
Submitted:
15 November 2024
Posted:
19 November 2024
You are already at the latest version
Abstract
Background: The extraction of impacted third molars presents anatomical challenges and surgical risks, prompting debate over prophylactic removal, particularly for impacted lower molars.
Types of Studies Reviewed: This meta-analysis was conducted according to PRISMA guidelines, included studies from 2000 to 2024. This meta-analysis examined the relationship between the mesioangular position of impacted third molars and pathological changes, including bone loss adjacent to the second molar.
Results: Of the 2943 studies initially identified, 10 studies (2163 patients) met the inclusion criteria, 4 studies included in the meta-analysis. Statistical analysis revealed that horizontally impacted third molars showed a higher percentage of pathological change (41%) compared to vertically (20.7%), mesioangular (21.4%), and distoangular (9.7%) molars. Additionally, cystic degeneration and bone loss distal to the second molar were frequently observed, with increased incidence in patients aged 20-25. Significant heterogeneity among studies was noted, and a need for consistent monitoring of impacted third molars was recommended.
Practical Implications: The findings suggest that impacted third molars, even when asymptomatic, pose a risk for adjacent structures and warrant careful evaluation. Routine imaging and close monitoring of follicular and bone changes may enhance preventive care, particularly for horizontally impacted third molars with higher rates of pathological changes.
Keywords:
impacted third molars
; pathological changes
; mesioangular position
; meta-analysis
; alveolar bone loss
1. Introduction
The extraction of impacted third molars is one of the most requested procedures in oral surgery clinics. Private professional studies often prefer to refer their patients to university clinics or hospitals due to the intrinsic operational difficulty of the intervention and the professional risk involved. Surgery involving the third molars can present intraoperative challenges and complex postoperative patient management, potentially requiring numerous appointments for dressings. Complications related to various surgical and anatomical factors can occur [1,2,3].
The extraction of lower third molars, in particular, is a complex surgery due to the anatomical position of the molars, proximity to vital anatomical structures, and limited operative space. The appropriateness of preventive extraction of the lower third molar is still debated [4].
In recent years, the number of extractions of impacted third molars in the UK has significantly decreased after the update of the NICE guidelines in 1997, during which the retention of asymptomatic third molars was recommended [5]. Until the mid-1990s, the extraction of impacted third molars was one of the most common surgical interventions performed on young adults in the UK. This surgical procedure requires substantial human and economic resources. A scientific study revealed that 20-30% of these interventions did not follow American guidelines in 1998, and there was insufficient evidence to justify the prophylactic removal of asymptomatic third molars [6,7].
The debate on the appropriateness of preventive extraction of impacted third molars has also been addressed in Celikoglu's 2010 [8]. While some impacted third molars remain asymptomatic, many can cause pathologies such as pain, recurrent infections, cystic or tumoral degeneration, and, in rare cases, mandibular fracture. The mispositioning of anterior teeth following the eruption or incomplete eruption of third molars is also a debated issue. Additionally, impacted third molars frequently contribute to caries and pathological root resorptions in the seventh molar [9,10].
2. Materials and Methods
The study protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO; http://www.crd.york.ac.uk/PROSPERO; registration number: CRD42024536337). This meta-analysis searched only English databases, and the relevant literature published in the PubMed, Web of Science, Embase and Cochrane Library databases was independently searched from inception to 30 January 2024 by two investigators (GM, SK). The review question was designed according to the PICO (Population or Problem, Intervention or Exposure, Comparison, Outcome) element. We used the following search string, and we consulted narrative texts (Chiapasco et al. 2013 [11], Illustrated Manual of Oral Surgery):
(((extraction impacted lower third molar) OR (periodontal defect distal second molar)) OR (alveolar bone defect)) NOT case report NOT (regeneration)) NOT furcation NOT (fibula) NOT implant NOT PRF NOT PRP NOT treatment NOT DRUGS Filters: Humans, English, Adult: 19+ years 2.2)
Search Strategies: A review of the scientific literature was conducted.
2.1. Study Selection:
The research was conducted using the Medline and PUBMED databases, and narrative texts (Chiapasco et al. 2013 [11], Illustrated Manual of Oral Surgery) were consulted. The following keywords were used:
"extraction impacted lower third molar,"
"periodontal defect distal second molar,"
"alveolar bone defect."
The keywords and Boolean operators used to construct the search strings are as follows:
(((extraction impacted lower third molar) OR (periodontal defect distal second molar)) OR (alveolar bone defect)) NOT (case report) NOT (regeneration)) NOT (furcation) NOT (fibula) NOT (implant) NOT (PRF) NOT (PRP) NOT (treatment) NOT (DRUGS) Filters: Humans, English, Adult: 19+ years
The initial search returned a total of 2943 results. Abstracts and titles obtained were screened independently by two of the authors, who subsequently met and discussed disagreements on citation inclusion.
2.2. Inclusion Criteria
Adult patients (aged >19 years)
Population: Human sex
Intervention: extraction of impacted third molars
Study characteristics: Literature published from 2000 to 2024;
2.3. Exclusion Criteria
Articles written in languages other than English
All case reports were excluded due to insufficient scientific evidence, as were studies related to periodontal regenerative techniques using autologous bone or synthetic bone substitutes, both on natural teeth and on implants affected by peri-implantitis.
Among the 2943 articles, 92 met the initial inclusion criteria according to both authors; thus, they were obtained and reviewed in detail by the same two authors, who met and discussed disagreements on article inclusion.
After reading the titles, studies off-topic related to periodontology, cranial anomalies, or three-dimensional studies of alveolar bone were excluded. Thus, 12 studies were obtained; after the entire abstract was read, 5 additional studies were excluded for the following reasons: multiple presentations, orthodontic studies, and radiological studies on CBCT.
Of the 7 selected studies, 2 concerned the surgical technique of coronectomy [12,13]. Therefore, a meta-analysis was performed on 5 studies [14,15,16,17,18,19]. During the reading of the scientific articles, one study was removed due to a lack of data on the position of the third molar, 1 study was added to the meta-analysis because it was mentioned by Goksel et al. 2011 [17] in a table, and the reported data were particularly interesting for our evaluation.
A further manual check was performed on the references included in the articles, and no additional studies were identified that met the inclusion criteria through a review of references and a concurrent PubMed search. The final number of articles included in the present review was identified, and the main information was extracted and summarized.
2.4. Statistical Analysis
We performed a proportional meta-analysis using MedCalc 14.8.1 software (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org; 2014) and applied the Freedman–Tukey transformation (square root arc-sine transformation) to calculate the weighted overall proportion (DerSimonian and Laird, 1986).
The proportions (expressed as percentages) with 95% confidence intervals (CIs) of the symptoms identified by each study were included in the meta-analysis.
The overall proportion with 95% CI was calculated using both the random effects model and the fixed effects model.
The fixed-effects model assumes that all included studies have a similar effect, so the summary effect is an estimate of the weight of similar effects in the studies.
The random-effects model assumes that effects vary among studies, and the summary analysis is a weighted average reported in different studies.
The forest plot is a graphical representation in which, for each study included in the meta-analysis, values related to the effect size and confidence interval are presented.
The forest plot also included the weighted effect size of pathological change for each angular position of the third molar, with a 95% CI.
The size of the marker (square) represents the weight of each study; studies with a smaller patient sample will have less weight.
The overall effect is represented in the plot by a diamond: its width represents precision, and its position represents the estimate of effects.
Heterogeneity among studies based on various angles was estimated using Cochran's Q statistic test and the I2 index. Heterogeneity was considered significant when P-was <0.01 for the Q statistic (to assess whether the observed variance exceeded the expected variance).
To interpret the I2 index of heterogeneity (I2=100% × (Q-df)/Q), I2=0-25%, homogeneous; I2=25-50%, moderate heterogeneity; I2= 50-75%, large heterogeneity; and I2=75-100%, extreme heterogeneity.
3. Results
In total, 2943 studies were identified in the database by two researchers independently following predefined search strategies and data collection methods. No additional studies were found in the gray literature search. After removing 2 duplicate studies, 2849 irrelevant studies were excluded based on title, letter and review, and 94 studies were assessed for the primary screening. After the abstracts and full texts were read, 84 studies were further excluded because they did not meet the inclusion criteria. Finally, 10 studies were deemed eligible for this meta-analysis; 6 of these studies were included in the review, and 4 studies were included in the proportional meta-analysis. The flow diagram of the literature search is shown in Figure 1.
Table 1 shows the detailed characteristics of the eligible studies.
Six studies involving 2163 patients and 610 patients with pathological alterations and angular tooth positions were assessed for the proportional meta-analysis.
The majority of patients were female (1246; 56.1%). Two studies did not specify the exact number of patients with pathological alterations. Among the studies reporting pathological alterations, 708 affected teeth were identified to have pathological changes, representing 17.7% (124 teeth) (Table 2).
The relationship between pathological changes and angular tooth position was analyzed, and proportions for each angular position were calculated from individual studies. The results of the proportional meta-analysis, including the combined proportion (95% CI), are summarized in Table 3, with estimates of the overall proportion shown in the Forest Plot (Figure 2). The overall proportion of patients in the mesioangular position was 21.4% (7.0-40.9), demonstrating significant and extreme heterogeneity (Q=33.4, I2=91.0%, p<0.001). For horizontally positioned teeth, the overall proportion was 41.1% (20.8-63.0), indicating significant and extensive heterogeneity (Q=11.4, df=3, I2=73.8%, p=0.009). There was an overall proportion of vertically positioned teeth of 20.7% (3.4-47.4), with significant and extreme heterogeneity (Q=42.2, df=3, I2=92.9%, p<0.001), while there was an overall proportion of disto-angular teeth of 9.7% (3.6-18.4), classified as not significant or homogeneous (Q=0.5, df=1, I2= 0.0%, p=0.447).
4. Discussion
Our study identified six relevant articles in accordance with PRISMA Statement guidelines [20]. Rayalat et al. 2018 [18] investigated the optimal age for extracting impacted third molars, highlighting the challenge of deciding on asymptomatic extractions. They analyzed 4600 orthopantomographs from the University of Jordan and revealed age-related changes in third molar inclination and impaction patterns. After exclusions, the sample consisted of 1810 molars, 1224 of which were impacted bilaterally and 586 of which were impacted unilaterally. Examiners reevaluated the orthopantomographs by measuring various parameters via the William Sciller method. The study showed that the inclination angle of the third molar changes with age, impacting the Pell and Gregory impaction patterns. The study suggested reevaluating X-rays in younger patients to consider changes in inclusion severity.
Baykul et al. 2005 [14] examined cystic changes in dental follicles and reported a significant association between cystic lesions and vertically impacted molars. Among the 117 selected patients, 94 were included in the study. Cystic changes were most frequent between 20 and 25 years of age, with a preference for males. The association between cystic lesions and vertical inclusion was statistically significant.
Celikoglu et al. (2010) [16] studied the frequency of agenesis, impaction, positional angle, and pathological changes in 368 orthodontic patients aged >20-26 years. Agenesis of the third molars was found in 17.3% of the patients. Pathological changes, including root resorption of the second molar and a reduction in the alveolar bone height, occurred in 10.4% of the third molars. A greater frequency of pathological changes was observed in horizontally positioned molars.
Goksel et al. 2011 [17] focused on dental follicle analysis and its cystic or inflammatory degeneration. Fifty selected patients were asymptomatic or had asymptomatic, included, or semi-included lower third molars. Radiographic evaluation of dental follicles is insufficient, and even asymptomatic third molars can cause pathological degeneration.
In summary, these studies provide insights into age-related changes in the inclusion patterns of third molars, the associations between inclusion types and cystic changes, and the potential for pathological degeneration in asymptomatic patients. This research highlights the importance of considering individual patient characteristics in decision-making regarding third molar extraction.
Our research focused on retrieving data from the literature using the keywords "extraction impacted third molar," "periodontal defect distal second molar," and "alveolar bone defect." Upon analyzing the selected studies, Baykul et al. 2005 [14] considered the presence of contact between the eighth and seventh teeth. Celikoglu et al. (2010) [16] reported conditions classified as pathological, including the height of the alveolar bone distal to the seventh tooth. Although the Goksel et al. 2011 [17] study did not include periodontal surveys of the seventh adjacent tooth, it was asserted, as a general finding, that greater inclusion depth correlated with a greater degree of tissue inflammation.
Yamaoka et al. 1997 [21]: This study highlighted the risk of inflammation in completely impacted third molars, emphasizing the need for careful monitoring.
Simşek-Kaya et al. 2011 [22]: Symptomatically impacted lower third molars could still be associated with significant soft tissue pathologies, such as cysts and tumors.
Yildirim et al. 2008 [23]: Symptomatically impacted third molars often exhibit associated pathological changes, advocating for regular imaging and possible prophylactic removal to prevent complications.
These studies collectively underscore the potential risks associated with impacted third molars, even in the absence of symptoms, and support the importance of regular dental assessments and imaging.
According to several authors, such as Chiapasco et al. 2013 and Kugelberg et al. 1985 [11,24], the close association between pericoronitis and impacted third molars (95%) appears to be due to the anatomical characteristics of the lower eights, such as the absence of keratinized gingiva on the distal wall of the tooth. This absence facilitates bacterial colonization of the sulcus and may lead to the formation of a deep pocket.
Saravana & Subhashraj et al. 2008 [25]: This study highlighted the occurrence of cystic changes in the dental follicles of radiographically normal impacted third molars, suggesting the importance of thorough clinical evaluation.
Adelsperger et al. (2000) [26] reported that early soft tissue pathologies can occur around impacted third molars without radiographic signs, emphasizing the need for careful clinical assessment.
Kan et al. (2002) [27] identified long-lasting periodontal defects distal to the second molar following third molar extraction, indicating the necessity for extended periodontal monitoring and care postextraction.
These studies collectively stress the importance of comprehensive clinical evaluations, even in the absence of radiographic abnormalities, and highlight the need for ongoing periodontal care following third molar extractions.
Many studies do not specify the level of alveolar bone in the distal site of the second molar adjacent to the impacted tooth, and routine radiological measurements of bone loss are not commonly performed before extraction surgery. Our statistical analysis of the collected data indicated that there was a greater percentage of pathological degeneration in horizontally impacted third molars (41%) than in vertically (21.4%), mesioangular (20.7%), or distoangular (9.7%) third molars. This pathological transformation would likely result in increased radiographic coronal translucency adjacent to the third molar, leading to increased loss of alveolar bone adjacent to the seventh tooth.
All the analyzed studies agree that the frequency of cystic degeneration and subsequent bone loss distal to the second molar occurs more frequently than has been reported in numerous epidemiological studies. This change is especially notable with increasing patient age, with most of these changes seemingly initiating between the ages of 20 and 25.
Therefore, it would be useful to investigate, through histological analysis, all follicles exhibiting an increase in radiographic width greater than 2.5 mm (accounting for the magnification factor of radiographic examination) after tooth removal. Additionally, we recommend closely monitoring all impacted third molars, even when they are asymptomatic or exhibit a reduced follicle according to radiographic examination. Our study has several limitations. The main concern was the significant heterogeneity. A statistical analysis revealed a greater incidence of pathological degeneration in horizontally impacted third molars (41%) than in vertically impacted third molars (20.9%), mesioangular third molars (21.4%), or distoangular third molars (9.7%). This transformation likely leads to increased radiographic translucency and subsequent alveolar bone loss adjacent to the second molar.
All the studies agree that cystic degeneration and bone loss distal to the second molar occur more frequently than previously reported, particularly in older age groups (20-25 years). Histological analysis of follicles with increased radiographic width postextraction is recommended, as is close monitoring of impacted third molars, even in asymptomatic patients or those with reduced follicles on radiographic examination.
5. Conclusions
Based on the research findings and analysis of the literature regarding impacted third molars and their impact on adjacent structures, the following conclusions can be drawn: Association with Periodontal Defects: studies such as those by Baykul et al. 2005 [14], Celikoglu et al. 2010 [16], and Goksel et al. 2011 [17] indicate various aspects of periodontal defects associated with impacted third molars. These defects include the presence of contact between adjacent teeth, pathological conditions affecting the alveolar bone, and the correlation between inclusion depth and tissue inflammation. Pericoronitis and Anatomical Characteristics: Authors such as Chiapasco et al. 2013 [11] and Kugelberg et al. 1985 [24] emphasize the close relationship between pericoronitis and impacted third molars, attributing it to anatomical factors such as the absence of keratinized gingiva, which facilitates bacterial colonization and pocket formation. Pathologic Degeneration: Statistical analysis revealed a greater percentage of pathological degeneration in horizontally impacted third molars than in other positions. This degeneration leads to increased radiographic translucency and subsequent loss of alveolar bone adjacent to the second molar. Cystic Degeneration and Bone Loss: All the analyzed studies agree that cystic degeneration and bone loss distal to the second molar occur more frequently than previously reported, especially with increasing patient age. Recommendations for Further Investigation: Histological analysis of follicles exhibiting an increase in radiographic width after tooth removal is recommended, as is close monitoring of impacted third molars, even when asymptomatic or when the follicle size is reduced on radiographic examination. In summary, this research highlights the significant impact of impacted third molars on adjacent structures, emphasizing the importance of thorough evaluation, monitoring, and consideration of various factors in treatment planning and management. In conclusion, the present research revealed significant periodontal defects, increased risk of pericoronitis due to anatomical factors, and increased pathological and cystic degeneration in patients with impacted third molars. Further investigations and close monitoring are recommended for comprehensive treatment planning and management.
Funding
The authors declare that no funds, grants, or other support was received during the preparation of this manuscript.
Ethical Approval
Not applicable.
Informed Consent
Not applicable.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Renton, T., & Al-Haboubi, M. (2012). What has been the United Kingdom's experience with retention of third molars? Journal of Oral and Maxillofacial Surgery, 70(9), S48-S57. [CrossRef]
- Liversedge, R. L. (2000). The removal of wisdom teeth: NICE guidelines. British Journal of Oral and Maxillofacial Surgery, 38(4), 350-353. [CrossRef]
- Berge, T. I. (1996). Complications associated with removal of impacted third molars: a prospective study of 4338 cases. Acta Odontologica Scandinavica, 54(5), 281-286. [CrossRef]
- Fernandes MJ, Ogden GR, Pitts NB, Ogston SA, Ruta DA.”Actuarial life-table analysis of lower impacted wisdom teeth in general dental practice.” Community Dent Oral Epidemiol. 2010 Feb;38(1):58-67. [CrossRef]
- National Institute for Health and Care Excellence. (2000). Guidance on the Extraction of Wisdom Teeth. Available from: https://www.nice.org.uk/guidance/ta1.
- Shepherd, J. P., & Brickley, M. (1994). Surgical removal of third molars. BMJ, 309(6955), 620-621. [CrossRef]
- Song, F., O'Meara, S., Wilson, P., Golder, S., Kleijnen, J. (2000). The effectiveness and cost-effectiveness of prophylactic removal of wisdom teeth. Health Technology Assessment, 4(15). Available from: https://www.journalslibrary.nihr.ac.uk/hta/hta4150.
- Celikoglu M, Miloglu O, Kazanci F.” Frequency of agenesis, impaction, angulation, and related pathologic changes of third molar teeth in orthodontic patients.” J Oral MaxillofacSurg. 2010 May;68(5):990-5. [CrossRef]
- McArdle, L. W., & Renton, T. F. (2012). The effects of NICE guidelines on the management of third molar teeth. British Dental Journal, 213(5), 231-236. [CrossRef]
- American Association of Oral and Maxillofacial Surgeons (AAOMS). (2016). Management of Third Molar Teeth. White Paper on Third Molar Data. Available from: https://www.aaoms.org.
- Chiapasco Matteo, Manuale Illustrato di Chirurgia Orale, Edra Masson terza edizione 2013.
- Pitros P, Jackson I, O'Connor N. ”Coronectomy: a retrospective outcome study.” Oral Maxillofac Surg. 2019 Dec;23(4):453-458. [CrossRef]
- Vignudelli E, Monaco G, Antonella Gatto MR, Costi T, Marchetti C, Corinaldesi G. ”Stability of Periodontal Healing Distal to the Mandibular Second Molar After Third Molar Coronectomy: A 3-Year Follow-Up Study.” J Oral Maxillofac Surg. 2019 Feb;77(2):254-261. [CrossRef]
- Baykul, T., Saglam, A. A., Aydin, U., & Basak, K. (2005). Incidence of cystic changes in radiologically normal impacted lower third molar follicles. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, 99(5), 542-545. [CrossRef]
- Yildirim, D., Gider, Y., Ozer, I., & Ozan, B. (2007). Pathologic changes in soft tissues associated with asymptomatic impacted third molars. Oral Surgery, Oral Medicine, Oral Pathology, Oral Radiology, and Endodontology, 103(1), 36-42. [CrossRef]
- Celikoglu, M., Miloglu, O., & Kazanci, F. (2010). Frequency of agenesis, impaction, angular positions, and related pathologic changes of third molar teeth in orthodontic patients. Journal of Oral and Maxillofacial Surgery, 68(5), 990-995. [CrossRef]
- Göksel, S., Salcıoğlu, Z., & Saruhan, N. (2011). The prevalence of pathologies related to impacted third molars among Turkish patients. International Journal of Oral and Maxillofacial Surgery, 40(10), 1245-1250. [CrossRef]
- Ryalat, S., Alawneh, T. N., & Hassona, Y. (2018). Impaction of lower third molars and their association with age: radiological perspectives. BMC Oral Health, 18(1), 58. [CrossRef]
- Naraya, A. S., Sharma, S., & Kumar, P. (2023). Evaluation of the incidence of complications related to impacted third molars: A cross-sectional study. Journal of Clinical and Diagnostic Research, 17(3), ZC12-ZC16. [CrossRef]
- Alberto Enrico Maraolo,” Una bussola per le revisioni sistematiche: la versione italiana della nuova edizione del PRISMA statement “, Unità Operativa Complessa di Malattie Infettive a Indirizzo Neurologico – AORN dei Colli, Ospedale Cotugno – Napoli, Medici Oggi, Anno XXV, anno 2021.
- Yamaoka, DDS, PhD* Akihiro Tambo, DDS† Kiyofumi Furusawa, DDS, “Incidence of inflammation in completely impacted lower third molars.” Minoru PhDAustralian Dental Journal 1997;42:(3):153-5.
- Simşek-Kaya G, Özbek E, Kalkan Y, Yapici G, Dayi E, Demirci T.”Soft tissue pathosis associated with asymptomatic impacted lower third molars.” Med Oral Patol Oral Cir Bucal. 2011 Nov 1;16(7):e929-36. [CrossRef]
- Gülsün Yildirim 1, Hanife Ataoğlu, Ahmet Mihmanli, Dilek Kiziloğlu, Mustafa Cihat Avunduk,”Pathologic changes in soft tissues associated with asymptomatic impacted third molars”Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008 Jul;106(1):14-8. [CrossRef]
- Kugelberg Carl F., Ulf Ahlstr JM, Sune E. and Anders H.,“Periodontal healing after impacted lower third molar surgery. A retrospective study” Departments of Oral Surgery, Dental Radiology and Periodontology, the Institute for Postgraduate Dental Education, Jdnkoping, Sweden, Int. J. Oral Surg. 1985: 14: 29-40.
- Saravana a,∗, Krishnaraj Subhashraj b a, ”Cystic changes in dental follicle associated with radiographically normal impacted mandibular third molar G.H.L. “Department of Oral and Maxillofacial Surgery, KGF College of Dental Science, Karnataka, India b Department of Oral and Maxillofacial Surgery, Jawaharlal Institute of Postgraduate Medical Education and Research, Pondicherry, India Accepted 11 February 2008.
- John Adelsperger, DDS,a John H. Campbell, DDS, MS,b David B. Coates, DDS,c Don-John Summerlin, DMD, MS,d and Charles E. Tomich, DDS, MSD,”Early soft tissue pathosis associated with impacted third molars without pericoronal radiolucency “, Indianapolis, Ind INDIANA UNIVERSITY, Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2000;89:402-6.
- Kan KW, Liu JKS, Lo ECM, Corbet EF, Leung WK, Residual periodontal defects distal to the mandibular second molar 6–36months after impacted third molar extraction. A retrospective cross-sectional study of young adults. J Clin Periodontol 2002; 29: 1004–1011. CBlackwell Munksgaard, 2002.
Figure 1.
Workflow diagram depicting the systematic selection of studies for inclusion in the meta-analysis.
Figure 1.
Workflow diagram depicting the systematic selection of studies for inclusion in the meta-analysis.
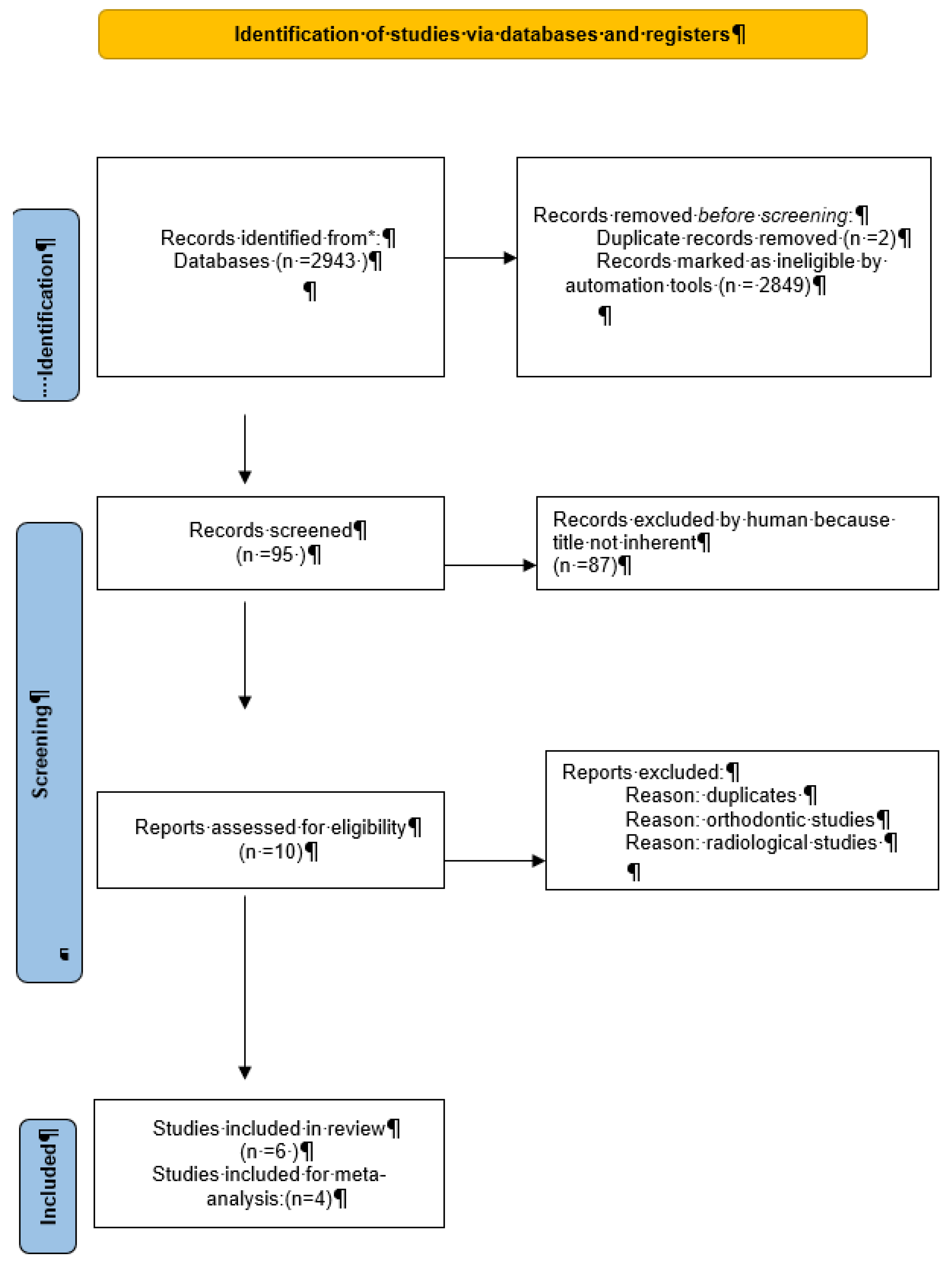
Figure 2.
Proportional meta-analysis of included studies with various frequent pathological changes in the angular position of teeth (A (mesioangular), B (horizontal), C (vertical), and D (distoangular)). Aggregate percentage of patients with different frequent causes of symptoms. Markers represent grouped effects. The position of the diamond represents the estimated effect size, and the width of the diamond reflects the precision of the estimate. Output generated by MedCalc software.
Figure 2.
Proportional meta-analysis of included studies with various frequent pathological changes in the angular position of teeth (A (mesioangular), B (horizontal), C (vertical), and D (distoangular)). Aggregate percentage of patients with different frequent causes of symptoms. Markers represent grouped effects. The position of the diamond represents the estimated effect size, and the width of the diamond reflects the precision of the estimate. Output generated by MedCalc software.
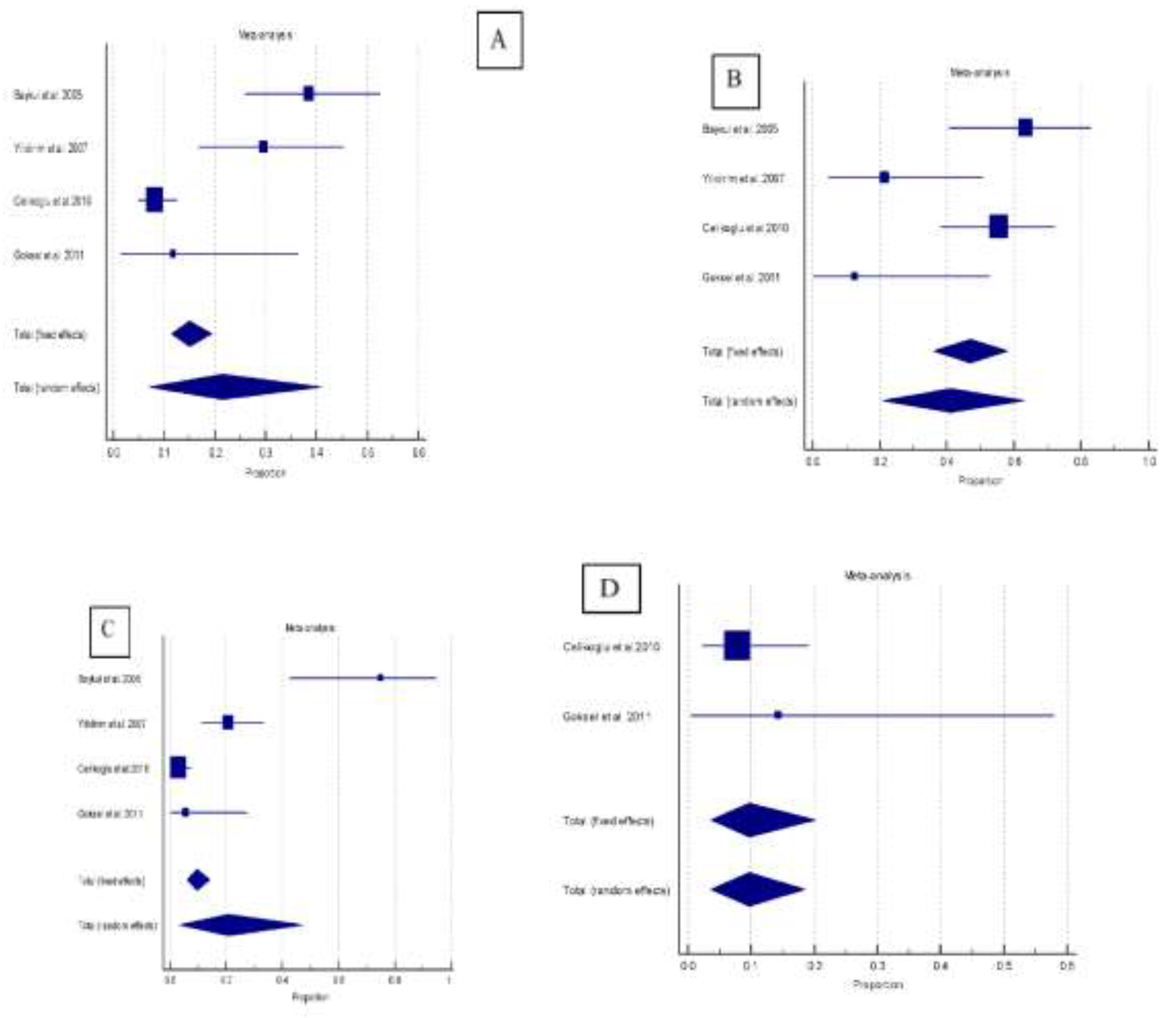

Table 1.
Characteristics of included studies.
| Study | Pts | Third molars | Age, mean | Male | Female |
|---|---|---|---|---|---|
| Baykul et al. 2005 | 94 | 94 | 21,1 | 30 | 64 |
| Yilidirim et al. 2007 | 115 | 120 | 24,74 | 38 | 77 |
| Celikoglu et al.2010 | 351 | 444 | 22,8 | 153 | 198 |
| Goksel et al. 2011 | 50 | 50 | 21,0 | 22 | 28 |
| Ryalat et al. 2018 | 1198 | 1810 | 566 | 632 | |
| Naraya et al. 2023 | 355 | 414 | 22,4 | 167 | 247 |
Table 2.
Distribution of angular position of teeth in selected studies and pathological alterations.
Table 2.
Distribution of angular position of teeth in selected studies and pathological alterations.
| Study | Third molars | Mesioangular | Horizontal | Vertical | Distoangular |
|---|---|---|---|---|---|
| Baykul et al. 2005 | 94 | 57 (60.6) | 22 (23.4) | 12 (12.8) | 3 (3.2) |
| Yilidirim et al. 2007 | 120 | 44 (36.7) | 14 (11.7) | 58 (48.3) | 4 (3.3) |
| Celikoglu et al.2010 | 444 | 222 (50.0) | 36 (8.1) | 135 (30.4) | 51 (11.5) |
| Goksel et al. 2011 | 50 | 17 (34.0) | 8 (16.0) | 18 (36.0) | 7 (14.0) |
| Ryalat et al. 2018 | 1810 | 1196 (66.1) | 273 (15.1) | 340 (18.8) | |
| Naraya et al. 2023 | 414 | 344 (83.1) | 126 30.4) | 249 (60.1) 39 (9.4) | |
| Pathologic changes | |||||
| Baykul et al. 2005 | 94 | 22 (38.6) | 14 (63.6) | 9 (75.0) | |
| Yilidirim et al. 2007 | 120 | 13 (29.5) | 3 (21.4) | 12 (20.7) | |
| Celikoglu et al.2010 | 444 | 18 (8.1) | 20 (55.6) | 4 (3.0) | 4 (7.8) |
| Goksel et al. 2011 | 50 | 2 (11.8) | 1 (12.5) | 1 (5.6) | 1 (14.3) |
Table 3.
Meta-analysis of the aggregated proportion of included studies with various frequent pathological changes in the angular position of teeth.
Table 3.
Meta-analysis of the aggregated proportion of included studies with various frequent pathological changes in the angular position of teeth.
| Sample size | n. event | Proportion (%) | 95% CI | |
|---|---|---|---|---|
| Pathologic changes | ||||
| Mesioangular | 340 | 55 | 21.4 | 7.0 to 40.9 |
| Horizontal | 80 | 38 | 41.1 | 20.9 to 63.0 |
| Vertical | 223 | 26 | 20.7 | 3.4 to 47.4 |
| Distoangular | 58 | 5 | 9.7 | 3.6 to 18.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



