
Submitted:
06 November 2024
Posted:
06 November 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Background/Objectives: Patients receiving solid organ transplantation require lifelong immunosuppression, making them more susceptible to COVID-19. Vaccination against COVID-19 is recommended for HTR. The aim of the present study was to compare the course of the disease in vaccinated and unvaccinated HTR hospitalized in a tertiary hospital in Slovenia and to evaluate possible hesitant groups. Methods: All SARS-CoV-2 positive HTR (N=79) between 1 March 2020 and 31 December 2023 at the Infectious Diseases Department, University Medical Centre Ljubljana, Slovenia, were included retrospectively. Demographic, clinical and vaccination data were extracted from medical documentation and statistical evaluation was performed. Results: The vaccination rate in the cohort was 63.3%. We found no statistically significant difference in vaccination rates regarding gender (male 68.4% vs. female 50%, p=0.128), but there was a statistically significant higher revaccination rate in males (male 52.7% vs. female 18.2%, p=0.021). Vaccinated HRT were statistically significantly older than unvaccinated (p=0.000) and had a significantly higher Charlson Comorbidity index (p=0.001). The vaccination rate among patients who received transplants before the pandemic (prior to 2020) was statistically significantly higher (71.7% vs. 46.2%; p=0.027). Conclusions: Our results indicate no significant differences in the clinical course of COVID-19 between vaccinated and unvaccinated HRT regarding acute respiratory insufficiency (ARI), length of hospital stay (LOS), intensive care unit admission and mortality. However, our findings do suggest statistically significant differences in COVID-19 vaccine acceptance rates; younger HRT and those transplanted after the pandemic are more hesitant to vaccination and female HRT accept booster doses less frequently.
Keywords:
heart transplant recipients
; COVID-19
; clinical course
; vaccination
; hesitancy
1. Introduction
Patients receiving solid organ transplantation (SOT) require lifelong immunosuppression, making them more susceptible to COVID-19. In addition to immunodeficiency, heart transplant recipients (HTR) often have comorbidities, which further affect the severity of the disease. There are few data on the prevalence and clinical features of COVID-19 in HTR. The data suggest that the odds of being diagnosed with COVID-19 are more than five times higher in HTR, the chances of hospitalization are approximately 80%, and the mortality rates range from 10% to 30% [1,2,3,4]. In 2022 there were 2444 heart transplants in Europe and, according to Slovenian Eurotransplant data, there were 21 heart transplants in Slovenia [5]. Since 2018 all heart transplants in Slovenia have been performed at UMC Ljubljana. Before 2018 Slovenian patients mostly received transplants in Vienna, Austria [6]. While vaccination against COVID-19 is recommended for HTR [7,8], the effectiveness of the vaccine might be reduced due to chronic immunosuppressive therapy [9,10]. Despite the relatively poor response to the vaccine, data from studies comparing the clinical course of COVID-19 in vaccinated and unvaccinated HTR are sparse, but they show a significantly more favorable course in vaccinated individuals [3]. Many associations therefore recommend that HTR be vaccinated before the transplantation; ideally with completion of the vaccine series a minimum of two weeks prior to the transplant [8]. Some heart transplant programs abroad even mandated immunization before listing for a transplant [11,12] and, subsequently, vaccination rates among HRT in some countries were extremely high. The vaccination rate of the Slovenian population against COVID-19 was low in comparison to other European countries, with primary course rates of 57% and 72.6%, respectively. Sociological studies point out that COVID-19 vaccine hesitancy is influenced by several factors, namely economic and political, as well as satisfaction with the health care system and the spread of conspiracy theories [13]. Estimated vaccination rates against COVID-19 in HTR reported in peer-reviewed literature range from 13.6 to 98.3% [2,14,15]. To the best of our knowledge, we have data neither on the HTR vaccination rate against COVID-19 nor on the clinical course of the disease in HTR in Slovenia.
The aim of the present study was for the first time to estimate the epidemiological and clinical characteristics of the course of COVID-19 in HTR in Slovenia. Our primary objective was to estimate the vaccination rate among HTR and its influence on clinical presentation, namely length of hospital stay, rate of acute respiratory insufficiency, rate of ICU admission and rate of in-hospital mortality, respectively. In addition, our secondary objective was to evaluate possible vaccination hesitant subgroups among the HRT in Slovenia.
2. Materials and Methods
2.1. Study Design and Population
We conducted a retrospective cohort study including all adult HTR (≥18 years) who were hospitalized at the Infectious Diseases Department, University Medical Centre Ljubljana, Slovenia, between 1 March 2020 and 31 December 2023 and had a positive nasopharyngeal swab for SARS-CoV-2 (Figure 1). In Slovenia, all heart transplantations are performed at University Medical Centre Ljubljana, where all HTR are also assessed for any complications (including infections). All patients received standard immunosuppressive therapy, based on the protocol prescribed by the treating cardiologist (corticosteroid, mycophenolate mofetil and calcineurin inhibitor). The diagnosis of SARS-CoV-2 infection was based on a positive polymerase chain reaction (PCR) test from upper and/or lower respiratory tract, mostly a nasopharyngeal swab. In cases of asymptomatic patients, a cycle threshold (Ct) of less than 30 was considered diagnostic for acute infection. According to the national recommendations, which have been changing depending on the current medical knowledge, availability of medications, and circulating viral type, patients received different therapies: convalescent plasma, corticosteroids, monoclonal antibodies and remdesivir. Regarding comorbidities, patients were categorized using the Charlson comorbidity index [16].
2.2. Data Retrieval
All vaccination data, including the timing of vaccination and the type of vaccine used, was obtained from the patient’s electronic medical records. These records also include comprehensive demographic, epidemiological, clinical, laboratory, and microbiological data, as well as radiological findings and a full record of the patient's therapeutic regimen. The study was conducted following the Declaration of Helsinki, and approved by the Slovenian National Medical Ethical Committee on 23 May 2024 (consent number: 0120-171/2024-2711-3).
2.3. Definitions
Definition of symptomatic COVID disease – symptomatic covid was defined as any other hospitalization in patients with clinical signs or symptoms, such as fever, cough, shortness of breath, fatigue, or other symptoms of respiratory illness except hospitalization due to monoclonal antibody or hyperimmune convalescent plasma or remdesivir application in asymptomatic patients.
2.4. Statistical Analysis
Statistical significance was conducted with SPSS Statistics 17 (International Business Machines Corporation, Armonk, New York, USA) and p value of < 0.05 was considered significant. In the case of a small number of patients in any of the nominal variable categories, the likelihood ratio test was used to test the association between two nominal variables. For nominal variables with more than two categories, the association was tested using the chi-square test or likelihood ratio test in the case of expected frequencies lower than five. The difference between two groups in a numerical variable was tested with the t-test in case the variable was normally distributed across groups, otherwise the Mann-Whitney U test was used. Bivariate Kendall’s tau correlation was used to study the relationship between different factors. We used the mean and standard deviation as measures of descriptive statistics, as all continuous variables were normally distributed.
3. Results
We included retrospectively all HTR (79) who were SARS-CoV-2 positive between 01.03.2020 and 31.12.2023 at Infectious Diseases Department, University Medical Centre, Ljubljana, Slovenia. The demographic, clinical and vaccination characteristics are presented in Table 1.
3.1. Comparison Between Vaccinated and Unvaccinated Patients
We performed a comparison between vaccinated and unvaccinated HTR, including a subgroup analysis of HTR receiving different vaccine types and the presence of symptomatic disease. The results are presented in Table 2. Only HTR who were vaccinated before the hospitalization were included in the analysis. The comparison between vaccinated and re-vaccinated HTR based on gender is presented in Figure 2.
3.2. Descriptive Analysis of Non-Survivors
Four out of 79 patients died (5%); all were hospitalized due to severe COVID-19 pneumonia, three were vaccinated and one was not. Their mean age was 71.3 years, the average sum of CCI was 4.5 and the average time from heart transplantation was 10 years. Two patients died because of COVID-19 related complications (severe pneumonia with pulmonary fibrosis; COVID-19 associated pulmonary aspergillosis with diffuse bleeding) and two patients due to non-COVID related complications (septic shock with multiorgan failure; hemorrhagic shock due to retroperitoneal bleeding).
3.3. Analysis of Heart Transplant Recipients Based on Time from Vaccination to Hospital Admission
We performed a comparison between HTR in terms of outcome based on time from vaccination to hospital admission. The results are presented in Table 3. Only HTR who were vaccinated before the hospitalization were included in the analysis.
3.4. Analysis of Heart Transplant Recipients Based on Time from Heart Transplant
We performed a comparison between HTR in terms of outcome based on time from heart transplant. The results are presented in Table 4. Only HTR who were vaccinated before the hospitalization were included in the analysis. The comparison between HTR vaccinated before or during the pandemics is represented in Figure 3.
3.5. Comparison of Patients with Symptomatic and Asymptomatic COVID Disease
We performed a comparison between symptomatic and asymptomatic HRT. The results are presented in Table 5.
3.6. Bivariate Correlation Analysis
We performed a bivariate correlation analysis for all measures. The results are presented in Table 6.
4. Discussion
HTR require lifelong immunosuppression, making them either more susceptible to COVID-19 or have a much higher risk of hospitalization and mortality and the data shows a significantly more favorable course in vaccinated individuals [1,2,3,4]. Also in our cohort, asymptomatic course was more often observed in vaccinated HTR, similarly as several other studies have confirmed in immunocompromised and non-immunocompromised vaccine recipients. In general, vaccinated patients tend to have less severe COVID-19-related respiratory failure, a better clinical course, lower mortality rate and a higher hospital discharge rate [3,17]. Furthermore, asymptomatic clinical course was more often observed in those vaccinated with mRNA-based vaccine and those receiving vaccine booster dose. This findings are in accordance with already published data as well; people vaccinated with mRNA-based vaccine have a stronger immune response to the vaccination than the recipients of vector based vaccine [18]. Data confirms that booster mRNA-based vaccine doses remain effective against severe COVID-19, regardless of patients’ immune status [19]. We also demonstrated that COVID-19 booster vaccination was associated with a significantly shorter LOS, despite re-vaccinated HTR having higher CCI (borderline statistical significance). Our findings align with research underscoring the importance of booster vaccination in HTR to reduce severe outcomes and hospitalization duration following COVID-19 infection [10].
In our cohort, unvaccinated HTRs were generally younger and had a lower CCI than those vaccinated against COVID-19. However, unvaccinated HTR were more frequently treated with COVID-19 convalescent plasma (CCP). Vaccinated HTR had at least partial immunity, while unvaccinated patients lacked protection against SARS-CoV-2 infection. In cases where a HTR was unvaccinated, we were more likely to choose treatment with CCP, due to concerns about a potentially more severe course of COVID-19. The use of CCP provides immediate passive immunity via neutralizing antibodies against SARS-CoV-2. When administered early in the disease course (within 72 hours of symptom onset), CCP can offer prompt protection, potentially reducing the risk of disease progression, hospitalization, and mortality [20].
Not only that HTR vaccinated with a vector-based vaccine had a longer LOS compared to those vaccinated with a mRNA-based vaccine, they also required ICU admission more frequently. Although the age difference between the two groups was not statistically significant, those HTR receiving vector-based vaccines had higher CCI scores, indicating a greater burden of comorbidities that may have influenced LOS and ICU admission. Although the differences were not statistically significant, the shorter time from heart transplantation to hospital admission, along with the longer interval from vaccination to hospital admission in patients vaccinated with vector-based vaccines, suggests a trend. This may indicate that patients receiving vector-based vaccines were more likely vaccinated during a period of more intense immunosuppression compared to those vaccinated with mRNA vaccines. Memenga and coll. found that advanced patient age and shorter time since heart transplantation were associated with lower concentrations of anti-SARS-CoV-2 spike IgG antibodies after three vaccine doses, but did not observe differences in antibody levels between the vaccine types (mRNA versus vector-based vaccine) [10]. Conversely, Huang and coll. reported that higher CCI values correlated with lower levels of IgG antibodies against the SARS-CoV-2 spike protein, which may also explain the prolonged hospitalization in patients vaccinated with vector vaccines due to greater comorbidity and, consequently, a poorer vaccine response [21].
There was a statistically significant higher revaccination rate in male HTR, probably reflecting the previously described phenomenon that, compared to men, women had less trust in vaccines [22,23,24]. The average time from vaccination to hospital admission in our cohort was more than a year, which confirms the sense of regular revaccinations for immunocompromised patients, according to the foreign and Slovenian recommendations [25].
Immunocompromised patients remain at an elevated risk of death from COVID-19, especially those who are critically ill [26], and the same applies to those who need treatment in the ICU [1,4,27]. Data from the Netherlands suggest that HTR were at increased risk of complicated COVID-19 and all-cause mortality was higher than in our cohort (14% vs. 5.1%), but their results were from the pre-vaccination era [28], which may suggest that mortality among our patients was lower due to the vaccination effect. Similarly, Peters et al. showed the association of COVID-19 vaccination with risk of infection, hospitalization and death among HTR in a US heart transplant program and the rates were significantly lower among those vaccinated [3]. In terms of the presence of immunocompromising conditions and vaccination status, Stupica et al. found that patients in Slovenia admitted to hospital during the Omicron period had similar odds of progressing to critically severe disease to those admitted during the Delta period. Patients completing at least primary vaccination had lower odds of progression to critically severe disease and had a shorter length of hospital stay (LOS) than unvaccinated patients [29]. On the other hand, in our ICU the cohort mortality rate, despite high vaccination status, was higher in comparison to other reports; meta-analyses of patients requiring ICU admission and mechanical ventilation reach mortality rates up to 50% [30]. In our opinion, the reason could be that our ICU patients were older and had several comorbidities. Additionally, the cohort of our patients treated in the ICU was very small. Older persons, those with higher CCI and the immunocompromised were statistically significantly more often vaccinated.
Vaccine hesitancy has been ranked by the World Health Organization among the top 10 threats to global health [31]. The results of our study suggest that the vaccination rate among HTR in our tertiary center was lower than reported from abroad and from the general Slovenian population. Some foreign reports also suggest a low acceptance rate of COVID-19 vaccines in HTR [14,32], while, on the other hand, reports from Argentina show extremely high rates of vaccination among HTR, which resulted in no confirmed COVID-19 cases during the Delta variant circulation [2]. There is a paucity of data regarding vaccination hesitancy factors among HTR in Slovenia. Our analysis suggests that younger HTR and those receiving transplants after the pandemic are more hesitant to get vaccinated, and female HTR accept a booster dose less frequently. We assume that the hesitancy factors in our cohort are similar to those in the general Slovenian population. A cross-sectional survey from Slovenia regarding COVID-19 vaccination intention, confidence and hesitancy among the working population revealed a 58% vaccination rate of the respondents, while 11.3% refused to be vaccinated. The hesitant group was most often deterred by distrust of COVID-19 vaccines, including the inability to choose a vaccine and the fear of side effects [33]. Reports suggest that mRNA vaccines were related to the adverse effect of myocarditis [34], and although studies have shown a significantly higher chance of myocarditis after SARS-CoV-2 infection than vaccination, some people were deterred from COVID-19 vaccination. An on-line survey by the National Institute of Public Health (NIPH) from Slovenia, dated December 2020, revealed the attitudes of the population regarding COVID-19 vaccination and the factors that affect these attitudes. A greater intention to get vaccinated was associated with men and older respondents, as was found in our cohort as well. Others more likely to get vaccinated were physicians and medical students, respondents who had got the influenza vaccination, those who knew someone who had been hospitalized or had died from COVID-19, and those who had more trust in experts, institutions and vaccines [35]. According to the NIPH publication, more than 71% of the respondents were vaccinated against COVID-19 in the year 2022, which is in concordance with data from the Slovenian Electronic Registry of Vaccinated Persons (eRCO). The main reasons to get vaccinated were to prevent a more severe course, to protect the health of relatives and to protect one’s own health [36]. Data from a US transplant center suggest that 82 (96.5%) HTR received a COVID-19 vaccine with the primary motivating factor being to protect their own health [15]. In our study, we found that the HTR vaccination rate was significantly higher in those receiving a transplant before the year 2020. The reason might be due to global vaccine hesitancy with a surge in misinformation and conspiracy theories against vaccination observed during the COVID-19. On the other hand, immunocompromised patients were among the first to be vaccinated against COVID-19 in our country, and soon after, reports regarding the side effect of myocarditis appeared.
Our study has several limitations. The study was conducted retrospectively and included a relatively small cohort of patients, which reduces the statistical power of our findings. Regarding clinical course, we did not assess antibody levels to SARS-CoV-2 nucleocapsid protein on admission and thus cannot entirely exclude the possibility that some of the patients included in the study had previously contracted SARS-CoV-2, which could have also influenced the clinical course of the COVID-19 episode for which they were hospitalized during the study period, as the research is retrospective. An added value would be if our HTR had completed a questionnaire on the reasons for and against vaccination and their social status. However, the advantage of our research being conducted at a single center is the comprehensive data capture and the uniform treatment regimen for HTR with COVID-19. The research was conducted in a single center, but it should be emphasized that heart transplants in Slovenia are performed only at UMC Ljubljana, where HTR come for regular check-ups, as well. As a rule, all Slovenian HTR who contracted COVID-19 were treated in our institution, so we assume that all HTR from Slovenia with SARS-CoV-2 infection who required hospital treatment during the study period were included in the study.
5. Conclusions
We have confirmed that vaccination is crucial in preventing more severe clinical presentations of COVID-19 in HTR in Slovenia. Clinical course of COVID-19 in our HTR cohort was more often asymptomatic in vaccinated HTR and LOS was shorter in recipients of mRNA-based vaccines and those revaccinated. Our results suggest that among HRT in Slovenia, younger patients and those receiving a transplant after the pandemic, as well as women, are more hesitant to COVID-19 vaccination, representing a subgroup who should be regarding vaccination addressed more actively.
The spread of expert advice and the creation of a safe and respectful communication environment to promote vaccination and debunk vaccination myths is crucial in health and vaccination promotion, especially among the immunocompromised, who are more prone to a severe course of COVID-19. Studies have shown that stimulation of positive feelings plays a significant role in overcoming vaccine hesitancy. HTR are more susceptible to COVID-19, especially a severe course, so it is crucial to promote high vaccination rates, especially in those who are more hesitant.
Author Contributions
Conceptualization, N.G.K. and R.S.; methodology, M.M.; software, M.M.; validation, N.G.K, R.S. and M.M.; formal analysis, M.M.; investigation, R.S. and M.M.; resources, M.M.; data curation, M.M.; writing—original draft preparation, N.G.K.; writing—review and editing, N.G.K. and M.M.; visualization, M.M.; supervision, N.G.K..; project administration, N.G.K.; funding acquisition, N.G.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee): National Medical Ethics Committee of the Republic of Slovenia on 23 May 2024 (consent number: 0120-171/2024-2711-3).
Informed Consent Statement
“Patient consent was waived due to retrospectivity.
Data Availability Statement
Dataset available on request from the authors.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Ahmed F, Abid M, et al. Incidence and prognosis of COVID-19 amongst heart transplant recipients: a systematic review and meta-analysis. Eur J Prev Cardiol 2022, 29, e224–e226. [Google Scholar] [CrossRef]
- Burgos LM, Baro Vila RC, et al. COVID-19 in heart transplant recipients: Outcomes according to vaccination status. Transpl Infect Dis 2022, 24, e13817. [Google Scholar] [CrossRef] [PubMed]
- Peters LL, Raymer DS, et al. Association of COVID-19 Vaccination With Risk of COVID-19 Infection, Hospitalization, and Death in Heart Transplant Recipients. JAMA Cardiol 2022, 7, 651–654. [Google Scholar] [CrossRef]
- Okumura K, Nishida S, et al. Trends in COVID-19 Mortality Among Solid Organ Transplant Recipients: Implications for Prevention. Transplantation 2022, 106, e380–e381. [Google Scholar] [CrossRef]
- www.slovenija-transplant.si. Available online: https://www.slovenija-transplant.si/wp-content/uploads/2024/04/kratko-letno-porocilo-2023-koncna.pdf (accessed on 2 October 2024).
- www.slovenija-transplant.si. Available online: https://www.slovenija-transplant.si/wp-content/uploads/2023/09/20-years-of-donation-programme-2021.pdf (accessed on 2 October 2024).
- Duly K, Farraye FA et al. COVID-19 vaccine use in immunocompromised patients: A commentary on evidence and recommendations. Am J Health Syst Pharm 2022, 79, 63–71. [Google Scholar] [CrossRef] [PubMed]
- www.ishlt.org. Available online: https://www.ishlt.org/docs/default-source/default-document-library/2023-11-15-ishlt-ast-asts-joint-statement-covid19-vaccination.pdf?sfvrsn=383b0c3e_1 (accessed on 2 October 2024).
- Aslam S, Ison MG. SARS-CoV-2 vaccination in heart transplantation: What we do and do not know. J Heart Lung Transplant 2022, 41, 58–160. [Google Scholar] [CrossRef]
- Memenga F, Kueppers ST, et al. SARS-CoV-2 Vaccination-Induced Immunogenicity in Heart Transplant Recipients. Transpl Int 2023, 36, 10883. [Google Scholar] [CrossRef]
- Chih S, Clarke BA, et al. The COVID-19 Pandemic and Adult Cardiac Transplantation: Impact, Interventions, and Implications. Can J Cardiol 2023, 39, 853–864. [Google Scholar] [CrossRef] [PubMed]
- Rosano G, Jankowska EA, et al. COVID-19 vaccination in patients with heart failure: a position paper of the Heart Failure Association of the European Society of Cardiology. Eur J Heart Fail 2021, 23, 1806–1818. [Google Scholar] [CrossRef]
- Lamot M, Kirbiš A. Multilevel analysis of COVID-19 vaccination intention: the moderating role of economic and cultural country characteristics. Eur J Public Health 2024, 34, 380–386. [Google Scholar] [CrossRef]
- Wu Q, Shen Y, et al. Low acceptance rate of COVID-19 vaccination and reduced quality of life among heart transplant recipients during the COVID-19 pandemic. J Card Surg 2022, 37, 4975–4981. [Google Scholar] [CrossRef] [PubMed]
- Mohney KL, Link CB, et al. COVID-19 Vaccination Motivation and Hesitancy in Heart Transplant Recipients During a Global Health Crisis. J Heart Lung Transplant 2022, 41, S178–9. [Google Scholar] [CrossRef]
- www.mdcalc.com. Available online: https://www.mdcalc.com/calc/3917/charlson-comorbidity-index-cci (accessed on 2 October 2024).
- Di Costanzo D, Mazza M, et al. Retrospective analysis of epidemiologic features and clinical course of COVID-19 patients and comparison between vaccinated and unvaccinated patients. Monaldi Arch Chest Dis 2023. [CrossRef]
- Slomka S, Zieba P, et al. Comparison of Post-Vaccination Response between mRNA and Vector Vaccines against SARS-CoV-2 in Terms of Humoral Response after Six Months of Observation. Vaccines (Basel) 2023, 11, 1625. [Google Scholar] [CrossRef]
- Sun J, Zheng Q, et al. Effectiveness of mRNA Booster Vaccine Against Coronavirus Disease 2019 Infection and Severe Outcomes Among Persons With and Without Immune Dysfunction: A Retrospective Cohort Study of National Electronic Medical Record Data in the United States. Open Forum Infect Dis 2024, 11, ofae019. [Google Scholar] [CrossRef]
- Senefeld JW, Franchini M, et al. COVID-19 Convalescent Plasma for the Treatment of Immunocompromised Patients: A Systematic Review and Meta-analysis. JAMA Netw Open 2023, 6, e2250647. [Google Scholar] [CrossRef]
- Huang CF, Jang TY, et al. Impact of comorbidities on the serological response to COVID-19 vaccination in a Taiwanese cohort. Virol J 2023, 20, 112. [Google Scholar] [CrossRef]
- Dimiter Toshkov, Explaining the gender gap in COVID-19 vaccination attitudes. European Journal of Public Health 2023, 33, 490–495. [CrossRef]
- Nassiri-Ansari T, Atuhebwe P, et al. Shifting gender barriers in immunisation in the COVID-19 pandemic response and beyond. Lancet 2022, 400, 24. [Google Scholar] [CrossRef]
- Zintel S, Flock C, et al. Gender differences in the intention to get vaccinated against COVID-19: a systematic review and meta-analysis. Z Gesundh Wiss, 2022, 7, 1–25. [CrossRef]
- www.nijz.si. Available online: https://nijz.si/nalezljive-bolezni/cepljenje/priporocila-za-cepljenje-proti-covidu-19-za-jesen-2024/ (accessed on 2 October 2024).
- Turtle L, Thorpe M, et al. Outcome of COVID-19 in hospitalised immunocompromised patients: An analysis of the WHO ISARIC CCP-UK prospective cohort study. PLoS Med 2023, 20, e1004086. [Google Scholar] [CrossRef]
- Dumas G, Bertrand M, et al. Prognosis of critically ill immunocompromised patients with virus-detected acute respiratory failure. Ann Intensive Care 2023, 13, 101. [Google Scholar] [CrossRef] [PubMed]
- Muller SA, Manintveld OC, et al. Characteristics and outcomes of COVID-19 in heart transplantation recipients in the Netherlands. Neth Heart J 2022, 30, 519–525. [Google Scholar] [CrossRef]
- Stupica D, Collinet-Adler S, et al. SARS-CoV-2 Vaccination and Clinical Presentation of COVID-19 in Patients Hospitalized during the Delta- and Omicron-Predominant Periods. J Clin Med 2023, 12, 961. [Google Scholar] [CrossRef]
- Auld SC, Harrington KRV, et al. Trends in ICU Mortality From Coronavirus Disease 2019: A Tale of Three Surges. Crit Care Med 2022, 50, 245–255. [Google Scholar] [CrossRef]
- www.who.int. Available online: https://www.who.int/news-room/spotlight/ten-threats-to-global-health-in-2019 (accessed on 2 October 2024).
- Tartof SY, Slezak JM, et al. Analysis of mRNA COVID-19 Vaccine Uptake Among Immunocompromised Individuals in a Large US Health System. JAMA Netw Open 2023, 6, e2251833. [Google Scholar] [CrossRef] [PubMed]
- Avsec L, Bilban M, et al. COVID-19 vaccination intention, confidence and hesitancy among working population in Slovenia: A Cross-Sectional Survey. Saf Health Work 2022, 13, S183. [Google Scholar] [CrossRef]
- Oster ME, Shay DK, et al. Myocarditis Cases Reported After mRNA-Based COVID-19 Vaccination in the US From December 2020 to August 2021. JAMA 2022, 327, 331–340. [Google Scholar] [CrossRef]
- Petravić L, Arh R, et al. Factors Affecting Attitudes towards COVID-19 Vaccination: An Online Survey in Slovenia. Vaccines (Basel) 2021, 9, 247. [Google Scholar] [CrossRef]
- www.nijz.si. Available online: https://nijz.si/wp-content/uploads/2023/06/SI-PANDA-21.-izvedba_ANG_.pdf (accessed on 2 October 2024).
Figure 1.
Flow chart of the vaccination and re-vaccination rate among included HTR.
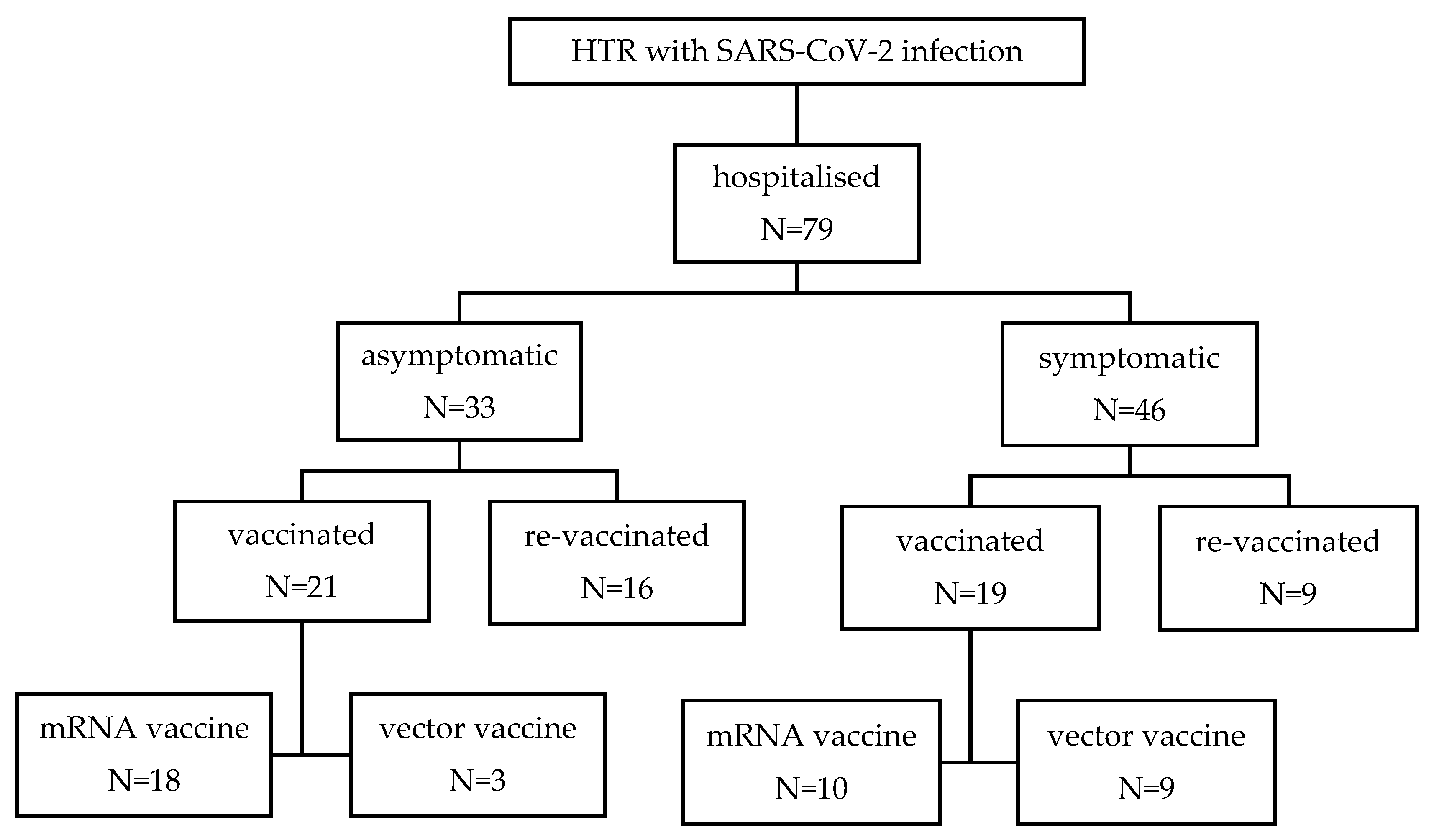
Figure 2.
Comparison between vaccinated and re-vaccinated heart transplant recipients based on gender.
Figure 2.
Comparison between vaccinated and re-vaccinated heart transplant recipients based on gender.
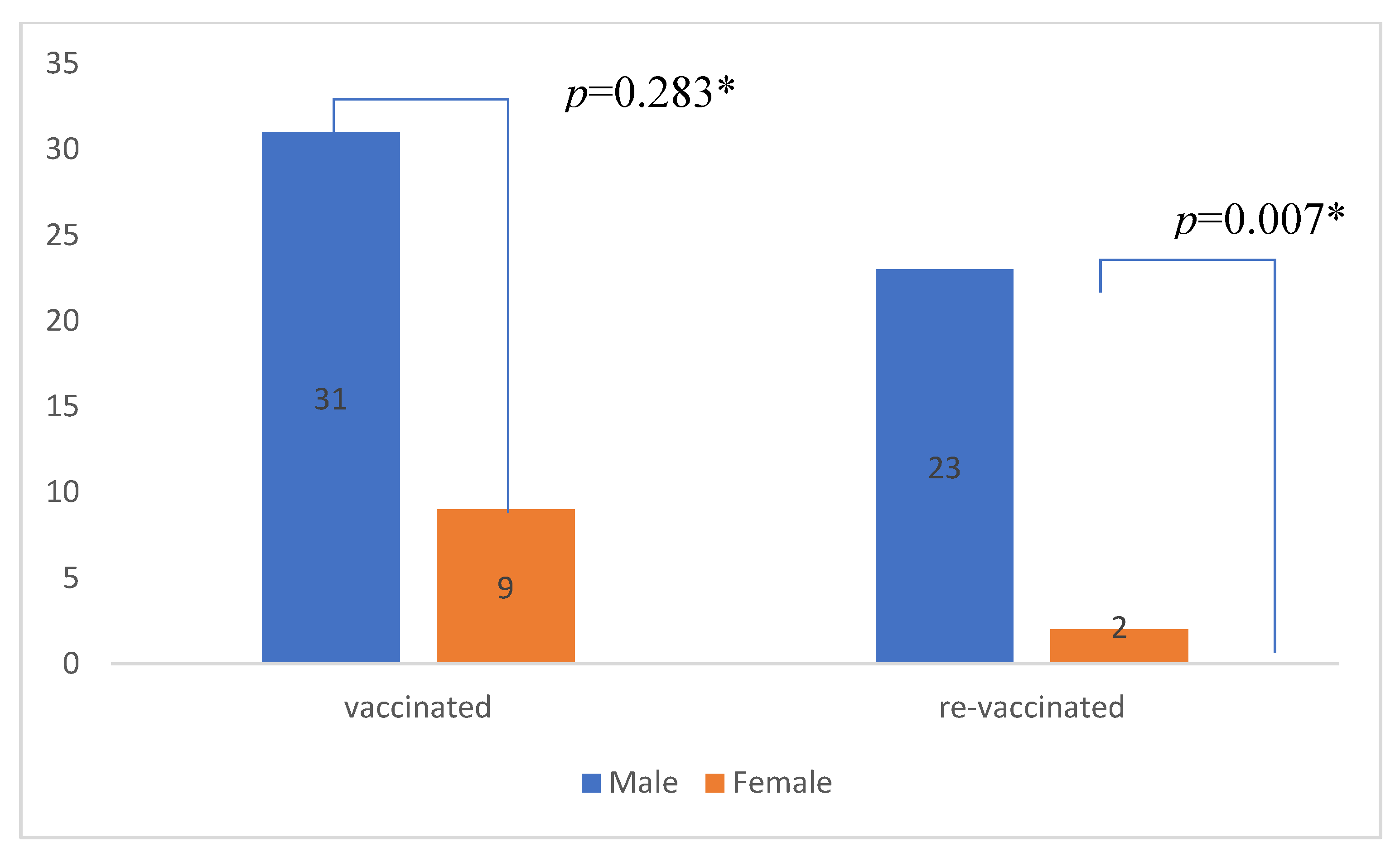
Figure 3.
Comparison between vaccination rate of heart transplant recipients that received their transplant before the start or during the pandemic tx prior to 2020 = heart transplant before year 2020; tx after 2020 = heart transplant including and after year 2020
Figure 3.
Comparison between vaccination rate of heart transplant recipients that received their transplant before the start or during the pandemic tx prior to 2020 = heart transplant before year 2020; tx after 2020 = heart transplant including and after year 2020
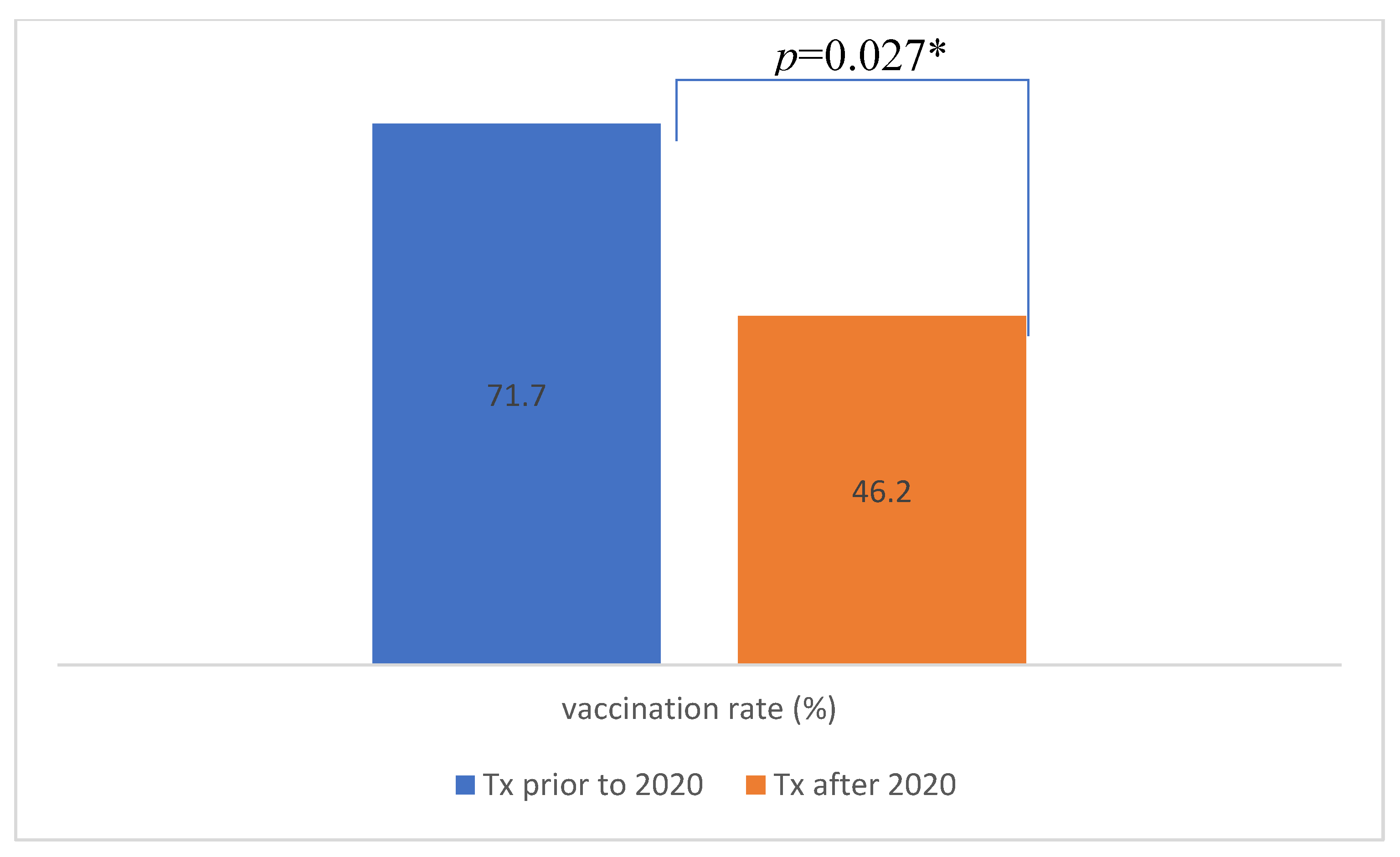

Table 1.
Demographic, clinical and vaccination characteristics of included patients.
| N=79 | |
| Mean age (years) (±SD) | 62.5 (±9.8) |
| Male gender (%) | 57 (72.2) |
| CCI (±SD) | 3.3 (±1.8) |
| Time from heart transplantation (years) (±SD) | 5.66 (±5.29) |
| Time from vaccination to hospital admission (days) (±SD) | 402 ±(232) |
| Length of hospital stay in days (±SD) | 10.4 (±11.9) |
| No. of patients with symptomatic COVID disease (%) | 46 (58.2) |
| No. of patients with respiratory insufficiency (%) | 28 (35.4) |
| No. of patients admitted to ICU (%) | 6 (7.6) |
| In-hospital mortality rate (%) | 4 (5.1) |
| ICU mortality rate (%) | 4 (66.7) |
| No. of patients on corticosteroid therapy at hospital addmision (%) | 51 (64.5) |
| No. of patients treated with | |
| -hyperimmune convalescent plasma (%) | 13 (16.5) |
| -mAb (%) | 19 (24.1) |
| -remdesivir (%) | 62 (78.4) |
| -corticosteroid(%) | 19 (24.0) |
| No. of patients vaccinated (%) | 50 (63.3) |
| No of patients vaccinated before hospitalization (%) | 40 (50.6) |
| No. of patients receiving mRNA-based vaccine (%) | 28 (70.0) |
| No. of patients receiving vector-based vaccine (%) | 12 (30.0) |
| No. of patients receiving a booster dose of vaccine (%) | 34 (43.1) |
| No. of patients receiving a booster dose of vaccine before hospitalization (%) | 25 (31.6) |
CCI – Charlson Comorbidity Index; ICU – Intensive Care Unit; mAb – Monoclonal Antibodies; mRNA – Messenger Ribonucleic Acid; N – Number of Patients; SD – Standard Deviation.
Table 2.
Comparison between vaccinated and unvaccinated heart transplant recipients.
|
Vaccinated N=40 |
Unvaccinated N=39 |
||
|---|---|---|---|
| Mean age (years) (±SD) | 65.6 (±8.9) | 59.3 (±9.8) | p=0.004* |
| Male gender (%) | 31 (77.5) | 26 (66.7) | p=0.283 |
| CCI (±SD) | 3.7 (±1.8) | 2.8 (±1.7) | p=0.018* |
| Time from heart transplantation (years) (±SD) | 6.4 (±4.8) | 4.9 (±5.7) | p=0.194 |
| Length of hospital stay (days) (±SD) | 9.0 (±11.8) | 12.0 (±12.0) | p=0.106 |
| No. of patients with respiratory insufficiency (%) | 11 (27.5) | 17 (43.6) | p=0.135 |
| No. of patients admitted to ICU (%) | 4 (10.0) | 2 (5.1) | p=0.414 |
| In-hospital mortality rate (%) | 3 (7.5) | 1 (2.6) | p=0.317 |
| No. of patients (%) treated with | |||
| -hyperimmune convalescent plasma | 1 (2.5) | 12 (30.8) | p=0.001* |
| -mAb | 9 (22.5) | 10 (25.6) | p=0.744 |
| -remdesivir | 34 (85.0) | 28 (71.8) | p=0.153 |
| -corticosteroid | 9 (22.5) | 10 (25.6) | p=0.744 |
| Subgroup analysis of heart transplant recipients receiving an mRNA-based vaccine or a vector-based vaccine | |||
|
mRNA vaccine N=28 |
vector vaccine N=12 |
||
| Mean age (years) (±SD) | 66.5 (±9.8) | 63.7 (±6.4) | p=0.371 |
| Male gender (%) | 22 (78.6) | 9 (75.0) | p=0.804 |
| CCI (±SD) | 3.5 (±2.0) | 4.2 (±1.3) | p=0.327 |
| Time from heart transplantation (years) (±SD) | 7.3 (±4.6) | 4.4 (±5.0) | p=0.085 |
| Time from vaccination to hospital admission (days) (±SD) | 388 (±215) | 431 (±218) | p=0.603 |
| Length of hospital stay (days) (±SD) | 6.6(±9.3) | 14.3 (±15.3) | p=0.011* |
| No. of patients with respiratory insufficiency (%) | 6 (21.4) | 5 (41.7) | p=0.189 |
| No. of patients admitted to ICU (%) | 2 (7.1) | 2 (16.7) | p=0.358 |
| In-hospital mortality rate (%) | 2 (7.1) | 1 (8.3) | p=0.896 |
| No. of patients (%) treated with | |||
| -hyperimmune convalescent plasma | 1 (3.6) | 0 | p=0.507 |
| -mAb | 6 (21.4) | 3 (25.0) | p=0.804 |
| -remdesivir | 24 (85.7) | 10 (83.3) | p=0.847 |
| -corticosteroid | 5 (17.9) | 4 (33.3) | p=0.283 |
| Subgroup analysis of vaccinated and unvaccinated heart transplant recipients with symptomatic COVID-19 | |||
|
Vaccinated N=19 |
Unvaccinated N=27 |
||
| Mean age (years) (±SD) | 66.7 (±7.2) | 61.2 (±7.7) | p=0.017* |
| Male gender (%) | 14 (73.7) | 17 (63.0) | p=0.445 |
| CCI (±SD) | 3.8 (±1.4) | 3.2 (±1.6) | p=0.154 |
| Time from heart transplantation (years) (±SD) | 5.9 (±4.7) | 4.6 (±4.7) | p=0.370 |
| No. of patients with respiratory insufficiency (%) | 11 (57.9) | 17 (63.0) | p=0.729 |
| No. of patients admitted to ICU (%) | 4 (21.1) | 2 (7.4) | p=0.176 |
| In-hospital mortality rate, % | 3 (15.8) | 1 (3.7) | p=0.152 |
| No. of patients (%) treated with | |||
| -hyperimmune convalescent plasma | 1 (5.3) | 12 (44.4) | p=0.004* |
| -mAb | 7 (36.8) | 6 (22.2) | p=0.278 |
| -remdesivir | 15 (78.9) | 18 (66.7) | p=0.362 |
| -corticosteroid | 9 (47.4) | 10 (37.0) | p=0.483 |
| Subgroup analysis of heart transplant recipients who received a booster dose of vaccine and does who did not | |||
|
Booster N=25 |
No booster N=15 |
||
| Mean age (years) (±SD) | 66.3 (±10.3) | 64.5 (±6.3) | p=0.556 |
| Male gender (%) | 23 (92.0) | 8 (53.3) | p=0.005* |
| CCI (±SD) | 4.2 (±1.9) | 3.0 (±1.5) | p=0.052 |
| Time from heart transplantation (years) (±SD) | 7.0 (±5.2) | 4.2 (±5.5) | p=0.372 |
| Length of hospital stay (days) (±SD) | 7.0 (±11.1) | 12.2 (±12.5) | p=0.030* |
| No. of patients with respiratory insufficiency (%) | 6 (24.0) | 5 (33.3) | p=0.522 |
| No. of patients admitted to ICU (%) | 3 (12.0) | 1 (6.7) | p=0.586 |
| In-hospital mortality rate, % | 3 (12.0) | 0 | p=0.163 |
| No. of patients (%) treated with | |||
| -hyperimmune convalescent plasma | 1 (4.0) | 0 | p=0.433 |
| -mAb | 4 (16.0) | 5 (33.3) | p=0.204 |
| -remdesivir | 22 (88.0) | 12 (80.0) | p=0.493 |
| -corticosteroid | 5 (20.0) | 4 (26.7) | p=0.625 |
CCI – Charlson Comorbidity Index; ICU – Intensive Care Unit; mAb – Monoclonal Antibodies; mRNA – Messenger Ribonucleic Acid; N – Number of Patients; SD – Standard Deviation.
Table 3.
Comparison between heart transplant recipients based on time from vaccination to hospital admission.
Table 3.
Comparison between heart transplant recipients based on time from vaccination to hospital admission.
| < 3 months N=4 |
3 – 6 months N=5 |
6 – 12 months N=9 |
> 12 months N=21 |
||
|---|---|---|---|---|---|
| Length of hospital stay (days) (±SD) | 4.5 (±1.3) | 11.8 (±7.8) | 11.6 (±16.0) | 7.4 (±11.6) | p=0.551 |
| No. of patients with respiratory insufficiency (%) | 2 (50.0) | 2 (40.0) | 2 (22.2) | 4 (19.0) | p=0.509 |
| No. of patients admitted to ICU (%) | 0 | 0 | 0 | 3 (14.3) | p=0.426 |
| In-hospital mortality rate (%) | 0 | 0 | 0 | 9.5 | p=0.613 |
| No. of patients (%) vaccinated with | |||||
| -mRNA-based vaccine | 3 (75.0) | 2 (40.0) | 8 (88.9) | 14 (66.7) | p=0.288 |
| -vector-based vaccine | 1 (25.0) | 3 (60.0) | 1 (11.1) | 7 (33.3) |
ICU – Intensive Care Unit; mRNA – Messenger Ribonucleic Acid; N – Number of Patients; SD – Standard Deviation.
Table 4.
Comparison between heart transplant recipients with recent (less than one year prior to admission) heart transplant and the rest of cohort.
Table 4.
Comparison between heart transplant recipients with recent (less than one year prior to admission) heart transplant and the rest of cohort.
| Transplant less than one year before admission N=23 |
Transplant more than one year before admission N=56 |
||
|---|---|---|---|
| Length of hospital stay in days (±SD) | 11.6 (±14.3) | 10.0 (±10.9) | p=0.918 |
| No. of patients with respiratory insufficiency (%) | 6 (26.1) | 22 (39.3) | p=0.265 |
| No. of patients admitted to ICU (%) | 2 (8.7) | 4 (7.1) | p=0.813 |
| In-hospital mortality rate (%) | 0 | 4 (7.1) | p=0.188 |
ICU – Intensive Care Unit; N – Number of Patients; SD – Standard Deviation.
Table 5.
Comparison between heart transplant recipients with symptomatic and asymptomatic COVID-19.
| Symptomatic N=46 |
Asymptomatic N=33 |
||
|---|---|---|---|
| Mean age(years) (±SD) | 63.5 (±7.9) | 61.2 (±12.0) | p=0.303 |
| Male gender (%) | 31 (67.4) | 26 (78.8) | p=0.265 |
| CCI (±SD) | 3.5 (±1.5) | 3.0 (±2.1) | p=0.141 |
| Time from heart transplantation (years) (±SD) | 5.2 (±4.7) | 6.4 (±6.1) | p=0.538 |
| No. of patients vaccinated (%) | 19 (41.3) | 21 (63.6) | p=0.050* |
| No. of patients receiving a booster dose of vaccine (%) | 9 (19.6) | 16 (48.5) | p=0.006* |
| No. of patients receiving a mRNA based vaccine (%) | 10 (52.6) | 18 (85.7) | p=0.023* |
| No. of patients receivig a vector based vaccine (%) | 9 (47.4) | 3 (14.3) | |
| No. of patients (%) treated with | |||
| -hyperimmune convalescent plasma | 13 (28.3) | 0 | p=0.001* |
| -mAb | 13 (28.3) | 6 (18.2) | p=0.301 |
| -remdesivir | 33 (71.7) | 29 (87.9) | p=0.085 |
| -corticosteroid | 19 (41.3) | 0 | p=0.000* |
Table 6.
Bivariate correlation for all measures (Kendall’s tau correlation coefficient).
| Measure | 1. | 2. | 3. | 4. | 5. | 6. | 7. | 8. | 9. | 10. | 11. | 12. | 13. | 14. | 15. | 16. | 17. |
| 1. Age | 1.00 | ||||||||||||||||
| 2. Gender | 0.14 | 1.00 | |||||||||||||||
| 3. CCI | 0.50** | 0.23* | 1.00 | ||||||||||||||
| 4. T-TX | 0.33** | 0.17 | 0.19* | 1.00 | |||||||||||||
| 5. T-VAC | -0.10 | -0.13 | -0.15 | -0.07 | 1.00 | ||||||||||||
| 6. LOS | 0.09 | -0.14 | 0.18* | 0.02 | -0.11 | 1.00 | |||||||||||
| 7. SYMP | 0.04 | -0.13 | 0.15 | -0.06 | -0.19 | 0.73** | 1.00 | ||||||||||
| 8. ARI | 0.12 | -0.07 | 0.07 | 0.07 | -0.20 | 0.59** | 0.63** | 1.00 | |||||||||
| 9. ICU | 0.07 | -0.04 | 0.09 | 0.05 | 0.17 | 0.32** | 0.24* | 0.39** | 1.00 | ||||||||
| 10. MORT | 0.17 | 0.02 | 0.16 | 0.17 | 0.05 | 0.25** | 0.20 | 0.31** | 0.81** | 1.00 | |||||||
| 11.HCP | -0.08 | 0.05 | 0.07 | -0.02 | -0.22 | 0.35** | 0.38** | 0.24* | -0.13 | -0.10 | 1.00 | ||||||
| 12. mAb | -0.05 | 0.09 | -0.02 | -0.05 | -0.33* | 0.01 | 0.12 | 0.08 | -0.05 | 0.01 | -0.25* | 1.00 | |||||
| 13. remde | 0.06 | 0.02 | 0.02 | -0.06 | 0.29* | -0.11 | -0.19 | 0.00 | 0.03 | -0.02 | 0.15 | -0.43 | 1.00 | ||||
| 14. stero | 0.02 | 0.14 | 0.10 | 0.16 | 0.33* | 0.44** | 0.48** | 0.76** | 0.29* | 0.41** | 0.15 | 0.10 | -0.14 | 1.00 | |||
| 15. VAC. | 0.28** | 0.12 | 0.25* | 0.18 | A | -0.16 | -0.22 | -0.17 | 0.09 | 0.11 | -0.38** | -0.04 | 0.16 | -0.04 | 1.00 | ||
| 16. mRNA | 0.19 | 0.04 | -0.21 | 0.26 | -0.09 | -0.35* | -0.36* | -0.21 | -0.15 | -0.02 | 0.11 | -0.04 | 0.03 | -0.17 | a | 1.00 | |
| 17.R-VAC. | 0.25** | 0.30** | 0.31** | 0.18 | 0.05 | -0.25** | -0.31** | -0.16 | 0.11 | 0.22 | -0.23* | -0.13 | 0.16 | -0.06 | 0.67** | 0.06 | 1.00 |
*significant at p <0.05; ** significant at p<0.01. Abbreviations: CCI – Charlson Comorbidity Index; T-TX – time from heart transplantation; T-VAC – time from vaccination to hospital admission; LOS – length of hospital stay; SYMP – symptomatic COVID disease; ARI – acute respiratory insufficiency; ICU – intensive care unit admission; MORT – in-hospital mortality; HCP – treatment with hyperimmune convalescent plasma; mAB – monoclonal antibodies application; remde – treatment with remdesivir; steroid – treatment with steroids; VAC – vaccinated; mRNA – vaccinated with mRNA vaccine; R-VAC – re-vaccinated. a – cannot be computed, as part of the same measure.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



