
Submitted:
25 October 2024
Posted:
28 October 2024
You are already at the latest version
Abstract
Background: Infections caused by S. aureus strains encoding Panton-Valentine leukocidin (PVL-SA) have become increasingly relevant in community settings and can cause severe conditions in pediatric populations. We present a pediatric case of invasive disease caused by PVL-SA and provide a literature review of severe manifestations caused by these strains in children. Methods: A PubMed search (February 2024) evidenced studies that included relevant clinical outcomes, diagnostics, and treatments, excluding cases of asymptomatic infection or adult populations. Logistical multivariate analysis was used to find predictors of the need for intensive care. Results: A 10-year-old boy came to the attention of our Pediatric Infectious Diseases Unit with fever, chest pain, and tachypnea. A rapid worsening of his clinical conditions was observed, with the development of necrotizing pneumonia, osteomyelitis, deep vein thrombosis (DVT), and multiple abscesses. Blood cultures confirmed the presence of PVL-producing methicillin-resistant S. aureus (MRSA). The initial treatment included linezolid and ceftaroline and was later adjusted to clindamycin, daptomycin, and fosfomycin, with clinical improvement. Discussion: Our review collected 36 articles, including 156 pediatric cases of severe PVL-SA infection. Bacteremia was present in 49% of cases, lung infection in 47%, and osteomyelitis in 37%. The presence of pulmonary localization was predictive of the need for intensive care, O.R. 25.35 (7.46 - 86.09; p<0.001). Anti-toxin molecules were used in about half the cases where information on treatment was reported. Our report highlights the capacity of PVL-SA to cause life-threatening complications in children, while also discussing the full range of its clinical spectrum and the most effective therapeutic approaches.
Keywords:
Panton-Valentine leukocidin (PVL)
; Staphylococcus aureus (S. aureus)
; methicillin-resistant Staphylococcus aureus (MRSA)
; pediatric infections
; necrotizing pneumonia
; osteomyelitis
; deep vein thrombosis (DVT)
; anti-toxin treatment
1. Background
Staphylococcus aureus (S. aureus) is a Gram-positive bacterium that frequently colonizes both human and animal skin and mucous membranes. It is the second bacterium, after Escherichia coli (E. coli), most commonly responsible for community-acquired bacteremia [1]. Further, S. aureus is the pathogen most often implicated in nosocomial infections and a significant cause of death in hospitalized patients [2]. The morbidity and mortality of S. aureus are mainly ascribable to the presence of genes for resistance to a variety of antibiotics, including the most effective and widely used anti-staphylococcal drugs. Until the mid-1990s, methicillin-resistant S. aureus (MRSA) infections were limited to hospitals, primarily affecting vulnerable individuals. However, over the past few decades, MRSA outbreaks have been reported in healthy individuals with no connection to healthcare settings. The presence of asymptomatic carriers facilitates the persistence and dissemination of staphylococci resistant to the most used antibiotics, especially in pediatric populations. Healthy carriers appear to be more at risk of developing invasive infections than non-carriers.
S. aureus can cause relatively benign skin infections such as folliculitis and furunculosis and life-threatening conditions such as deep-seated abscesses, osteomyelitis, pneumonia, endocarditis, and sepsis. Further, S. aureus can cause toxin-mediated diseases, such as toxic shock syndrome (TSS), staphylococcal scalded skin syndrome (SSSS), and food poisoning. Panton-Valentine leukocidin (PVL) is one of the main virulence factors of S. aureus, and it has become increasingly relevant over the past decade. PVL-producing strains of S. aureus (PVL-SA) tend to cause more severe and harder-to-treat conditions and can spread rapidly in community settings where people spend time in close contact with one another, such as in schools and sports events. We present a severe case of invasive disease caused by PVL-SA and provide a scoping literature review of invasive infections caused by these bacteria in pediatric populations.
2. Results
2.1. Case Report
In June 2023, a previously healthy 10-year-old boy was admitted to the Emergency Room due to pain in his left knee that appeared after a football match. An X-ray was performed to rule out fractures, and, after immobilization of the limb, the boy was discharged. Only two days later, the child was again admitted to the Emergency Room, due to the onset of fever, chest pain, and tachypnea, and subsequently transferred to the Pediatric Infectious Diseases Unit.
Upon admission, the patient was febrile (temperature 38.5°C) and tachypneic, with a respiratory rate of 65 breaths per minute (bmp). Physical examination revealed a reduction in vesicular breath sounds at the base of the right lung, and a diffuse hyporesonance on percussion across all fields of the left lung. The abdomen was soft but tender to deep palpation. The left lower limb appeared painful, warm, and immobile.
Blood tests showed a white blood cell count (WBC) of 13.24 x 10^3/µL, with a neutrophil count of 12.22 x 103/µL, and a C-reactive protein (CRP) level of 52.77 mg/dL. A contrast-enhanced chest CT scan documented severe bilateral pneumonia.
On contrast-enhanced CT of the left femur, the presence of an effusion at the knee joint was documented, along with irregularities of the distal femoral metaphysis and liponecrosis of the distal third of the vastus medialis.
Color-Doppler ultrasound of the lower limbs showed a sub-occlusive thrombosis of the left posterior tibial, popliteal, superficial femoral, and common femoral veins, as well as thrombosis of the right posterior tibial vein. However, an extensive investigation of the patient’s coagulation profile revealed no genetically determined coagulopathy.
Antibiotic treatment with linezolid and ceftaroline was initiated, together with heparin.
A bronchoscopy with bronchoalveolar lavage (BAL) was performed and evidenced blood traces, aligned with the presence of necrotizing pneumonia. The BAL sample culture revealed the presence of MRSA, which was also isolated from blood cultures. The presence of genes encoding Panton-Valentine Leukocidin (PVL) was evidenced through polymerase chain reaction (PCR).
On the sixth day of hospitalization, the patient underwent a magnetic resonance imaging (MRI) scan of the left lower limb, which documented the presence of osteomyelitis of the femoral diaphysis, arthritis of the knee, and extensive supra- and subfascial femoral abscess collections. The positron emission tomography (PET) scan also revealed osteomyelitis of the proximal right tibial epiphysis.
Immunological investigations were normal, including immunoglobulins, IgG subclasses, and lymphocyte subpopulations.
Due to the anticipated long treatment duration and in light of worsening anemia, linezolid and ceftaroline were discontinued, and clindamycin, daptomycin, and fosfomycin were initiated. The first was introduced because of its anti-toxin effect, and the latter two were added to ensure effective osteoarticular and pulmonary foci clearance. This change had a positive outcome with progressive normalization of inflammation markers.
After a 4-week long antibiotic treatment, a follow-up chest CT was performed, and a reduction of the focal lung lesions was observed. However, pain and reduced mobility of the left lower limb persisted. Treatment was continued for an additional 4 weeks and upon improvement of clinical conditions, the boy was discharged after administration of a single dose of dalbavancin (18 mg/kg). A follow-up MRI, performed about two months after discharge, showed improvement in the femoral bone structure.
Notably, on the third day of hospitalization of our patient, his seventeen-year-old brother, a professional wrestler, was admitted to our unit because of fever associated with widespread pustular lesions on his trunk and limbs. The culture of the drained material yielded PVL-SA. Upon screening of the household, PVL-SA was evidenced from nasopharyngeal swabs of the patient’s sister and cousin. All family members received antibiotic treatment to eradicate bacterial colonization, prevent relapses, and resolve this familiar outbreak.
2.2. Literature Review
The search yielded 927 results without filters. After the application of filters, 408 results remained. The main reasons for exclusion were the non-eligibility of article types or population, the inability to extract data regarding pediatric populations or subgroups of children with PVL-SA infections, and the lack of relevance to the research question (studies that did not focus on PVL-SA infections). Thirty-six studies were therefore included in the final selection (Figure 1).
The main clinical-epidemiological data gathered from the selected studies are summarized in Table 1.
The collective number of cases gathered from the included studies is 156. In 56 cases, gender was not specified. Of the remaining cases, 72 were boys (72%) and 28 were girls (28%). The mean age of the 137 patients for whom information was available is 5,9 years. Some authors reported aggregated data with group means and this subsample is composed of 82 children. The mean age in this subgroup is 5.08 years (range 0.72 to 9.06 years), with a weighted standard deviation of 3.36 years. As for the group of individual patients, the mean age is 7.12 years (range 0 to 17 years), with a median of 8.3 years, and an interquartile range (IQR) of 0.875 to 12 years.
PVL was evidenced from MRSA strains in 61 cases (39%), and from MSSA strains in 95 cases (61%). Children most likely contracted the infection in the area where they were treated, except for 4 cases, where a history of recent travel was mentioned. In particular, 36% of cases were observed in Europe, 33% in Africa, 22% in Asia, and 4% and 5% in North and South America, respectively (Figure 2).
Immune compromise affected 21 children out of 89 cases where data were reported (23%). Comorbidities were present in 48 cases out of 108 where information was available (34%).
PVL-SA was identified from a variety of samples based on clinical presentation: nasal swab (n=6), blood samples (n=76), drained fluid or surgical samples (n=86), broncho-alveolar lavage (n=18), sputum culture (n=25). The affected organs and systems, with relative frequencies, are summarized in Table 2.
Information on complications such as deep vein thrombosis (DVT) and pulmonary embolism (PE) was extractable in 137 cases. Deep vein thrombosis (DVT) was reported in 9 cases (6%), and pulmonary embolism (PE) in 6 cases (4%).
In 24% of cases (n=37) the infection affected multiple systems. Lung foci and osteomyelitis were both present in 13 cases, and pulmonary and SST infections coexisted in 16 cases. In 11 cases, all three systems were affected.
Information on hospitalization length was infrequently reported (n=68, 44% of cases). Among these cases, the mean length of hospital stay was 23 days, ranging from 1 to 88 days. Information on the infective status of the patient’s family members was reported in 18 cases (11%). Of these, in 11 cases (61%), some family members were infected as well, and in the remaining 7 cases (39%), the patient’s relatives were unaffected.
Thirty-four patients out of 63 cases where this information was reported (54%) needed intensive care. The presence of pulmonary localization was predictive of the need for intensive care, O.R. 25.35 (7.46 - 86.09; p<0.001).
Treatment was detailed in 61 cases (39%). Of these cases, in 35 cases (57%) molecules with anti-toxin action were included during the treatment course.
Information on outcomes, including possible sequelae and relapses, was reported in most cases (n=143, 92%). In 71% of cases (n=102) a full recovery was described, or there was no mention of any sequelae or relapses. Fifteen children (10%) recovered with sequelae, and 23 deceased (16%). In six cases (4%), patients recovered after one or more relapses.
The reported sequelae included the following manifestations: venous insufficiency and stenosis of the iliac vein, amputation (n=2), chronic osteomyelitis (n=2) and femoral necrosis, resolving hemiplegia, hemiparesis, unspecified functional impairment of the limbs, post-intensive care syndrome with reduced lung capacity and critical illness polyneuropathy, growth arrest (n=2), pathological fracture, and suicidality.
3. Discussion
The case we describe is a stark example of the potential for acute and aggressive onset in PVL-SA infections. Our patient was a previously healthy child who, after being initially discharged with a leg cast, returned to the hospital within 48 hours with deep vein thrombosis (DVT), a serious complication of PVL-associated infection. This highlights the capacity of PVL-SA to have a sudden onset with life-threatening complications. The boy’s condition progressed to bilateral necrotizing pneumonia, osteomyelitis of the left femur and right tibia, as well as a deep-seated abscess, all within a short period.
At the same time, this report serves as a reminder of the broad clinical spectrum associated with PVL-SA infections, ranging from mild presentations to life-threatening diseases. In contrast with our patient’s aggressive course, his older brother experienced only localized skin abscesses, and both his younger sister and cousin were asymptomatic carriers. This variability we observed within a single family illustrates the width of the clinical expressivity of PVL-SA infection.
The reported case further highlights an important risk factor for PVL-SA infection: involvement in skin-to-skin contact sports. In fact, the boy’s older brother, who was likely the primary carrier who transmitted the infection to the rest of the family, is a professional wrestler. Of the cases included in our review, a history of sports activities was reported four times (rugby [16,23], basketball and soccer [36,37]), and a recent travel history was mentioned in 5 instances [17,18,30,34]. Risk factors for PVL-SA infection are poor hygiene practices, compromised skin integrity, recent antibiotic use, and crowded living conditions, such as those that occur in care institutions, prisons, conflict-zone shelters, nurseries and schools. Of the cases in our review where gender was specified, 72% were boys. This could reflect the greater socialized tendency in boys to engage in contact sports or play that exposes them to skin-to-skin contact and a higher risk of superficial tissue injuries.
PVL was first described in 1894 by Van de Velde [39] and it consists of two proteins (LukS-PV and LukF-PV), capable of assembling into an exotoxin on the cell cytoplasmic membrane, creating pores [40]. The lukS/lukF genes are located on phages that can be transferred from one strain to another [41]. The main target cells of the toxin are polymorphonuclear leukocytes (PMNLs, neutrophils), with high species specificity [42]. Depending on its concentration, PVL can induce cytolysis or apoptosis of leukocytes, leading to the release of inflammatory factors and interfering with the host’s immune defense mechanisms. This results in the typical dissociation between a low or normal leukocyte count and high levels of inflammatory parameters (e.g., CRP, PCT) [43].
PVL’s cytolytic properties and the associated tissue destruction can facilitate local spread and bloodstream dissemination of bacteria. PVL-SA infections have been associated with invasive disease, greater symptom severity, an increased risk of complications and ICU admissions, and longer hospitalizations, when compared to PVL- Sa [6]. PVL-SA -associated disease spectrum can range from SSTIs to musculoskeletal, pulmonary, cardiovascular, and CNS infections. Our patient had osteomyelitis and extensive abscess collections along with necrotizing pneumonia. Our review evidenced 13 similar cases where the infection affected the osteoarticular and respiratory systems. Pneumonia appears to be the most common manifestation of severe PVL-SA associated infections in pediatric age (47%), followed by severe SSTIs (38%) and osteoarticular localization (37%). When caused by non-toxin-producing S. aureus, pneumonia is generally less aggressive, less likely to evolve into a necrotic type, and has a slower progression. Unlike PVL-SA, PVL- Sa pneumonia is most often associated with hospital-acquired infections [3,41]. Furthermore, necrotizing pneumonia has been identified as the most severe of PVL-SA infection manifestations, often leading to ARDS and the need for mechanical ventilation [44]. In line with these findings, our analysis evidenced a strong association between pulmonary involvement and the need for intensive care (p<0.001).
The prevalence of the PVL gene in S. aureus strains varies in different parts of the world and is higher in low- and middle-income countries. PVL can be produced by either MSSA or MRSA strains. It has been reported that between 70% and 100% of isolated community-associated MRSA (CA-MRSA) strains carry the PVL genes, as opposed to only 9-46% of the MSSA strains [4,45,46]. Consistent with these findings, most invasive PVL-SA infections in the US are caused by CA-MRSA strains, while in Europe the most commonly isolated PVL+ strains are MSSA [40,47,48,49,50]. Among the cases included in our review, PVL+ strains were more frequently MSSA (61%). In line with this finding, 36% of the cases in our review were from Europe, and only 4% and 5% were from North and South America, respectively.
Regarding the therapeutic approach, Gillet et al. underline the necessity to act against PVL-SA infections on multiple fronts: (1) source control, as in the removal of PVL through timely surgical drainage, (2) inhibiting its production, and (3) stopping its toxic effects post-production (44,50). Clindamycin, linezolid and rifampicin are able to reduce PVL production [51]. These molecules also have the advantage of maintaining effectiveness even at suboptimal concentrations, while beta-lactams and vancomycin may aggravate PVL effects when below their MICs [39,51,52]. A combination of beta-lactam with an anti-toxin molecule has been indicated as the most effective treatment for PVL-SA infections [44,53]. According to UK guidelines on managing PVL-SA infections, in pediatric cases with features suggestive of PVL-SA, clindamycin should be added to the first line empiric antibiotic treatment, which depends on the infection type and local epidemiology [53]. Linezolid should be added if MRSA is suspected or, importantly, upon evidence of PVL. In cases of sepsis and pneumonia, rationalization of treatment upon confirmation of PVL and strain sensitivities should include clindamycin plus rifampicin +/- linezolid, and linezolid plus rifampicin in case of resistance to clindamycin [53]. In cases of bone and joint infections, recommendations include an initial treatment phase with clindamycin, linezolid and rifampicin until normalization of inflammatory markers (with linezolid treatment not longer than 4 weeks), and a continuation phase with clindamycin plus rifampicin, following a pediatric infectiologist’s guidance on duration and route [53]. Our first-line treatment, motivated by the suspicion of PVL+ CA-MRSA, consisted of linezolid and ceftaroline, Upon the development of anemia, confirmation of the presence of PVL, and confirmation of methicillin resistance, treatment was rationalized to clindamycin (for its anti-toxic effect and lung penetration), and fosfomycin plus daptomycin for their synergistic effect against S. aureus in bone infections [54]. Despite lack of treatment data in the cases included in our review, available for 39% of cases, 57% of the described treatments included anti-toxin molecules.
As part of managing PVL-SA infection cases, investigations should be undertaken to identify a possible familiar and individual history of PVL-SA infections in the previous year [53]. In our case, family members were treated to ensure the resolution of the outbreak and prevent relapses. Further, the addition of a single dose of a long-acting antibiotic, such as dalbavancin, upon discharge aligns with the potential risk of relapse posed by the relatives’ contamination, ensuring prolonged protection and optimal recovery. Surprisingly, in our review, information on familiar involvement was reported only in 18% of the cases we collected, which reflects a possible underestimation of the risk posed by family outbreaks. Familiar anamnesis is fundamental in that it could lead to timely identification of PVL-SA in other possibly infected children and help prevent potentially severe relapses and further spread of the infection.
4. Materials and Methods
We searched PubMED in February 2024 for articles describing pediatric cases of severe infections caused by PVL-SA in pediatric populations. We used keywords such as “Panton-Valentine leucocidin,” “pvl,” “children,” “pediatric,” and relevant synonyms to broaden our results. Our main inclusion criteria were (1) a focus on pediatric populations, (2) evidence of PVL-SA strains as causative agents of the described conditions, (3) the severity and clinical significance of the infection, and (4) the clinical focus of the article, with information on diagnosis, treatment and outcome. We excluded articles that (1) did not have a focus on children or where information on pediatric cases could not be extracted; (2) did not clearly report evidence of PVL-SA strains; (3) focused on asymptomatic carriers or contamination with PVL-SA; (4) did not include enough information on diagnosis, treatment and outcome. However, where only some information was missing, we included the article and reported where data was unavailable. To refine our search, we applied filters, selecting our population of interest and articles published in English. No automation tools were used.
Clinical and demographic characteristics were summarized through descriptive statistics, using mean, median, and interquartile range (IQR) for continuous variables, and absolute and relative frequencies for categorical variables. Logistical multivariate analysis was used to assess through odds ratios (OR) the correlation between the need for intensive care (dependent variable), and the variables relative to clinical manifestations (independent variables). These were selected according to the Hosmer-Lemeshow methodology. After univariate analysis, only variables with p < 0,20 were included in the final model; then, through a backward elimination process dictated by the Hosmer-Lemeshow method, variables were excluded until a significance level of p < 0.05 was reached for each variable. The application of the test is a measure of how well the model fits the data without any variable selection by the researcher to be included in the multivariate model. A two-tailed p-value <0.05 was considered statistically significant. 'STATA version 17.0' was the database management and analysis software.
5. Conclusions
The case we described of PVL-SA infection in a previously healthy 10-year-old boy exemplifies how this condition can manifest abruptly, causing a severe, multiorgan disease in pediatric age. Given that the boy was likely infected by his teenage brother, a wrestler, and that a full-blown family outbreak occurred, this case brings light to the importance of familiar anamnesis both for the identification of risk factors that can aid clinical suspicion and for optimal management of the infection, that includes decolonization of the household.
Necrotizing pneumonia, the main life-threatening manifestation of PVL-SA infection, is strongly linked with the need for ICU in our review, reinforcing pre-existing findings. Treatment of severe cases should include an anti-toxin molecule (such as clindamycin, linezolid, and rifampicin), and timely source control. Considering the risks posed by outbreaks, the use of long-acting antibiotics might be considered when investigation and decolonization of the entire household are not feasible.
Author Contributions
Conceptualization, CC and VG; methodology, VG and LV; software, GN; validation, VG, LV, CC and AC; formal analysis, VG, LV, and GN; investigation, VG, LV, GB, CA, AC, VFP, SB and LAC; resources, CC, AC and GN; data curation, VG, LV, GN, GB, CA, AC, VFP, SB and LAC; writing—original draft preparation, VG, LV and GN; writing—review and editing, VG, LV, CC, GN, and AC; visualization, VG and LV; supervision, CC and AC; project administration, CC. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study did not require ethical approval as it involved secondary data from a literature review.
Informed Consent Statement
Patient consent was waived due to the lack of any identifiable patient information.
Data Availability Statement
This study is based on secondary data from existing literature, and all data necessary to understand and interpret the findings are included within the manuscript.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Bonten M, Johnson JR, van den Biggelaar AHJ, Georgalis L, Geurtsen J, de Palacios PI, et al. Epidemiology of Escherichia coli Bacteremia: A Systematic Literature Review. Clin Infect Dis. 2021 Apr 1;72(7):1211–9.
- Otto, M. Community-associated MRSA: what makes them special? Int J Med Microbiol IJMM. 2013 Aug;303(6–7):324–30.
- Castellazzi, M.L.; Bosis, S.; Borzani, I.; Tagliabue, C.; Pinzani, R.; Marchisio, P.; di Pietro, G.M. Panton-valentine leukocidin Staphylococcus aureus severe infection in an infant: a case report and a review of the literature. Ital. J. Pediatr. 2021, 47, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Albiski MK, Lutz N, Ceroni D, NDele D, Zambelli PY, Bregou A. Paediatric musculoskeletal infections with Panton-Valentine leucocidin. Swiss Med Wkly [Internet]. 2018 Sep 23 [cited 2024 Aug 31]. Available online: https://smw.ch/index.php/smw/article/view/2519.
- Oumokhtar, B.; Moutaouakkil, K.; Abdellaoui, H.; Arhoune, B.; Atarraf, K.; El Fakir, S.; Yahyaoui, G.; Mahmoud, M.; Afifi, M.A. Paediatric osteoarticular infections caused by staphylococcus aureus producing panton–valentine leucocidin in morocco: Risk factors and clinical features. Afr. J. Paediatr. Surg. 2022, 19, 78–82. [Google Scholar] [CrossRef]
- Hoppe, P.-A.; Holzhauer, S.; Lala, B.; Bührer, C.; Gratopp, A.; Hanitsch, L.G.; Humme, D.; Kieslich, M.; Kallinich, T.; Lau, S.; et al. Severe infections of Panton-Valentine leukocidin positive Staphylococcus aureus in children. Medicine 2019, 98, e17185. [Google Scholar] [CrossRef] [PubMed]
- Fujita, Y.; Matsudera, S.; Watanabe, S.; Yamaguchi, T.; Suzuki, K.; Ohkusu, M.; Ishiwada, N.; Yoshihara, S. Extensive Subcutaneous Abscess due to Panton-Valentine Leucocidin-Positive Community-Associated Methicillin-Resistant Staphylococcus aureus in an Infant. Tohoku J. Exp. Med. 2022, 258, 303–307. [Google Scholar] [CrossRef]
- Disseminated Panton-Valentine Leukocidin-Positive Staphylococcus aureus infection in a child. Arch Argent Pediatr [Internet]. 2016 Apr 1 [cited 2024 Aug 31]. Available online: http://www.sap.org.ar/docs/publicaciones/archivosarg/2016/v114n2a14e.pdf.
- Ahoyo TA, Martin-Odoom A, Bankolé HS, Baba-Moussa L, Zonon N, Prevost G, et al. EPIDEMIOLOGY AND PREVENTION OF NOSOCOMIAL PNEUMONIA ASSOCIATED WITH PANTON-VALENTINE LEUKOCIDIN (PVL) PRO- DUCING STAPHYLOCOCCUS AUREUS IN DEPARTMENTAL HOSPI- TAL CENTRE OF ZOU COLLINES IN BENIN. GHANA Med J. 2012;46(4).
- Hardy, C.; Osei, L.; Basset, T.; Elenga, N. Bone and joint infections with Staphylococcus aureus strains producing Panton–Valentine Leukocidin in French Guiana. Medicine 2019, 98, e16015. [Google Scholar] [CrossRef]
- Ogawa, E.; Shoji, K.; Uehara, Y.; Miyairi, I. Retropharyngeal Abscess Caused by Community-Acquired MRSA USA300 Clone in a 1-Year-Old Japanese Girl. Jpn. J. Infect. Dis. 2022, 75, 403–406. [Google Scholar] [CrossRef] [PubMed]
- Oshima, N.; Hamada, H.; Hirose, S.; Shimoyama, K.; Fujimori, M.; Honda, T.; Yasukawa, K.; Ishiwada, N.; Ohkusu, M.; Takanashi, J.-I. PantoneValentine leukocidin-positive novel sequence type 5959 community-acquired methicillin-resistant Staphylococcus aureus meningitis complicated by cerebral infarction in a 1-month-old infant. J. Infect. Chemother. 2021, 27, 103–106. [Google Scholar] [CrossRef]
- Vanbiervliet, V.; Demeyer, I.; Claus, F.; Van Vaerenbergh, K. A case report: septic shock due to (tropical) pyomyositis and multiple metastatic embolisms caused by Panton Valentine Leukocidin-positive methicillin-sensitive staphylococcus aureus in a 12-year-old boy. Acta Clin. Belg. 2021, 77, 421–424. [Google Scholar] [CrossRef]
- Chen, J.; Luo, Y.; Zhang, S.; Liang, Z.; Wang, Y.; Zhang, Y.; Zhou, G.; Jia, Y.; Chen, L.; She, D. Community-acquired necrotizing pneumonia caused by methicillin-resistant Staphylococcus aureus producing Panton–Valentine leukocidin in a Chinese teenager: case report and literature review. Int. J. Infect. Dis. 2014, 26, 17–21. [Google Scholar] [CrossRef]
- Schwartz, K.L.; Nourse, C. Panton–Valentine leukocidin-associated Staphylococcus aureus necrotizing pneumonia in infants: a report of four cases and review of the literature. Eur. J. Pediatr. 2011, 171, 711–717. [Google Scholar] [CrossRef] [PubMed]
- Irenji N, Pillai SKG, West-Jones JS. Serious life-threatening multifocal infection in a child, caused by Panton-Valentine leucocidin-producing Staphylococcus aureus (PVL-MSSA). BMJ Case Rep. 2018 Jun 5;bcr-2017-222138.
- Elledge, R.O.; Dasari, K.K.; Roy, S. Panton-Valentine leukocidin-positive Staphylococcus aureus osteomyelitis of the tibia in a 10-year-old child. J. Pediatr. Orthop. B 2014, 23, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Cocchi, P.; Taccetti, G.; Montagnani, C.; Campana, S.; Galli, L.; Braggion, C.; de Martino, M. Evidence of transmission of a Panton-Valentine leukocidin-positive community-acquired methicillin-resistant Staphylococcus aureus clone: a family affair. Clin. Microbiol. Infect. 2013, 19, 1158–1162. [Google Scholar] [CrossRef] [PubMed]
- Lehman, D.; Tseng, C.W.; Eells, S.; Miller, L.G.; Fan, X.; Beenhouwer, D.O.; Liu, G.Y. Staphylococcus aureusPanton-Valentine Leukocidin Targets Muscle Tissues in a Child with Myositis and Necrotizing Fasciitis. Clin. Infect. Dis. 2010, 50, 69–72. [Google Scholar] [CrossRef] [PubMed]
- Green, K.; Chranioti, I.; Singh, S.; Jäger, H.R.; Drebes, A.; Gabbie, S.; Cohen, J. Panton-Valentine Leukocidin Producing Staphylococcus Aureus Facial Pyomyositis Causing Partial Cavernous Sinus Thrombosis. Pediatr. Infect. Dis. J. 2017, 36, 1102–1104. [Google Scholar] [CrossRef] [PubMed]
- Khattak, S.G.; Dady, I.; Mukherjee, D. Unusual presentation of late-onset disseminated staphylococcal sepsis in a preterm infant. BMJ Case Rep. 2019, 12, e226325. [Google Scholar] [CrossRef] [PubMed]
- Gadelsayed, M.N.; Greally, P.; Elnazir, B. Methicillin-resistant Staphylococcus aureus (Panton-Valentine leucocidin) cavitating pneumonia in a healthy child. Arch. Dis. Child. 2012, 97, 980–981. [Google Scholar] [CrossRef]
- Fitzgerald, F.; Howard, J.; Bailey, F.; Soleimanian, S. Back pain in a previously healthy teenager. BMJ Case Rep. 2013, 2013. [Google Scholar] [CrossRef]
- Karlı, A.; Belet, N.; Yanık, K. ; Köken, ; Kilic, M.; Bilgici, M.C.; Şensoy, G. Panton-Valentine leukocidin positive Staphylococcus aureus infection in childhood: a case report.. 2015, 57, 615–617. [Google Scholar]
- Daskalaki, M.; Rojo, P.; Marin-Ferrer, M.; Barrios, M.; Otero, J.R.; Chaves, F. Panton–Valentine leukocidin-positive Staphylococcus aureus skin and soft tissue infections among children in an emergency department in Madrid, Spain. Clin. Microbiol. Infect. 2010, 16, 74–77. [Google Scholar] [CrossRef] [PubMed]
- Geng W, Yang Y, Wu D, Zhang W, Wang C, Shang Y, et al. Community-acquired, methicillin-resistant Staphylococcus aureus isolated from children with community-onset pneumonia in China. Pediatr Pulmonol. 2010 Apr;45(4):387–94.
- Kechrid, A.; Pérez-Vázquez, M.; Smaoui, H.; Hariga, D.; Rodríguez-Baños, M.; Vindel, A.; Baquero, F.; Cantón, R.; del Campo, R. Molecular analysis of community-acquired methicillin-susceptible and resistant Staphylococcus aureus isolates recovered from bacteraemic and osteomyelitis infections in children from Tunisia. Clin. Microbiol. Infect. 2011, 17, 1020–1026. [Google Scholar] [CrossRef] [PubMed]
- Noguchi, Y.; Nishisho, S.; Okada, H.; Shimono, R.; Kusaka, T. An infant with necrotizing pneumonia caused by methicillin-resistant Staphylococcus aureus strain USA300. Pediatr. Int. 2021, 64, e14658. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, A.B.; Larsen, A.R.; Petersen, A.; Schønheyder, H.C.D.; Westh, H.D.; Benfield, T.D.; Nygaard, U. Clinical Manifestations in Children with Staphylococcal Bacteremia Positive for Panton-Valentine Leucocidin A Nationwide Survey in a Low Methicillin-Resistance Setting. Pediatr. Infect. Dis. J. 2020, 39, E274–E276. [Google Scholar] [CrossRef] [PubMed]
- Mutale, W.; Sahay, K.M.; Hartley, J.; Thompson, D.; Ratnasinghe, D.; Hudson, L.; Hulse, E.; Fellows, G. Community acquired Panton-Valentine Leukocidin (PVL) positive Methicilin Resistant Staphylococcal aureus cerebral abscess in an 11-month old boy: a case study. BMC Res. Notes 2014, 7, 862. [Google Scholar] [CrossRef] [PubMed]
- E Bukhari, E.; E Al-Otaibi, F.; El-Hazmi, M.M.; Somily, A.M. Panton-Valentine leukocidin Staphylococcus aureus osteomyelitis of the femur in a Saudi child. . 2012, 33, 201–4. [Google Scholar]
- Ambrozova, H.; Maresova, V.; Fajt, M.; Pavlicek, P.; Rohacova, H.; Machova, I.; Petras, P. The first case of fatal pneumonia caused by Panton–Valentine leukocidin-producing Staphylococcus aureus in an infant in the Czech Republic. Folia Microbiol. 2012, 58, 225–228. [Google Scholar] [CrossRef] [PubMed]
- Isobe, H.; Miyasaka, D.; Ito, T.; Takano, T.; Nishiyama, A.; Iwao, Y.; Khokhlova, O.E.; Okubo, T.; Endo, N.; Yamamoto, T. Recurrence of pelvic abscess from Panton-Valentine leukocidin-positive community-acquired ST30 methicillin-resistantStaphylococcus aureus. Pediatr. Int. 2013, 55, 120–123. [Google Scholar] [CrossRef] [PubMed]
- Obando, I.; Valderrabanos, E.S.; A Millan, J.; Neth, O.W. Necrotising pneumonia due to influenza A (H1N1) and community-acquired methicillin-resistant Staphylococcus aureus clone USA300: successful management of the first documented paediatric case. Arch. Dis. Child. 2010, 95, 305–306. [Google Scholar] [CrossRef] [PubMed]
- Dunlop, R.L.; Eadie, P. Idiopathic neonatal necrotising fasciitis caused by community-acquired MSSA encoding Panton Valentine Leukocidin genes. J. Plast. Reconstr. Aesthetic Surg. 2011, 64, 1522–1524. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, C.d.O.; Chamon, R.C.; de Oliveira, T.L.R.; Nouér, S.A.; dos Santos, K.R.N. Systemic infection caused by the methicillin-resistant Staphylococcus aureus USA300-LV lineage in a Brazilian child previously colonized. Braz. J. Infect. Dis. 2023, 27, 102737. [Google Scholar] [CrossRef]
- Higuchi, W.; Takano, T.; Iwao, Y.; Ozaki, K.; Isobe, H.; Yamamoto, T.; Hung, W.-C.; Teng, L.-J.; Shimazaki, T.; Honda, A.; et al. Molecular characteristics of the Taiwanese multiple drug-resistant ST59 clone of Panton-Valentine leucocidin-positive community-acquired methicillin-resistant Staphylococcus aureus from pediatric cellulitis. J. Infect. Chemother. 2010, 16, 144–149. [Google Scholar] [CrossRef] [PubMed]
- Kefala-Agoropoulou, K.; Protonotariou, E.; Vitti, D.; Sarafidou, S.; Anastasiou, A.; Kollios, K.; Roilides, E. Life-threatening infection due to community-acquired methicillin-resistant Staphylococcus aureus: case report and review. Eur. J. Pediatr. 2009, 169, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Libert N, Batjom E, Cirodde A, de Rudnicki S, Grasser L, Borne M, et al. [Antitoxin treatments for necrotizing pneumonia due to Panton-Valentine leukocidin-secreting Staphylococcus aureus]. Med Mal Infect. 2009 Jan;39(1):14–20.
- Shallcross, L.J.; Fragaszy, E.; Johnson, A.M.; Hayward, A.C. The role of the Panton-Valentine leucocidin toxin in staphylococcal disease: a systematic review and meta-analysis. Lancet Infect. Dis. 2013, 13, 43–54. [Google Scholar] [CrossRef] [PubMed]
- Lina, G.; Piémont, Y.; Godail-Gamot, F.; Bes, M.; Peter, M.-O.; Gauduchon, V.; Vandenesch, F.; Etienne, J. Involvement of Panton-Valentine Leukocidin--Producing Staphylococcus aureus in Primary Skin Infections and Pneumonia. Clin. Infect. Dis. 1999, 29, 1128–1132. [Google Scholar] [CrossRef] [PubMed]
- Boyle-Vavra, S.; Daum, R.S. Community-acquired methicillin-resistant Staphylococcus aureus: the role of Panton–Valentine leukocidin. Mod. Pathol. 2007, 87, 3–9. [Google Scholar] [CrossRef] [PubMed]
- Couvé-Deacon E, Tristan A, Pestourie N, Faure C, Doffoel-Hantz V, Garnier F, et al. Outbreak of Panton-Valentine Leukocidin–Associated Methicillin-Susceptible Staphylococcus aureus Infection in a Rugby Team, France, 2010–2011 - Volume 22, Number 1—January 2016 - Emerging Infectious Diseases journal - CDC. [cited 2024 Sep 7]. Available online: https://wwwnc.cdc.gov/eid/article/22/1/15-0597_article.
- Gillet, Y.; Dumitrescu, O.; Tristan, A.; Dauwalder, O.; Javouhey, E.; Floret, D.; Vandenesch, F.; Etienne, J.; Lina, G. Pragmatic management of Panton–Valentine leukocidin-associated staphylococcal diseases. Int. J. Antimicrob. Agents 2011, 38, 457–464. [Google Scholar] [CrossRef] [PubMed]
- Miller, L.G.; Remington, F.P.; Bayer, A.S.; Diep, B.; Tan, N.; Bharadwa, K.; Tsui, J.; Perlroth, J.; Shay, A.; Tagudar, G.; et al. Clinical and Epidemiologic Characteristics Cannot Distinguish Community-Associated Methicillin-Resistant Staphylococcus aureus Infection from Methicillin-Susceptible S. aureus Infection: A Prospective Investigation. Clin. Infect. Dis. 2007, 44, 471–482. [Google Scholar] [CrossRef]
- Chiu, Y.-K.; Lo, W.-T.; Wang, C.-C. Risk factors and molecular analysis of Panton-Valentine leukocidin-positive methicillin-susceptible Staphylococcus aureus colonization and infection in children. J. Microbiol. Immunol. Infect. 2012, 45, 208–213. [Google Scholar] [CrossRef] [PubMed]
- Shallcross LJ, Williams K, Hopkins S, Aldridge RW, Johnson AM, Hayward AC. Panton-Valentine leukocidin associated staphylococcal disease: a cross-sectional study at a London hospital, England. Clin Microbiol Infect Off Publ Eur Soc Clin Microbiol Infect Dis. 2010 Nov;16(11):1644–8.
- Tinelli M, Monaco M, Vimercati M, Ceraminiello A, Pantosti A. Methicillin-Susceptible Staphylococcus aureus in Skin and Soft Tissue Infections, Northern Italy - Volume 15, Number 2—February 2009 - Emerging Infectious Diseases journal - CDC. [cited 2024 Oct 1]. Available online: https://wwwnc.cdc.gov/eid/article/15/2/08-0010_article.
- Rao, G.G.; Batura, R.; Nicholl, R.; Coogan, F.; Patel, B.; Bassett, P.; Kearns, A.M. Outbreak report of investigation and control of an outbreak of Panton-Valentine Leukocidin-positive methicillin-sensitive Staphylococcus aureus (PVL-MSSA) infection in neonates and mothers. BMC Infect. Dis. 2019, 19, 178. [Google Scholar] [CrossRef]
- Goemanne, S.; Tilmanne, A.; Biarent, D.; Smeesters, P.; Simoni, P.; Mahadeb, B.A.; Vicinanza, A. Severe Staphylococcus aureus infections in children: Case reports and management of positive Panton-Valentine leucocidin cases. Front. Pediatr. 2022, 10, 1003708. [Google Scholar] [CrossRef] [PubMed]
- Dumitrescu, O.; Boisset, S.; Badiou, C.; Bes, M.; Benito, Y.; Reverdy, M.-E.; Vandenesch, F.; Etienne, J.; Lina, G. Effect of Antibiotics on Staphylococcus aureus Producing Panton-Valentine Leukocidin. Antimicrob. Agents Chemother. 2007, 51, 1515–1519. [Google Scholar] [CrossRef] [PubMed]
- Dumitrescu O, Badiou C, Bes M, Reverdy ME, Vandenesch F, Etienne J, et al. Effect of antibiotics, alone and in combination, on Panton-Valentine leukocidin production by a Staphylococcus aureus reference strain. Clin Microbiol Infect Off Publ Eur Soc Clin Microbiol Infect Dis. 2008 Apr;14(4):384–8.
- Health Protection Agency. Guidance on the Diagnosis and Management of PVL-Associated Staphylococcus aureus Infections (PVL-SA) in England. 2008.
- Lee, Y.-C.; Chen, P.-Y.; Wang, J.-T.; Chang, S.-C. A study on combination of daptomycin with selected antimicrobial agents: in vitro synergistic effect of MIC value of 1 mg/L against MRSA strains. BMC Pharmacol. Toxicol. 2019, 20, 1–6. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Flow chart describing the study selection process.
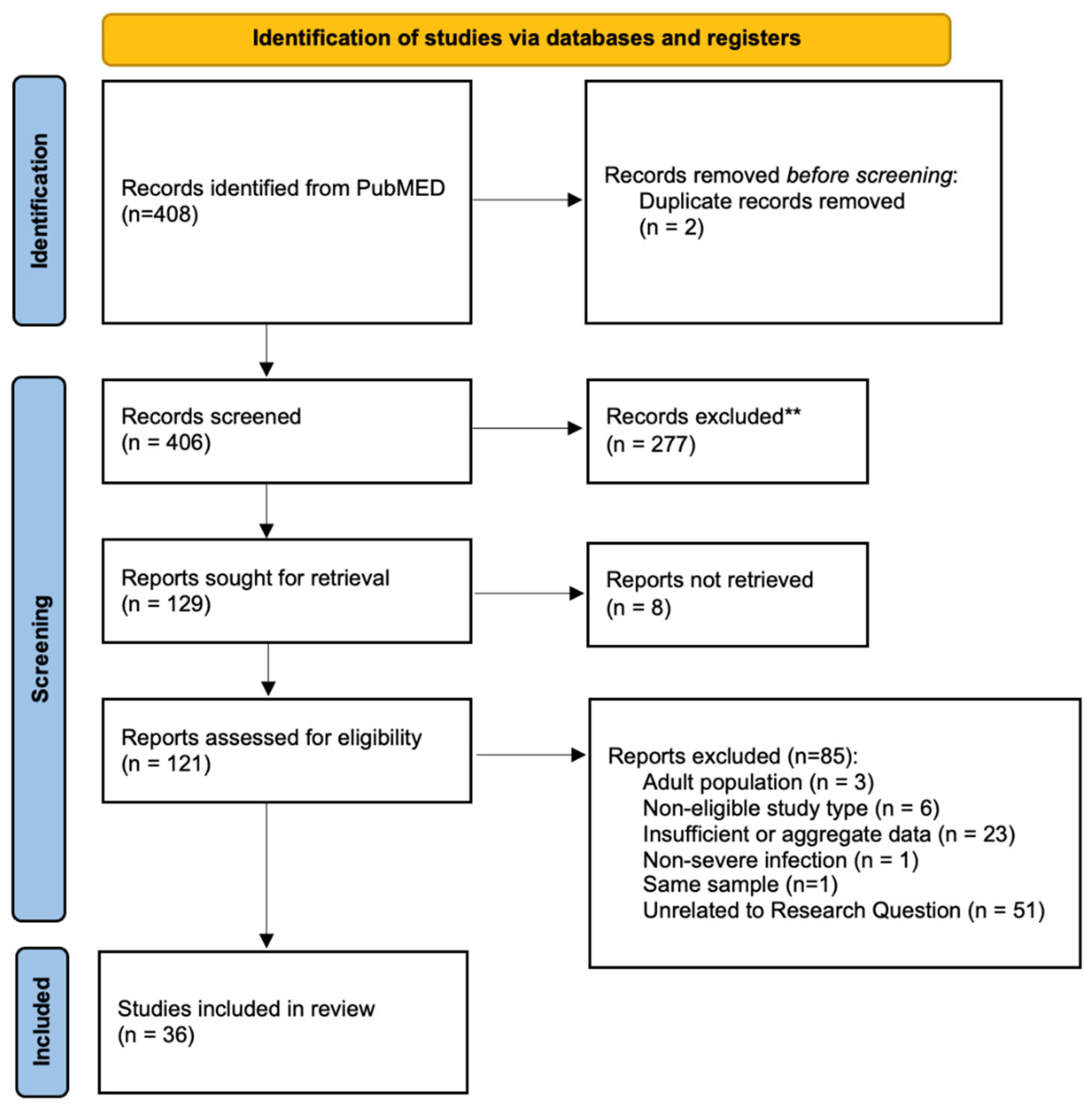
Figure 2.
- Bar chart describing the countries where patients were treated and/or where they likely contracted the infection. Fifty-six patients from 14 studies were observed in Europe, 52 from 3 studies in Africa, 34 from 13 studies in Asia, and 6 and 8 from North America and South America, respectively.
Figure 2.
- Bar chart describing the countries where patients were treated and/or where they likely contracted the infection. Fifty-six patients from 14 studies were observed in Europe, 52 from 3 studies in Africa, 34 from 13 studies in Asia, and 6 and 8 from North America and South America, respectively.
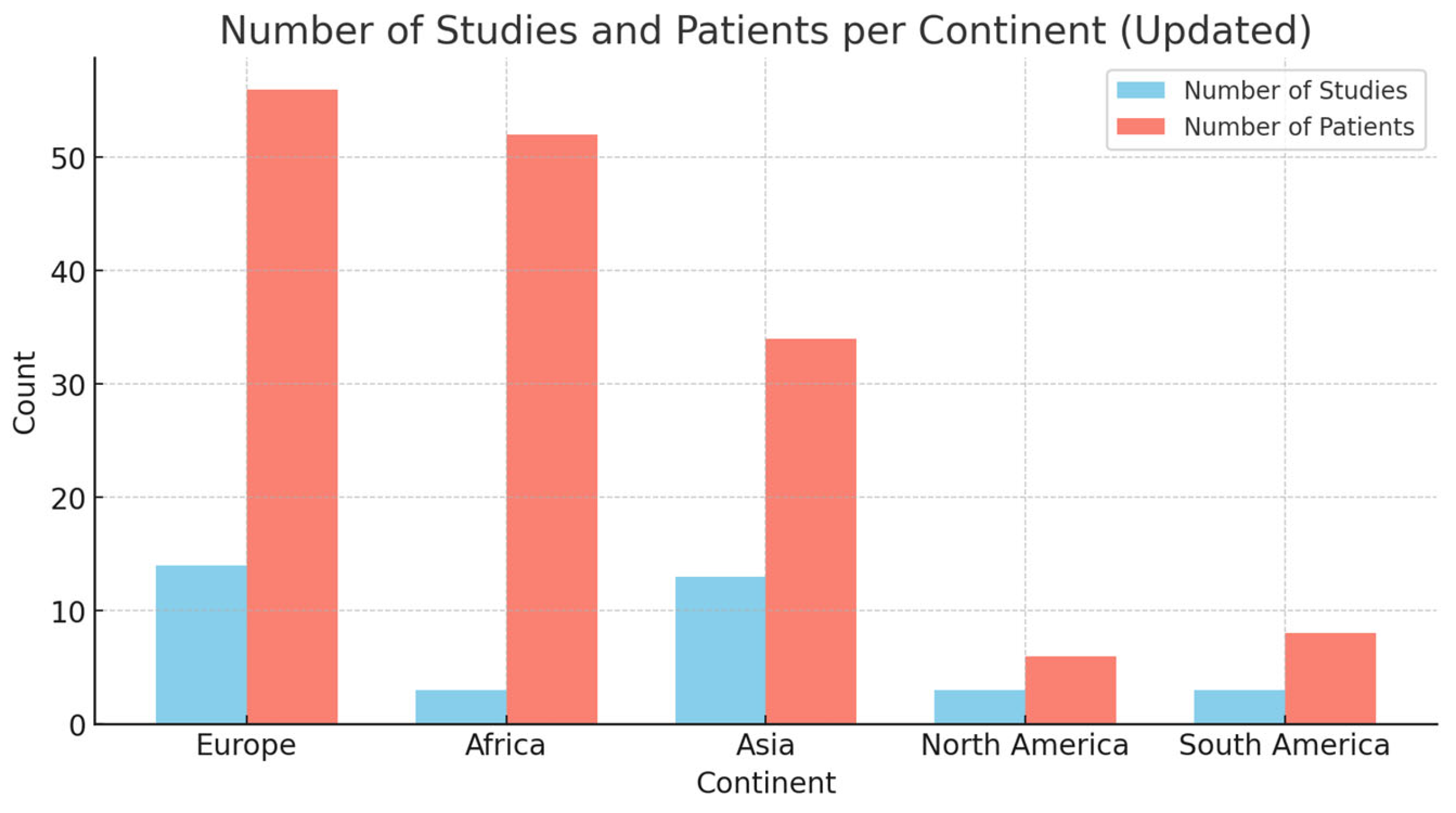

Table 1.
– Overview of the main clinical-epidemiological characteristics extracted from the included studies. *Age is expressed in years and, when cases are grouped together, the mean age is reported. Acronyms: ICU - Intensive Care Unit, MRSA - Methicillin-Resistant Staphylococcus Aureus, MSSA - Methicillin-Sensitive Staphylococcus Aureus, URTI - Upper Respiratory Tract Infection, RSV - Respiratory Syncytial Virus, CMV - Cytomegalovirus, PE - Pulmonary Embolism, TVP - Thrombosis Veinous Profunda (Deep Vein Thrombosis), SSTI - Skin and Soft Tissue Infections, DIC - Disseminated Intravascular Coagulation, RZHE - (likely a combination of antibiotics, but it's not standard; may require clarification), BAL - Bronchoalveolar Lavage, Sa - Staphylococcus Aureus, HL - Hospitalization Length, (d) - Days, os - Orally (in this context: medication administered orally).
Table 1.
– Overview of the main clinical-epidemiological characteristics extracted from the included studies. *Age is expressed in years and, when cases are grouped together, the mean age is reported. Acronyms: ICU - Intensive Care Unit, MRSA - Methicillin-Resistant Staphylococcus Aureus, MSSA - Methicillin-Sensitive Staphylococcus Aureus, URTI - Upper Respiratory Tract Infection, RSV - Respiratory Syncytial Virus, CMV - Cytomegalovirus, PE - Pulmonary Embolism, TVP - Thrombosis Veinous Profunda (Deep Vein Thrombosis), SSTI - Skin and Soft Tissue Infections, DIC - Disseminated Intravascular Coagulation, RZHE - (likely a combination of antibiotics, but it's not standard; may require clarification), BAL - Bronchoalveolar Lavage, Sa - Staphylococcus Aureus, HL - Hospitalization Length, (d) - Days, os - Orally (in this context: medication administered orally).
| Reference | Patients | Age* | Immune compromission and comorbidities | Samples used for diagnosis | Methicillin Sensitivity | Clinical Picture | Complications and ICU | Treatment | HL (d) | Outcome |
| Castellazzi et al. (2021) [3] | F (1) | 0,5 | Left bronchus malformation, history of apnea, URTI, bronchiolitis. | Blood, drainage material, BAL. S. pneumoniae and Haemophilus influenzae detected in the BAL culture. | MRSA | Muscle abscesses, femoral osteomyelitis, lung nodules, pulmonary septic emboli, sepsis | PE, ICU | Cefotaxime ➔ Ceftaroline + Daptomycin + Clindamycin ➔ Ceftaroline ➔ Linezolid (os) | 49 | Full recovery |
| Albiński et al. (2018) [4] | M (1) | 12 | N/A | Blood | MSSA | Osteomyelitis (tibia) Sepsis | Absent | Cefuroxime + Flucloxacillin + Gentamicin | 39 | growth arrest |
| Albiński et al. (2018) | M (1) | 10 | N/A | Blood and drainage material | MSSA | Osteomyelitis (humerus) | Absent | Amoxicillin-clavulanic + Clindamycin + Flucloxacillin ➔ Clindamycin (os) | 16 | pathological fracture |
| Albiński et al. (2018) | M (1) | 12 | N/A | Blood and drainage material | MSSA | Panosteomyelitis (femur, tibia) | ICU | Amoxicillin-clavulanic + Amikacin + Flucloxacillin + Vancomycin ➔ Levofloxacin + Rifampicin (os) | 83 | suicidality |
| Albiński et al. (2018) | M (1) | 13 | Acute Lymphoid Leukemia | Blood and drainage material | MSSA | Necrotizing pandiaphysitis (tibia), sepsis | Absent | Cefuroxime + Flucloxacillin | 35 | growth arrest |
| Albiński et al. (2018) | M (1) | 10 | N/A | Blood and drainage material | MSSA | Arthritis (hip) | Absent | Flucloxacillin + Gentamicin ➔ Clindamycin (os) | 27 | Full recovery |
| Albiński et al. (2018) | M (1) | 15 | N/A | Blood and drainage material | MSSA | Arthritis (knee) | ICU | Amoxicillin-clavulanic + Clindamycin + Flucloxacillin + Imipenem + Vancomycin | 74 | Relapse |
| Albiński et al. (2018) | M (1) | 2 | N/A | Drainage material | MRSA | Abscess (foot) | Absent | Amoxicillin-clavulanic + Clindamycin + Flucloxacillin | 17 | Full recovery |
| Albiński et al. (2018) | F (1) | 2 | N/A | Drainage material | MSSA | Abscess (gluteal) | Absent | Amoxicillin-clavulanic + Clindamycin | 1 | Full recovery |
| Albiński et al. (2018) | F (1) | 12 | N/A | Drainage material | MSSA | Abscess (finger) | Absent | Flucloxacillin | 8 | Full recovery |
| Moutaouakkil et al. (2022) [5] | M (12) F (5) | 8,12 | NR | Blood cultures, articular fluids, synovial tissues and/orbone fragments. | MRSA | Osteomyelitis (17), STTI (8) | Absent | NR | 17,41 | Full recovery |
| Hoppe et al. (2019) [6] | M (6) F (4) | 5,73 | URTI (RSV-B3, Influenza A) (4); Neonatal drug withdrawal; congenital CMV; heart transplantation. | Blood, pleural exudate, sputum, and bronchial lavage samples. | MSSA (6) MRSA (4) | Necrotizing pneumonia (5), necrotizing fasciitis of the thorax (2), pyomyositis (2), axillary abscess (1), mastoiditis and cerebellitis (1), multiple and recurrent abscesses (1), preorbital cellulitis (1), purulent conjunctivitis (1). | DVT (2), ICU (4) | NR | 22,6 | FR (9), S (1); persisting post intensive care syndrome,including reduced lung capacity and critical illnesspolyneuropathy |
| Fujita et al. (2022)[7] | F (1) | 0,3 | N/A | Lumbar abscess drainage, nasal swab. Negative blood culture. | MRSA | Extensive subcutaneous abscess of the lumbar region. | Absent | Cefotaxime ➔ Vancomycin ➔ Oral Sulfamethoxazole-trimethoprim | 21 | Full recovery |
| Karli et al. (2016)[8] | M (1) | 12 | N/A | Blood | MSSA | Multiple peripherally localized cavitary round lesions in both lungs (CT). Left psoas muscle abscess and left femoral trochanter osteomyelitis. Sepsis | PE, ICU | Vancomycin ➔ Linezolid + Clindamycin | 30 | Full recovery |
| Ahoyo et al. (2012)[9] | NR (19) | NR | Malnourishment after severe malaria, anemia, hospitalization | Pleural fluid (6), nasal swab (2), BAL (11) | MSSA | Pneumonia (19) | NR | NR | NR | Full recovery (2); Deceased (17) |
| Hardy et al. (2019)[10] | F (1) | 4,6 | N/A | Blood, drainage material | MSSA | Acute osteomyelitis, dermohypodermitis, septic arthritis, multifocal lesions, cardiac tamponade. | DVT, ICU | Amoxicillin-clavulanic + Gentamicin ➔ Cefotaxime + Fosfomycin + Clindamycin | 11 | Deceased; cardiac tamponade |
| Hardy et al. (2019) | M (1) | 14,7 | N/A | Blood, drainage material.Staphylococcus haemolticus in pericardial effusion. | MSSA | Acute osteomyelitis, open skin wound. | Absent | Cefotaxime + Gentamicin + Fosfomycin ➔ Clindamycin + Ciprofloxacin ➔ Ciprofloxacin (os) + Rifampicin (os) | 14 | Full recovery |
| Hardy et al. (2019) | F (1) | 11,2 | N/A | Blood, drainage material | MSSA | Acute osteomyelitis, open skin wound. | Absent | Amoxicillin-clavulanate + Gentamicin ➔ Clindamycin + Ciprofloxacin + Fosfomycin ➔ Ciprofloxacin (os) + Rifampicin (os) | 18 | Full recovery |
| Hardy et al. (2019) | F (1) | 13 | Active chronic Hepatitis B | Blood, drainage material | MSSA | Acute osteomyelitis, dermohypodermitis, septic arthritis, multifocal lesions, necrotizing fasciitis, pyomyositis, necrotizing pneumonia. | ICU | Cefotaxime + Gentamicin + Vancomycin ➔ Cloxacillin + Clindamycin + Rifampicin ➔ Clindamycin (os) + Rifampicin (os) | 88 | Functional impairment (ankle) |
| Hardy et al. (2019) | M (1) | 8,4 | N/A | Blood, drainage material | MSSA | Acute osteomyelitis, septic arthritis, multifocal lesions. | Absent | Cefotaxime + Gentamicin ➔ Cefotaxime + Vancomycin ➔ Clindamycin (os) + Rifampicin (os) | 20 | Full recovery |
| Hardy et al. (2019) | M (1) | 6,5 | N/A | Blood, drainage material, sputum culture. | MSSA | Acute osteomyelitis, septic arthritis, multifocal lesions, necrotizing pneumonia. | Absent | Cefotaxime + Gentamicin + Vancomycin ➔ Cloxacillin + Clindamycin ➔ Clindamycin (os) + Rifampicin (os) | 42 | Functional impairment, chronic osteomyelitis |
| Ogawa et al. (2022)[11] | F (1) | 1 | N/A | Surgical drainage. | MRSA | Retropharyngeal abscess | ICU | Ampicillin/sulbactam + Vancomycin ➔ Clindamycin | 22 | Full recovery |
| Oshima et al. (2021)[12] | M (1) | 0,08 | N/A | Blood. | MRSA | SSTI, necrotizing pneumonia and cerebral infarction. Sepsis | DVT, ICU | Meropenem and Cefotaxime ➔ Vancomycin + Meropenem ➔ Linezolid | 68 | right-sided hemiparesis |
| Vanbiervliet et al. (2022)[13] | M (1) | 12 | N/A | Blood. | MSSA | Subperiosteal abscess, osteomyelitis (ankle), pyomyositis, septic cardiomyopathy. Sepsis | DVT, PE, ICU | Piperacillin-tazobactam + Vancomycin ➔ Flucloxacillin, Linezolid, Clindamycin, and Levofloxacin | 42 | amputation; hospitalization was probably longer |
| Chen et al. (2014)[14] | F (1) | 15 | N/A | Pleural fluid and sputum. | MRSA | Necrotizing pneumonia with cavitary lung lesions and bilateral pleural effusion. Sepsis | ICU | Linezolid + Fosfomycin + Teicoplanin | 62 | Full recovery |
| Schwartz et al. (2012)[15] | F (1) | 0,67 | N/A | Pleural fluid. | MSSA | Necrotizing pneumonia, Pulmonary hemorrhage. | ICU | Cefotaxime ➔ Flucloxacillin + Vancomycin ➔ Linezolid + Rifampicin + Gentamicin ➔ Flucloxacillin + Rifampicin (after MSSA confirmed) | 17 | Deceased |
| Schwartz et al. (2012) | M (1) | 1,25 | N/A | Blood, pleural fluid. | MRSA | Necrotizing pneumonia, pulmonary hemorrhage, cerebral septic emboli and abscesses, erythroderma. Sepsis | ICU | Flucloxacillin, Cefotaxime, Ampicillin, and Azithromycin ➔ Hydrocortisone and IVIG ➔ Flucloxacillin + Vancomycin | 28 | Deceased |
| Schwartz et al. (2012) | F (1) | 0,67 | N/A | Pleural fluid and tracheal aspirate. | MRSA | Necrotizing pneumonia with multiple pneumatoceles. | ICU | Clindamycin and Cefotaxime ➔ Vancomycin ➔ Clindamycin + Linezolid + Rifampicin | 7 | Full recovery |
| Schwartz et al. (2012) | M (1) | 0,42 | N/A | Scalp lesion, endotracheal tube, and blood. | MRSA | Necrotizing pneumonia, infarction of the right cerebral and cerebellar hemispheres, purulent subcutaneous scalp lesion with surrounding erythema. Sepsis | ICU | Cefotaxime, Flucloxacillin, and Vancomycin ➔ Linezolid + Lincomycin + Rifampicin ➔ Clindamycin | 7 | resolving hemiplegia |
| Irenji et al. (2018)[16] | M (1) | 13 | N/A | Blood, abscesses material. | MSSA | Extensive pelvic abscesses, bilateral pneumonia, pericardial effusion and osteomyelitis. Sepsis | ICU | Flucloxacillin + Cefotaxime ➔ Linezolid + Clindamycin | 41 | Full recovery |
| Elledge et al. (2014)[17] | M (1) | 10 | N/A | Blood. | MRSA | Osteomyelitis of the proximal tibia, history of boils on the buttocks and thighs. | Absent | Flucloxacillin + Rifampicin + Linezolid ➔ Flucloxacillin (os) + Rifampicin (os) ➔ Linezolid (os) | 14 | Full recovery |
| Cocchi et al. (2013)[18] | M (1) | 0,25 | N/A | Pleural drainage sample. | MRSA | Necrotizing pneumonia, pyopneumothorax. | ICU | Ampicillin-sulbactam + Gentamicin (initial treatment; adjustments not mentioned) | NR | NR |
| Lehman et al. (2010) [19] | M (1) | 6 | N/A | Blood, abscess drainage material. | MSSA | Necrotizing pneumonia and necrotizing fasciitis, septic osteomyelitis and arthritis, pulmonary consolidation. Sepsis | PE, ICU | Vancomycin + Cefotaxime ➔ Oxacillin + Gentamicin | 42 | Full recovery |
| Green et al. (2017) [20] | M (1) | 13 | Heterozygous factor V Leiden mutation | Blood. | MSSA | Periorbital cellulitis. | DVT | Ceftriaxone + Metronidazole ➔ Ceftriaxone + Clindamycin (os) | NR | Full recovery |
| Khattak et al. (2019)[21] | M (1) | 0 | Preterm infant (30th week) | Blood. | MSSA | Cavitating pneumonia, shoulder abscess, cerebral abscess, osteomyelitis. Sepsis | ICU | Cefotaxime + Vancomycin ➔ Flucloxacillin + Linezolid | 42 | Full recovery |
| Gadelsayed et al. (2012)[22] | F (1) | 11 | N/A | Nasal swab, BAL. | MRSA | Cavitating pneumonia. | Absent | Trimethoprim/sulfamethoxazole | NR | Full recovery |
| Fitzgerald et al. (2013)[23] | M (1) | 14 | N/A | Blood. | MSSA | Discitis with an epidural abscess at L3–L4, necrotizing pneumonia. Sepsis | ICU | Flucloxacillin, Clindamycin, and Gentamicin ➔ Ceftriaxone, Clindamycin and Clarithromycin ➔ Linezolid added + IVIG ➔ Ceftriaxone and Clindamycin (oral) | NR | Full recovery |
| Karli et al. (2015)[24] | M (1) | 12 | N/A | Blood. | MSSA | Necrotizing pneumonia, psoas abscess, cellulitis, and osteomyelitis. Sepsis | PE, ICU | Ceftriaxone + Vancomycin ➔ Vancomycin discontinued ➔ Linezolid ➔ Clindamycin (os) | 30 | Full recovery |
| Daskalaki et al. (2009)[25] | M (10) F (2) | 2,3 | N/A | Drainage material or skin samples (12). | MRSA (5) MSSA (7) | SSTI (12). Cellulitis, abscesses (9). | Absent | NR | NR | NR |
| Geng et al. (2010)[26] | NR (22) | 0,72 | Pneumonia with RSV (2), measles (2), CMV (1) | Sputum culture, pleural fluid and blood. | MRSA (22) | Necrotizing pneumonia (22), complicated in 3 cases with empyema, pneumopyothorax, septicemia. Sepsis (1) | Absent | NR | NR | Ful recovery (21) |
| Kechrid et al. (2010)[27] | M (13) F (3) | 6,18 | N/A | Blood or bone tissues. | MRSA (8) MSSA (8) | Osteomyelitis (10), bacteremia (6). Sepsis (1) | Absent | Oxacillin + Gentamicin (9); Teicoplanin + Gentamicin (3); Vancomycin + Gentamicin (1); Fosfomycin + Cefotaxime (1); Teicoplanin + Pristinamycin (2) | NR | Full recovery (14), Sequelae (2); Chronic osteomyelitis, necrosis of femur |
| Noguchi et al. (2021)[28] | M (1) | 0,92 | N/A | Sputum culture. Negative blood culture. | MRSA | Necrotizing pneumonia, left-sided abscess and pyothorax, DIC | ICU | Cefotaxime ➔ Meropenem and Vancomycin ➔ Linezolid and Clindamycin ➔ Vancomycin and Clindamycin | 31 | Full recovery |
| Bybeck et al. (2020)[29] | NR (15) | 9,06 | N/A | Blood (15), and surgical drainage in cases with abscesses. | MRSA (2) MSSA (13) | Pulmonary localization (6); osteoarticular localization (5); SSTI (2); pericardial effusion (1); DIC (1), pneumothorax (2), respiratory insufficiency (4), one rhabdomyolysis and one local abscess. Sepsis (1). | DVT (1), ICU (4) | NR | NR | Full recovery (11), Deceased (1); Sequelae (3); venous insufficiency and stenosis of the iliac vein (1); above-knee amputation (1); chronic heart failure (1 case, unrelated to infection) |
| Mutale et al. (2014)[30] | M (1) | 0,92 | N/A | Blood, brain abscess sample. Negative nasal swab. | MRSA | Parietal lobe abscess in the brain. | ICU | Ceftriaxone + RZHE ➔ Vancomycin + Amikacin + Metronidazole + Cefotaxime + Rifampicin ➔ Rifampicin + Vancomycin + Linezolid | 42 | Full recovery |
| Bukhari et al. (2012)[31] | F (1) | 0,75 | N/A | Blood, drainage material. | MSSA | Abscess formation and osteolytic lesions of the femur, left iliofemoral thrombosis | DVT | Ceftriaxone + Cloxacillin ➔ Clindamycin + Cloxacillin | 56 | Full recovery |
| Ambrozova et al. (2012)[32] | M (1) | 0,83 | Citrobacter youngae identified in stool culture | Blood, pleural fluid. | MSSA | Pleuropneumonia and empyema, mediastinitis, SSTI. Sepsis | ICU | Cefotaxime ➔ Cefotaxime, Clindamycin, Gentamicin, Fluconazole, Corticosteroids ➔ Oxacillin + Clindamycin + Gentamicin. | 16 | Deceased; progressive respiratory failure, pneumothorax, pneumoperitoneum, and circulatory failure, leading to death. |
| Isobe et al. (2013)[33] | F (1) | 17 | N/A | Drainage material. | MRSA | Osteomyelitis and multifocal pelvic (iliopsoas and piriformis) abscesses, adjacent to the sacroiliac joint. | Absent | Vancomycin + Pazufloxacin ➔ Post-discharge: Vancomycin + Minocycline (os)Second episode: Vancomycin + Fosfomycin ➔ Vancomycin (post-discharge) + Minocycline (os) | 27 | Relapse (3 episodes requiring hospitalization) |
| Obando et al. (2010)[34] | M (1) | 12 | Influenza A (H1N1) co-infection. | Pleural fluid culture. | MRSA | Necrotizing pneumonia and bilateral pleural empyemaand pneumothorax. | ICU | Ceftriaxone + Vancomycin + Clarithromycin ➔ Vancomycin + Clindamycin ➔ Linezolid + Clindamycin | 28 | Full recovery |
| Dunlop et al. (2011)[35] | M (1) | 0,03 | N/A | Cultures taken at the time of the first debridement. | MSSA | Necrotizing fasciitis. | ICU | Cefotaxime + Gentamicin + Flucloxacillin ➔ Vancomycin + Clindamycin ➔ High-dose Flucloxacillin + Clindamycin + Gentamicin | 35 | Full recovery |
| Whitaker et al. (2023)[36] | M (1) | 15 | N/A | Blood, drainage materials, nasal swab. | MRSA | Abscess in left psoas, subduralempyema in the sacral region extending to the lumbarspine. | PE | Vancomycin ➔ Daptomycin ➔ Sulfamethoxazole/trimethoprim (os) | 45 | Full recovery |
| Higuchi et al. (2010)[37] | M (1) | 7 | N/A | Drainage material. | MRSA | Abdominal cellulitis | Absent | Cefdinir (os) | 7 | Relapse |
| Kefala-Agoropoulou et al. (2010)[38] | F (1) | 10 | N/A | Blood, drainage material. | MRSA | Pneumonia, signs of encephalopathy, severe osteomyelitis on the whole right femur and pyomyositis and thrombosis of the right femoral andright external iliac vein. Sepsis | DVT, ICU | Cloxacillin ➔ Vancomycin + Clindamycin + Gentamicin ➔ Teicoplanin + Clindamycin (os) | 56 | Full recovery |
Table 2.
Organs and systems affected by PVL-SA infection, with absolute and relative frequencies. Children were often affected by more than one manifestation.
Table 2.
Organs and systems affected by PVL-SA infection, with absolute and relative frequencies. Children were often affected by more than one manifestation.
| Bloodstream (bacteremia) | 76 (49%) |
| Respiratory system | 73 (47%) |
| Skin and soft tissues | 59 (38%) |
| Osteo-articular system | 58 (37%) |
| Central Nervous System | 9 (6%) |
| Cardiovascular system | 6 (4%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



