
Submitted:
29 October 2024
Posted:
29 October 2024
You are already at the latest version
Abstract
Background/Objectives: Thoracic aortic aneurysms (TAA) represent medical conditions having causes that can range from genetic determinations to various risk factors, having potential life-threatening complications, the familial TAA (FTAA) being a cluster of non-syndromic thoracic aortic aneurysms. This review aims to emphasize the importance of genetic testing in patients diagnosed with thoracic aortic aneurysms, the genetic implications accounting for roughly 20% of these cases. The reported case presents a patient who was genetically tested 10 years after a Bentall procedure, which was performed for acute DeBakey type I aortic dissection developed in her second pregnancy, when the patient started presenting recurrent prolonged febrile syndrome. She was tested positive for a missense variant in the actin alpha-2 (ACTA2) gene, in heterozygous status, but also serological tests revealed the presence of an infection with Coxiella burnetii. Methods: For a better understanding of both conditions, our research was conducted on two directions, one reviewing the literature on patients with Coxiella burnetii blood culture-negative infective endocarditis (BCNIE) and the other one, focusing on patients having familial thoracic aortic aneurysm (FTAA) due to ACTA2 mutation. This review incorporates studies found on PubMed and ResearchGate up to August 2024. Conclusions: BCNIE represents a condition with several diagnosis challenges and may lead to severe complications if timely treatment is not initiated. Also, diagnosing FTAA requires more frequent genetic testing, enabling a better follow-up and management.
Keywords:
thoracic aortic aneurysms
; ACTA2 gene variant
; Coxiella burnetii
; infective endocarditis
; chronic Q fever
1. Introduction
Thoracic aortic aneurysms (TAA) are known as dilation of the vessel calibre, the aortic diameter thresholds having to always be adapted to physical measurements, such as height and weight (1,2). In addition to the etiology involving inflammatory and infectious diseases or risk factors, such as hypertension and hypercholesterolemia, genetic factors implicated in the physiopathology of vascular wall syndromes have gained significant importance in recent years, classification and management of aortic aneurysms being guided by the presence of positive family history [3,4]. The latest AHA Guidelines for the Diagnosis and Management of Aortic Disease recommends routine genetic testing of patients diagnosed with thoracic aortic aneurysm at young ages or having features associated with specific syndromes, but also DNA sequencing should be performed on known at-risk relatives of individuals with positive results [2]. FTAA are caused by the association with mutations of either extracellular matrix proteins function or vascular smooth muscle proteins [1]. TAA can be divided into two main subtypes depending on multiorgan damage, the branches being referred as syndromic or non-syndromic. The syndromic ones refer to diseases affecting both the vascular system and other connective tissue abnormalities, the most notable examples of this group being represented by Loeys-Dietz syndrome, Marfan syndrome or vascular Ehlers-Danlos syndrome. In addition, non-syndromic TAA are defined by their impact solely on the cardiovascular system [5].
The pathogenic genes involved in the pathway of FTAA are the ones affecting proteins that ensure the integrity of the vascular wall, particularly vascular smooth muscle cells. There are multiple genes that can determine a familial pattern of thoracic aortic aneurysms, most of them having autosomal dominant inheritance, the highest studied and prominently featured in the academic field being ACTA2, MYH11, MYLK, PRKG1 and those involved in TGF-β pathway [6,7]. Pathogenic variants of ACTA-2 gene, the one that encodes α-actin, are some of the most frequent etiologies of FTAA. Alfa-actin expresses almost half of the total proteins in smooth muscle cells (up to 40%), thus making it the most representative protein at this level [6]. The pathogenic variants of the ACTA-2 gene, in addition to the cardiovascular disorders it produces, predispose the patients to other forms of vascular pathologies, including Moyamoya-like occlusions which can lead to early onset of cerebrovascular events or occlusions of internal carotid arteries or intracranial aneurysms [8,9,10].
On the other hand, the reported case is one with complex particularities, several medical specialties being involved, both the patients’ genetic and infectious pathology leading to consequences on the cardiovascular system. The infectious disease that the patient contacted during the last years was the infection with Coxiella burnetii. This micro-organism is the causative agent of Q fever, being intracellular gram-negative bacteria, and is usually transmitted from animals, like goats or sheep, directly, or indirectly by ticks [11,12]. It has been repeatedly stated as a potential biological thread because it can be transmitted through inhalation, it has a low infective dose and its environmental stability [13,14]. The acute onset of the disease reveals high fever and flu-like symptoms, for example nonproductive cough, but because of the non-specific symptoms, the treatment is not always administered on time, converting the Q fever into a chronic disease [15,16]. The only method of preventing the disease is through the immunization achieved by the Q-vax vaccine, but it is currently only administered in Australia [17].
The most common manifestation of chronic Q fever is blood culture-negative infective endocarditis, but in some cases the onset form may be represented by hepatitis, osteomyelitis, febrile illness lasting up to fifty days and even neurological pathology, illustrated by encephalitis, meningitis or peripheral neuropathy [18,19].
The specific treatment of Coxiella Burnetii infection is the administration of Doxycicline for 14 days for the acute infection, but in case of chronic Q fever, a combination of Doxycicline and Hydroxichloroquine should be administered up to 18 months [20,21]. According to the 2023 ESC Guidelines for the management of endocarditis, blood culture-negative infective endocarditis caused by Coxiella burnetii should consists of Doxycycline 200 mg/24h and hydroxychloroquine 200-600 mg/24h for minimum of 18 months [22].
2. Materials and Methods
The main information sources of the studies examined in this review are PubMed and ResearchGate. The database was selected based on the inclusions criteria described above, the elected articles that resemble the reported case including only those published since January 2000. The following keywords were used to maximize search accuracy: “Coxiella bunetii infection”, “Q fever”, “mechanical aortic valve”, “blood culture negative infective endocarditis”, for the first quest and “familial thoracic aortic aneurysm”, “ACTA2 mutation”, “aortic dissection”, “ACTA2 gene”. The MeSH function on PubMed was used to increase the specificity of the research, by using combinations of the keywords. The discovered articles were added to Zotero application, the ones intentified as duplicates being removed.
3. Results
The reported case describes a 45-year-old woman known to have multiple cardiovascular conditions and positive family history, namely her mother died at 36 years of unknown causes (possible, spontaneous carotid artery dissection). The patient developed during her second pregnancy acute aortic dissection DeBakey type I treated surgically by a Bentall procedure in 2006 by replacing the aortic valve and the ascending aorta with a valved composite graft with re-implantation of the coronary arteries into the graft.
The clinical evolution of the patient was favourable for the first 15 years, following only chronic anticoagulant treatment with Acenocumarol 4 mg, adjusted in accordance with the INR test. In December 2021 she started developing a prolonged febrile syndrome, which was extensively investigated and treated with antibiotics several times. For two years, the patient was hospitalized in various clinics and repeatedly sets of blood cultures were performed, all with negative results. After all investigations carried out, the established diagnoses were blood culture-negative infective endocarditis on mechanical aortic valve, anti-neutropfil cytoplasmic antibodies (ANCA)-associated systemic vasculitis, chronic glomerulonephritis (nephritic syndrome form), with splenic infarction and diet-controlled type 2 diabetes.
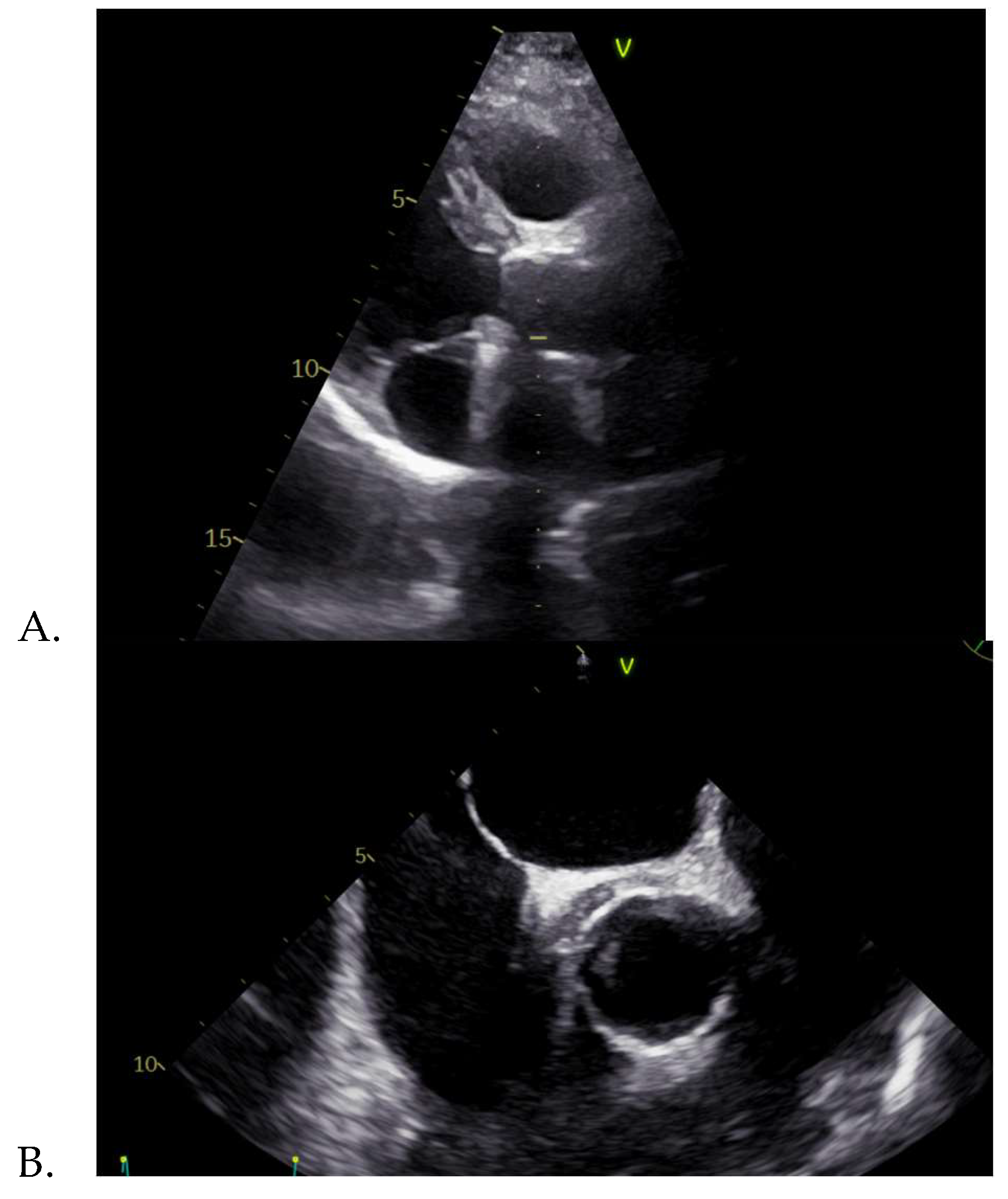
In June 2024, the patient was admitted in our clinic, accusing intermittent febrile syndrome with subfebrile onset for about 3 months, accompanied by vertigo. The medical examination revealed normal vital signs, pale skin and the cardiac examination highlighted a systolic murmur, heard loudest at aortic area, closing click on aortic area. The ECG was normal. The pathological blood samples collected at admission revealed an inflammatory syndrome, i.e. highly elevated ESR and C- reactive protein, with positive procalcitonin. The transthoracic echocardiography showed an apparently normal mechanical prosthesis in aortic position, mild intraprosthetic aortic regurgitation, mild mitral regurgitation, mild functional tricuspid regurgitation, mild secondary pulmonary hypertension and a roughly 12 mm, echo-dense mass surrounding the ascending aorta, this image being also found on the transesophageal echocardiography. Transesophageal echocardiography is an investigation that provides additional information on heart morphology, usually being used for a better view of the left atrium and the left atrial appendage in order to detect thrombi, but in our case it was used for a better acquisition of the aortic valve [23,24].
Figure 1.
A. Transthoracic and B. Transesophageal echocardiography showing an echo-dense mass surrounding the ascending aorta.
Figure 1.
A. Transthoracic and B. Transesophageal echocardiography showing an echo-dense mass surrounding the ascending aorta.
On the second day after admission, the patient experienced a subfebrile episode, which prompted the collection of blood cultures, but the results were negative. Consequently, more specific investigations were performed, serological tests for infective endocarditis of diverse etiology being acquired, IgG and IgM antibodies for Mycoplasma pneumoniae, Bartonella henselae, Chlamydophila pneumoniae, Brucella spp., Legionella pneumophila, but also Coxiella burnetii. All results were negative, except for Coxiella burnetii IgG and IgM phase I and phase II antibodies, and the results highlighted both phase I and phase II immunofluorescent assay (IFA) increased antibody titre, as seen in Table 1. Likewise, the PCR for Coxiella burnetii in blood by molecular hybridization with amplification test revealed also a positive result. Therefore, the diagnosis of acute onset of a chronic Q fever disease was confirmed and the targeted therapy with Hydroxychloroquine 200 mg tid and Doxycycline 100 mg bid was initiated and will continue to be administered for 18 months. A relevant reference is the patient travel history, starting with 2021 year the patient was not traveling abroad and no direct link could be made to a potential source of infection, such as domestic animals. However, from 2006 to 2011 the patient travelled to several African countries for about 3 months/year and staring 2012 she travelled several times to Switzerland and Germany.
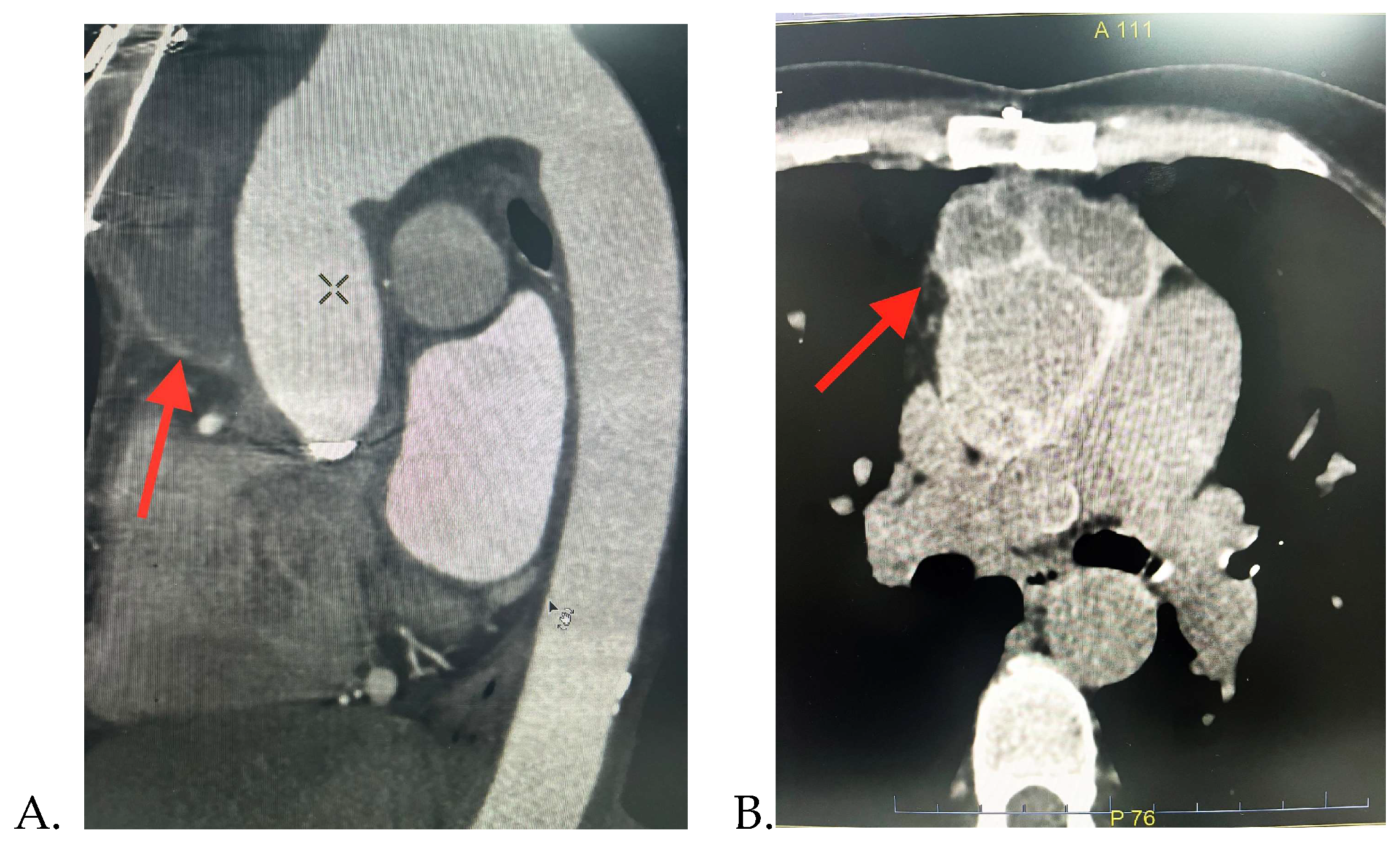
Alternatively, due to the echocardiographic images revealing a significant peri-aortic mass, it was decided to perform further investigations. The thorax CT scan detected a multiloculated right semi-circumferential fluid accumulation with iodophilic walls that extends from the level of the aortic valve along the aortic prosthesis to the anterior mediastinum, suggesting a peri-aortic abscess. Pericardial and pleural fluid collection and mediastinal adenopathies were also found.
Figure 2.
Thorax CT-scan images showing the periaortic fluid accumulation (red arrow): A. Sagittal; and B. Axial section.
Figure 2.
Thorax CT-scan images showing the periaortic fluid accumulation (red arrow): A. Sagittal; and B. Axial section.
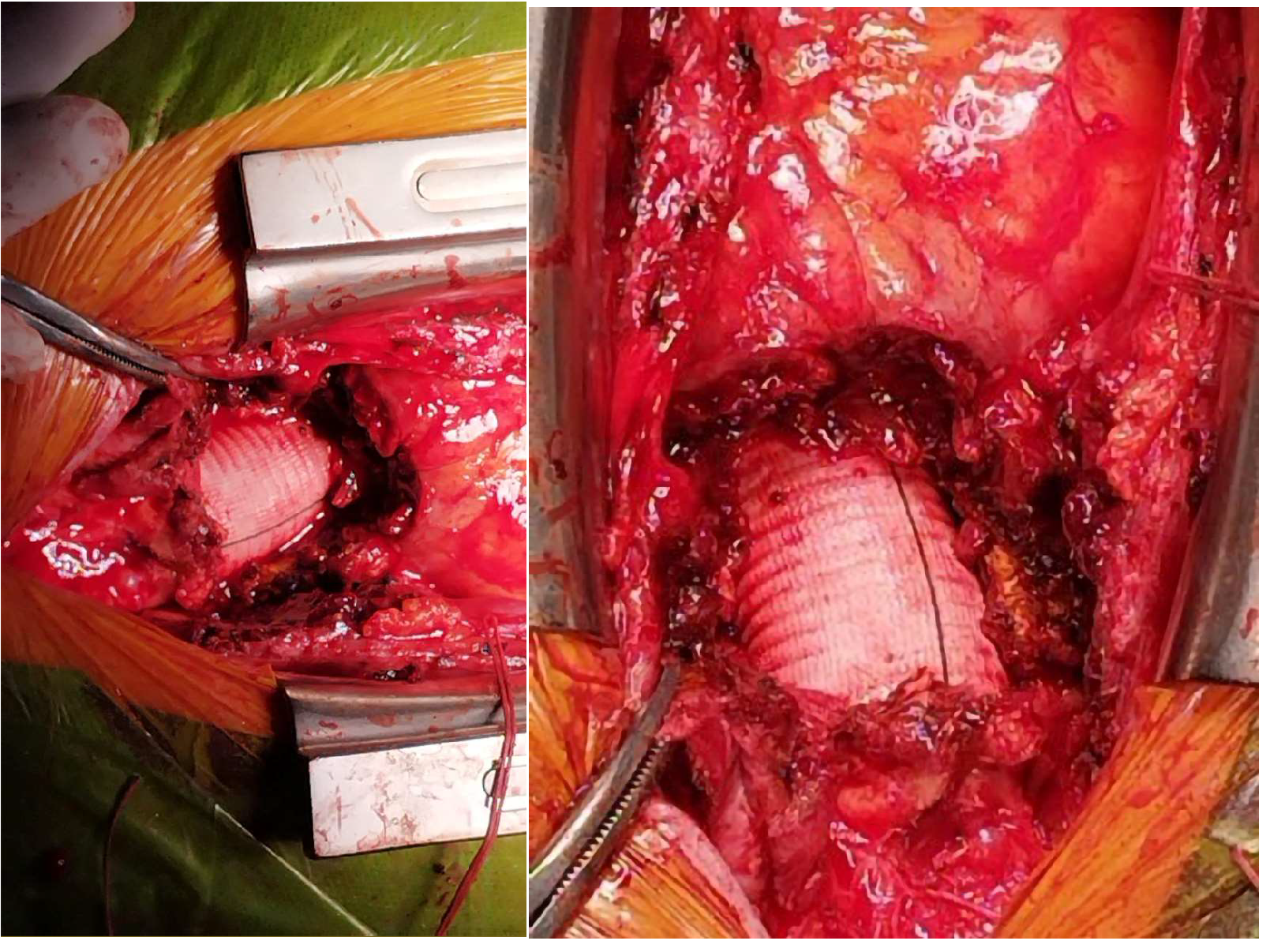
The preliminary diagnosis was Coxiella burnetii infective endocarditis complicated with mediastinal abscess; thus, a multidisciplinary team, consisting of a cardiologist, cardiovascular surgeon, infectionist and intensive care physician decided that the optimal management in this case would be a surgical redo operation with antibiotic protection. The surgery involved the removal of the periaortic fluid mass, the macroscopic examination being suggestive with a liquefied chronic haematoma. The bacteriological examination of the collected biological products, pericardial fragment, periprosthetic and subprosthetic tissue and clot fragment revealed no bacterial or fungal growth on the inoculated culture media.
The post-operative evolution was favorable and the investigations continued with the genetic testing of the patient, considering the family history and the onset at a young age of her aortic pathology. A missense variant was detected, in heterozygous status, in the ACTA2 gene, located on chromosome 10q23.31. This variant has been found in several individuals with FTA, segregated by phenotype. The variant was classified as one with pathogenic significance, according to the American College of Medical Genetics and Genomics (ACMG) guideline [25]. As a result, the suspicion of a genetic disease was confirmed, establishing the diagnosis of familial thoracic aortic aneurysm 6, being part of non-syndromic FTAA cluster. In some cases, the pathogenic variant of ACTA2 is associated with intracranial aneurysms and Moyamoya-like cerebrovascular disease, so the patient will be undergoing a cranial CT-scan [26]. Hence, her two daughters are proposed to be genetically tested and will be followed-up with echocardiographic examinations.
Figure 3.
Intraoperative images showing the periaortic fluid accumulation.
The patient was discharged having a good general condition with the following diagnosis: blood culture-negative infective endocarditis with Coxiella burnetii, liquefied chronic periprosthetic haematoma (surgically treated), status post Bentall operation, normofunctional double disc mechanical prosthesis in aortic position, mild mitral regurgitation, mild functional tricuspid regurgitation, mild secondary pulmonary hypertension, NYHA I chronic heart failure with preserved ejection fraction, diet-controlled type 2 diabetes, ANCA-associated systemic vasculitis, chronic glomerulonephritis (nephritic syndrome form), enlarged spleen with subcapsular infarction, mild normochromic normocytic anaemia and the following treatment being recommended at home: Hydroxychloroquine 200 mg/tid, Doxycycline 100 mg bid, Acenocoumarol 4 mg (dose controlled by INR test in order to maintain a value between 2,5-3,5), diuretics (association between Furosemide/Spironolactone 20/50 mg/day) and a probiotic. The only side effects reported by the patient regarding the specific medication for Coxiella burnetii was insomnia and tinnitus.
4. Discussion
In order to perform an accurate review starting with the reported case, which included two major significant pathologies, both a genetically inherited disease, ACTA2 mutation gene leading to a familial thoracic aortic aneurysm and dissection, as well as a rare infectious disease, namely blood culture-negative infective endocarditis on a mechanical aortic valve, the research on the medical literature started by looking for the coexistence of both pathologies, but it failed to identify any patient similar to the case presented above.
Therefore, our research was oriented toward searching separately the two intricate pathologies, the review encompassing medical articles describing, on one hand, blood culture-negative infective endocarditis with Coxiella burnetii on mechanical aortic valve and, on the other hand, studies presenting patients having familial thoracic aortic aneurysm and/or dissection due to ACTA2 mutation.
Firstly, in the interest of achieving similarities between the described patient’s infectious disease with cardiovascular implications and the patients included in the chosen studies, we identified articles published on the medical literature between 2000 and August 2024, available on PubMed and ResearchGate. The inclusion criteria the articles selected had to meet were: patients already having in their medical history a surgery of replacing the native aortic valve with a prosthetic one; patients diagnosed with Coxiella burnetii blood culture-negative infective endocarditis; studies including clear diagnosis and management parameters, having an explicit outcome of the patients; articles published in the target period of time; studies defined as case reports. The exclusion criteria were: studies published before 2000; studies having other qualities than case reports; articles that did not follow an accurate patient managements detail; studies not including human participants. The designed research strategy was designed using keywords and phrases closely relevant to the reported case, thus the keywords included were: “Coxiella bunetii infection”, “Q fever”, “mechanical aortic valve”, “blood culture negative infective endocarditis”.
There were 4 identified case reports describing Coxiella burnetii associated blood culture-negative infective endocarditis on prosthesis aortic valve, as seen in Table 2.
The most frequently described symptom in these patients was fever and in most of the cases the febrile symptomatology started about a month before the presentation. In our patient, fever was a present for about 2 and half years, with periods of remission, subfebrility or aggravation episodes.
The treatment in two of the cases was exclusively medical, one patient benefited from surgical intervention and one case was managed through both medical and surgical therapy. One case was treated with a special antibiotic, as Afrasiabian et al. [29] described intolerance to doxycycline, and thus the antibiotic treatment chosen instead was levofloxacin. Krol et al. [30] also preferred the administration of monotherapy with doxycycline for 5 months, having a favorable result, the patient outcome being an improved one. The treatment preferred by Bozza et al. [27] was the administration of doxycycline 100 mg/bid in association with hydroxychloroquine 200 mg/tid for 24 months, with a long-term follow-up of the patient, which proved the efficacity of the used antibiotics with a decreasing trend of the serological tests. This combination of antibiotics was also chosen for the patient treated in our clinic, being well tolerated by the patient, without fever remissions.
In addition, a second part of the research was the comparison of the patients’ evolution regarding the aortic disease caused by ACTA2 mutation with the patients described in the chosen articles. The accomplished research among the medical literature provided five case reports published between 2000 and August 2025, cases describing patients having thoracic aortic aneurysm with a positive history family and ACTA2 mutation, as seen in Table 3. The inclusion criteria were: patients presenting any type of mutation in ACTA2 gene expressing vascular smooth muscle cells; studies having the quality of case reports; studies providing clear evidence of patient management. On the other hand, the exclusion criteria were: studies not involving human participants; studies published before the year 2000; studies with other characteristics than case reports. The examination was conducted among the database found on PubMed and ResearchGate.
The prevalence of the targeted aortic pathology was found to be higher among men, with 57.1% of the patients described in the selected studies being males. Similar to these results, the ACTA2 mutation gene was discovered to be more significant among the male population. Concerning the average age of patients with familial thoracic aortic aneurysm, the oldest patient experiencing an acute onset of the condition was 41 years old as described by Hoffjan et al. [31], while the youngest was just 15 years old, namely the study published by Ware et al. [32] presenting the twins who developed acute aortic dissection at the same time. On the other hand, in the patients’ family history, cases carrying the mutant gene were identified, cases being discovered after genetic counselling and testing, but who did not experience any clinical manifestation of the disease. Similar to the reported data in the literature, our clinical patient onset was very early, the acute aortic dissection occurred at the age of 27.
Among the included patients, only two of them presented a notable phenotypic manifestation, namely congenital mydriasis in the twins described by Ware et al [32]. This clinical expression was also described in the specialized literature as being strongly associated with a particular missense mutation in arginine 179 in the ACTA2 gene [5].
The complexity of the reported case arises from the early onset of the aortic disease, the patient being 7 months pregnant when she presented at the hospital for acute aortic dissection. This circumstance is consistent to the documented data regarding the evolution of pregnancies in females with ACTA2 mutation [33]. Thus, Hoffjan et al [31]. described two patients having a history of physiological pregnancy before being diagnosed with mild aortic dilation and acute aortic dissection. The academic literature describes a powerful connection between an underlying aortic disease and aortic dissection associated with pregnancy. Fluctuations in pregnancy hormone levels along with the hemodynamic stress experienced by the pregnant women can exacerbate a subjacent aortic condition, particularly during the third trimester [34].

Table 3.
Patients presenting ACTA2 mutation and their characteristics.
| No | First author/Year/Reference | No. of patiens/Gender/Age | Medical history of aortic disease | Family history of aortic disease | Clinical features | Healthy pregnancy |
|---|---|---|---|---|---|---|
| 1. |
Hoffjan et al., 2011, [31] |
3 patients a.F,38 b.F,37 c.M, 41 |
a.Mild aortic dilation b.acute aortic dissection c. Thoracic aortic aneurysm |
a.1 brother-ascending aorta aneurysm and died at 46 years old; 1 brother and the father-thoracic aortic aneurysm b. 1 brother-died at 29 years old from acute aortic dissection c.no data available |
Not described |
a.2 healthy pregnancies b.2 healthy pregnancies c.- |
| 2. |
Keravnou et al., 2018, [35] |
1/M/30 | Type A aortic dissection | Father-aortic root and ascending aorta aneurysm (Bentall procedure performed) Mother-ascending aortic dilation |
Not described |
- |
| 3. | Marutani et al., 2023 [36] | 1/M/15 | Extensive dissection from the ascending aorta to the common iliac artery | Genetical tests not performed |
Not described |
- |
| 4. | Ware et al., 2014 [32] | 1/M/17 | Recurrent aortic dissection, severe aortic regurgitation | Twin brother- aortic dissection | Congenital mydriasis (both twins) |
- |
| 5. | Delsart et al., 2021 [37] | 1/F/29 | DeBakey type I aortic dissection | 2 siblings-acute aortic dissection Mother-died at 49 years old from type B aortic dissection |
Not described | No pregnancies |
5. Conclusions
To summarise, familial thoracic aortic aneurysm is a condition with high rate of mortality if not properly diagnosed and monitored over time. These findings should encourage more frequent genetic testing in patients having aortic aneurysms, especially those with significant familial medical history or having an early onset of the aortic disease. Additionally, a condition with particular importance, but meaningful diagnostic and therapeutical challenges is blood culture-negative infective endocarditis. Rare causes should be investigated and serological testing for infectious agents such as Coxiella burnetii ought to consider.
Author Contributions
Conceptualization, A.-R.C., C.G.S., M.-I.B., S.C., M.-A.L., M.-D.V., A.-T.I., R.-E.S., D.-C.D., A.E.-M., A.L., D.G., C.-T.L.; methodology, A.-R.C., C.G.S., C.-T.L. ; software, A.-R.C., C.G.S., M.-I.B., C.-T.L.; validation, A.-R.C., C.G.S., M.-I.B., S.C., M.-A.L., M.-D.V., A.-T.I., R.-E.S., D.-C.D., A.E.-M., A.L., C.-T.L. ; formal analysis, A.-R.C., C.G.S., C.-T.L.; investigation, A.-R.C., C.G.S., M.-I.B. C.-T.L..; resources, A.-R.C., C.G.S., M.-I.B., C.-T.L.; data curation, A.-R.C., C.G.S., C.-T.L.; writing—original draft preparation, A.-R.C., C.G.S., M.-I.B., S.C., M.-A.L., M.-D.V., A.-T.I., R.-E.S., D.-C.D., A.E.-M., A.L., D.G., C.-T.L.; writing—review and editing, A.-R.C., C.G.S., M.-I.B., A.L., C.-T.L..; visualization, A.-R.C., C.G.S., C.-T.L.; supervision, A.-R.C., C.G.S., C.-T.L.; project administration, A.-R.C., C.G.S., C.-T.L.; funding acquisition, A.-R.C., C.G.S., C.-T.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. Internal funding: we would like to acknowledge the “Victor Babeș” University of Medicine and Pharmacy, Timișoara, for their support in covering the costs of publication for this research paper.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki, and was approved by the Ethics Committee of the Institute for Cardiovascular Diseases of Timisoara (Nr. 5300/9 July 2024).
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Data Availability Statement
All data are mentioned in the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Goyal, A.; Keramati, A.R.; Czarny, M.J.; Resar, J.R.; Mani, A. The Genetics of Aortopathies in Clinical Cardiology. Clin. Med. Insights: Cardiol. 2017, 11. [Google Scholar] [CrossRef] [PubMed]
- Isselbacher, E.M.; Preventza, O.; Black, J.H.; Augoustides, J.G.; Beck, A.W.; Bolen, M.A.; Braverman, A.C.; Bray, B.E.; Brown-Zimmerman, M.M.; Chen, E.P.; et al. 2022 ACC/AHA Guideline for the Diagnosis and Management of Aortic Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation 2022, 146, E334–E482. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Z.; Cecchi, A.C.; Prakash, S.K.; Milewicz, D.M. Risk Factors for Thoracic Aortic Dissection. Genes 2022, 13, 1814. [Google Scholar] [CrossRef] [PubMed]
- Ince, H.; A Nienaber, C. Etiology, pathogenesis and management of thoracic aortic aneurysm. Nat. Clin. Pr. Cardiovasc. Med. 2007, 4, 418–427. [Google Scholar] [CrossRef]
- Isselbacher, E.M.; Cardenas, C.L.L.; Lindsay, M.E. Hereditary Influence in Thoracic Aortic Aneurysm and Dissection. Circulation 2016, 133, 2516–2528. [Google Scholar] [CrossRef]
- Pinard, A.; Jones, G.T.; Milewicz, D.M. Genetics of Thoracic and Abdominal Aortic Diseases: Aneurysms, Dissections, and Ruptures. Circ. Res. 2019, 124, 588–606. [Google Scholar] [CrossRef]
- Renard, M.; Francis, C.; Ghosh, R.; Scott, A.F.; Witmer, P.D.; Adès, L.C.; Andelfinger, G.U.; Arnaud, P.; Boileau, C.; Callewaert, B.L.; et al. Clinical Validity of Genes for Heritable Thoracic Aortic Aneurysm and Dissection. Circ. 2018, 72, 605–615. [Google Scholar] [CrossRef]
- Guo, D.-C.; Pannu, H.; Tran-Fadulu, V.; Papke, C.L.; Yu, R.K.; Avidan, N.; Bourgeois, S.; Estrera, A.L.; Safi, H.J.; Sparks, E.; et al. Mutations in smooth muscle α-actin (ACTA2) lead to thoracic aortic aneurysms and dissections. Nat. Genet. 2007, 39, 1488–1493. [Google Scholar] [CrossRef]
- Guo, D.-C.; Papke, C.L.; Tran-Fadulu, V.; Regalado, E.S.; Avidan, N.; Johnson, R.J.; Kim, D.H.; Pannu, H.; Willing, M.C.; Sparks, E.; et al. Mutations in Smooth Muscle Alpha-Actin (ACTA2) Cause Coronary Artery Disease, Stroke, and Moyamoya Disease, Along with Thoracic Aortic Disease. Am. J. Hum. Genet. 2009, 84, 617–627. [Google Scholar] [CrossRef]
- Roder, C.; Peters, V.; Kasuya, H.; Nishizawa, T.; Wakita, S.; Berg, D.; Schulte, C.; Khan, N.; Tatagiba, M.; Krischek, B. Analysis of ACTA2 in European Moyamoya disease patients. Eur. J. Paediatr. Neurol. 2011, 15, 117–122. [Google Scholar] [CrossRef]
- Dragan, A.L.; Voth, D.E. Coxiella burnetii: international pathogen of mystery. Microbes Infect. 2019, 22, 100–110. [Google Scholar] [CrossRef] [PubMed]
- Neupane K, Kaswan D. Coxiella burnetii Infection. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 [cited 2024 Oct 22]. Available from: http://www.ncbi.nlm.nih.gov/books/NBK557893/.
- Madariaga, M.G.; Rezai, K.; Trenholme, G.M.; A Weinstein, R. Q fever: a biological weapon in your backyard. Lancet Infect. Dis. 2003, 3, 709–721. [Google Scholar] [CrossRef] [PubMed]
- Oyston, P.C.F.; Davies, C. Q fever: the neglected biothreat agent. J. Med Microbiol. 2011, 60, 9–21. [Google Scholar] [CrossRef] [PubMed]
- Cherry, C.C.; Nichols Heitman, K.; Bestul, N.C.; Kersh, G.J. Acute and chronic Q fever national surveillance – United States, 2008–2017. Zoonoses Public Health 2022, 69, 73–82. [Google Scholar] [CrossRef]
- España, P.P.; Uranga, A.; Cillóniz, C.; Torres, A. Q Fever (Coxiella Burnetii). Semin. Respir. Crit. Care Med. 2020, 41, 509–521. [Google Scholar] [CrossRef]
- Chiu, C.K.; Durrheim, D.N. A review of the efficacy of human Q fever vaccine registered in Australia. New South Wales Public Heal. Bull. 2007, 18, 133–6. [Google Scholar] [CrossRef]
- Raoult, D.; Tissot-Dupont, H.; Foucault, C.; Gouvernet, J.; Fournier, P.E.; Bernit, E.; Stein, A.; Nesri, M.; Harle, J.R.; Weiller, P.J. Q Fever 1985-1998: Clinical and Epidemiologic Features of 1,383 Infections. Medicine 2000, 79, 109–123. [Google Scholar] [CrossRef]
- Kofteridis, D.P.; Mazokopakis, E.E.; Tselentis, Y.; Gikas, A. Neurological complications of acute Q fever infection. Eur. J. Epidemiology 2004, 19, 1051–1054. [Google Scholar] [CrossRef]
- Million, M.; Lepidi, H.; Raoult DFièvre, Q. actualités diagnostiques et thérapeutiques. Médecine Mal Infect. 2009, 39, 82–94. [Google Scholar] [CrossRef]
- Raoult, D.; Houpikian, P.; Dupont, H.T.; Riss, J.M.; Arditi-Djiane, J.; Brouqui, P. Treatment of Q Fever Endocarditis: Comparison of 2 Regimens Containing Doxycycline and Ofloxacin or Hydroxychloroquine. Arch Intern Med. 1999, 159, 167. [Google Scholar] [CrossRef]
- Delgado, V.; Marsan, N.A.; de Waha, S.; Bonaros, N.; Brida, M.; Burri, H.; Caselli, S.; Doenst, T.; Ederhy, S.; Erba, P.A.; et al. Correction to: 2023 ESC Guidelines for the management of endocarditis: Developed by the task force on the management of endocarditis of the European Society of Cardiology (ESC) Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Nuclear Medicine (EANM). Eur. Hear. J. 2023, 45, 56–56. [Google Scholar] [CrossRef]
- Cozma, D.; Streian, C.G.; Vacarescu, C.; Mornos, C. Back to sinus rhythm from atrial flutter or fibrillation: dabigatran is safe without transoesophageal control. Kardiologia Polska 2016, 74, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Arnautu, S.F.; Arnautu, D.A.; Lascu, A.; Hajevschi, A.A.; Rosca, C.I.I.; Sharma, A.; Jianu, D.C. A Review of the Role of Transthoracic and Transesophageal Echocardiography, Computed Tomography, and Magnetic Resonance Imaging in Cardioembolic Stroke. Med Sci. Monit. 2022, 28, e936365–1. [Google Scholar] [CrossRef]
- Richards, S.; Aziz, N.; Bale, S.; Bick, D.; Das, S.; Gastier-Foster, J.; Grody, W.W.; Hegde, M.; Lyon, E.; Spector, E.; et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet. Med. 2015, 17, 405–424. [Google Scholar] [CrossRef]
- Roder, C.; Nayak, N.R.; Khan, N.; Tatagiba, M.; Inoue, I.; Krischek, B. Genetics of Moyamoya disease. J. Hum. Genet. 2010, 55, 711–716. [Google Scholar] [CrossRef]
- Bozza, S.; Graziani, A.; Borghi, M.; Marini, D.; Duranti, M.; Camilloni, B. Case report: Coxiella burnetii endocarditis in the absence of evident exposure. Front. Med. 2023, 10, 1220205. [Google Scholar] [CrossRef]
- Deyell, M.W.; Chiu, B.; Ross, D.B.; Alvarez, N. Q fever endocarditis: A case report and review of the literature. Can. J. Cardiol. 2006, 22, 781–785. [Google Scholar] [CrossRef]
- Afrasiabian, S.; Esmaeili, S.; Hajibagheri, K.; Hadizadeh, N.; Lotfi, G.; Veysi, A. Endocarditis Caused by Coxiella burnetii: A Case Report in Western Iran. J. Arthropod-Borne Dis. 2024, 18, 78–83. [Google Scholar] [CrossRef]
- Krol, V.; Kogan, V.; Cunha, B.A. Q fever bioprosthetic aortic valve endocarditis (PVE) successfully treated with doxycycline monotherapy. Hear. Lung 2008, 37, 157–160. [Google Scholar] [CrossRef]
- Hoffjan, S.; Waldmüller, S.; Blankenfeldt, W.; Kötting, J.; Gehle, P.; Binner, P.; Epplen, J.T.; Scheffold, T. Three novel mutations in the ACTA2 gene in German patients with thoracic aortic aneurysms and dissections. Eur. J. Hum. Genet. 2011, 19, 520–524. [Google Scholar] [CrossRef]
- Ware, S.M.; Shikany, A.; Landis, B.J.; James, J.F.; Hinton, R.B. Twins With Progressive Thoracic Aortic Aneurysm, Recurrent Dissection and ACTA2 Mutation. Pediatrics 2014, 134, e1218–e1223. [Google Scholar] [CrossRef] [PubMed]
- Coulon, C. Thoracic aortic aneurysms and pregnancy. Presse Médicale 2015, 44, 1126–1135. [Google Scholar] [CrossRef] [PubMed]
- Braverman, A.C.; Mittauer, E.; Harris, K.M.; Evangelista, A.; Pyeritz, R.E.; Brinster, D.; Conklin, L.; Suzuki, T.; Fanola, C.; Ouzounian, M.; et al. Clinical Features and Outcomes of Pregnancy-Related Acute Aortic Dissection. JAMA Cardiol. 2021, 6, 58–66. [Google Scholar] [CrossRef] [PubMed]
- Keravnou, A.; Bashiardes, E.; Michailidou, K.; Soteriou, M.; Moushi, A.; Cariolou, M. Novel variants in the ACTA2 and MYH11 genes in a Cypriot family with thoracic aortic aneurysms: a case report. BMC Med Genet. 2018, 19, 208. [Google Scholar] [CrossRef]
- Marutani, S.; Nishino, T.; Shimokawa, O.; Pooh, R.K.; Morisaki, H.; Inamura, N. Aortic Dissection and a Previously Unreported ACTA2 Missense Variant Mutation in a Young Patient: A Case Report. Pediatr. Dev. Pathol. 2023, 26, 494–498. [Google Scholar] [CrossRef]
- Delsart, P.; Vanlerberghe, C.; Juthier, F.; Sobocinski, J.; Domanski, O.; Longere, B.; Hanna, N.; Arnaud, P.; Marsili, L. The natural history of a family with aortic dissection associated with a novel ACTA2 variant. Ann. Vasc. Surg. 2021, 77, 348–e7. [Google Scholar] [CrossRef]
Table 1.
Serology of Coxiella burnetii antibodies.
| Serology | Value |
|---|---|
| IgG phase I antibodies | |
| >1:4096 | |
| IgM phase I antibodies | |
| 1:2024 | |
| IgG phase II antibodies | |
| >1:4096 | |
| IgM phase II antibodies | |
| 1:1024 |
Table 2.
Patients presenting Coxiella burnetii blood culture-negative endocarditis and their characteristics.
Table 2.
Patients presenting Coxiella burnetii blood culture-negative endocarditis and their characteristics.
| No | First author/Year/Reference | No. of patiens/Gender/Age | History of cardiovascular surgery | Fever history | Surgical or medical treatment |
|---|---|---|---|---|---|
| 1 | Bozza et al, 2023[27] | 1/M/55 | Aortic valve replacement (aortic regurgitation and aneurysm) | 1 month | Medical: doxycycline (100 mg/bid) and hydroxychloroquine (200 mg/tid |
| 2 | Deyell et al, 2006 [28] | 1/M/31 | Open valvulotomy for congenital aortic stenosis + mechanical aortic replacement for severe aortic regurgitation | Not described | Surgical: Aortic root replacement of the ascending aorta and aortic valve replacement |
| 3 | Afrasiabian et al, 2024 [29] | 1/F/67 | Aortic valve replacement | 1 month | Medical (Levofloxacin-intolerance of doxycycline) |
| 4 | Krol et al, 2008 [30] | 1/F/43 | Aortic valve replacement (bicuspid aortic valve) | Fever history, but no time described | Both: Medical (doxycycline monotherapy) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



