
Submitted:
29 October 2024
Posted:
30 October 2024
You are already at the latest version
Abstract
Cancer ranks among the primary contributors to global mortality. In 2022, the global incidence of new cancer cases reached about 20 million, while the number of cancer-related fatalities reached 9.7 million. Exclusively in Saudi Arabia, there are 13,399 deaths caused by cancer and 28,113 newly diagnosed cases of cancer. Drug repurposing is a drug discovery strategy that gained special attention and implementation to enhance the process of drug development due to its time and money saving effect. It involves repositioning existing medications to new clinical applications. Cancer treatment is one of the most therapeutic areas where drug repurposing has shown prominent impact. This review presents a compilation of medications that have been repurposed for the treatment of various types of cancers. It describes the initial therapeutic and pharmacological classes of the repurposed drugs and their new applications and mechanism of action in cancer treatment. The review reports on drugs from various pharmacological classes that have been successfully repurposed for cancer treatment including approved ones and those in clinical trials and preclinical development. It stratifies drugs based on their anticancer repurpose as multi-type, type-specific, and mechanism directed and according to their pharmacological classes. The review also reflects on the future potential that drug repurposing has in the clinical development of novel anticancer therapies.
Keywords:
Repurposing
; Anticancer
; Drug Discovery
; Therapeutic Classes
; Translational Research
; Drug Targets
1. Introduction
Cancer is a collection of multiple diseases that occur progressively due to uncontrollable cell proliferation [1,2]. Each type has unique characteristics, but all share fundamental processes contributing to the disease’s development [3,4]. Cancer cells can be malignant or normal, and they expand when not provided with signals, disregarding signals to cease proliferation or undergo apoptosis. They direct vascular proliferation towards malignancies, providing oxygen and nutrition while eliminating toxic materials. They also avoid the immune system’s attention, facilitating their proliferation and survival. Cancer cells often obtain a diverse array of chromosomal modifications, which they rely on to the extent they cannot function normally [5].
Tumor progression is typically illustrated through stages of mutation and growth. A normal cell is transformed into a malignant cell with less than 10 mutations [6,7]. Stages include initial mutation, hyperplasia, dysplasia, in situ cancer, and invasive/malignant tumor. In situ cancer is characterized by abnormal development and appearance of the cell and its progeny, while invasive/malignant tumors allow the tumor to disseminate to other tissues and discharge cells into the lymph or bloodstream, potentially generating new malignancies.
Malignant tumors can spread throughout the body, causing resistance to targeted therapy [8]. Cancer-critical genes are categorized into two primary categories: proto-oncogenes and tumor suppressor genes [9]. Proto-oncogenes facilitate cell proliferation, while tumor suppressor genes prevent it. Mutations in these genes can lead to the overactivity of proteins involved in growth-promoting pathways, causing cells to multiply faster than they would without mutation [10].
Most malignancies are classified into three main categories: carcinomas, sarcomas, leukemias or lymphomas. Carcinomas account for 90% of human cancers, while sarcomas are solid tumors affecting connective tissues. Lymphomas and leukemias are caused by the immune system and blood-forming cells, accounting for 8% of all human malignancies. Tumors are further classified by cell type and tissue of origin [11].
Mutations and DNA damage are induced by radiation and chemical carcinogens, which are considered "starting agents" because mutations in critical target genes are the earliest event leading to cancer formation (Figure 1). Carcinogenic chemicals in tobacco smoke, sunlight ultraviolet radiation, and aflatoxin are the primary initiating agents contributing to human cancers. Smoking is responsible for 80 to 90% of lung malignancies and is associated with other body regions [12].
Hormones, especially estrogens, can promote certain human malignancies, such as endometrial cancer and breast cancer. Excessive estrogen exposure increases the risk, while progesterone therapy can mitigate this risk. Prolonged use of estrogen and progesterone combinations can also increase breast cancer risk [13].
1.1. Cancer Statistics for Saudi Arabia
In 2022, Saudi Arabia experienced 13,399 cancer-related fatalities and 28,113 new cancer cases. Breast cancer, colon-rectum cancer (CRC), and thyroid cancer comprise the most prevalent malignancies. Hormonal variations, diet, lifestyle, and obesity were the most frequently reported risk factors associated with breast cancer. 13.3% of all malignancies in the nation are attributed to CRC in 2022. Genetic, environmental, age, gender, and other inflammatory conditions of the digestive tract may all be risk factors for CRC. Thyroid carcinoma is a thyroid disorder that is frequently diagnosed, with a prevalence of 9.3%. Goitre disease, exposure to excessive levels of radiation, and family history are all risk factors for thyroid cancer [14].
In Saudi Arabia, the age-standardized rates (ASR) indicate that the incidence of all malignancies is 87.1, with ASR incidence rates of 81.0 in males and 100.4 in females. The estimated mortality rate was 13,399 cases, regardless of gender or age. The mortality rates of ASR were 48.4 in males and 45.0 in females. Among all Arabian Gulf countries, Saudi Arabia has the second highest cancer mortality rate [15].
In Saudi Arabia, breast cancer ranked first among other cancer types, with a mortality rate of 7.6% and an incidence rate of 25.3% for both genders. The incidence of breast cancer among females was 25.3% in 2022 [16].
Colorectal cancer was the second most prevalent form of cancer in Saudi Arabia, with an incidence of 11.7% and a mortality rate of 6.2% for both genders. Males experienced a 13% incidence rate, while females experienced a 9.8% incidence rate [17].
1.2. Challenges Associated with the Development of Anticancer Drugs
The ideal approach in pharmacotherapy involves medications that precisely target and eliminate malignant cells while minimizing side effects. However, significant differences between normal and cancerous cells, such as variations in signaling pathway activation, hormone or growth factor sensitivity, and growth behaviors, complicate the development of effective cancer treatments. Despite these challenges, advancements in effective medications, interdisciplinary and personalized treatments, and enhanced palliative care services, including targeted therapies and potent chemotherapeutic agents, have contributed to improved patient survival rates [19].
Despite these advancements, numerous treatment failures persist, primarily due to various drug resistance mechanisms. Additionally, the cost of new cancer therapies has significantly risen due to extensive pharmacological research. This financial burden is becoming increasingly difficult for most healthcare systems to sustain, necessitating innovative approaches to repurpose and improve existing medications [19].
The cost of cancer care surged by approximately 19%, 31%, and 28% in 2020 for the initial, ongoing, and final phases of therapy, respectively, compared to 2010 [19]. Another significant challenge in oncologic research is the complexity of cancer, which involves numerous molecular patterns with varying susceptibilities and resistances to different therapies. Therefore, developing more effective cancer treatments is crucial [19].
1.3. Drug Repurposing
Drug repurposing is one strategy under extensive investigation and implementation to tackle this issue [20,21,22,23,24,25]. Drug repurposing is the use of an already-approved medication for a new medical condition or treatment, often leveraging unexpected side effects or unknown therapeutic effects [26,27]. This approach saves time and money in pharmaceutical research by bypassing the traditional drug development pathway and transitioning to preclinical and clinical trials [28]. Traditional drug development is known for its lengthy timelines and high costs, often requiring at least $1 billion and ten years to bring a new medication to the market [29]. Drug repurposing focuses on quickly identifying existing medications that can effectively treat conditions beyond their original intended use, particularly when traditional de novo drug development is impractical or when urgent therapeutic solutions are needed [30]. There are several methods of drug repurposing, including developing approved drugs for new indications, repurposing approved and marketed molecules for off-label use through clinical testing, and rescuing molecules abandoned due to issues like poor efficacy or toxicity [31]. Regulatory bodies like the FDA attribute a substantial proportion of newly approved medications and biologics to drug repurposing [32].
The application of drug repurposing in cancer therapy provides better mitigation options for cancer patients faster and at a lower cost by repositioning non-oncology medications to combat cancer cells. Various techniques were employed to investigate the potential anticancer effects of non-cancerous medications. Numerous in vivo and in vitro studies using cancer cell lines and pharmacological models were conducted to explore the drug repurposing of non-oncology drugs. Several comprehensive electronic databases, including the Molecular Libraries Initiative and the National Institutes of Health (NIH), have been used in the analysis of chemical compounds, biological assays, and the genetic significance of active chemical compounds in the context of drug repurposing.
Repurposing non-oncology drugs could be at any level of the cancer pathophysiological mechanisms, including induction of apoptosis, inhibition of growth signaling and transducers, inhibiting cancer cell metabolism, activation of antitumor immunity, reactivation of growth suppressors, interference with replication, reduction of tumor blood supply, and suppression of invasion and metastasis [33,34,35,36].
2. Drug Repurposing Cases for Cancer Treatment
This section will outline medications that have been repurposed in cancer treatment to the best of our knowledge and report on their current status. A summary is provided in Table 1, Table 2 and Table 3.
2.1. Repurposing with a Multi-Type Anticancer Activity
2.1.1. Repurposing Anti-Platelet Medication for Cancer Treatment
Aspirin, initially used for cardiovascular conditions, has shown anti-tumoral activity and is now being repurposed for treating triple-negative breast cancer. Studies demonstrated that regular aspirin use is associated with a lower risk of breast cancer. Aspirin has been found to inhibit the growth of breast cancer cells with PIK3CA mutations by activating signaling pathways that inhibit mTORC1 and AMPK. Additionally, variations in PIK3CA SNPs have been linked to different outcomes of aspirin therapy in breast cancer patients. As a result, Henry et al. propose that combining PI3K inhibitors with aspirin could be an effective treatment strategy for breast cancer, provided patients are stratified based on their genetic profile concerning the PI3K gene [37].
Aspirin inhibits cyclooxygenases (COXs), which are enzymes involved in the production of prostaglandins and thromboxane, chemical messengers that contribute to pain signaling, blood clotting, and inflammation. By reducing inflammation, aspirin may help prevent cancer development and progression. Additionally, aspirin may enhance anti-tumor immune activity and support other anti-cancer immunotherapies by reducing platelet activity. Studies have shown that aspirin can inhibit various tumor cell activities and disrupt the tumor microenvironment, hindering cancer cell growth and spread [38,39,40,41,42,43].
Low-dose aspirin use has been linked to a reduced risk of various cancers, including gastric, esophageal, colorectal, pancreatic, ovarian, endometrial, breast, and prostate cancers. However, a meta-analysis found no significant difference in cancer incidence or mortality between aspirin users and non-users. Regular low-dose aspirin use has also been associated with improved survival rates, with studies showing a lower 10-year risk of cancer and total mortality compared to non-users. After a cancer diagnosis, low-dose aspirin use has been associated with lower mortality in patients with digestive tract cancers. A meta-analysis of eight studies found a strong correlation between aspirin use and a reduced risk of hepatocellular carcinoma, the most common type of primary liver cancer. Low-dose aspirin use is also associated with a 10% lower risk of developing ovarian cancer. However, the relationship between aspirin uses and survival in ovarian cancer patients has not been thoroughly studied. [44,45].
2.1.2. Repurposing Anti-Diabetic Medication for Cancer Treatment
Several studies have documented the benefits of anti-diabetic medications in cancer management. Anti-diabetic drugs, from various pharmacological classes and different chemical groups including the classic groups, sulfonylureas, thiazolidinediones, biguanides, as well as the recent groups, sodium-glucose co-transporter-2 (SGLT2) inhibitors, and dipeptidyl-peptidase IV inhibitors, are effective in treating certain cancers. The metabolic links between diabetes and cancer, including the direct effects, hyperglycemia, hyperinsulinemia, and the indirect effects, inflammation, oxidative stress, and obesity, are thought to contribute to the anti-cancer effects of these drugs.
Recent studies have demonstrated that anti-diabetic drugs can decrease the occurrence of cancer by directly impacting the metabolism of cancer cells and indirectly by modifying markers associated with the risk of tumor development. Special attention was given to insulin sensitizers including metformin and the thiazolidinedione group due to their impressive results in clinical trials. Metformin is the principal treatment for type 2 diabetes and is widely recognized as the most prominent example. Multiple meta-analyses of case-control, cohort studies, observational, and clinical trials have provided evidence of its efficacy in cancer prevention and treatment, whether used alone or in conjunction with other drug therapies. Metformin substantially lowers the likelihood of developing colorectal, breast, pancreatic, prostate, lung, and cervical malignancies. Research suggests that using biguanides is associated with a 20–30% reduction in the incidence of all cancers and cancer-related deaths [46,47]. Thirty-seven clinical trials have assessed metformin as a stand-alone treatment or in combination with conventional therapy. Its efficacy against colon cancer has progressed to Phase II and III clinical trials when used alone before and during surgery and in combination with conventional therapy. Metformin induces cell cycle arrest in various colon cell lines through specific mechanisms [48,49,50,51]. Metformin is particularly effective in preventing breast cancer, with over seven clinical trials currently evaluating its potential as a breast cancer treatment. It has progressed to Phase III when used alone or in combination with atorvastatin and to Phase II when combined with chemotherapeutic drugs, diet, or fasting. Metformin suppresses cancer stem cells (CSCs) in vitro by down-regulating CSC-specific genes and re-expressing miRNAs. It also decreases pSTAT3 phosphorylation, inhibits the activity of S6 kinase and mTOR, increases AMPK, and reduces mRNA translation in breast cancer. Studies have demonstrated that metformin effectively prevents skin cancer through several mechanisms. For example, metformin inhibits the production of TRB3 (tribbles pseudo kinase 3) in vivo, halting melanoma cells in the G0/G1 phase and reducing melanoma growth and spread. Additionally, metformin activates AMPK, affecting the tumor microenvironment and melanoma cell death and proliferation. In various melanoma cell lines, metformin also reduces cell proliferation and invasion by modulating the miR-192-5p/EFEMP1 and miR-584 3p/SCAMP3 axis [52,53,54].
Both preclinical and clinical research have demonstrated the potential of thiazolidinediones (TZDs) in the treatment of breast and prostate cancer. The primary constituents of this category are troglitazone, rosiglitazone, and pioglitazone. These compounds exert their anti-cancer actions by both PPAR γ (peroxisome-proliferator-activated receptor gamma) dependent and independent pathways. TZDs stimulate the PPAR γ receptor, which then combines with the retinoid X-receptor to create a heterodimer. This interaction results in enhanced apoptosis and differentiation, as well as reduced cell population division. Targeted cytotoxic drugs (TZDs) depend on the expression of PTEN/AMPK, AKT/mTOR, and the breakdown of cyclins D1 and D3, regardless of PPAR γ [55,56].
While there are currently no other anti-diabetic therapies undergoing phase II studies specifically for colon cancer, two pharmacological agents, desmopressin and pioglitazone, have demonstrated effectiveness against colon cancer cells by distinct methods. In vitro and in vivo, desmopressin, a selective agonist for vasopressin receptor 2 (AVPR2), suppresses the growth of colon cancer cells. By decreasing the expression of COX-2 and cyclin D1, pioglitazone, a synthetic PPAR ligand that enhances insulin sensitivity and glycemic management, inhibits metastasis of different colon cancer cells [57,58,59,60].
The mechanism by which pioglitazone induces G0/G1 arrest in MCF7 breast cancer cells, which is partly dependent on PPAR and partly dependent on MAPK, has not been investigated in clinical trials for breast cancer therapy [61,62,63,64].
Two anti-diabetic drugs are now undergoing clinical studies to determine their efficacy in preventing pancreatic cancer. Current Phase II trials are studying the use of pioglitazone in conjunction with conventional medication, while Phase I trials are investigating the use of metformin in combination with digoxin and simvastatin. Administering pioglitazone alone enhances the production of carcinoembryonic antigen mRNA both in laboratory settings and in living organisms. Furthermore, metformin by itself demonstrates encouraging inhibitory actions against several pancreatic cancer cells both in laboratory settings and in living organisms [65,66,67].
2.1.3. Repurposing Anti-Helminthic Medication for Cancer Treatment
Anti-parasitic medications, such as chloroquine, ivermectin, as well as mebendazole, flubendazole, albendazole, have shown potential as anti-cancer agents. These drugs, initially used to treat intestinal parasites, have demonstrated anti-cancer activity by targeting pathways like Wnt/β-catenin, NF-kB, signal transducer, and activator transcription proteins [68,69].
Flubendazole, a well-known benzimidazole, exhibits antineoplastic properties against various cancers, including neuroblastoma, multiple myeloma, leukemia, and breast cancer. It induces apoptosis, generation of reactive oxygen species, and activation of caspase 3 and 7. Flubendazole suppresses the proliferation of tumors and the formation of new blood vessels in lung, liver, and breast cancer by selectively attacking cancer cells, triggering cell death, and augmenting the expression of human epidermal growth factor receptor 2 (HER2) in breast cancer [70,71,72].
By inhibiting the autophagy pathway, signal transducer, and transcription protein 3, flubendazole exerts lethal effects in human colorectal cancer. It also inhibits melanoma cell proliferation and metastasis, leads the accumulation of myeloid-derived suppressor cells and induces programmed cell death protein-1 [73,74].
Benzimidazole-based anthelmintics, have also shown in vitro and in vivo antitumor effects in various cancer models, including pancreatic cancer (PC). Parbendazole, administered at therapeutic plasma concentrations, induces apoptosis, disrupts the cell cycle, and triggers a DNA damage response, inhibiting PC cell growth and clonogenicity. Parbendazole significantly alters microtubule organization in PC cells, leading to rapid polyploid cell formation and aberrant mitotic spindles. The potential of parbendazole is further underscored by its synergistic effect with the standard PC chemotherapeutic drug gemcitabine. Bioinformatic tools identified several unexplored cancer-related targets for benzimidazoles, including the MAP kinase p38 alpha, VEGFR2, and tyrosine-protein kinase ABL, suggesting the need for further in vitro and in vivo studies in PC and other tumor models to validate these findings [57].
Mebendazole (MZ), commonly used to treat intestinal parasite infections, inhibits tubulin polymerization, leading to anti-parasitic effects. As a repositioning drug, mebendazole has shown synergistic effects with temozolomide in treating malignant gliomas, inhibiting tumor growth more effectively than temozolomide alone in both xenograft and syngeneic glioma models. Mebendazole also shows synergistic effects with docetaxel in blocking tubulin polymerization, inducing mitotic arrest in the G2/M phase, increasing apoptosis, and reducing prostate cancer cell proliferation and tumor growth. In vivo and in vitro studies demonstrate that mebendazole halts mitotic progression in the G2/M phase, induces double-strand breaks, and triggers apoptosis in breast cancer [75,76].
Additionally, mebendazole causes apoptosis by activating the caspase-3 pathway and prevents pulmonary metastases in advanced thyroid cancer. It also exhibits cytotoxicity in brain tumors, ovarian, colon, and endocrine cancers. Mebendazole induces apoptosis in cholangiocarcinoma by upregulating caspase 3, preventing cell division. Additional research indicates that mebendazole inhibits the growth of various cancer cell lines, including glioblastoma, medulloblastoma, melanoma, lung cancer, and colorectal cancer, both in vivo and ex vivo. Mebendazole induces apoptotic cell death in melanoma by activating caspases and the pro-apoptotic Bcl-2, while suppressing XIAP, the regulator of the apoptotic pathway [77].
Moreover, mebendazole exhibits high affinity for colon cancer cells, indicating its potential role as a suppressor of Hedgehog signaling in medulloblastoma and as an inhibitor of kinases and oncogenes, such as ABL and BRAF. Mebendazole-treated rats show reduced tumor growth and angiogenesis, with a decreased incidence of metastases. Case studies indicate that therapeutic mebendazole administration can have anticancer effects, with one early study by Mukhopadhyay et al. showing slowed lung cancer cell growth without affecting fibroblasts or normal endothelial cells. Patients with metastatic colorectal cancer received mebendazole after first- and second-line treatments, experiencing minimal side effects and significant reductions in pulmonary and lymphatic metastases, as well as partial hepatic metastasis recovery. Patients with adrenocortical carcinoma receiving mebendazole after unsuccessful chemotherapy had stable disease for about a year and a half, with no side effects and reduced metastases size [78].
Niclosamide, an FDA-approved anthelmintic drug, has been shown to interfere with anaerobic metabolism and glucose absorption in prostate, breast, and ovarian cancer cells. It also acts on increasing the transduction of transcription proteins Wnt/β-catenin and NF-KB, affecting various signaling pathways, including metastasis and signal activation. Niclosamide significantly slows the growth of colon, liver, and breast cancers and prevents colorectal cancer cells from metastasizing to the liver and breast cancer metastases to the lungs. However, its clinical development is hindered by poor solubility and lower bioavailability, which might be addressed by intravenous administration [79,80].
2.1.4. Repurposing Anti-Viral Medication for Cancer Treatment
Recognized for their anticancer properties, antiretroviral therapies (ARTs) can induce cell edema, apoptosis, and altered membrane permeability, leading to cell death. ARTs trigger apoptosis, inhibit angiogenesis, and enhance the effectiveness of chemotherapy or radiation by producing toxic free radicals through a ferrous iron-mediated reaction. Reactive oxygen species (ROS) generated by ARTs cause oxidative DNA damage and apoptosis, making cancer cells more vulnerable due to their lack of antioxidant enzymes. ARTs, particularly dihydroartemisinin, increase ROS before cytotoxic effects occur, indicating ROS as a primary cause of cell damage. ARTs target iron-rich cancer cells, enhancing their efficacy against tumor cells with high transferrin receptor (TfR) expression. Studies show that ARTs combined with amino acetic ferrous sulfate increase ART susceptibility in cancer cells, while deferoxamine mesylate pretreatment counteracts dihydroartemisinin-induced apoptosis in leukemia cells [83].
Protease inhibitors used in antiretroviral therapy, such as ritonavir, target HIV and have shown anticancer effects in ovarian, pancreatic, and breast cancers by triggering apoptosis and inhibiting cancer cell growth. Ritonavir acts synergistically with other drugs, including temozolomide in glioma cancer cells and bortezomib in kidney carcinoma. Ritonavir has demonstrated efficacy in treating lymphocytic leukemia and inhibits Akt phosphorylation in breast cancer cells [84,85,86].
Ribavirin is a guanosine ribonucleoside-based antiviral drug, competes with guanylyl transferase and inhibits 5’-mRNA, reducing cyclins D1 protein levels and inhibiting oncogene transformation. Ribavirin also induces VEGF mRNA translation, suppressing human lymphocyte progression. Cidofovir, another FDA-approved antiviral drug, inhibits viral DNA polymerase and treats various viral infections by blocking diphosphate metabolites. It activates caspase and PARP in epithelial cells, promoting apoptosis and mitotic arrest. Cidofovir inhibits DNA synthesis and cancer cell proliferation in glioblastoma cell lines. Both in vitro and xenograft models show cidofovir’s anti-proliferative properties, suppressing apoptosis-related genes in glioblastomas [87].
2.1.5. Repurposing Cardiovascular Medications for Cancer Treatment
FDA-approved cardiovascular drugs have shown potential anticancer properties in various studies.
- Anti-Hypertension Medication
Losartan, an angiotensin receptor blocker (ARB), normalizes the tumor microenvironment by depleting the matrix and reducing collagen I levels, inhibiting tumor growth and cell proliferation. Losartan has shown promise in phase II clinical trials for treating pancreatic cancer. Similar mechanisms are employed by other ARBs like irbesartan, valsartan, telmisartan, and olmesartan. Captopril inhibits colorectal liver metastases by reducing tumor viability and hindering metastasis formation. Carvedilol has been found to inhibit breast cancer cell invasion and metastasis by interfering with growth factor receptors and mitochondrial function [88,89,90].
Propranolol, the first effective beta-blocker, is used to treat cardiac illness, hypertension, and conditions like infantile hemangiomas. Cumulative studies have shown that beta-blockers, including propranolol, possess anti-proliferative properties and can inhibit the spread of various cancers, such as ovarian, colorectal, lung, and prostate cancer. Better clinical outcomes in multiple myeloma have also been observed. One hypothesis is that beta-blockers inhibit the sympathetic nervous system in the bone marrow niche, thereby enhancing the clinical outcomes for patients with multiple myeloma, especially those undergoing hematopoietic stem cell transplantation. Clinical trials indicate that propranolol, combined with hematopoietic stem cell transplantation, can be used to treat multiple myeloma, despite some adverse events like dizziness, hypotension, and hypokalemia [91,92].
Research suggests that COX-2 inhibitors and beta-blockers together may slow disease progression in some cancer types. COX-2 inhibitors have anti-angiogenic and apoptotic effects, and some cancers, like renal cell carcinoma, release prostaglandins to evade eradication. Preoperative beta-blockers combined with COX-2 inhibitors may enhance immunological response and reduce metastasis. Propranolol and etodolac-treated patients with primary operable breast cancer showed increased tumor-infiltrating β-cells, decreased tumor-infiltrating monocytes, and reduced premetastatic/pro-inflammatory transcription factor activity. Nausea was the most frequent adverse event, with no moderate or severe ones reported [93,94,95].
Preclinical studies have demonstrated that certain antihypertensive drugs augment tumor susceptibility to chemotherapy, decrease cell proliferation, and function as co-adjuvants against chemo-resistant cell lines in different types of cancer. Evidence from a retrospective study suggests that the use of propranolol for a duration over 1000 days reduces the likelihood of acquiring malignancies in the prostate, colon, stomach, and esophagus. Additional evidence indicates that statins, ACE inhibitors, and ARBs decrease the likelihood of breast cancer recurring. Combined administration of sunitinib with ARBs and ACE inhibitors enhances overall survival, response rate, progression-free survival, and decreases initial treatment relapse in patients with renal cell carcinoma [96,97,98].
Candesartan and irbesartan (ARBs) are inhibitors of angiogenesis and tumor vascularization in colon cancer cell lines. Furthermore, irbesartan inhibits the JUN gene and AP-1 DNA binding in a patient with metastatic colon cancer, resulting in a total elimination in radiological testing. The efficacy of ACE inhibitors such as captopril and enalapril in inhibiting the conversion of angiotensin I to angiotensin II has been demonstrated against colon cancer cells both in vitro and in vivo. Enalapril alone decreases the expression of IGF-IR 1, when coupled with 5-fluorouracil, and it enhances radiosensitivity via activating the NF-κB/STAT3 pathway. While enalapril is not now undergoing clinical studies, the existing data indicates its promise as a modified immunotherapy for cancer. The ca channel blocker, nifedipine, solely and selectively suppresses the expression of PDL-1 in colon cancer cell lines [99,100,101].
Eighteen clinical trials have assessed propranolol, a non-selective beta-blocker, alone or with other therapies against various cancers, including pancreatic, neuroblastoma, angiosarcoma, breast, lung, melanoma, and leukemia. Propranolol in combination with etodolac is currently undergoing Phase II and III trials for the treatment of colorectal cancer. In vivo, propranolol reduces the expression of p-AKT/p-ERK/p-MEK and stimulates autologous CD8+ T cells thereby suppressing colorectal cancer. Two Phase I trials are currently being conducted to evaluate the effects of propranolol on ovarian cancer. Its mechanism of action involves activating protective autophagy and apoptosis through the JNK signaling pathway and ROS [102,103].
Two antihypertensive medications are in Phase II trials for prostate cancer: carvedilol, and propranolol. Carvedilol is assessed before surgery, while propranolol is examined preoperatively alone or with etodolac. A retrospective study shows that long-term atenolol use significantly reduces prostate cancer risk by over 50% [104,105].
In vitro and in vivo studies show that captopril and candesartan inhibit prostate cancer cells, despite not undergoing clinical trials. Captopril increases p53 expression, inducing apoptosis in prostate cancer cells, while candesartan reduces tumor growth and angiogenesis by inhibiting VEGF expression. Hydralazine induces demethylation in prostate cancer cells, re-expressing suppressed genes [106,107].
A Phase II trial is currently underway to evaluate minoxidil, a direct vasodilator antihypertensive medication, as a single treatment for ovarian cancer. Activating a caspase-3 independent cell death pathway, it induces mitochondrial disruption and substantial DNA damage, hence modifying the metabolic and oxidative state of cancer cells [108,109].
The activation of a caspase-3 independent cell death pathway by minoxidil results in mitochondrial disruption, substantial DNA damage, and alterations in the metabolic and oxidative state of cancer cells [110].
Although there are no clinical trials specifically assessing their efficacy, four anti-hypertensive drugs including captopril, telmisartan, irbesartan, and candesartan have demonstrated promise in combating liver and kidney cancer in both in vitro and in vivo studies. Telmisartan and irbesartan inhibit the proliferation of liver cancer cells by downregulating the expression of pErbB3 and phosphorylating p38/MAPK, therefore lowering the expression of VCAM-1 downstream [111].
Telmisartan triggers apoptosis in kidney or renal cancer cell lines by increasing the expression of caspase-3 and Bax, while decreasing the expression of Bcl-2 (PI3/AKT pathway). Furthermore, captopril suppresses the proliferation of SN12K-1 kidney cancer cells in laboratory and animal models [112].
Tezosentan has been demonstrated to possess the potential to serve as a novel anticancer agent by inhibiting endothelin receptors, which are overexpressed in a variety of cancer cells.
Furthermore, tezosentan has demonstrated promising preclinical results in the inhibition of cancer cell proliferation and the induction of apoptosis, particularly in malignancies with the highest expression of endothelin receptor type A [113,114].
- Antihyperlipidemic
Fenofibrate, initially developed for treating hyperlipidemia, has shown anticancer properties in various human cancer types. Fenofibrate activates AMPK, reduces ATP levels, and increases ROS accumulation, leading to apoptosis and inhibition of metastasis in cancer cells. Fenofibrate also promotes apoptosis and cell cycle arrest by modulating growth factor receptors and NF-κB activity, in breast cancer and also inhibiting ERK signaling in lung cancer. Fenofibrate’s anticancer effects are independent of PPARα, making it a potential candidate for repurposing in cancer treatment [115,116].
- Repurposing Ion Channels modulators for Cancer Treatment
Ion channels play a critical role in specific excitable cells like cardiac myocytes and neurons. The study of ion channels’ roles in the pathophysiology of various diseases has led to the development of drugs targeting these channels. Groundbreaking research highlighting the role of K+ channels in mitogenesis and oncogenesis spurred interest in their potential as targets for cancer treatment. Consequently, ion channels are now considered potential therapeutic targets, as they influence cancer cell growth through various mechanisms, including regulating membrane potential and critical survival signaling pathways like Ca2+ and Na+/K+ [117,118,119].
During different stages of the cell cycle, cancer cells experience volume changes, controlled primarily by ions such as potassium, calcium, sodium, and chloride. Cancer cells use water flow in restricted areas to propel themselves during migration, with aquaporin channels facilitating water passage between cells. According to the "osmotic engine model," AQP5 (aquaporin 5) and NHE-1 (Na+/H+ exchanger-1) are polarized at the cell’s leading edge during migration, allowing water to enter at the front and exit at the rear, resulting in cell displacement [120,121].
With 77 genes encoding K+ channels, they are highly diverse, and any member of this large family can be dysregulated in a particular cancer type. Among these, Kv10.1 (EAG1) channels have been extensively studied and are often up regulated in cancer cells. Therefore, specific blockers for these various K+ channels are required for optimal function, opening the possibility of tailored medication. Identifying the dysregulated K+ channel in a patient allows for treatment with a specific inhibitor of that K+ channel family member. For example, Kv10.1 is expressed in about 70% of cancers but is almost absent from non-CNS organs, making it less harmful to target these channels in tumors than in normal tissues [122,123].
Although Kv10.1 is virtually absent in healthy non-CNS tissues, it is significantly upregulated in several cancer cell lines such as neuroblastoma, cervical carcinoma, melanoma, and breast cancer. An overexpression of Kv11.1 (hERG) is observed in human leukemia cell lines. Kv10.1 channels are notably upregulated in patient tumor tissues, such as soft tissue sarcoma (70%), cervical cancer (100%), gliomas (Kv10.1 and Kv11.1), endometrial cancer (Kv11.1), and chronic lymphocytic leukemia (Kv11.1), as compared to non-cancerous cells. After conducting an extensive analysis of more than 470 clinical tumor samples, it was determined that Kv10.1 was over-expressed in 15 out of 17 different carcinoma types [124,125].
Preclinical research on potassium channel inhibition’s anticancer effects primarily focuses on Kv10.1, Kv10.2 (EAG2), and Kv11.1 channels. Existing drugs, like the anti-arrhythmic verapamil, anti-epileptic retigabine, and anti-diabetic sulfonylureas, are known for their inhibitory effects on potassium channels such as KATP, Kv11.1, and KCNQ, respectively.
Sulfonylurea medications, like glipalamide, have shown efficacy against melanoma, lung, stomach, and breast cancers. Verapamil, an anti-arrhythmic, is effective against neuroblastoma and prostate cancer. Its combination inhibitory action against potassium and calcium channels contributes to its anticancer effects. Astemizole, originally developed as an H1-antagonist, now shows potential as an anticancer medication due to its ability to inhibit Kv10.1. Current research suggests that potassium channel blockers could be repurposed as anticancer drugs [126,127].
Calcium channel blockers (CCBs) of the T-type can halt the cell cycle in the G1 or S phases, and increases it’s susceptibility to chemotherapy. Combining CCBs with existing drugs enhances their effectiveness. Additionally, CCBs block p-glycoproteins, which contribute to cancer cells’ multi-drug resistance [111,128,129].
Mibefradil, a T- and L-type Ca2+ channel blocker, was initially marketed as an antihypertensive medication but was withdrawn due to interactions with other drugs. Modifications to mibefradil, such as those by Bui et al., could create more selective T-type Ca2+ channel blockers with less CYP450 3A4 inhibition, potentially improving their use in cancer therapy. TAU Therapeutics LLC has repositioned mibefradil for the treatment of high-grade glioma tumors using Interlaced Therapy TM, combining it with temozolomide to enhance the chemotherapy drug’s efficacy in S-phase active cells. This approach is currently undergoing Phase 1b clinical trials to validate its effectiveness [130,131].
2.1.6. Repurposing Antibiotic Medications for Cancer Treatment
Antibiotics are being researched for their potential to target cancer cells in addition to treating bacterial infections. Some antibiotics, including anti-TB medications, tetracyclines, and β-lactam antibiotics, show antitumor activity. Bedaquiline, an antibiotic approved by the FDA for treating pulmonary tuberculosis, has been shown to suppress the development and multiplication of MCF7-derived stem-like cancer cells, as well as reduce mitochondrial oxygen consumption. The promise of bedaquiline as a cancer chemotherapeutic option arises from its ability to target mitochondrial ATP-synthase, which may result in m-ATP depletion and mitochondrial malfunction in cancer cells. However, further research is required to confirm this hypothesis [132,133,134].
Tetracyclines, such as tigecycline and doxycycline, can impede the spread of cancer by specifically targeting the system of oxidative mitochondrial metabolism. By targeting pathways such as AMPK-mediated mTOR, WNT/b-catenin, and PI3K/AKT, they elicit oxidative stress, autophagy, cell cycle arrest, and eventually apoptosis in cancer cells, so suppressing cell proliferation, migration, invasion, and angiogenesis [84,135,136].
Clofoctol, a medical agent employed in France and Italy for the treatment of upper respiratory tract infections, has the ability to inhibit protein translation in mammalian cells, therefore indicating its potential utility in the field of cancer therapy. Clofoctol promotes endoplasmic reticulum (ER) stress via activating the unfolded protein response (UPR) pathway, resulting in G1 phase cell cycle arrest in cancer cells. Given that many cancer cells exhibit elevated levels of ER stress, additional augmentation of ER stress may elicit exaggerated stress responses, leading to cell cycle arrest or cell death. [137,138].
Anthracyclines (AC), such as doxorubicin, daunorubicin, epirubicin, and idarubicin, intercalate between DNA base pairs, forming a ternary complex with DNA and Topoisomerase II that inhibits DNA and RNA synthesis in actively reproducing cancer cells. Doxorubicin-containing chemotherapy regimens, including FAC (5-fluorouracil, AC), TAC (taxotere, AC), and AC (adriamycin, cyclophosphamide), have been effective in treating breast cancer. Myocet, a non-PEGylated liposomal form of doxorubicin, is licensed for metastatic breast cancer treatment in Europe and Canada when used with cyclophosphamide [139,140,141].
The broad-spectrum tetracycline antibiotic minocycline has demonstrated effectiveness in the treatment of several forms of cancer. Cell cycle arrest and down-regulation of cyclins A, B, and E are mechanisms by which it inhibits the proliferation of ovarian cancer cells. The concurrent administration of minocycline and celecoxib in breast cancer causes a decrease in tumor cell proliferation, microvessel density, and the synthesis of matrix metalloproteinase and VEGF. Autophagy activation is the mechanism by which minocycline suppresses glioma cell proliferation. Ongoing clinical trials are evaluating its capacity to enhance the outcomes of cancer patients by mitigating the adverse effects of chemotherapy [142,143].
The broad-spectrum tetracycline antibiotic tigecycline is effective against multi-resistant bacteria and has anticancer properties, including inhibition of gliomas, myeloid leukemia, non-small cell lung cancer, and retinoblastoma transcriptional corepressor 1 negative breast cancer. Current Phase I trials are investigating the use of Tigecycline for the treatment of acute myeloid leukemia [136,144,145].
Fluoroquinolones, including ciprofloxacin, moxifloxacin, levofloxacin, enoxacin, and fleroxacin, disrupt DNA synthesis by inhibiting bacterial gyrase and exhibiting strong anti-cancer properties. Ciprofloxacin, for example, has been shown to inhibit leukemia, osteoblastoma, osteosarcoma, colon, bladder, and prostate cancers. Enoxacin modulates miRNA production specifically in cancer, highlighting the potential of fluoroquinolones as anti-cancer medications [146,147].
2.1.7. Repurposing Anti-Malarial Medications for Cancer Treatment
Chloroquine, artesunate, and mefloquine, originally developed to treat malaria, have shown efficacy against various diseases, including cancer. Chloroquine suppresses autophagy, slows tumor development in glioblastoma xenografts, and enhances the overall outcome when used with chemotherapy drugs. Artesunate induces ROS production and apoptosis in T-cell leukemia and slows tumor growth and angiogenesis in Kaposi’s sarcoma [148].
2.1.8. Repurposing Anti-Psychotic Medications for Cancer Treatment
Anti-psychotic medications have been shown to possess anti-cancer properties, affecting biochemical pathways that result in tumor cell death. Haloperidol and penfluridol, hydroxypiperidine-based antipsychotics, inhibit DRD2 activity, promoting ER stress and suppressing pancreatic cancer cell proliferation with minimal toxicity. Penfluridol stimulates autophagy and death in malignant pancreatic cells and has synergistic effects when combined with gemcitabine. Penfluridol specifically affects the JAK2 binding site in PRLR, therefore blocking the JAK2–STAT3 and ERK/AKT signaling pathways. This action effectively inhibits the proliferation of pancreatic cancer cells. [151,152,153].
2.1.9. Repurposing NSAID Medications for Cancer Treatment
Chronic inflammation is linked to cancer risk, with inflammatory mediators like growth factors, chemokines, and cytokines facilitating cancer cell survival and proliferation. NSAIDs, such as mesalazine, sulindac, piroxicam, and ibuprofen, have shown potential in reducing tumor growth and cancer recurrence. Diclofenac has been found to slow pancreatic tumor growth, while the selective COX-2 inhibitor, celecoxib, inhibits breast cancer cell proliferation and tumor formation. The correlation between NSAID usage and slower cancer development suggests potential repurposing opportunities [154,155].
2.1.10. Repurposing Disease-Modifying Antirheumatic Drug (DMARD) for Cancer Treatment
Auranofin, a disease-modifying antirheumatic drug (DMARD), was once used to treat rheumatoid arthritis by suppressing inflammation and stimulating cell-mediated immunity. However, it was found to be less effective than other DMARDs, such as methotrexate, and its use declined due to its adverse effects, including gastrointestinal complaints, skin irritations, and oral ulcerations. However, it has potential for novel applications in treating certain malignancies. Auranofin is effective against cancer cells through two mechanisms: inhibiting mammalian TrxR (mTrxR) and targeting the UPS system (Understanding the Unstable Cells) system. These mechanisms induce apoptosis, indicating that auranofin may no longer be the preferred medication for rheumatoid arthritis [156,157].
2.1.11. Repurposing Anti-Epileptic Medications for Cancer Treatment
Oxcarbazepine is a commonly used pharmaceutical agent specifically designed to treat epilepsy. Numerous preclinical studies have provided evidence of anticancer capabilities. One study has shown that oxcarbazepine results in cell cycle arrest specifically during mitosis. Additional studies suggest that it works as an inhibitor of HDAC, therefore suppressing the subsequent PI3K-Akt-mTOR pathway. The ultimate result of this inhibition is the prevention of cell growth and migration. Ultimately, this suppression hinders the manifestation of mTOR and the proteins Bax and Bcl-2, so facilitating the expression of caspase-3 and caspase9, leading to apoptosis and autophagy [158,159].
The compound lacosamide belongs to the third generation of antiepileptic drugs, which improve the delayed deactivation of voltage-gated Na+ channels. It is used as an adjunctive treatment as it has the capacity to reduce seizure frequency without substantially affecting mood [160]. Lacosamide was found to also inhibits HDAC during processing. This activity may indicate the need to undertake an investigation into the anticancer properties. Moreover, this process has been suggested as a possible rationale for the inhibition of cell cycle migration in glioma cells, which may be triggered by the increase in miR-195-5p levels [161]. The same research proposed that lacosamide might dampen cellular proliferation, impede cell migration and invasions, and stimulate apoptotic processes via altering the production of other microRNAs, such miR-107. A study team presented evidence indicating that the phosphorylation of collapsin-response-mediator-protein (CRMP2) is a strong indicator of glioblastoma cell proliferation [160,161].
In order to examine the impact of CRMP2 phosphorylation at S522 on tumor growth, the researchers utilized the CRMP2 phosphorylation inhibitor (S)-lacosamide. Inhibiting CRMP2 phosphorylation with (S)-lacosamide was shown to decrease the proliferation of glioblastoma cells in all glioblastoma cell lines. Furthermore, they provide evidence that (S)-lacosamide suppresses the growth of glioblastoma in live animal models [162,163].
Lamotrigine is another antiepileptic medication that inhibits salt transport. Aside from primarily blocking voltage-gated Na+ channels, it also inhibits N-, L-, and P-type Calcium channels and, to a lesser degree, 5-HT3 receptors. Through the reduction of glutamate synthesis, these effects enhance the stability of neuronal membranes. Similar to lacosamide, lamotrigine is a potential adjunctive drug for patients diagnosed with brain tumors. Published research suggests that pairing it with valproic acid can enhance the treatment of refractory epilepsies by leveraging synergy [164,165].
2.1.12. Repurposing Anesthetic Medications for Cancer Treatment
Ketamine is primarily used in the induction and maintenance of anesthesia due to its antagonistic action on the N-methyl-D-aspartate (NMDA) receptor. It produces a dissociative anesthesia described as a trance-like state, and it can also cause amnesia and alleviate pain. Therefore, ketamine is recommended to cancer patients in order to minimize pain. Furthermore, initial investigations have shown that the introduction of ketamine to specific cells leads to the cessation of the cell cycle and the suppression of cell division, therefore suggesting a possible future use of ketamine in the prevention of cancer advancement. Zhou et al. have shown that the administration of ketamine promotes apoptosis in lung cancer cells by increasing the expression of CD69, a marker associated with the activation of leukocytes and natural killer (NK) cells. Ketamine exerts its anti-cancer properties in ovarian cancer by specifically reducing the expression of RNA PVT1. Moreover, ketamine therapy decreased the interaction between PVT1 and histone methyltransferase enhancer of zeste homolog 2. The aforementioned relationship leads to the increase in expression of P57, a cell cycle inhibitor that subsequently hinders the advancement of the cell cycle in malignant cells. In breast cancer cells and hepatocellular carcinomas, the administration of ketamine can inhibit cell growth and trigger ferroptosis, as well as apoptosis, by specifically inhibiting glutathione peroxidase 4 [57].
Propofol is a rapid, effective intravenous anesthetic with analgesic, hypnotic, and sedative properties. It elicits the central inhibitory neurotransmitter response by activating central GABA receptors, similar to barbiturates and benzodiazepines. Propofol has been found to have anti-inflammatory properties and may enhance the immunological response in older individuals. Studies show that propofol can reduce the cytotoxic activity of NK cells in individuals with gastrointestinal conditions, while increasing their efficacy in patients with propofol anesthesia. Propofol has also been studied for its anti-proliferation effects in various cancer cells, suppressing cell replication and stimulating caspase and MAPK pathways. It can induce apoptosis in oral squamous cell cancer resistant to 5-fluorouracil and reverse the resistance of OSCC to 5-fluorouniprolactone [166,167].
2.2. Repurposing with Type-Specific Anticancer Activity
2.2.1. Repurposing Medications for Prostate Cancer (PC) Treatment
- Anti-Dyslipidemic Drugs
Prostate cancer (PC) severity is linked to circulating androgen levels, primarily derived from cholesterol. PC cells rely on endogenous cholesterol production, making patients with high serum cholesterol levels more susceptible to PC. Statins, which inhibit HMG-CoA reductase, block cholesterol synthesis and androgen production, enhancing prognosis, reducing tumor volume, and decreasing PSA levels. Statins like atorvastatin, have shown potential in PC treatment, either as monotherapy or in combination [168,169].
- Antiarrhythmic Drugs
The sodium-potassium pump is inhibited by cardiac glycosides, including digoxin and ouabain, resulting in intracellular calcium buildup and death of PC cells. Furthermore, these medications stimulate cell cycle arrest and autophagy. Digoxin suppresses the activity of topoisomerase II and lowers the levels of PSA in the blood, while ouabain increases the susceptibility of PC cells to apoptosis by blocking the production of survivin and STAT3. Ouabain also demonstrates anticancer cytotoxicity in castration-resistant PC [170,171].
- Anti-Inflammatory Drugs
Indomethacin, a non-selective COX inhibitor, inhibits angiogenesis and cancer cell growth through various pathways. Diclofenac inhibits COX, prostaglandin synthesis, and MYC gene family expression, disrupting glucose metabolism in PC cells. Aspirin inhibits COX, prostaglandins, and NF-κB, making it a potential candidate for PC treatment, especially when combined with statins [172].
- Antidepressant Drugs
Sertraline, a selective serotonin reuptake inhibitor, reduces PC cell proliferation and induces apoptosis through mitochondrial dysfunction and ROS production. Sertraline also inhibits tumorigenesis, angiogenesis, and metastasis, disrupting PC stem cells’ viability by modulating iron homeostasis. Stress mitigation is crucial for successful cancer treatment, and sertraline has shown potential in reducing PC cell viability, inhibiting cell proliferation, and enhancing autophagy [173].
- Beta-Blockers
Beta-blockers are cardioprotective medications with potential anticancer properties. They inhibit β-adrenergic receptors involved in carcinogenesis, angiogenesis, and tumor metastasis. Beta-blockers have shown promising results in reducing cancer cell proliferation, migration, and tumor growth, particularly in neuroendocrine prostate cancer (NEPCA). Propranolol disrupts the CREB1-EZH2-TSP1 pathway, down-regulating NE markers and promoting xenograft development from NEPCA cells [174].
- Miscellaneous
Heparin, an anticoagulant, has shown potential as an anti-inflammatory and antimetastatic agent in cancer treatment. It inhibits cytokine, adhesion molecule, and angiogenic factor expression, disrupting the tumor-mediated coagulation cascade. Low molecular weight heparin (LMWH) exhibits antiangiogenic and antimetastatic effects, significantly reducing metastases in a murine CRPCA model [175].
The bisphosphonate medication zoledronic acid blocks bone resorption by suppressing osteoclast activity. Therefore, it is employed in the management of osteoporosis. The therapeutic application of this repurposed medication in the management of prostate cancer has received approval. Corey and colleagues showed the anti-PC properties of zoledronic acid in vitro is by causing G1 arrest, deceleration of cell proliferation, and death, and in vivo by reducing the ability to metastasize. Zinc azithromycin effectively decreases skeletal-related problems in PC patients with bone metastases, while it suppresses the growth of osteoblastic and osteolytic metastases in PC. Celecoxib, a COX-2 inhibitor, in combination with zametaxel did not improve survival rates in advanced PC patients. However, docetaxel and zaetaxel significantly improved prognosis in PC patients. Mifepristone, a potent anti-progesterone, has shown anti-cancer properties in androgen-sensitive and androgen-insensitive PC. It inhibits tumor proliferation by suppressing over-expressed cell surface receptors in CRPC cells. Rapamycin, an anti-restenosis medication and immunosuppressant for kidney transplantation, has been repurposed for cancer treatment by binding to the FRB domain of mTOR, inhibiting mTORC1 [176,177].
2.2.2. Repurposed Medications in the Treatment of Gastric Cancer (GC)
- Antidepressant
Fluoxetine is a selective serotonin reuptake inhibitor (SSRI) used to treat depression, anxiety, and post-traumatic stress disorder. It has shown anticancer potential in cancer cells, causing apoptosis and cell cycle disruption. Fluoxetine suppresses cell proliferation in AGS GC cells and induces apoptosis, which is partially suppressed by the inhibition of the endoplasmic reticulum stress marker (CHOP). It also enhances apoptosis and autophagosome formation in AGS cells.
Sertraline, an SSRI, has shown antitumor activity in lung, prostate, breast, melanoma, and acute myeloid leukemia. It induces apoptosis and cell cycle arrest in resistant GC cells, leading to growth advantage, resistance to therapy, angiogenesis, and metastatic potential. Sertraline and its derivatives can be repurposed as chemosensitizers for drug-resistant GC.
Paroxetine, an SSRI, also has anticancer properties by inducing apoptosis and suppressing cancer cell proliferation in colon, hepatocellular carcinoma, osteosarcoma, and lymphoma. Its cytotoxicity in AGS cells is facilitated by enhanced DNA damage and reduced DNA repair. However, it is incapable of inducing apoptosis or DNA damage in MKN-45 cells. Combining paroxetine with chemotherapy or anticancer agents can enhance GC treatment [178].
- Antiepileptic
Valproic acid (VPA) is a fatty acid with antiseizure properties and has been shown to possess anticancer properties in various cancers. VPA induces apoptosis and suppresses cell proliferation in AGS GC cells, inhibiting the HDAC1/PTEN/Akt signaling pathway, which influences cell proliferation, differentiation, and immunity. It also enhances Beclin1 expression, a tumor suppressor, and inhibits Bcl-2 expression. However, high HDAC1 and reduced PTEN expression in MKN-74 GC cells render them resistant to VPA treatment. In vivo, VPA inhibits GC cell growth through apoptosis and autophagy, and increases the expression of survivin, a protein essential for cell division. In a separate study, VPA exhibited an elevated apoptotic index and decreased tumor volume. However, a randomized phase II trial showed that VPA does not provide a survival advantage compared to paclitaxel alone in second- or third-line therapy for advanced GC [178,179].
- Antipsychotic
Thioridazine and risperidone are antipsychotic compounds that are employed in the treatment of acute mania, bipolar disorder, and schizophrenia in the psychiatric field. In glioblastoma, lung, and colon malignancies, thioridazine demonstrates antitumor properties. Thioridazine induces apoptosis in a caspase-dependent manner and inhibits colony formation capacity and nuclear fragmentation in NCI-N87 and AGS GC cells, thereby exerting cytotoxic effects in a fashion that reduces the quantity of caspase-9, caspase-8, and caspase-3 precursors. This medication has the capacity to inhibit the growth of tumors in vivo. Risperidone prevents the proliferation of KATO-III GC cells by increasing the level of ROS and inducing apoptosis.
Additionally, this medication inhibits the growth of tumors in vivo. In a population-based cohort study, the anticancer effects of risperidone were demonstrated. Patients who used risperidone had a lower risk of GC compared to those who did not [180,181].
- Agents that chelate iron
Deferasirox, a tridentate iron chelator, has been shown to have antitumor activity in various malignancies, including pancreatic and breast cancers, mantle cell lymphoma, and lymphoma. It suppresses the proliferation of AGS, MKN-28, SNU-484, and SNU-638 GC cells, induces apoptosis, and upregulates N-myc downstream regulated gene 1, inhibiting metastasis. It also downregulates phospho-mTOR and c-myc expression, suggesting that deferasirox may enhance the antitumor effect of cisplatin in GC [178,182].
2.2.3. Repurposed Medications in the Treatment of Blood Malignancies
Thalidomide was developed in the 1950s originally as a sedative and was used to alleviate morning sickness in pregnant women. Following its introduction, Thalidomide was withdrawn from the market because of its capacity to cause serious congenital abnormalities. An estimated minimum of 10,000 newborns were born with limb and other body extremity abnormalities in more than 46 countries throughout this timeframe. Over the following decades, scientists, persistently explored the medicinal applications of thalidomide [183,184].
Judah Folkman’s laboratory provided evidence that thalidomide significantly decreased the formation of new blood vessels. After careful evaluation in patients with refractory multiple myeloma, the medication demonstrated the ability to produce long-lasting effects by blocking TNF-α. Thalidomide was granted FDA approval in 2006 as a therapeutic option for multiple myeloma when administered in combination with dexamethasone [185,186].
It is rather typical for cancer treatment drugs to be repurposed within the same disease subtype for which they were originally indicated. For example, imatinib mesylate, was originally approved for the treatment of chronic myelogenous leukemia. Nevertheless, imatinib displayed cross-reactivity with and the ability to suppress KIT kinase, since it acts as an inhibitor of the ABL kinase. The identification of mutations that activate the KIT tyrosine kinase as a genetic factor contributing to gastrointestinal stromal tumors (GISTs) suggests that imatinib should be evaluated for its effectiveness in treating GISTs. The notion of the possible indication was examined by preclinical analyses, which confirmed that imatinib indeed caused cell death in GIST cells. This phenomenon was theoretically linked to the suppression of KIT kinase. The therapeutic use of imatinib for GISTs was approved based on these studies [187]. The current indication for imatinib is the treatment of certain blood malignancies, such as acute lymphoblastic leukemia, chronic eosinophilic leukemia, and myelodysplastic/myeloproliferative neoplasms. Furthermore, it has received approval for the management of systemic macrocytosis and dermatofibrosarcoma due to an allergic response [187,188].
Dasatinib, originally approved for chronic myeloid leukemia, was subsequently adapted for the treatment of individuals with Philadelphia chromosome-positive acute lymphoblastic leukemia who had shown resistance or intolerance to previous pharmaceutical treatments, akin to Imatinib. Dasatinib, is an orally administered inhibitor of tyrosine kinase that is actively being studied in clinical studies for the therapy of glioblastoma. Furthermore, it has been used for the therapy of brain metastases caused by breast cancer using network-based techniques, which utilize the reconstruction of disease-specific networks to pinpoint important targets [189,190].
2.2.4. Repurposed Medications in the Treatment of Breast Cancer
Fluorouracil (5-FU) is a heterocyclic aromatic molecule that has a ribinoid structure similar to the pyridine ring present in DNA and RNA. More precisely, the Uracil homologue substitutes hydrogen with fluorine at position C-5. Therapeutic use of 5-FU for cerebral palsy patients has been authorized by the US-FDA. Basal cell carcinoma is commonly treated with 5-FU.
There are several recognized methods by which it exerts its anti-cancer effects, including the stimulation of apoptosis and the suppression of cancer growth (e.g., the Ras/ERK pathway). The compound 5-FU exhibited apoptotic effects and reduced the expression of the H-ras gene in in-vitro studies using the MDA-MB-231 and Tumor2 cell lines [191].
Moreover, the Ras/ERK pathway is suppressed from eliciting antiproliferative actions. Furthermore, 5-FU reduces the expression of the Rho-A gene, therefore reducing apoptosis and metastasis. 5-FU markedly reduced the expression of Rac1 protein in Tumor2 and MDA-MB-231 cells, which plays a crucial role in cell movement, invasion, and resistance to cell death. 5-FU downregulated the expression of the p53 gene in Tumor2. The activation of NF-κB is commonly detected in breast cancer cells. An investigation found that the proliferation and survival of cancer cells, as well as the expression of the NF-κB gene, were decreased following treatment with 5-FU. A research investigation found that 5-FU decreased protein expression in the tumor2 cell line compared to its equivalents. Multiple results corroborate the notion that NF-κB activation decreases medication resistance to 5-FU in human cancer cell lines. This confers a clear superiority over the presently accessible medications, which are at the pinnacle of drug resistance. Additional studies provide further evidence supporting previous studies, demonstrating that the therapeutic effectiveness of 5-FU has been enhanced as a result of decreased NF-κB expression. The combination of (5-FU) with other treatments enhances the probability of a significant response in the setting of drug-resistant cancers [192].
Nitroxoline (NTX) is an antibiotic that is extensively used in Asian, European, and African countries for the effective treatment of urinary tract infections. It is chemically known as 5-nitro-8-hydroxy-quinoline. Nitroxoline is currently experiencing significant popularity due to its potent anticancer properties. The anti-angiogenic activity of nitroxoline was the first anticancer activity to be documented in human bladder cancer. NTX exhibited prospective antineoplastic activity against a variety of malignancies, including lymphoma, glioma, leukemia, breast, bladder, pancreatic, and ovarian cancers [193]. This is particularly noteworthy. NTX has been reported to decrease the volume of tumors in the BC xenografts model by 60% and to inhibit the development of bladder cancer in the orthotopic mouse model. In the MMTV-PyMT and LPB fibrosarcoma breast cancer mouse models, nitroxoline significantly inhibited tumor development, angiogenesis, and metastasis in vivo. The cathepsin B is inhibited by NTX, which is elevated in BC patients. The inhibition of cathepsin B results in a decrease in ECM degradation and a subsequent invasion in 2D and 3D tumor models [193].
NTX significantly reduces tumor growth and metastasis by co-operating with MetAP2, SIRT1, and Cat B in vivo, thereby inhibiting the development of endothelial cell tubes. A study found that NTX eliminates cancer hallmarks such as invasion, angiogenesis, and metastasis in in-vivo models, irrespective of the route of administration. It is a superior drug against breast cancer than current regimens due to its exceptional pharmacokinetic profile and lack of systemic toxicities [166].
2.2.5. Repurposed Medications in the Treatment of Colon Cancer
- Antihypertensive and Antiarrhythmic Medications
The drugs ACEIs and ARBs are commonly used and provide significant therapeutic benefits for patients undergoing treatment for many diseases, including hypertension and heart failure. An in vivo investigation conducted by Kubota et al. revealed that both ACEIs and ARBs effectively suppressed colitis-induced colorectal cancer (CRC) in obese mice by lowering chronic inflammation and oxidative stress. In an independent trial carried out by Kedika et al., individuals who had one or more adenomatous polyps confirmed by histological analysis on a first colonoscopy and were given lisinopril, an antineoplastic chemotherapeutic agent, experienced a 41% reduction in the probability of acquiring similar polyps during the following 3–5 years. Furthermore, Engineer et al. showed that the use of ACEI/ARB and beta blockers together resulted in higher survival rates, reduced hospitalization, and slowed tumor progression in advanced colorectal cancer [194,195,196].
Beta blockers are pharmacological agents classified as class II antiarrhythmic drugs, mainly indicated for the treatment of cardiovascular disorders and several other syndromes. An investigation by Tapioles et al. showed that nebivolol specifically suppresses mitochondrial respiration in an HCT-116 colon cancer cell line. This was accomplished by impeding the function of complex I in the respiratory chain and inhibiting the proliferation of colon cancer cells. Such evidence implies that this medication has the capacity to be repurposed for the treatment of colon cancer [197,198,199].
- Anti-Helminthic
For a range of CRC cell lines, including HCT-116, RKO, HT-29, HT-8, and SW626, mebendazole demonstrates cytotoxic action. Nygren and Larsson observed that mebendazole successfully caused partial regression of metastatic lesions in a patient with refractory metastatic CRC. A separate study found that the combination of mebendazole and sulindac (an NSAID) reduced the quantity and size of intestinal microadenomas in mice with a constitutional mutation in the Adenomatous polyposis coli (APC) gene by blocking the MYC and COX-2 pathways, angiogenesis, and the release of pro-tumorigenic cytokines [68,76,200].
A salicylamide derivative, niclosamide, modulates several signaling pathways and dissociates oxidative phosphorylation. In both laboratory and animal studies, niclosamide suppressed the Wnt/β-catenin cascade, which is abnormally active in 80% of sporadic CRC. Possibly through the stimulation of autophagy, this downregulation led to reduced proliferation in several human CRC cell lines, including HCT-116, Caco2, and HT-29. Moreover, a recent investigation carried out by Kang et al. has demonstrated that the combination of niclosamide and metformin can effectively decrease Wnt and YAP, thereby cooperatively inhibiting APC-mutant CRC [201,202,203].
Sirolimus, often known as Rapamycin, is an FDA-approved inhibitor of the mTOR pathway employed for the prevention of rejection following renal transplantation. The synergistic inhibition of colon tumor growth by a combination of sirolimus and metformin has been demonstrated by Mussin et al. in both in vitro and in vivo settings. In their study, he and his colleagues provided evidence that mTOR inhibitors trigger death in colon cancer cells by promoting the dephosphorylation of 4EBP1 through CHOP-dependent DR5. This process ultimately results in a decrease in tumor growth, angiogenesis, and invasion. Wang et al. demonstrated that sirolimus suppresses mTOR activity, which in turn decreases the migration and invasion of CRC cells, therefore inhibiting the EMT induced by FBXW7 deletion [204,205,206].
2.2.6. Repurposed Medications in the Treatment of Hepatocellular Carcinoma (HCC)
Pimozide, an antipsychotic medication, can potentially suppress the growth of hepatocellular carcinoma (HCC) cell lines in laboratory settings by triggering apoptosis during the G0/G1 phase. Moreover, pimozide exhibited an inhibitory effect on HCC stem-like cells, specifically targeting the CD133-positive cell population. The luciferase assay activity of pimozide specifically targeted the expression of STAT3, leading to a decrease in the transcription levels of downstream oncogenes involved in STAT3 signaling activities. Further validation of the anticancer effect of pimozide was conducted in vivo using nude rodents [207,208,209].
Amiodarone, a class III antiarrhythmic drug and aggressive mTOR inhibitor, was shown to decrease liver tumor development by promoting autophagy activity in both the mouse xenograft model and the rat orthotropic model. Moreover, a comprehensive examination of 32,625 case control participants from Taiwan’s National Health Insurance program revealed that consistent long-term use of amiodarone significantly decreases the incidence of HCC. Amiodarone, a repurposed medication, has anticancer properties via stimulating autophagy activity, which can inhibit the development of liver tumors and prevent the onset of HCC [210,211].
Lanatoside C is an endogenous compound derived from Digitalis lanata, known for its antiarrhythmic properties. The capacity of lanatoside C to modulate HCC both in laboratory settings and in living organisms was shown by incorporating a systems biology repositioning strategy, leading to a significant decrease in tumor proliferation. Molecular mechanistic analysis revealed that lanatoside C can cause cell death by promoting the depletion of mitochondrial membrane potential. Thus, the activation of apoptotic markers ensues. Through the suppression of Thr505 phosphorylation for protein kinase delta (PKCd), lanatoside C reversed lanatoside Ce-induced mitochondrial membrane potential loss and death, so validating its molecular mechanism, which involves the AKT/mTOR pathway through control of PKCd activation [212,213].
An FDA-approved medication for pneumocystis pneumonia, atovaquone, significantly suppressed the growth of HCC by arresting the S phase of the cell cycle and enhancing both intrinsic and extrinsic apoptotic pathways, which were linked to the elevated expression of p53 and p21. Through the induction of double-stranded DNA breaks, atovaquone has been demonstrated to suppress hepatoma cell growth by generating prolonged activation of ataxia telangiectasia mutant and its downstream components, including cell cycle checkpoint kinase-2 and H2AX. Furthermore, atovaquone suppressed cell proliferation and angiogenesis in vivo, promoted apoptosis, and prolonged the survival period of tumor-bearing mice, all without any noticeable negative consequences [214,215].
2.3. Repurposing with a Mechanism-Directed Anticancer Activity
2.3.1. Repurposed Medications to Target Mitochondrial Energy Metabolism in Cancer
- Anti-diabetic
Another notable characteristic of Metformin is its capacity to specifically target oxidative phosphorylation. Empirical data indicates that Metformin may exert its anti-diabetic properties by specifically targeting complex I of the mitochondrial respiratory chain. Indeed, recent studies have shown that metformin blunts the function of complex I in a wide range of cancers [216,217].
Moreover, metformin is believed to inhibit complex I, which is responsible for the reduction in oxygen consumption in various cancer models. Metformin also decreases ATP production in a variety of malignancies. In some instances, the expression levels of complex I transcripts were altered, and the NADH/NAD ratio was reduced. Recent research indicates that the metabolic milieu of the tumor is the determining factor in the antiproliferative effect of metformin, as it has the potential to significantly alter the sensitivity to the drug [217,218]. In general, metformin primarily affects cancer progression by increasing the rate of cell death and decreasing the proliferation of tumorous cells. Phenformin has been demonstrated to enhance the radiosensitivity of cancer cells and suppress complex I expression and oxygen consumption in CRC. Phenformin has been shown to inhibit tumor growth in mouse models of cancer with oxidative phosphorylation failure. Moreover, phenformin and the oxamate inhibitor of lactate dehydrogenase synergistically decrease respiration and ATP generation [219,220].
Similarly, this drugs combination suppresses the proliferation of cells and the growth of malignancies. Canaglifozin, a pharmacological agent used to treat diabetes, suppresses the proliferation of complex I and carcinoma cells in prostate and lung cancer, and exhibits a synergistic impact when combined with radiation and chemotherapy. Pioglitazione, when combined with the glycolysis inhibitor 2-deoxyglucose, produces an antiproliferative action, suppresses oxygen consumption, and specifically affects mitochondria [222–225].
- Anti-microbe
Indeed, adverse metabolic events (AMs) have the potential to cause mitochondrial malfunction in both healthy and cancerous cells. However, malignant cells that undergo rapid division and need a substantial energy input are particularly vulnerable to AMs. Additional comprehensive examples of antimicrobials that inhibit cancer by altering mitochondrial aerobic metabolism are presented below. Members of the tetracycline and chloramphenicol families of frequently used antibiotics block both mitochondrial and bacterial translation. According to the inhibition of mitochondrial translation, these antibiotics reduce the activities of oxidative phosphorylation complexes I, IV, and V, which consist of components encoded by mitochondria [226–228].
Originally designed to eliminate aerobic bacteria, the antibiotic Bedaquiline specifically targets mitochondrial and bacterial ATP synthase [229]. The antimalarial medication atovaquone acts as an inhibitor of the oxidative phosphorylation complex III. Ivermectin, a therapy that is particularly effective against a range of parasites, inhibits Complex I activity [230,231].
Pyrvinium pamoate prevents the activity of the mitochondrial NADH-fumarate reductase machinery, consisting of complex I and II, which is responsible for treating malaria and pinworm infections [232,233].
The broad-spectrum antifungal drug itraconazole binds to the voltage-dependent mitochondrial protein anion-selective channel 1 (VDAC1) and reduces ATP synthesis [234–236].
Furthermore, quinolones, aminoglycosides, β-lactams, and oxazolidinones are further categories of antibacterial substances that cause impairment of mitochondrial activity in mammalian cells. Nevertheless, the impact of their antibacterial properties on aerobic metabolism in cancer cells has not been thoroughly investigated [237,238].
2.3.2. Repurposed Drugs as a ROS Inducer in Cancer
Tigecycline is an antibiotic approved by the FDA for treating pneumonia, complex infections, and multidrug-resistant bacterial infections. It inhibits protein synthesis, leading to bacterial death. Tigecycline is highly potent against cancer by increasing reactive oxygen species levels. It suppresses mitochondrial respiration, membrane potential, and ATP levels, causing cell death. It also enhances the effectiveness of traditional cisplatin against human hepatocellular carcinoma. In addition, a phase I clinical trial evaluating the safety and biological efficacy of intravenous tigecycline infusions for acute myeloid leukemia was successfully completed [239,240].
Levofloxacin, a third-generation fluoroquinolone antibiotic, also shown potential for cancer treatment. It suppresses lung cancer cell proliferation and apoptosis by inhibiting mitochondrial electron transport chain complex function and ROS production. It selectively targets breast cancer cells and works with 5-FU to inhibit mitochondria production [241,242].
Albendazole is a non-toxic antiparasitic medication that eliminates parasites by suppressing ATP synthesis and restricting glycogen reserves. It has been shown to induce oxidative stress in cancer treatment, triggering apoptosis and cell death in MCF-7 cells. This is linked to reduced glutathione levels, enrichment of oxidative biomarkers, and increased antioxidant enzyme activity [243,244].
Pimozide, an FDA-approved antipsychotic medication, was first identified as a dopamine antagonist with antimelanoma cancer activity in 1979. It was tested in cancer cells, showing it suppressed cancer cells by generating ROS. However, clinical trials investigating its anticancer effects have not been conducted [245–248].
3. Conclusions
The approach to cancer treatment known as drug repurposing is promising, as it provides a window of opportunity for drug discovery and is a developing trend in the field. Globally, cancer is one of the most prevalent causes of mortality, which has led to economic and public health concerns. Nevertheless, cancer treatment encounters numerous challenges, including the development of resistance mechanisms in tumor cells to anticancer agents and the reduction of the therapeutic efficacy of existing treatments. This underscores the pressing necessity for the creation of innovative medicines or strategies to combat cancer.
Drug repurposing is a cost-effective and time-saving method for enhancing the number of clinically available drugs to treat cancer, thereby contributing to the development of more personalized treatments. The current popular topic in cancer treatment is medicine of precision, which is a result of the heterogeneity associated with this disease.
Human malignancies are distinct maladies that necessitate distinct treatment options and approaches. In the past two decades, there has been substantial progress in the discovery of novel pharmaceuticals for a variety of malignant diseases. However, a considerable proportion of cancer patients are ultimately untreatable due to the development of resistance to existing drugs, which is a cause of exasperation for scientists and physicians. Many nations lack the financial capabilities to cover the escalating costs of contemporary chemotherapy treatment. Hence, drug repurposing is seen as a highly promising approach for the identification of novel anticancer treatments that are both economically efficient and can be promptly authorized for commercialization.
Clinical trials are currently being conducted with repurposed medications that proved promising anticancer activities in preclinical studies. Certain medications have been successfully repurposed and received FDA approval for the treatment of human malignant disorders, while others still in the development phase. Pharmacological meta-analysis of drugs including aspirin, statins, and metformin found a significant association with a decreased risk of cancer. These medications are expected to progress further with clinical approval for cancer therapy.
The significance of drug repurposing as a strategy for the rapid and cost-effective identification of potential anticancer agents is now being increasingly supported by a growing body of evidence.
In summary, drug repurposing presents substantial opportunities in cancer therapy, enabling the development of more cost-effective and expedited treatment options. The development of innovative cancer therapies and the improvement of patient outcomes can be expedited by confronting the challenges encountered by repurposed medicines and capitalizing on their unique opportunities.
This raises the question of whether it is worthwhile to focus more on the clinical development of approved medications that can be used to treat cancer because of their proven effectiveness in preclinical and early clinical studies, rather than new molecules discovery, which is more expensive and time-consuming.
Author Contributions
Not applicable.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Pina-Sanchez, Patricia, et al. "Cancer biology, epidemiology, and treatment in the 21st century: current status and future challenges from a biomedical perspective." Cancer Control 28 (2021). [CrossRef]
- National Institutes of Health. NIH curriculum supplement series. The Institutes, 2007. https://www.ncbi.nlm.nih.gov/books/NBK20362/.
- Cooper, Geoffrey M., and Robert E. Hausman. "The development and causes of cancer." The cell: A molecular approach 2 (2000): 725-766.
- Correia, Ana Salomé, Fátima Gärtner, and Nuno Vale. "Drug combination and repurposing for cancer therapy: the example of breast cancer." Heliyon 7.1 (2021). [CrossRef]
- Brown, Joel S., et al. "Updating the definition of cancer." Molecular Cancer Research 21.11 (2023): 1142-1147. [CrossRef]
- National Institutes of Health. NIH curriculum supplement series. The Institutes, 2007.
- Goodman, Emily N. "“What is the Environment Doing to Our Genes?”: A Pedigree Analysis of the Possible Genetic Basis of a Set of Familial Clinical Disorders." (2022).
- Cooper, Geoffrey M., and Robert E. Hausman. "The development and causes of cancer." The cell: A molecular approach 2 (2000): 725-766.
- Ramalingam, Satish, ed. Cancer Genes. Bentham Science Publishers, 2023.
- National Institutes of Health. NIH curriculum supplement series. The Institutes, 2007.
- Pelengaris, Stella, and Michael Khan, eds. "The molecular biology of cancer: A bridge from bench to bedside." (2013). https://library.iau.edu.sa/scholarly-journals/molecular-biology-cancer-bridge-bench-bedside-2nd/docview/1349242751/se-2.
- Hejmadi, Momna. Introduction to cancer biology. Bookboon, 2014.
- Greenwald, Peter, and Barbara K. Dunn. "Landmarks in the history of cancer epidemiology." Cancer research 69.6 (2009): 2151-2162. [CrossRef]
- Almatroudi, Ahmad. "The incidence rate of colorectal cancer in Saudi Arabia: An observational descriptive epidemiological analysis." International Journal of General Medicine (2020): 977-990. [CrossRef]
- Alqahtani, Wedad Saeed, et al. "Epidemiology of cancer in Saudi Arabia thru 2010–2019: a systematic review with constrained meta-analysis." AIMS public health 7.3 (2020): 679. [CrossRef]
- Basudan, Ahmed M. "Breast cancer incidence patterns in the Saudi female population: A 17-year retrospective analysis." Medicina 58.11 (2022): 1617. [CrossRef]
- Elwali, Nasr Eldin, et al. "Colorectal cancer in Saudi Arabia: The way forward." Asian Pacific journal of cancer prevention: APJCP 24.1 (2023): 13. [CrossRef]
- Flemban, Arwa F., et al. "Patterns of thyroid cancer mortality and incidence in Saudi Arabia: a 30-year study." Diagnostics 12.11 (2022): 2716. [CrossRef]
- Youk, Tae Mi, et al. "Estimation of the Three Phases by Direct Cost of Care for Non-surviving Patients with Cancer: A National Population-based Patient-level Study." Journal of Cancer 15.1 (2024): 20. [CrossRef]
- Correia, Ana Salomé, Fátima Gärtner, and Nuno Vale. "Drug combination and repurposing for cancer therapy: the example of breast cancer." Heliyon 7.1 (2021). [CrossRef]
- Sleire, Linda, et al. "Drug repurposing in cancer." Pharmacological research 124 (2017): 74-91. [CrossRef]
- Kulkarni, V. S., et al. "Drug repurposing: an effective tool in modern drug discovery." Russian Journal of Bioorganic Chemistry 49.2 (2023): 157-166. [CrossRef]
- Song, Jae W., and Kevin C. Chung. "Observational studies: cohort and case-control studies." Plastic and reconstructive surgery 126.6 (2010): 2234-2242. [CrossRef]
- Weth, Freya R., et al. "Unlocking hidden potential: advancements, approaches, and obstacles in repurposing drugs for cancer therapy." British Journal of Cancer 130.5 (2024): 703-715. [CrossRef]
- Cheng, Xi, et al. "Drug repurposing for cancer treatment through global propagation with a greedy algorithm in a multilayer network." Cancer Biology & Medicine 19.1 (2022): 74. [CrossRef]
- Sung, Hyuna, et al. "Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries." CA: a cancer journal for clinicians 71.3 (2021): 209-249. [CrossRef]
- Li, Mengyuan, et al. "An algorithm to quantify intratumor heterogeneity based on alterations of gene expression profiles." Communications biology 3.1 (2020): 505. [CrossRef]
- Turnbull, Arran K., et al. "Unlocking the transcriptomic potential of formalin-fixed paraffin embedded clinical tissues: comparison of gene expression profiling approaches." BMC bioinformatics 21 (2020): 1-10. [CrossRef]
- Rheinbay, Esther, et al. "Analyses of non-coding somatic drivers in 2,658 cancer whole genomes." Nature 578.7793 (2020): 102-111. [CrossRef]
- Hanahan, Douglas, and Robert A. Weinberg. "Hallmarks of cancer: the next generation." cell 144.5 (2011): 646-674. [CrossRef]
- World Health Organization. WHO report on cancer: setting priorities, investing wisely and providing care for all. World Health Organization, 2020. Licence: CC BY-NC-SA 3.0 IGO. https://apps.who.int/iris/handle/10665/330745.
- Creighton, Chad J. "Making use of cancer genomic databases." Current protocols in molecular biology 121.1 (2018): 19-14.
- Pushpakom, Sudeep et al. “Drug repurposing: progress, challenges and recommendations.” Nature reviews. Drug discovery vol. 18,1 (2019): 41-58. [CrossRef]
- Schcolnik-Cabrera, Alejandro et al. “Perspectives on Drug Repurposing.” Current medicinal chemistry vol. 28,11 (2021): 2085-2099. [CrossRef]
- Schein, Catherine H. "Repurposing approved drugs for cancer therapy." British Medical Bulletin 137.1 (2021): 13-27. [CrossRef]
- Rodrigues, Rafaela, Diana Duarte, and Nuno Vale. "Drug repurposing in cancer therapy: influence of patient’s genetic background in breast cancer treatment." International journal of molecular sciences 23.8 (2022): 4280. [CrossRef]
- Aggarwal, Sadhna, et al. "Drug repurposing for breast cancer therapy: Old weapon for new battle." Seminars in cancer biology. Vol. 68. Academic Press, 2021. [CrossRef]
- Elwood, Peter, et al. "Aspirin and cancer treatment: systematic reviews and meta-analyses of evidence: for and against." British Journal of Cancer 130.1 (2024): 3-8. [CrossRef]
- Zhang, Xiaoyuan, et al. "Aspirin mediates histone methylation that inhibits inflammation-related stemness gene expression to diminish cancer stemness via COX-independent manner." Stem Cell Research & Therapy 11 (2020): 1-15. [CrossRef]
- Guo, Yue, et al. "The epigenetic effects of aspirin: the modification of histone H3 lysine 27 acetylation in the prevention of colon carcinogenesis in azoxymethane-and dextran sulfate sodium-treated CF-1 mice." Carcinogenesis 37.6 (2016): 616-624. [CrossRef]
- Elwood, Peter, et al. "Aspirin and cancer: biological mechanisms and clinical outcomes." Open Biology 12.9 (2022): 220124. [CrossRef]
- Motta, Rodrigo, et al. "Immunotherapy in microsatellite instability metastatic colorectal cancer: Current status and future perspectives." Journal of clinical and translational research 7.4 (2021): 511. PMCID: PMC8445628 PMID: 34541365.
- Nounu, Aayah, et al. "A combined proteomics and Mendelian randomization approach to investigate the effects of aspirin-targeted proteins on colorectal cancer." Cancer Epidemiology, Biomarkers & Prevention 30.3 (2021): 564-575. [CrossRef]
- Rodrigues, Rafaela, Diana Duarte, and Nuno Vale. "Drug repurposing in cancer therapy: influence of patient’s genetic background in breast cancer treatment." International journal of molecular sciences 23.8 (2022): 4280. [CrossRef]
- Malik, Jonaid Ahmad, et al. "Drugs repurposed: An advanced step towards the treatment of breast cancer and associated challenges." Biomedicine & Pharmacotherapy 145 (2022): 112375. [CrossRef]
- Lord, Simon R., and Adrian L. Harris. "Is it still worth pursuing the repurposing of metformin as a cancer therapeutic?." British Journal of Cancer 128.6 (2023): 958-966. [CrossRef]
- Jourdan, Jean-Pierre, et al. "Drug repositioning: a brief overview." Journal of Pharmacy and Pharmacology 72.9 (2020): 1145-1151. [CrossRef]
- Siddiqui, Shafina, et al. "Drug repurposing: re-inventing therapies for cancer without re-entering the development pipeline—a review." Journal of the Egyptian National Cancer Institute 34.1 (2022): 33. [CrossRef]
- Zhu, Lin et al. “Metformin as anticancer agent and adjuvant in cancer combination therapy: Current progress and future prospect.” Translational oncology vol. 44 (2024): 101945. [CrossRef]
- LaMoia, Traci E., and Gerald I. Shulman. "Cellular and molecular mechanisms of metformin action." Endocrine reviews 42.1 (2021): 77-96. [CrossRef]
- Bose, Sminu, Cissy Zhang, and Anne Le. "Glucose metabolism in cancer: The Warburg effect and beyond." Adv Exp Med Biol 1311 (2021): 3-15. http://www.springercom/series/5584.
- Bailey, Clifford J. "Metformin: historical overview." Diabetologia 60.9 (2017): 1566-1576. [CrossRef]
- Hunter, Roger W., et al. "Metformin reduces liver glucose production by inhibition of fructose-1-6-bisphosphatase." Nature medicine 24.9 (2018): 1395-1406. [CrossRef]
- Qi, Jiying, et al. "Cancer risk among patients with type 2 diabetes: A real-world study in Shanghai, China." Journal of Diabetes 11.11 (2019): 878-883. [CrossRef]
- Olatunde, Ahmed, et al. "Cancer and diabetes: the interlinking metabolic pathways and repurposing actions of antidiabetic drugs." Cancer cell international 21 (2021): 1-27. [CrossRef]
- Liu, Yi-Chun, et al. "Does long-term use of antidiabetic drugs changes cancer risk?." Medicine 98.40 (2019): e17461. [CrossRef]
- Hijazi, Mohamad Ali, André Gessner, and Nahed El-Najjar. "Repurposing of chronically used drugs in cancer therapy: a chance to grasp." Cancers 15.12 (2023): 3199. [CrossRef]
- Schcolnik-Cabrera, Alejandro, Daniel Juárez-López, and Alfonso Duenas-Gonzalez. "Perspectives on drug repurposing." Current Medicinal Chemistry 28.11 (2021): 2085-2099. [CrossRef]
- Kirtonia, Anuradha, et al. "Repurposing of drugs: An attractive pharmacological strategy for cancer therapeutics." Seminars in cancer biology. Vol. 68. Academic Press, 2021. [CrossRef]
- Dąbrowski, Mariusz. "Diabetes, antidiabetic medications and cancer risk in type 2 diabetes: focus on SGLT-2 inhibitors." International Journal of Molecular Sciences 22.4 (2021): 1680. [CrossRef]
- Kole, Labanyamoy et al. “Pioglitazone, an anti-diabetic drug requires sustained MAPK activation for its anti-tumor activity in MCF7 breast cancer cells, independent of PPAR-γ pathway.” Pharmacological reports: PR vol. 68,1 (2016): 144-54. [CrossRef]
- Chi, Tiange, et al. "PPAR-γ modulators as current and potential cancer treatments." Frontiers in oncology 11 (2021): 737776. [CrossRef]
- Tan, Yan, et al. "PPAR-α modulators as current and potential cancer treatments." Frontiers in oncology 11 (2021): 599995. [CrossRef]
- Mirza, Agha Zeeshan, Ismail I. Althagafi, and Hina Shamshad. "Role of PPAR receptor in different diseases and their ligands: Physiological importance and clinical implications." European journal of medicinal chemistry 166 (2019): 502-513. [CrossRef]
- Galal, Mariam Ahmed, et al. "Metformin: A Dual-Role Player in Cancer Treatment and Prevention." International Journal of Molecular Sciences 25.7 (2024): 4083. [CrossRef]
- Hua, Yu, et al. "Metformin and cancer hallmarks: shedding new lights on therapeutic repurposing." Journal of Translational Medicine 21.1 (2023): 403. [CrossRef]
- Brown, Jason R., et al. "Phase II clinical trial of metformin as a cancer stem cell–targeting agent in ovarian cancer." JCI insight 5.11 (2020). [CrossRef]
- Pantziarka, Pan, et al. "Repurposing Drugs in Oncology (ReDO)—mebendazole as an anti-cancer agent." ecancermedicalscience 8 (2014). [CrossRef]
- Laudisi, Federica, et al. "Repositioning of anthelmintic drugs for the treatment of cancers of the digestive system." International Journal of Molecular Sciences 21.14 (2020): 4957. [CrossRef]
- Younis, Nancy S., Amal MH Ghanim, and Sameh Saber. "Mebendazole augments sensitivity to sorafenib by targeting MAPK and BCL-2 signalling in n-nitrosodiethylamine-induced murine hepatocellular carcinoma." Scientific reports 9.1 (2019): 19095. [CrossRef]
- Chen, Haifeng, Zhen Weng, and Chunfang Xu. "Albendazole suppresses cell proliferation and migration and induces apoptosis in human pancreatic cancer cells." Anti-Cancer Drugs 31.5 (2020): 431-439. [CrossRef]
- Lee, Ming Cheng, et al. "Niclosamide inhibits the cell proliferation and enhances the responsiveness of esophageal cancer cells to chemotherapeutic agents." Oncology reports 43.2 (2020): 549-561. [CrossRef]
- Xing, Xing, et al. "Anticancer role of flubendazole: Effects and molecular mechanisms." Oncology Letters 28.6 (2024): 558. [CrossRef]
- Venugopal, Sneha, et al. "Recent advances of benzimidazole as anticancer agents." Chemical Biology & Drug Design 102.2 (2023): 357-376. [CrossRef]
- Mohi-Ud-Din, Roohi, et al. "Repurposing approved non-oncology drugs for cancer therapy: a comprehensive review of mechanisms, efficacy, and clinical prospects." European journal of medical research 28.1 (2023): 345. [CrossRef]
- Guerini, Andrea Emanuele, et al. "Mebendazole as a candidate for drug repurposing in oncology: An extensive review of current literature." Cancers 11.9 (2019): 1284. [CrossRef]
- Rushworth, Linda K., et al. "Repurposing screen identifies mebendazole as a clinical candidate to synergise with docetaxel for prostate cancer treatment." British journal of cancer 122.4 (2020): 517-527. [CrossRef]
- Zhang, Zhenzhan, Jianguang Ji, and Hao Liu. "Drug repurposing in oncology: Current evidence and future direction." Current Medicinal Chemistry 28.11 (2021): 2175-2194. [CrossRef]
- Zhang, Zhe, et al. "Overcoming cancer therapeutic bottleneck by drug repurposing." Signal transduction and targeted therapy 5.1 (2020): 113. [CrossRef]
- Lu, Lu, et al. "Activation of STAT3 and Bcl-2 and reduction of reactive oxygen species (ROS) promote radioresistance in breast cancer and overcome of radioresistance with niclosamide." Oncogene 37.39 (2018): 5292-5304. [CrossRef]
- Cao, Biyin, et al. "The antiparasitic clioquinol induces apoptosis in leukemia and myeloma cells by inhibiting histone deacetylase activity." Journal of Biological Chemistry 288.47 (2013): 34181-34189. [CrossRef]
- Cao, Biyin, et al. "The Proteasomal Inhibitor Clioquinol Induces Apoptosis in Leukemia and Myeloma Cells by Inhibiting Histone Deacetylase Activity." Blood 120.21 (2012): 2449. [CrossRef]
- Borcherding, Nicholas, Yogesh Jethava, and Praveen Vikas. "Repurposing anti-cancer drugs for COVID-19 treatment." Drug design, development and therapy (2020): 5045-5058. [CrossRef]
- Pfab, Christina, et al. "Repurposing of antimicrobial agents for cancer therapy: what do we know?." Cancers 13.13 (2021): 3193. [CrossRef]
- Aldea, Mihaela, et al. "Repurposing of anticancer drugs expands possibilities for antiviral and anti-inflammatory discovery in COVID-19." Cancer Discovery 11.6 (2021): 1336-1344. [CrossRef]
- Pal, Dilipkumar, et al. "Indazole-based microtubule-targeting agents as potential candidates for anticancer drugs discovery." Bioorganic Chemistry 122 (2022): 105735. [CrossRef]
- De Lellis, Laura, et al. "Drug repurposing, an attractive strategy in pancreatic cancer treatment: preclinical and clinical updates." Cancers 13.16 (2021): 3946. [CrossRef]
- Sung, Hyuna, et al. "Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries." CA: a cancer journal for clinicians 71.3 (2021): 209-249. [CrossRef]
- Regulska, Katarzyna, et al. "Can cardiovascular drugs support cancer treatment? The rationale for drug repurposing." Drug discovery today 24.4 (2019): 1059-1065. [CrossRef]
- Hashemzehi, Milad, et al. "Angiotensin receptor blocker Losartan inhibits tumor growth of colorectal cancer." Excli Journal 20 (2021): 506. [CrossRef]
- Tan, Xin, Shu Guo, and Chenchao Wang. "Propranolol in the treatment of infantile hemangiomas." Clinical, Cosmetic and Investigational Dermatology (2021): 1155-1163. [CrossRef]
- Kwak, Ji Hee, et al. "Cardiac Evaluation before and after Oral Propranolol Treatment for Infantile Hemangiomas." Journal of Clinical Medicine 13.11 (2024): 3332. [CrossRef]
- Benish, Marganit, et al. "Perioperative use of β-blockers and COX-2 inhibitors may improve immune competence and reduce the risk of tumor metastasis." Annals of surgical oncology 15 (2008): 2042-2052. [CrossRef]
- De Lellis, Laura, et al. "Drug repurposing, an attractive strategy in pancreatic cancer treatment: preclinical and clinical updates." Cancers 13.16 (2021): 3946. [CrossRef]
- Li, Zhe, et al. "Artemisinin and its derivatives as a repurposing anticancer agent: what else do we need to do?." Molecules 21.10 (2016): 1331. [CrossRef]
- Chae, Young Kwang, et al. "Reduced risk of breast cancer recurrence in patients using ACE inhibitors, ARBs, and/or statins." Cancer investigation 29.9 (2011): 585-593. [CrossRef]
- Coulson, Rhiannon et al. “The angiotensin receptor blocker, Losartan, inhibits mammary tumor development and progression to invasive carcinoma.” Oncotarget vol. 8,12 (2017): 18640-18656. [CrossRef]
- Vinson, Gavin P. "Why isn’t the angiotensin type 1 receptor a target in cancer?." Oncotarget 8.12 (2017): 18618. [CrossRef]
- Tabatabai, Ehsan, et al. "Inhibition of angiotensin II type 1 receptor by candesartan reduces tumor growth and ameliorates fibrosis in colorectal cancer." Excli Journal 20 (2021): 863. [CrossRef]
- Asgharzadeh, Fereshteh, et al. "Inhibition of angiotensin pathway via valsartan reduces tumor growth in models of colorectal cancer." Toxicology and Applied Pharmacology 440 (2022): 115951. [CrossRef]
- Hashemzehi, Milad, et al. "Angiotensin receptor blocker Losartan inhibits tumor growth of colorectal cancer." Excli Journal 20 (2021): 506. [CrossRef]
- Pantziarka, Pan, et al. "ReDO_DB: the repurposing drugs in oncology database." ecancermedicalscience 12 (2018). [CrossRef]
- Carnet Le Provost, Killian, et al. "Trial watch: beta-blockers in cancer therapy." (2023): 2284486. [CrossRef]
- Bravo-Calderón, Diego Mauricio, et al. "Beta adrenergic receptor activation inhibits oral cancer migration and invasiveness." Archives of Oral Biology 118 (2020): 104865. [CrossRef]
- Kwon, Soon Young, et al. "β2 adrenergic receptor expression and the effects of norepinephrine and propranolol on various head and neck cancer subtypes." Oncology Letters 22.5 (2021): 1-8. [CrossRef]
- Shebl, Rania Ibrahim. "Anti-cancer potential of captopril and botulinum toxin type-A and associated p53 gene apototic stimulating activity." Iranian Journal of Pharmaceutical Research: IJPR 18.4 (2019): 1967. [CrossRef]
- Hassani, Bahareh, Zeinab Attar, and Negar Firouzabadi. "The renin-angiotensin-aldosterone system (RAAS) signaling pathways and cancer: foes versus allies." Cancer Cell International 23.1 (2023): 254. [CrossRef]
- Fukushiro-Lopes, Daniela, et al. "Repurposing Kir6/SUR2 channel activator minoxidil to arrests growth of gynecologic cancers." Frontiers in Pharmacology 11 (2020): 577. [CrossRef]
- Salanci, Šimon, et al. "The Induction of G2/M Phase Cell Cycle Arrest and Apoptosis by the Chalcone Derivative 1C in Sensitive and Resistant Ovarian Cancer Cells Is Associated with ROS Generation." International Journal of Molecular Sciences 25.14 (2024): 7541. [CrossRef]
- Qiu, Shiwen, et al. "Anti-invasive effects of minoxidil on human breast cancer cells: Combination with ranolazine." Clinical & Experimental Metastasis 39.4 (2022): 679-689. [CrossRef]
- Carlos-Escalante, José A., et al. "The use of antihypertensive drugs as coadjuvant therapy in cancer." Frontiers in oncology 11 (2021): 660943. [CrossRef]
- Ioakeim-Skoufa, Ignatios, et al. "Drug repurposing in oncology: a systematic review of randomized controlled clinical trials." Cancers 15.11 (2023): 2972. [CrossRef]
- Ribeiro, Eduarda, and Nuno Vale. "Repurposing of the Drug Tezosentan for Cancer Therapy." Current Issues in Molecular Biology 45.6 (2023): 5118-5131. [CrossRef]
- Wang, Rong, and Roderick H. Dashwood. "Endothelins and their receptors in cancer: identification of therapeutic targets." Pharmacological research 63.6 (2011): 519-524. [CrossRef]
- Lian, Xin, et al. "Anticancer properties of fenofibrate: a repurposing use." Journal of Cancer 9.9 (2018): 1527. [CrossRef]
- Chen, Lulu, et al. "Fenofibrate-induced mitochondrial dysfunction and metabolic reprogramming reversal: the anti-tumor effects in gastric carcinoma cells mediated by the PPAR pathway." American Journal of Translational Research 12.2 (2020): 428. PMCID: PMC7061836 PMID: 32194894.
- Kale, Vijay Pralhad, Shantu G. Amin, and Manoj K. Pandey. "Targeting ion channels for cancer therapy by repurposing the approved drugs." Biochimica et Biophysica Acta (BBA)-Biomembranes 1848.10 (2015): 2747-2755. [CrossRef]
- Zhao, Jiayu, et al. "The modulation of ion channels in cancer chemo-resistance." Frontiers in Oncology 12 (2022): 945896. [CrossRef]
- Altamura, Concetta, et al. "Ion channel involvement in tumor drug resistance." Journal of personalized medicine 12.2 (2022): 210. PMCID: PMC8878471 PMID: 35207698.
- Leanza, Luigi, et al. "Pharmacological targeting of ion channels for cancer therapy: in vivo evidences." Biochimica et Biophysica Acta (BBA)-Molecular Cell Research 1863.6 (2016): 1385-1397. [CrossRef]
- Bell, Damian C., et al. "News and views on ion channels in cancer: is cancer a channelopathy?." Frontiers in Pharmacology 14 (2023): 1258933. [CrossRef]
- Li, Meizeng, et al. "Potassium channels: Novel targets for tumor diagnosis and chemoresistance." Frontiers in Oncology 12 (2023): 1074469. [CrossRef]
- Dupuy, Maryne, et al. "SKCa-and Kv1-type potassium channels and cancer: Promising therapeutic targets?." Biochemical Pharmacology 216 (2023): 115774. [CrossRef]
- Luis, Enoch, et al. "The Kv10. 1 channel: a promising target in cancer." International journal of molecular sciences 23.15 (2022): 8458. [CrossRef]
- Sakellakis, Minas, et al. "Novel insights into voltage-gated ion channels: Translational breakthroughs in medical oncology." Channels 18.1 (2024): 2297605. [CrossRef]
- Pasello, Giulia, et al. "Effects of sulfonylureas on tumor growth: a review of the literature." The oncologist 18.10 (2013): 1118-1125. [CrossRef]
- Zúñiga, Leandro, et al. "Potassium channels as a target for cancer therapy: Current perspectives." OncoTargets and therapy 15 (2022): 783. PMCID: PMC9309325 PMID: 35899081.
- Wong, Bing-Sang, et al. "Anticancer effects of antihypertensive L-type calcium channel blockers on chemoresistant lung cancer cells via autophagy and apoptosis." Cancer Management and Research (2020): 1913-1927. [CrossRef]
- Huang, Ting, Jingyi Zhou, and Jianliu Wang. "Calcium and calcium-related proteins in endometrial cancer: opportunities for pharmacological intervention." International Journal of Biological Sciences 18.3 (2022): 1065. PMCID: PMC8771838 PMID: 35173539.
- Correia, Ana Salomé, Fátima Gärtner, and Nuno Vale. "Drug combination and repurposing for cancer therapy: the example of breast cancer." Heliyon 7.1 (2021). [CrossRef]
- Wang, Xiyue, et al. "A pathology foundation model for cancer diagnosis and prognosis prediction." Nature (2024): 1-9. [CrossRef]
- Parvathaneni, Vineela, et al. "Repurposing bedaquiline for effective non-small cell lung cancer (NSCLC) therapy as inhalable cyclodextrin-based molecular inclusion complexes." International journal of molecular sciences 22.9 (2021): 4783. [CrossRef]
- Fiorillo, Marco, et al. "Bedaquiline, an FDA-approved antibiotic, inhibits mitochondrial function and potently blocks the proliferative expansion of stem-like cancer cells (CSCs)." Aging (Albany NY) 8.8 (2016): 1593. [CrossRef]
- Fu, Leilei, et al. "Repurposing non-oncology small-molecule drugs to improve cancer therapy: Current situation and future directions." Acta Pharmaceutica Sinica B 12.2 (2022): 532-557. [CrossRef]
- Li, Jiayu, et al. "Tetracycline antibiotics: Potential anticancer drugs." European journal of pharmacology (2023): 175949. [CrossRef]
- Dong, Zhen, et al. "Biological functions and molecular mechanisms of antibiotic tigecycline in the treatment of cancers." International journal of molecular sciences 20.14 (2019): 3577. [CrossRef]
- Bailly, Christian, and Gérard Vergoten. "A new horizon for the old antibacterial drug clofoctol." Drug Discovery Today 26.5 (2021): 1302-1310. [CrossRef]
- Wang, Minghua, et al. "Identification of an old antibiotic clofoctol as a novel activator of unfolded protein response pathways and an inhibitor of prostate cancer." British journal of pharmacology 171.19 (2014): 4478-4489. [CrossRef]
- van der Zanden, Sabina Y., Xiaohang Qiao, and Jacques Neefjes. "New insights into the activities and toxicities of the old anticancer drug doxorubicin." The FEBS journal 288.21 (2021): 6095-6111. [CrossRef]
- Shandilya, Manish, et al. "Molecular-level understanding of the anticancer action mechanism of anthracyclines." Advances in precision medicine oncology (2020). [CrossRef]
- Mukai, Hirofumi, et al. "A first-in-human Phase 1 study of epirubicin-conjugated polymer micelles (K-912/NC-6300) in patients with advanced or recurrent solid tumors." Investigational new drugs 35 (2017): 307-314. [CrossRef]
- Pourgholami, Mohammad H., et al. "Minocycline inhibits growth of epithelial ovarian cancer." Gynecologic oncology 125.2 (2012): 433-440. [CrossRef]
- Afshari, Amir R., Hamid Mollazadeh, and Amirhossein Sahebkar. "Minocycline in treating glioblastoma multiforme: far beyond a conventional antibiotic." Journal of oncology 2020.1 (2020): 8659802. [CrossRef]
- Reed, Gregory A., et al. "A Phase 1 study of intravenous infusions of tigecycline in patients with acute myeloid leukemia." Cancer medicine 5.11 (2016): 3031-3040. [CrossRef]
- Novella, Pugliese, et al. "Tigecycline-Based Front-Line Antibiotic Therapy Significantly Decreases Mortality Among Patients with Neutropenic Enterocolitis Following Cytarabine-Containing Chemotherapy for the Remission Induction of Acute Myeloid Leukemia." Blood 128.22 (2016): 3550. [CrossRef]
- Nowakowska, Justyna, et al. "Recent Development of Fluoroquinolone Derivatives as Anticancer Agents." Molecules 29.15 (2024). PMCID: PMC11314068 PMID: 39124943.
- AbuBaih, Rania Hamdy, Michael Atef Fawzy, and Maiiada Hassan Nazmy. "The prospective potential of fluoroquinolones as anticancer agents." Journal of Modern Research 5.1 (2023): 4-10. [CrossRef]
- Zhou, Wenmin, et al. "Chloroquine against malaria, cancers and viral diseases." Drug Discovery Today 25.11 (2020): 2012-2022. [CrossRef]
- Liu, Yanqing, et al. "Pharmacology Progresses and Applications of Chloroquine in Cancer Therapy." International Journal of Nanomedicine (2024): 6777-6809. [CrossRef]
- Mauthe, Mario, et al. "Chloroquine inhibits autophagic flux by decreasing autophagosome-lysosome fusion." Autophagy 14.8 (2018): 1435-1455. [CrossRef]
- Vlachos, Nikolaos, et al. "Repurposing antipsychotics for cancer treatment." Biomedicines 9.12 (2021): 1785. [CrossRef]
- Lianos, Georgios D., et al. "Repurposing antipsychotic drugs for cancer treatment: current evidence and future perspectives." Expert Review of Anticancer Therapy 22.2 (2022): 131-134. [CrossRef]
- Moura, Catarina, and Nuno Vale. "The role of dopamine in repurposing drugs for oncology." Biomedicines 11.7 (2023): 1917. [CrossRef]
- Sousa, Sofia M., et al. "Repurposing some of the Well-known Non-steroid Anti-inflammatory Drugs (NSAIDs) for Cancer Treatment." Current Topics in Medicinal Chemistry 23.13 (2023): 1171-1195. [CrossRef]
- Ozleyen, Adem, et al. "Looking at NSAIDs from a historical perspective and their current status in drug repurposing for cancer treatment and prevention." Journal of Cancer Research and Clinical Oncology 149.5 (2023): 2095-2113. [CrossRef]
- Joo, Young Bin, et al. "Use of disease-modifying antirheumatic drugs after cancer diagnosis in rheumatoid arthritis patients." Journal of Rheumatic Diseases 29.3 (2022): 162-170. [CrossRef]
- Calip, Gregory S., et al. "Targets of biologic disease-modifying antirheumatic drugs and risk of multiple myeloma." International journal of cancer 147.5 (2020): 1300-1305. [CrossRef]
- Aroosa, Mir, et al. "The evidence for repurposing anti-epileptic drugs to target cancer." Molecular Biology Reports 50.9 (2023): 7667-7680. [CrossRef]
- Sulsenti, Roberta, et al. "Repurposing of the antiepileptic drug levetiracetam to restrain neuroendocrine prostate cancer and inhibit mast cell support to adenocarcinoma." Frontiers in immunology 12 (2021): 622001. [CrossRef]
- Malla, RamaRao, et al. "Revitalizing Cancer Treatment: Exploring the Role of Drug Repurposing." Cancers 16.8 (2024): 1463. [CrossRef]
- Rizzo, Ambra, et al. "In vitro antineoplastic effects of brivaracetam and lacosamide on human glioma cells." Journal of Experimental & Clinical Cancer Research 36 (2017): 1-13. [CrossRef]
- Moutal, Aubin, et al. "CRMP2 phosphorylation drives glioblastoma cell proliferation." Molecular neurobiology 55 (2018): 4403-4416. [CrossRef]
- Morales-Urteaga, Xabier, et al. "CRMP2 as a candidate target to interfere with lung cancer cell migration." (2021). [CrossRef]
- Costa, Bárbara, and Nuno Vale. "Understanding Lamotrigine’s role in the CNS and possible future evolution." International journal of molecular sciences 24.7 (2023): 6050. [CrossRef]
- Kim, Ki Jung, Seung Hyun Jeun, and Ki-Wug Sung. "Lamotrigine, an antiepileptic drug, inhibits 5-HT3 receptor currents in NCB-20 neuroblastoma cells." The Korean Journal of Physiology & Pharmacology: Official Journal of the Korean Physiological Society and the Korean Society of Pharmacology 21.2 (2017): 169. [CrossRef]
- Wu, King-Chuen, et al. "Drug repurposing: the mechanisms and signaling pathways of anti-cancer effects of anesthetics." Biomedicines 10.7 (2022): 1589. [CrossRef]
- Zhou, Daipeng, et al. "Repositioning lidocaine as an anticancer drug: the role beyond anesthesia." Frontiers in Cell and Developmental Biology 8 (2020): 565. [CrossRef]
- Lourenço, Tânia, and Nuno Vale. "Pharmacological efficacy of repurposing drugs in the treatment of prostate cancer." International Journal of Molecular Sciences 24.4 (2023): 4154. [CrossRef]
- Alfaqih, Mahmoud A., et al. "CYP27A1 loss dysregulates cholesterol homeostasis in prostate cancer." Cancer research 77.7 (2017): 1662-1673. [CrossRef]
- Geng, Xinran, et al. "Cardiac glycosides inhibit cancer through Na/K-ATPase-dependent cell death induction." Biochemical pharmacology 182 (2020): 114226. [CrossRef]
- Kumavath, Ranjith, et al. "Emergence of cardiac glycosides as potential drugs: Current and future scope for cancer therapeutics." Biomolecules 11.9 (2021): 1275. [CrossRef]
- Thiruchenthooran, Vaikunthavasan, Elena Sánchez-López, and Anna Gliszczyńska. "Perspectives of the application of non-steroidal anti-inflammatory drugs in cancer therapy: Attempts to overcome their unfavorable side effects." Cancers 15.2 (2023): 475. [CrossRef]
- Duarte, Diana, and Nuno Vale. "Antidepressant drug sertraline against human cancer cells." Biomolecules 12.10 (2022): 1513. [CrossRef]
- Peixoto, Rita, Maria de Lourdes Pereira, and Miguel Oliveira. "Beta-blockers and cancer: where are we?." Pharmaceuticals 13.6 (2020): 105. [CrossRef]
- Ma, Sai-Nan, et al. "The anti-cancer properties of heparin and its derivatives: A review and prospect." Cell adhesion & migration 14.1 (2020): 118-128. [CrossRef]
- Rawla, Prashanth. "Epidemiology of prostate cancer." World journal of oncology 10.2 (2019): 63. [CrossRef]
- Bahmad, Hisham F., et al. "Overcoming drug resistance in advanced prostate cancer by drug repurposing." Medical Sciences 10.1 (2022): 15. [CrossRef]
- Araújo, Diana, et al. "Repurposed drugs in gastric cancer." Molecules 28.1 (2022): 319. [CrossRef]
- Fatemi, Nayeralsadat, et al. "Current trends and future prospects of drug repositioning in gastrointestinal oncology." Frontiers in Pharmacology 14 (2024): 1329244. [CrossRef]
- Mu, Jiasheng, et al. "Thioridazine, an antipsychotic drug, elicits potent antitumor effects in gastric cancer." Oncology reports 31.5 (2014): 2107-2114. [CrossRef]
- Yang, Zheng-Yan, et al. "Thioridazine reverses trastuzumab resistance in gastric cancer by inhibiting S-phase kinase associated protein 2-mediated aerobic glycolysis." World Journal of Gastroenterology 29.45 (2023): 5974. [CrossRef]
- Bedford, Matthew R., et al. "Iron chelation in the treatment of cancer: a new role for deferasirox?." The Journal of Clinical Pharmacology 53.9 (2013): 885-891. [CrossRef]
- Stewart, A. Keith. "How thalidomide works against cancer." Science 343.6168 (2014): 256-257. [CrossRef]
- Kale, Vijay P., et al. "Old drugs, new uses: Drug repurposing in hematological malignancies." Seminars in cancer biology. Vol. 68. Academic Press, 2021. [CrossRef]
- Licht, Jonathan D., Jake Shortt, and Ricky Johnstone. "From anecdote to targeted therapy: the curious case of thalidomide in multiple myeloma." Cancer cell 25.1 (2014): 9-11. [CrossRef]
- Mhatre, Vishruti, Lokesh Kumar Vyas, and Dileep Kumar Bharati. "Rebirth of thalidomide." World Journal of Pharmaceutical Research 11.7 (2022): 842-854.
- Iqbal, Nida, and Naveed Iqbal. "Imatinib: a breakthrough of targeted therapy in cancer." Chemotherapy research and practice 2014.1 (2014): 357027. [CrossRef]
- Phuar, Hsiao Ling, et al. "Tyrosine kinase inhibitors initiation, cost sharing, and health care utilization in patients with newly diagnosed chronic myeloid leukemia: A retrospective claims-based study." Journal of Managed Care & Specialty Pharmacy 25.10 (2019): 1140-1150.
- Jabbour, Elias, and Hagop Kantarjian. "Chronic myeloid leukemia: 2018 update on diagnosis, therapy and monitoring." American journal of hematology 93.3 (2018): 442-459. [CrossRef]
- Senapati, Jayastu, et al. "Pathogenesis and management of accelerated and blast phases of chronic myeloid leukemia." Leukemia 37.1 (2023): 5-17. [CrossRef]
- Anjum, Sadia, et al. "Enhancing therapeutic efficacy: sustained delivery of 5-fluorouracil (5-FU) via thiolated chitosan nanoparticles targeting CD44 in triple-negative breast cancer." Scientific Reports 14.1 (2024): 11431. [CrossRef]
- Shivani, Dave, et al. "Drug repurposing: a retrospective revolution in breast cancer medicine." Discover Medicine 1.1 (2024): 11. [CrossRef]
- Zhang, Q. I., et al. "Preclinical pharmacodynamic evaluation of antibiotic nitroxoline for anticancer drug repurposing." Oncology Letters 11.5 (2016): 3265-3272. [CrossRef]
- El Zarif, Talal, et al. "Overcoming therapy resistance in colon cancer by drug repurposing." Cancers 14.9 (2022): 2105. [CrossRef]
- Qi, Jia, et al. "Antihypertensive medications and risk of colorectal cancer in British Columbia." Frontiers in Pharmacology 14 (2023): 1301423. [CrossRef]
- Kedika, Ramalinga, et al. "Long-term use of angiotensin converting enzyme inhibitors is associated with decreased incidence of advanced adenomatous colon polyps." Journal of clinical gastroenterology 45.2 (2011): e12-e16. [CrossRef]
- Massalee, Rachel, and Xuefang Cao. "Repurposing beta-blockers for combinatory cancer treatment: effects on conventional and immune therapies." Frontiers in Pharmacology 14 (2024): 1325050. [CrossRef]
- El Zarif, Talal, et al. "Overcoming therapy resistance in colon cancer by drug repurposing." Cancers 14.9 (2022): 2105.
- Schein, Catherine H. "Repurposing approved drugs for cancer therapy." British Medical Bulletin 137.1 (2021): 13-27. [CrossRef]
- Pinto, Laine Celestino, et al. "Mebendazole induces apoptosis via C-MYC inactivation in malignant ascites cell line (AGP01)." Toxicology in Vitro 60 (2019): 305-312. [CrossRef]
- Arend, Rebecca C., et al. "Niclosamide and its analogs are potent inhibitors of Wnt/β-catenin, mTOR and STAT3 signaling in ovarian cancer." Oncotarget 7.52 (2016): 86803. [CrossRef]
- Wang, Jiangbo, et al. "Niclosamide-induced Wnt signaling inhibition in colorectal cancer is mediated by autophagy." Biochemical Journal 476.3 (2019): 535-546. [CrossRef]
- Hamilton, Gerhard, and Barbara Rath. "Repurposing of anthelminthics as anticancer drugs." Oncomedicine 3 (2018): 1-8. [CrossRef]
- Mussin, Nadiar, et al. "Sirolimus and metformin synergistically inhibits colon cancer in vitro and in vivo." Journal of Korean Medical Science 32.9 (2017): 1385-1395. [CrossRef]
- Sanchez-Plumed, J. A. , et al. "Sirolimus, the first mTOR inhibitor." Nefrología (English Edition) 26 (2006): 21-32.
- Granata, Simona, et al. "mTOR-inhibitors and post-transplant diabetes mellitus: a link still debated in kidney transplantation." Frontiers in Medicine 10 (2023): 1168967. [CrossRef]
- Jiang, Ge, et al. "The antipsychotic drug pimozide promotes apoptosis through the RAF/ERK pathway and enhances autophagy in breast cancer cells." Cancer Biology & Therapy 25.1 (2024): 2302413. [CrossRef]
- Lianos, Georgios D., et al. "Repurposing antipsychotic drugs for cancer treatment: current evidence and future perspectives." Expert Review of Anticancer Therapy 22.2 (2022): 131-134. [CrossRef]
- Chen, Jia-Jie, et al. "Antipsychotic agent pimozide promotes reversible proliferative suppression by inducing cellular quiescence in liver cancer." Oncology reports 42.3 (2019): 1101-1109. [CrossRef]
- Attia, Yasmeen M., Heba Ewida, and Mahmoud Salama Ahmed. "Successful stories of drug repurposing for cancer therapy in hepatocellular carcinoma." Drug Repurposing in Cancer Therapy. Academic Press, 2020. 213-229. [CrossRef]
- Huang, Sheng-Teng, et al. "Improved survival in hepatocellular carcinoma patients with cardiac arrhythmia by amiodarone treatment through autophagy." International journal of molecular sciences 20.16 (2019): 3978. [CrossRef]
- Attia, Yasmeen M., Heba Ewida, and Mahmoud Ahmed. "Successful Stories of Drug Repurposing for Cancer Therapy in Hepatocellular Carcinoma, To and Cho_Drug Repurposing in Cancer Therapy." (2020). https://buescholar.bue.edu.
- Chao, Min-Wu, et al. "Lanatoside C, a cardiac glycoside, acts through protein kinase Cδ to cause apoptosis of human hepatocellular carcinoma cells." Scientific reports 7.1 (2017): 46134. [CrossRef]
- Gao, Xiaoge, et al. "Anti-malarial atovaquone exhibits anti-tumor effects by inducing DNA damage in hepatocellular carcinoma." American Journal of Cancer Research 8.9 (2018): 1697. PMCID: PMC6176191 PMID: 30323964.
- Stevens, Alexandra McLean, et al. "Repurposing atovaquone as a therapeutic against acute myeloid leukemia (AML): combination with conventional chemotherapy is feasible and well tolerated." Cancers 15.4 (2023): 1344. [CrossRef]
- Hua, Yu, et al. "Metformin and cancer hallmarks: shedding new lights on therapeutic repurposing." Journal of Translational Medicine 21.1 (2023): 403. [CrossRef]
- Kalyanaraman, Balaraman, et al. "Modified metformin as a more potent anticancer drug: mitochondrial inhibition, redox signaling, antiproliferative effects and future EPR studies." Cell biochemistry and biophysics 75 (2017): 311-317. [CrossRef]
- Hua, Yu, et al. "Metformin and cancer hallmarks: shedding new lights on therapeutic repurposing." Journal of Translational Medicine 21.1 (2023): 403. [CrossRef]
- Cheng, Gang, et al. "Mitochondria-targeted analogues of metformin exhibit enhanced antiproliferative and radiosensitizing effects in pancreatic cancer cells." Cancer research 76.13 (2016): 3904-3915. [CrossRef]
- Amengual-Cladera, Emilia, et al. "Metformin: From Diabetes to Cancer—Unveiling Molecular Mechanisms and Therapeutic Strategies." Biology 13.5 (2024): 302. [CrossRef]
- Basak, Debasish, David Gamez, and Subrata Deb. "SGLT2 inhibitors as potential anticancer agents." Biomedicines 11.7 (2023): 1867. [CrossRef]
- Aminzadeh-Gohari, Sepideh, et al. "From old to new—Repurposing drugs to target mitochondrial energy metabolism in cancer." Seminars in cell & developmental biology. Vol. 98. Academic Press, 2020. doi.org/10.1016/j.semcdb.2019.05.025.
- Papadopoli, David, et al. "Perturbations of cancer cell metabolism by the antidiabetic drug canagliflozin." Neoplasia 23.4 (2021): 391-399. [CrossRef]
- Jin, Ping, et al. "Mitochondrial adaptation in cancer drug resistance: prevalence, mechanisms, and management." Journal of Hematology & Oncology 15.1 (2022): 97. [CrossRef]
- Raafat, Shereen Nader, et al. "Enhancing the anticancer potential of metformin: fabrication of efficient nanospanlastics, in vitro cytotoxic studies on HEP-2 cells and reactome enhanced pathway analysis." International Journal of Pharmaceutics: X 6 (2023): 100215. [CrossRef]
- Aminzadeh-Gohari, Sepideh, et al. "From old to new—Repurposing drugs to target mitochondrial energy metabolism in cancer." Seminars in cell & developmental biology. Vol. 98. Academic Press, 2020. [CrossRef]
- Wang, Sheng-Fan, Ling-Ming Tseng, and Hsin-Chen Lee. "Role of mitochondrial alterations in human cancer progression and cancer immunity." Journal of biomedical science 30.1 (2023): 61. [CrossRef]
- Yang, Yi, et al. "The mechanisms of action of mitochondrial targeting agents in cancer: inhibiting oxidative phosphorylation and inducing apoptosis." Frontiers in Pharmacology 14 (2023): 1243613. [CrossRef]
- Fiorillo, Marco, et al. "Bedaquiline, an FDA-approved antibiotic, inhibits mitochondrial function and potently blocks the proliferative expansion of stem-like cancer cells (CSCs)." Aging (Albany NY) 8.8 (2016): 1593. [CrossRef]
- Greene, John, Ashvina Segaran, and Simon Lord. "Targeting OXPHOS and the electron transport chain in cancer; Molecular and therapeutic implications." Seminars in Cancer Biology. Vol. 86. Academic Press, 2022. [CrossRef]
- Fiorillo, Marco, et al. "Repurposing atovaquone: targeting mitochondrial complex III and OXPHOS to eradicate cancer stem cells." Oncotarget 7.23 (2016): 34084. [CrossRef]
- Schultz, Christopher W., and Avinoam Nevler. "Pyrvinium pamoate: Past, present, and future as an anti-cancer drug." Biomedicines 10.12 (2022): 3249. [CrossRef]
- Tomitsuka, Eriko, Kiyoshi Kita, and Hiroyasu Esumi. "An anticancer agent, pyrvinium pamoate inhibits the NADH–fumarate reductase system—a unique mitochondrial energy metabolism in tumour microenvironments." The journal of biochemistry 152.2 (2012): 171-183. [CrossRef]
- Weng, Ningna, et al. "Repurposing antifungal drugs for cancer therapy." Journal of Advanced Research 48 (2023): 259-273. [CrossRef]
- Tsubamoto, Hiroshi, et al. "Repurposing itraconazole as an anticancer agent." Oncology letters 14.2 (2017): 1240-1246. [CrossRef]
- Head, Sarah A., et al. "Antifungal drug itraconazole targets VDAC1 to modulate the AMPK/mTOR signaling axis in endothelial cells." Proceedings of the National Academy of Sciences 112.52 (2015): E7276-E7285. [CrossRef]
- Pancu, Daniel Florin, et al. "Antibiotics: conventional therapy and natural compounds with antibacterial activity—a pharmaco-toxicological screening." Antibiotics 10.4 (2021): 401. [CrossRef]
- Stokes, Jonathan M., et al. "A deep learning approach to antibiotic discovery." Cell 180.4 (2020): 688-702. [CrossRef]
- Bano, Nilofer, et al. "Drug Repurposing of Selected Antibiotics: An Emerging Approach in Cancer Drug Discovery." ACS omega 9.25 (2024): 26762-26779. [CrossRef]
- Wang, Jiabing, et al. "Targeting reactive oxygen species capacity of tumor cells with repurposed drug as an anticancer therapy." Oxidative medicine and cellular longevity 2021.1 (2021): 8532940. [CrossRef]
- Yadav, Vikas, and Puneet Talwar. "Repositioning of fluoroquinolones from antibiotic to anti-cancer agents: An underestimated truth." Biomedicine & Pharmacotherapy 111 (2019): 934-946. [CrossRef]
- Bano, Nilofer, et al. "Drug Repurposing of Selected Antibiotics: An Emerging Approach in Cancer Drug Discovery." ACS omega 9.25 (2024): 26762-26779. [CrossRef]
- Chai, Jong-Yil, Bong-Kwang Jung, and Sung-Jong Hong. "Albendazole and mebendazole as anti-parasitic and anti-cancer agents: an update." The Korean Journal of Parasitology 59.3 (2021): 189. PMCID: PMC8255490 PMID: 34218593.
- Castro, L. S. E. P. W., et al. "Albendazole as a promising molecule for tumor control." Redox biology 10 (2016): 90-99. [CrossRef]
- Jiang, Ge, et al. "The antipsychotic drug pimozide promotes apoptosis through the RAF/ERK pathway and enhances autophagy in breast cancer cells." Cancer Biology & Therapy 25.1 (2024): 2302413. [CrossRef]
- Kim, Ukjin, et al. "Pimozide inhibits the human prostate cancer cells through the generation of reactive oxygen species." Frontiers in Pharmacology 10 (2020): 1517. [CrossRef]
- El-Habib, Dakir, et al. "The anti-psychotic drug pimozide is a novel chemotherapeutic for breast cancer." Oncotarget 9.79 (2018): 34889-34910. [CrossRef]
- Vlachos, Nikolaos, et al. "Repurposing antipsychotics for cancer treatment." Biomedicines 9.12 (2021): 1785. [CrossRef]
Figure 1.
Illustration of chemical carcinogens that induce DNA damage and mutations.
Figure 2.
(a) ASR incidence rates per sex; (b) ASR incidence and mortality rates.
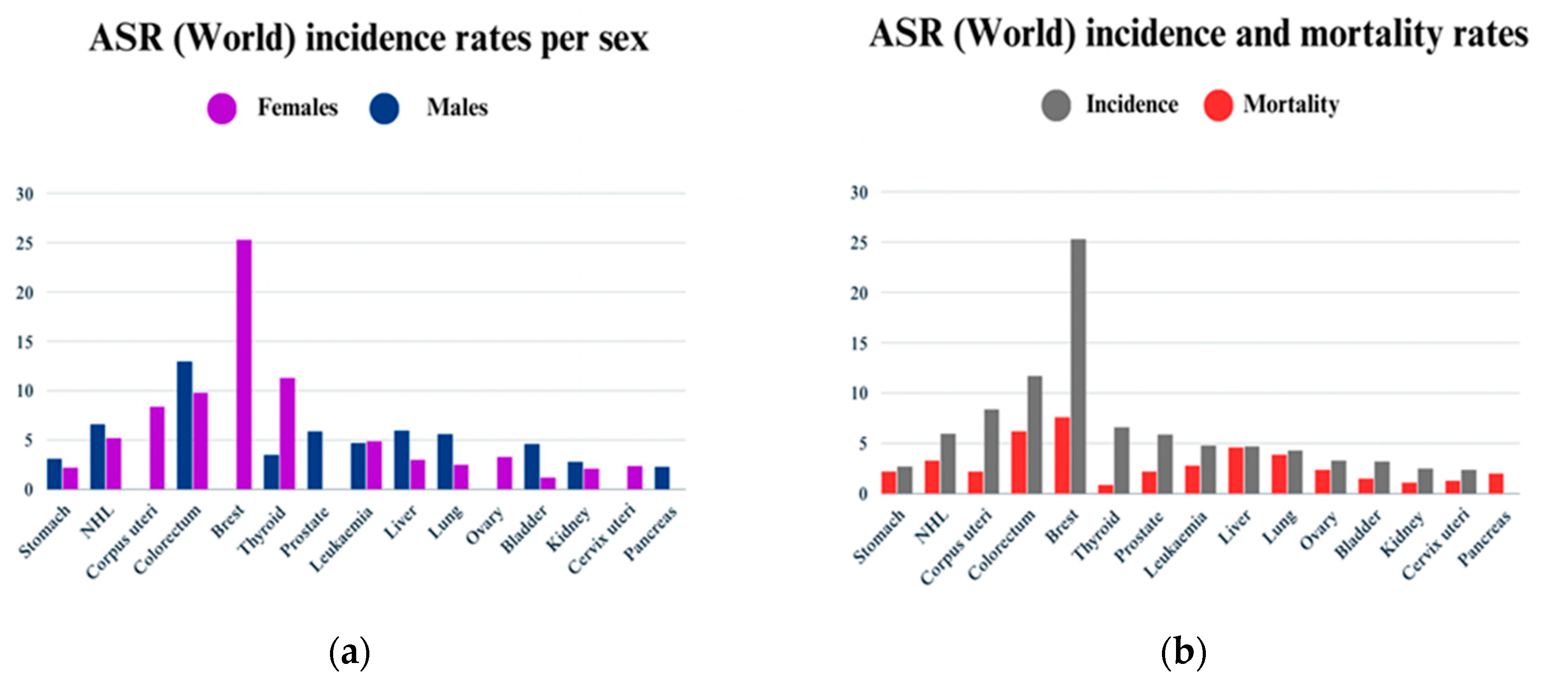

Table 1.
Repurposed drugs for cancer treatment with their chemical structure, new indication, old and new targets, and development status.
Table 1.
Repurposed drugs for cancer treatment with their chemical structure, new indication, old and new targets, and development status.
| Pharmacological class | Drug name | Chemical structure | New therapeutic indication | New target | Original target | Development status | References |
|---|---|---|---|---|---|---|---|
| Anti-Platelet | Aspirin |  |
gastric, esophageal, colorectal, pancreatic, ovarian, endometrial, breast, and prostate cancers | PIK3CA, mTORC1 and AMPK. | COXs | Phase II and III clinical trials, meta-analysis | 37-45 |
| Anti-Diabetic | Metformin (biguanides) |
 |
Colorectal, breast, pancreatic, prostate, lung, and cervical malignancies. | cell cycle/pSTAT3, S6 kinase, and mTOR/AMPK/ | Mitochondrial respiration | Phase II and III clinical trials. | 46-54,65-67, 201-206, 216-220, 225 |
| Pioglitazone (TZDs) |
|
Breast, prostate, and colon cancer |
PPAR γ | PPAR γ | Phase II trials. | 61-67 | |
| Desmopressin |  |
Colon cancer | COX-2 and CD1 | AVPR2 | Preclinical | 57-60 | |
| Anti-Helminthic | Flubendazole (benzimidazole) |
 |
Neuroblastoma, multiple myeloma, leukemia, lung, liver, colorectal, and breast cancer. | Apoptosis (caspase 3 and 7) | Tubulin polymerization | Preclinical | 70-74 |
| Parbendazole |  |
pancreatic cancer | Apoptosis, cell cycle, and DNA damage. | Tubulin polymerization | Preclinical | 57 | |
| Mebendazole (MZ) |  |
Glioblastoma, melanoma, prostate, breast, brain, ovarian, colon, lung, colorectal and endocrine cancers. | Cell cycle, apoptosis (caspase-3 pathway), ABL and BRAF. | Tubulin polymerization | Preclinical | 68-70,75-78, 200,243 | |
| Niclosamide |
 |
Colon, prostate, liver, ovarian, and breast cancers. | Wnt/β-catenin, NF-KB, mTOR, and JAK/STAT3 pathways. | uncoupling of oxidative phosphorylation | Preclinical | 72,79-80,201-203 | |
| Clioquinol |  |
leukemia and malignant myeloma. |
HDAC | DNA replication | Preclinical | 81-82 | |
| Anti-Viral | Ritonavir |  |
Ovarian, pancreatic, and breast cancer, lymphocytic leukemia | Apoptosis | Protease inhibitors target HIV | Preclinical | 84-86 |
| Ribavirin |  |
acute myeloid leukemia (AML) | Induces VEGF mRNA translation | RNA replicating | phase II clinical trial | 87 | |
| Cidofovir |  |
Glioblastomas | Apoptosis | viral DNA polymerase | Preclinical | 87 | |
|
Cardiovascular Anti-Hypertension Medication | |||||||
| Angiotensin receptor blocker | Losartan |  |
Pancreatic cancer | depleting the matrix and reducing collagen I levels | Angiotensin receptor | phase II clinical trials. | 88-90,97,101 |
| Candesartan |  |
Colon cancer, prostate cancer, liver and kidney cancer | VEGF expression | Angiotensin receptor | Preclinical | 99-101,106-107,111 | |
| Irbesartan |  |
Colon cancer, liver and kidney cancer | AP-1 DNA binding, pErbB3, and p38/MAPK | Angiotensin receptor | Preclinical | 88-90,99-101,111 | |
| Telmisartan |  |
Colon cancer, liver and kidney cancer | pErbB3, p38/MAPK caspase-3, Bcl-2, PI3/AKT pathway |
Angiotensin receptor | Preclinical | 88-90,111-112 | |
| ACE inhibitors | Captopril |  |
Colorectal liver metastases prostate cancer liver and kidney cancer |
p53 expression | ACE | Preclinical | 88-90,99-101,106-107,111-112 |
| Enalapril |  |
Colorectal cancer (CRC) | IGF-IR 1 | ACE | Preclinical | 99-101 | |
| Beta-blockers | Carvedilol |  |
Breast cancer | Growth factor receptors and mitochondrial function | Beta receptors | Phase II trials for prostate cancer. | 88-90,104-105 |
| Propranolol |
 |
Ovarian, colorectal, lung, prostate, breast cancer, multiple myeloma. pancreatic, neuroblastoma, angiosarcoma, melanoma, and leukemia. |
p-AKT/p-ERK/p-MEK and CD8+ T cells JNK signaling pathway and ROS. |
Beta receptors | Phase I trials for ovarian cancer Phase II trials for prostate cancer. | 91-92,93-95,96-98,104-105 | |
| Direct vasodilator | Minoxidil |  |
Ovarian cancer | caspase-3 |
ATP-sensitive potassium channels | Phase II trial | 108-110 |
| Hydralazine |
 |
Prostate cancer |
Induces demethylation, re-expressing suppressed genes | Direct vasodilator | Preclinical | 106-107 | |
| Tezosentan |  |
Various cancer types especially with high expression of endothelin receptor type A | Endothelin receptor A | Endothelin receptor A/B | Preclinical | 113-114 | |
|
Cardiovascular Antihyperlipidemic |
Fenofibrate |
 |
Breast cancer lung cancer |
AMPK, NF-κB and ERK signaling | PPARα | Preclinical | 115-116 |
| Ion Channels modulators | |||||||
|
Potassium K+ Channel Inhibitors |
Glipalamide |
 |
Melanoma, lung, stomach, and breast cancers |
Kv10.1, Kv10.2 (EAG2), and Kv11.1 channels | K channel (SUR). | Preclinical | 126-27 |
| Verapamil |
 |
Neuroblastoma and prostate cancer | K and Ca channels | T- and L-type Ca2+ channel antagonist | Preclinical | 126-127 | |
| Astemizole |  |
Various cancer cell lines | Kv10.1 | H1-antagonist | Preclinical | 126-127 | |
|
Calcium (Cav) Channel Blockers |
Mibefradil |  |
High-grade glioma tumors |
T-type Ca2+ channel | T and L-type Ca2+ channel | Phase 1b clinical trials | 130-131 |
| Nifedipine |  |
Colon cancer | PDL-1 | Calcium Channel | Preclinical | 99-101 | |
| Antibiotic | Bedaquiline |  |
Breast | Mitochondrial ATP-synthase | ATP synthase | Preclinical | 132-134,229 |
| Doxycycline (Tetracycline) |  |
Various cancer cell lines | AMPK-mediated mTOR, WNT/b-catenin, and PI3K/AKT | 30S ribosomal subunit | Preclinical | 84,135-136,142-145,226-228 | |
| Clofoctol |
 |
Various cancer cell lines | UPR pathway | bacterial protein synthesis | Preclinical | 137-138 | |
| Doxorubicin (Anthracyclines) |  |
Breast cancer | DNA intercalator | DNA intercalator | Approved | 139-141 | |
| Minocycline (Tetracycline) |
 |
Ovarian, breast cancer, glioblastoma | Cell cycle arrest, cyclins A, B, and E | Inhibit the 30S ribosomal subunit | Clinical trials | 142-142 | |
| Tigecycline (Tetracycline) |  |
Gliomas, myeloid leukemia, non-small cell lung cancer. |
Cell cycle arrest | Inhibit the 30S ribosomal subunit | Phase I trials for acute myeloid leukemia | 135-136,144-145,239-240 | |
| Ciprofloxacin (Fluoroquinolones) |
 |
leukemia, osteoblastoma, osteosarcoma, colon, bladder, and prostate cancers. | miRNA production | Inhibit bacterial gyrase | Preclinical | 146-147 | |
| Anti-Malarial | Chloroquine |
 |
Glioblastoma | Autophagy | Inhibits heme polymerase | Preclinical | 68-69,148-150 |
| Artesunate |
 |
Leukemia Kaposi’s sarcoma |
ROS production and apoptosis | Free radicals generation | Preclinical | 148 | |
| Mefloquine |
 |
Breast, leukemia, gastric, cervical, and colon cancers. | P-gp expression, production of ROS | Inhibits 80S ribosome | Preclinical | 148-150 | |
| Anti-Psychotic | Haloperidol |
 |
Pancreatic cancer | DRD2 | DRD2 | Preclinical | 151-153 |
| Penfluridol |  |
Pancreatic cancer | DRD2, autophagy, JAK2–STAT3 and ERK/AKT signaling pathways | DRD2 | Preclinical | 151-153 | |
| nonsteroidal anti-inflammatory drug (NSAID) | Diclofenac |
 |
Pancreatic cancer | Wnt/β-catenin signaling pathway | COXs | Preclinical | 154-155,172 |
| Celecoxib (selective COX-2 inhibitor) |
 |
Breast cancer | Wnt/β-catenin signaling pathway | COX-2 | Clinical trials | 142-143 | |
| disease-modifying antirheumatic drug (DMARD) | Auranofin |
 |
Various cancer types | TrxR, UPS system | redox enzymes | Phase I, and phase II | 156-157 |
| anti-epileptic | Oxcarbazepine |
 |
Various cancer types | cell cycle arrest, HDAC, PI3K-Akt-mTOR pathway | Na channel inhibitor | Preclinical | 158-159 |
| lacosamide |  |
Glioblastoma | CRMP2 | Na channel | Preclinical | 160-165 | |
| Lamotrigine |  |
brain tumors | N-, L-, and P-type Ca channels, 5-HT3 receptors. | Na+ channels | Preclinical | 164-165 | |
| anesthetic medications | ketamine |
 |
lung cancer ovarian cancer breast cancer hepatocellular carcinomas |
CD69, P57, glutathione peroxidase 4 | NMDA receptor | Preclinical | 57 |
| Propofol |  |
Squamous cell carcinoma | caspase and MAPK pathways | GABA receptors | Preclinical | 166-167 | |
Table 2.
Repurposed drugs for specific cancer type treatment with their chemical structure, old and new targets, and development status.
Table 2.
Repurposed drugs for specific cancer type treatment with their chemical structure, old and new targets, and development status.
| New Therapeutic Indication | Pharmacological Class | Drug Name | Chemical Structure | New Target | Original Target | Status | References |
|---|---|---|---|---|---|---|---|
| Prostate Cancer | Anti-Dyslipidemic Drugs | Atorvastatin (Statins) |
 |
Block cholesterol synthesis and androgen production | HMG-CoA reductase | Clinical trials | 52-54,168-169 |
| Antiarrhythmic Drugs | Digoxin |  |
Cell cycle topoisomerase II |
Na/K pump inhibition | Preclinical | 65-67,170-171 | |
| Ouabain |  |
Apoptosis by blocking the production of survivin and STAT3 | Na/K pump inhibition | Preclinical | 170-171 | ||
| Anti-Inflammatory Drugs | Indomethacin |  |
MYC gene family expression | Cyclooxygenases (COXs) | Preclinical | 172 | |
| Antidepressant Drugs | Sertraline |  |
Angiogenesis, metastasis, and autophagy | Selective serotonin reuptake inhibitor | Preclinical | 173 | |
|
Beta-Blockers |
Propranolol |  |
CREB1-EZH2-TSP1 pathway | Beta receptors | phase II trial | 174 | |
| Miscellaneous | Heparin |  |
Cytokine, adhesion molecule, and angiogenic factor expression | Antithrombin | Preclinical | 175 | |
| zoledronic acid |  |
G1 arrest, metastasis | osteoclast proliferation | Preclinical | 176-177 | ||
| Mifepristone |  |
suppressing over-expressed cell surface receptors in CRPC cells | Anti-progesterone | Preclinical | 176-177 | ||
| Rapamycin |  |
Binding to the FRB domain of mTOR, inhibiting mTORC1 | cytokine signaling | Preclinical | 55-56, 176-177, 204-206 | ||
| Gastric cancer (GC) | Antidepressant | Fluoxetine |  |
Inhibition of the endoplasmic reticulum stress marker (CHOP) | Serotonin reuptake inhibitor (SSRI) |
Preclinical | 178 |
| Paroxetine |  |
Enhanced DNA damage and reduced DNA repair | Preclinical | 178 | |||
| Antiepileptic | Valproic acid (VPA) |  |
HDAC1/PTEN/Akt signaling pathway | Na channel | phase II trial | 164-165,178-179 | |
| Antipsychotic | Risperidone |  |
Caspase 3, 8,9, ROS | Serotonin and norepinephrine reuptake inhibition | Preclinical | 180-181 | |
| Agents that chelate iron | Deferasirox |  |
NDRG1, mTOR and c-myc expression | Iron chelator/iron toxicity | Preclinical | 178,182 | |
|
Blood malignancies |
Antiemetic | Thalidomide |
 |
TNF-α | Immunomodulation | Approved | 183-186 |
| Tyrosine kinase inhibitor | Imatinib |  |
suppression of KIT kinase gastrointestinal stromal tumors (GISTs) | chronic myelogenous leukemia | approved | 187-190 | |
| Dasatinib |  |
Philadelphia chromosome-positive acute lymphoblastic leukemia (ALL) | chronic myeloid leukemia (CML) | Approved | 189-190 | ||
| Breast cancer | Antibiotic | Nitroxoline (NTX) |  |
anti-angiogenic activity, cathepsin B | chelation of divalent cations | Preclinical | 166,193 |
| Colon cancer | Antibiotic | Rapamycin |  |
mTOR pathway | mTOR pathway | Preclinical | 55-56,176-177,204-206 |
| Anti-Helminthic | Mebendazole (benzimidazole) |
 |
MYC pathway | Tubulin polymerization | Phase I and II clinical trials. | 68,76,200 | |
| Niclosamide |  |
Wnt/β-catenin cascade | Phase I clinical trials. | 201-203 | |||
| Hepatocellular carcinoma | Antipsychotic | Pimozide |  |
Apoptosis expression of STAT3 |
DRD2 | Preclinical | 207-209,245-248 |
| Antiarrhythmic | Amiodarone |  |
mTOR inhibitor | Na and K channels | Preclinical, meta-analysis | 210-211 | |
| Lanatoside C |  |
mitochondrial membrane potential (MMP), AKT/mTOR, PKCd | Na channel | Preclinical | 212-213 | ||
| Anti-microbe | Atovaquone |  |
p53 and p21, kinase-2 and H2AX | ETC at the bc1 complex | Preclinical | 214-214,230-231 |
Table 3.
Repurposed drugs for cancer treatment with their chemical structure, new indication, old and new targets, and development status.
Table 3.
Repurposed drugs for cancer treatment with their chemical structure, new indication, old and new targets, and development status.
| Targeted Mechanism |
Pharmacological Class | Drug Name | Chemical Structure | New Therapeutic Indication | Development Status | References |
|---|---|---|---|---|---|---|
| Mitochondrial energy metabolism | Anti-diabetic | Metformin (biguanides) |
 |
Colorectal, breast, pancreatic, prostate, lung, and cervical malignancies. | Phase II and III clinical trials. | 216-218 |
| Phenformin |  |
colorectal cancer | phase I | 219-220 | ||
| Canagliflozin |  |
prostate and lung cancer | Preclinical | 222-224 | ||
| Pioglitazone |  |
Breast, prostate, and colon cancer | Phase II trials. | 61-67, 222 & 224 |
||
| Anti-microbe | Bedaquiline |  |
Breast | Preclinical | 229 | |
| Ivermectin |  |
pancreatic and colorectal cancers. | Preclinical | 230-231 | ||
| Pyrvinium |  |
Pancreatic, colorectal, and breast cancers | phase I | 232-233 | ||
| Itraconazole |  |
Non-small cell lung cancer (NSCLC), prostate cancer, and basal cell carcinoma (BCC) | Phase II | 234-236 | ||
| ROS inducer | Antibiotic | Tigecycline |  |
hepatocellular carcinoma and acute myeloid leukemia |
phase I clinical trial for acute myeloid leukemia | 239-240 |
| Levofloxacin |  |
lung and breast cancer | Preclinical | 241-242 | ||
| Antiparasitic | Albendazole |  |
Ovarian, colorectal, and pancreatic cancers | phase I | 243-244 | |
| Antipsychotic | Pimozide |  |
Hepatocellular carcinoma | Preclinical | 245-248 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



