
Submitted:
06 November 2024
Posted:
07 November 2024
You are already at the latest version
Abstract
Background/Objectives: The standard of care for acute bacterial skin and skin structure infections (ABSSSIs) requiring intravenous (IV) antibiotics includes vancomycin, administered over several days, in a hospital or outpatient setting resulting in significant costs. Dalbavancin, a long-acting single-dose lipoglycopeptide IV therapy may offer a cost-effective option for adult patients with ABSSSIs in Canada. Methods: A cost-utility analysis (CUA) was performed to evaluate the potential benefits of dalbavancin compared to other IV antibiotics for the treatment of adult patients with ABSSSIs who require IV antibiotics but whose hospitalization, if necessary, is anticipated to be £ 72 hours. Results: This analysis utilized a decision-analytic model showing that dalbavancin was dominant against all IV antibiotic comparators when considering the healthcare system or societal perspective and was associated with lower costs and improved patient adherence. For the sub-population analysis against PWID (people who inject drugs) and the homeless, dalbavancin generated even greater cost savings. Conclusions: We report that dalbavancin when used to treat ABSSSI requiring IV antibiotics may offer cost savings for Canadian healthcare providers through reduced hospitalization time, lower administration and labor costs, minimized risk of healthcare-acquired infections (HAIs), improved patient compliance and optimized resource allocation particularly in patients at risk of non-compliance (First Nations, the homeless and PWID).
Keywords:
Acute Bacterial Skin and Skin Structure Infections (ABSSSI)
; Dalbavancin
; Antibiotics
; Cost-Utility Analysis
; People Who Inject Drugs (PWID)
; The Homeless
; First Nations
; Hospitalization
; Healthcare Resource Usage
1. Introduction
Acute bacterial skin and skin structure infections (ABSSSIs) include cellulitis, erysipelas, wound infections, and major cutaneous abscesses.[1,2,3] They are defined by lesion size—as measured by the area of redness, edema, or induration—and must be at least 75 cm2.[1,2,3] These infections represent a significant proportion of the cases that lead Canadian patients to seek emergency room (ER) services. Among these, cellulitis is notably the most prevalent skin disease responsible for emergency department visits and subsequent inpatient admissions.[4] ABBSIs are primarily caused by Staphylococcus aureus, including methicillin-resistant strains (MRSA), which complicate treatment, leading to higher failure rates and prolonged hospitalizations.[5,6,7] MRSA prevalence in Canadian populations varies widely (11% - 100%) with higher rates in Western Canada and First Nations communities.[8,9,10] In 2022, an estimated 40,821 adults in Canada were treated for ABSSSI,[11] significantly increasing morbidity, with average hospital stays of 7.1 days, extending to 7.7-13.4 days for MRSA cases.[3,5,6,12,13,14,15]
Inadequate initial antibiotic therapy in 20%-25% of cases results in wasted resources, longer hospital stays, and increased morbidity and mortality.[3,14,15,16,17] Key ABSSSIs recurrence risk factors include MRSA, substance abuse, homelessness, obesity, and comorbidities like diabetes and HIV.[18,19,20,21,22] Outpatient treatment compliance is notably low at 57%, resulting in suboptimal outcomes and frequent recurrences. These outcomes often include relapses of skin infections, the emergence of new skin infections, the necessity for extended or alternative antibiotic therapies, and the requirement for additional incision-and-drainage procedures.[23,24,25] At-risk populations, including the homeless and people who inject drugs (PWID), many of whom also suffer from psychiatric illnesses, represent 30.4% of ABSSSI cases and encounter significant treatment barriers. [24,25] Key challenges in treating these populations include:
- Loss to follow-up; This is the most significant barrier to successful treatment. Homeless PWID are more likely to be lost to follow-up compared to other groups, resulting in uncertain clinical outcomes.[26]
- Lower clinical cure rates; Including patients lost to follow-up, homeless PWID exhibit significantly lower cure rates (47.2%) compared to housed non-PWID (73.1%).[26]
- Higher readmission rates; Homeless PWID have the highest 30-day readmission rates related to outpatient parenteral antimicrobial therapy (OPAT) (26.4%) among all groups studied.[26]
- Line tampering; Secondary bacteremia and line tampering are more common among homeless PWID, indicating challenges with maintaining the integrity of intravenous access.[26]
- Engagement in care; While cure rates are similar across groups for patients who remain engaged in care, maintaining this engagement is particularly challenging for homeless PWID.[26]
- Psychosocial factors; Studies suggest that addiction and associated mental health disorders often require additional treatment, complicating adherence to OPAT.[26]
- Lack of a suitable environment’ Many homeless patients lack a home environment suitable for the provision of OPAT, making treatment logistics more difficult.[26]
Patients living in remote areas where ambulatory care cannot be organized also face significant barriers to effective and efficient treatment for ABSSSIs. This group includes a substantial number of individuals from First Nations communities, who exhibit disproportionately high rates of community-associated MRSA and are typically transported to urban areas for the full course of intravenous antibiotic treatment.[9] Remote communities often rely on nurses or community health workers and have limited access to hospitals, advanced treatment facilities, physicians, and specialists who can effectively diagnose and treat ABSSSIs. Consequently, patients frequently need to be transported long distances to receive necessary care.[27] Weather conditions and limited transportation options, often requiring air travel, can delay medical evacuations and timely access to care for ABSSSI patients. Additional barriers include cultural and linguistic obstacles, as the lack of culturally sensitive care and language barriers can impact the quality of healthcare First Nations patients receive. Historical abuses in the healthcare system have also led to mistrust among First Nations communities, resulting in delayed seeking of care for ABSSSIs. Furthermore, the lack of resources in smaller First Nations communities can make it challenging to provide adequate follow-up care for ABSSSI patients after initial treatment.[28]
Clinical management of ABSSSI is becoming increasingly complex due to multidrug-resistant Gram-positive pathogens especially Staphylococci (eg. MRSA), leading to higher morbidity, mortality, and healthcare costs. The current standard of care when IV antibiotics are required, vancomycin, poses significant toxicity risks, ototoxicity but particularly nephrotoxicity in high-risk patients.[29] Vancomycin’s most common adverse reaction is “vancomycin flushing syndrome” (VFS), also previously called “Redman Syndrome”, and occurs in 3.7% to 47% of patients. It is characterized by a pruritic erythematous rash on the face, neck, and upper torso, typically associated with a rapid infusion (< 1 hour).[30,31] Due to these risks, vancomycin dosing is inherently complex and necessitates adjustments based on individual patient factors such as age, weight, renal function, and the concurrent use of other potentially nephrotoxic medications. This variability often complicates the establishment of an appropriate dosing regimen. Recent guidelines addressing this complexity recommend using an Area Under the Curve (AUC)-guided approach rather than relying solely on trough serum concentrations.[32,33] The AUC/MIC (minimum inhibitory concentration) ratio is now considered a better predictor of vancomycin microbiologic and clinical efficacy and safety. This requires more frequent monitoring and potentially complex calculations to determine the optimal dosing strategy. In critically ill patients, loading doses of vancomycin (25-35 mg/kg) may be necessary to achieve therapeutic concentrations quickly. However, determining the correct dose without risking toxicity is challenging, particularly in patients with fluctuating renal function. In addition, patients’ renal function can change rapidly, especially in critically ill or elderly patients. This necessitates frequent reassessment of dosing and monitoring serum concentrations, complicating the management of therapy.[32,33]
Daptomycin is another antibiotic frequently employed in the treatment of ABSSSIs. Clinical studies have demonstrated that its efficacy is comparable to that of standard treatments such as vancomycin.[34] It is particularly advantageous for patients with renal impairment, as it does not necessitate the same level of renal monitoring required by vancomycin. Despite its efficacy, it is essential to monitor for potential side effects, including muscle toxicity (myopathy) and eosinophilic pneumonia. Regular monitoring of creatine kinase (CK) levels is advisable, especially for patients undergoing prolonged therapy or those with risk factors for muscle injury. While daptomycin is a valuable option for treating ABSSSIs, its use requires careful monitoring and management of potential complications. Regular assessments of muscle function, renal and liver function, and overall patient response to therapy are essential components of managing patients on daptomycin.[34]
Another aspect of treating ABSSSIs is the heightened risk of subsequent infections for hospitalized patients. The recent COVID-19 pandemic exemplifies the increased risk of transmission for both ABSSSI patients and healthcare workers.[35,36,37] Standard treatments, such as vancomycin, often require infusions two to three times daily over several days. This frequent interaction with healthcare professionals not only raises the risk of COVID-19 exposure but also exacerbates staffing challenges if healthcare workers need to quarantine following exposure. Consequently, this can lead to a shortage of healthcare staff, complicating the management of outpatient care and further hindering the treatment process for patients.[35,37] This risk is similarly applicable to other types of nosocomial infections.
The economic burden of ABSSSI is growing, encompassing both direct and indirect treatment costs. Hospitalizations, often prolonged, treatment failures, and disease recurrence significantly contribute to this financial impact.[4,38,39,40,41,42,43,44] ABSSSIs are a notable concern in the Canadian healthcare system, contributing to significant healthcare utilization highlighting the need for effective infection prevention and control measures. Approved by Health Canada in September 2018 as a treatment for adult patients with ABSSSI, dalbavancin is the first single-dose IV therapy for Gram-positive bacteria, including MRSA.[45] Available as a single 1500 mg dose or as a 2-dose regimen of 1000 mg IV, followed one week later by 500 mg IV, dalbavancin offers flexibility in emergency or outpatient care settings. This reduces the need for hospitalization, enhances patient compliance, and supports outpatient parenteral antimicrobial therapy (OPAT). The efficacy and safety of dalbavancin were demonstrated in the DISCOVER1 and DISCOVER2 trials, which showed it to be non-inferior to vancomycin IV followed by linezolid PO. These findings were further confirmed in phase 3 and phase 3b trials that compared single-dose and two-dose regimens of dalbavancin. The phase 3b trial revealed comparable early response and clinical success rates, with no significant differences in adverse events across the dosing regimens.[46,47] Excreted through both renal and fecal routes, dalbavancin further eliminates the need for dose adjustment and unlike vancomycin does not require renal function monitoring or therapeutic drug monitoring (TDM).[29] Recent real-world studies using data from the Canadian LEadership on Antimicrobial Real-life Usage (CLEAR) registry have reported the clinical usage of dalbavancin as a treatment for acute bacterial skin and skin structure infections (ABSSSI) and its potential in facilitating early hospital discharge in Canada.[48]
By incorporating dalbavancin into the treatment regimen for ABSSSI, healthcare providers may be able to improve patient outcomes, optimize antibiotic use, and support the goals of antimicrobial stewardship. This approach promotes the efficient use of healthcare resources by preventing un-necessary hospitalization and minimizes the risk of hospital-acquired infections, aligning with the objectives of antimicrobial stewardship in managing ABSSSIs and other Gram-positive infections.[49]
The objective of this study was to evaluate the cost-effectiveness of dalbavancin as a single-dose treatment for adult patients with ABSSSI in Canada, particularly in scenarios where hospitalization could potentially be avoided. Additionally, the study aimed to identify specific situations where dalbavancin could generate cost savings and improve patient adherence, including at-risk and hard-to-treat populations such as the homeless, PWID, and First Nations.
2. Results
Base case deterministic results are presented in Table 1. These results show that although dalbavancin is the most expensive antibiotic in terms of acquisition drug cost, its use is associated with a lower number of days of hospitalization leading to lower hospitalization cost. Dalbavancin is also linked with a lower cost for subsequent treatments due to improved adherence to treatment leading to a lower rate of ABSSSI recurrence. As expected, dalbavancin is associated with lower administration costs but higher expenses for ’other medical resources’ due to the increased number of doctor visits required for the larger volume of discharged patients.
When the societal perspective is considered, patients treated with dalbavancin miss less workdays (lower productivity loss) for either hospitalization or outpatient antibiotic administration. As such, in terms of total cost, dalbavancin is the least expensive option with savings between $301 and $541 when the healthcare perspective is considered and with savings between $590 and $887 when the societal perspective is considered instead.
Dalbavancin is also associated with a higher quality-adjusted life year (QALY) due to less time spent in hospital. With a higher QALY and a lower total cost, dalbavancin is the dominant treatment strategy when using the healthcare or the societal perspective. Probabilistic sensitivity analysis leads to similar results.
2.1. Scenario Analyses
The results of the scenario analyses are presented deterministically from the healthcare perspective for simplicity, but similar results were obtained when the probabilistic analysis was used, and greater savings could be expected when the societal perspective is considered.
2.1.1. Scenario 1: Sub-Population: Patients with Kidney Dysfunction
In patients with kidney dysfunction increased savings are associated with dalbavancin as this condition requires dose adjustment for most antibiotics, which decreases the overall success rate of these treatments. For linezolid IV that does not require dose adjustments in this patient population, this scenario analysis does not show an impact. Table 2 summarizes the results of the analysis.
2.1.2. Scenario 2: Sub-Population: PWID and the Homeless Population
As shown by the considerable savings demonstrated in this scenario analysis, dalbavancin has the potential to generate important savings on this specific sub-population. Table 3 summarizes the results of the analysis.
2.1.3. Scenario 3: No Hospitalization for Dalbavancin and 100% Hospitalization for Comparators
As expected, this scenario shows great savings for dalbavancin because of the one-dose administration associated with this treatment which allows preventing hospitalization. Table 4 summarizes the results of the analysis.
2.1.4. Scenario 4: Comparator Days of Treatment: 12 Days
In this scenario, the cost of comparators is decreased so the savings associated with dalbavancin are lower compared to the base case while dalbavancin remains the dominant treatment strategy. Table 5 summarizes the results of the analysis.
3. Discussion
Dalbavancin is unique as the only IV antibiotic treatment for ABSSSI that can be administered using a short infusion time (< 30 minutes) and more importantly as a single dose as opposed to antibiotic treatments requiring lengthy infusion times, usually administered more than once daily, and for multiple days.[46] The safety and efficacy of dalbavancin have been shown to be equivalent to the main comparator treatment considered in this model, vancomycin IV, as well as compared to other comparators.[46,50]
The objective of our study was to evaluate the cost-effectiveness of dalbavancin as a single-dose treatment for adult patients with ABSSSI in Canada who presented to the emergency room and required IV antibiotics but whose hospitalization, if necessary, was anticipated to be approximately 72 hours or less. Our findings are that dalbavancin offers cost savings for Canadian healthcare providers through reduced hospitalization time, lower administration and labor costs, minimized risk of hospital-acquired infections (HAIs), improved patient compliance and optimized resource allocation. Specifically, we report that due to the savings in total resource utilization associated with dalbavancin, the higher drug acquisition cost compared to its comparators (vancomycin IV, linezolid IV, and daptomycin IV) is completely offset, meaning that dalbavancin is less expensive than its comparators for the treatment of ABSSSI when IV antibiotics are required and hospitalization, if any, is expected to be of short duration (72 hours or less). The reduced hospitalization length of stay (LOS) is also associated with an increase in the patient’s utility in the model. As a result, in the deterministic analysis dalbavancin is a dominant treatment compared to vancomycin IV for the relevant population.
Other studies report similar findings including Talan et al. (2021) who found that using a single IV dose of dalbavancin in a clinical pathway significantly reduced hospitalization rates for stable patients with moderately severe infections. As well, dalbavancin is correlated with reduced costs due to outpatient infusion.[51,52]
Although this report shows that dalbavancin generates savings on an average patient, the main driver for these results is the dalbavancin capacity of reducing hospitalization. As one can imagine, dalbavancin may not generates savings for a patient requiring additional in-hospital procedures or observation. However, there are many other situations where it will (see also Section 3.1.2). To minimize the uncertainty associated with the impact of dalbavancin on the overall cost, a customizable cost-calculator tool has been created (see Supplemental File S1), allowing the user to adjust the different inputs to the specific patient/hospital situations, including the length of treatment and hospitalization, dosage requirements, and the costs. Note that this is not the cost-utility model that was used to perform this analysis, but a simple user-modifiable cost calculator tool meant for health professional decision makers.
3.1. Limitations
3.1.1. Healthcare-Acquired Bacterial and Viral Infections
The model does not account for the increased risk of healthcare-acquired infections (HAIs) associated with hospitalization. Lipsky et al. (2012) identified recent hospitalization as a significant risk factor for ABSSSI, linked to over 20% of soft tissue abscesses and more than 30% of cellulitis cases.[53] Although data are lacking, it is reasonable to assume that the reduction in hospitalization with dalbavancin, compared to vancomycin IV and other comparators, may lower the risk of HAIs. Additionally, other HAIs or viral infections, such as COVID-19, were not considered. Considering COVID-19 protocols, treatments that minimize hospitalization, like dalbavancin, should be prioritized to reduce infection risks, as supported by increased dalbavancin sales in the US during the pandemic.
3.1.2. Impact of Dalbavancin on Hospitalization
The model assumes that dalbavancin reduces hospitalization by 1.0–1.2 days compared to other treatments. International studies support this assumption, demonstrating significant reductions in hospital stays and associated costs with dalbavancin. For example, Streifel et al. (2019) [54] reported 617 hospital days prevented for 37 patients, saving $40,414 per patient in the USA. Similarly, Falconer et al. (2019) [55] estimated savings of £203,000 for NHS Grampian over two years in Scotland, and Wilke et al. (2019) [56] found that hospital stays in Germany were reduced by 6.45 days, saving €2,865 per patient. These studies collectively indicate that dalbavancin is effective in reducing hospitalization duration and costs.
Although there are uncertainties associated with the impact of dalbavancin on admission rates or the length of hospitalization, there are some sub-populations and scenarios for which dalbavancin usage is especially dominant compared to standard IV antibiotics including patients experiencing homelessness, PWID, and First Nations populations but also when ambulatory care cannot be organised in timely manner.
Although this analysis focussed on the most obvious comparators for dalbavancin (vancomycin IV, linezolid IV, and daptomycin IV) which are all IV antibiotics used in the treatment of MRSA, dalbavancin could also be a cost-effective approach for other, less expensive IV antibiotics used empirically for non-MRSA ABSSSI such as cefazolin IV and ceftriaxone IV when there is a certain gain associated with the reduction of hospitalization or for patients that are known to be non-compliant to antibiotics. This was not explored in this analysis.
3.1.3. Efficacy and Adverse Events
While direct head-to-head data exist for dalbavancin versus vancomycin IV, no such comparisons are available for dalbavancin against linezolid IV, or daptomycin IV. The model nonetheless assumes similar efficacy and safety profiles for all antibiotics, which is supported by a meta-analysis.[50]
The model did not include adverse events (AEs), potentially biasing results against dalbavancin. Pivotal trials showed no differences in serious AEs,[46] but indicated higher rates of nausea, headache, diarrhea, and pruritus with vancomycin IV. Real-life settings might differ; for example, vancomycin infusion-related reactions like “Red Man Syndrome”, nephrotoxicity, ototoxicity and catheter infections might be more prevalent with vancomycin outside trial conditions. These factors were not accounted for, as the trials were double-blind, with placebo infusions mimicking the frequency of vancomycin administration.[46]
4. Materials and Methods
A cost-utility analysis (CUA) was developed to assess the cost-effectiveness of dalbavancin for treating ABSSSI in adult patients using a decision analytic framework. This model considers patient admission, antibiotic clinical success or failure, subsequent treatment lines, and disease recurrence.
The target population for the CUA comprised adult patients with ABSSSI, who require IV antibiotics in situations where hospitalization could potentially be avoided. For this reason, this analysis focused on patients for which hospitalization, if any, is expected to be 72 hours or less.[51] The intervention of interest is dalbavancin and the comparators are vancomycin IV, linezolid IV, and daptomycin IV. The reference case adopted a Canadian public payer perspective, considering direct medical costs such as antibiotics, hospitalization, infusion, catheter, and peripherally inserted central catheter (PICC) lines. The societal perspective that also includes costs of lost productivity due to hospitalization, doctor visits, and infusions is presented as well. No discounting of costs or outcomes was applied due to the time horizon being less than one year.
4.1. Model Design
Patients with ABSSSI begin treatment in the emergency department (ED) with empiric IV therapy, as shown in Figure 1. They either receive a single dose of dalbavancin or are started with one of the comparators for at least three days of IV antibiotics. Regardless of the choice of treatment, from the emergency room, they can either be directly returned home or hospitalized for three days. On the fourth day, treatment success is assessed either in hospital or via a doctor visit in an outpatient setting for patients who were returned home. Successful treatment with comparators continues for an additional 11 days, potentially switching to oral therapy and managed at home or in an outpatient clinic. If treatment with dalbavancin or comparators fails, patients are assumed to be switched to another antibiotic and hospitalized for 14 days. A 6-month follow-up period monitors for recurrence, with patients hospitalized and treated if recurrence occurs.
4.2. Additional Model Assumptions
Death was not modeled due to the short time horizon and low mortality rate in ABSSSI clinical trials. Patients experiencing treatment failure are assumed to be switched to a different antibiotic class, typically linezolid IV, unless already receiving it, in which case they are assumed to be switching to dalbavancin IV. Patients successfully treated with one of the comparators may continue initial IV treatment, switch to oral treatment, or switch to another IV with a simplified administration schedule, reducing the frequency from twice daily to once daily. For patients who are switched to an oral treatment, they are assumed to be switched to a weighted average of linezolid PO, clindamycin PO, cephalexin PO, cloxacillin PO, trimethoprim/sulfamethoxazole PO, and amoxicillin clavulanic acid PO. For patients who are switched to a simplified IV treatment, a weighted average of ceftriaxone IV, daptomycin IV, and ertapenem IV was used.
Following the initial treatment episode, patients with recurrent infections receive a standard IV treatment, with costs based on a weighted average of vancomycin IV, linezolid IV, cefazolin IV, and ceftriaxone IV. Weights used for treatment average costs are based on the opinion of three clinical experts.
4.3. Treatment Efficacy Parameters
Table 6 summarizes all inputs used within the model. The probability of treatment success (91.4%) and failure (8.6%) was based on pooled results from Boucher et al. (2014),[46] applied uniformly across all compared products. Meta-analyses showed efficacy equivalence among dalbavancin, vancomycin IV, linezolid IV, and daptomycin IV.[50,57] Approximately 16% of ABSSSI patients have kidney dysfunction.[58] For IV antibiotics primarily excreted through the kidneys, such as vancomycin and daptomycin, this condition increases the risk of renal and hepatic toxicity. Consequently, dose reductions are often necessary to manage cumulative toxicity, but this can also result in reduced treatment efficacy.[59] Given that only around 0.6% of the population has severely reduced kidney function, as described in a Coresh et al. study on the prevalence of chronic kidney disease in the US [60], no dosage adjustments for dalbavancin or linezolid were assumed in the model.
For patients with kidney dysfunction, defined as creatinine clearance of 30-70 ml/min,[61] and receiving vancomycin IV or daptomycin IV, the daily dose was reduced: vancomycin IV from 2000 mg to 850 mg and daptomycin IV was administered every other day instead of daily. This dosage adjustment led to reduced treatment costs but also lower treatment success rate. The physician experts consulted during the development of the model provided varying opinions on the treatment success rates for patients with chronic kidney disease (CKD) with reduced dose. Their perspectives ranged from no impact on treatment failure rate (i.e., 8.6% as for the other patients) to a failure rate of 25%. Using the middle point, an average failure rate of 16.8% was used. [62]

Table 6.
Base-case model input parameters.
| Parameter | Base Case | SD | Distribution | Source/Assumptions |
|---|---|---|---|---|
| Proportion with kidney dysfunction | 16.0% | 1.2% | Beta | Lipsky et al, 2012 [53] |
| Rate of clinical failure for patients without kidney dysfunction | 8.6% | 0.8% | Beta | Boucher et al, 2014[46] |
| Rate of clinical failure for patients with kidney dysfunction | 16.8% | 1.7% | Beta | Clinical expert opinion |
| Dalbavancin hospitalization rate | 17.6% | 3.1% | Beta | Talan et al, 2021[63] |
| Other IV hospitalization rate | 37.5% | 3.8% | Beta | Talan et al, 2021[63] |
| Rate of recurrence with IV antibiotics | 16.3% | 0.1% | Beta | May et al. 2017 [19] |
| Increase in recurrence when using oral antibiotics | 24.6% | 2.5% | Beta | Eells et al, 2016[23] |
| Proportion of patients switching to oral antibiotics | 62.0% | 6.2% | Beta | Clinical expert opinion |
| Proportion of patients switching to a q.d. IV | 7.0% | 0.7% | Beta | Clinical expert opinion |
| Dalbavancin treatment cost (1,500 mg) | $2,871.50 | Not varied | Paladin data on file | |
| Vancomycin daily cost without kidney dysfunction (2,000 mg daily) | $37.56 | Not varied | Vancomycin PM [59] and RAMQ « liste des médicaments » [64] | |
| Vancomycin daily cost with kidney dysfunction (850 mg daily) | $15.96 | Not varied | Assumption | |
| Linezolid IV daily cost (1,200 mg daily) | $177.48 | Not varied | Linezolid PM[65] and ODBF[66] | |
| Daptomycin IV cost without kidney dysfunction (456 mg daily, 6 mg/kg or a 76 kg patient) | $148.06 | Not varied | Dose: expert opinion; cost: ODBF[66] | |
| Daptomycin IV cost with kidney dysfunction (456 mg every other day, 6 mg/kg or a 76 kg patient) | $74.03 | Not varied | Assumption: same dosage as without kidney dysfunction but provided every other day instead of daily | |
| Linezolid PO daily cost (1,200 mg daily) | $38.61 | Not varied | Linezolid PM[65] and ODBF[66] | |
| Trimethoprim/salfamethoxazole PO / Trimethoprim PO daily cost (2,400 mg daily) | $0.63 | Not varied | Sulfamethoxazole PM[67] and ODBF[66] | |
| Amoxicillin clavulanic acid PO daily cost (1,750 mg daily) | $1.10 | Not varied | Amoxicillin clavulanic acid PM[68] and ODBF[66] | |
| Clindamycin PO daily cost (1,500 mg daily) | $48.26 | Not varied | Clindamycin PM[69] and ODBF[66] | |
| Cephalexin PO daily cost (2,000 mg daily) | $0.69 | Not varied | Cephalexin PM[70] and ODBF[66] | |
| Cloxacillin PO daily cost (1,500 mg daily) | $1.28 | Not varied | Cloxacillin PM[71] and ODBF[66] | |
| Ertapenem IV daily cost (1,000 mg daily) | $52.27 | Not varied | Ertapenem PM[72] and ODBF[66] | |
| Length of treatment (days) | 14 | 1.4 | Normal | Assumption |
| Hospital cost: 3 days | $7,671.79 | 767.18 | Gamma | CIHI Patient Cost Estimator (2021-2022)[73] |
| Doctor office cost (per visit) | $75.39 | 7.54 | Gamma | RAMQ Manuel Rénumération à l’acte. Médecin spécialiste[64] |
| Catheter (62% utilisation, cost: $36.49) or PICC-line (38% utilisation; cost: $392.99) cost | $171.96 | 17.20 | Gamma | PICC cost: CADTH HTIS[74], catheter cost: RAMQ, Manuel Rémunération à l’acte[64]; distribution: expert opinion |
| Infusion cost (nurse hourly rate) | $42.99 | 4.30 | Gamma | CANSIM 282-0152[75] |
| Infusion times (hours per day) | ||||
| Dalbavancin | 0.50 | Not varied | Dalbavancin PM [45] | |
| Vancomycin IV | 3.33 | Not varied | Vancomycin PM [58] | |
| Linezolid IV | 2.50 | Not varied | Linezolid PM [65] | |
| Daptomycin IV | 0.50 | Not varied | Daptomycin PM [76] | |
| Ertapenem IV | 0.50 | Not varied | Ertapenem PM [72] | |
| Productivity loss cost | ||||
| Employment rate | 61% | Statistics Canada[77] | ||
| Average hourly earnings | $35.35 | Statistics Canada[78] | ||
| Hours lost per days of hospitalisation (8 hours per day 5/7 days) | 5.71 | Assumption | ||
| Utility admitted patients | 0.600 | 0.060 | Gamma | Lipsky 2012[53] |
| Utility discharged patients | 0.800 | 0.080 | Gamma | Lipsky 2012[53] |
| Utility cured | 0.832 | 0.083 | Gamma | Health Quality Council of Alberta 2016[79] |
IV, intravenous; PO, per os (oral); PM, Product monograph; ODBF, Ontario Drug Benefit Formulary. Note: All costs are expressed in Canadian 2024 dollars, inflated to 2024 when needed using an Ontario Consumer Price Index[66]. Costs are based on Ontario values when available, Québec values were used otherwise.
4.4. Resource Utilisation
The hospitalization rates for ABSSSI patients were sourced from Talan et al. (2021).[63] This study conducted a pre- and post-intervention trial showing that only 17.6% of patients treated with dalbavancin were hospitalized, compared to 37.5% under usual care. For patients not admitted to the hospital, one additional doctor visit at Day 4 was included. For comparator treatments, 62% of patients used catheters [64] and 38% used PICC lines.[80] Infusion costs were calculated using a nurse’s hourly rate.[75] Infusion duration for the different IV antibiotics were based on treatment respective product monographs [45,58,59,65,72,76].
4.5. Costs
4.6. Sub-Population and Scenario Analyses
Sub-populations of particular interest for dalbavancin were examined separately. These included:
- Patients with kidney dysfunction: The base case includes 16% of patients with kidney dysfunction requiring dose adjustments for vancomycin IV and daptomycin IV. This scenario focuses on this subpopulation.
- PWID, the homeless population, and patients in remote locations: Approximately 893,000 Canadians (2.2% of the total population) are homeless, PWID (many of whom also suffer from psychiatric illness), or both [81,82,83]. This group faces a significantly higher risk of developing ABSSSI, accounting for 30.4% of ABSSSI patients [24,25]. Analysis explored treatment pathways for these three sub-populations, comparing the use of dalbavancin, with discharge probabilities and hospital admission rates maintained the same as in the base case, versus other IV antibiotics, necessitating full-course hospitalization.
A particularly noteworthy scenario analysis that merits highlighting:
- No hospitalization for dalbavancin, 100% hospitalization for comparators (non-severe): Because of its convenient administration as a single-dose treatment, dalbavancin has the potential to reduce the hospital admission rates; however, the exact impact is associated with uncertainty. The other treatments considered in the model are administered daily (e.g., vancomycin IV typically is administered twice (or three times) daily using a 100-minute infusion for a period of treatment of 3 to 14 days, or more). A Canadian clinical expert that was consulted explained that there are situations where an ABSSSI patient requires IV antibiotics but may not need to be hospitalized for additional intervention or observation. If this situation occurs and the patient is being administered dalbavancin, the patient can return home. If the patient is administered any other IV treatment and ambulatory care is not available, hospitalization is required until ambulatory care can be organised, and patients may remain in the emergency room or a corridor because no beds are available. This scenario analyzes the impact of discharging non-severe ABSSSI patients treated with dalbavancin directly from the ED versus hospitalizing those treated with comparators.
An additional scenario analysis was conducted reducing the length of treatment for comparators:
- 12-Day comparator treatment: Dalbavancin administered as a single 1500 mg dose was considered equivalent to 14 days of IV vancomycin followed by a possible switch to oral antibiotics based on clinical trials [46,84]. The base case relies on these efficacy data and considered that patients using one of the comparators would be treated for 14 days. This scenario explored a shorter length of antibiotic administration: 12 days.
4.6. HRQoL
Utilities in the model were based on Lipsky et al. 2012 [53]. This was a US prospective observational study of hospitalized complicated skin and soft tissue treatment. infections (cSSTI) patients reporting the EQ-5D at hospital admission and at hospital discharge. These values were used in the model to distinguish patients who were treated in hospital vs, those who were treated at home [53].
The utility of patients cured was based on the EQ-5D index norms from the Health Quality Council of Alberta, 2016 [79]. The index norm was provided by gender and age group. The utility for proportion of male of 58% and the 50–59 years old age group (based on an average age of 50 years) were selected from Boucher et al. 2014 [46]. The resulting utility values used in the model are reported in Table 6.
5. Conclusions
According to the model presented in this study, dalbavancin is a cost-effective treatment option, that enables clinicians to treat Canadian adult patients with ABSSSI across various clinical settings using a single-dose treatment. This medication is particularly beneficial for at-risk populations, including First Nations, the homeless, and PWID. These groups often face barriers to accessing hospital care, have difficulties with treatment adherence and may find outpatient treatment suboptimal.
Dalbavancin may offer cost-saving advantages for Canadian healthcare providers due to several key factors:
- Reduced hospitalization time; Dalbavancin’s long half-life allows for a single-dose regimen, significantly reducing hospital stays compared to standard treatments that require multiply daily infusions administered for multiple days. Shorter hospital stays can lead to lower hospitalization costs.
- Lower administration costs; Traditional antibiotics like vancomycin IV require multiple daily infusions administered for multiple days. Dalbavancin’s shorter dosing schedule reduces the need for frequent professional involvement, thereby decreasing labor costs.
- Optimized patient compliance; Dalbavancin’s shorter dosing regimen optimizes patient adherence to the treatment plan, leading to better outcomes and potentially reducing the need for additional treatments or hospital readmissions.
- Cost savings through resource optimization; By decreasing the need for repeated infusions and extended hospital stays, cost savings occur, and healthcare resources can be optimized and reallocated to other critical areas.
- Minimized risk of nosocomial infections; With fewer hospital visits and reduced patient interaction with healthcare environments, the risk of HAIs may be lower. This reduction in HAIs can lead to cost savings associated with treating such infections.
- Quarantine and staffing considerations; Minimizing patient-HCP interactions reduces the risk of virus transmission. This reduction can help maintain a stable workforce by decreasing the number of healthcare workers needing to quarantine, thus avoiding staffing shortages and the associated costs of hiring temporary staff.
In summary, as shown in our model, dalbavancin offers significant cost savings for Canadian healthcare providers through reduced hospitalization time, lower administration and labor costs, minimized risk of HAIs, improved patient compliance, and optimized resource allocation.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Supplemental File S1: Dalbavancin Cost Calculator.
Author Contributions
Conceptualization, V.L. and K.P-A.; methodology, V.L.; software, V.L. and K.P-A.; validation, V.L..; formal analysis, V.L.; investigation, V.L.; data curation, V.L..; writing—original draft preparation, D.C. and V.L.; writing—review and editing, G.G.Z., J.B., and N.J-S.; visualization, V.L. and D.C.; project administration, V.L. and D.C..; funding acquisition, K.P-A. and N.J-S. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Paladin Pharma.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All model inputs are based on literature or on expert opinion. Other than averaging expert estimates, no new data was created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
Veronique Lauzon and Dagmara Chojecki are consultants for Paladin Pharma, manufacturer of dalbavancin. Dr. George G. Zhanel and Dr. Joseph Blondeau received compensation from Paladin Pharma for time spent consulting on this analysis. Kayla Paulo-Alexandre and Natasha Jakac-Sinclair are employees of Paladin Pharma. Paladin Pharma provided financial support for the analysis described in this article, for writing assistance, and for publishing this article.
References
- US Department of Health and Human Services; Center for Drug Evaluation and Research (CDER). Guidance for Industry: Acute Bacterial Skin and Skin Structure Infections: Developing Drugs for treatment. 2013.
- Esposito, S.; Leone, S.; Petta, E.; Noviello, S.; Ianniello, F. Treatment options for skin and soft tissue infections caused by meticillin-resistant Staphylococcus aureus: oral vs.parenteral; home vs. hospital. Int J Antimicrob Agents 2009, 34 Suppl 1, S30-35. [CrossRef]
- Pulido-Cejudo, A.; Guzman-Gutierrez, M.; Jalife-Montano, A.; Ortiz-Covarrubias, A.; Martinez-Ordaz, J.L.; Noyola-Villalobos, H.F.; Hurtado-Lopez, L.M. Management of acute bacterial skin and skin structure infections with a focus on patients at high risk of treatment failure. Ther Adv Infect Dis 2017, 4, 143–161. [Google Scholar] [CrossRef] [PubMed]
- Baibergenova, A.; Drucker, A.M.; Shear, N.H. Hospitalizations for cellulitis in Canada: A database study. J Cutan Med Surg 2014, 18, 33–37. [Google Scholar] [CrossRef] [PubMed]
- Soriano, A.; Rossolini, G.M.; Pea, F. The role of dalbavancin in the treatment of acute bacterial skin and skin structure infections (ABSSSIs). Expert Rev Anti Infect Ther 2020, 18, 415–422. [Google Scholar] [CrossRef]
- Russo, A.; Concia, E.; Cristini, F.; De Rosa, F.G.; Esposito, S.; Menichetti, F.; Petrosillo, N.; Tumbarello, M.; Venditti, M.; Viale, P.; et al. Current and future trends in antibiotic therapy of acute bacterial skin and skin-structure infections. Clin Microbiol Infect 2016, 22 Suppl 2, S27–36. [Google Scholar] [CrossRef]
- Leuthner, K.D.; Buechler, K.A.; Kogan, D.; Saguros, A.; Lee, H.S. Clinical efficacy of dalbavancin for the treatment of acute bacterial skin and skin structure infections (ABSSSI). Ther Clin Risk Manag 2016, 12, 931–940. [Google Scholar] [CrossRef]
- Potashman, M.H.; Stokes, M.; Liu, J.; Lawrence, R.; Harris, L. Examination of hospital length of stay in Canada among patients with acute bacterial skin and skin structure infection caused by methicillin-resistant Staphylococcus aureus. Infect Drug Resist 2016, 9, 19–33. [Google Scholar] [CrossRef]
- Jeong, D.; Nguyen, H.N.T.; Tyndall, M.; Schreiber, Y.S. Antibiotic use among twelve Canadian First Nations communities: A retrospective chart review of skin and soft tissue infections. BMC Infect Dis 2020, 20, 118. [Google Scholar] [CrossRef]
- Borgundvaag, B.; Ng, W.; Rowe, B.; Katz, K. Prevalence of methicillin-resistant Staphylococcus aureus in skin and soft tissue infections in patients presenting to Canadian emergency departments. CJEM 2013, 15, 141–160. [Google Scholar] [CrossRef]
- Institut national d’excellence en santé et services sociaux. ZYVOXAMMC – Infections à staphylocoques résistants à la méthicilline - Février 2013. 1–6.
- Stevens, D.L.; Bisno, A.L.; Chambers, H.F.; Dellinger, E.P.; Goldstein, E.J.; Gorbach, S.L.; Hirschmann, J.V.; Kaplan, S.L.; Montoya, J.G.; Wade, J.C.; et al. Practice guidelines for the diagnosis and management of skin and soft tissue infections: 2014 update by the Infectious Diseases Society of America. Clin Infect Dis 2014, 59, e10–52. [Google Scholar] [CrossRef]
- Scott, L.J. Dalbavancin: a review in acute bacterial skin and skin structure infections. Drugs 2015, 75, 1281–1291. [Google Scholar] [CrossRef]
- Schrock, J.W.; Laskey, S.; Cydulka, R.K. Predicting observation unit treatment failures in patients with skin and soft tissue infections. Int J Emerg Med 2008, 1, 85–90. [Google Scholar] [CrossRef] [PubMed]
- Walsh, T.L.; Chan, L.; Konopka, C.I.; Burkitt, M.J.; Moffa, M.A.; Bremmer, D.N.; Murillo, M.A.; Watson, C.; Chan-Tompkins, N.H. Appropriateness of antibiotic management of uncomplicated skin and soft tissue infections in hospitalized adult patients. BMC Infect Dis 2016, 16, 721. [Google Scholar] [CrossRef] [PubMed]
- Berger, A.; Oster, G.; Edelsberg, J.; Huang, X.; Weber, D.J. Initial treatment failure in patients with complicated skin and skin structure infections. Surg Infect (Larchmt) 2013, 14, 304–312. [Google Scholar] [CrossRef] [PubMed]
- Nathwani, D.; Dryden, M.; Garau, J. Early clinical assessment of response to treatment of skin and soft-tissue infections: how can it help clinicians? Perspectives from Europe. Int J Antimicrob Agents 2016, 48, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Crum-Cianflone, N.; Weekes, J.; Bavaro, M. Recurrent community-associated methicillin-resistant Staphylococcus aureus infections among HIV-infected persons: incidence and risk factors. AIDS Patient Care STDS 2009, 23, 499–502. [Google Scholar] [CrossRef]
- May, L.; Klein, E.Y.; Martinez, E.M.; Mojica, N.; Miller, L.G. Incidence and factors associated with emergency department visits for recurrent skin and soft tissue infections in patients in California, 2005-2011. Epidemiol Infect 2017, 145, 746–754. [Google Scholar] [CrossRef]
- May, L.S.; Zocchi, M.; Zatorski, C.; Jordan, J.A.; Rothman, R.E.; Ware, C.E.; Eells, S.; Miller, L. Treatment failure outcomes for emergency department patients with skin and soft tissue infections. West J Emerg Med 2015, 16, 642–652. [Google Scholar] [CrossRef]
- Miller, L.G.; Eells, S.J.; David, M.Z.; Ortiz, N.; Taylor, A.R.; Kumar, N.; Cruz, D.; Boyle-Vavra, S.; Daum, R.S. Staphylococcus aureus skin infection recurrences among household members: an examination of host, behavioral, and pathogen-level predictors. Clin Infect Dis 2015, 60, 753–763. [Google Scholar] [CrossRef]
- Sreeramoju, P.; Porbandarwalla, N.S.; Arango, J.; Latham, K.; Dent, D.L.; Stewart, R.M.; Patterson, J.E. Recurrent skin and soft tissue infections due to methicillin-resistant Staphylococcus aureus requiring operative debridement. Am J Surg 2011, 201, 216–220. [Google Scholar] [CrossRef]
- Eells, S.J.; Nguyen, M.; Jung, J.; Macias-Gil, R.; May, L.; Miller, L.G. Relationship between adherence to oral antibiotics and postdischarge clinical outcomes among patients hospitalized with staphylococcus aureus skin infections. Antimicrob Agents Chemother 2016, 60, 2941–2948. [Google Scholar] [CrossRef]
- Moran, G.J.; De Anda, C.; Das, A.F.; Green, S.; Mehra, P.; Prokocimer, P. Efficacy and safety of tedizolid and linezolid for the treatment of acute bacterial skin and skin structure infections in injection drug users: Analysis of two clinical trials. Infect Dis Ther 2018, 7, 509–522. [Google Scholar] [CrossRef] [PubMed]
- Bork, J.T.; Heil, E.L.; Berry, S.; Lopes, E.; Dave, R.; Gilliam, B.L.; Amoroso, A. Dalbavancin use in vulnerable patients receiving outpatient parenteral antibiotic therapy for invasive Gram-positive infections. Infect Dis Ther 2019, 8, 171–184. [Google Scholar] [CrossRef] [PubMed]
- Beieler, A.; Magaret, A.; Zhou, Y.; Schleyer, A.; Wald, A.; Dhanireddy, S. Outpatient parenteral antimicrobial therapy in vulnerable populations-- People who inject drugs and the momeless. J Hosp Med 2019, 14, 105–109. [Google Scholar] [CrossRef]
- Oosterveer, T.M.; Young, T.K. Primary health care accessibility challenges in remote indigenous communities in Canada’s North. Int J Circumpolar Health 2015, 74, 29576. [Google Scholar] [CrossRef]
- National Collaborating Centre for Indigineous Health. Social Determinants of Health: ACCESS TO HEALTH SERVICES AS A SOCIAL DETERMINANT OF FIRST NATIONS, INUIT AND MÉTIS HEALTH; 2019.
- Gonzalez, P.L.; Rappo, U.; Mas Casullo, V.; Akinapelli, K.; McGregor, J.S.; Nelson, J.; Nowak, M.; Puttagunta, S.; Dunne, M.W. Safety of dalbavancin in the treatment of acute bacterial skin and skin structure infections (ABSSSI): Nephrotoxicity rates compared with vancomycin: A post hoc analysis of three clinical trials. Infect Dis Ther 2021, 10, 471–481. [Google Scholar] [CrossRef]
- Sivagnanam, S.; Deleu, D. Red man syndrome. Crit Care 2003, 7, 119–120. [Google Scholar] [CrossRef]
- Martel, T.; Jamil, R.; King, K. Vancomycin Flushing Syndrome. StatPearls [Internet] 2024.
- Martin, J.H.; Norris, R.; Barras, M.; Roberts, J.; Morris, R.; Doogue, M.; Jones, G.R. Therapeutic monitoring of vancomycin in adult patients: A consensus review of the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, and the Society Of Infectious Diseases Pharmacists. Clin Biochem Rev 2010, 31, 21–24. [Google Scholar]
- Rybak, M.J.; Le, J.; Lodise, T.P.; Levine, D.P.; Bradley, J.S.; Liu, C.; Mueller, B.A.; Pai, M.P.; Wong-Beringer, A.; Rotschafer, J.C.; et al. Therapeutic monitoring of vancomycin for serious methicillin-resistant Staphylococcus aureus infections: A revised consensus guideline and review by the American Society of Health-System Pharmacists, the Infectious Diseases Society of America, the Pediatric Infectious Diseases Society, and the Society of Infectious Diseases Pharmacists. Am J Health Syst Pharm 2020, 77, 835–864. [Google Scholar] [CrossRef]
- Liu, C.; Mao, Z.; Yang, M.; Kang, H.; Liu, H.; Pan, L.; Hu, J.; Luo, J.; Zhou, F. Efficacy and safety of daptomycin for skin and soft tissue infections: A systematic review with trial sequential analysis. Ther Clin Risk Manag 2016, 12, 1455–1466. [Google Scholar] [CrossRef]
- Vargese, S.S.; Dev, S.S.; Soman, A.S.; Kurian, N.; Varghese, V.A.; Mathew, E. Exposure risk and COVID-19 infection among frontline health-care workers: A single tertiary care centre experience. Clin Epidemiol Glob Health 2022, 13, 100933. [Google Scholar] [CrossRef]
- Caputo, W.J.; Johnson, E.S.; Fahoury, G.; Monterosa, P. Dalbavancin during the COVID-19 pandemic. Surg Technol Int 2022, 41. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, L.H.; Drew, D.A.; Joshi, A.D.; Guo, C.G.; Ma, W.; Mehta, R.S.; Sikavi, D.R.; Lo, C.H.; Kwon, S.; Song, M.; et al. Risk of COVID-19 among frontline healthcare workers and the general community: A prospective cohort study. medRxiv 2020. [Google Scholar] [CrossRef]
- Kaye, K.S.; Patel, D.A.; Stephens, J.M.; Khachatryan, A.; Patel, A.; Johnson, K. Rising United States hospital admissions for acute bacterial skin and skin structure infections: recent trends and economic impact. PLoS One 2015, 10, e0143276. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.Y.; Singh, A.; David, M.Z.; Bartsch, S.M.; Slayton, R.B.; Huang, S.S.; Zimmer, S.M.; Potter, M.A.; Macal, C.M.; Lauderdale, D.S.; et al. The economic burden of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA). Clin Microbiol Infect 2013, 19, 528–536. [Google Scholar] [CrossRef]
- Ostermann, H.; Blasi, F.; Medina, J.; Pascual, E.; McBride, K.; Garau, J. Resource use in patients hospitalized with complicated skin and soft tissue infections in Europe and analysis of vulnerable groups: the REACH study. J Med Econ 2014, 17, 719–729. [Google Scholar] [CrossRef]
- Edelsberg, J.; Taneja, C.; Zervos, M.; Haque, N.; Moore, C.; Reyes, K.; Spalding, J.; Jiang, J.; Oster, G. Trends in US hospital admissions for skin and soft tissue infections. Emerg Infect Dis 2009, 15, 1516–1518. [Google Scholar] [CrossRef]
- Lipsky, B.A.; Weigelt, J.A.; Gupta, V.; Killian, A.; Peng, M.M. Skin, soft tissue, bone, and joint infections in hospitalized patients: epidemiology and microbiological, clinical, and economic outcomes. Infect Control Hosp Epidemiol 2007, 28, 1290–1298. [Google Scholar] [CrossRef]
- Suaya, J.A.; Mera, R.M.; Cassidy, A.; O’Hara, P.; Amrine-Madsen, H.; Burstin, S.; Miller, L.G. Incidence and cost of hospitalizations associated with Staphylococcus aureus skin and soft tissue infections in the United States from 2001 through 2009. BMC Infect Dis 2014, 14, 296. [Google Scholar] [CrossRef]
- Itani, K.M.; Merchant, S.; Lin, S.J.; Akhras, K.; Alandete, J.C.; Hatoum, H.T. Outcomes and management costs in patients hospitalized for skin and skin-structure infections. Am J Infect Control 2011, 39, 42–49. [Google Scholar] [CrossRef]
- XYDALBA® (dalbavancin for injection) Product Monograph. 2021, 1–33.
- Boucher, H.W.; Wilcox, M.; Talbot, G.H.; Puttagunta, S.; Das, A.F.; Dunne, M.W. Once-weekly dalbavancin versus daily conventional therapy for skin infection. N Engl J Med 2014, 370, 2169–2179. [Google Scholar] [CrossRef]
- Dunne, M.W.; Puttagunta, S.; Giordano, P.; Krievins, D.; Zelasky, M.; Baldassarre, J. A randomized clinical trial of single-dose versus weekly dalbavancin for treatment of acute bacterial skin and skin structure infection. Clin Infect Dis 2016, 62, 545–551. [Google Scholar] [CrossRef] [PubMed]
- Zhanel, G.; Silverman, M.; Malhotra, J.; Baxter, M.; Rahimi, R.; Irfan, N.; Girouard, G.; Dhami, R.; Kucey, M.; Stankus, V.; et al. Real-life experience with IV dalbavancin in Canada; results from the CLEAR (Canadian LEadership on Antimicrobial Real-life usage) registry. J Glob Antimicrob Resist 2024, 38, 154–157. [Google Scholar] [CrossRef] [PubMed]
- Di Gennaro, F. Prescriptive appropriateness of dalbavancin in acute bacterial skin and skin structure infections in adults: An integrated approach between clinical profile, patient- and health system-related factors and focus on environmental impact. Front Antibiot 2024, 3. [Google Scholar] [CrossRef]
- Guest, J.F.; Esteban, J.; Manganelli, A.G.; Novelli, A.; Rizzardini, G.; Serra, M. Comparative efficacy and safety of antibiotics used to treat acute bacterial skin and skin structure infections: Results of a network meta-analysis. PLoS One 2017, 12, e0187792. [Google Scholar] [CrossRef] [PubMed]
- Marcellusi, A.; Viti, R.; Sciattella, P.; Sarmati, L.; Streinu-Cercel, A.; Pana, A.; Espin, J.; Horcajada, J.P.; Favato, G.; Andretta, D.; et al. Economic evaluation of the treatment of acute bacterial skin and skin structure infections (ABSSSIs) from the national payer perspective: introduction of a new treatment to the patient journey. A simulation of three European countries. Expert Rev Pharmacoecon Outcomes Res 2019, 19, 581–599. [Google Scholar] [CrossRef]
- All Wales Medicines Strategy Group. Secretariat Assessment Report Dalbavancin (XYDALBA®) 500 mg powder for concentrate for solution for infusion. 1–20.
- Lipsky, B.A.; Moran, G.J.; Napolitano, L.M.; Vo, L.; Nicholson, S.; Kim, M. A prospective, multicenter, observational study of complicated skin and soft tissue infections in hospitalized patients: Clinical characteristics, medical treatment, and outcomes. BMC Infect Dis 2012, 12, 227. [Google Scholar] [CrossRef]
- Streifel, A.C.; Sikka, M.K.; Bowen, C.D.; Lewis, J.S., 2nd. Dalbavancin use in an academic medical centre and associated cost savings. Int J Antimicrob Agents 2019, 54, 652–654. [Google Scholar] [CrossRef]
- Falconer, S. Two years’ experience treating acute bacterial skin and skin-structure infections with dalbavancin in a real-world OPAT setting. P2296 Abstract presented at the 29th ECCMID; Amsterdam, Netherlands; 13–16 April 2019.
- Wilke, M.; Worf, K.; Preisendörfer, B.; Heinlein, W.; Kast, T.; Bodmann, K.F. Potential savings through single-dose intravenous dalbavancin in long-term MRSA infection treatment - a health economic analysis using German DRG data. GMS Infect Dis 2019, 7, Doc03. [Google Scholar] [CrossRef]
- Vardakas, K.Z.; Mavros, M.N.; Roussos, N.; Falagas, M.E. Meta-analysis of randomized controlled trials of vancomycin for the treatment of patients with gram-positive infections: Focus on the study design. Mayo Clin Proc 2012, 87, 349–363. [Google Scholar] [CrossRef]
- Vancomycin hydrochloride for injection USP for intravenous use: Prescribing Information. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2018/209481s000lbl.pdf (accessed on October 27, 2024).
- Vancomycin hydrochloride for injection USP. (Vancomycin Hydrochloride) 500 mg, 1 g, 5 g and 10 g of vancomycin (as vancomycin hydrochloride) per vial. Sterile lyophilized powder for solution. Product Monograph. 2021, 1–29.
- Coresh, J.; Selvin, E.; Stevens, L.A.; Manzi, J.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Levey, A.S. Prevalence of chronic kidney disease in the United States. JAMA 2007, 298, 2038–2047. [Google Scholar] [CrossRef]
- Matzke, G.R.; Zhanel, G.G.; Guay, D.R. Clinical pharmacokinetics of vancomycin. Clin Pharmacokinet 1986, 11, 257–282. [Google Scholar] [CrossRef] [PubMed]
- Zhanel, G.; Loeb, M. Consultation on treatment success rates for patients with chronic kidney disease (CKD) with reduced dose vacomycin. and 22, 2021. 3 June.
- Talan, D.A.; Mower, W.R.; Lovecchio, F.A.; Rothman, R.E.; Steele, M.T.; Keyloun, K.; Gillard, P.; Copp, R.; Moran, G.J. Pathway with single-dose long-acting intravenous antibiotic reduces emergency department hospitalizations of patients with skin infections. Acad Emerg Med 2021. [CrossRef] [PubMed]
- Régie de l’assurance maladie du Québec. Manuels et guides de facturation. Available online: https://www.ramq.gouv.qc.ca/fr/professionnels/medecins-specialistes/manuels/Pages/remuneration-acte.aspx (accessed on July 7, 2024).
- Linezolid Injection Product Monograph. 2018.
- Government of Ontario. Ontario Drug Benefit Formulary/Comparative Drug Index. Available online: https://www.formulary.health.gov.on.ca/formulary/ (accessed on Jan 21, 2024).
- Sulfamethoxazole and Trimethoprim Product Monograph. 2018.
- Clavulin Product Monograph. 2020.
- Clindamycin Product Monograph. 2015, 1–28.
- Cephalexin Tablets and Oral Suspensions Product Monograph. 2018.
- Cloxacillin capsules Product Monograph. 2018, 1–13.
- Ertapenem for Injection Product Monograph. 2019.
- Canadian Institute for Health Information. Patient Cost Estimator. Available online: https://www.cihi.ca/en/patient-cost-estimator (accessed on July 18, 2024).
- Canadian Agency for Drugs and Technologies in Health; Health Technology Inquiry Service. Peripherally Inserted Central Catheter (PICC) Stabilization Devices: Clinical and Cost-Effectiveness and Guidelines for Use. Available online: https://www.cadth.ca/media/pdf/htis/Peripherally%20Inserted%20Central%20Catheter%20(PICC)%20Stabilization%20Devices%20Clinical%20and%20Cost-Effectiveness.pdf (accessed on day month year).
- Statistics Canada. Employee wages by occupation, annual, inactive. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1410030701&pickMembers%5B0%5D=1.9&pickMembers%5B1%5D=2.2&pickMembers%5B2%5D=3.1&pickMembers%5B3%5D=5.1&pickMembers%5B4%5D=6.1&cubeTimeFrame.startYear=2014&cubeTimeFrame.endYear=2018&referencePeriods=20140101%2C20180101 (accessed on July 7, 2024).
- Cubist, Pharmaceuticals; Inc., S.P.C. Cubist Pharmaceuticals; Inc., S.P.C. Daptomycin for Injection Product Monograph. 2020.
- Statistics Canada. Table 14-10-0287-03 Labour force characteristics by province, monthly, seasonally, adjusted (Ontario) Available online:. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1410028703&pickMembers%5B0%5D=3.1&pickMembers%5B1%5D=4.6&cubeTimeFrame.startMonth=05&cubeTimeFrame.startYear=2021&referencePeriods=20210501%2C20210501 (accessed on July 7, 2024).
- Statistics Canada. Statistics Canada: Average hourly earnings for employees paid by the hour, by industry, annual (Ontario) adjusted to 2021 using the annual growth rate from 2016 to 2020. Available online: https://www150.statcan.gc.ca/t1/tbl1/en/tv.action?pid=1410020601&pickMembers%5B0%5D=1.7&pickMembers%5B1%5D=2.1&cubeTimeFrame.startYear=2016&cubeTimeFrame.endYear=2020&referencePeriods=20160101%2C20200101 (accessed on November 2, 2023).
- Health Quality Council of Alberta. EQ-5D-5L index norms for Alberta population. 2016, 1–8.
- Canadian Agency for Drugs and Technologies in Health. Peripherally inserted central catheter (PICC) stabilization devices: clinical and cost-effectiveness and guidelines for use. 2008, 1–9.
- The Homelessness Partnering Secretariat (HPS) Canada 2019. Available online: https://www.homelesshub.ca/about-homelessness/homelessness-101/how-many-people-are-homeless-canada (accessed on October 28, 2024).
- Grinman, M.N.; Chiu, S.; Redelmeier, D.A.; Levinson, W.; Kiss, A.; Tolomiczenko, G.; Cowan, L.; Hwang, S.W. Drug problems among homeless individuals in Toronto, Canada: Prevalence, drugs of choice, and relation to health status. BMC Public Health 2010, 10, 94. [Google Scholar] [CrossRef] [PubMed]
- Health Canada. Canadian Alcohol and Drug Use Monitoring Survey, 2012. Available online: https://www.canada.ca/en/health-canada/services/health-concerns/drug-prevention-treatment/drug-alcohol-use-statistics/canadian-alcohol-drug-use-monitoring-survey-summary-results-tables-2012.html (accessed on January 10, 2024).
- Ramdeen, S.; Boucher, H.W. Dalbavancin for the treatment of acute bacterial skin and skin structure infections. Expert Opin Pharmacother 2015, 16, 2073–2081. [Google Scholar] [CrossRef]
Figure 1.
Schematic overview of the decision tree for the patients with non-severe ABSSSI IV, intravenous. Note: Boxed letter (ie, A, B, etc.) indicate the structure is mirrored on both branches of the decision tree.
Figure 1.
Schematic overview of the decision tree for the patients with non-severe ABSSSI IV, intravenous. Note: Boxed letter (ie, A, B, etc.) indicate the structure is mirrored on both branches of the decision tree.
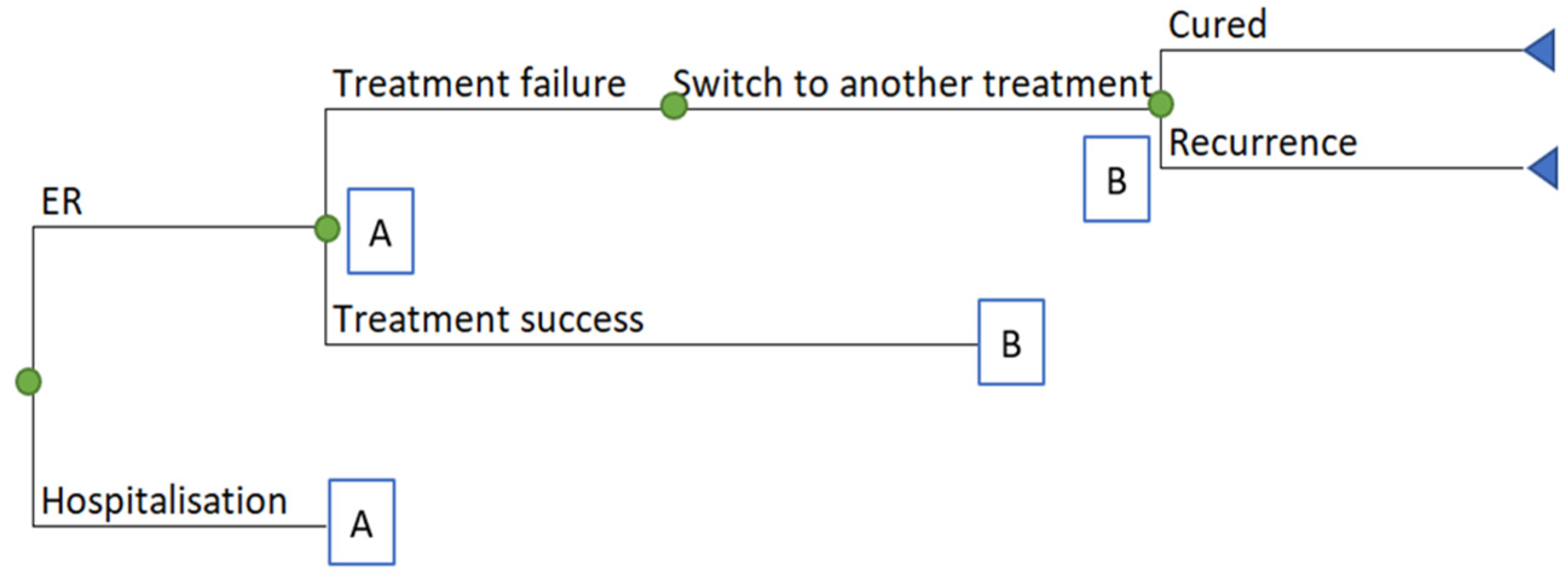
Table 1.
Base-case deterministic results.
| Parameter | Dalbavancin | Vancomycin | Linezolid IV | Daptomycin IV |
|---|---|---|---|---|
| Days of hospital saved | ||||
|
Number of days of hospital |
1.7 | 2.5 | 2.3 | 2.5 |
| Costs ($) | ||||
|
Total cost healthcare perspective (without productivity loss) |
7,668 | 7,968 | 8,208 | 8,041 |
|
Total cost societal perspective (with productivity loss) |
7,955 | 8,685 | 8,842 | 8,545 |
| Drug | 2,872 | 284 | 1,164 | 957 |
| Subsequent treatment | 214 | 246 | 247 | 246 |
| Hospitalization | 4,436 | 6,429 | 5,969 | 6,429 |
|
Drug administration (infusion) |
15 | 894 | 722 | 293 |
| Other medical resources | 131 | 115 | 116 | 115 |
| Productivity | 288 | 717 | 634 | 504 |
| QALYs | 0.4467 | 0.4462 | 0.4463 | 0.4462 |
Table 2.
Sub-population. Patients with kidney dysfunction.
| Comparison | Δ QALY | Δ Costs | Cost/QALY |
|---|---|---|---|
| dalbavancin vs. vancomycin IV | 0.0010 | –2,775 | Dominant |
| dalbavancin vs. linezolid IV | 0.0003 | –541 | Dominant |
| dalbavancin vs daptomycin IV | 0.0010 | –2,551 | Dominant |
Table 3.
Sub-population. PWID and the homeless population.
| Comparison | Δ QALY | Δ Costs | Cost/QALY |
|---|---|---|---|
| dalbavancin vs. vancomycin IV | 0.0069 | –29,598 | Dominant |
| dalbavancin vs. linezolid IV | 0.0069 | –30,377 | Dominant |
| dalbavancin vs daptomycin IV | 0.0069 | –30,271 | Dominant |
Table 4.
No hospital admission for dalbavancin and 100% admission for comparators.
| Comparison | Δ QALY | Δ Costs | Cost/QALY |
|---|---|---|---|
| dalbavancin vs. vancomycin IV | 0.0017 | –6,120 | Dominant |
| dalbavancin vs. linezolid IV | 0.0016 | –6,427 | Dominant |
| dalbavancin vs daptomycin IV | 0.0017 | –6,421 | Dominant |
Table 5.
Comparator days of treatment: 12 days.
| Comparison | Δ QALY | Δ Costs | Cost/QALY |
|---|---|---|---|
| dalbavancin vs. vancomycin IV | 0.0004 | –113 | Dominant |
| dalbavancin vs. linezolid IV | 0.0003 | –393 | Dominant |
| dalbavancin vs daptomycin IV | 0.0004 | –187 | Dominant |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



