a more precise diagnosis of hypersensitivity to beta-lactams — an EAACI position paper. Allergy 2020, 75, 1300–1315. [Google Scholar] [CrossRef]
- Stone, C.A., Jr.; Stollings, J.L.; Lindsell, C.J.; Dear, M.L.; Buie, R.B.; Rice, T.W.; Phillips, E.J. Risk-stratified Management to Remove Low-Risk Penicillin Allergy Labels in the ICU. Am. J. Respir. Crit. Care Med. 2020, 201, 1572–1575. [Google Scholar] [CrossRef]
- Blumenthal, K.G.; Huebner, E.M.; Fu, X.; Li, Y.; Bhattacharya, G.; Levin, A.S.; Mancini, C.M.; Slawski, B.R.; Banerji, A. Risk-based pathway for outpatient penicillin allergy evaluations. J. Allergy Clin. Immunol. Pract. 2019, 7, 2411–2414.e1. [Google Scholar] [CrossRef] [PubMed]
- Koo, G.; Yu, R.; Phillips, E.J.; Stone, C.A. Retrospective stratification of cephalosporin allergy label risk using validated penicillin allergy frameworks. J. Allergy Clin. Immunol. Pract. 2022, 10, 2472–2475.e1. [Google Scholar] [CrossRef]
- Trubiano, J.A.; Vogrin, S.; Chua, K.Y.L.; Bourke, J.; Yun, J.; Douglas, A.; Stone, C.A.; Yu, R.; Groenendijk, L.; Holmes, N.E.; et al. Development and Validation of a Penicillin Allergy Clinical Decision Rule. JAMA Intern. Med. 2020, 180, 1. [Google Scholar] [CrossRef]
- Devchand, M.; Urbancic, K.F.; Khumra, S.; Douglas, A.P.; Smibert, O.; Cohen, E.; Sutherland, M.; Phillips, E.J.; Trubiano, J.A. Pathways to improved antibiotic allergy and antimicrobial stewardship practice: The validation of a beta-lactam antibiotic allergy assessment tool. J. Allergy Clin. Immunol. Pract. 2019, 7, 1063–1065.e5. [Google Scholar] [CrossRef] [PubMed]
- Phillips, E.J.; Demoly, P.; Torres, M.J. Addressing beta-lactam allergy: A time for action. Allergy 2022, 77, 1091–1093. [Google Scholar] [CrossRef] [PubMed]
- Shenoy, E.S.; Macy, E.; Rowe, T.; Blumenthal, K.G. Evaluation and Management of Penicillin Allergy: A Review. JAMA 2019, 321, 188–199. [Google Scholar] [CrossRef] [PubMed]
- Romano, A.; Gaeta, F.; Valluzzi, R.L.; Maggioletti, M.; Zaffiro, A.; Caruso, C.; Quaratino, D. IgE-mediated hypersensitivity to cephalosporins: Cross-reactivity and tolerability of alternative cephalosporins. J. Allergy Clin. Immunol. 2015, 136, 685–691.e3. [Google Scholar] [CrossRef] [PubMed]
- Inglis, J.M.; Caughey, G.E.; Smith, W.; Shakib, S. Documentation of penicillin adverse drug reactions in electronic health records: inconsistent use of allergy and intolerance labels. Intern. Med. J. 2017, 47, 1292–1297. [Google Scholar] [CrossRef]
- Albin, S.; Agarwal, S. Prevalence and characteristics of reported penicillin allergy in an urban outpatient adult population. Allergy Asthma Proc. 2014, 35, 489. [Google Scholar] [CrossRef]
- Vyles, D.; Chiu, A.; Simpson, P.; Nimmer, M.; Adams, J.; Brousseau, D.C. Parent-Reported Penicillin Allergy Symptoms in the Pediatric Emergency Department. Acad. Pediatr. 2017, 17, 251–255. [Google Scholar] [CrossRef]
- Zembles, T.; Zhan, Y.; Chiu, A.; Brousseau, D.C.; Vyles, D. Cephalosporin allergy symptoms in children presenting to a pediatric emergency department. Ann. Allergy Asthma Immunol. 2021, 127, 259–260. [Google Scholar] [CrossRef]
- Touati, N.; Cardoso, B.; Delpuech, M.; Bazire, R.; El Kara, N.; Ouali, D.; Demoly, P.; Chiriac, A.-M. Cephalosporin Hypersensitivity: Descriptive Analysis, Cross-Reactivity, and Risk Factors. J. Allergy Clin. Immunol. Pract. 2021, 9, 1994–2000.e5. [Google Scholar] [CrossRef]
- Macy, E.; Contreras, R. Adverse reactions associated with oral and parenteral use of cephalosporins: A retrospective population-based analysis. J. Allergy Clin. Immunol. 2015, 135, 745–752.e5. [Google Scholar] [CrossRef]
- Macy, E.M.; Chen, L.H. The Incidence of Anaphylaxis Associated with Oral and Parenteral Penicillin-Class Antibiotic Exposures. J. Allergy Clin. Immunol. 2017, 139, AB33. [Google Scholar] [CrossRef]
- Yang, M.S.; Kang, D.Y.; Seo, B.; Park, H.J.; Park, S.Y.; Kim, M.; Park, K.H.; Koo, S.; Nam, Y.; Kim, S.; et al. Incidence of cephalosporin-induced anaphylaxis and clinical efficacy of screening intradermal tests with cephalosporins: A large multicenter retrospective cohort study. Allergy 2018, 73, 1833–1841. [Google Scholar] [CrossRef] [PubMed]
- Bogas, G.; Doña, I.; Dionicio, J.; Fernández, T.D.; Mayorga, C.; Boteanu, C.; Montañez, M.I.; Al-Ahmad, M.; Rondón, C.; Moreno, E.; et al. Diagnostic Approach of Hypersensitivity Reactions to Cefazolin in a Large Prospective Cohort. J. Allergy Clin. Immunol. Pract 2021, 9, 4421–4430.e4. [Google Scholar] [CrossRef]
- Jagpal, P.K.; Alshareef, S.; Marriott, J.F.; Thirumala Krishna, M. Characterization, epidemiology and risk factors of multiple drug allergy syndrome and multiple drug intolerance syndrome: A systematic review. Clin. Transl. Allergy. 2022, 12. [Google Scholar] [CrossRef]
- Blumenthal, K.G.; Li, Y.; Acker, W.W.; Chang, Y.; Banerji, A.; Ghaznavi, S.; Camargo, C.A.; Zhou, L. Multiple drug intolerance syndrome and multiple drug allergy syndrome: Epidemiology and associations with anxiety and depression. Allergy 2018, 73, 2012–2023. [Google Scholar] [CrossRef]
- Voelker, D.; D’Netto, M.; Park, M. Multiple drug allergies as a risk factor for IgE mediated penicillin drug allergy in a pediatric population. J. Allergy Clin. Immunol. 2021, 147, AB5. [Google Scholar] [CrossRef]
- Park, C.S.; Yang, M.S.; Kang, D.Y.; Park, H.J.; Park, S.Y.; Nam, Y.H.; Drug Allergy Work Group of, K.A.A.A.C.I.; et al. Risk factors of beta-lactam anaphylaxis in Korea: A 6-year multicenter retrospective adult case-control study. World Allergy Organ. J. 2021, 14. [Google Scholar] [CrossRef]
- Piotin, A.; Godet, J.; Trubiano, J.A.; Grandbastien, M.; Guénard-Bilbault, L.; de Blay, F.; Metz-Favre, C. Predictive factors of amoxicillin immediate hypersensitivity and validation of PEN-FAST clinical decision rule. Ann. Allergy Asthma Immunol. 2022, 128, 27–32. [Google Scholar] [CrossRef]
- Courtemanche, J.; Baril, L.; Clément, A.; Bédard, M.A.; Plourde, M.; Émond, M. Is it possible to identify patients at low risk of having a true penicillin allergy? CJEM 2022, 24, 366–368. [Google Scholar] [CrossRef]
- Chiriac, A.M.; Wang, Y.; Schrijvers, R.; Bousquet, P.J.; Mura, T.; Molinari, N.; Demoly, P. Designing Predictive Models for Beta-Lactam Allergy Using the Drug Allergy and Hypersensitivity Database. J. Allergy Clin. Immunol. Pract. 2018, 6, 139–148.e2. [Google Scholar] [CrossRef]
- Stevenson, B.; Trevenen, M.; Klinken, E.; Smith, W.; Yuson, C.; Katelaris, C.; Perram, F.; Burton, P.; Yun, J.; Cai, F.; et al. Multicenter Australian Study to Determine Criteria for Low-and High-Risk Penicillin Testing in Outpatients. J. Allergy Clin. Immunol. Pract. 2019, 8, 681–690. [Google Scholar] [CrossRef] [PubMed]
- Siew, L.Q.C.; Li, P.H.; Watts, T.J.; Thomas, I.; Ue, K.L.; Caballero, M.R.; Rutkowski, K.; Till, S.J.; Pillai, P.; Haque, R. Identifying Low-Risk Beta-Lactam Allergy Patients in a UK Tertiary Centre. J. Allergy Clin. Immunol. Pract. 2019, 7, 2173–2181.e1. [Google Scholar] [CrossRef]
- Soria, A.; Autegarden, E.; Amsler, E.; Gaouar, H.; Vial, A.; Francès, C.; Autegarden, J.-E. A clinical decision-making algorithm for penicillin allergy. Ann. Med. 2017, 49, 710–717. [Google Scholar] [CrossRef] [PubMed]
- Devchand, M.; Kirkpatrick, C.M.J.; Stevenson, W.; Garrett, K.; Perera, D.; Khumra, S.; Urbancic, K.; Grayson, M.L.; A Trubiano, J. Evaluation of a pharmacist-led penicillin allergy de-labelling ward round: a novel antimicrobial stewardship intervention. J. Antimicrob. Chemother. 2019, 74, 1725–1730. [Google Scholar] [CrossRef] [PubMed]
- Owens, R.; Sandoe, J.; Whyte, A.F.; Wilcock, M.; West, R.; Stonell, R.; Slatter, M.; Powell, N. A randomized evaluation of an antibiotic allergy assessment tool for supporting penicillin allergy de-labelling by non-allergists. Clin. Exp. Allergy. 2021, 51, 1246–1249. [Google Scholar] [CrossRef]
- Dunham, T.B.; Gardner, R.M.; Lippner, E.A.; Fasani, D.E.; Moir, E.; Halpern-Felsher, B.; Sundaram, V.; Liu, A.Y. Digital Antibiotic Allergy Decision Support Tool Improves Management of β-Lactam Allergies. J. Allergy Clin. Immunol. Pract. 2023, 11, 1243–1252.e6. [Google Scholar] [CrossRef]
- Wells, D.; DeNiro, K.L.; Ramsey, A. Telemedicine in Drug Hypersensitivity. Immunol. Allergy Clin. North. Am. 2022, 42, 323–333. [Google Scholar] [CrossRef]
- Allen, H.I.; Gillespie, P.; Vazquez-Ortiz, M.; Murphy, A.W.; Moylett, E.M. A cost-analysis of outpatient paediatric penicillin allergy de-labelling using telemedicine. Clin. Exp. Allergy 2021, 51, 495–498. [Google Scholar] [CrossRef]
| Single factor model | ||||
|---|---|---|---|---|
| Variable | p | OR | 95% CI | |
| Gender [F] | 0,22 | 1,56 | 0,77 | 3,19 |
| Age <45 vs ≥45 years old | 0,26 | 1,01 | 0,99 | 1,03 |
| BMI <25 vs ≥25 | 0,24 | 0,97 | 0,93 | 1,02 |
| SAR, PAR | 0,92 | 0,97 | 0,49 | 1,91 |
| Hypersensitivity to PN | < 0,001 | 3,08 | 1,52 | 6,27 |
| Hypersensitivity to CF | 0,07 | 0,60 | 0,35 | 1,04 |
| Hypersensitivity to >1 BL antibiotic | 0,5103 | 1,229 | 0,666 | 2,267 |
| Hypersensitivity to other drugs | 0,35 | 1,28 | 0,76 | 2,15 |
| Time from BL administration to symptoms <1hr | < 0,001 | 0,15 | 0,07 | 0,30 |
| Time from BL administration too symptoms ≥1h-24h | 0,59 | 0,83 | 0,43 | 1,63 |
| Time from BL administration to symptoms >24hrs | < 0,001 | 6,64 | 2,80 | 15,74 |
| Time from BL antibiotic administration to symptoms - unknown | 0,01 | 2,13 | 1,23 | 3,70 |
| >1 episode of hypersensitivity to BL antibiotic | 0,01 | 2,13 | 1,22 | 3,73 |
| HtD time ≥6 wks. - 6 months. | 0,16 | 0,45 | 0,15 | 1,37 |
| HtD time >6 months-1 year | 0,11 | 0,56 | 0,28 | 1,13 |
| HtD time – several years | 0,01 | 0,46 | 0,25 | 0,84 |
| HtD time – 10-20 years | 0,16 | 1,75 | 0,80 | 3,82 |
| HtD time – several decades | 0,05 | 2,21 | 1,00 | 4,86 |
| HtD time – unknown | 0,01 | 2,26 | 1,19 | 4,30 |
BL – indicates beta-lactam, CF - cephalosporins, HtD time - time from hypersensitivity episode to allergologic diagnosis, ns – non-significant, PAR - perennial allergic rhinitis, PN - penicillins, SAR - seasonal allergic rhinitis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



