
Submitted:
04 November 2024
Posted:
06 November 2024
You are already at the latest version
Abstract
Objectives: To analyze the treatment options for peritonsillar abscess (PTA) in children.
Methods: We searched PubMed and EMBASE for studies regarding treatment of PTA in children. Relevant studies were reviewed based on systematic review (PRISMA) guidelines. A qualitative and quantitative analysis of the extracted data was performed.
Results: A total of 12 articles with 2211 cases of PTA were found eligible. All the identified studies were retrospective cohorts. The mean age varied from 8.5 to 15.4 years without gender difference. Treatment options included broad spectrum antibiotic therapy with incision and drainage of the abscess, needle aspiration and immediate tonsillectomy in 69%, 7.6% and 7% of cases, respectively. Antibiotics alone were administered to 16.4% of the subjects. Rate of recurrence of PTA after primary treatment ranged from 2% to 15.8% of cases. Time of recurrence is considered within one or two months. Complications in children with PTA were torticollis, prolonged fever, sepsis, dyspnea and parapharyngeal involvement.
Conclusions: The mainstay of treatment of PTA in children is antibiotic therapy with incision and drainage of the abscess. Alternatives include antibiotic treatment alone or in association with needle aspiration. Immediate tonsillectomy is reserved only a few high-risk patients.
Keywords:
peritonsillar abscess
; children
; treatment
; surgery
; review
Introduction
Peritonsillar abscess (PTA) is the most common deep neck infection in children [1]. It is defined as collection of pus between the tonsillar capsule, superior constrictor muscle and palatopharyngeus muscles. The usual course of developing PTA may result from suppuration of soft tissue due to an acute tonsillitis or pharyngitis. Infrequently, the obstruction of Weber’s gland located in the superior tonsillar pole may be the inciting factor [2]. In the vast majority of cases PTA is unilateral and affects most common adolescents.1
The infection often is polymicrobial, including aerobes and anaerobes. The most frequently cultured pathogens are Streptococcus pyogenes [3]. Although recurrent tonsillitis has been considered a risk factor for PTA, an association has not yet been demonstrated.4 Indeed, it is still unclear why in pediatric population there is a low incidence of PTA in the face of a high prevalence of tonsillitis [5].
The diagnosis is based on history, clinical evaluation and laboratory tests. In uncooperative child or in case of suspicious of extended abscess to parapharyngeal space additional a computed tomography (CT) scan may be needed [6]. Transcutaneous ultrasound can differentiate PTA from other tonsillar infections therefore, it has been considered useful in identifying patients who do not require surgery [7,8]. The most definitive diagnostic procedure for PTA is needle aspiration which can provide microbiological analysis and some drainage of the abscess. Surgical treatments consist of the incision and drainage (I&D) of the abscess that can be performed in local or general anesthesia depending on the age and cooperation of the patient and, in selected patients, the immediate tonsillectomy. Medical therapy involves hydration, pain control and, antibiotics such as amoxicillin/clavulanate or clindamycin and cefotaxime or piperacillin/tazobactam [9] which can be adjusted accordingly as bacterial sensitivities obtained from abscess culture. Corticosteroids can be also use to reduce the inflammation and edema of oropharynx and improve pain control although their indication is still controversial [2].
Untreated or neglected PTA can result in serious complications due to the spread of the infection such as airway compromise, aspiration pneumonia, mediastinitis, sepsis and jugular vein thrombosis [10].
There is still controversy surrounding the management of PTA in children with different proposed protocols [5,11] and a systematic literature review is lacking.
We perform this systematic review focused on the treatment of PTA in children in order to identify the current medical and surgical trends.
2. Materials and Methods
2.1. Search Strategy
A systematic review of the literature was completed. Literature search was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-analyses (PRISMA) guidelines [12]. PubMed and EMBASE databases were systematically searched through July, 2024. Searches were conducted by combining the following terms (“peritonsillar abscess”) AND (“children” OR “pediatric”) AND (“treatment” OR “therapy”). Bibliographies were searched for additional articles. The last search was performed on 30 September 2024. The review protocol was registered in the International Prospective Register of Systematic Reviews (PROSPERO; registration number: CRD42022302437).
2.2. Study Selection
Study eligibility criteria were applied independently by two authors (F.G. and W.G.). Any disagreements were resolved by consensus. Articles were selected in two phases, first screening titles and abstracts for those apparently meeting inclusion criteria, and then reading the full text of selected articles, excluding those that did not meet the review eligibility criteria.
Inclusion criteria: (1) Studies regarding the treatment of peritonsillar abscess in children (2) Studies published from 1990 in peer-review journals (3) English language. Exclusion criteria: (1) Reviews, meta-analyses, case reports, editorials, letters, meeting abstracts, personal comments or book chapters (2) Studies considering adult population (3) Studies reporting incomplete data.
2.3. Data Extraction
Data extraction from the included studies was performed and independently verified by F.G and W.G.
A standardized full-text analysis was performed and data were gathered on the main characteristics of the studies (first author, year of publication, type of study, number of cases of PTA, age, sex, symptoms, signs, microbiological findings) and concerning the type treatment (needle aspiration, I&D, tonsillectomy, antibiotics), recurrence (number and timing), complications and duration of follow-up.
2.4. Quality of Evidence Assessment
The Joanna Briggs Institute (JBI) critical appraisal checklist for case series assessment tools were used to appraise the quality of the studies (Tab. S1). Each item is rated yes, no, or unclear. A “yes” response was scored 1 point, and “no” and “unclear” responses were scored 0 points. For each case series, “Good” was defined as at least 7 out of 10 criteria met, “Fair” as 5 or 6 criteria met, and “Poor” as 4 or less criteria met (Tab. S2). The average score for each article was independently assessed by two authors (F.G. and G.W.), and discrepancies were resolved by consensus [13]. Overall, only studies with a “good” rating of the JBI of critical appraisal were included (Tab. S2).
2.5. Data Synthesis
We performed a qualitative and quantitative analysis of the extracted data. A meta-analysis providing statistical evidence was not achieved due to the heterogenicity and limited data of the included studies.
3. Results
Following a systematic review, 12 articles were finally included. The PRISMA flow diagram is shown in Figure 1.
All the included studies were retrospective. A total of 2211 children with PTA were included. Sample sizes among the studies ranged from 19 [14] to 777 [15]. As detailed in Table 1, mean age varied from 8.5 [16] to 15.4 [17] year and the male to female ratio is 1, 1 [4,15,16,18-22]. Seven studies reported clinical and microbiological data [11,14,16-19,23]. All patient complaint sore throat with or without drooling, fever, odynophagia, muffled voice and neck pain. The main oropharyngeal sign was unilateral peritonsillar bulge with uvular deviation associated with trismus and neck adenopathy. Two authors described airways compromise [17] and dehydration [11] The most frequent isolated bacterium was that beta-hemolytic Streptococcus group A and mixed flora with or without anaerobes.
Treatment modalities, recurrences and complications are described in Table 2. I&D, needle aspiration and immediate tonsillectomy were performed in 1372, [4,11,14,15,18-22] 153 [4,14,19,23] and 139 [4,11,14-16,20,23] subjects, respectively. Antibiotics alone were administrated to 328 children [11,16,19,20,23]. Three authors did not specify the surgical treatment modalities [16,17,20] and only two authors reported the type of antibiotic therapy [4,20].
The percentage of different types of surgical treatment modalities for PTA is shown in Figure 2.
Seven authors reported the rate of recurrence of PTA after primary treatment [11,14,15,17,18,20,21] ranging from 2% [20] to 15.8% [18] of cases depending on the studies. Time of recurrence is considered within one [18,21] or two months [17].
Four authors described complications in children with PTA: torticollis, prolonged fever, sepsis, dyspnea and parapharyngealinvolvement [14,15,18,20]. Only three authors specified the duration of follow-up ranged from one month [15,18] to two years [14].
Figure 3 shows a treatment algorithm for PTA in children.
4. Discussion
As a result of this review, in the evaluation of treatment options for pediatric PTA, antibiotic therapy associated with the I&D of the abscess was the modalities of choice (69% of cases) (Figure 2). This procedure involves an incision in the mucosa superior to the tonsil and the drainage of the abscess. Due to inability of children to cooperate, this procedure may require treatment in the operating room in up to half of cases [11,24]. However, especially in older children, it can be performed in a controlled setting such as the emergency department with a proper equipment [2,18].
Considering the others treatment options, we found that antibiotics alone, needle aspiration and tonsillectomy were performed in 16.4%, 7.6%, and 7% of cases, respectively (Figure 2). Supporting our results, a US national survey including 20546 subjects found a significant increase in the rate of I&D from 26.4% to 33.7% (p<0.001) and a significant decrease in the rate of tonsillectomy from 13.8% to 7.8% (p<0.001) [24,25]. Differently, Nguyen et al., in a retrospective study including 2994 patients who presented with peritonsillar cellulitis or abscess found that the most common treatment of choice was medical therapy alone (30.8%), followed by I&D (30.5%) and tonsillectomy (9.4%) [25,26].
Antibiotic therapy alone is a valid option and, as reported by Kim et al., the predictive factors of its efficacy were: younger patients, fewer episodes of acute tonsillitis, and smaller abscess size [16]. However, Hsiao et al. comparing children with PTA receiving surgical (n=48) and non-surgical procedures (n=8), found that children with antibiotic treatment alone were younger and had a longer duration of hospital stay (5.7 vs 8.1 p<0.001) [20]. To date, there are no studies that compare the effectiveness of different types of antibiotics used as sole therapy.
Needle aspiration as treatment modality for PTA appears to be an efficacious and safe method [19,23]. Weinberg et al. treated 41 children and resolved the infection in 87% of cases. Two patients needed to repeat aspiration (6%) and two underwent to immediate tonsillectomy (6%) for persistent abscess. No complications have been described [23]. Though injury of internal carotid artery (ICA) is a feared complication during needle aspiration, it has never been reported in medical literature. Some authors advocated the use of transoral ultrasound which helps visualize important neighboring structures such as ICA and avoid this possible adverse event [26,27].
Immediate tonsillectomy, also known as quinsy tonsillectomy, is rarely indicated. It allows the complete drainage of abscess and avoidance any recurrence. Controversy over the indications remains due to the unclear balance between surgical risks and benefits [24,27]. Most authors suggest to perform immediate tonsillectomy in case of failure of I&D, recurrent PTA, recurrent tonsillitis and obstructive sleep apnea symptoms [11,14,18]. However recently, Rosi-Schumacher et al. studying 777 children treated for PTA found that for quinsy tonsillectomy versus I&D there was no statistically significant difference in length of stay (1.9 v. 1.7 days, p=.523), readmission (17 v. 0, p=.265) or return to the operating room (18 v.1, p=.810). Therefore, they considered quinsy tonsillectomy a good option in case of PTA or recurrent tonsillitis [15].
In order to improve the decision-making process for the treatment of PTA in children we proposed an algorithm that shows the different therapeutic approaches (Figure 3). As previously described by Schraff et al. the treatment decision is based on the level of cooperativeness of the child and previous history of adenotonsillar disease [11].
Few authors have studied the recurrence rate of PTA reporting a ranged between 2% [20] to 15.8% [18] with time of recurrence within one [18,21] or two months [17]. Allen et al. studying 566 pediatric PTA found that recurrence was associated with older age (p=0.005) and history of recurrent tonsillitis (p<0.0001). They also noted that there was not a statistically difference in term of recurrence for patients managed in the outpatient than inpatient setting [21].
Chang BA et al. in a systematic review including 674 participants (adults and children) compared the effectiveness of needle aspiration and I&D for the treatment of PTA. They found that very low-quality evidence suggested that I&D may be associated with a lower chance of recurrence than needle aspiration and that there was very low-quality evidence to suggest that needle aspiration was less painful [28,29].
Considering the characteristics of the population studied, we found that PTA affects mainly adolescents without a gender difference. Typical symptoms (sore throat, fever, odynophagia, muffled voice and neck pain) and signs (unilateral peritonsillar bulge with uvular deviation, trismus and neck adenopathy) allow to PTA diagnosis (Tab. 1) even if some difficulties may be present in younger or uncooperative subjects [5]. Complications are described in case of severe abscess, untreated or non-responder patients [14,18,20]. Though rare, airways compromise and parapharyngeal involvement are the most critical conditions that may require an urgent management.
As detailed in Table 1, the microbiological aspect of PTA revealed that beta-hemolytic Streptococcus group A and mixed flora with or without anaerobes were the most frequently isolated germs. To date, there is no consensus on appropriate antibiotic therapy and most recommendations are based on studies on antibiotics sensitivities of microorganisms identified in the purulent secretion of PTA suggesting initial empiric therapy with a broad-spectrum antibiotic such as penicillin or amoxicillin/ac clavulanate with metronidazole [3]. Only two authors of the included studies reported the types of antibiotics used [4,20] therefore no conclusions could be drawn.
Therefore, considering the low level of the reviewed evidence, further studies comparing the different treatments options (needle aspiration, I&D, antibiotic therapy alone and immediate tonsillectomy) are needed to ensure the best possible care for children with PTA, especially in this era of increased antimicrobial resistance.
This review has some limitations. One, it includes only retrospective studies with a wide range of samples. Two, some of the included studies have incomplete data such as the evaluation of recurrences and the duration of follow-up. Three, only one of the included retrospective studies compared groups of children undergoing different treatment options.
5. Conclusions
Treatment of PTA in children is currently considered antibiotic therapy with the I&D of the abscess. Antibiotics alone or combined with needle aspiration may be a valid alternative option in selected patients. Rarely, immediate tonsillectomy can help in children with high risk of recurrence or airway obstruction. Future studies comparing the different treatment options may allow to define a validate protocol for the management of pediatric PTA.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1, The Joanna Briggs Institute Critical Appraisal Checklist; Table S2. The JBI Critical Appraisal Checklist of the included studies.
Author Contributions
Conceptualization, F.G. and W.G.; methodology, W.G.; software, F.G.; vali dation, F.G. and W.G.; formal analysis, W.G.; investigation, W.G.; resources, F.G.; data curation, F.G.; writing—original draft preparation, F.G.; writing—review and editing, F.G and W.G.; visualization, F.G.; supervision, W.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data extracted from the included articles are available in PubMed and EMBASE databases.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Novis SJ, Pritchett CV, Thorne MC, et al. Pediatric deep space neck infections in U.S. children, 2000–2009. Int J Pediatr Otorhinolaryngol 2014, 78, 832–836. [Google Scholar] [CrossRef]
- Baldassari C, K. Shah R. Pediatric Peritonsillar Abscess: An Overview. IDDT. 2012, 12, 277–280. [Google Scholar] [CrossRef] [PubMed]
- Slouka D, Hanakova J, Kostlivy T, et al. Epidemiological and Microbiological Aspects of the Peritonsillar Abscess. Int J Environ Res Public Health 2020, 17, 4020. [Google Scholar] [CrossRef] [PubMed]
- Segal N, El-Saied S, Puterman M. Peritonsillar abscess in children in the southern district of Israel. Int J Pediatr Otorhinolaryngol 2009, 73, 1148–1150. [Google Scholar] [CrossRef] [PubMed]
- Herzon FS, Nicklaus P. Pediatric peritonsillar abscess: Management guidelines. Current Problems in Pediatrics 1996, 26, 265–278. [Google Scholar] [CrossRef] [PubMed]
- Varelas AN, LoSavio PS, Misch E, et al. Utilization of emergency department computed tomography and otolaryngology consultation in the diagnosis of pediatric peritonsillar abscess. Int J Pediatr Otorhinolaryngol 2019, 117, 189–193. [Google Scholar] [CrossRef]
- Bandarkar AN, Adeyiga AO, Fordham MT, et al. Tonsil ultrasound: technical approach and spectrum of pediatric peritonsillar infections. Pediatr Radiol 2016, 46, 1059–1067. [Google Scholar] [CrossRef]
- Fordham MT, Rock AN, Bandarkar A, et al. Transcervical ultrasonography in the diagnosis of pediatric peritonsillar abscess: Transcervical US in Pediatric PTA. The Laryngoscope 2015, 125, 2799–2804. [Google Scholar] [CrossRef]
- Pong AL, Bradley JS. Guidelines for the Selection of Antibacterial Therapy in Children. Pediatric Clinics of North America 2005, 52, 869–894. [Google Scholar] [CrossRef]
- Rafei K, Lichenstein R. Airway Infectious Disease Emergencies. Pediatric Clinics of North America. 2006, 53, 215–242. [Google Scholar] [CrossRef]
- Schraff S, McGinn JD, Derkay CS. Peritonsillar abscess in children: a 10-year review of diagnosis and management. Int J Pediatr Otorhinolaryngol 2001, 57, 213–218. [Google Scholar] [CrossRef] [PubMed]
- Moher D, Liberati A, Tetzlaff J et al. The PRISMA Group. Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, e1000097.
- Munn Z, Barker TH, Moola S, et al. Methodological quality of case series studies: an introduction to the JBI critical appraisal tool. JBI Database of Systematic Reviews and Implementation Reports. 2019, Publish Ahead of Print.
- Wolf M, Even-Chen I, Talmi YP, et al. The indication for tonsillectomy in children following peritonsillar abscess. Int J Pediatr Otorhinolaryngol 1995, 31, 43–46. [Google Scholar] [CrossRef] [PubMed]
- Rosi-Schumacher M, Nagy R, Virgen C, et al. Peritonsillar abscess on NSQIP: Safety of indicated quinsy tonsillectomy. Int J Pediat Otorhinolaryngol 2023, 171, 111636. [Google Scholar] [CrossRef] [PubMed]
- Kim DK, Lee JW, Na YS et al. Clinical factor for successful nonsurgical treatment of pediatric peritonsillar abscess. Laryngoscope. 2015, 125, 2608–2611. [Google Scholar] [CrossRef] [PubMed]
- Millar KR, Johnson DW, Drummond D et al. Suspected Peritonsillar Abscess in Children: Pediatric Emergency Care. 2007, 23, 431–438.
- Apostolopoulos NJ, Nikolopoulos TP, Bairamis TN. Peritonsillar abscess in children. Is incision and drainage an effective management? Int J Pediatr Otorhinolaryngolol 1995, 31, 129–135. [Google Scholar]
- Chang L, Chi H, Chiu NC, et al. Deep Neck Infections in Different Age Groups of Children. Journal of Microbiology, Immunology and Infection 2010, 43, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Hsiao HJ, Huang YC, Hsia SH, et al. Clinical Features of Peritonsillar Abscess in Children. Pediatrics & Neonatology. 2012, 53, 366–370. [Google Scholar]
- Allen DZ, Rawlins K, Onwuka A, et al. Comparison of inpatient versus outpatient management of pediatric peritonsillar abscess outcomes. Int J Pediatr Otorhinolaryngol 2019, 123, 47–50. [Google Scholar] [CrossRef]
- Chisholm AG, Little BD, Johnson RF. Validating peritonsillar abscess drainage rates using the Pediatric hospital information system data. Laryngoscope. 2020, 130, 238–241. [Google Scholar] [CrossRef]
- Weinberg E, Brodsky L, Stanievich J, et al. Needle Aspiration of Peritonsillar Abscess in Children. Archives of Otolaryngology - Head and Neck Surgery. 1993, 119, 169–172. [Google Scholar] [CrossRef]
- Ghantous J, Heiman E, Zelman A, Hadar A, Schwarz Y, Attal P, Sichel JY, Shaul C. Conscious sedation for the management of peritonsillar abscess in pediatric patients: A prospective case series and literature review. Int J Pediatr Otorhinolaryngol. 2024, 183, 112032. [Google Scholar] [CrossRef] [PubMed]
- Qureshi H, Ference E, Novis S, et al. Trends in the management of pediatric peritonsillar abscess infections in the U.S., 2000–2009. Int J Pediatr Otorhinolaryngol 2015, 79, 527–531. [Google Scholar] [CrossRef] [PubMed]
- Nguyen T, Haberland CA, Hernandez-Boussard T. Pediatric Patient and Hospital Characteristics Associated With Treatment of Peritonsillar Abscess and Peritonsillar Cellulitis. Clin Pediatr (Phila) 2015, 54, 1240–1246. [Google Scholar] [CrossRef]
- Akhavan, M. Ear, Nose, Throat. Emergency Medicine Clinics of North America. 2021, 39, 661–675. [Google Scholar] [CrossRef] [PubMed]
- Simon LM, Matijasec JWD, Perry AP, et al. Pediatric peritonsillar abscess: Quinsy ie versus interval tonsillectomy. Int J Pediatr Otorhinolaryngol 2013, 77, 1355–1358. [Google Scholar] [CrossRef]
- Chang BA, Thamboo A, Burton MJ, et al. Needle aspiration versus incision and drainage for the treatment of peritonsillar abscess. Cochrane Database Syst Rev. 2016, 23, CD006287. [Google Scholar]
Figure 1.
PRISMA flowchart for selection of studies.
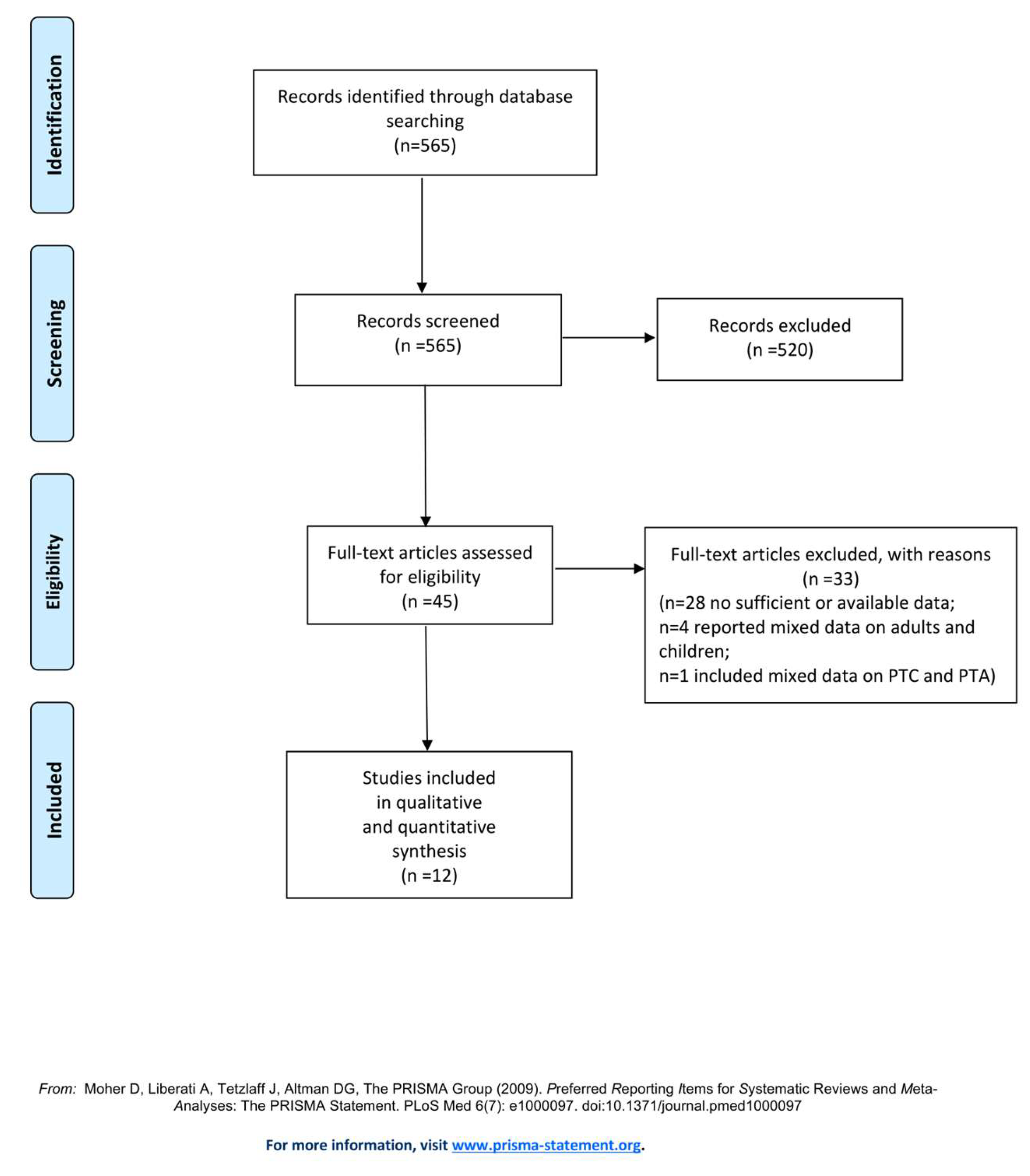
Figure 2.
Treatment modalities for PTA in children.
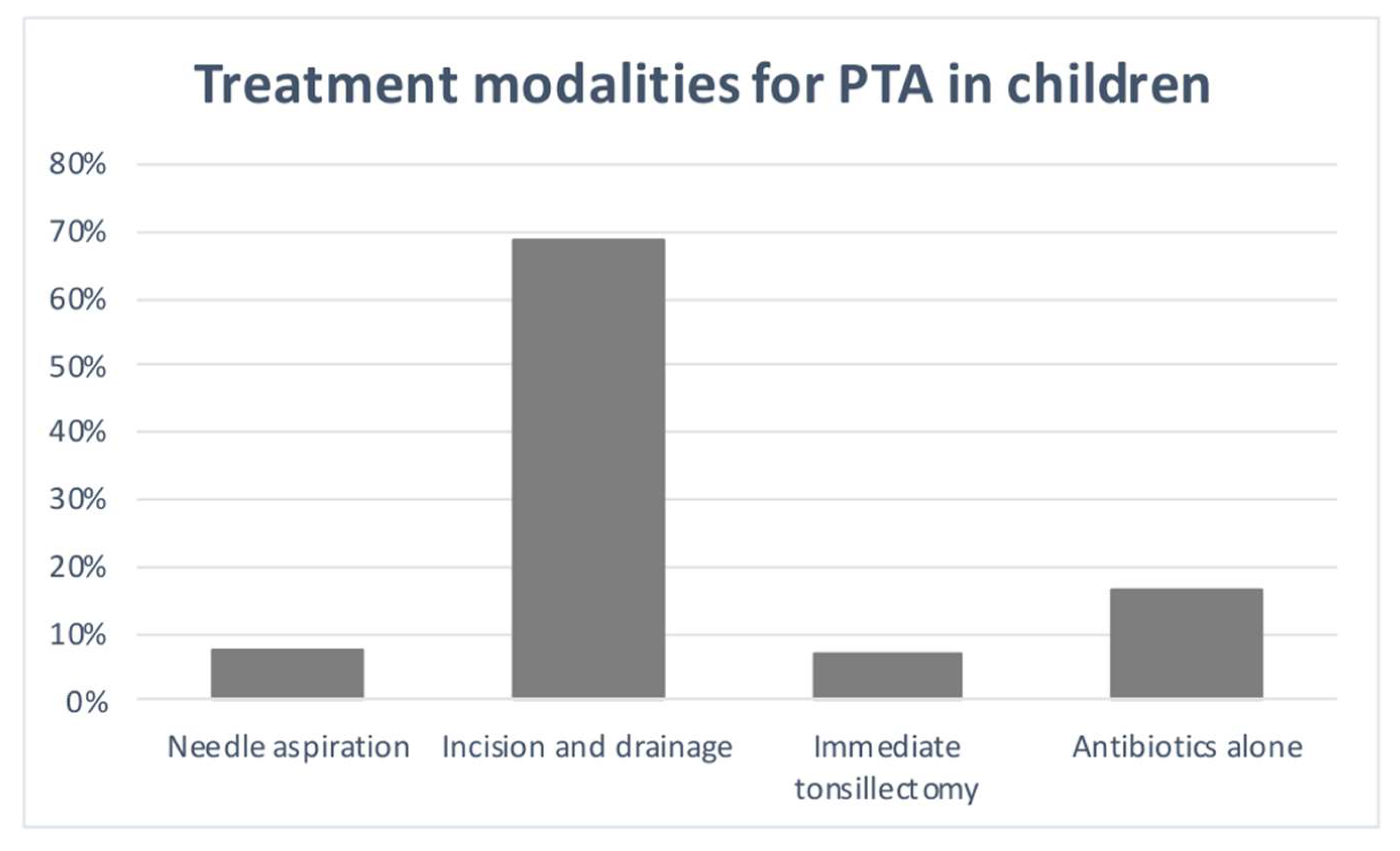
Figure 3.
Treatment algorithm for PTA in children.
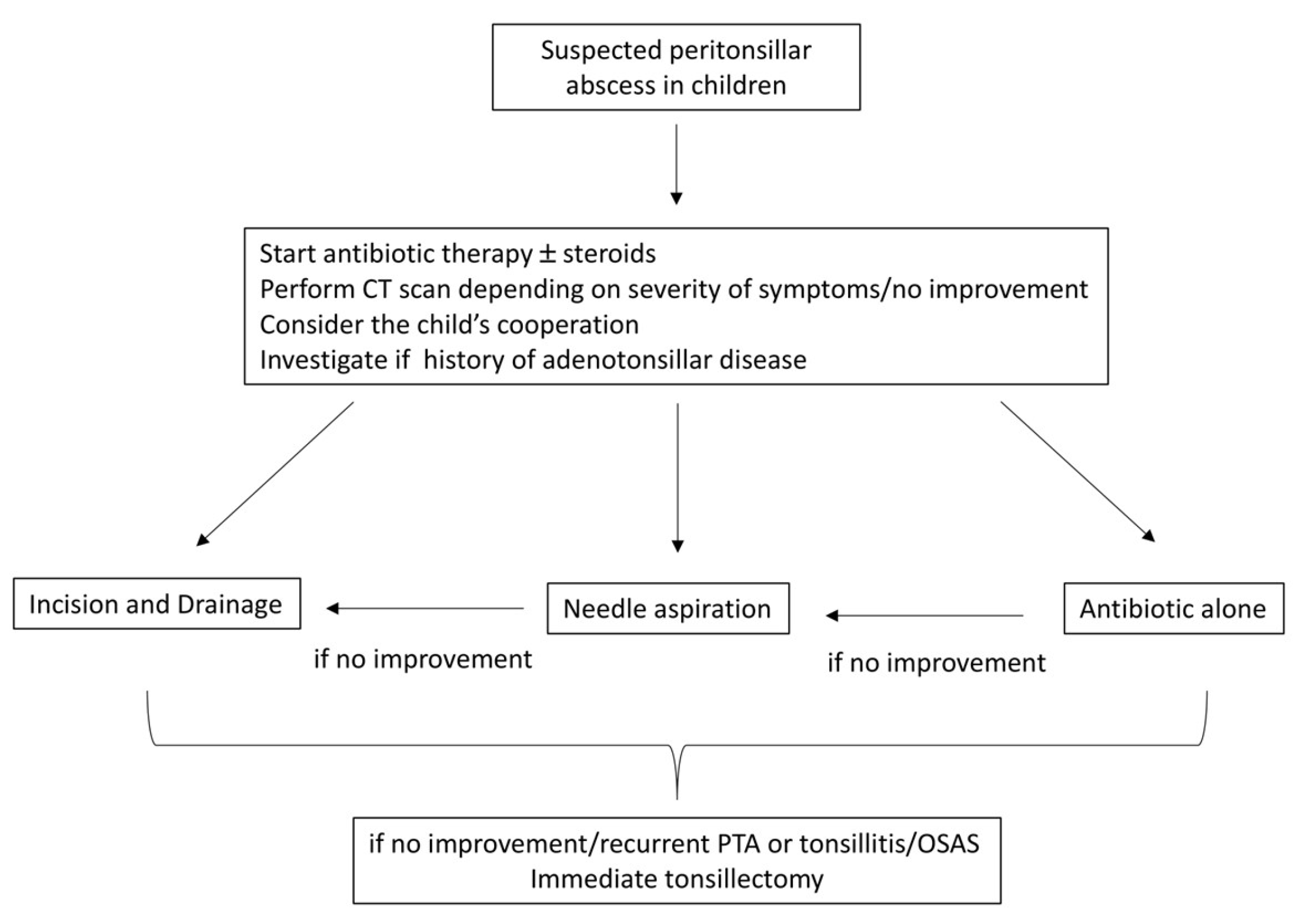

Table 1.
Characteristics of the included studies.
| Authors, year | Study | N° cases PTA | Mean Age (y) |
Sex | Symptoms PTA |
Signs | Microbiology |
|---|---|---|---|---|---|---|---|
| Weinberg et al.,1993 [23] | Retrospective | 43 | 13.9 | - | Shore throat 100% Drooling 34% Muffled voice 59% |
Unilateral peritonsillar bulge 100% Trismus |
GABHS, Str. Viridans Fusobacterium necrophorum H. influenzae |
| Apostolopoulos et al., 1995 [18] | Retrospective | 189 | 9 | 86M:103F | Sore throat | Peritonsillar bulge Trismus |
GABHS 35% Anaerobs 12% Others 12% Str. Viridans 10% Str. non-A 7% St. Aureus 6% Candida 6% H. Influenzae 4.5% Str. pneumoniae 4.5% Str. Sanguis 3% |
| Wolf et al., 1995 [14] |
Retrospective | 19 | 10-16y | - | Pain and dysphagia |
Trismus 50% Fever |
GABHS St. Aureus Str. Viridans Str. Non-A Pneumococci Peptostreptococci Mixed flora |
| Schraff et al., 2001 [11] |
Retrospective | 83 | 12.1 | - | Sore throat/neck pain 93% Odynophagia 83% Muffled voice 37% |
Neck adenopathy 94% Uvular deviation 52% Trismus 30% Dehydration 47% Fever 55% |
Mixed flora with Str. pyogenes the predominant organism |
| Millar et al., 2007 [17] |
Retrospective | 43 PTA 178 PTC |
15.4 PTA 3.2 PTC |
- | Sore throat 100% Painful swallowing 100 % Voice changes 86.7% Decrease oral intake 90.6% Drooling 75% |
Peritonsillar swelling 100% Cervical adenopathy 96.1% Trismus 78.9% Uvular deviation 73.3% Airway compromise 8% Fever 59.5% |
GABHS Str. non group A St. Aureus |
| Segal et al., 2009 [4] |
Retrospective | 126 | 12.8 | 55M:71F | - | - | GABHS 45.3% Anaerobes 14% Mixed w/o anaerobes 15.6% Str. C 6.2% others 17.3 |
| Chang et al., 2010 [19] |
Retrospective | 21 | 14.8 | 10M:11F | Odynophagia 21% | Fever 61.9% Trismus 4% Uvular deviation 6% Neck pain/mass1% |
Mixed flora |
| Hsiao et al., 2012 [20] |
Retrospective | 56 | 12.9 | 31M:24F | Sore throat |
Fever Asymmetric Swollen/bulging tonsil Uvular deviation |
Str.72% Fusobacterium species 44% Anaerobes 74% |
| Kim et al., 2015 [16] |
Retrospective | 88 | 8.5 | 52M:36F | - | - | - |
| Allen et al., 2019 [21] |
Retrospective | 566 | 12.9 outpt 9.9 inpt | 261M:305F | - | - | - |
| Chisholm et al., 2020 [22] | Retrospective | 200 |
12.6 |
77M:123F | - | - | - |
| Rosi-Schumacher et al., 2023 [15] |
Retrospective | 777 | 10.7 |
357M:420F | Sepsis 45.9% Systemic inflammatory response syndrome 4.8% |
- | - |
PTA: peritonsillar abscess; PTC: peritonsillar cellulitis; GABHS: beta-hemolytic Streptococcus group A; Str: streptococcus; St: staphylococcus m: month; y: year; outpt: outpatient; inpt: inpatient.
Table 2.
Types of treatments for pediatric PTA.
| Authors, year | Needle aspiration and/or Incision&drainage |
Tonsillectomy | Antibiotics | Recurrence (%) |
Time of recurrence | Complications | Follow-up |
|---|---|---|---|---|---|---|---|
| Weinberg et al.,1993 [23] |
41 needle aspiration (31 positive, 10 negative) |
5 immediate |
7 antibiotics alone | - | - | - | - |
| Apostolopoulos et al., 1995 [18] |
136 I&D (53 negative) |
- | - | 15.8% | 1 m | 12 (6.3%) torticollis, prologed fever |
1m-7y |
| Wolf et al., 1995 [14] |
7 needle aspiration (6 LA, 1 GA) 12 I&D (5 LA, 7 GA) |
2 immediate 1 elective |
17 antibiotics initiated 1-8 d prior the admission |
0 | - | 1 torticollis 1 dyspnea |
2 y |
| Schraff et al., 2001 [11] |
54 I&D | 25 immediate | 3 antibiotics alone | 0 | - | - | - |
| Millar et al., 2007 [17] |
43 needle aspiration or I&D | - | - | 4.7% | within 60 d | - | - |
| Segal et al., 2009 [4] |
95 needle aspiration 30 I&D GA |
1 immediate | 64.2% amoxicillin-clavulanate, 19% cefuroxime 13.5% cefuroxime + metronidazole 2.1% azithromycin |
- | - | - | - |
| Chang et al., 2010 [19] |
3 I&D 10 needle aspiration |
- | 8 antibiotics alone | - | - | no complications | - |
| Hsiao et al., 2012 [20] |
48 |
1 elective | 9 penic. 15 penic.+genta. 4 penic.+clyndamicina 5 penic.+clyndamicina+genta 12 amox.cl. 5 amox.cl+ genta. 1 amox.cl+ ciprofloxacina 3 ampicillina/sulbactam 1 oxacillin + genta. 1 vancomycin + ceftazidime 8 intravenous antibiotics alone |
2% | 1 IOT 2 parapharyngeal involvement |
||
| Kim et al., 2015 [16] |
55 any surgery “Poor responder “ | 0 | 33 antibiotic alone “good responder” |
- | - | - | - |
| Allen et al., 2019 [21] |
113 I&D outpt 184 I&D inpt |
immediate 12 outpt + 42 inpt elective 22 outpt + 33 inpt |
antibiotics only 181 outpt + 88 inpt |
9.1% 29 outpt 23 inpt |
within 30 d | - | - |
| Chisholm et al., 2020 [22] |
115 I&D | - | - | - | - | - | - |
| Rosi-Schumacher et al., 2023 [15] |
725 I&D | 52 immediate 6 elective |
- | 2.5% | - |
357 sepsis 37 systemic inflammatory response syndrom |
1m |
LA: local anesthesia, GA: general anesthesia; d: days; m:month; y: year; I&D: Incision&Drainage; outpt: outpatients; inpt: inpatient: amox.cl.: amoxicillin + clavulanic acid; penic: penicillin; genta: gentamicin.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



