
Submitted:
26 October 2024
Posted:
28 October 2024
You are already at the latest version
Abstract
Background/Objectives: Fats, although essential for the proper functioning of the body, have been linked to an increased risk of developing chronic diseases, especially cardiovascular disease. The aim of this study was to evaluate the intake of total fat, and its components (saturated, monounsaturated, polyunsaturated, and trans fats) in men and women aged 15 to 65 years of the urban population in eight Latin American countries. Methods: Survey data were collected for the ELANS, including 9218 subjects from Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, Peru, and Venezuela. Results: In general, 76.2% of the subjects consumed fat within normal ranges (20-35% of the total caloric value (TCV)). When analyzing its components, a majority of the subjects consumed saturated and polyunsaturated fats within the recommended ranges. However, 94.5% of the population does not comply with the recommended maximum intake of MUFA (10-20%) and only 57.5% comply with the intake recommendation for TFA (0 - 2%). Likewise, on average, women had a significantly higher intake of all types of fat compared to men. Finally, the average fat intake by age indicates that regardless of the age range, the consumption of all fats except MUFA and TRANS are within the recommended ranges, with MUFA being slightly below and TRANS above. Conclusions: Even though the fat intake of the population falls within the recommended range, it is necessary to improve the quality by favoring the consumption of MUFA and reducing the consumption of TRANS.
Keywords:
dietary fats
; dietary intake
; saturated fatty acids
; monounsaturated fatty acids
; polyunsaturated fatty acids
; trans fatty acids
; diet
; Latin America
; ELANS
1. Introduction
Dietary patterns encompass the balance, variety, and combination of foods and beverages that are routinely consumed. This includes all foods and beverages, whether prepared and consumed at home or outside the home [1]. Being so, that the WHO recommends the adoption of a healthy lifestyle that reduces the risk of being seriously ill or of early death. Within the healthy lifestyle, a healthy and balanced diet in macro and micronutrients is included.
Fats and lipids play a fundamental role in maintaining health. They are essential in the body’s energy reserve and are involved in important processes, such as the regulation of body temperature or the transport of nutrients, among others. Additionally, the quality and type of fat consumed can affect intellectual and mental capacity. High intake of saturated fats has been linked to cognitive decline, while consumption of polyunsaturated fatty acids has beneficial effects in their prevention. Thus, consuming diets with an adequate ratio (5:1) of omega-6:3 fatty acids are associated with better memory and a lower risk of cognitive decline [2]. On the other hand, lipids are key to assimilating certain vitamins and for metabolism to function properly, so their importance is very prominent. [3].
Among macronutrients, fat intake has long been a topic of interest and discussion in the scientific community. Early animal studies, dating back to the 1930s, reported a relationship between fat intake and the development of cardiovascular disease (CVD) [4]. A 1950s study by Keys et al. reinforced this interest by correlating a high fat intake with increased plasma cholesterol, which, in turn, increases the risk of developing CVD. This hypothesis was later reinforced by a seven-country study, which pointed out that saturated fats were at the center of the public health problem caused by CVD [5,6]. Contradictory messages from the scientific community have distorted the general public’s understanding of the importance of quality fat as opposed to quantity. Despite widespread views derived from early studies that fat is the “bad guy,” researchers and scientists now agree that the intake of quality fats is instrumental in maintaining human health [7]. Despite extensive studies spanning several decades, controversy still exists about the effects of the different types of fatty acids on human health. Particularly those of saturated fatty acid (SFA) in chronic diseases, with major emphasis on the risk of CVD [8].
Since the early 2000s, dietary recommendations have increasingly acknowledged the consequences of focusing on a low-fat diet. This has shifted mainstream views toward the importance of specific types of dietary fat. It is often reported that SFAs raise LDL cholesterol levels, while monounsaturated fatty acids (MUFA) and PUFAs generally lower LDL cholesterol levels, being so, that long-chain omega-3 fatty acids, such as eicosapentaenoic acid (EPA) (20:5n-3) and docosahexaenoic acid (DHA) (22:6n-3), are linked to lower triglyceride levels in hypertriglyceridemic patients and a reduced risk of developing coronary heart disease (CHD), while dietary trans-fatty acids are associated with higher LDL cholesterol levels [1,8]. However, recent studies have shown that high saturated fat intake tends to increase large LDL particles and/or decrease small LDL particles. Conversely, limited studies have found that diets rich in polyunsaturated fatty acids (PUFAs) decrease both large and small LDL particles, compared to diets high in saturated fats. However, higher-fat diets containing a mix of different fatty acids have shown no significant differences in LDL particle size [9].
On the other hand, trans fats, or trans-fatty acids (TFA), unsaturated fats derived from either industrial processes or natural sources, have been linked to an increased risk of CVD. Each year, more than 278,000 deaths worldwide are attributed to the consumption of industrial TFA. WHO guidelines advise that adults should limit their intake of TFA to less than 1% of their total daily energy, which equates to less than 2.2 grams per day for a diet of 2000 calories [10]. TFA are commonly found in processed foods like margarine, vegetable shortening, and ghee; fried foods, and various baked goods like cookies, and pies; as well as in many street and restaurant foods. Naturally occurring TFA are present in red meat and dairy products.
Considering the important role of fats in human health and disease processes, population dietary assessments should include a comprehensive analysis of fat intake, detailing both the total amount and the specific breakdown of each fatty acid. Excessive fat intake is linked to obesity and an increased risk of chronic diseases, while insufficient fat intake can lead to undernutrition, skin disorders, and immune system impairments [7].
Given the significant social impact of dietary advice, it is crucial that recommendations provided to the public are grounded in solid scientific evidence. Recent research has highlighted that the quality of fat and the replacement of certain fats are more critical for chronic disease prevention than the total fat intake.
Finally, rising obesity rates in Latin American countries are closely linked to poor-quality diets for a significant portion of the population, highlighting the importance of analyzing fat intake. The ELANS data offer a unique opportunity to gather reliable information, as the foundation for programs and policies, aimed at improving public education and enhancing population well-being. Therefore, this study aims to describe the consumption of total fats and their subtypes, identify their dietary sources, and assess adherence to the recommendations of international organizations across eight Latin American countries, while also exploring differences based on sociodemographic variables.
2. Materials and Methods
2.1. Study Design
The Latin American Nutrition and Health Survey (ELANS) is a household-based, multicenter, cross-sectional study of nutrition and health surveillance [11]. The aim of this study is to evaluate the nutritional intake, physical activity levels, and anthropometric data of its participants. The ELANS was carried out simultaneously in eight Latin American countries (Argentina, Brazil, Chile, Colombia, Costa Rica, Ecuador, Peru, and Venezuela), from September 2014 to July 2015. The study protocol was approved by the Institutional Review Boards (IRB) in each country, and by the Western Institutional Review Board (#20140605), it is registered at ClinicalTrials.gov (#NCT02226627). Moreover, the protocol was approved by the Institutional Review Boards (IRB) in each country. Prior of their involvement in the survey, all participants written informed consent/assent. To safeguard participants anonymity, numerical identification codes were used instead of names, and secure file sharing systems facilitated data transfer. The design and methodology of the ELANS study can be found on Fisberg et al. [11].
2.2. Sample
The study used a sample of 9,218 participants, aged 15 to 65 years, from urban populations across eight Latin American countries. A randomized, complex, multistage sampling process was employed, with data stratified by geographical region, sex, age, and socio-economic level (SEL). The sample size was calculated with a 95% confidence level and a margin of error of 3.49%. Sampling weights were applied for each country to ensure representativeness. SEL was assessed using country-specific questionnaires, developed in accordance with legislative requirements or established local standards. For a detailed overview of the study’s structure and methodology, refer to Fisberg et al. [11].
2.3. Dietary Assessment
Trained interviewers used a two-face-to-face, 24-hour dietary recall (R24h) to collect dietary intake data, including detailed information on all food and beverages, including alcoholic beverages, recipes, and supplements consumed. Following the Multiple Pass Method (MSM) [12], interviews were conducted on two non-consecutive days.
A photographic album illustrating common household utensils and portion sizes were employed to quantify reported dietary intakes, with each album tailored to the specific context of the respective country. Data collected was converted into grams and milliliters by nutritionists trained in standardized data transformation methodologies. Subsequently, these measurements were translated into energy units. A food-matching standardization procedure was conducted by trained dietitians in each country using the Nutrition Data System for Research (NDS-R) software, developed by the Nutrition Coordinating Center at the University of Minnesota [13].
Energy intake included the intake of not only macronutrients but also total sugars including intrinsic and added sugar. Usual water intake and energy from foods and beverages was determined using the Multiple Source Method (MSM) (http://msm.dife.de/), a web-based tool developed by the European Prospective Investigation into Cancer and Nutrition (EPIC) to estimate the usual intake of nutrients, foods (beverages) and energy consumed of the participants. The MSM technic is used to convert individual intakes from the R24H to usual intake distributions [14].
Energy intake included quantification of macro and micronutrient intake, where usual fat intake and energy from food were determined using the multi-source method (MSM), an online tool developed by the European Prospective Investigation into Cancer and Nutrition (EPIC). The MSM is employed to estimate participants’ typical intake of nutrients, foods, and energy. This technique, employed to convert individual intake data gathered from 24-hour dietary recall (R24H) sessions into distributions reflecting usual intake patterns, it facilitates a comprehensive assessment of dietary habits, enabling a more accurate understanding of nutritional intake among study participants.
The fat consumption record for this study included information on the type of fatty acid and cholesterol and the sources of fat intake. The types of fatty acids included were saturated, monounsaturated, polyunsaturated, and trans fatty acids.
Fat intake was assessed and evaluated against the US Institute of Medicine (IOM) Dietary Reference Intakes (DRI) standards [15], which establish an estimate of total fat of 20-35% of total intake of calories, or which an approximate of 10% should be coming from SFA, 6-11% of PUFA, and the remaining percentage from MUFA, which translate into ranges of frequent intake of 15 to 21 grams per day for women and 21 to 34 grams per day for men of SFA, 18 to 24 grams per day for women and 25 to 39 grams per day for men of MUFA, and 9 to 11grams per day for women and 12 to 17 grams per day for men PUFA, and <300 mg of cholesterol per day. There are no recommended values for trans-fat, as this should be near zero [15].
2.4. Statistical Analysis
Descriptive statistics analysis was done for continuous variables as means, standard error of the mean (SEM), and confidence intervals. Categorical measures are presented as counts and percentages. Analysis of variance tests were performed to assess whether there are significant differences in the behavior of continuous variables in subpopulations defined by qualitative variable categories. With the purpose of describing the consumption of total fats (TF), in terms of four of its most important components, SFA, MUFA, PUFA and TRANS fats, a decision tree was built based on the CHAID segmentation. In all cases, tests were performed with a statistical significance level of 0.05. Microsoft Excel® 2016 software and the IBM SPSS® version 25 statistical packages were used for data loading and analysis. To evaluate the effect of sociodemographic factors (country, SEL, gender and age groups) on fat intake, a multivariate analysis of variance (MANOVA) model was used, supported by the Wilks Lambda statistic. The percentage contribution of several food groups to total fat intake and each of its components was also obtained.
2.5. Ethics
The ELANS protocol, which was registered at Clinical Trials (#NCT02226627) and approved by the Western Institutional Review Board (#20140605), also received approval from the ethical review boards of the participating institutions. Participants provided informed consent for inclusion in the country-level study, and their confidentiality was maintained using identification codes instead of names. Data transfers were securely conducted through a file-sharing system.
3. Results
The sample characteristics are shown in Table 1. Overall, 9218 adults aged 15–65 completed the questionnaire. The sociodemographic characteristics of the participants, including age and socioeconomic status, across countries were included to assess the variables presented in Table 1.
The overall analysis of fat intake in the ELANS countries showed that 76.2% of the subjects consumed fat within normal ranges (20-35% of the total caloric value (TCV)). 18.9% consumed more fat than the recommended amounts, and 4.9% were below the recommended intake.
Breaking down fat consumption into its components, saturated fats (SFA), monounsaturated fats (MUFA), polyunsaturated fats (PUFA) and TRANS fats, it can be seen that most people consume saturated and polyunsaturated fats within the recommended ranges. However, it stands out that 94.5% of the population do not comply with the MUFA consumption recommendations and only 57.5% comply with the TRANS recommendations. [16] (Table 1)
When broken down by categories (SFA, MUFA, PUFA, and TFA), a majority of the subjects consumed saturated and polyunsaturated fats within the recommended ranges. However, it stands out that 94.5% of the population does not comply with the recommended maximum intake of MUFA (10-20%) and only 57.5% comply with the intake recommendation for TFA (0 - 2%) [16]
Regarding cholesterol intake, it was observed that 61.3% of the population met the consumption recommendation of <300 mg. (Table 1).
Detailed analysis of the intake for each fatty acid, revealed that regardless of country, age, sex, or socioeconomic status; the most consumed saturated fatty acids are the long-chain, palmitic (16:0), and stearic (18:0), followed by medium-chain lauric acid (12:0), and short chain butyric acid (4:0).
3.1. Average Daily Fat Intake by Sex and Age
The analysis revealed that, on average, women had a significantly higher intake of all types of fat compared to men. Notably, the 95% confidence intervals for the average intake of TF, as well SFA and PUFA, fell within the recommended ranges for both men and women (20%-35% for TF, 6%–11% for PUFA and 10% for SFA (Joint, F. A. O., 2010)). However, the average intake of MUFA was below the recommended range for both sexes (15-20%), while the intake of TFA exceeded the recommended levels (<1%) [15].

Table 2.
Percentage of energy from fat by sex.
| Variable | Sex | Media | Standard error | CI 95% | |
| Lower limit | Upper limit | ||||
| % Total fat | Male | 29,37 | 0,087 | 29,20 | 29,54 |
| Female | 30,30 | 0,082 | 30,14 | 30,46 | |
| Total | 29,85 | 0,060 | 29,74 | 29,97 | |
| % MUFA | Male | 9,71 | 0,035 | 9,64 | 9,78 |
| Female | 10,02 | 0,033 | 9,95 | 10,08 | |
| Total | 9,87 | 0,024 | 9,82 | 9,92 | |
| % PUFA | Male | 7,42 | 0,028 | 7,37 | 7,48 |
| Female | 7,70 | 0,028 | 7,65 | 7,76 | |
| Total | 7,57 | 0,020 | 7,53 | 7,61 | |
| % SFA | Male | 9,47 | 0,039 | 9,39 | 9,54 |
| Female | 9,92 | 0,037 | 9,85 | 9,99 | |
| Total | 9,70 | 0,027 | 9,65 | 9,76 | |
| % TRANS | Male | 1,06 | 0,011 | 1,04 | 1,08 |
| Female | 1,11 | 0,011 | 1,08 | 1,13 | |
| Total | 1,08 | 0,008 | 1,07 | 1,10 | |
The ANOVA test indicate that no significant differences are observed in the average consumption of MUFA type fats (p = 0.998), SAT (p = 0.205) and TRANS (p = 0.592), by age groups. However, it can be seen that the energy from PUFA shows a significant decrease as age increases (p = 0.000), finding that the Tukey test of multiple comparisons indicates a marked decrease between the age groups more advanced PUFA20-34 vs PUFA35-49 (p = 0.02) and PUFA35-49 vs PUFA50-65 (p = 0.04). Additionally, for all age groups, the 95% confidence intervals for the average percentage of energy provided by TF, SFA and PUFA indicate that their behavior is within the range of recommendations, while MUFA is below the recommendations, and that of TRANS fats is above the range of recommendations (Table 3).
Additionally, for all age groups, the 95% confidence intervals for the average intake of TF, SAT and PUFA indicate that their behavior is within the range of recommendations, while the consumption of MUFA fats is below the recommendations, and that of TRANS fats slightly above the range of the recommendations
3.2. Average Daily Fat Intake by Socioeconomic Level
Regarding fat consumption by socioeconomic level (SEL), the ANOVA test indicates that the average consumption of TF and all of its components is significantly differentiated by social class (p < 0.05), with an exception of PUFA-type fats (p = 0.270), which does not differ between social classes. Tukey’s ad-hoc tests show that the differences in the intake of TF, MUFA, SAT and TRANS between social classes are essentially determined by the fact that the middle class has a significantly higher intake when compared to the other classes TFmedium vs TFhigh (p = 0.000), TFmedium vs TFlow (p = 0.000), MUFAmedium vs MUFAhigh (p = 0.000), MUFAmedium vs MUFAlow (p = 0.000), SATmedium vs SAThigh (p = 0.000), SATmedium vs SATlow (p = 0.000); TRANSmedium vs. TRANShigh (p = 0.021), TRANSmedium vs. TRANSlow (p = 0.000).
Additionally for all social classes, the 95% confidence intervals for the average intake of TF, SAT and PUFA indicate that their behavior is within the range of recommendations, while the consumption of MUFA fats is below the recommendations, and that of TRANS fats, is above the range of the recommendations (Table 4).
3.3. Average Intake by Country
As shown in Figure 1, the majority of individuals (64.2% to 84.7%) meet the recommended intake levels, with Costa Rica standing out as the country where the population most adheres to the guidelines followed by Ecuador, and Argentina as the country with the lowest compliance. Notably, Argentina also has the highest percentage of individuals exceeding the recommended intake, followed by Colombia, Venezuela, and Brazil. In contrast, Peru has the highest percentage of individuals who tend to follow a low-fat diet (<20% TCV) (Figure 1).
Regarding PUFA intake, there is a notable pattern of high omega-6 fatty acid consumption and low omega-3 intake, resulting in an overall ω6:ω3 ratio of 10.2:1. Argentina has the highest ratio at 18.2:1, followed by Ecuador at 12.6:1 and Chile at 11.3:1. Conversely, Venezuela presents the most favorable ratio, with 7.1:1 (See Supplementary Material).
To describe the consumption of total fats, focusing on four key components—SFA, MUFA, PUFA, and TRANS fats—a decision tree was constructed using the CHAID segmentation algorithm (Figure 2). This resulted in 4 levels of segmentation and 14 terminal groups, as shown below.
The analysis reveals that 29.4% of the population consumes SFA, PUFA, and TRANS fats at levels within the recommended range, but their MUFA intake falls below the recommended levels. This group is followed by individuals who have excessive SFA and TRANS fat intake, with PUFA consumption within the recommended range, but with deficient MUFA intake (17%).
It should be highlighted that MUFA, in the decision tree, are identified as having the largest capacity to explain the total consumption of fats, because of the categories of consumption: low (< 13.6%), within (13.6-14.3%) or higher than (>= 14.3%) of the recommendations do establish the most important differences in the distribution of the participants according to their consumption of total fats (p=0.000)
Then, within the first level of segmentation there is a segment where almost all the participants in the study (91.3%) are characterized by a MUFA consumption below the recommendations. In this segment, the distribution shows a first small group with a low consumption of total fats (5.3%) a second large group with total fat consumption within the recommendations (82.4%) and a third group (12.3%) with a consumption of total fats above the recommendations. In the other two segments, with smaller number of individuals, when the MUFA consumption is within the recommendations, the consumption of total fats is high, whereas when MUFA intake is above the recommended values, total fats are also high.
In the second level of segmentation when the MUFA intake is below the recommendations, it is shown that saturated fats intake introduces a new segmentation in two more groups
Interestingly, in the segment where MUFA is below recommendations, SAT fats intake derives into another two-group segmentation: the first when MUFA is below the recommendations and the SAT are excessive, then a total fat intake is within the recommendations. The second when MUFA is below the recommended values and SAT are within the recommendations, total fats fall within the recommendations, confirming the interesting findings of MUFA consumption, and the distribution of the different quality of fats.
To assess the impact of sociodemographic factors (country, SEL, gender, and age group) on fat intake, a multivariate analysis of variance (MANOVA) was conducted, using Wilks’ Lambda statistic for support. Table 5 displays the significance of each sociodemographic factor, as measured by the Wilks’ Lambda statistic, in jointly explaining the behavior of the different types of fat under consideration. This allows for a comparison of the average intake patterns of SFA, MUFA, PUFA, and TRANS fats across the categories of each sociodemographic variable (gender, country, age group, and SEL) separately.
These results indicate that sociodemographic variables significantly affect the intake of the components of total fat, SFA, MUFA, PUFA, and TRANS.
Analyzing the contribution of energy coming from de components of Total fat by country and SEL, it can be observed that the averages of SFA and MUFA, in all countries, does not differ between upper and middle social classes, decreasing significantly in the lower social class. In Argentina, Brazil and Venezuela, the energy coming from PUFA in the lower social class is relatively higher, or similar, than the middle class; in Colombia, Ecuador and Chile there are not differences by social classes; Peru, in contrast to the other countries, presents a markedly different behavior: the energy contribution by the different components of fats is significantly different by social class, and it is also found in addition that the contribution determined by SFA is significantly lower than that corresponding as MUFA and PUFA, in all social classes. The energy provided by TRANS (not showed in the figure) is similar in all countries except in Costa Rica and Brazil, which are the countries with the highest level of TRANS fats (Figure 3).
3.4. Food Sources of Fats
Finally, it is important to consider not only the consumption of fats and their components but also the sources of these fats. Therefore, a detailed analysis of food sources is presented below.
Across the whole sample, the primary source of total fats are vegetable oils, contributing between 29.5% in Ecuador and 15.2% in Chile. This is followed by unprocessed meats (beef, poultry, pork, and lamb), which contributed an average of 16.9%, with Brazil and Ecuador showing the highest percentages (20.4% and 20.8%, respectively) and Chile the lowest (11.9%). Cheese is the third major contributor to total fat intake, with significant variation across countries, ranging from 18.4% in Venezuela to 3.5% in Peru (Table 7).
As shown in Table 8, unprocessed meats are the primary source of saturated fats in all countries except Venezuela, where cheese is the leading source. Across the entire sample, cheese ranks as the second major source of saturated fats, with contributions ranging from 6.9% in Peru to 32.9% in Venezuela. Additionally, vegetable oils and processed meats are significant contributors, each accounting for approximately 10% of saturated fat intake on average.
In the entire sample, monounsaturated fats primarily come from unprocessed meat, contributing an average of 23.6%. The second main source is vegetable oils, with contributions ranging from 4.1% in Colombia to 21.0% in Peru (Table 9).
The mean contribution of vegetable oils to polyunsaturated fats consumption is 38.6%, followed by a 7.8% of not-processed meat and 4.8% of salad dressings. (Table 10)
The primary sources of trans fats are unprocessed meats, which account for 24.8% of trans fat intake for the overall sample. Industrial trans fats are mainly contributed by breads, which provide an average of 12.6%, with a range from 5.8% in Venezuela to 24.6% in Peru. For more details, see Table 11.
4. Discussion
This study aimed to assess consumption of fatty acids, sources and adherence to the recommendations for the intake of different dietary fatty acids in eight Latin American countries. To our knowledge, this is the first time that fat intake, its sources and adherence to international recommendations have been evaluated at regional level. Our results indicates that while most of the population consumes fats within the recommended range, there are notable exceptions that warrant further attention.
4.1. Total and Saturated Fat
The data reveals that 76.2% of the overall ELANS’ population meets the recommendations for total fat intake, while 18.9% exceed the recommended levels, and a small percentage falls below the recommendations. Also, the segmentation according to the quality of consumed fat, shows an interesting pattern, reporting that when MUFA are low, total fats might be above the recommended values. This variability highlights the need for targeted nutritional interventions to address both overconsumption and underconsumption of fats. Additionally, 55.5% of the population consumes more SFA fatty acids than recommended. These findings align with those from previous studies, such as Harika et al., which reported that out of 40 countries analyzed, 25 (62.5%) met the recommended range of 20–35% of total caloric intake from fats, while 14 out of the remaining 15 countries had a mean total fat intake exceeding 35%. Furthermore, 67.5% of the countries had SFA intakes higher than the recommended level of >10% of total caloric intake [17].
Similarly, Eilander et al. (2015) reported that 62.5% of the 24 European countries studied met the recommendations for total fat intake, but only 8.3% adhered to the SFA recommendations. The recommendation to limit dietary SFA intake to less than 10% of TCV has been a central focus of dietary guidelines. However, recent research has called this recommendation into question, suggesting that restricting SFA intake may not yield significant health benefits, particularly concerning cardiovascular diseases and total mortality [18,19].
The Cochrane Database systematic review by Hooper et al. (2020) analyzed data from 11 randomized controlled trials involving 55,858 participants and found little to no effect of lowering saturated fat intake on mortality [20]. In contrast, a systematic review and dose-response meta-analysis of prospective cohort studies demonstrated that each additional 10 grams per day of SFA intake was associated with a 6% relative risk reduction for stroke [21]. Some studies have shown that replacing fats with carbohydrates is not necessarily associated with a lower risk of cardiovascular heart disease and may even be linked to increased total mortality, depending on the type of carbohydrates consumed. Conversely, replacing SFA with PUFAs has been shown to reduce the incidence of CVD [22]
A detailed analysis of saturated fatty acid intake reveals that long-chain saturated fatty acids (palmitic and stearic) are the most commonly consumed, followed by medium-chain lauric and short-chain butyric acids. This is significant because not all saturated fats have the same effects on serum cholesterol or LDL cholesterol [23]. For example, butter and other dairy fats high in myristic acid tend to raise LDL cholesterol to a greater extent than beef fat, which contains palmitic and stearic acids and has a lesser impact on LDL cholesterol [23,24,25].
4.2. Mono and Poliunsaturated Fat
Only 2.5% of individuals consume the recommended amount of MUFA fatty acids. This is concerning given the documented beneficial effects of MUFAs on cardiovascular health. For example, Schwingshackl et al. found that individuals in the highest tertile of the MUFA:SFA ratio experienced an overall risk reduction of 11% for all-cause mortality, 12% for cardiovascular mortality, 17% for stroke, and 9% for cardiovascular events compared to those in the lowest tertile [26]. However, it is important to highlight that a systematic review and meta-analysis published recently showed mixed results for monounsaturated fatty acids (MUFA) and polyunsaturated fatty acids (PUFA). Thirty studies reported an inverse association between various fats, including MUFA and PUFA, and all-cause mortality, indicating potential health benefits. However, 22 studies found a positive association, primarily linked to saturated fatty acids (SFA). The meta-analysis found no significant association between MUFA or PUFA intake and cardiovascular disease (CVD) or stroke morbidity, suggesting that while some studies indicate potential benefits, the overall impact of MUFA and PUFA on mortality and CVD events remains inconclusive [27].
The health effects of MUFAs can differ depending on their origin. Plant-derived MUFAs (MUFA-P) from sources such as olive oil, nuts, and salad dressings are associated with lower mortality. In contrast, animal-derived MUFAs (MUFA-A) from meat and dairy are linked to higher mortality. Replacing saturated fats, refined carbohydrates, or trans fats with MUFA-P has been shown to significantly reduce mortality. This is likely due to the bioactive nutrients and phytochemicals in plant sources, which improve metabolic health, lower blood pressure, and obesity, and enhance antioxidant and anti-inflammatory effects, thereby reducing the risk of CVD, diabetes, and all-cause mortality [27].
Despite most findings linking olive oil with a reduced risk of morbidity and mortality, it is not the primary source of MUFAs in this study. Instead, unprocessed meat accounts for 23.6% of MUFA consumption in the overall sample MUFAs; for example, in the case of oleic and palmitoleic acids, present in chicken meat are related to endogenous synthesis or intestinal absorption of the diet [28]. One hypothesis is that the association of fatty acids with coronary heart disease (CHD) may vary depending on the food source. For instance, dairy intake is often associated with a protective or neutral effect on CHD risk, whereas meat intake, particularly red or processed meat, is generally linked to a higher risk of CHD [29].
In contrast with MUFA intake, almost 75% of participants met the recommendations for PUFA consumption. Both MUFAS and PUFAS have been negatively associated with CVD [30], kidney diseases [31], mental disorders [32], and cognitive impairment [33].
Epidemiological studies have demonstrated that adequate intake of linoleic acid (LA) can reduce plasma LDL-C levels. Dietary intervention studies have shown that replacing 5% of dietary saturated fat (SFA) energy with ω-6 PUFAs can lower LDL-C by up to 10%, reduce the risk of coronary events by 13%, and decrease the risk of coronary death by 26% [34].
4.3. Trans Fat
It is noteworthy that 42.5% of the overall sample reported an intake of trans fats exceeding the recommended levels. This is concerning because numerous studies have established a direct association between the intake of industrial trans fats and the development of cardiovascular disease (CVD), prompting national regulations to restrict their presence in food products [35]. This high intake may be related to the consumption of processed foods and partially hydrogenated oils commonly used in the food industry.
4.4. Food Sources
The main sources of total fat were vegetable oils and unprocessed meat, followed by cheese and processed meats. Vegetable oils, which are rich in essential fatty acids (EFAs), phytosterols, tocopherols, carotenoids, and phenolics, offer significant health benefits. They contribute to cardiovascular health by improving lipid profiles and reducing inflammation, have potential anti-cancer effects, and support chronic disease prevention through their diverse biological activities [33,36].
Red and processed meats have been associated with potential health effects due to their saturated fatty acids and cholesterol content [37]. It is crucial to promote the consumption of high-quality monounsaturated fats, such as those found in olive oil and avocados.
An analysis of fat intake by country and socioeconomic level reveals notable differences. For example, Costa Rica has the highest compliance of fat intake recommendations, whereas Argentina showed the lowest compliance. Previous analysis has shown that Argentina also reported the highest added sugar intake [38] and the lower overall diet quality index [39]. Furthermore, trans fat intake is higher in lower socioeconomic levels across most countries, which may be linked to increased consumption of processed and affordable foods.
As shown and discussed above, consumption of fats in Latin America might not be what the audience expect: a diet high in fat, probably because people identify traditional foods as deep fried and loaded with oils, butter, whole dairy products and more. However, the evidence is showing an intake of total fats within the recommendations for the majority, but also a distribution of the type and quality of fats that is different than other populations. What is very interesting from the public health perspective is that taking into account the cultural traditions of Latin American population the new guidelines could explore giving more recommendations toward the use of the MUFA available in the region that people already use such as avocados or fish. Trying to incorporate for instance olive oil, might not be as successful as it is imported and expensive for households of the region.
It is relevant that emphasis should be made on the qualitative aspects of the guidelines instead of quantities for consumption. The new trends on guidelines are showing an important and better adherence when quality recommendations are made, instead of focusing on eliminating foods or diminishing the amounts of those.
This study has limitations such as being a cross-sectional study, therefore, being able to establish causality is not possible. However, it has some strengths as having two 24-hour recalls, the implemented standardized methodology across the eight countries and the use of the multiple pass method. In consequence, valuable information was obtained from this research, as it shows that the majority of the population have a fat consumption that falls between the limits of normal intake. It should be noted from the public policy perspective that some enhancement to the traditional sources of MUFA needs to be done in the region, while olive oil is not a traditional source of fats for Latin American population, avocado, fish, particularly sardines and some nuts are, but show low overall consumption. This is a relevant key issue for giving recommendations, building upon educational strategies and programs with the aim of enhancing a diverse, balanced, and healthier diet. It is true that people’s beliefs go toward “Latin American excessive consumption of fats” probably because the use of deep-frying methods or other traditional use of fats, however this study shows a need to better implement policies and programs that reinforce the consumption of quality traditional foods in our region, and we call the regional authorities to reflect on this issue and go for recommendations that include the interesting cultural culinary roots the region has.
5. Conclusions
The findings of this study highlight the need to improve the quality of fats in the diet of the Latin American population. Interventions should aim to increase MUFA intake while reducing SFA and trans-fat consumption. Additionally, it is crucial to consider the socioeconomic context when designing policies and educational programs to ensure that all sectors of society have access to healthy fat options.
Supplementary Materials
The following supporting information can be downloaded at website of this paper posted on Preprints.org, Table S1: Mean of the w6/w3 ratio by country.
Author Contributions
Conceptualization, M.H.-C., M.C.Y.G. and L.Y.C.S.; methodology, M.F., I.K., M.H.-C., M.C.Y.G., L.Y.C.S. and M.L.-J.; software, G.R. and M.V.; validation, P.H. and Y.S.; formal analysis, G.R. and M.V.; investigation, P.H. and Y.S.; data curation, G.R., M.V., P.H. and Y.S.; writing—original draft preparation, M.H.-C., M.C.Y.G., L.Y.C.S. and M.L.-J.; writing—review and editing, G.G., M.R.L.-D., A.R., M.F. and I.K.; supervision, M.H.-C. and M.L.-J.; project administration, M.H.-C. All authors have read and agreed to the published version of the manuscript.
Funding
The ELANS was initially supported by a scientific grant from the Coca-Cola Company and support from the Ferrero, Instituto Pensi/Hospital Infantil Sabara, International Life Science Institute of Argentina, Universidad de Costa Rica, Pontificia Universidad Católica de Chile, Pontificia Universidad Javeriana, Universidad Central de Venezuela/Fundación Bengoa, Universidad San Francisco de Quito, and Instituto de Investigación Nutricional de Peru. The founding sponsors had no role in study design, data collection, analyses, or interpretation; writing of the manuscript; or the decision to publish the results. A grant from Abbott was received for the analysis of choline and EFA. The sponsor was not involved in any of the stages of this research.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. The complete ELANS protocol was registered at Clinical Trials (#NCT02226627) and was approved by the Western Institutional Review Board (#20140605). Site-specific protocols were further approved by the ethical review boards of participating institutions.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available upon request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
We would like to thank the following individuals at each of the participating sites who made substantial contributions to the ELANS: Luis A. Moreno, Brenda Lynch, Mariela Jauregui, Alejandra Guidi, Luis Costa, Regina Mara Fisberg, Viviana Guajardo, and Gerson Ferrari. The following are members of the ELANS Study Group: Chairs: Mauro Fisberg and Irina Kovalskys; Co-chair: Georgina Gómez Salas; core group members: Attilio Rigotti, Lilia Yadira Cortés Sanabria, Martha Cecilia Yépez García, Rossina Gabriella Pareja Torres, and Marianella Herrera-Cuenca; Steering Committee: Berthold Koletzko, Luis A. Moreno, and Michael Pratt; Project Managers: Viviana Guajardo and Ioná Zalcman Zimberg; International Life Sciences Institute-Argentina: Irina Kovalskys, Viviana Guajardo, María Paz Amigo, Ximena Janezic, and Fernando Cardini; Universidad I Salud: Myriam Echeverry and Martin Langsman; Instituto Pensi-Hospital Infantil Sabara-Brazil and Federal University of Sao Paulo: Mauro Fisberg, Ioná Zalcman Zimberg, and Natasha Aparecida Grande de França; Pontificia Universidad Católica de Chile: Attilio Rigotti, Guadalupe Echeverría, Leslie Landaeta, and Óscar Castillo; Pontificia Universidad Javeriana Colombia: Lilia Yadira Cortés Sanabria, Luz Nayibe Vargas, Luisa Fernanda Tobar, and Yuri Milena Castillo; Universidad de Costa Rica: Georgina Gómez Salas, Rafael Monge Rojas, and Anne Chinnock; Universidad San Francisco de Quito-Ecuador: Martha Cecilia Yépez García, Mónica Villar Cáceres, and María Belén Ocampo; Instituto de Investigación Nutricional-Peru: Rossina Pareja Torres, María Reyna Liria, Krysty Meza, Mellisa Abad, and Mary Penny; Universidad Central de Venezuela: Marianella Herrera-Cuenca, Maritza Landaeta-Jiménez, Betty Méndez-Pérez, Maura Vásquez, Omaira Rivas, Carmen Meza, Guillermo Ramírez, and Pablo Hernández; accelerometry analysis: Priscila Bezerra.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Lichtenstein AH. Dietary fat and cardiovascular disease risk: quantity or quality? J Womens Health (Larchmt) [Internet]. 2003;12(2):109–14. [CrossRef]
- Martínez García RM, Jiménez Ortega AI, López-Sobaler AM, Ortega RM. Estrategias nutricionales que mejoran la función cognitiva. Nutr Hosp 2018;35(N.º Extra. 6):16-19. [CrossRef]
- Berdanier CD, Berdanier LA. Advanced nutrition: Macronutrients, micronutrients, and metabolism. 3a ed. Londres, Inglaterra: CRC Press; 2021.
- Gordon T. The diet-heart idea. Am J Epidemiol [Internet]. 1988;127(2):220–5. [CrossRef]
- Keys A. Atherosclerosis: a problem in newer public health. J Mt Sinai Hosp N Y. 1953;20(2):118-139.
- Keys A, Menotti A, Aravanis C, Blackburn H, Djordevic BS, Buzina R, et al. The seven countries study: 2,289 deaths in 15 years. Prev Med [Internet]. 1984;13(2):141–54. [CrossRef]
- Liu AG, Ford NA, Hu FB, Zelman KM, Mozaffarian D, Kris-Etherton PM. A healthy approach to dietary fats: understanding the science and taking action to reduce consumer confusion. Nutr J [Internet]. 2017;16(1):53. [CrossRef]
- Wang DD, Hu FB. Dietary fat and risk of cardiovascular disease: Recent controversies and advances. Annu Rev Nutr [Internet]. 2017;37:423–46. [CrossRef]
- Froyen E. The effects of fat consumption on low-density lipoprotein particle size in healthy individuals: a narrative review. Lipids Health Dis [Internet]. 2021;20(1):86. [CrossRef]
- WHO. (2024, January 24). Trans fat. World Health Organization (WHO). Retrieved August 6, 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/trans-fat.
- Fisberg M, Kovalskys I, Gómez G, Rigotti A, Cortés LY, Herrera-Cuenca M, et al. Latin American Study of Nutrition and Health (ELANS): rationale and study design. BMC Public Health [Internet]. 2015;16(1). [CrossRef]
- Moshfegh AJ, Rhodes DG, Baer DJ, Murayi T, Clemens JC, Rumpler WV, et al. The US Department of Agriculture Automated Multiple-Pass Method reduces bias in the collection of energy intakes. Am J Clin Nutr [Internet]. 2008;88(2):324–32. [CrossRef]
- Previdelli AN, Gómez G, Kovalskys I, Fisberg M, Cortés LY, Pareja RG, et al. Prevalence and determinants of misreporting of energy intake among Latin American populations: results from ELANS study. Nutr Res [Internet]. 2019;68:9–18. [CrossRef]
- Harttig U, Haubrock J, Knüppel S, Boeing H, on behalf of the EFCOVAL Consortium. The MSM program: web-based statistics package for estimating usual dietary intake using the Multiple Source Method. Eur J Clin Nutr [Internet]. 2011;65(S1):S87–91. [CrossRef]
- Institute of Medicine (IOM). Dietary Reference Intakes for Energy, Carbohydrate, Fiber, Fat, Fatty Acids, Cholesterol, Protein, and Amino Acids. Washington, DC: The National Academies Press;2005. [CrossRef]
- Schwingshackl, L., Zähringer, J., Beyerbach, J., Werner, S. S., Nagavci, B., Heseker, H., Koletzko, B., Meerpohl, J. J., & International Union of Nutritional Sciences (IUNS) Task force on Dietary Fat Quality. A Scoping Review of Current Guidelines on Dietary Fat and Fat Quality. Annals of nutrition & metabolism, 2021;77(2), 65–82. [CrossRef]
- Harika RK, Eilander A, Alssema M, Osendarp SJM, Zock PL. Intake of fatty acids in general populations worldwide does not meet dietary recommendations to prevent coronary heart disease: a systematic review of data from 40 countries. Ann Nutr Metab [Internet]. 2013;63(3):229–38. [CrossRef]
- Eilander A, Harika RK, Zock PL. Intake and sources of dietary fatty acids in Europe: Are current population intakes of fats aligned with dietary recommendations?: European fatty acid intake and sources. Eur J Lipid Sci Technol [Internet]. 2015;117(9):1370–7. [CrossRef]
- Astrup A, Magkos F, Bier DM, Brenna JT, de Oliveira Otto MC, Hill JO, et al. Saturated fats and health: A reassessment and proposal for food-based recommendations. J Am Coll Cardiol [Internet]. 2020;76(7):844–57. [CrossRef]
- Hooper L, Martin N, Jimoh OF, Kirk C, Foster E, Abdelhamid AS. Reduction in saturated fat intake for cardiovascular disease. Cochrane Database Syst Rev [Internet]. 2020;5:CD011737. Disponible en: http://dx.doi.org/10.1002/14651858.CD011737.pub2 Update in: Cochrane Libr [Internet]. 2020;8. [CrossRef]
- Kang Z-Q, Yang Y, Xiao B. Dietary saturated fat intake and risk of stroke: Systematic review and dose-response meta-analysis of prospective cohort studies. Nutr Metab Cardiovasc Dis [Internet]. 2020;30(2):179–89. [CrossRef]
- Sacks FM, Lichtenstein AH, Wu JHY, Appel LJ, Creager MA, Kris-Etherton PM, et al. Dietary fats and cardiovascular disease: A presidential advisory from the American Heart Association. Circulation [Internet]. 2017;136(3):e1–23. Disponible en: http://dx.doi.org/10.1161/CIR.0000000000000510. Erratum in: Circulation [Internet]. 2017;136(10):e195. [CrossRef]
- Hunter JE, Zhang J, Kris-Etherton PM. Cardiovascular disease risk of dietary stearic acid compared with trans, other saturated, and unsaturated fatty acids: a systematic review. Am J Clin Nutr [Internet]. 2010;91(1):46–63. [CrossRef]
- Mensink RP, Katan MB. Effect of dietary fatty acids on serum lipids and lipoproteins. A meta-analysis of 27 trials. Arterioscler Thromb [Internet]. 1992;12(8):911–9. [CrossRef]
- Teicholz N. A short history of saturated fat: the making and unmaking of a scientific consensus. Curr Opin Endocrinol Diabetes Obes [Internet]. 2023;30(1):65–71. [CrossRef]
- Schwingshackl L, Hoffmann G. Monounsaturated fatty acids, olive oil and health status: a systematic review and meta-analysis of cohort studies. Lipids Health Dis [Internet]. 2014;13(1):154. [CrossRef]
- Ma Y, Zheng Z, Zhuang L, Wang H, Li A, Chen L, et al. Dietary macronutrient intake and cardiovascular disease risk and mortality: A systematic review and dose-response meta-analysis of prospective cohort studies. Nutrients [Internet]. 2024;16(1). [CrossRef]
- Dal Bosco A, Cartoni Mancinelli A, Vaudo G, Cavallo M, Castellini C, Mattioli S. Indexing of fatty acids in poultry meat for its characterization in healthy human nutrition: A comprehensive application of the scientific literature and new proposals. Nutrients [Internet]. 2022;14(15):3110. [CrossRef]
- Vissers LET, Rijksen J, Boer JMA, Verschuren WMM, van der Schouw YT, Sluijs I. Fatty acids from dairy and meat and their association with risk of coronary heart disease. Eur J Nutr [Internet]. 2019;58(7):2639–47. [CrossRef]
- Zhen J, Liu S, Zhao G, Peng G, Xu A, Li C, Jun W, Cheung BMY. Impact of healthy lifestyles on risk of hypertension in the Chinese population: finding from SHUN-CVD study. Family Practice. 2023;40:737–741. [CrossRef]
- Mazidi M, Kengne AP, Siervo M, Kirwan R. Association of dietary intakes and genetically determined serum concentrations of mono and poly unsaturated fatty acids on chronic kidney disease: Insights from dietary analysis and Mendelian randomization. Nutrients [Internet]. 2022;14(6):1231. [CrossRef]
- Gao X, Su X, Han X, Wen H, Cheng C, Zhang S, et al. Unsaturated fatty acids in mental disorders: An umbrella review of meta-analyses. Adv Nutr [Internet]. 2022;13(6):2217–36. [CrossRef]
- Chen X, Maguire B, Brodaty H, O’Leary F. Dietary patterns and cognitive health in older adults: A systematic review. J Alzheimers Dis [Internet]. 2019;69(2):595–6. [CrossRef]
- Marangoni F, Agostoni C, Borghi C, Catapano AL, Cena H, Ghiselli A, et al. Dietary linoleic acid and human health: Focus on cardiovascular and cardiometabolic effects. Atherosclerosis [Internet]. 2020;292:90–8. [CrossRef]
- Oteng A-B, Kersten S. Mechanisms of Action of trans Fatty Acids. Adv Nutr [Internet]. 2020;11(3):697–708. [CrossRef]
- Tian M, Bai Y, Tian H, Zhao X. The chemical composition and health-promoting benefits of vegetable oils-A review. Molecules [Internet]. 2023;28(17). [CrossRef]
- Møller SP, Mejborn H, Christensen AI, Biltoft-Jensen A, Thygesen LC. Meat consumption, stratified by dietary quality, and risk of heart disease. Br J Nutr [Internet]. 2021;126(12):1881–7. [CrossRef]
- Kovalskys I, Cavagnari BM, Favieri A, Zonis L, Guajardo V, Gerardi A, et al. Total and added sugars consumption in Argentina: Their contribution to daily energy intake. Results from Latin American Study of Nutrition and Health (ELANS). Nutr Diet [Internet]. 2019;76(3):313–20. [CrossRef]
- Gómez G, Cavagnari BM, Brenes JC, Quesada D, Guajardo V, Kovalskys I; Grupo ELANS. Calidad y diversidad de la dieta en la población urbana de Argentina [Diet quality and diversity in the urban population of Argentina]. Medicina (B Aires). 2022;82(1):81-90.
Figure 1.
Percentage of energy from fat by country.
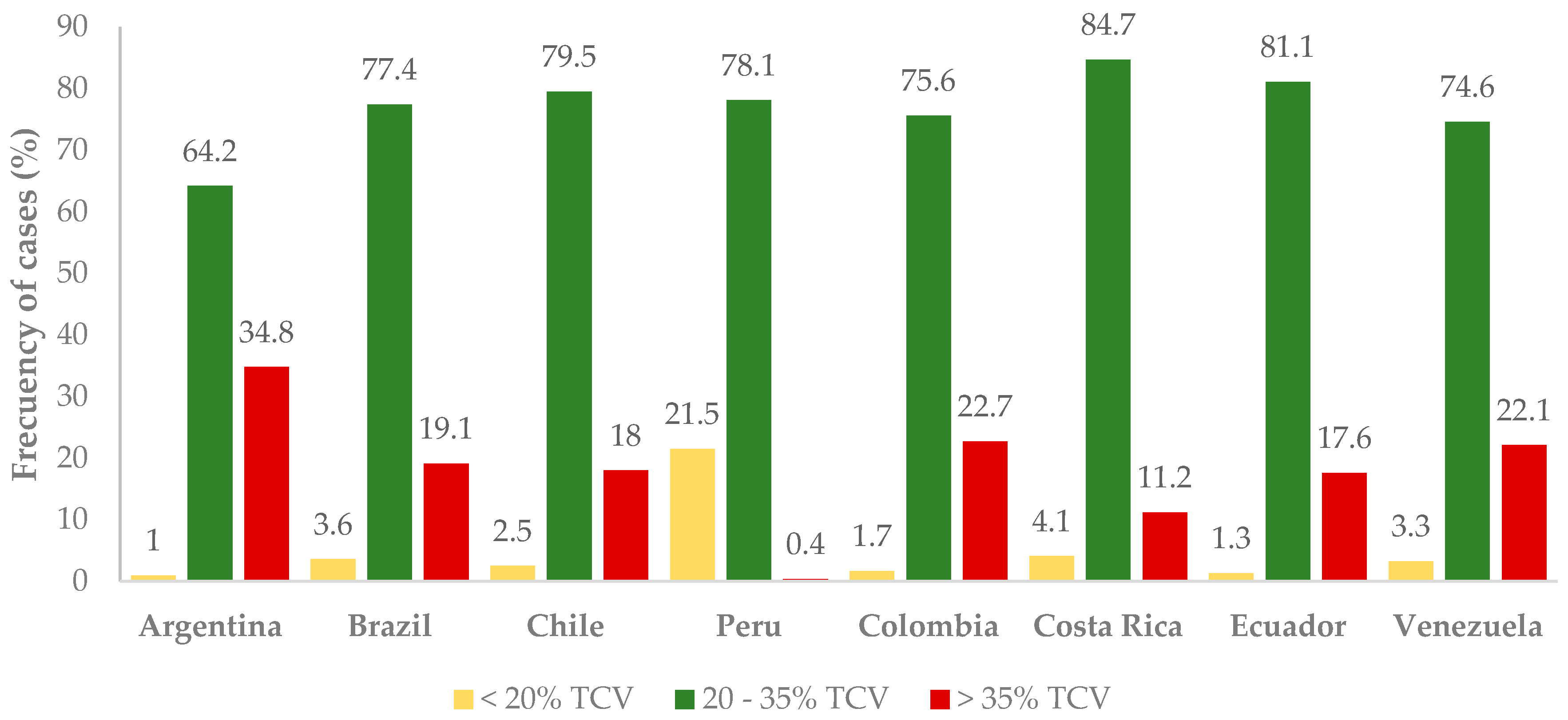
Figure 2.
CRT Tree for fat intake adequacy in three level.
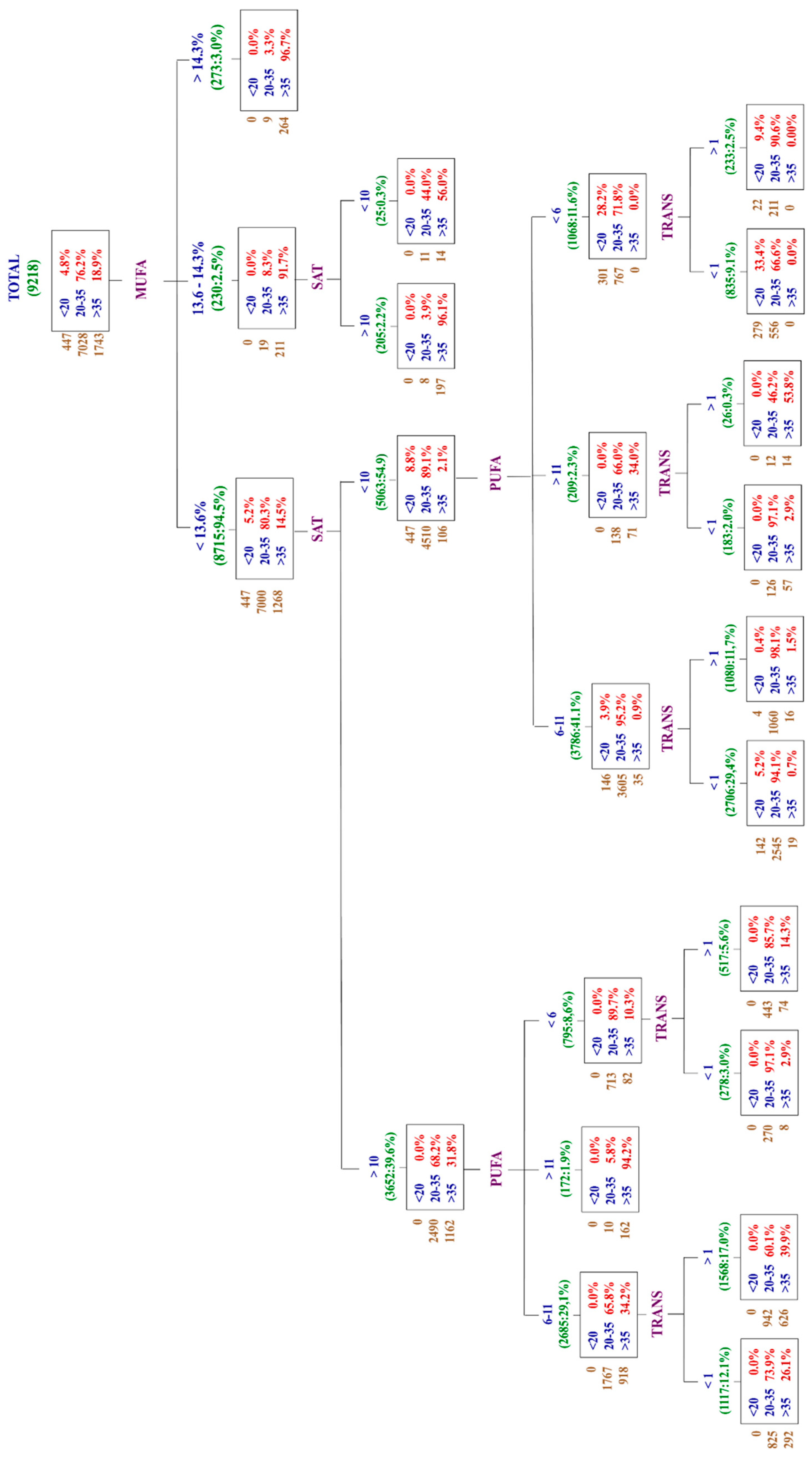
Figure 3.
Percentage of energy from fat by country and socioeconomic level.
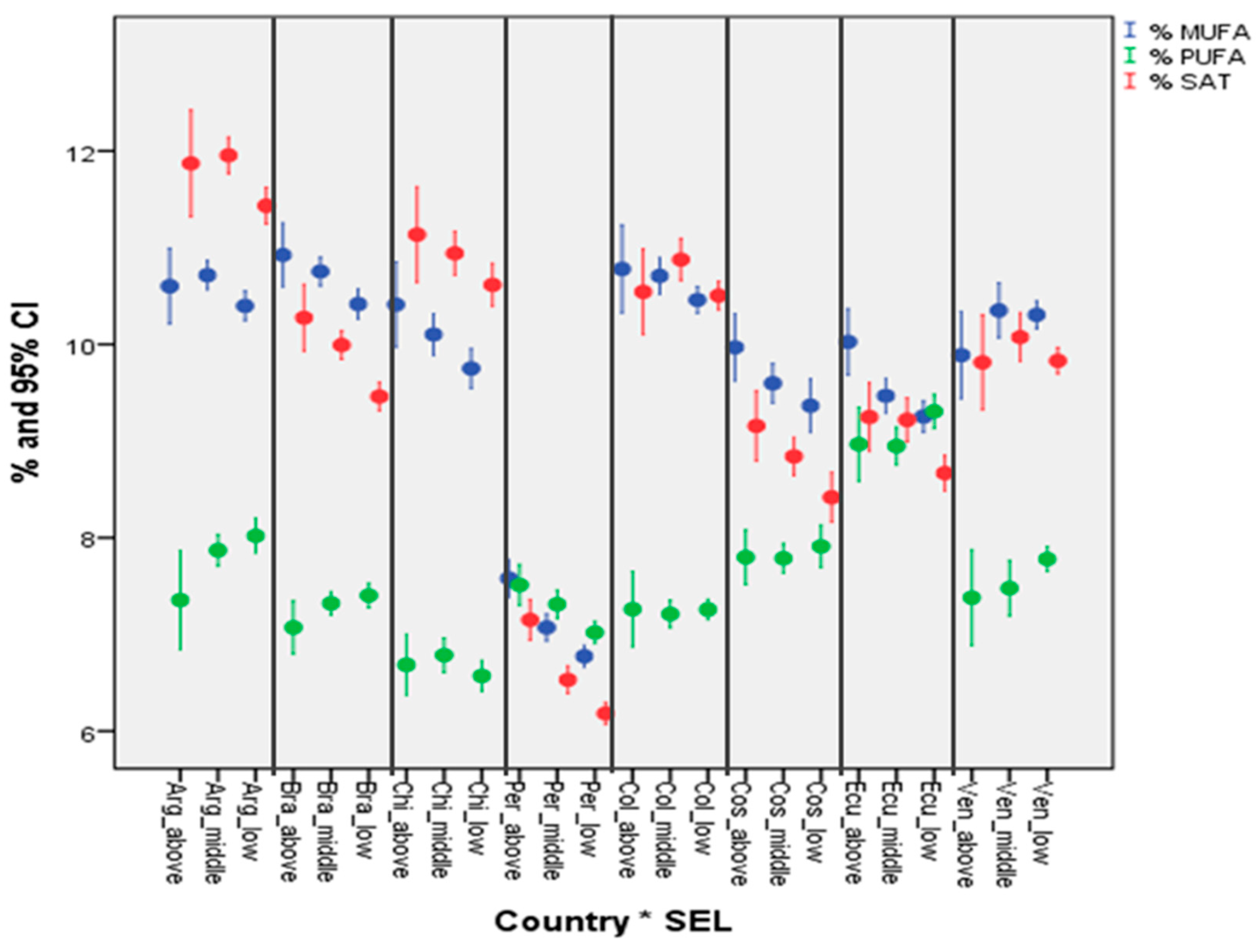
Table 1.
Participants (n, %) meeting the recommended dietary intake for fats as percentage of total energy intake.
Table 1.
Participants (n, %) meeting the recommended dietary intake for fats as percentage of total energy intake.
| Recommendation | n | % | |
|---|---|---|---|
| % total fat | < 20 % | 447 | 4,8 |
| 20–35 % | 7028 | 76,2 | |
| > 35 % | 1743 | 18,9 | |
| % SFA | < 10% | 5112 | 55,5 |
| > 10% | 4106 | 44,5 | |
| % MUFA | < 13,6% | 8715 | 94,5 |
| 13,6 - 14,3% | 230 | 2,5 | |
| > 14,3% | 273 | 3,0 | |
| % PUFA | < 6% | 1891 | 20,5 |
| 6 - 11% | 6893 | 74,8 | |
| > 11% | 434 | 4,7 | |
| % TRANS | < 1% | 5303 | 57,5 |
| > 1% | 3915 | 42,5 | |
| Cholesterol | < 300 mg | 5652 | 61,3 |
| > 300 mg | 3566 | 38,7 |
Table 3.
Percentage of energy from fat by age group.
| Variable | Sex | Media | Standard error | CI 95% | |
| Lower limit | Upper limit | ||||
| % Total fat | 15 - 19 | 30,24 | 0,160 | 29,93 | 30,56 |
| 20 - 34 | 29,95 | 0,097 | 29,76 | 30,14 | |
| 35 - 49 | 29,73 | 0,114 | 29,51 | 29,96 | |
| 50 - 65 | 29,60 | 0,134 | 29,33 | 29,86 | |
| Total | 29,85 | 0,060 | 29,74 | 29,97 | |
| % MUFA | 15 - 19 | 9,87 | 0,065 | 9,74 | 10,00 |
| 20 - 34 | 9,87 | 0,039 | 9,79 | 9,95 | |
| 35 - 49 | 9,87 | 0,045 | 9,78 | 9,96 | |
| 50 - 65 | 9,88 | 0,055 | 9,77 | 9,99 | |
| Total | 9,87 | 0,024 | 9,82 | 9,92 | |
| % PUFA | 15 - 19 | 7,77 | 0,054 | 7,66 | 7,87 |
| 20 - 34 | 7,66 | 0,032 | 7,60 | 7,73 | |
| 35 - 49 | 7,52 | 0,037 | 7,45 | 7,59 | |
| 50 - 65 | 7,33 | 0,044 | 7,24 | 7,42 | |
| Total | 7,57 | 0,020 | 7,53 | 7,61 | |
| % SFA | 15 - 19 | 9,77 | 0,072 | 9,63 | 9,92 |
| 20 - 34 | 9,67 | 0,043 | 9,58 | 9,75 | |
| 35 - 49 | 9,66 | 0,052 | 9,56 | 9,76 | |
| 50 - 65 | 9,79 | 0,061 | 9,67 | 9,91 | |
| Total | 9,70 | 0,027 | 9,65 | 9,76 | |
| % TRANS | 15 - 19 | 1,10 | 0,023 | 1,05 | 1,14 |
| 20 - 34 | 1,07 | 0,012 | 1,05 | 1,10 | |
| 35 - 49 | 1,10 | 0,015 | 1,07 | 1,12 | |
| 50 - 65 | 1,08 | 0,018 | 1,05 | 1,12 | |
| Total | 1,08 | 0,008 | 1,07 | 1,10 | |
Table 4.
Percentage of energy intake from fat by socioeconomic level.
| Variable | SES | Media | Standard error | CI 95% | |
| Lower limit | Upper limit | ||||
| % Total fat | Low | 29,40 | 0,182 | 29,04 | 29,75 |
| Middle | 30,28 | 0,095 | 30,10 | 30,47 | |
| High | 29,62 | 0,085 | 29,46 | 29,79 | |
| Total | 29,85 | 0,060 | 29,98 | 29,97 | |
| % MUFA | 15 - 19 | 9,69 | 0,075 | 9,54 | 9,84 |
| 20 - 34 | 10,03 | 0,038 | 9,96 | 10,11 | |
| 35 - 49 | 9,78 | 0,034 | 9,72 | 9,85 | |
| Total | 9,87 | 0,024 | 9,82 | 9,92 | |
| % PUFA | 15 - 19 | 7,52 | 0,062 | 7,40 | 7,64 |
| 20 - 34 | 7,54 | 0,031 | 7,48 | 7,60 | |
| 35 - 49 | 7,60 | 0,028 | 7,54 | 7,65 | |
| Total | 7,57 | 0,020 | 7,53 | 7,61 | |
| % SFA | 15 - 19 | 9,40 | 0,083 | 9,24 | 9,56 |
| 20 - 34 | 9,97 | 0,044 | 9,88 | 10,06 | |
| 35 - 49 | 9,56 | 0,037 | 9,49 | 9,64 | |
| Total | 9,70 | 0,027 | 9,65 | 9,76 | |
| % TRANS | 15 - 19 | 1,09 | 0,030 | 1,03 | 1,14 |
| 20 - 34 | 1,16 | 0,014 | 1,13 | 1,19 | |
| 35 - 49 | 1,03 | 0,009 | 1,01 | 1,05 | |
| Total | 1,08 | 0,008 | 1,07 | 1,10 | |
Table 5.
Effect of each sociodemographic factor on daily fat intake.
| Effect | Value | F | dof hipotesis | dof error | Sig |
|---|---|---|---|---|---|
| Sex | 0,982 | 42,7 | 4 | 9159 | 0,000 |
| SES | 0,988 | 13,4 | 8 | 18318 | 0,000 |
| Age | 0,991 | 6,8 | 12 | 24233 | 0,001 |
| Country | 0,512 | 240,4 | 28 | 33025 | 0,000 |
| Sex * country | 0,994 | 2,1 | 28 | 33025 | 0,001 |
| Age * country | 0,987 | 1,4 | 84 | 36180 | 0,007 |
| SES * country | 0,988 | 2,0 | 56 | 35629 | 0,000 |
Table 7.
Percentual contribution of food groups to total fats consumption (%).
| Food group | Argentina | Brazil | Chile | Colombia | Costa Rica | Ecuador | Peru | Venezuela | ELANS |
|---|---|---|---|---|---|---|---|---|---|
| Vegetable oils | 18.4 | 19.6 | 15.2 | 17.4 | 23.8 | 29.5 | 28.5 | 21.2 | 21.7 |
| Not-processed meat | 15.4 | 20.4 | 11.9 | 18 | 16 | 20.8 | 15.3 | 17.6 | 16.9 |
| Cheese | 9.1 | 4.0 | 8.3 | 4.2 | 5.2 | 7.7 | 3.5 | 18.4 | 7.5 |
| Processed meats | 7.6 | 5.1 | 6.5 | 5.8 | 10.8 | 4.4 | 9.0 | 8.3 | 7.2 |
| Refine grains (Breads and pasta) | 12.6 | 4.4 | 9.4 | 2.5 | 2.7 | 3.6 | 2.9 | 3.4 | 5.2 |
| Chips, Popcorn and others snacks | 6.0 | 6.8 | 9.6 | 7.0 | 3.5 | 2.4 | 1.5 | 1.7 | 4.8 |
| Eggs | 4.5 | 2.6 | 4.2 | 5.8 | 4.2 | 2.9 | 5.7 | 3.2 | 4.1 |
| Margarine | 0.0 | 11.0 | 2.4 | 4.2 | 3.8 | 1.9 | 1.6 | 7.3 | 4.0 |
| Butter | 5.3 | 4.0 | 8.6 | 3.8 | 1.7 | 3.7 | 0.0 | 0.0 | 3.4 |
| Milk, Whole and Whole Milk Products | 2.1 | 5.5 | 1.7 | 6.7 | 2.0 | 3.0 | 3.5 | 2.6 | 3.4 |
Table 8.
Percentual contribution of food groups to saturated fatty acids consumption (%).
| Food group | Argentina | Brazil | Chile | Colombia | Costa Rica | Ecuador | Peru | Venezuela | ELANS |
|---|---|---|---|---|---|---|---|---|---|
| Not-processed meats | 16.6 | 24.7 | 11.1 | 20.4 | 18.1 | 26.4 | 24.9 | 19.3 | 20.2 |
| Cheese | 15.9 | 7.6 | 14.5 | 7.0 | 9.7 | 14.6 | 6.9 | 32.9 | 13.6 |
| Vegetable oils | 5.5 | 8.9 | 5.5 | 7.9 | 11.2 | 11.8 | 17.0 | 10.4 | 9.8 |
| Processed Meat | 10.1 | 9.8 | 12.5 | 12.4 | 13.2 | 8.2 | 4.0 | 6.5 | 9.6 |
| Milk and milk products | 3.4 | 9.2 | 4.1 | 11.4 | 5.5 | 7.9 | 9.6 | 5.4 | 7.0 |
| Butter | 9.5 | 7.4 | 15.2 | 7.0 | 3.0 | 0.0 | 2.3 | 0.0 | 5.5 |
| Breads, Refined Grain | 5.1 | 3.6 | 8.8 | 1.7 | 2.0 | 8.0 | 2.4 | 2.2 | 4.2 |
| Eggs | 4.0 | 2.4 | 3.6 | 5.2 | 4.3 | 3.1 | 6.3 | 3.1 | 4.0 |
| Cakes, pies and cookies | 5.1 | 1.5 | 2.4 | 1.0 | 2.9 | 2.5 | 2.8 | 1.2 | 2.4 |
| Margarine | 6.5 | 0.0 | 0.0 | 2.6 | 2.7 | 1.1 | 1.4 | 2.5 | 2.1 |
Table 9.
Percentual contribution of food groups to monounsaturated fatty acids consumption (%).
| Food group | Argentina | Brazil | Chile | Colombia | Costa Rica | Ecuador | Peru | Venezuela | ELANS |
|---|---|---|---|---|---|---|---|---|---|
| Not-processed meat | 24.8 | 29.8 | 15.5 | 27.2 | 20.4 | 26.1 | 27.8 | 17.3 | 23.6 |
| Vegetable oils | 12.2 | 16.6 | 11.2 | 4.1 | 16.7 | 21.0 | 20.9 | 14.0 | 14.6 |
| Processed meat | 6.3 | 6.9 | 8.1 | 8.1 | 10.7 | 6.2 | 2.1 | 4.3 | 6.6 |
| Cheese, Processed | 8.0 | 3.4 | 6.7 | 2.7 | 3.7 | 6.2 | 2.9 | 14.2 | 6.0 |
| Eggs, Regular | 5.5 | 3.1 | 4.9 | 6.6 | 4.9 | 3.7 | 7.3 | 3.7 | 4.9 |
| Fats, margarine | 0.0 | 7.2 | 2.8 | 5.1 | 5.4 | 3.1 | 1.4 | 13.5 | 4.8 |
| Breads, White Bread, Regular | 4.2 | 2.4 | 5.1 | 1.7 | 1.3 | 3.1 | 0.0 | 1.4 | 2.4 |
| Butter, Regular | 4.3 | 2.9 | 6.7 | 2.0 | 0.0 | 2.4 | 0.0 | 0.0 | 2.3 |
| Avocado | 0.0 | 0.0 | 9.2 | 1.3 | 1.9 | 1.1 | 2.9 | 0.0 | 2.1 |
| Bread, white, sweet bread, regular | 1.2 | 0.0 | 0.0 | 0.0 | 0.0 | 0.0 | 2.1 | 10.8 | 1.8 |
Table 10.
Percentual contribution of food groups to PUFA consumption (%).
| Food group | Argentina | Brazil | Chile | Colombia | Costa Rica | Ecuador | Peru | Venezuela | ELANS |
|---|---|---|---|---|---|---|---|---|---|
| Vegetable oils | 48.7 | 42.0 | 40.2 | 38.6 | 25.9 | 13.2 | 52.2 | 48.0 | 38.6 |
| Not-processed meat | 5.8 | 7.2 | 6.0 | 8.0 | 7.2 | 8.9 | 11.1 | 8.2 | 7.8 |
| Salad Dressing | 8.4 | 2.9 | 9.3 | 3.6 | 3.8 | 1.9 | 4.1 | 3.9 | 4.8 |
| White Bread | 5.1 | 3.2 | 9.6 | 4.7 | 4.0 | 4.8 | 3.6 | 3.0 | 4.7 |
| Fars, margarine | 11.8 | 2.6 | 5.5 | 2.6 | 1.3 | 1.6 | 6.4 | 4.0 | |
| Processed meat | 2.8 | 2.5 | 4.4 | 2.2 | 3.2 | 1.2 | 1.7 | 2.2 | 2.5 |
| Eggs, Regular | 2.6 | 1.4 | 2.6 | 3.4 | 2.1 | 1.3 | 2.5 | 1.7 | 2.2 |
| Potato Chips | 1.3 | 1.4 | 0.0 | 3.1 | 0.8 | 0.7 | 0.8 | 0.0 | 1.0 |
| Crackers, | 2.5 | 0.0 | 0.0 | 0.8 | 1.4 | 0.8 | 1.4 | 1.1 | 1.0 |
| Vegetable shortening | 0.0 | 0.0 | 0.0 | 3.3 | 1.1 | 0.0 | 0.9 | 2.6 | 1.0 |
Table 11.
Percentual contribution of food groups to trans fats consumption (%).
| Food group | Argentina | Brazil | Chile | Colombia | Costa Rica | Ecuador | Peru | Venezuela | ELANS |
|---|---|---|---|---|---|---|---|---|---|
| Not processed meat | 26.5 | 28.3 | 14.0 | 25.6 | 19.5 | 31.5 | 24.0 | 29.0 | 24.8 |
| Breads | 12.5 | 10.9 | 24.0 | 9.0 | 1.8 | 11.8 | 24.6 | 5.8 | 12.6 |
| Cheese | 7.1 | 4.6 | 6.4 | 3.2 | 6.6 | 11.8 | 5.3 | 19.0 | 8.0 |
| Vegetable oils | 5.1 | 3.1 | 6.0 | 9.1 | 8.2 | 7.6 | 10.1 | 6.3 | 6.9 |
| Margarine | 2.1 | 20.6 | 0.0 | 9.0 | 0.0 | 6.1 | 0.0 | 17.5 | 6.9 |
| Butter | 7.0 | 5.0 | 10.5 | 4.8 | 1.7 | 6.7 | 1.8 | 0.0 | 4.7 |
| Cakes and cookies | 9.2 | 0.0 | 4.9 | 0.0 | 11.8 | 1.6 | 3.5 | 2.8 | 4.2 |
| Milk and milk products | 0.0 | 4.9 | 2.4 | 7.4 | 2.6 | 3.2 | 4.6 | 2.5 | 3.4 |
| Processed meat | 2.7 | 1.4 | 4.3 | 3.4 | 9.2 | 3.4 | 0.0 | 1.4 | 3.2 |
| Vegetable shortening | 0.0 | 0.0 | 2.6 | 7.9 | 2.3 | 0.0 | 4.2 | 5.8 | 2.8 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



