
Submitted:
28 October 2024
Posted:
31 October 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
In a series of publications, we attempt to demonstrate the prophylactic role of bromhexine hydrochloride (BHH) and the curative role of high colchicine doses against COVID-19. Effects of long-term prophylaxis with BHH are presented in two cases of elderly women with severe comorbidity. After long-term prophylactic use of BHH from 3 to 6 months, one does not get sick from COVID-19, and the other passes it almost asymptomatically, even though all their family members fall ill. The dramatic healing effect of colchicine was demonstrated in a family in which both spouses became ill with COVID-19 almost simultaneously. They are treated in different hospitals, and where colchicine is administered in high doses, the patient recovered. The other patient developed complications and died on standard treatment without high doses of colchicine. An outpatient accidentally overdosed on colchicine (12.5mg). The therapy was stopped immediately. Clinically, on the third day, there are absolutely no symptoms. These cases reaffirm the prophylactic effect of BRH and the curative effect of high-dose colchicine
Keywords:
COVID-19
; Bromhexine
; Colchicine
; Cytokine storm
; Prophylaxis
Introduction
More than 4.5 years since the start of the coronavirus disease 2019 (COVID-19) pandemic, despite the enormous expenditure of financial and intellectual resources, an effective treatment has not been found. The outpatient and hospital therapy proposed by the WHO is controversial, partially effective or downright harmful [1,2,3]. For years we have been trying to convince the scientific community that with the correct timing and dosage of bromhexine hydrochloride (BRH) and colchicine, the treatment problem is solvable [3,4,5,6,7,8,9,10,11,12].
We think that the effect of BRH is best when given continuously for prophylaxis during the next wave of COVID-19. BRH is also effective when given by inhalation for post-exposure prophylaxis, but when COVID-19 manifests itself clinically, the efficacy of BRH drops sharply because the virus is already in the cell [3,4,12]. Colchicine in high doses has a remarkable effect in inhibiting the cytokine storm (CS) and preventing multiorgan damage and death [3,4,5,6,7,8,9,10,11,12]. Colchicine is effective in outpatient and inpatient treatment, but only in high but safe doses. We have demonstrated this in a series of publications [3,5,6,8,12] and dramatic clinical cases [4,7,9,10,11].
In this case series, we show two cases of adults with major comorbidities receiving long-term prophylactic BRH; a family one treated with colchicine, the other without and an outpatient accidentally overdosed with colchicine, confirming our prophylactic and therapeutic regimen.
Prophylactic Role of BRH
The first case was a 77-year-old vaccinated woman with multiple comorbidities: Chronic kidney disease with acute decline October 2021 associated with pyelonephritis – some recovery in kidney function but not back to baseline; History of recurrent urinary tract infection; Hypertension 30 years ago; Pulmonary hypertension; Sjogren Larsson syndrome diagnosed 24 years ago; Rheumatoid arthritis III-IV X-ray grade; Hashimoto's thyroiditis; Breast malignancy 2018 – previous surgery under regular follow-up at the breast clinic; Peripheral vascular disease; Anemic syndrome; Cataracts; Uterovaginal prolapse with previous surgery; Multiple orthopaedic surgery hip/shoulder ongoing. From October 2021 she took BRH prophylactically for 6 months (3x1 tabl. per day). While staying in Bristol, UK with his daughter's family, he fell ill with COVID-19 in March 2022, proven by an antigen test. The symptoms are only mild irritation of the throat and nose. Without any treatment, after one week the antigen test was negative. At the same time, her daughter and son-in-law (both vaccinated), who did not take BRH, became ill and had severe COVID-19.
The second case concerns an 88-year-old unvaccinated woman, with comorbid hypertension and type II diabetes. She took prophylactic BRH (3x1 tabl. per day) for 4 months in 2021 and 3 months in 2022. She has never been sick with COVID-19, despite direct contact with her family members who have contracted the disease (in September, 2021).
The test done for Anti-SARS-CoV-2 IgG (ECLIA, Roche) on 01.12.2022 was 6.04 [BAU]/ml. It can only be assumed that after her family became ill, the woman developed anti-SARS-CoV-2 antibodies, which were detected 14 months later.
Life-Saving Effect of High-Dose Colchicine
The presented cases illustrate a family, consisting of a man and a woman, both infected with the SARS-CoV-2 virus, which led to complications of bilateral pneumonia in December 2020. The patients underwent treatment in two different healthcare facilities, each following distinct therapeutic regimens and resulting in varying clinical outcomes. Initially, both individuals exhibited symptoms of general fatigue and elevated temperature, with the man falling ill first, followed by his wife two days later.
Onset of the Disease
The man is a 64-year-old, weighing 93 kg, with comorbidities that include type 2 diabetes, which is managed with oral therapy (Metformin 2000 mg/day) and demonstrates good glycemic control, as evidenced by a last measured HbA1c of 6.4% taken ten days prior to the onset of symptoms. He also suffers from stage 2 arterial hypertension, treated with Nebivolol 5 mg/day and Amlodipine 10 mg/day. Notably, there is no history of underlying pulmonary diseases.
On the fifth day following the initial symptoms, he experienced a sudden deterioration, with oxygen saturation levels dropping to 91% and a persistent fever reaching 38°C. He consulted his family doctor, who performed a rapid antigen test for SARS-CoV-2, which returned positive. A chest X-ray was conducted, revealing an enlarged cardiac silhouette along with bilateral infiltrative changes in both lung bases, but without any pleural effusions (Figure 1).
Consequently, he was evaluated for hospitalization in a healthcare facility.
The therapy conducted in the hospital setting included the administration of Meropenem 3 times a day at 1.0 g intravenously, Metronidazole 2 times a day at 500 mg intravenously, Dexamethasone 2 times a day at 4 mg intravenously, Bromhexine 3 times a day at 4 mg orally, and Nadroparin 0.4 ml per day subcutaneously. Oxygen therapy was provided at 4 liters per minute via a nasal mask.
During the 3-day stay in the therapeutic department, the patient experienced worsening respiratory failure with increased oxygen requirements and deteriorating inflammatory marker values from laboratory tests. The lack of clinical improvement and the worsening overall condition necessitated the continuation of treatment in the intensive care unit.
Oxygen needs continued to rise, and the lack of effect from non-invasive ventilation therapy required the patient to be intubated and placed on invasive ventilation. The therapy included Meropenem 3 times a day at 1.0 g intravenously, Doxycycline 2 times a day at 100 mg intravenously, Nadroparin 2 times a day at 0.4 ml subcutaneously, Methylprednisolone 2 times a day at 60 mg intravenously, and Bromhexine 2 times a day at 4 mg intravenously (Table 1).
Table 1 Presents the laboratory results chronologically during the hospitalization period. Laboratory results demonstrated rising levels of inflammatory markers and worsening respiratory failure. Along with this, there was an increase in the values of D-dimer, Creatinine, LDH, ALAT, ASAT, ESR, blood glucose, and a reduction of lymphocytes in absolute number and percentage. Neutrophil-type leukocytes progressively increase.
A follow-up chest X-ray showed bilateral involvement of both lung halves with extensive ground-glass opacities affecting two-thirds of the lung parenchyma bilaterally, without evidence of pleural effusions (Figure 2).
Laboratory results were presented chronologically during the hospitalization period, demonstrating increasing values of inflammatory markers and worsening respiratory failure. Additionally, there was an increase in D-dimer and creatinine levels, very high elevation of the “deadly markers” LDH and CRP, along with a reduction in lymphocytes both in absolute numbers and percentage. Neutrophil type leukocytes progressively increased.
The patient died three days after being transferred to the intensive care unit.
The second patient is a 59-year-old woman weighing 60 kg, with no significant medical history. She visits her general practitioner accompanied by her husband and undergoes a rapid antigen test for SARS-CoV-2, which returns positive. The patient presents with asthenia, fatigue, and a fever reaching up to 38 degrees Celsius.
A chest X-ray (Figure 3) reveals bilateral interstitial pneumonia, prompting the decision for hospitalization.
She is admitted to a different healthcare facility than her husband. The initiated treatment plan includes:
Colchicine: 0.5 mg tablets—3 tablets three times on the first day (0.075mg/kg), then 1 tablet three times daily thereafter; Doxycycline: 200 mg IV twice daily; Methylprednisolone: 40 mg IV three times daily for the first three days, followed by 40 mg twice daily for two days, and then 40 mg IV daily for the next two days; Bromhexine: Inhalation of 4 mg in 1 ampoule three times daily, mixed with 2 ml of saline for the duration of her hospitalization; Nadroparin: 0.4 ml subcutaneously twice daily; Quamatel: 40 mg orally twice daily throughout her hospital stay.
Upon admission, the patient exhibited respiratory failure, which was addressed with oxygen therapy at 3 L/min via nasal cannula, maintaining an average oxygen saturation of 91%-93%. By the second day of hospitalization, the patient became afebrile, experiencing a significant reduction in subjective complaints of fatigue during routine physical activities, with no reports of dyspnea.
Laboratory tests performed during the treatment period, illustrated in Table 2, showed a decrease in inflammatory markers and lower levels of D-dimer. A follow-up chest X-ray taken on the seventh day of treatment, shown in Figure 4, indicated signs of improvement in the radiological findings. Based on these results, the patient was assessed as appropriate for discharge.
Table 2 Demonstrates a reduction in inflammatory markers over the treatment period. Neutrophil leukocytes reach normal values, lymphocytes increase in number and percentage reaching normal. D-dimer values from pathologically elevated values show a tendency towards normalization during the course of treatment. The values of oxygen saturation improve, reaching the norm without oxygen substitution. CRP values reach normal.
The two cases demonstrate the progression of disease due to SARS-CoV-2 viral pneumonia, with both patients showing a similar onset of initial symptoms. Neither patient has a history of pulmonary disease or has been on medications related to previous respiratory issues. Two distinct therapeutic regimens were implemented (with or without colchicine), leading to different therapeutic outcomes.
An Accidental Overdose of Colchicine Results in Immediate Recovery of the Patient
A 55 kg 42-year-old unvaccinated woman was with complaints of persistent fever up to 39°C, general fatigue, dry cough, muscle and joint pain. She was diagnosed with COVID-19 with an antigen test. At the time of the illness (September, 2021) the dominant variant of SARS-CoV-2 in Bulgaria was Delta. The woman is prescribed to take 5 tablets of colchicine on the first day. In addition, bromhexine 4 X 2 tablets was prescribed, doxycycline (2X1), antithrombotic therapy with clopidogrel, aulin (2X1) and nexium. Due to a misunderstanding, the patient took 5 tablets 5 times on the first day (12.5mg or 0.23mg/kg). On the second day, until the attending physician was called, she took another 3-4 tablets. The woman had diarrhea, more than 5 bowel movements. Colchicine was stopped immediately, as was any other therapy. Clinically, on the third day, there are absolutely no symptoms. She feels more lost. No diarrhea. On the 10th day, an X-ray was taken. The lung was clean. From the laboratory tests: ESR-22mm/h [1–20]; CRP-12mg/L [0–5]; Leukocytes - 8.9 X 109/L [3.5-10.5]; Ne% - Neutrophilic granulocytes - 76 [40–70]; D-dimer-0.6mg/L [0-0.55]; Alanine aminotransferase (ALAT)-34U/L [0–41]; Aspartate aminotransferase (ASAT)- 38U/L [0-40]; creatinine-76µmol/L [53-97.2]. Antigen test was negative.
Discussion
Our strategy to combat COVID-19 is to block Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) from entering the cell and to inhibit the hyperactivated nucleotide-binding oligomerization domain-like receptor containing pyrin domain 3 (NLRP3) inflammasome which is a central mediator of severe COVID-19 causing the CS, with subsequent multiorgan damage and death [3,12].
The principal SARS-CoV-2 cell entry (via plasma membrane) is related to the cell-surface transmembrane protease serine subtype 2 (TMPRSS2) which cleaves the spike protein leading to the fusion of the viral and host membranes [13]. BRH has a selective inhibitory effect on TMPRSS2, thus inhibiting the SARSCoV-2 entry into the cell [13,14,15]. BRH is most effective when taken prophylactically (Figure 5), because it blocks in advance the entrance of the SARS-CoV-2 to the cell [3]. Our two cases of elderly women with severe comorbidity who took BRH tabl. prophylactically for 3 to 6 months demonstrate just that. However, in the cases of post-exposure prophylaxis and manifestation of COVID-19, the time and method of administration (inhalations) are the leading factors for the successful action of BRH [3]. Positive results for the effect of BRH in post-exposure prophylaxis were reported [16,17]. Prevention of COVID-19 with cheap BRH can reduce illnesses, if any, they are mild, hospital admissions are reduced, the pandemic is contained and millions of lives can be saved [18].
The NLRP3 inflammasome plays a central role in the complications of COVID-19 [19]. If we want to save the severely ill COVID-19 patient, the hyperactivated NLRP3 inflammasome must be inhibited. Colchicine has the remarkable property of accumulating in white blood cells, where life-threatening CS develops [20]. Increasing doses of colchicine in these cells achieved the micromolar concentrations required to inhibit the NLRP3 inflammasome [3,12]. High doses of colchicine may be particularly helpful in treatment of COVID-19 obese or diabetic patients with higher metaflammation and NLRP3 activation [21]. Our results strongly support this view [9,10].
The case of the family affected almost simultaneously by COVID-19, is an eloquent and tragic example of the life-saving effect of high doses of colchicine. It should be strongly emphasized that the colchicine doses we use have been used in the past and are completely safe [3,6,8,12].
Not long ago we described an inpatient with COVID-19 pneumonia and pericardial effusion mistakenly took 15 mg of colchicine over 10 hours. Remarkably, this single overdose of colchicine, without any additional therapy, resulted in the complete recovery of bilateral pneumonia and pericardial effusion [7]. Two other outpatients took 12.5 mg/24h, their symptoms resolved within three days. In all three patients, a lower dyspeptic syndrome was observed, controlled with symptomatic medicines for 24 hours [7]. The case described by us is the fourth one with an accidental taken overdose of colchicine 12.5mg [0.23mg/kg]. Clinically, on the third day, there are absolutely no symptoms.
We do not recommend such doses, but these cases raise the question of whether, in particularly severe COVID-19, the maximum dose we give (0.045mg/kg) should be increased to 0.1mg/kg, which is below the threshold of intoxication [8,12].
The effectiveness of BRH is highly dependent on the timing of administration (Figure 5). It is most effective when given prophylactically, for more than 1 month. It can be very effective when taken immediately by inhalation for post-exposure prophylaxis. By the time symptoms are present, the virus has already entered the cell, but BRH can limit its spread. As an 3Clpro/Mpro protease inhibitor, it could inhibit SARS-CoV-2 replication. Its active demethylated metabolite, ambroxol, is a potent inducer of surfactant synthesis. In addition, BRH can support the healing process as cough suppressant, expectorant, mucolytic and anti-inflammatory agent thus reducing swelling and irritation in the respiratory tract. The timing of colchicine administration is also important, but the dose is decisive. Only high doses of colchicine could inhibit the NLRP3 inflammasome and prevent CS.
Acknowledgements
This study is financed by the European Union-NextGenerationEU, through the National Recovery and Resilience Plan of the Republic of Bulgaria, project № BG-RRP-2.004-0004-C01.
References
- Morgenstern, J. Paxlovid evidence: Still very little reason to prescribe. First10EM. 2024. [CrossRef]
- Sax, P. The Rise and Fall of Paxlovid—HIV and ID Observations. NEJM Journal Watch. 2024. Available online: https://blogs.jwatch.org (accessed on 3 June 2024).
- Mitev, V. Comparison of treatment of COVID-19 with inhaled bromhexine, higher doses of colchicine and hymecromone with WHO-recommended paxlovid, molnupiravir, remdesivir, anti-IL-6 receptor antibodies and baricitinib. Pharmacia. 2023, 70:1177-1193. [CrossRef]
- Mondeshki, T.; Bilyukov, R.; Tomov, T.; et al. Complete, rapid resolution of severe bilateral pneumonia and acute respiratory distress syndrome in a COVID-19 patient: role for a unique therapeutic combination of inhalations with bromhexine, higher doses of colchicine, and hymecromone. Cureus. 2022, 14:e30269. [CrossRef]
- Mitev, V.; Mondeshki, T.; Marinov, K.; et al. Colchicine, bromhexine, and hymecromone as part of COVID19 treatment - cold, warm, hot. Current Overview on Disease and Health Research. Khan BA (ed): BP International, London, UK; 2023, 10:106-13.
- Tiholov, R.; Lilov, AI.; Georgieva, G.; et al. Effect of increasing doses of colchicine on thetreatment of 333 COVID-19 inpatients. Immun Inflamm Dis. 2024, 12: e1273.
- Mondeshki, T.; Bilyukov, R.; Mitev, V. Effect of an Accidental Colchicine Overdose in a COVID-19 Inpatient With Bilateral Pneumonia and Pericardial Effusion. Cureus. 2023, 15:e35909. [CrossRef]
- Mitev, V. What is the lowest lethal dose of colchicine? Biotechnol & Biotechnol Equip. 2023, 37, 1:2288240. [CrossRef]
- Lilov, A.; Palaveev, K.; Mitev, V. High Doses of Colchicine Act As “Silver Bullets” Against Severe COVID-19. Cureus. 2024, 16:e54441. [CrossRef]
- Mondeshki, T.; Mitev, V. High-Dose Colchicine: Key Factor in the Treatment of Morbidly Obese COVID-19 Patients. Cureus. 2024, 16:e58164. [CrossRef]
- Bulanov, D.; Yonkov, A.; Arabadzhieva, E.; et al. Successful Treatment With High-Dose Colchicine of a 101-Year-Old Patient Diagnosed With COVID-19 After an Emergency Cholecystectomy. Cureus. 2024, 16:e63201. [CrossRef]
- Mitev, V. Colchicine—The Divine Medicine against COVID-19. J Pers Med. 2024, 14:756. [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020, 181:271–280. [CrossRef]
- Lucas, JM.; Heinlein, C.; Kim, T.; et al. The androgen-regulated protease TMPRSS2 activates a proteolytic cascade involving components of the tumor microen-vironment and promotes prostate cancer metastasis. Cancer Discovery. 2014, 4:1310–1325. [CrossRef]
- Depfenhart, M.; De Villiers, D.; Lemperle, G.; et al. Potential new treatment strategies for COVID-19: is there a role for bromhexine as add-on therapy? Intern Emerg Med. 2020, 15:801–812. [CrossRef]
- Tolouian, R.; Moradi, O.; Mulla, ZD.; et al. Bromhexine for post-exposure COVID-19 prophylaxis: A randomized, double-blind, placebo-controlled trial. Jundishapur J Microbiol. 2022, 15:e130198.
- Mikhaylov, EN.; Lyubimtseva, TA.; Vakhrushev, AD.; et al. Bromhexine hydrochloride prophylaxis of COVID-19 for medical personnel: A randomized open-label study. Interdiscip Perspect Infect Dis. 2022, 4693121. [CrossRef]
- Mitev, V.; Mondeshki, T.; Miteva, A.; et al. COVID-19 Prophylactic effect of Bromhexine Hydrochloride Preprints. 2024. [CrossRef]
- Freeman, TL.; Swartz, TH. Targeting the NLRP3 Inflammasome in Severe COVID-19. Front. Immunol. 2020, 11:1518. [CrossRef]
- Leung, YY.; Hui, LLY.; Kraus, VB. Colchicine—update on mechanisms of action and therapeutic uses. Semin Arthritis Rheum. 2015, 45:341-350. [CrossRef]
- Rabbani, AB.; Oshaughnessy, M.; Tabrizi, R.; et al. Colchicine and COVID-19: A Look Backward and a Look Ahead. Medical Research Archives. 2024, 12 (9).
Figure 1.
Radiographic data showing an enlarged cardiac shadow with bilateral investment changes in both lung bases without the presence of pleural effusions of first patient on the fifth day following the initial symptoms.
Figure 1.
Radiographic data showing an enlarged cardiac shadow with bilateral investment changes in both lung bases without the presence of pleural effusions of first patient on the fifth day following the initial symptoms.
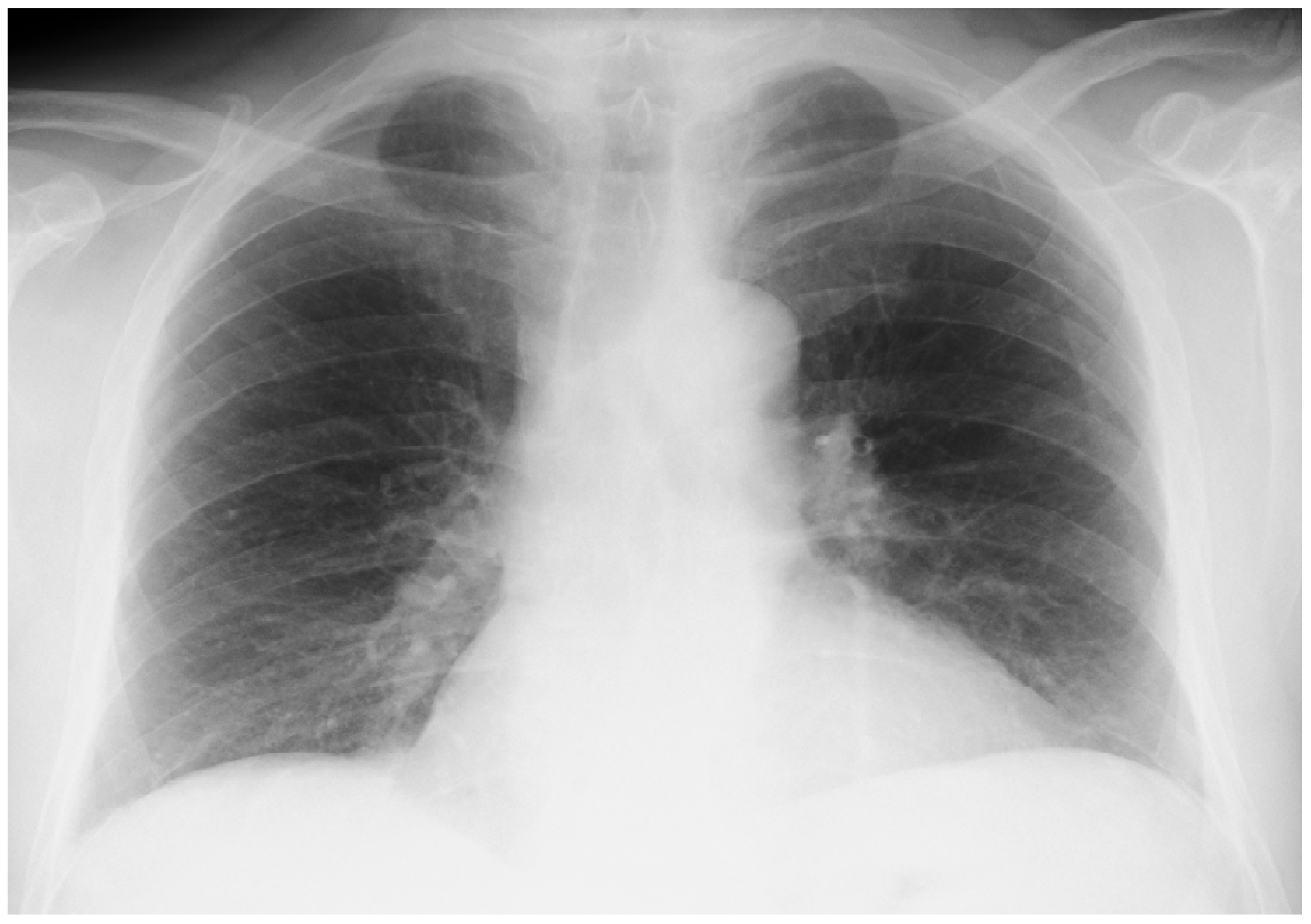
Figure 2.
Control X-ray examination and transaxial computed tomography of the chest (Chest CT) of the chest of first patient on day 5.
Figure 2.
Control X-ray examination and transaxial computed tomography of the chest (Chest CT) of the chest of first patient on day 5.
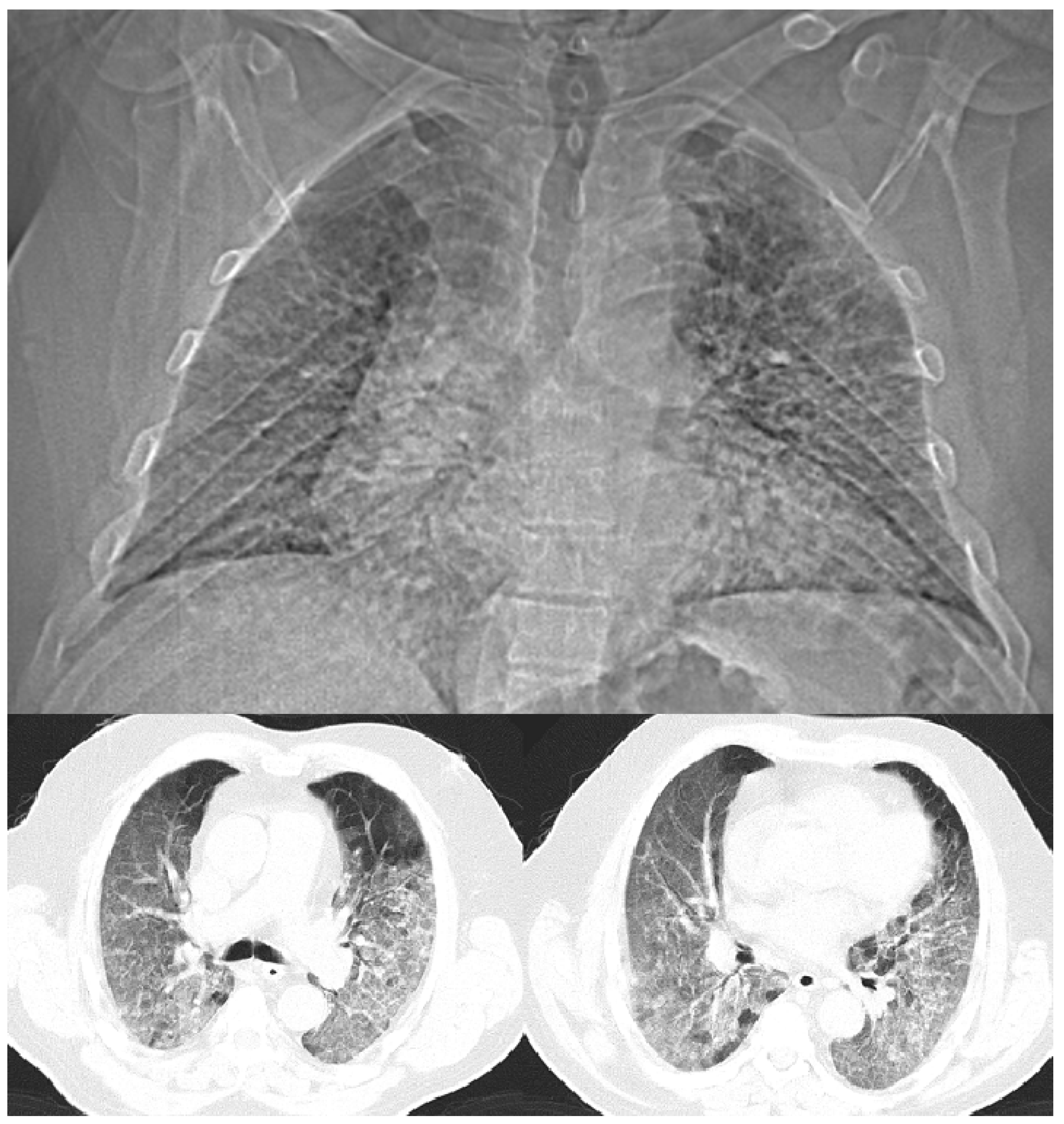
Figure 3.
An X-ray of second patient upon admission.
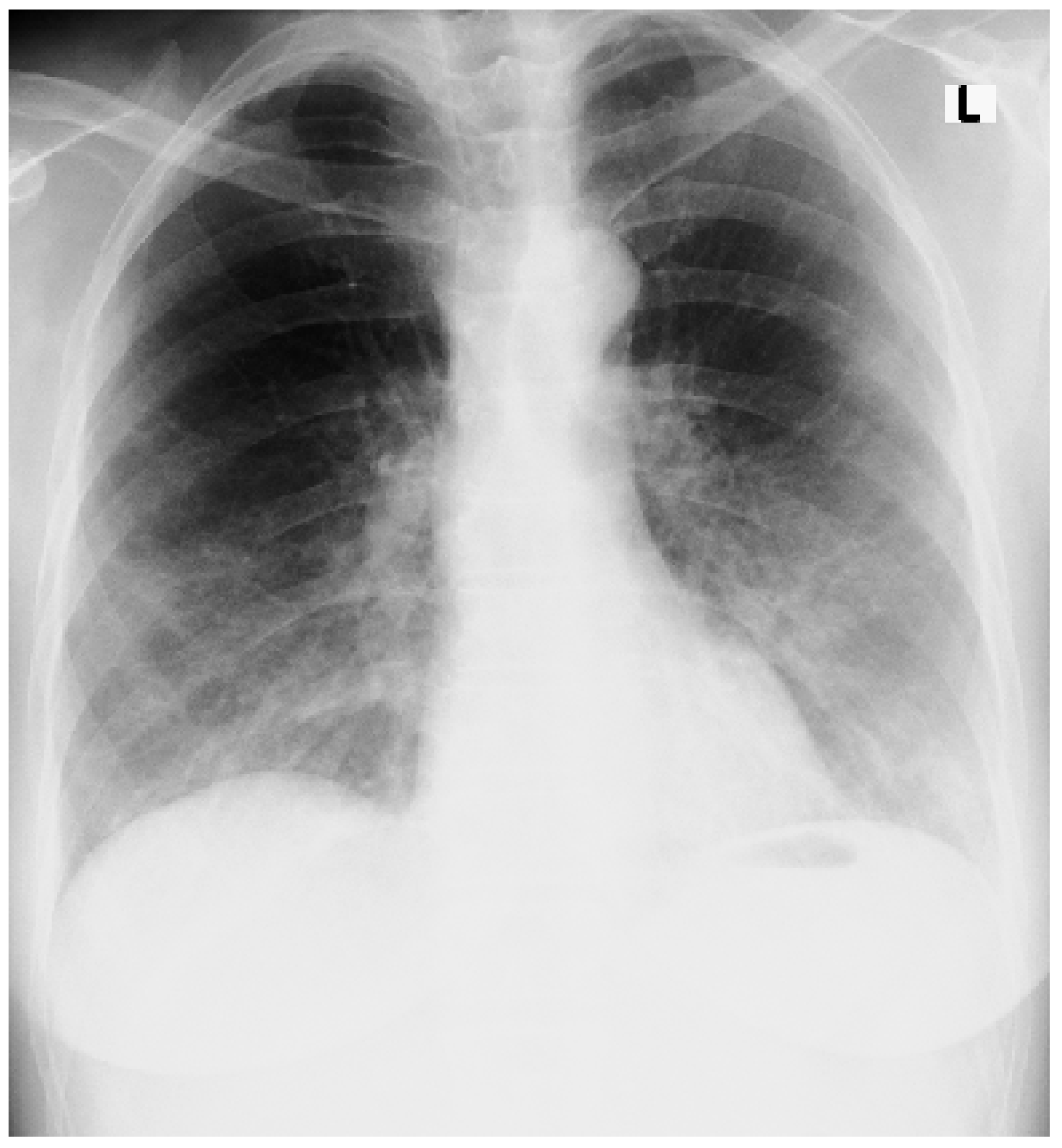
Figure 4.
Shows the control radiograph taken on the 7th day after the start of treatment of second patient, upon discharge from the hospital. Demonstrates the reverse development of the X-ray morphological changes, without the presence of pleural effusions.
Figure 4.
Shows the control radiograph taken on the 7th day after the start of treatment of second patient, upon discharge from the hospital. Demonstrates the reverse development of the X-ray morphological changes, without the presence of pleural effusions.
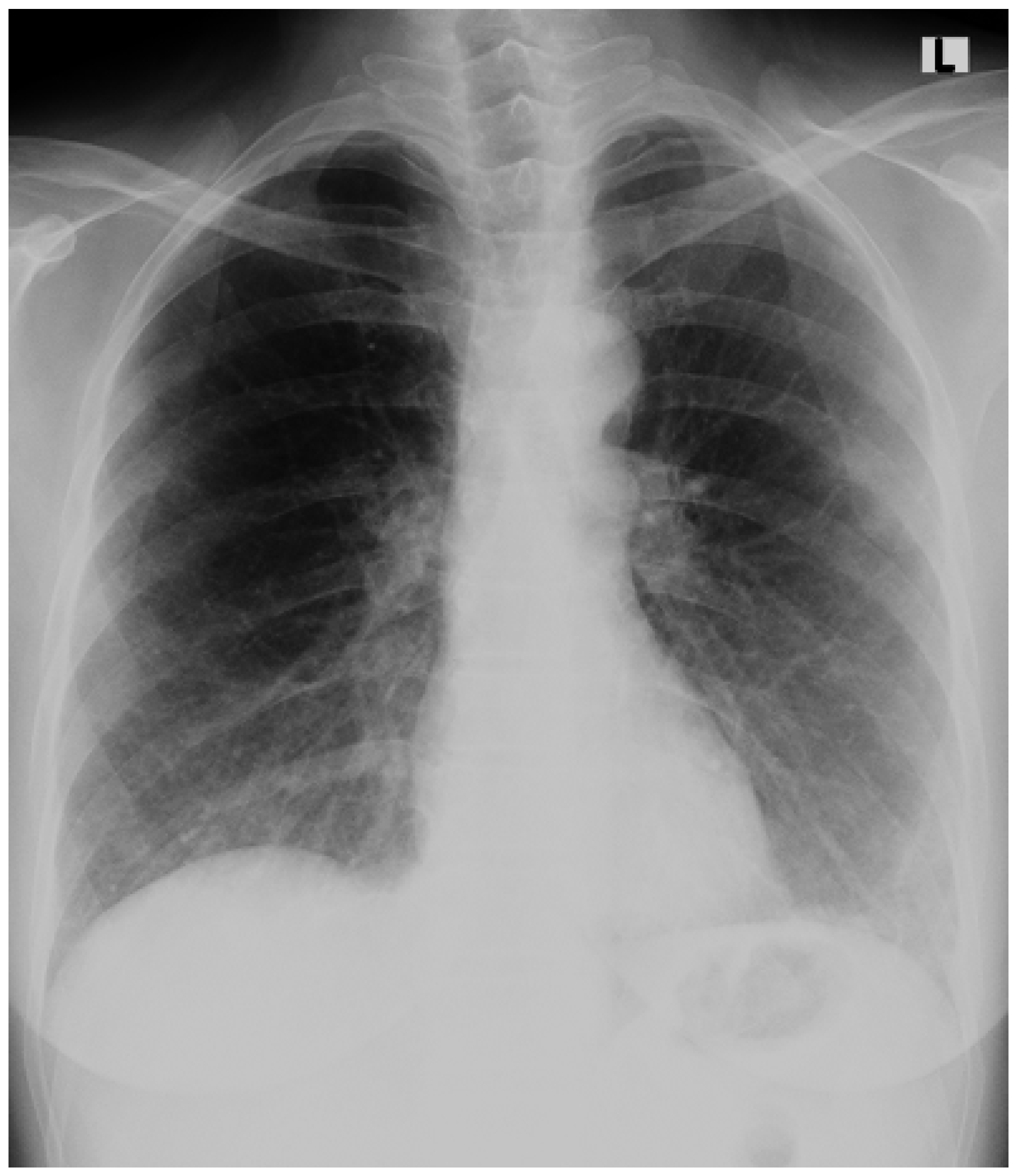
Figure 5.
Time and dose dependence for effective treatment of COVID-19 with BRH and colchicine.
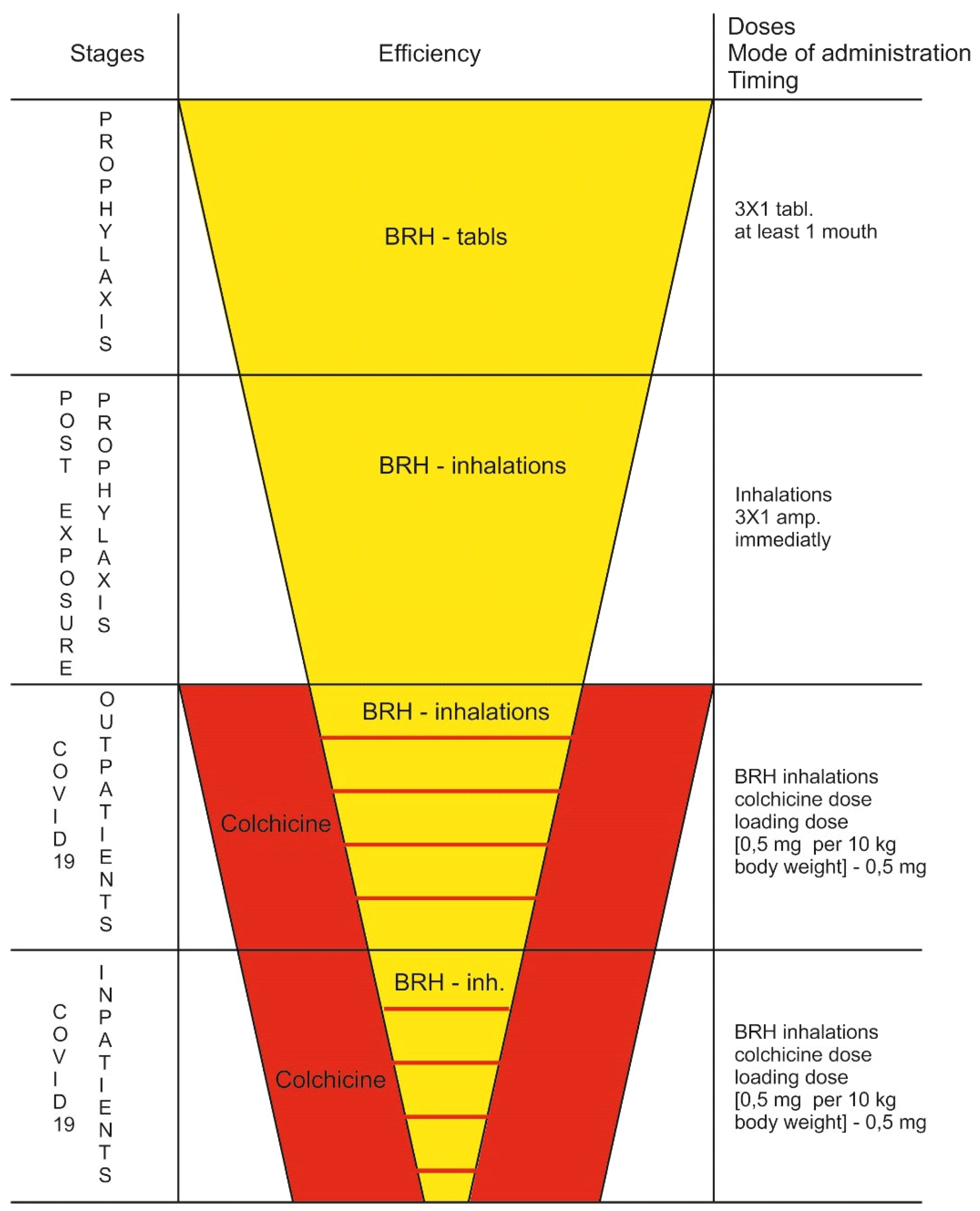

Table 1.
Laboratory results of first patient.
| Marker | Unit | Min. | Max. | Day 1 | Day 2 | Day 5 |
| 4751-PCR test for COVID-19 (SARS-CoV-2 RNA) | (+) positive | |||||
| Leukocytes (Leu) | 109/L | 3.5 | 10.5 | 5.0 | 5.7 | 8.8 |
| Erythrocytes (Er) | 1012/L | 4.4 | 5.9 | 4.8 | 4.7 | 5.1 |
| Hemoglobin (Hb) | g/L | 135 | 180 | 160 | 153 | 150 |
| Hematocrit (Ht) | g/L | 0.4 | 0.53 | 0.44 | 0.45 | 0.44 |
| MCV | fL | 82 | 96 | 91 | 87 | 88 |
| MCH | pg | 27 | 33 | 34 | 31 | 30 |
| MCHC | g/L | 300 | 360 | 366 | 356 | 345 |
| Platelets (Tr) | 109/L | 130 | 440 | 180 | 160 | 141 |
| NE % - Neutrophil granulocytes % | % | 40 | 70 | 82.9 | 84.6 | 88.2 |
| EO % - Eosinophilic granulocytes % | % | 0 | 6.5 | 0 | 0.0 | 0.0 |
| BA% - Basophilic granulocytes % | % | 0 | 2 | 1 | 0 | 0 |
| MO % - Monocytes % | % | 1 | 11 | 5 | 6 | 6 |
| LY % - Lymphocytes % | % | 20 | 48 | 11 | 9 | 5.2 |
| NE# -Neutrophil granulocytes-count | 109/L | 2 | 7 | 4.16 | 4.82 | 7.76 |
| ЕО# -Eosinophilic granulocytes-count | 109/L | 0 | 0.5 | 0.1 | 0.0 | 0.0 |
| BA# -Basophilic granulocytes-count | 109/L | 0 | 0.14 | 0.05 | 0 | 0.00 |
| MO# -Monocytes-count | 109/L | 0 | 0.8 | 0.25 | 0.34 | 0.53 |
| LY# -Lymphocytes-count | 109/L | 1 | 4 | 1.4 | 0.51 | 0.46 |
| IG (%) - Immature granulocytes - % | % | 0 | 5 | 0.1 | 0.4 | 0.6 |
| IG # - Immature granulocytes - count | 109/L | 0 | 0.7 | 0.0 | 0.02 | 0.0 |
| D-dimer | μg/L | 0 | 0.55 | 1.2 | 2.1 | 3.1 |
| Creatinine - serum | μmol/L | 62 | 106 | 196 | 201 | 210 |
| pH | 7.35 | 7.45 | 7.4 | 7.45 | 7.3 | |
| pCO2 | kPa | 4.67 | 6 | 3.5 | 4.11 | 3.9 |
| pO2 | kPa | 10 | 13 | 6.75 | 5.6 | 5.2 |
| SB | mmol/L | 21 | 25 | 20.5 | 23.7 | 28 |
| BE (w) | mmol/L | -2.5 | 2.5 | -3.3 | 4.1 | 5.1 |
| O2 Sat | % | 94 | 98 | 91 | 60 | 55 |
| tCO2 | mmol/L | 20 | 27 | 19.5 | 21.5 | 25 |
| CRP | mg/L | 0 | 5 | 56 | 148.1 | 231 |
| LDH | E/L | 140 | 370 | 577 | 1893 | 2012 |
| ESR | mm/h | 0 | 20 | 92 | ||
| ALAT | U/L | 0 | 40 | 66 | 84 | 102 |
| ASAT | U/L | 0 | 40 | 56 | 68 | 83 |
Table 2.
Laboratory results of second patient.
| Marker | Unit | Min. | Max. | Day 1 | Day 4 | Day 8 |
| 4751-PCR тест за COVID-19 (SARS-CoV-2 RNA) | (+) positive | (-) negative | ||||
| Leukocytes (Leu) | 109/L | 3.5 | 10.5 | 7.8 | 8.1 | 9.2 |
| Erythrocytes (Er) | 10^12/L | 4.4 | 5.9 | 4.8 | 4.9 | 4.7 |
| Hemoglobin (Hb) | g/L | 135 | 180 | 123 | 121 | 120 |
| Hematocrit (Ht) | g/L | 0.4 | 0.53 | 0.39 | 0.41 | 0.4 |
| MCV | fL | 82 | 96 | 81 | 82 | 85 |
| MCH | pg | 27 | 33 | 26 | 28 | 27 |
| MCHC | g/L | 300 | 360 | 315 | 324 | 315 |
| Platelets (Tr) | 109/L | 130 | 440 | 316 | 340 | 354 |
| NE % - Neutrophil granulocytes % | % | 40 | 70 | 78.4 | 74.9 | 62 |
| EO % - Eosinophilic granulocytes % | % | 0 | 6.5 | 2.1 | 0.0 | 0.0 |
| BA% - Basophilic granulocytes % | % | 0 | 2 | 1 | 0 | 0 |
| MO % - Monocytes % | % | 1 | 11 | 7.1 | 8 | 10.5 |
| LY % - Lymphocytes % | % | 20 | 48 | 11 | 15.9 | 26 |
| NE# -Neutrophil granulocytes-count | 109/L | 2 | 7 | 6.12 | 6 | 5.7 |
| ЕО# -Eosinophilic granulocytes-count | 109/L | 0 | 0.5 | 0.16 | 0.0 | 0.0 |
| BA# -Basophilic granulocytes-count | 109/L | 0 | 0.14 | 0.08 | 0.01 | 0.00 |
| MO# -Monocytes-count | 109/L | 0 | 0.8 | 0.55 | 0.65 | 0.96 |
| LY# -Lymphocytes-count | 109/L | 1 | 4 | 0.86 | 1.28 | 2.39 |
| IG (%) - Immature granulocytes - % | % | 0 | 5 | 0.4 | 1.2 | 1.5 |
| IG # - Immature granulocytes - count | 109/L | 0 | 0.7 | 0.0 | 0.1 | 0.14 |
| D-dimer | μg/L | 0 | 0.55 | 1.5 | 1.1 | 0.85 |
| Creatinine - serum | μmol/L | 62 | 106 | 89 | 95 | 82 |
| pH | 7.35 | 7.45 | 7.4 | 7.41 | 7.39 | |
| pCO2 | kPa | 4.67 | 6 | 4.1 | 4.5 | 4.5 |
| pO2 | kPa | 10 | 13 | 7.8 | 8.1 | 8.4 |
| SB | mmol/L | 21 | 25 | 20.5 | 24 | 25 |
| BE (w) | mmol/L | -2.5 | 2.5 | 2.8 | 2.5 | 2.3 |
| O2 Sat | % | 94 | 98 | 91 | 92 | 94 |
| tCO2 | mmol/L | 20 | 27 | 23 | 25 | 24 |
| CRP | mg/L | 0 | 5 | 22 | 15 | 9 |
| LDH | E/L | 140 | 370 | 572 | 511 | 480 |
| ESR | mm/h | 0 | 20 | 40 | 22 | |
| ALAT | U/L | 0 | 40 | 45 | 41 | 42 |
| ASAT | U/L | 0 | 40 | 35 | 32 | 38 |
| blood glucose | mmol/L | 3.9 | 5.6 | 5.5 | 6.5 | 5.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



