Submitted:
05 November 2024
Posted:
05 November 2024
You are already at the latest version
Abstract
Tracheotomy as an emergency surgical procedure appeared and developed in ancient times1. The surgical techniques for its performance in our time have reached a level of perfection, and in adults it is one of the most frequent surgical procedures performed in emergency and intensive care units worldwide.
Children's tracheotomy, on the other hand, presents far more serious challenges to the medical teams involved in its performance. A number of issues related to it - indications and contraindications, time for performance and protocols for decannulation and others are still subject to clarification.
In the past years, the development of medical science, the introduction of vaccination programs, the use of many improved medical materials and technologies, as well as the achievements of neonatal and pediatric intensive care practice, have shifted the emphasis of pediatric tracheotomy from its emergency performance to solve an acute asphyxiation problem, to its implementation in children, representing a complex group of patients, with permanent dependence on tracheostomy and related medical technologies for long-term survival2.
There are a growing number of children who have experienced complex therapy, for whom tracheostomy care and mechanical ventilation2, including at home environment, are part of their care. This, in turn, puts new questions on the agenda: who will take care for the child in the early postoperative period and during the days of hospitalization afterwards, who will train the people who will care for the tracheotomized child at home, what precautions should be applied in these children during their daily activities – eating, bathing, playing inside and outside the home and others.
Keywords:
planned tracheotomy in children
; hospital and home care
1. Introduction
Children's tracheotomy is a procedure of great complexity due to the huge number of questions and emerging problems related to it, starting from indications and contraindications assessment for its performance in each child, going through the choice of an exact surgical method for its implementation and reaching the care of the tracheotomized child in all their complexity, comprehensiveness and incessantness.
There are two main stages in the care of the young tracheotomized patient – care in the medical facility and care at home, the former being mainly performed by trained medical personnel, therefore, although more complicated, they represent a smaller problem, while the latter are most often performed by the child's parents or people with non-medical training took over the care of the child after its discharge from the medical facility, usually after a short training course [3].
From a physiological point of view, the tracheostomy is a pathological opening of the neck, allowing air to enter the trachea, bronchi and lungs without passing through the upper respiratory tract, where it is warmed and moistened [2]. Therefore, the air inhaled through the cannula must be warmed and moist. This helps to avoid discomfort, thickening of secretions and formation of a mucus plug [1]. To humidify the inhaled air, a passive humidifier (artificial nose’) [2,4] can be used, which captures the water vapor and temperature exhaled by the child and transmits part of them to the inhaled air. The effect of using humidifiers in children is good, and their tolerance by the child in most cases is problem-free.
Since the cough reflex is usually absent in tracheotomized children, the collected secretions must be aspirated regularly, and atraumatically/care is taken not to injure the inner surface of the trachea/. The aspiration frequency is strictly individual and relies on the "as needed" principle. In the first days after tracheotomy, the child needs more frequent aspiration of secretions, and gradually the aspiration decreases, but not less than twice a day [4,5]. The aspiration pressure is usually between 80 and 150 mm Hg. Its measurement is essential for the effectiveness and safety of tracheal aspiration. For routine suction, a catheter with outer diameter approximately 50% of the tube’s lumen is used, and if rapid removal of secretions is needed, catheter with outer diameter of approximately 75% of the lumen is used [4].
There is a greater tendency for respiratory tract infection and foreign body aspiration after tracheostomy. Therefore, aspiration catheters should be changed frequently (single use only if possible) and the rules of aseptic should be observed during aspiration to prevent possible infection. Care should be taken to prevent foreign bodies falling into the tracheostomy opening.
Caring for a tracheostomized child, and especially for the tracheostomy opening of a pediatric patient, is a 24/7 stressful commitment. This care begins the moment the child leaves the operating room and can be divided into hospital care and home care.
1.1. Care at Hospital
It is desirable to create a team of nurses, doctors and respiratory therapists in order to manage all situations (from harmless to high-risk) related to the tracheostomy even before the surgery is carried out. This team discusses all tracheostomy related issues - humidification and aspiration (frequency and depth), behavior algorithm in case of accidental decannulation (switching to endotracheal intubation or reinsertion of the cannula and its fixation to the skin with several stitches) and others.
The first change of the cannula is usually done a week after its placement in order to give the tracheostomy time to "mature" [2,3]. This first change is usually done by the surgical team that performed the tracheostomy, and the team that will take care of it usually(as a rule) observes the procedure. The team must be ready for possible intubation if the airway is lost during the shift due to inability to reinsert the cannula. The ties and gauze pad should be replaced with new ones every daiy or more often if necessary. The frequency of changing the cannula varies widely, depending directly on care taken - aspiration and humidification.
Children can be fed soon after the surgery – as soon as they fully wake up from anesthesia. Some of them may lose certain reflexes and feeding may be difficult - this necessitates the placement of a feeding tube for a certain period of time.
Tracheotomized children lose ability to communicate through speech. The older ones use signs or writing. If its condition is stable, the child can phonate if the cannula (cannula without balloon) does not exceed 2/3 of the diameter of the trachea. In some patients, the ability to vocalize is observed when the cannula is occluded (cannula without balloon). Another way to preserve phonation is the use of fenestrated cannulas, which are not recommended in the early postoperative period.
Both the team performed the tracheotomy and the care team perform daily assessment of the tracheostomy condition, watching for signs of an emerging complication - bleeding, inflammation, etc.
Simultaneously with the care of the child, the training of the parents (the people who will nurse the child outside the hospital) begins [3], and in many cases they themselves need psychological support. Education is started preferably before elective tracheotomy [4].
Children should not be discharged from the hospital until their parents or caregivers have been trained in all routine care procedures and in providing emergency care in life-threatening situation[4,6].
1.2. Care at Home
The care of a child with a tracheostomy at home is usually taken over by his parents/guardians, and for children raised in orphanages or other social facilities by the staff of the respective institution. Despite the preliminary training, the commitments related to the care of the small patient have severe physical and especially psychological influence on them, especially in the first days and weeks after discharge. Happily gradually solving the problems surrounding raising a child with a tracheostomy is becoming a routine and the pressure decreases. In a number of countries, home care is provided by nurses by law.
When a child with a tracheostomy is discharged from hospital, the medical team is required to provide a list of the necessary items for the care of the tracheostomy and cannula [7]. The most basic consumables are spare cannulas, gauzes, canula bandages, plasters, syringes, tweezers, scissors, aspiration catheters, sterile and non-sterile gloves, saline solution and local antiseptics. The necessary equipment includes a mobile aspiration pump, air humidifier, oxygen source, saturation monitor and, in a few cases respiratory device may also be necessary.
How often the cannula must be changed is an important question. In children, it is generally accepted that the change is carried out once a week [2], although the need for this is strictly individual - in some patients it is necessary to change more often, in others much less often. This mostly depends on the material of the tube and the presence of infection and/or secretions [4].
The life of modern tracheostomy tubes is usually 4-6 months, after that they have to be thrown away and replaced with new ones. When children with a tracheostomy are raised at home, their parents should always have spare tracheostoma tubes available for emergency situations: first identical to the one currently in use, and second – with diameter one size smaller.
The tracheostoma tube ties have to be changed daily and immediately after contamination or wetting. After tying the new ties, it should be possible for the attendant to slip a finger under them without difficulty [4]. Over-tightening the tracheostoma tube ties over the child's neck quickly and easily leads to complications (Figure 1 and Figure 2).
Proper care of the tracheostomy is essential. The skin around the stoma opening should be cleaned with damp, but not wet, clean cloth. Dried crusts under the tracheostoma tube plate are removed using saline-soaked swab.
Normal speech and language development require vocal exploration and social interaction, both of which are limited when a tracheostomy tube is in place, especially in an infant. The best way for dealing with that problem is the use of speaking valves [2,7].
The pad (usually gauze) that is placed under the cannula to prevent tracheostomy opening trauma (Figure 3) is changed daily or when it gets wet or soiled.
Many of the daily activities associated with raising a child are additionally complicated by the presence of a tracheostomy, including feeding. The main problem in most cases is the possibility of food particles getting in the vicinity of the tracheostomy opening and their aspiration. Water and other liquids (milk) intake should also be done carefully, otherwise a large amount of liquid may be aspired with subsequent respiratory problems. That is why it is absolutely contraindicated to let these children eat and drink liquids without adult supervision [4].
Bathing is one of the most enjoyable activities for parents and children. In cases with a tracheostomy, however, a number of problems arise again, related to water splashes entering the trachea and bronchi through the tracheostomy opening. It is generally recommended tracheostomized children to take bathe not shower, where it is much easier water drops to enter the cannula opening. To minimize this rick, collar waterproof protectors is recommended to be used [4] Figure 4.
Older tracheotomized children can take shower, as the placement of protective devices over the cannula opening is mandatory. Specially designed shower protectors are used, which are attached directly to the opening of the cannula and provide a high degree of protection against splashes of water entering its opening Figure №5.
Getting out of the house is also a challenge for a child with a tracheostomy. There he faces many problems and challenges not typical of the non-tracheotomized individual. Garden sprinklers, fountains, swimming pools, sandboxes should be avoided. Playing with furry animals as well as birds is also not a good idea due to the risk of particles getting into the cannula opening. Dust on the streets and buildings, polluted air, smoke, fog and pollens are irritants for him that should not be underestimated. Adequate protection from environmental factors can be achieved by using tracheostomy protectors. They are made of high quality breathable materials and are available in different sizes, shapes and colors Figure 6.
When the child is outside the environment in which it is raised, a set of tools and supplies necessary for tracheostomy care and emergency situations need to accompany it. It is recommended that this 'travel' service kit to be different from the kit used at the child's home to avoid the risk of forgetting or misplacing apparatus, instrument or consumable that may prove vital in an emergency situation.
Following the tracheostomized child taking care rulesin the hospital, at home, and outside helps minimize the risks associated with the tracheostomy and cannula, but does not eliminate them completely.
2. Discussion
Pediatric tracheotomy is a relatively rare surgical intervention with a literature incidence of 6.6 per 100,000.
Despite the huge number of articles on the subject, the only aspects related to it that are fully clarified are the indications, contraindications and methods of its performance. A large number of problems surrounding the performance of planned pediatric tracheotomy are still subject to discussion and clarifying – especially topics related to postoperativemand home care.
The increased number of tracheostomies in children with chronic diseases also suggests the real possibility that many of them will be discharged from the hospital with a cannula and raised at home.This raises questions such as who will serve the child and who will carry out the training and instruction of the relevant people - caregivers, people from social homes or, in the best case the parents of the small patient.
When a child with a permanent tracheostomy is nursed at home, problems of a socio-domestic and financial nature also arise [8], requiring the involvement of the state and social institutions with them. It is also increasingly urgent to pay attention to the issue of "indirect victims" of pediatric tracheotomy - the parents and relatives of the child, who in most cases need support themselves, especially in the first days, weeks and months after the intervention.
The problems surrounding the tracheotomized child in different countries receive a different response, and in the best case, the child is cared for by nurses and trained parents under periodic medical supervision, carried out by the team that performed the tracheotomy, furthermore the parents receive psychological, logistical and financial support from the social organizations or the state [3]. However, it is also the most expensive approach, inapplicable in the common case.
In our country, usually after short training, the child falls under the full care of his parents at home or the staff of the social institution who is caring for children with health problems, where, if it is lucky, a staff who have previous experience with tracheotomized children takes care of it too.
3. Conclusions
Much is being done worldwide to improve the quality of care given to tracheostomized children, and recent years they are more and more successful, due to the formation of multidisciplinary teams analyzing the full complexity of the problems connected to pediatric tracheostomy – starting from indications, contraindications and time for its implementation to training of the persons taking care for the child, preparation of the home environment in which he will be nursed, provision of psychological and financial support to him and his family [3]. If proper care is provided domiciliary tracheostomy care even in children is as safe as, and in many other aspects superior to, long-term hospitalisation [4].
References
- Lesley-Ann Cochrane, C. Martin Bailey; Surgical aspects of tracheostomy in children; Paediatric respiratory reviews (2006) 7, 169–174.
- Watters K. F.; “Tracheostomy in Infants and Children”; Respiratory Care • June 2017 Vol. 62 No 6.
- Duncan B. W., Howell L. J., deLorimier A. A., Adzick N. S., Harrison M. R.; “Tracheostomy in Children with Emphasis on Home Care”; Journal of Pediatric Surgery, Vol27, No 4 (April), 1992: pp 432-435.
- Oberwaldner B., Eber E.;” Tracheostomy care in the home”; Mini-Simposium Tracheostomy in children, Pediatric Respiratory Reviews (2006) 7, 185–190; Elsevier.
- Davis G. M.; “Tracheostomy in children”; Pediatric Respiratory Reviews (2006) 7S, S206–S209; Elsevier.
- Kohn J., McKeon M., Munhall D., Blanchette S., Wells S., Watters K.; “Standardization of pediatric tracheostomy care with “Go-bags””; International Journal of Pediatric Otorhinolaryngology Volume 121, June 2019, Pages 154-156.
- Deutsch E. S.; Tracheostomy: Pediatric Considerations; Respiratory Care • August 2010 Vol 55 No 8.
- Hopkins C., Whetstone S., Foster T., Blaney S., Morrison G.; “The impact of pediatric tracheostomy on both patient and parent”; International Journal of Pediatric Otorhinolaryngology (2009) 73, 15—20.
- Gower W. A., Golden S. L., King N. M. P., Nageswaran S.; “Decision-Making About Tracheostomy for Children With Medical Complexity: Caregiver and Health Care Provider Perspectives”; Article in Press - Academic Pediatrics Vol 000 xx2020, accepted June 6, 2020.
- Amin R. S., Fitton C. M.; “Tracheostomy and home ventilation in children”; Seminars in Neonatology (2003) 8, 127–135; Saunders.
- Edwards E. A., O’Toole M., Wallis C.;” Sending children home on tracheostomy dependent ventilation: pitfalls and outcomes”; Arch Dis Child 2004;89:251–255.
- Fraga J. C., de Souza J. C. K., Kruel J.; “Pediatric tracheostomy”; J Pediatr (Rio J). 2009;85(2):97-103.
- Perez-Ruiz E., Caro P., Perez-Frıas J., Cols M., Barrio I., Torrent A., Garcıa M. A., Asensio O., Pastor M. D., Luna C., Torres J., Osona B., Salcedo A., Escribano A., Cortell I, Gaboli M., Valenzuela A., Alvarez E., Velasco R., Garcıa E.;” Paediatric patients with a tracheostomy: a multicentre epidemiological study”; Eur Respir J 2012; 40: 1502–1507.
- Serra A., Cocuzza S., Longo M. R., Grillo C., Bonfiglio M., Pavone P.;” Tracheostomy in childhood new cases for an old strategy”; European Review for Medical and Pharmacological Sciences, 2012; 16: 1719-1722.
- Veder L. L., Joosten K. F. M., Zondag M. D., Pullens B.; “Indications and clinical outcome in pediatric tracheostomy: Lessons learned”; International Journal of Pediatric Otorhinolaryngology 151(2021) 110927.
- Wood D., McShane P., Davis P.; “Tracheostomy in children admitted to paediatric intensive care”; Arch Dis Child 2012;97:866–869. doi:10.1136/archdischild-2011-301494.
- Zenk J., Fyrmpas G., Zimmermann T., Koch M., Constantinidis J., Heinrich Iro H.; “Tracheostomy in young patients: indications and long-term outcome”; Eur Arch Otorhinolaryngol (2009) 266:705–711.
Figure 1.
and Figure 2 consequences of over-tightening the tracheostoma tube ties over the patient's neck.
Figure 1.
and Figure 2 consequences of over-tightening the tracheostoma tube ties over the patient's neck.
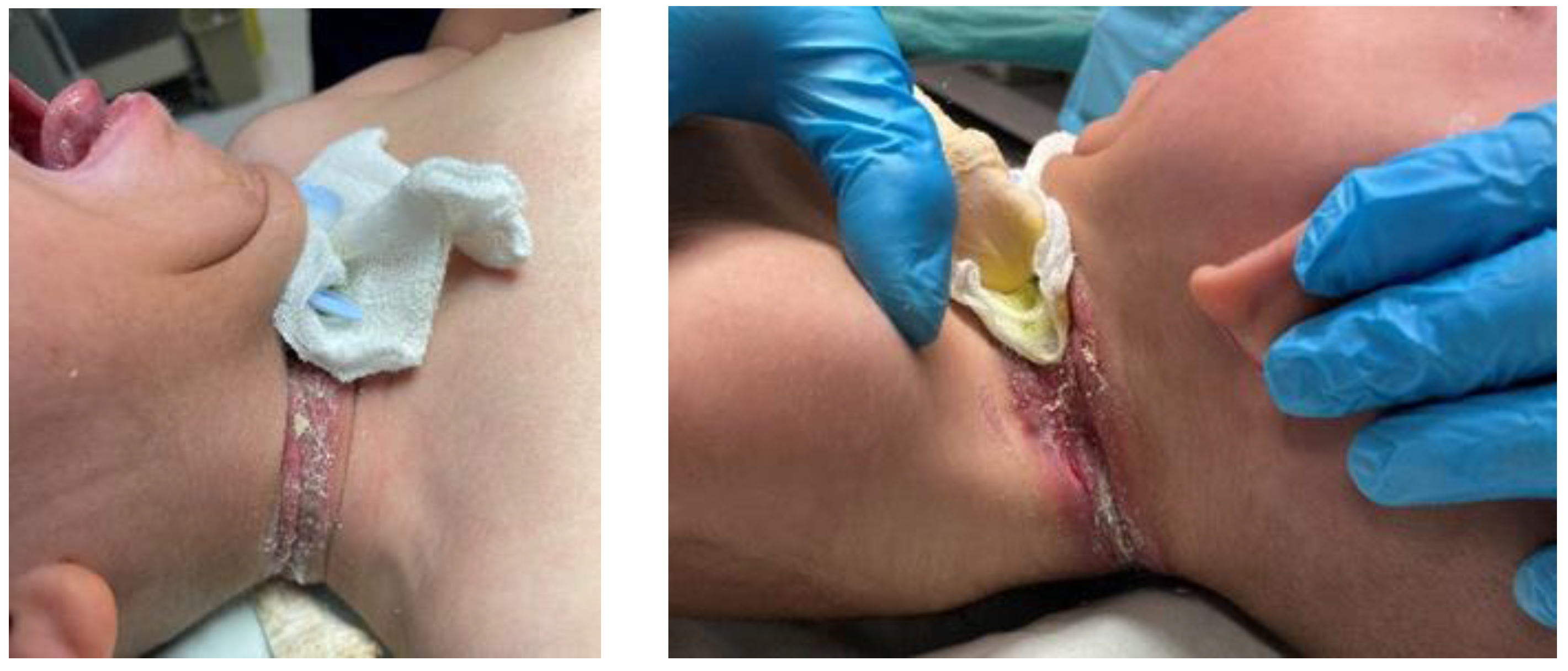
Figure 3.
Tracheostoma tube pads./Pictures from internet/.

Figure 4.
Collar waterproof protectors./Pictures from internet/.

Figure 5.
shower protectors for tracheostoma tubes./Pictures from internet/.
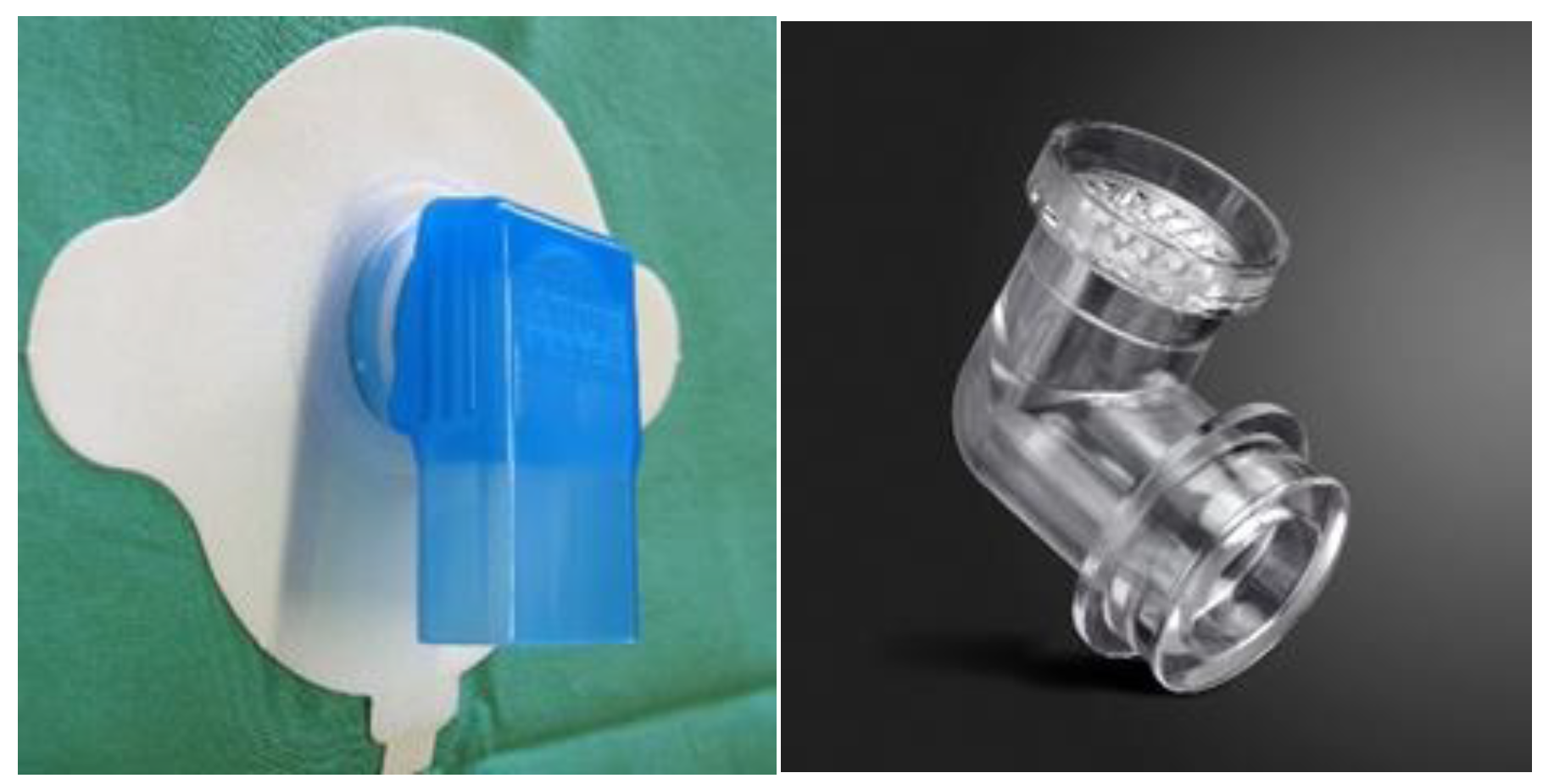
Figure 6.
Tracheostomy protectors./Pictures from internet/.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



