
Submitted:
01 November 2024
Posted:
05 November 2024
You are already at the latest version
Abstract
Background: The prevalence of multidrug-resistant Acinetobacter baumannii is gradually increasing globally, posing a serious burden on patients and society, which is a significant public health issue.Testing the homology of multidrug-resistant Acinetobacter baumannii clones in hospitals in Xinjiang autonomous region can enable the hospital infection control department to better monitor the source and prevent the spread of drug-resistant characteristics.
Method: Multidrug resistant Acinetobacter baumannii detected in intensive care units of 9 urban hospitals in Xinjiang autonomous region were collected. After drug sensitivity testing, DNA was extracted, and homology analysis was performed.
Conclusion: 72 strains of carbapenem resistant Acinetobacter baumannii were multi drug resistant; The resistance rate of this bacterium to polymyxin B (1.3%) and tigecycline (1.7%) was low. The genotype of type 3 was unique to Urumqi; Type 4 is mainly distributed in Changji and Hotan, showing a unique significant band; Type 2 appeared in Urumqi and Hotan, and type 1 was prevalent throughout Xinjiang. It is distributed in all regions, and the similarity coefficient is 99%.
Keywords:
dcineiobacier baumannii
; bacterial clone
; multi-drug resistance
; homology
; spread
Introduction
Acinetobacter baumannii is a non-fermenting gram-negative bacterium, which is one of the important opportunistic pathogens causing hospital infection. In recent years, hospital infection caused by Acinetobacter baumannii has increased year by year, especially in intensive care unit ( ICU ).
Currently, there is a growing number of reports on the isolation, infection, and drug resistance of Acinetobacter baumannii.
Isolated from human infections and hospital outbreaks [1]. According to the latest CHINET data in China, the clinical isolation rate of Acinetobacter in 2012 was 10.1 %, of which Acinetobacter baumannii accounted for 91.5 %[2]. Respiratory tract marker
The isolation rate of Acinetobacter baumannii in this study was 17.3 % . Multidrug-resistant strains of A.baumannii have been found in hospitals in Europe, North America, Argentina, Brazil, China, Japan and South Korea, as well as in the South Pacific island of Tahiti. [3,4] In recent years, Acinetobacter baumannii has shown increasing resistance to commonly used antibiotics worldwide.
Medicinal properties [5]. According to the latest drug resistance survey published on CHINET ( 2023 ), the resistance rate of Acinetobacter baumannii to imipenem was 66.7 %, and the resistance rate to meropenem was 69.3 %. The resistance rates to cefoperazone-sulbactam and minocycline were 43. 5 % and 44. 4 %, respectively. The resistance rates to polymyxin B and tigecycline were low ( 0. 1 % and 6. 0 % ).
The drug resistance rate of the test drugs was more than 40 % [6].
Acinetobacter baumannii is the most important opportunistic pathogen of nosocomial infection in the world. Due to the failure of clinical anti-infection treatment caused by bacterial resistance and the outbreak of nosocomial infection, Acinetobacter baumannii poses a great threat to human health. In particular, patients with weak immune resistance are more likely to be infected by this opportunistic pathogen. Therefore, the study of Acinetobacter baumannii has extremely important clinical significance.
This study aims to clarify the distribution of multidrug-resistant Acinetobacter baumannii strains detected in ICUs of major hospitals in Xinjiang Uygur Autonomous Region through homology analysis,the results can be used to monitor the hospital infection management and monitoring departments of hospitals at all levels in Xinjiang. Provide important theoretical basis.
Materials and Methods
Strain Collection
Strain collection occurred from May 2022 to October 2023, during which 72 strains of multidrug-resistant Acinetobacter baumannii were collected from nine regions (prefectures) in Xinjiang, excluding repeated strains from the same patient's same body part. Among them, there were 38 strains from Urumqi, 4 strains from Turpan, 3 strains from Yili, 2 strains from Shihezi, 7 strains from Changji, 4 strains from Korla, 5 strains from Aksu, 3 strains from Kashgar and 6 strains from Hotan. All strains were from hospitalized patients : 30 strains in ICU, 18 strains in Surgical ICU ( SICU ), 8 strains in respiratory ICU ( RICU ), 9 strains in burn wound repair department, 5 strains in respiratory department and 2 strains in Neurosurgical ICU ( NSICU ). A total of 40 strains were isolated from sputum, 11 strains from blood, 11 strains from wound secretion, 6 strains from venous catheter tip, 4 strains from tracheal aspirate. All the collected strains were initially identified as Acinetobacter baumannii complex by VITEK 2-Compact system. The collection of bacterial strains has been approved by the Ethics Committee of Xinjiang Uygur Autonomous Region People's Hospital.
Antimicrobial Susceptibility Testing
The sensitivity of drug was determined using VITEK2 Compat (bioMerieux Inc., France) in accordance with standard operating procedures, referring to the US FDA recommended standard, Clinical Laboratory Standards Institute (CLSI) and interpreted according to CLSI 2023 guidelines. The quality control strains Escherichia coli ATCC 25922, Escherichia coli ATCC 35218, Pseudomonas aeruginosa ATCC 27853 and Klebsiella pneumoniae ATCC 700603 were purchased from Shanghai Hanni Biotechnology Co., Ltd. Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC ultra 27853 standard strains were used for drug sensitivity control every week.
DNA Preparation
DNA extraction: select a single colony on a blood plate and extract bacterial DNA using Mo bio ultracleantm microbial DNA extraction kit. The concentration of DNA was detected by the spectrophotometer nanodrop 1000, and the concentration of DNA was adjusted to 25 ~ 50mg/l using distilled water.
Diversilab Acinetobacter DNA fingerprinting kit was used to prepare 25 μ l PCR amplification system; A 2720 PCR instrument was used for amplification. Pre denaturation at 94 ℃ for 2 min, denaturation at 94 ℃ for 30 s, annealing at 50 ℃ for 30 s, and extension at 70 ℃ for 90 s were one amplification cycle, with a total of 35 cycles; The final extension was at 70 ℃ for 3min.
Detection of PCR amplification products the amplification products and the gel were injected into the microfluidic chip labchips in sequence. The microfluidic chip prepared by shaking with a vortex Genie 2 oscillator for 1min was put into the Agilent 2100 Bioanalyzer to detect the amplified product fragments in the microfluidic chip labchips.
We conducted gene detection for efflux pumps, biofilms, and carbapenemases (OXA). The primer sequences and amplification lengths of the relevant genes are shown in Table 1
Statistical Analysis
Through the independent and safe diversilab Internet analysis software, the results of amplified products are grouped according to the real-time analysis of DNA and fingerprint data, and the report is generated online. There was no difference in similarity coefficient and bands, and more than 97% of similarity coefficient indicated that they originated from the same clone; Only 1-2 bands were different, and the similarity coefficient was 95% - 97%. The suspected outbreak indicated that it was related; Three or more bands from different sources are different, and the similarity coefficient is less than 95%, indicating no kinship
Results
Drug Susceptibility Test Results
According to this study, 72 strains of multidrug-resistant Acinetobacter baumannii were identified, with the clinical diagnosis mainly being postoperative infection; samples were collected from May 2022 to October 2023. In other regions, except for 2 strains from Hotan, which were distributed in the respiratory department, the other strains originated from the Department of critical care medicine; The main clinical diagnosis was pulmonary infection; All sputum specimens were judged as qualified specimens by smear. 72 strains of Acinetobacter baumannii were multidrug-resistant bacteria, see Table 2
Biofilm-Related Gene Analysis
Through genetic testing, it was found that the drug resistance of Acinetobacter baumannii in this region is not due to the upregulation of AdeR caused by the insertion of the ISAba1 gene, but rather a mutation in the efflux pump gene AdeRS. The increase in AdeB also affects the expression level of CarO, resulting in a decrease in the outer membrane porin protein, which hinders the entry of antibiotics into bacterial channels and promotes the enhancement of Acinetobacter baumannii drug resistance. Among the detected biofilm genes, the expression level of biofilm growth gene bfs significantly increased, see Figure 1 and Figure 2.
Homology Analysis
The similarity between strains was compared according to the polymorphism of amplified fragments. According to the standard of 95%, it can be divided into four types: type 1 is the main clone, accounting for 59.7%; The second is type 3, accounting for 16.7%; Type 4 and type 2 were 12.5% and 11.1%, respectively. Among them, type 3 is a unique clone strain in Urumqi; Type 2 is mainly distributed in Urumqi and Hotan; Type 1 was distributed in 9 regions of Xinjiang, of which Urumqi accounted for 46.5%; Type 4 is mainly distributed in Changji and Hotan areas, showing a unique significant band. The type 1 similarity coefficient is 95% - 97%, while the type 2, 3 and 4 similarity coefficients are greater than 97%. According to the list, it can be seen that Acinetobacter baumannii causing various infections in Xinjiang is mainly type 1 clonal strain. See Table 3.
In view of the fact that type 1 clonal strains are epidemic strains in Xinjiang, while type 3 clonal strains are unique to Urumqi, the comparison of their drug resistance results showed that the drug resistance rate of type 1 clonal strains was slightly lower than that of type 3, except for tigecycline 2 strains, polymyxin B 1 strain was all from type 3 clonal strains, and the comparison of the drug resistance rate of other antibiotics. See Table 4.
Discussion
Acinetobacter baumannii is one of the major pathogens causing nosocomial infections worldwide in recent years [7], especially carbapenem resistant strains, which bring great difficulties to clinical treatment. Some literatures have reported that Acinetobacter baumannii has strong biofilm forming ability. When the bacteria exist in the form of biofilm, the drug resistance and pathogenicity are significantly enhanced [8,9]. According to the data analysis of the expert committee of the bacterial drug resistance monitoring network of Xinjiang Autonomous Region, the resistance rate of Acinetobacter baumannii to carbapenems was 56.4% in 2023, which was 75.5% in our hospital, which was also higher than the report of nearly 70% in Chinet bacterial drug resistance monitoring in 2023 [10]. In addition, prolonged hospitalization and the use of expensive antibiotics have significantly increased the incidence, mortality and medical costs of iatrogenic infections caused by multidrug-resistant bacteria.
In this study, we collected 72 multidrug-resistant Acinetobacter baumannii strains that met our criteria from the ICUs of nine hospitals across Xinjiang.The purpose was to understand the distribution of drug-resistant clones in hospitals in various regions. The results of this study can provide important theoretical basis for the monitoring of nosocomial infection management and monitoring departments in hospitals at all levels in Xinjiang. Many scholars have successively reported the advantages and disadvantages of various genotyping methods [11,12]. The diversilab system was used in this study. According to the analysis reported by quyanyan et al. [13], this method has the advantages of simple operation, high throughput and strong typing ability. Repeat based PCR primers are paired with many repeats that are specific to the entire genome; After PCR amplification, multiple fragments with different lengths were formed. According to their quality differences, these amplified fragments were electrophoretically analyzed to obtain repetitive sequence PCR DNA fingerprints composed of multiple bands with different strengths and specificities. This method was used to study the homology of multidrug-resistant Acinetobacter baumannii in Xinjiang, and the results were divided into four different clonal types: 43 strains of multidrug-resistant Acinetobacter baumannii from the same source were detected in 9 regions (prefectures) of Xinjiang with genotype 1, which were distributed in all regions. The experimental results showed that 20 strains were distributed in Urumqi, 5 strains in Aksu, 4 strains in Turpan, 3 strains in Kashgar, 4 strains in Korla, 2 strains in Shihezi, 3 strains in Ili, 1 strain in Hetian and 1 strain in Changji, indicating the spread of multidrug-resistant Acinetobacter baumannii in different regions, hospitals, wards or the same region, hospitals, wards in Xinjiang. Whether it is due to the clonal transmission of carbapenem resistant Acinetobacter baumannii remains to be further studied. Type 3 is a unique clone strain in Urumqi. Clinical data showed that five strains of multidrug-resistant Acinetobacter baumannii were simultaneously cultured from blood, secretions, and sputum samples of different burn patients in SICU in August 2017; At the same time, another multidrug-resistant Acinetobacter baumannii was isolated from the drainage fluid sample of another patient in SICU. The patient was clinically diagnosed with spinal stenosis; At the end of August and the beginning of September, all burn patients were transferred to the burn wound repair department, and the same drug-resistant bacteria as SICU were cultured from the venous catheter tip, secretion, and sputum samples; At the same time, the same drug-resistant bacteria as SICU were also cultured from the secretion samples of patients with electrical injury in this department. According to the polymorphism of amplified fragments, the similarity coefficient between strains was 95% - 100%, suggesting that multidrug-resistant Acinetobacter baumannii from the same source was detected; It showed that the clone had cross transmission in SICU, and there was cross transmission between SICU and burn wound repair ward. One of the cloned strains originated from the ICU of Hotan District Hospital, which may be related to the transfer of patients. The genotype of type 2 appeared in Urumqi and Hetian area. The characteristics of this group were that six strains of the same genotype were isolated from different ICU (RICU, SICU, nsicu) patient specimens, and the three ICUs were distributed in different areas and floors of the hospital. Secondly, ICU did not accompany, and medical staff did well in personal protection when entering and leaving the ward. However, the patients were transferred. The main factors leading to the spread were closely related to environmental pollution and hand hygiene, which was consistent with the report of liuyanyuan et al. [14]. At the same time, it was found that there were different strains in SICU, suggesting that different clonal strains may cross infect in the hospital. There are two strains of bacteria isolated from the respiratory ward in Hotan, belonging to the same genotype, suggesting that Urumqi and Hotan also have homology. The genotype of type 4 was distributed in Changji and Hotan regions, showing a unique significant band; Through the analysis of clinical data: isolated from the respiratory ward on August 10, 2022, the specimen was sputum, which was clinically diagnosed as pulmonary infection; Isolated from ICU on August 23 of the same year, the specimen was sputum, which was clinically diagnosed as acute attack of chronic bronchitis; On September 6 of the same year, it was isolated from the respiratory ward. The specimen was sputum. The clinical diagnosis of emphysema was made. The above three strains of drug-resistant Acinetobacter baumannii were from Hotan hospital, and the similarity coefficient was 99%. It showed that the same clonal strain existed in the patient standard of ICU 20 days after discharge of the former infected patient and 1 month after discharge, and the multi drug-resistant Acinetobacter baumannii with homology was still detected in the patient specimens of the same department. It is suggested that the environmental sanitation disinfection of the ward is not complete, and the multi drug resistant Acinetobacter baumannii cannot be completely killed: this clone strain is an epidemic strain in Hotan area, and there are 6 strains in Changji area. It belongs to type 4 clonal strain, and all strains are from ICU. The difference between hospital and discharged patients is 45 months. The specimen is sputum. The clinical diagnosis of severe pneumonia and lung infection: it indicates that there is cross infection between ICU patients, indicating that Changji and Hotan regions have homology, and it is also the main epidemic strain in Changji region. At the same time, the drug resistance rate of type 1 and type 3 clones was compared, and type 3 was slightly higher than type 1.
In this experiment, 8 biofilm related genes and several significant resistance efflux pump genes of Acinetobacter baumannii isolated from clinical samples were amplified by PCR to explore the potential correlation between tigecycline resistance and biofilm formation ability. This study indicates that the multidrug resistance group increased the transcription level of BFS genes and the corresponding biofilm formation ability. BFS is closely related to the formation of biofilms. The drug resistance rate of the BFS gene positive group was higher than that of the relative gene negative group (chi square test, P<0.05). Consistent with this, the expression level of the efflux pump gene AdeB in the multidrug-resistant Acinetobacter baumannii group was significantly higher than that in the non resistant group. Therefore, it can be considered that the multidrug-resistant Acinetobacter baumannii isolated clinically in our hospital is significantly correlated with BFS. Drug resistance is mainly caused by the efflux pump genes adeB and bfs. However, the potential regulatory mechanisms of these two genes at the transcriptional level need further explanation.
In conclusion, analyzing the epidemic characteristics of clonal strains in Xinjiang, local (state) hospitals should attach great importance to monitoring Acinetobacter baumannii in the ward environment, especially when it is necessary to transfer hospitals and departments: cut off the spread and scattered transmission of multidrug-resistant Acinetobacter baumannii in Xinjiang, hospitals, departments and wards, and prevent cross infection.
Funding
This research was funded by Xinjiang Uygur Autonomous Regional Science and Technology Support Program (2022E02118)
References
- Shakibaie, M.R.; Modaresi, F.; Ghaemi, T.M.M. Amphiphilic peptide mastoparan-b induces conformational changes within the adeb efflux pump, down-regulates adeb gene expression, and restores antibiotic susceptibility in an mdr strain of acinetobacter baumannii. Proteins: Structure, Function, and Genetics 2023, 91, 1205–1221. [Google Scholar] [CrossRef] [PubMed]
- Yang, F., Wei, Y., Sun, C., Yuan, M., Zeng, W., & Liu, C., et al. (2022). Pinoxaden degradation characteristics of acinetobacter pittobacter and prediction of related genes. Microbiology. [CrossRef]
- 3. Mendoza Cedeno, L. G. M. , Pincay Cantos, M. F. P. , & Giler-Molina, Jose MiguelZambrano Cedeno, Ider Josue Zambrano. (2022). Influence of bacterial microbiota on the organic matter content of shrimp pond soil. journal of ecological engineering, 23(12), 21-28. [CrossRef]
- Chen, C., Huang, P. Y., Cui, C. Y., He, Q., Sun, J., & Liu, Y., et al. (2022). Classification and molecular characteristics of tet(x)-carrying plasmids in acinetobacter species. Frontiers in Microbiology, 13. [CrossRef]
- Melike, G.; Ayegül, S.S. Combined in silico approach and whole genome sequencing: acinetobacter baumannii st218 isolate harboring adc-73 β-lactamase which has a similar c-loop with adc-56 and adc-68 β-lactamase. Journal of molecular graphics & modelling 2022, 114, 108195. [Google Scholar] [CrossRef]
- Gautam, L. K., Sharma, P., & Capalash, N.. (2022). Structural insight into substrate binding of acinetobacter baumannii polyphosphate-amp phosphotransferase (ppk2), a novel drug target. Biochemical and Biophysical Research Communications. [CrossRef]
- Castro-Jaimes, S.; Guerrero, G.; Bello-López, E.; Cevallos, M.A. Replication initiator proteins of acinetobacter baumannii plasmids: an update note. Plasmid 2022, 119–120, 102616. [Google Scholar] [CrossRef] [PubMed]
- Chen, Q. , Zhou, W. , Cheng, Y. , Wang, G. , San, Z. , & Guo, L. , et al. (2024). Four novelacinetobacter lwoffiistrains isolated from the milk of cows in china with subclinical mastitis. BMC Veterinary Research, 20(1). [CrossRef]
- Gautam, L.K.; Sharma, P.; Capalash, N. Structural insight into substrate binding of acinetobacter baumannii polyphosphate-amp phosphotransferase (ppk2), a novel drug target. Biochemical and biophysical research communications 2022, 626, 107–113. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, N. , Singh, A. , Gupta, A. , Pant, P. , Singh, T. P. , & Sharma, S. , et al. (2022). Discovery of the lead molecules targeting the first step of the histidine biosynthesis pathway of acinetobacter baumannii. Journal of chemical information and modeling(7), 62. [CrossRef]
- Vered, S., Adi, C., & Yehuda, C.. (2024). Tailoring interventions for control of endemic carbapenem-resistant acinetobacter baumannii: an interrupted time series analysis. Open Forum Infectious Diseases(6), 6. [CrossRef]
- 12. Sabry, M. M. , El-Halawany, A. M. , Fahmy, W. G. , Eltanany, B. M. , Pont, L. , & Benavente, F. , et al. (2024). Evidence on the inhibitory effect ofbrassicaplants againstacinetobacter baumanniilipases: phytochemical analysis, in vitro, and molecular docking studies. BMC Complementary Medicine and Therapies, 24(1). [CrossRef]
- María Pérez-Varela, Singh, R., Colquhoun, J. M., Starich, O. G., Tierney, A. R. P., & Tipton, K. A., et al. (2024). Evidence for rho-dependent control of a virulence switch in acinetobacter baumannii. mBio, 15(1). [CrossRef]
- Yoon, J.G.; Lim, S.; Hyun, H.J.; Seong, H.; Noh, J.Y.; Song, J.Y.; et al. Respiratory microbiome and clinical course of carbapenem-resistantacinetobacter baumanniipneumonia in critically ill patients. Medicine 2024, 103, e38988-63. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Gene expression level of biofilm.
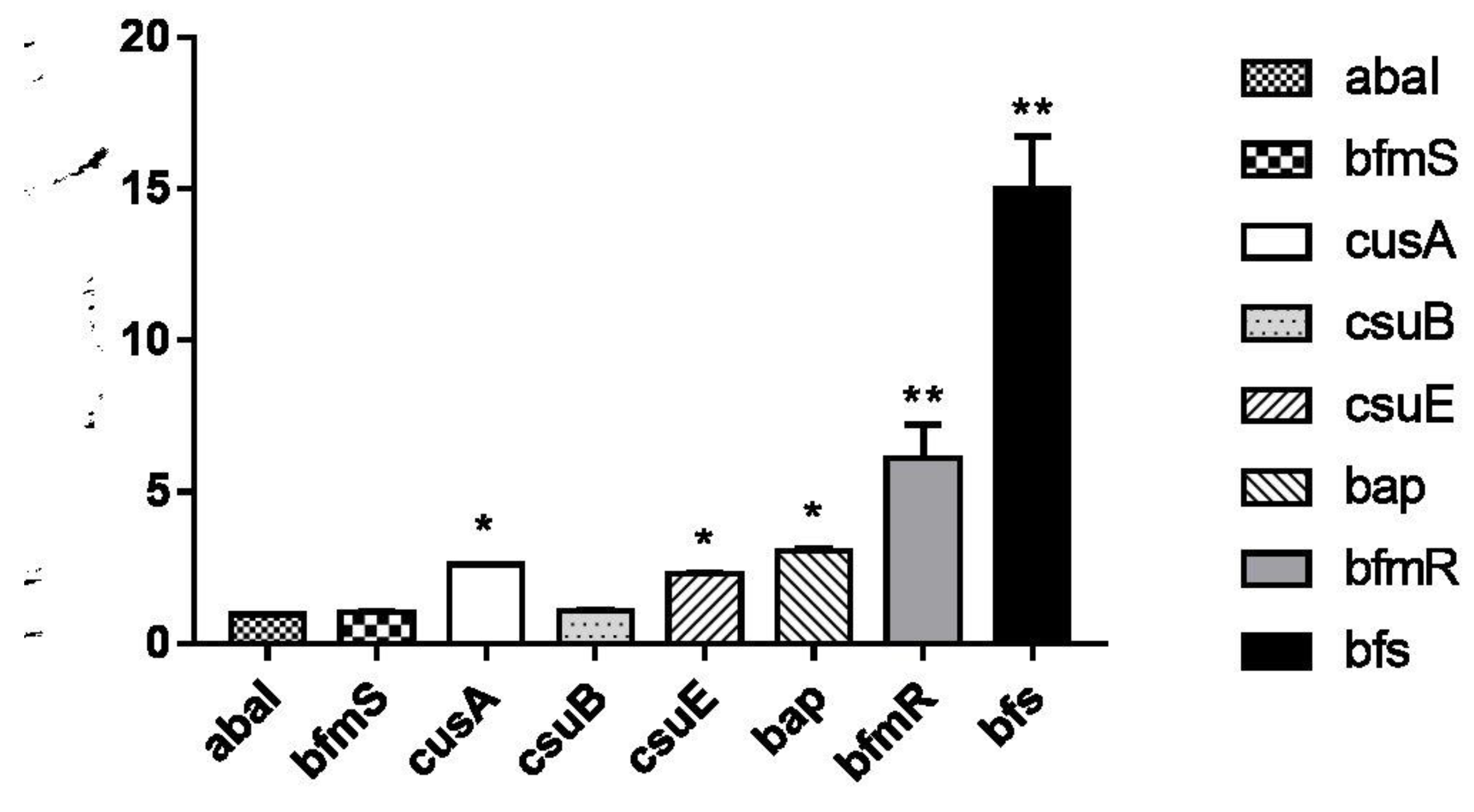
Figure 2.
Comparison of expression levels of carbapenem resistance and multidrug resistance genes.
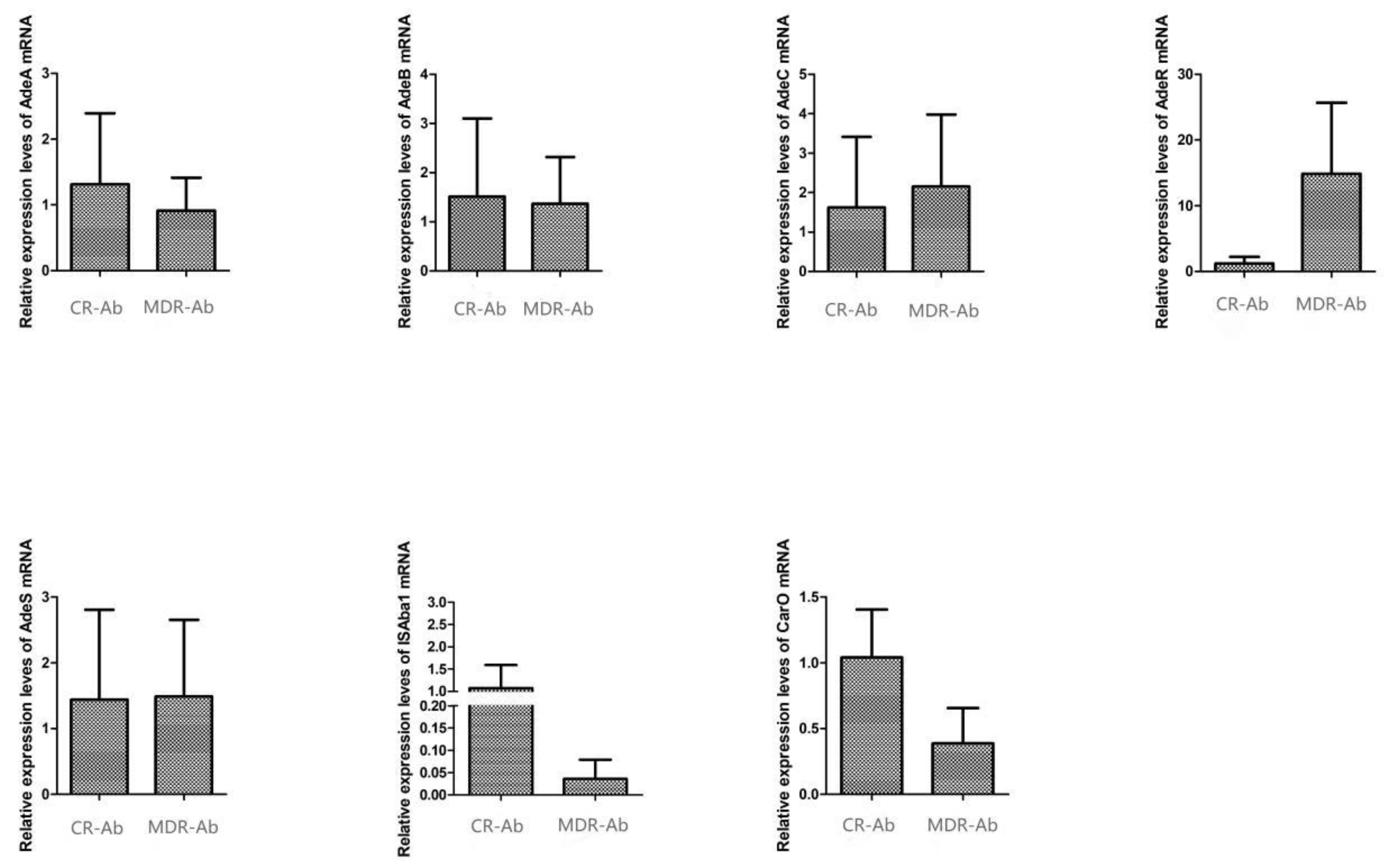

Table 1.
Primers for genes.
| Genes | 5’-3' | product length |
| blaOXA-23 -F | GATCGGATTGGAGAACCAGA | 501 |
| blaOXA-23 -R | ATT TCTGACCGCATT TCCAT | |
| blaOXA- 51 -F | TAATGCTTTGATCGGCCTTG | 353 |
| blaOXA- 51 -R | TGGATTGCACTTCATCTTGG | |
| blaOXA- 58 -F | AAGTATTGGGGCTTGTGCTG | 599 |
| blaOXA- 58 -R | CCCCTCTGCGCTCTACATAC | |
| adeB(16)-F | ATTCGTCGTCCTGTTTTTGC | 271 |
| adeB(126)-R | CGGAGCTACACTTGGAAAGC | |
| adeA(118)-F | ATTCAACCGCAATCGGTAAA | 280 |
| adeA(260) -R | GCTTGCCCTGCTCTAACTTC | |
| AdeC 2F(AN) | TGTCGAAATCGGCAACTGTA | 310 |
| AdeC 159R(AN) | TTGTTCAGCAATCGTTTTTCC | |
| adeRS_1F(an) | ATGTTCGATCATTCTTTTTCTTTTG | 272 |
| adeRS_1849R(an) | TTACTAATCCATAGAAATTTTTATG | |
| abaI-F | GTACAGTCGACGTATTTGTTGAATATTTGGG | 382 |
| abaI-R | CGTACGTCTAGAGTAATGAGTTGTTTTGCGCC | |
| bap-F | CGTTTCCTGGGTCTGATGTATT | 942 |
| bap-R | GTTATTGAAGGCTTCTTTAGTG | |
| bfmS-F | F:CGTATGCATCAGGTCGAC | 355 |
| bfmS-R | R: ACAGACAAAAGCCTGCC | |
| bfmR-F | CACCATGAGCCAAGAAGAAAAG | 750 |
| bfmR-R | GACCAACCTTATAGGAAG | |
| bfs-F | GCGCATATGAAAAATGATGCAAATATC | 490 |
| bfs-R | GCGCTCGAGTCATTTCAAATCATATCGAG | |
| csuAB-F | ATGAATATGAAAAACATTCA | 530 |
| csuAB-R | TTAGAAATTTACAGTGACTA | |
| csuE -F | CATCTTCTATTTCGGTCCC | 372 |
| csuE -R | CGGTCTGAGCATTGGTAA | |
| DNA-N-F | TTTGGCTTCCTCTACTTC | 500 |
| DNA-N-R | CATCTTGTTCAGGGTTAT |
Table 2.
Susceptibility profile of 72 multi-drug resistant Acetobacter baumannii strains.
| Antimicrobial agent | Acinetobacter baumannii (n=72) | |
| R | S | |
| Cefoperazone-sulbactam | 95.8 | 4.2 |
| Piperacillin-tazobactam | 100 | 0 |
| Trimethoprim- sulfamethoxazole | 40.3 | 59.7 |
| Ceftazidime | 100 | 0 |
| Cefepime | 100 | 0 |
| Amikacin | 100 | 0 |
| Gentamicin | 100 | 0 |
| Imipenem | 100 | 0 |
| Meropenem | 100 | 0 |
| Ciprofloxacin | 100 | 0 |
| Minocycline | 20.8 | 79.2 |
| Tigecycline | 2.7 | 97.3 |
| Polymixin B | 1.4 | 98.6 |
Table 3.
Homology among the 72 clinical strains of multidrug-resistant Acinetobacter baumannii isolated from Xinjiang and the related infections.
Table 3.
Homology among the 72 clinical strains of multidrug-resistant Acinetobacter baumannii isolated from Xinjiang and the related infections.
| Bacterial clone (No. of strains) | City | n | Sickroom | n | Specimen | n | Diagnosis | Number of patients |
| 1 (43) | Urumqi | 20 | SICU | 12 | Blood | 4 | Burns | 4 |
| Secretions | 6 | Burns | 1 | |||||
| Burns | 4 | |||||||
| Electric injury | 1 | |||||||
| Catheter tip | 2 | Burns | 2 | |||||
| RICU | 5 | Sputum | 2 | Severe pneumonia | 2 | |||
| Pulmonary infection | 1 | |||||||
| Blood | 2 | Severe pneumonia | 2 | |||||
| NSICU | 1 | Blood | 1 | Cerebralinfarction | 1 | |||
| Burns | 2 | Secretions | 2 | Burns | 1 | |||
| Electric injury | 1 | |||||||
| Aksu | 5 | ICU | 5 | Sputum | 5 | Severe pneumonia | 2 | |
| Pulmonary infection | 2 | |||||||
| Community pneumonia | 1 | |||||||
| Turpan | 4 | ICU | 4 | Sputum | 4 | Severe pneumonia | 2 | |
| Tuberculous meningitis | 1 | |||||||
| Cerebrel hemorrhage | 1 | |||||||
| Korla | 4 | ICU | 4 | Sputum | 4 | Tuberculous meningitis | 1 | |
| Severe pneumonia | 1 | |||||||
| Pulmonary infection | 2 | |||||||
| 3 (12) | Kashi | 3 | ICU | 3 | Sputum | 3 | Pulmonary infection | 3 |
| Ili | 3 | ICU | 3 | Sputum | 3 | Pulmonary infection | 2 | |
| Cerebrel hemorrhage | 1 | |||||||
| Shihezi | 2 | ICU | 2 | Alveolar lavage | 1 | Pulmonary infection Severe pneumonia | 1 | |
| Sputum | 1 | 1 | ||||||
| Changji | 1 | ICU | 1 | Sputum | 1 | Severe pneumonia | 1 | |
| Hotan | 1 | Respiratory | 1 | Sputum | 1 | Emphysema | 1 | |
| Urumqi | 12 | Burns | 7 | Catheter tip | 4 | Burns | 3 | |
| Scald | 1 | |||||||
| Sputum | 2 | Burns | 2 | |||||
| Secretions | 1 | Electric injury | 1 | |||||
| Blood | 3 | Burns | 3 | |||||
| SICU | 4 | Drain fluid | 1 | Spinal stenosis | 1 | |||
| ICU | 1 | Sputum | 1 | Pulmonary infection | 1 | |||
| 4 (9) | Changji | 6 | ICU | 6 | Sputum | 6 | Severe pneumonia | 4 |
| Pulmonary infection | 2 | |||||||
| Hotan | 3 | Respiratory | 2 | Sputum | 2 | Pulmonary infection | 1 | |
| Emphysema | 1 | |||||||
| ICU | 1 | Sputum | 1 | AECB | 1 | |||
| 2 (8) | Urumqi | 6 | SICU | 2 | Alveolar lavage | 2 | Radius fracture | 1 |
| Thoracic vertebral fracture | 1 | |||||||
| RICU | 3 | Sputum | 1 | Severe pneumonia | 1 | |||
| Secretions | 2 | Severe pneumonia | 1 | |||||
| Acute pancreatitis | 1 | |||||||
| NSICU | 1 | Blood | 1 | Cerebrel hemorrhage | 1 | |||
| Hotan | 2 | Respiratory | 2 | Sputum | 2 | Severe pneumonia Pulmonary infection | 1 | |
| 1 |
Table 4.
Susceptibility profiles of Clone 1 and Clone 3 multidrug resistant Acinetobacter baumannii strains.
Table 4.
Susceptibility profiles of Clone 1 and Clone 3 multidrug resistant Acinetobacter baumannii strains.
| Antimicrobial agent | Clone 1 A. baumannii (n=43) | Clone 3 A. baumannii (n=12) | ||
| R | S | R | S | |
| Cefoperazone-sulbactam | 76.6 | 23.4 | 83.3 | 16.7 |
| Piperacillin-tazobactam | 100 | 0 | 100 | 0 |
| Trimethoprim- sulfamethoxazole | 34.9 | 65.1 | 41.7 | 58.3 |
| Ceftazidime | 100 | 0 | 100 | 0 |
| Cefepime | 100 | 0 | 100 | 0 |
| Amikacin | 100 | 0 | 100 | 0 |
| Gentamicin | 100 | 0 | 100 | 0 |
| Imipenem | 100 | 0 | 100 | 0 |
| Meropenem | 100 | 0 | 100 | 0 |
| Ciprofloxacin | 100 | 0 | 100 | 0 |
| Minocycline | 20.9 | 79.1 | 25 | 75 |
| Tigecycline | 0 | 100 | 16.7 | 83.3 |
| Polymixin B | 0 | 100 | 8.3 | 91.7 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



