
Submitted:
29 October 2024
Posted:
31 October 2024
You are already at the latest version
Abstract
Background: Since the introduction of the SLICC criteria in 2012, biopsy-proven lupus nephritis (LN) has been the only independent diagnostic criterion for systemic lupus erythematosus (SLE). This was reaffirmed by the EULAR/ACR in 2019, emphasizing the importance of renal biopsy in LN. However, the current classification lacks specific histopathological criteria for defining LN. This study describes the histological findings of patients with LN, compares them with those of other glomerular diseases, and evaluates their diagnostic accuracy. Methods: This retrospective cohort included 731 kidney biopsies. The patients were divided into two groups: a LN group and a control group comprising patients with membranous nephropathy, IgA nephropathy, membranoproliferative glomerulonephritis, pauci-immune glomerulonephritis, and proliferative glomerulonephritis. Sensitivity and specificity analyses were conducted for various histopathological features. Results: We identified five features strongly correlated with LN: mesangial proliferation, subendothelial deposits, C1q staining ≥ 1+, dominant IgG, and ≥ 4 positive immunofluorescence elements. Combined, these features yielded an area under the ROC curve of 0.94 (95% CI: 0.91–0.95). In membranous nephropathy, histological features such as mesangial deposits, C1q positivity, and ≥ 4 positive immunofluorescence elements effectively distinguished class V LN from non-lupus membranous nephropathy, with an area under the ROC curve of 0.85 (95% CI: 0.76–0.93). Conclusion: The combination of mesangial proliferation, subendothelial deposits, C1q staining ≥1+, dominant IgG, and ≥ 4 positive immunofluorescence elements offer good accuracy for diagnosing renal involvement in SLE. In the absence of pathognomonic features, combined criteria are valuable diagnostic tools, particularly when other SLE criteria are lacking.
Keywords:
lupus nephritis
; systemic lupus erythematosus
; renal biopsy
; histopathologic features
; glomerular diseases
1. Introduction
Lupus nephritis (LN) is one of the most severe manifestations of systemic lupus erythematosus (SLE) [1,2,3]. It is considered the leading secondary cause of glomerular diseases, excluding diabetic nephropathy [4,5,6,7]. The SLE behavior differs across different populations according to ethnicity and geographical distribution, and renal involvement occurs more frequently and with worse outcomes in non-Caucasian populations, resulting in a higher progression to end-stage renal disease (ESRD) [2,8]. More than 25% of patients with severe LN are expected to progress to ESRD after 20 years [1,3,9].
Several updates have been made since the first World Health Organization (WHO) LN classification in 1974, the most recent being by the International Society of Nephrology/Renal Pathology Society (ISN/RPS) in 2003 [10,11]. Nonetheless, renal biopsy cannot be used in isolation for the diagnosis of SLE, it must be interpreted within the appropriate clinical context, including serological markers.
Formerly, LN was diagnosed by demonstrating proteinuria > 500 mg/day or 3+ and abnormal cylindruria in a patient meeting at least four of the eleven American College of Rheumatology (ACR) criteria [12,13]. In 2012, the Systemic Lupus International Collaboration Clinics (SLICC) established that biopsy-confirmed renal involvement alone was definitive for SLE without needing additional criteria [14]. In 2019, the ACR and the European League Against Rheumatism (EULAR) introduced a new classification confirming the renal criterion, albeit with differences from SLICC. LN class II or V contributes 8 points and class III or IV contributes 10 points, which is sufficient to diagnose SLE [15,16]. However, none of the histopathological findings are sufficiently specific to definitively ascertain LN.
Certain histological findings strongly suggest LN. The full-house staining is one of the most common histopathological characteristics associated with LN, as well as strong immunofluorescence C1q staining. Other suggestive characteristics include tissue antinuclear factors in immunofluorescence, tubuloreticular inclusions in electron microscopy, extraglomerular deposits in immunofluorescence and/or electron microscopy, and combined subepithelial and subendothelial deposits [17,18,19].
This study aimed to describe the histological findings in LN biopsies and compare them with those of other glomerular diseases presenting similar clinical features. The objective of this study was to identify the histopathological findings most specific to LN in an ethnically diverse population.
2. Materials and Methods
2.1. Population and Sampling
This retrospective, observational cohort study focused on individuals aged > 14 years who underwent renal biopsy at two major nephrology referral centers of Brazil’s public health system, both associated with public universities: Hospital Ana Nery (HAN), affiliated with the Federal University of Bahia in Salvador, Bahia, and Hospital das Clínicas of the University of São Paulo Medical School (HCFMUSP) in São Paulo, São Paulo.
All individuals who underwent renal biopsy between January 2015 and December 2019 at HCFMUSP and between January 2014 and December 2020 at HAN with a reported diagnosis of LN, IgA nephropathy, membranous nephropathy, pauci-immune glomerulonephritis, membranoproliferative glomerulonephritis, crescentic and/or necrotizing glomerulonephritis, or proliferative glomerulonephritis (mesangial, focal, diffuse, or unspecified) were included in the study. The exclusion criteria were renal biopsies with insufficient material, inconclusive results, or diagnoses of diabetic nephropathy, thrombotic microangiopathy, minimal change disease, focal segmental glomerulosclerosis, isolated tubulointerstitial nephropathy, and hereditary nephropathy. If a patient had more than one biopsy, the second was excluded unless the first was inconclusive or lacked sufficient material, in which case only the second biopsy was included. Patients were classified as LN if they met the SLICC 2012 and/or ACR/EULAR 2019 criteria.
2.2. Data Assessment
Renal biopsies were indicated by the attending nephrologists according to the commonly recommended indications and personal experience. For HAN, the fragments for optical microscopy were placed in an acidic alcoholic formalin container. At HCFMUSP, some specimens were stored in Duboscq Brasil solution, while others were stored in formalin. Fragments for immunofluorescence microscopy were transported in 0.9% sodium chloride solution at 4-8°C, embedded in Tissue-Tek O.C.T. compound, frozen in liquid nitrogen, sectioned in a cryostat, and incubated with antibodies against IgA, IgG, IgM, kappa, lambda, C3, C1q, and fibrinogen. Electron microscopy is not routinely performed by either service. All HAN samples were analyzed by the same pathologist at the Gonçalo Moniz Research Centre of Fiocruz-BA, and those from HCFMUSP were analyzed by a team of pathologists from the Pathology Division.
The principal investigator collected data from reports provided by pathology services and medical records at both research sites, using a data collection instrument. The following histological variables were analyzed: histopathological diagnosis; mesangial proliferation; endocapillary hypercellularity; cellular, fibrocellular, and fibrous crescents; mesangial, subendothelial, subepithelial, tubular, vascular, and extraglomerular deposits; immunofluorescence positivity and intensity for IgA, IgG, IgM, C3, C1q, kappa, lambda, and fibrinogen with any result from trace (±) onwards considered positive; global glomerulosclerosis, tubular atrophy, and interstitial fibrosis; and acute and chronic vascular changes. The immunofluorescence pattern was considered ’full house’ when positivity for IgA, IgG, IgM, C3, and C1q was observed.
2.3. Statistical Analysis
The patients were divided into the reference LN group and a control group of non-SLE cases. Qualitative variables are expressed as absolute frequencies and proportions. Numerical variables not normally distributed were summarized as medians and interquartile ranges.
Logistic regression analyses were performed to identify the histopathological characteristics associated with LN. The sensitivity, specificity, accuracy, positive and negative predictive values, and positive and negative likelihood ratios were analyzed for each correlated factor. The same tests were conducted to assess the accuracy of differentiating class V LN from non-lupus membranous nephropathy. Multivariate analysis was performed to identify features independently correlated with LN, followed by multinomial logistic regression to determine the best combination of histopathological elements with high accuracy. These analyses were used to construct the receiver-operating characteristic (ROC) curves. All analyses were conducted using R software (version 4.2.2) with 95% confidence intervals (CIs).
The researchers followed local ethics guidelines for human research. The project was approved by the ethics committees of Hospital Ana Nery in Salvador and Hospital das Clinicas at the University of São Paulo Medical School. As this was a retrospective observational study, an exemption from obtaining informed consent was requested and granted. The researchers also signed a confidentiality agreement for the information obtained from medical records and renal biopsy reports.
3. Results
A total of 731 patients were included: 488 from the HCFMUSP and 243 from the HAN. The LN group comprised 433 patients: 269 from the HCFMUSP and 164 from the HAN. The control group comprised 298 individuals: 219 from HCFMUSP and 79 from HAN.
3.1. HCFMUSP Population
3.1.1. General Characteristics
Patients with LN at HCFMUSP were younger (median age 31.5 years) and predominantly female (84.8%). Most patients were white, but the LN group had a higher proportion of black and mixed-race individuals (24.9%). The control group was older (median age, 44 years) and included more men (55.2%). Patients in the LN group had better renal function, with a median baseline creatinine level of 1.00 mg/dL compared to 1.96 mg/dL in the control group. Proteinuria and hemoglobin, albumin, and cholesterol levels differed slightly between the groups (Table 1).
3.1.2. Histological Diagnosis
The most prevalent histological class of LN was the diffuse form (class IV), accounting for 38.7% of the histopathological reports, followed by the focal (class III) and membranous (class V) forms, both accounting for 17.1% of cases (Table S1). In the control group, IgA nephropathy was the most prevalent diagnosis (40.2%), followed by membranous nephropathy (21.5%), pauci-immune glomerulonephritis (14.6%), membranoproliferative glomerulonephritis (including C3 glomerulopathy) (14.3%), and proliferative glomerulonephritis (9.6%) (Table S2).
3.1.3. Optical Microscopy - HCFMUSP
Mesangial proliferation was found in 88.8% of the LN biopsies and in 63.9% of the control group. Endocapillary hypercellularity was present in 64% and 36.5% of patients in the LN and control groups, respectively. Cellular and/or fibrocellular crescents appeared in 53.8% of the LN biopsies and 33.8% of the controls. Interstitial fibrosis and tubular atrophy (IF/TA) percentages were similar to global glomerulosclerosis among the groups. A high degree of chronicity, defined as global glomerulosclerosis and/or IF/TA > 50%, was observed in 11.4% of LN biopsies, and 18.1% of the control group. Acute vascular changes were noted in 14.5% of patients with LN and 12.8% of the controls, while chronic vascular changes occurred in 67.7% and 74.4% of the patients, respectively (Table S3).
3.1.4. Characterization of Immune Deposits - HCFMUSP
Mesangial, subendothelial, and subepithelial deposits were present in 87.3%, 73.8%, and 49.2% of LN biopsies and 77.8%, 24.2%, and 23.5%, in the control group, respectively. Combined subepithelial and subendothelial deposits occurred in 29.8% of the LN cases and only 1.8% of the controls. Extraglomerular deposits were present in 15.7% and 2.8% of the LN and control groups, respectively. Tubulointerstitial deposits were scarce, but more frequent in the lupus nephritis group (Table 2).
In LN, IgG was positive in 97.6% of cases, followed by C3 (91.5%). In the control group, C3 was the most prevalent (75.5%), followed by lambda (64.9%), and IgA (49.0%). Full-house staining was found in 36.8% of the LN cases and in only 3.8% of the control group. By removing the requirement for IgA or IgM, prevalence increased to 71.3% in LN and 6.2% in control groups. When considering the positivity of at least four of the five immunofluorescence elements indiscriminately, the prevalence in LN increased to 75.7% and to 10.7% in the control group. LN showed dominant IgG staining in 91.5% of patients compared to 32.5% in the control group. C1q staining ≥1+ was found in 79.4% of LN and 11.1% in the control group.
3.1.5. Histopathological Features Diagnostic Performance - HCFMUSP
Table 3 presents the sensitivity and specificity of histopathological features. Mesangial proliferation had 89% sensitivity and 36% specificity and endocapillary hypercellularity had 64% and 63% for lupus nephritis. The mesangial area was the most frequent deposition site in lupus nephritis, with 87% sensitivity, followed by the subendothelial area, with 74% sensitivity and 76% specificity. Extraglomerular and combined subendothelial and subepithelial deposits showed very high specificity (97% and 98 %, respectively) but low sensitivity. The immunofluorescence elements that best correlated with lupus nephritis were IgG and C1q. Although IgG showed the highest sensitivity (98%), C1q showed the highest specificity (82%). IgG staining as a dominant or co-dominant element improved the specificity from 60% to 67%. C1q ≥1+ increased its specificity from 82% to 89% and reduced its sensitivity from 87% to 79%. The full-house pattern showed 37% sensitivity and 96% specificity. When considering the positivity of the four elements with IgG, C3, and C1q as requirements and IgA or IgM as a fourth positive element, the sensitivity was 71% and specificity was 94%. However, the most balanced performance was obtained when considering positivity for four elements indiscriminately, with 76% sensitivity and 89% specificity.
3.1.6. LN Histopathological Criteria Combination - HCFMUSP
Mesangial proliferation, subendothelial deposits, C1q positivity ≥1+, dominant or co-dominant IgG, and four or more positive elements in immunofluorescence remained independently related to the diagnosis of LN in multivariate analysis. Table 4 shows the sensitivity and specificity values for one or more combined histopathological elements. The best performance was found for a combination of three or more factors, with 91% sensitivity and 87% specificity, and four or more factors, with 74% sensitivity and 96% specificity. The area under the ROC curve for these five histopathological features in distinguishing LN from non-lupus nephropathy was 94%. (Figure 1)
3.1.7. Criteria for Differentiating Class V LN and Non-Lupus Membranous Nephropathy - HCFMUSP
The factors correlated with lupus membranous nephropathy in the univariate analysis are presented in Table 5. Mesangial proliferation showed 68% sensitivity and 60% specificity, whereas mesangial deposits showed 76% sensitivity and 58% specificity. The immunofluorescence elements correlating with LN were IgA, IgM, and C1q, with 76% sensitivity. IgA showed the highest specificity (82%). C1q positivity ≥1+ increased specificity to 82%. Full-house staining showed 22% sensitivity and 93% specificity, and positivity for four factors (IgG, C3, and C1q with IgA or IgM) increased the sensitivity to 57%. The best performance was found when considering the positivity for four elements indiscriminately, with 61% sensitivity and 91% specificity. Three factors remained in the multivariate analysis: mesangial deposits, C1q positivity, and four or more positive elements in immunofluorescence. The best performance occurred with a combination of two or more factors, with 76% sensitivity and 89% specificity (Table S4). The area under the ROC curve was 85% (Figure S1).
3.2. HAN Population
3.2.1. Histopathological Features Diagnostic Performance - HAN
The general characteristics and distribution of histopathological diagnoses of the HAN population are provided in the Supplementary Appendix. Table 6 presents the sensitivity and specificity values of the histopathological elements for distinguishing LN from non-lupus glomerulopathy. Mesangial proliferation and endocapillary hypercellularity had sensitivity values of 69% and 74% and specificity values of 43% and 61%, respectively. Mesangial, subendothelial, and subepithelial deposits had sensitivities of 70%, 74%, and 49%, and specificities of 36%, 58%, and 55%, respectively. Extraglomerular deposits and combined subendothelial and subepithelial deposits had high specificity (90% and 100%, respectively) but low sensitivity. IgG staining showed a sensitivity of 96% and a specificity of 35%. C1q showed a sensitivity of 69% and a specificity of 77%. Dominant or co-dominant IgG improved its specificity to 48% but reduced its sensitivity to 85%. C1q ≥1+ positivity increased its specificity to 83% and reduced its sensitivity to 64%. Full-house staining showed 40% sensitivity and 97% specificity. IgG, C3, and C1q as requirements, and IgA or IgM as the fourth positive element had 58% sensitivity and 94% specificity. When considering positivity for four elements indiscriminately, the sensitivity was 64% and the specificity was 80%.
3.2.2. LN Histopathological Criteria Combination - HAN
Subendothelial deposits, C1q positivity ≥1+, dominant or co-dominant IgG, and four or more positive elements in immunofluorescence remained independently related to LN and were selected for combined analysis. The sensitivity and specificity analyses for the combined elements are presented in Table 7. The best performance was achieved when two or more positive factors were combined, with 85% sensitivity and 65% specificity, and when three or more factors were combined, with 66% sensitivity and 92% specificity. Figure 2 shows an area under the ROC curve of 86%.
4. Discussion
We described the histopathological findings of patients with LN from two nephrology referral centers and compared them with those of patients with other glomerular diseases that can mimic LN. The data were presented separately because of differences in clinical profiles and histopathological methods between the centers. The HAN population served as a validation cohort for data from the HCFMUSP, with a socially and ethnically diverse sample. São Paulo ranks first in per capita income among Brazilian states, with 57.8% of its population declaring themselves as white in the last census. Bahia ranks 23rd out of 26 states in terms of income, with 79.7% of its population declaring themselves black [20].
Various histopathological features are associated with LN. At HCFMUSP, features showing better diagnostic performance included: mesangial proliferation, subendothelial deposits, C1q staining ≥1+, dominant IgG, and four or more positive elements in immunofluorescence. Individually, they exhibited sensitivity values between 74% and 92%, and specificity values between 36% and 89% for LN. The area under the curve (AUC) was 94% when combined and plotted on a ROC curve. Similar analyses were conducted for HAN, with findings largely consistent with those from HCFMUSP, except for mesangial proliferation. While mesangial proliferation showed a near-significant association in univariate analysis (p = 0.07), it did not remain significant in the multivariate analysis. The small sample size of the HAN population may have influenced the number of elements retained in the combined analysis. Despite these differences, the results were similar, strengthening the purpose of validation.
Few studies have defined LN based on histological findings. Kudose et al. identified intense C1q staining, full-house staining, tubuloreticular inclusions, extraglomerular deposits, and combined subepithelial and subendothelial deposits as significant features of lupus. Their specificities ranged from 80% to 96%, sensitivities from 68% to 80%, and the ROC curve to differentiate LN from other diagnoses had an AUC of 96% [18]. Albeit with differences, two criteria described by Kudose are similar to our study: intense C1q staining is a variation of the staining ≥1+ used in this cohort, and full-house was modified in our analysis to four or more positive elements in immunofluorescence. Both changes should be regarded as refinements that improve their performance as a diagnostic criterion. Extraglomerular deposits and combined subepithelial and subendothelial deposits were analyzed showing high specificities (97% and 98% in HCFMUSP and 100% and 90% in HAN). However, their low sensitivities (16% and 30% in HCFMUSP and 33% and 24% in HAN) limit their use as valid histological criteria. Tubuloreticular inclusions were not evaluated in this cohort because of the lack of routine electron microscopy.
Full-house staining is highly suggestive of LN; even considering lupus-like synonyms by many authors [21]. We found a low sensitivity for this feature in both populations (37% for HCFMUSP and 40% for HAN). However, in the study by Kudose et al., the sensitivity was 71%. On the other hand, we found 96% specificity for HCFMUSP and 97% specificity for HAN, which is similar to that previously described (90% in Kudose) [18]. In our study, selecting positivity for four or more elements in the final model provided a better balance between sensitivity and specificity, with comparable accuracy. The full-house pattern’s association with LN has been reinforced by various authors over decades, but it remains essential to exclude other primary and secondary causes before establishing a diagnosis of idiopathic full-house nephropathy [22,23,24].
In the absence of a published consensus, the categorization of a biopsy as LN by a nephropathologist depends on a combination of clinical history, laboratory evaluations and histological features. Ahmed et al. used a combination of the following criteria to classify a biopsy as lupus-like: 1) full-house staining in immunofluorescence with at least 1+ intensity, 2) tubuloreticular inclusions on electron microscopy, and 3) extraglomerular immune deposits with IgG and/or C1q [19].
Lupus membranous nephropathy differs clinically and histologically from the so-called "proliferative" forms [10]. Histological features accurate for LN did not exhibit the same reliability in these cases. We analyzed the histopathological factors that could aid in distinguishing class V LN from non-lupus membranous nephropathy. Our analysis identified a combination of three factors: mesangial deposits, simple C1q staining, and four or more positive elements in immunofluorescence, with an area under the ROC curve of 85%. Mesangial proliferation is also associated with lupus membranous nephropathy, highlighting the significance of mesangial changes as predictors of SLE. Utilizing the same elements to differentiate between LN and other glomerular diseases, Kudose achieved an AUC of 98% to distinguish anti-phospholipase A2 receptor (anti-PLA2R) positive membranous glomerulopathy from class V LN [18]. In Jennette’s study, significant histopathological findings in lupus membranous biopsies included mesangial dense deposits, small subendothelial dense deposits, tubuloreticular inclusions, and deposits in tubular basement membranes. In immunofluorescence, only C1q positivity was more prevalent in membranous LN, with a stronger correlation for intense staining (≥2+). Full-house staining was not assessed [17].
This study has several limitations. First, its retrospective nature, which relied on medical records, presents challenges. To mitigate potential biases, the lead researcher was responsible for data collection. Second, the histopathological findings were evaluated by a single nephropathologist at each center and in an unblinded manner. However, the involvement of experienced pathologists in reputed centers enhances the reliability of anatomical pathology reports. The lack of electron microscopy is another limitation, as it prevented the evaluation of certain histological features, such as tubuloreticular inclusions, and reduced the sensitivity of extraglomerular deposits and combined subepithelial/subendothelial deposits. However, routine electron microscopy is not commonly performed in renal pathology laboratories, particularly when LN is clinically suspected. Additionally, owing to convenience sampling, the LN group was larger than the control group, despite the latter including multiple renal pathologies. Conditions such as minimal change disease and focal segmental glomerulosclerosis, which contributed significantly to biopsies at the research sites, were excluded because they did not present challenges compared to LN. Finally, separate analyses may have minimized the power to detect statistically significant associations, particularly in multivariate analyses. Nevertheless, even with different populations and biopsy methods, the features with good accuracy remained similar.
Advances in renal histopathology incorporating new techniques, such as proteomic analysis, promise to enhance the accuracy of renal biopsy in identifying disease etiology. Recently, new serological and immunofluorescence markers have emerged to distinguish primary and secondary membranous nephropathies [25]. Examples include anti-PLA2R [26] and anti-THSD7A antibodies [27], which are specific to the primary form, as well as exostosin (EXT-1 and EXT-2) as markers of membranous nephropathy secondary to autoimmune diseases, particularly LN [28]. While similar discoveries are not yet available for proliferative forms of LN, these advances complement findings from optical, electron, and conventional immunofluorescence microscopy, broadening diagnostic possibilities.
5. Conclusions
In conclusion, the combination of mesangial proliferation, subendothelial deposits, C1q staining ≥1+, dominant IgG, and four or more positive elements in immunofluorescence offers good accuracy in defining renal involvement in SLE in clinical practice. These findings may also hold significant importance for scientific research and diagnostic consensus, addressing the current conceptual gap. This is particularly relevant following the introduction of renal biopsy-confirmed LN as a definitive criterion for SLE.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
E.R.L.N. and L.Y designed and conducted this study. E.R.L.N collected the data, analyzed the results, and wrote the manuscript. A.G.J.T.M collected the data. M.B.T analyzed the results. W.L.C.S and D.M.A.M supervised the interpretation of biopsy data. L.Y reviewed the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki for studies involving humans and approved by the the ethics committees of Hospital Ana Nery in Salvador (protocol code 4.067.007 / 03-jun-2020) and Hospital das Clinicas at the University of São Paulo Medical School (protocol code 4.734.329 / 26-may-2021). The researchers also signed a confidentiality agreement for the information obtained from medical records and renal biopsy reports.
Informed Consent Statement
As this was a retrospective observational study, an exemption from obtaining informed consent was requested and granted.
Data Availability Statement
The original contributions presented in the study are included in the Article/Supplementary Material, and further enquiries can be directed to the corresponding author (epitacio.rafael@gmail.com).
Acknowledgments
The authors thank all the patients from both hospitals for their participation in this study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Tektonidou, M.G., A. Dasgupta, and M.M. Ward, Risk of End-Stage Renal Disease in Patients With Lupus Nephritis, 1971-2015: A Systematic Review and Bayesian Meta-Analysis. Arthritis Rheumatol, 2016. 68(6): p. 1432-41.
- Bernatsky, S., et al., Mortality in systemic lupus erythematosus. Arthritis Rheum, 2006. 54(8): p. 2550-7.
- Faurschou, M.; Dreyer, L.; Kamper, A.; Starklint, H.; Jacobsen, S. Long-term mortality and renal outcome in a cohort of 100 patients with Lupus Nephritis. Arthritis Care Res. 2010, 62, 873–880. [CrossRef]
- O’Shaughnessy, M.M.; Hogan, S.L.; Thompson, B.D.; Coppo, R.; Fogo, A.B.; Jennette, J.C. Glomerular disease frequencies by race, sex and region: results from the International Kidney Biopsy Survey. Nephrol. Dial. Transplant. 2017, 33, 661–669. [CrossRef]
- Polito, M.G.; de Moura, L.A.R.; Kirsztajn, G.M. An overview on frequency of renal biopsy diagnosis in Brazil: clinical and pathological patterns based on 9617 native kidney biopsies. Nephrol. Dial. Transplant. 2009, 25, 490–496. [CrossRef]
- Dos-Santos, W.L.C., et al., Current distribution pattern of biopsy-proven glomerular disease in Salvador, Brazil, 40 years after an initial assessment. J Bras Nefrol, 2017. 39(4): p. 376-383. [CrossRef]
- Malafronte, P.; Mastroianni-Kirsztajn, G.; Betônico, G.N.; Romão, J.E.; Alves, M.A.R.; Carvalho, M.F.; Neto, O.M.V.; Cadaval, R.A.M.; Bérgamo, R.R.; Woronik, V.; et al. Paulista registry of glomerulonephritis: 5-year data report. Nephrol. Dial. Transplant. 2006, 21, 3098–3105. [CrossRef]
- Alarcón, G.S., Multiethnic lupus cohorts: what have they taught us? Reumatol Clin, 2011. 7(1): p. 3-6.
- Yap, D.Y.; Tang, C.S.; Ma, M.K.; Lam, M.F.; Chan, T.M. Survival analysis and causes of mortality in patients with lupus nephritis. Nephrol. Dial. Transplant. 2012, 27, 3248–3254. [CrossRef]
- Weening, J.J.; ON Behalf of the International Society of Nephrology and Renal Pathology Society Working Group on the Classification Oflupus Nephritis; D’Agati, V.D.; Schwartz, M.M.; Seshan, S.V.; Alpers, C.E.; Appel, G.B.; Balow, J.E.; Bruijn, J.A.; Cook, T.; et al. The classification of glomerulonephritis in systemic lupus erythematosus revisited. Kidney Int. 2004, 65, 521–530. [CrossRef]
- Bajema, I.M.; Wilhelmus, S.; Alpers, C.E.; Bruijn, J.A.; Colvin, R.B.; Cook, H.T.; D’agati, V.D.; Ferrario, F.; Haas, M.; Jennette, J.C.; et al. Revision of the International Society of Nephrology/Renal Pathology Society classification for lupus nephritis: clarification of definitions, and modified National Institutes of Health activity and chronicity indices. Kidney Int. 2018, 93, 789–796. [CrossRef]
- Tan, E.M.; Cohen, A.S.; Fries, J.F.; Masi, A.T.; Mcshane, D.J.; Rothfield, N.F.; Schaller, J.G.; Talal, N.; Winchester, R.J. The 1982 revised criteria for the classification of systemic lupus erythematosus. Arthritis Rheum. 1982, 25, 1271–1277. [CrossRef]
- Hochberg, M.C. Updating the American College of Rheumatology revised criteria for the classification of systemic lupus ery-thematosus. Arthritis Rheum. 1997, 40, 1725. [CrossRef]
- Petri, M.; Orbai, A.; Alarcón, G.S.; Gordon, C.; Merrill, J.T.; Fortin, P.R.; Bruce, I.N.; Isenberg, D.; Wallace, D.J.; Nived, O.; et al. Derivation and validation of the Systemic Lupus International Collaborating Clinics classification criteria for systemic lupus erythematosus. Arthritis Rheum. 2012, 64, 2677–2686. [CrossRef]
- Aringer, M.; Costenbader, K.; Daikh, D.; Brinks, R.; Mosca, M.; Ramsey-Goldman, R.; Smolen, J.S.; Wofsy, D.; Boumpas, D.T.; Kamen, D.L.; et al. 2019 European League Against Rheumatism/American College of Rheumatology classification criteria for systemic lupus erythematosus. Ann. Rheum. Dis. 2019, 78, 1151–1159. [CrossRef]
- Wang, H.; Gao, Y.; Ma, Y.; Cai, F.; Huang, X.; Lan, L.; Ren, P.; Wang, Y.; Chen, J.; Han, F. Performance of the 2019 EULAR/ACR systemic lupus erythematosus classification criteria in a cohort of patients with biopsy-confirmed lupus nephritis. Lupus Sci. Med. 2021, 8, e000458. [CrossRef]
- Jennette, J.C.; Iskandar, S.S.; Dalldorf, F.G. Pathologic differentiation between lupus and nonlupus membranous glomerulopathy. Kidney Int. 1983, 24, 377–385. [CrossRef]
- Kudose, S.; Santoriello, D.; Bomback, A.S.; Stokes, M.B.; D’agati, V.D.; Markowitz, G.S. Sensitivity and Specificity of Pathologic Findings to Diagnose Lupus Nephritis. Clin. J. Am. Soc. Nephrol. 2019, 14, 1605–1615. [CrossRef]
- Ahmed, M.; Love, T.; Moore, C.; Le, T.H.; Jean-Gilles, J.; Goldman, B.; Choung, H.Y.G. The spectrum of renal diseases with lupus-like features: a single-center study. Ren. Fail. 2022, 44, 581–593. [CrossRef]
- IBGE), I.B.d.G.e.E., Censo demográfico 2022: identificação étnico-racial da população, por sexo e idade: resultados do universo. 2023, IBGE: Rio de Janeiro.
- Rijnink, E.C.; Teng, Y.O.; Kraaij, T.; Dekkers, O.M.; Bruijn, J.A.; Bajema, I.M. Validation of the Systemic Lupus International Collaborating Clinics classification criteria in a cohort of patients with full house glomerular deposits. Kidney Int. 2018, 93, 214–220. [CrossRef]
- Rijnink, E.C.; Teng, Y.O.; Kraaij, T.; Wolterbeek, R.; Bruijn, J.A.; Bajema, I.M. Idiopathic non-lupus full-house nephropathy is associated with poor renal outcome. Nephrol. Dial. Transplant. 2017, 32, 654–662. [CrossRef]
- Zahir, Z.; Wani, A.; Gupta, A.; Agrawal, V. Clinicopathological pattern of non-lupus full house nephropathy. Indian J. Nephrol. 2020, 30, 301–306. [CrossRef]
- Ruggiero, B.; Vivarelli, M.; Gianviti, A.; Pecoraro, C.; Peruzzi, L.; Benetti, E.; Ventura, G.; Pennesi, M.; Murer, L.; Coppo, R.; et al. Outcome of childhood-onset full-house nephropathy. Nephrol. Dial. Transplant. 2016, 32, gfw230–1204. [CrossRef]
- Caza, T.N.; Storey, A.J.; Hassen, S.I.; Herzog, C.; Edmondson, R.D.; Arthur, J.M.; Kenan, D.J.; Larsen, C.P. Discovery of seven novel putative antigens in membranous nephropathy and membranous lupus nephritis identified by mass spectrometry. Kidney Int. 2023, 103, 593–606. [CrossRef]
- Debiec, H. and P. Ronco, PLA2R autoantibodies and PLA2R glomerular deposits in membranous nephropathy. N Engl J Med, 2011. 364(7): p. 689-90.
- Seifert, L.; Hoxha, E.; Eichhoff, A.M.; Zahner, G.; Dehde, S.; Reinhard, L.; Koch-Nolte, F.; Stahl, R.A.; Tomas, N.M. The Most N-Terminal Region of THSD7A Is the Predominant Target for Autoimmunity in THSD7A-Associated Membranous Nephropathy. J. Am. Soc. Nephrol. 2018, 29, 1536–1548. [CrossRef]
- Sethi, S.; Madden, B.J.; Debiec, H.; Charlesworth, M.C.; Gross, L.; Ravindran, A.; Hummel, A.M.; Specks, U.; Fervenza, F.C.; Ronco, P. Exostosin 1/Exostosin 2–Associated Membranous Nephropathy. J. Am. Soc. Nephrol. 2019, 30, 1123–1136. [CrossRef]
Figure 1.
ROC curve to distinguish lupus nephritis and non-lupus glomerulopathies – HCFMUSP.
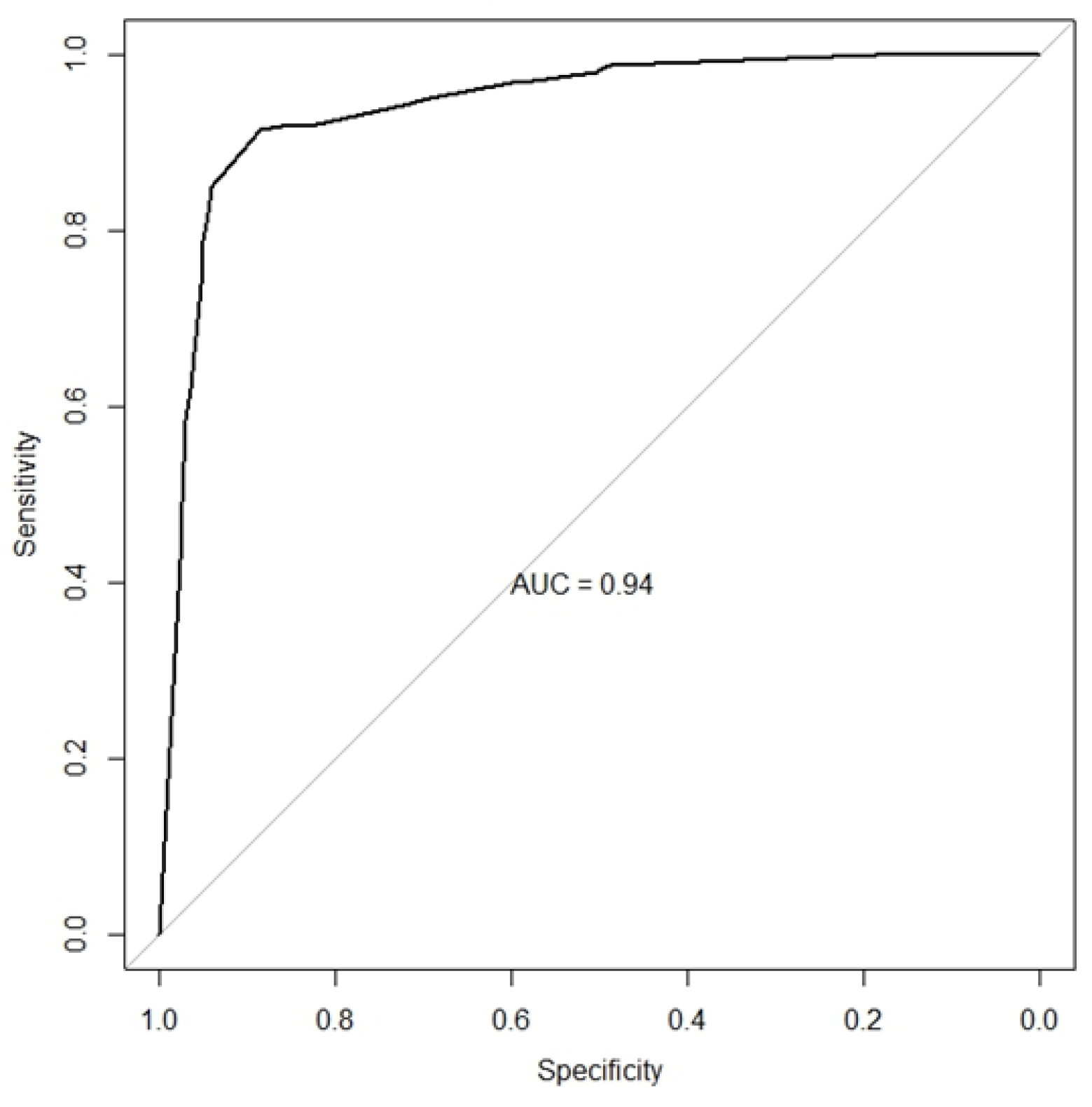
Figure 2.
ROC curve to distinguish lupus nephritis and non-lupus glomerulopathies – HAN.
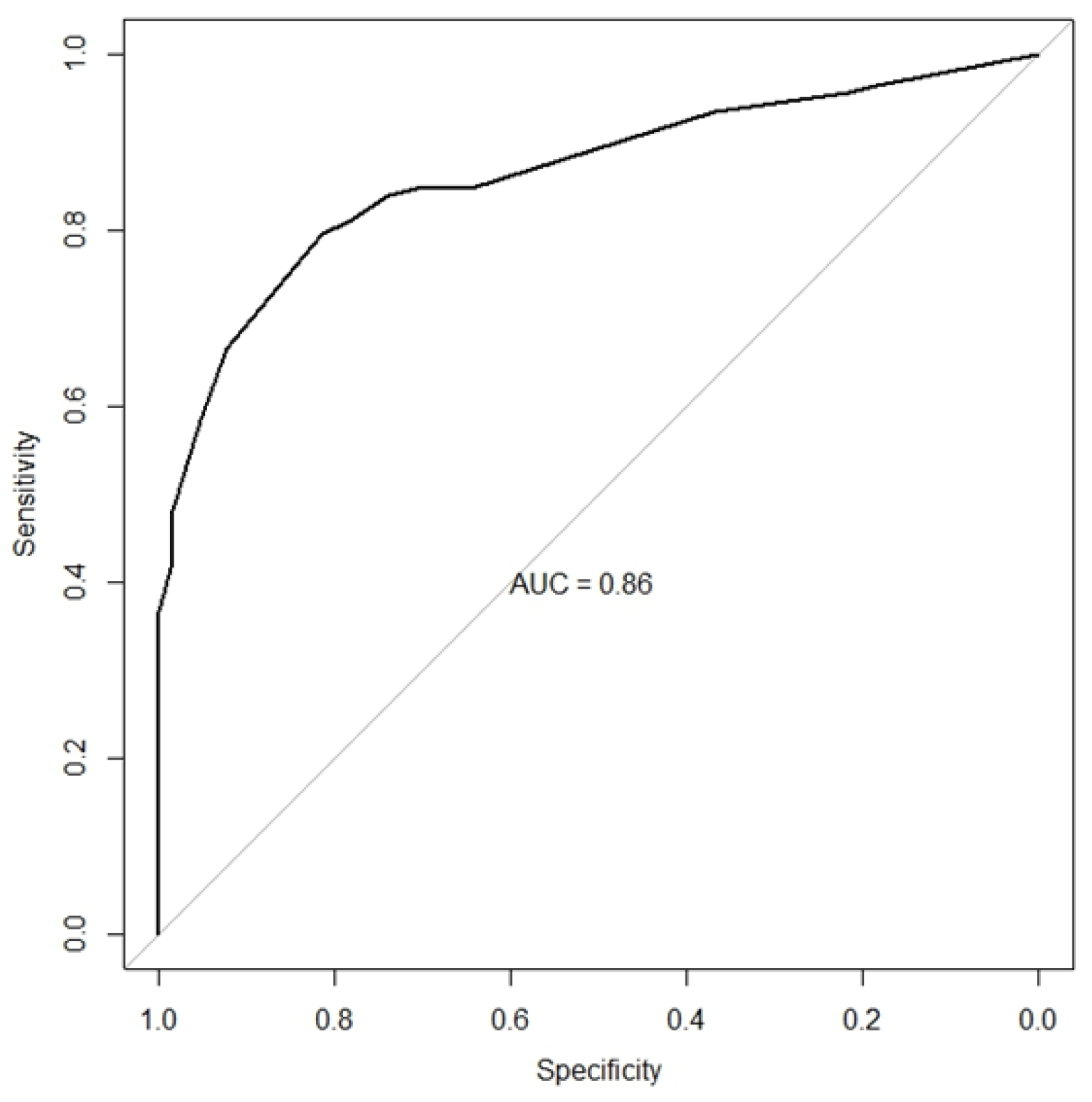

Table 1.
Demographic and clinical characteristics - HCFMUSP patients.
| Lupus Nephritis (n 269) |
Control (n 219) |
|||
|---|---|---|---|---|
| Demographic data: | ||||
| Age | 31.5 (25-40) | 44 (32-58) | p<0.001 | |
| Sex | p<0.001 | |||
| Male | 41 (15.2) | 121 (55.2) | ||
| Female | 228 (84.8) | 98 (44.8) | ||
| Race/Ethnicity | p<0.001 | |||
| Black | 49 (18.2) | 14 (6.4) | ||
| Mixed | 18 (6.7) | 9 (4.1) | ||
| White | 183 (68.0) | 168 (76.7) | ||
| Yellow | 0 | 5 (2.3) | ||
| Unknown | 19 (7.1) | 23 (10.5) | ||
| Clinical data: | ||||
| Creatinine (mg/dl): | 1.00 (0.73-2.03) | 1.96 (1.12-3.41) | p<0.001 | |
| eGFR (CKD-EPI): | 73 (29-110) | 34 (17-71) | p<0.001 | |
| Hemoglobin (g/dl): | 10.9 (9.6-12.2) | 11.1 (9.6-13.2) | p=0.06 | |
| Albumin (g/dl): | 3.0 (2.4-3.5) | 3.2 (2.5-3.6) | p=0.15 | |
| Cholesterol (mg/dl): | 218 (173-274) | 200 (164-252) | p=0.06 | |
| Proteinuria (g/d or g/g): | 2.010 (0.900-4.093) | 2.300 (1.200-4.453) | p=0.29 | |
| Hematuria (%): | 186 (72.7) | 144 (75.4) | p=0.51 | |
| Positive ANA (%): | 214 (98.2) | 57 (32.7) | p<0.001 | |
| Renal syndrome (%): | p<0.001 | |||
| Acute glomerulonephritis | 35 (13.7) | 47 (25.0) | ||
| Nephrotic syndrome | 15 (5.9) | 25 (13.3) | ||
| Nephritic/nephrotic syndrome | 74 (29.0) | 32 (17.0) | ||
| Rapidly progressive GN | 13 (5.1) | 25 (13.3) | ||
| Unknown etiology renal injury | 15 (5.9) | 17 (9.0) | ||
| Asymptomatic urinary abnormalities | 103 (40.4) | 42 (22.3) | ||
|
All data are displayed as median (interquartile range) or N (%). HCFMUSP, Hospital das Clínicas of the University of São Paulo Medical School; eGFR, estimated glomerular filtration rate; CKD-EPI, Chronic Kidney Disease Epidemiology Collaboration; ANA, anti-nuclear antibody; GN, glomerulonephritis |
||||
Table 2.
Characterization of immune deposits in optic and immunofluorescence microscopy - HCFMUSP.
| Immune deposit sites | Lupus nephritis (n 269) | Control (n 219) | IgA nephropathy (n 88) | MN (n 47) | MPGN (n 31) | Pauci-immune GN (n 32) | Proliferative GN (n 21) | |
|---|---|---|---|---|---|---|---|---|
| Mesangial | 220 (87.3) | 165 (77.8) | 88 (100) | 19 (42.2) | 25 (86.2) | 17 (53.1) | 16 (88.9) | |
| Subendothelial | 194 (73.8) | 52 (24.2) | 10 (11.4) | 2 (4.3) | 29 (93.5) | 1 (3.1) | 10 (55.6) | |
| Subepithelial | 130 (49.2) | 51 (23.5) | 0 | 47 (100) | 1 (3.3) | 0 | 3 (15.0) | |
| Subendothelial and subepithelial | 78 (29.8) | 4 (1.8) | 0 | 2 (4.3) | 1 (3.3) | 0 | 1 (5.0) | |
| Tubular | 36 (14.5) | 3 (1.4) | 0 | 0 | 1 (3.6) | 0 | 2 (11.1) | |
| Vascular | 7 (2.8) | 3 (1.4) | 1 (1.1) | 0 | 0 | 1 (3.1) | 1 (5.6) | |
| Extraglomerular | 39 (15.7) | 6 (2.8) | 1 (1.1) | 0 | 1 (3.5) | 1 (3.1) | 3 (16.7) | |
| Immunofluorescence positivity | ||||||||
| IgA | 141 (56.8) | 102 (49.0) | 88 (100) | 8 (17.8) | 4 (14.8) | 0 | 2 (12.5) | |
| IgG | 242 (97.6) | 83 (40.3) | 11 (12.8) | 45 (100) | 14 (51.8) | 4 (12.5) | 9 (56.2) | |
| IgM | 172 (69.6) | 89 (43.2) | 36 (41.9) | 15 (33.3) | 23 (85.2) | 10 (32.3) | 5 (29.4) | |
| Kappa | 148 (59.9) | 66 (32.0) | 17 (19.8) | 36 (80.0) | 12 (44.4) | 0 | 1 (5.9) | |
| Lambda | 222 (89.9) | 133 (64.9) | 73 (85.9) | 41 (93.2) | 15 (55.6) | 0 | 4 (23.5) | |
| C3 | 227 (91.5) | 157 (75.5) | 74 (85.1) | 27 (60.0) | 22 (84.6) | 19 (59.4) | 14 (82.3) | |
| C1q | 215 (86.7) | 38 (18.3) | 8 (9.3) | 10 (22.2) | 15 (55.6) | 2 (6.2) | 3 (17.6) | |
| Fibrinogen | 27 (10.8) | 11 (5.3) | 5 (5.7) | 0 | 0 | 4 (12.9) | 2 (11.8) | |
| Other | ||||||||
| Full-house staining | 91 (36.8) | 8 (3.8) | 2 (2.3) | 3 (6.7) | 2 (7.4) | 0 | 1 (5.9) | |
| Dominant IgG | 227 (91.5) | 66 (32.5) | 0 | 45 (100) | 11 (40.7) | 3 (9.7) | 7 (43.7) | |
| C1q ≥ 1+ | 197 (79.4) | 23 (11.1) | 2 (2.3) | 8 (17.8) | 11 (40.7) | 1 (3.1) | 1 (5.9) | |
| IgG/C3/C1q plus IgA or IgM | 176 (71.3) | 13 (6.2) | 2 (2.3) | 3 (6.7) | 7 (25.9) | 0 | 1 (5.9) | |
| ≥ 4 elements staining in IF | 187 (75.7) | 22 (10.7) | 10 (11.6) | 4 (8.9) | 7 (25.9) | 0 | 1 (6.2) | |
| Note: Data are presented as n (%). Missing data were excluded from the analysis. HCFMUSP, Hospital das Clínicas of the University of São Paulo Medical School; MN, membranous nephropathy; MPGN, membranoproliferative glomerulonephritis; IF, immunofluorescence. | ||||||||
Table 3.
Diagnostic performance of histopathological features for lupus nephritis - HCFMUSP.
| Feature | Sensitivity (IC 95%) | Specificity (IC 95%) | Accuracy (IC 95%) | PPV (IC 95%) | NPV (IC 95%) | Positive LR (IC 95%) | Negative LR (IC 95%) | |
|---|---|---|---|---|---|---|---|---|
| Mesangial proliferation | 0.89 (0.84, 0.92) | 0.36 (0.30, 0.43) | 0.65 (0.61, 0.69) | 0.63 (0.58, 0.68) | 0.72 (0.63, 0.81) | 1.39 (1.25, 1.55) | 0.31 (0.21, 0.46) | |
| Endocapillary hypercellularity | 0.64 (0.58, 0.70) | 0.63 (0.57, 0.70) | 0.64 (0.59, 0.68) | 0.68 (0.62, 0.74) | 0.59 (0.53, 0.65) | 1.75 (1.44, 2.13) | 0.57 (0.47, 0.68) | |
| Mesangial deposits | 0.87 (0.83, 0.91) | 0.22 (0.17, 0.28) | 0.58 (0.53, 0.62) | 0.57 (0.52, 0.62) | 0.59 (0.48, 0.70) | 1.12 (1.03, 1.22) | 1.12 (1.03, 1.22) | |
| Subendothelial deposits | 0.74 (0.68, 0.79) | 0.76 (0.70, 0.81) | 0.75 (0.71, 0.79) | 0.79 (0.73, 0.84) | 0.70 (0.64, 0.76) | 3.05 (2.38, 3.91) | 0.35 (0.28, 0.43) | |
| Subepithelial deposits | 0.49 (0.43, 0.55) | 0.76 (0.70, 0.82) | 0.62 (0.57, 0.66) | 0.72 (0.65, 0.78) | 0.55 (0.50, 0.61) | 2.10 (1.60, 2.74) | 0.66 (0.58, 0.76) | |
| Combined subendothelial and subepithelial deposits | 0.30 (0.24, 0.36) | 0.98 (0.95, 0.99) | 0.61 (0.56, 0.65) | 0.95 (0.88, 0.99) | 0.54 (0.48, 0.59) | 16.08 (5.98, 43.20) | 0.72 (0.66, 0.78) | |
| Extraglomerular deposits | 0.16 (0.11, 0.21) | 0.97 (0.94, 0.99) | 0.53 (0.48, 0.58) | 0.87 (0.73, 0.95) | 0.49 (0.44, 0.54) | 5.51 (2.38, 12.75) | 0.87 (0.82, 0.92) | |
| Positive IgA | 0.57 (0.50, 0.63) | 0.51 (0.44, 0.58) | 0.54 (0.49, 0.59) | 0.58 (0.52, 0.64) | 0.50 (0.43, 0.57) | 1.16 (0.97, 1.38) | 0.85 (0.70, 1.03) | |
| Positive IgG | 0.98 (0.95, 0.99) | 0.60 (0.53, 0.66) | 0.80 (0.76, 0.84) | 0.74 (0.69, 0.79) | 0.95 (0.90, 0.98) | 2.42 (2.05, 2.86) | 0.04 (0.02, 0.09) | |
| Positive IgM | 0.70 (0.63, 0.75) | 0.57 (0.50, 0.64) | 0.64 (0.59, 0.68) | 0.66 (0.60, 0.72) | 0.61 (0.54, 0.68) | 1.61 (1.35, 1.92) | 0.53 (0.43, 0.67) | |
| Positive C3 | 0.92 (0.87, 0.95) | 0.25 (0.19, 0.31) | 0.61 (0.56, 0.65) | 0.59 (0.54, 0.64) | 0.71 (0.59, 0.81) | 1.21 (1.11, 1.32) | 0.35 (0.22, 0.55) | |
| Positive C1q | 0.87 (0.82, 0.91) | 0.82 (0.76, 0.87) | 0.84 (0.81, 0.88) | 0.85 (0.80, 0.89) | 0.84 (0.78, 0.88) | 4.72 (3.53, 6.32) | 0.16 (0.12, 0.23) | |
| C1q ≥ 1+ | 0.79 (0.74, 0.84) | 0.89 (0.84, 0.93) | 0.84 (0.80, 0.87) | 0.90 (0.85, 0.93) | 0.78 (0.72, 0.83) | 7.15 (4.84, 10.56) | 0.23 (0.18, 0.30) | |
| Dominant IgG | 0.92 (0.87, 0.95) | 0.67 (0.61, 0.74) | 0.81 (0.77, 0.84) | 0.77 (0.72, 0.82) | 0.87 (0.80, 0.92) | 2.82 (2.30, 3.44) | 0.13 (0.08, 0.19) | |
| Full-house staining | 0.37 (0.31, 0.44) | 0.96 (0.93, 0.98) | 0.64 (0.60, 0.69) | 0.92 (0.85, 0.96) | 0.56 (0.51, 0.62) | 9.73 (4.84, 19.57) | 0.65 (0.59, 0.72) | |
| IgG/C3/C1q plus IgA or IgM | 0.71 (0.65, 0.77) | 0.94 (0.90, 0.97) | 0.82 (0.78, 0.85) | 0.93 (0.89, 0.96) | 0.73 (0.68, 0.79) | 11.46 (6.73, 19.51) | 0.31 (0.25, 0.37) | |
| ≥ 4 elements staining in IF | 0.76 (0.70, 0.81) | 0.89 (0.84, 0.93) | 0.82 (0.78, 0.85) | 0.89 (0.84, 0.93) | 0.75 (0.70, 0.81) | 7.09 (4.75, 10.59) | 0.27 (0.22, 0.34) | |
| HCFMUSP, Hospital das Clinicas of the University of São Paulo Medical School; PPV, positive predictive value; NPV, negative predictive value; LR, likelihood ratio; IF, immunofluorescence. | ||||||||
Table 4.
Combined diagnostic performance of histopathological features for lupus nephritis – HCFMUSP.
Table 4.
Combined diagnostic performance of histopathological features for lupus nephritis – HCFMUSP.
| No. of Features* | Sensitivity (IC 95%) | Specificity (IC 95%) | Accuracy (IC 95%) | PPV (IC 95%) | NPV (IC 95%) | Positive LR (IC 95%) | Negative LR (IC 95%) |
|---|---|---|---|---|---|---|---|
| One or more | 1.00 (0.99, 1.00) | 0.19 (0.14, 0.25) | 0.63 (0.59, 0.68) | 0.60 (0.55, 0.65) | 1.00 (0.91, 1.00) | 1.23 (1.15, 1.31) | 0.00 (0.00, NA) |
| Two or more | 0.96 (0.93, 0.98) | 0.61 (0.54, 0.67) | 0.80 (0.76, 0.84) | 0.75 (0.70, 0.79) | 0.93 (0.87, 0.97) | 2.44 (2.06, 2.90) | 0.06 (0.03, 0.12) |
| Three or more | 0.91 (0.87, 0.94) | 0.87 (0.81, 0.91) | 0.89 (0.86, 0.92) | 0.89 (0.85, 0.93) | 0.89 (0.84, 0.93) | 6.84 (4.81, 9.74) | 0.10 (0.07, 0.15) |
| Four or more | 0.74 (0.68, 0.80) | 0.96 (0.92, 0.98) | 0.84 (0.80, 0.87) | 0.95 (0.91, 0.98) | 0.75 (0.70, 0.81) | 16.76 (8.81, 31.87) | 0.27 (0.22, 0.33) |
| Five | 0.46 (0.40, 0.53) | 0.98 (0.94, 0.99) | 0.69 (0.65, 0.74) | 0.96 (0.90, 0.99) | 0.60 (0.54, 0.65) | 18.73 (7.80, 44.97) | 0.55 (0.49, 0.62) |
| *Mesangial proliferation, subendothelial deposits, C1q ≥ 1+, dominant IgG and 4 or more positive elements in immunofluorescence. HCFMUSP, Hospital das Clinicas of the University of São Paulo Medical School; PPV, positive predictive value; NPV, negative predictive value; LR, likelihood ratio; | |||||||
Table 5.
Diagnostic performance of histopathological features in distinguishing class V lupus nephritis and non-lupus membranous nephropathy – HCFMUSP.
Table 5.
Diagnostic performance of histopathological features in distinguishing class V lupus nephritis and non-lupus membranous nephropathy – HCFMUSP.
| Feature | Sensitivity (IC 95%) | Specificity (IC 95%) | Accuracy (IC 95%) | PPV (IC 95%) | NPV (IC 95%) | Positive LR (IC 95%) | Negative LR (IC 95%) |
|
|---|---|---|---|---|---|---|---|---|
| Mesangial proliferation | 0.68 (0.52, 0.81) | 0.60 (0.44, 0.74) | 0.64 (0.53, 0.74) | 0.61 (0.46, 0.75) | 0.67 (0.50, 0.80) | 1.69 (1.13, 2.52) | 0.53 (0.33, 0.87) | |
| Mesangial deposits | 0.76 (0.61, 0.87) | 0.58 (0.42, 0.72) | 0.67 (0.56, 0.77) | 0.65 (0.51, 0.77) | 0.70 (0.53, 0.84) | 1.80 (1.23, 2.63) | 0.41 (0.23, 0.73) | |
| Positive IgA | 0.43 (0.29, 0.59) | 0.82 (0.68, 0.92) | 0.63 (0.52, 0.73) | 0.71 (0.51, 0.87) | 0.59 (0.46, 0.71) | 2.45 (1.20, 4.97) | 0.69 (0.52, 0.92) | |
| Positive IgM | 0.70 (0.54, 0.82) | 0.67 (0.51, 0.80) | 0.68 (0.58, 0.78) | 0.68 (0.53, 0.81) | 0.68 (0.52, 0.81) | 2.09 (1.32, 3.29) | 0.46 (0.28, 0.74) | |
| Positive C1q | 0.76 (0.61, 0.87) | 0.78 (0.63, 0.89) | 0.77 (0.67, 0.85) | 0.78 (0.63, 0.89) | 0.76 (0.61, 0.87) | 3.42 (1.94, 6.06) | 0.31 (0.18, 0.53) | |
| C1q ≥ 1+ | 0.65 (0.50, 0.79) | 0.82 (0.68, 0.92) | 0.74 (0.63, 0.82) | 0.79 (0.63, 0.90) | 0.70 (0.56, 0.82) | 3.67 (1.89, 7.12) | 0.42 (0.28, 0.64) | |
| Full-house staining | 0.22 (0.11, 0.36) | 0.93 (0.82, 0.99) | 0.57 (0.46, 0.67) | 0.77 (0.46, 0.95) | 0.54 (0.42, 0.65) | 3.26 (0.96, 11.08) | 0.84 (0.71, 1.00) | |
| IgG/C3/C1q plus IgA or IgM | 0.57 (0.41, 0.71) | 0.93 (0.82, 0.99) | 0.75 (0.65, 0.83) | 0.90 (0.73, 0.98) | 0.68 (0.55, 0.79) | 8.48 (2.76, 26.04) | 0.47 (0.33, 0.65) | |
| ≥ 4 elements staining in IF | 0.61 (0.45, 0.75) | 0.91 (0.79, 0.98) | 0.76 (0.66, 0.84) | 0.88 (0.71, 0.96) | 0.69 (0.56, 0.81) | 6.85 (2.61, 17.95) | 0.43 (0.30, 0.62) | |
| HCFMUSP, Hospital das Clinicas of the University of São Paulo Medical School; PPV, positive predictive value; NPV, negative predictive value; LR, likelihood ratio; IF, immunofluorescence. | ||||||||
Table 6.
Diagnostic performance of histopathological features for lupus nephritis - HAN.
| Feature | Sensitivity (IC 95%) | Specificity (IC 95%) | Accuracy (IC 95%) | PPV (IC 95%) | NPV (IC 95%) | Positive LR (IC 95%) | Negative LR (IC 95%) |
|---|---|---|---|---|---|---|---|
| Mesangial proliferation | 0.69 (0.61, 0.76) | 0.43 (0.32, 0.55) | 0.60 (0.54, 0.67) | 0.71 (0.64, 0.78) | 0.40 (0.30, 0.51) | 1.21 (0.97, 1.50) | 0.73 (0.52, 1.02) |
| Endocapillary hypercellularity | 0.74 (0.67, 0.81) | 0.61 (0.49, 0.72) | 0.70 (0.64, 0.76) | 0.80 (0.72, 0.86) | 0.53 (0.43, 0.64) | 1.89 (1.42, 2.53) | 0.42 (0.31, 0.58) |
| Mesangial deposits | 0.70 (0.62, 0.77) | 0.36 (0.25, 0.49) | 0.59 (0.52, 0.66) | 0.71 (0.63, 0.78) | 0.35 (0.24, 0.47) | 1.09 (0.89, 1.34) | 0.84 (0.56, 1.24) |
| Subendothelial deposits | 0.74 (0.66, 0.80) | 0.58 (0.45, 0.70) | 0.69 (0.62, 0.75) | 0.80 (0.72, 0.86) | 0.49 (0.38, 0.61) | 1.75 (1.31, 2.35) | 0.46 (0.33, 0.64) |
| Subepithelial deposits | 0.49 (0.41, 0.57) | 0.55 (0.43, 0.67) | 0.51 (0.44, 0.58) | 0.71 (0.61, 0.79) | 0.33 (0.25, 0.42) | 1.10 (0.82, 1.48) | 0.92 (0.71, 1.19) |
| Combined subendothelial and subepithelial deposits |
0.24 (0.18, 0.31) | 0.90 (0.80, 0.96) | 0.44 (0.37, 0.51) | 0.84 (0.71, 0.94) | 0.34 (0.27, 0.41) | 2.37 (1.11, 5.04) | 0.85 (0.75, 0.95) |
| Extraglomerular deposits | 0.33 (0.26, 0.41) | 1.00 (0.95, 1.00) | 0.54 (0.48, 0.61) | 1.00 (0.93, 1.00) | 0.41 (0.34, 0.49) | Inf (NaN, Inf) | 0.67 (0.60, 0.75) |
| Positive IgA | 0.63 (0.55, 0.71) | 0.55 (0.42, 0.67) | 0.60 (0.53, 0.67) | 0.75 (0.66, 0.82) | 0.41 (0.31, 0.52) | 1.39 (1.04, 1.86) | 0.68 (0.50, 0.92) |
| Positive IgG | 0.96 (0.91, 0.98) | 0.35 (0.24, 0.48) | 0.76 (0.70, 0.82) | 0.76 (0.69, 0.82) | 0.79 (0.60, 0.92) | 1.47 (1.23, 1.76) | 0.12 (0.05, 0.29) |
| Positive IgM | 0.65 (0.57, 0.73) | 0.44 (0.32, 0.57) | 0.59 (0.51, 0.65) | 0.71 (0.62, 0.79) | 0.38 (0.27, 0.49) | 1.17 (0.91, 1.49) | 0.79 (0.55, 1.12) |
| Positive C3 | 0.84 (0.77, 0.90) | 0.32 (0.21, 0.45) | 0.68 (0.61, 0.74) | 0.73 (0.66, 0.80) | 0.49 (0.33, 0.65) | 1.25 (1.04, 1.50) | 0.48 (0.29, 0.81) |
| Positive C1q | 0.69 (0.61, 0.77) | 0.77 (0.65, 0.87) | 0.72 (0.65, 0.78) | 0.87 (0.79, 0.93) | 0.54 (0.43, 0.64) | 3.06 (1.93, 4.83) | 0.40 (0.30, 0.52) |
| C1q ≥ 1+ | 0.64 (0.55, 0.72) | 0.83 (0.72, 0.91) | 0.70 (0.63, 0.76) | 0.89 (0.82, 0.95) | 0.51 (0.42, 0.61) | 3.83 (2.20, 6.67) | 0.43 (0.34, 0.55) |
| Dominant IgG | 0.85 (0.78, 0.90) | 0.48 (0.36, 0.61) | 0.73 (0.66, 0.79) | 0.77 (0.70, 0.84) | 0.60 (0.46, 0.74) | 1.65 (1.29, 2.10) | 0.31 (0.20, 0.50) |
| Full-house staining | 0.40 (0.32, 0.49) | 0.97 (0.89, 1.00) | 0.58 (0.51, 0.65) | 0.97 (0.88, 1.00) | 0.43 (0.35, 0.52) | 13.20 (3.32, 52.46) | 0.62 (0.54, 0.71) |
| IgG/C3/C1q plus IgA or IgM | 0.58 (0.49, 0.66) | 0.95 (0.87, 0.99) | 0.70 (0.63, 0.76) | 0.96 (0.90, 0.99) | 0.51 (0.42, 0.60) | 12.47 (4.09, 38.00) | 0.44 (0.36, 0.54) |
| ≥ 4 elements staining in IF | 0.64 (0.55, 0.72) | 0.80 (0.68, 0.89) | 0.69 (0.62, 0.75) | 0.87 (0.79, 0.93) | 0.51 (0.41, 0.61) | 3.20 (1.94, 5.29) | 0.45 (0.35, 0.58) |
| HAN, Hospital Ana Nery; PPV, positive predictive value; NPV, negative predictive value; LR, likelihood ratio; IF, immunofluorescence. | |||||||
Table 7.
Combined diagnostic performance of histopathological features for lupus nephritis - HAN.
| No. of features* | Sensitivity (IC 95%) | Specificity (IC 95%) | Accuracy (IC 95%) | PPV (IC 95%) | NPV (IC 95%) | Positive LR (IC 95%) | Negative LR (IC 95%) |
|---|---|---|---|---|---|---|---|
| One or more | 0.96 (0.92, 0.99) | 0.18 (0.10, 0.30) | 0.71 (0.65, 0.77) | 0.71 (0.64, 0.78) | 0.71 (0.44, 0.90) | 1.18 (1.05, 1.33) | 0.20 (0.07, 0.54) |
| Two or more | 0.85 (0.78, 0.90) | 0.65 (0.52, 0.76) | 0.78 (0.72, 0.84) | 0.83 (0.76, 0.89) | 0.67 (0.54, 0.78) | 2.39 (1.71, 3.35) | 0.24 (0.15, 0.37) |
| Three or more | 0.66 (0.58, 0.74) | 0.92 (0.83, 0.97) | 0.75 (0.68, 0.81) | 0.95 (0.88, 0.98) | 0.57 (0.47, 0.67) | 8.64 (3.69, 20.21) | 0.36 (0.28, 0.47) |
| Four | 0.36 (0.28, 0.45) | 1.00 (0.94, 1.00) | 0.57 (0.50, 0.64) | 1.00 (0.93, 1.00) | 0.43 (0.35, 0.51) | Inf (NaN, Inf) | 0.64 (0.56, 0.72) |
| *Subendothelial deposits, C1q ≥ 1+, dominant IgG and 4 or more positive elements in immunofluorescence. HAN, Hospital Ana Nery; PPV, positive predictive value; NPV, negative predictive value; LR, likelihood ratio; IF, immunofluorescence. | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



