
Submitted:
19 November 2024
Posted:
21 November 2024
You are already at the latest version
Abstract
Background:
Hyperkalemia is a common electrolyte disorder in patients with heart failure and reduced ejection fraction (HFrEF). Renin-angiotensin-aldosterone system inhibitors (RAASi) have been shown to improve survival and decrease hospitalization rates, although they may increase the serum potassium levels. Hyperkalemia has significant clinical and economic implications, and is associated with increased healthcare resource utilization. The main objective of this study was to analyze the management of hyperkalemia and the associated medical costs in a cohort of patients with HFrEF.
Methods:
An observational, longitudinal, retrospective, single-center retrospective study was made in patients with HFrEF who started follow-up in a specialized heart failure unit between 2010 and 2021.
Results:
The study population consisted of 1181 patients followed-up on for 64.6 ± 38.8 months. During follow-up, 11,059 control visits were conducted, documenting 438 episodes of hyperkalemia in 262 patients (22.2%).
Of the hyperkalemia episodes, 3.0% required assistance in the Emergency Department, 1.4% required hospitalization, and only 0.2% required admission to the Intensive Care Unit. No episode required renal replacement therapy. Reduction or withdrawal of RAASi was necessary in 69.9% of the hyperkalemia episodes. The total cost of the 438 hyperkalemia episodes was €89,178.82; the expense during the first year accounted for 48.8% of the total cost.
Conclusions:
Hyperkalemia is common in patients with HFrEF. It is often accompanied by a modification of treatment with RAASi. Hyperkalemia generates substantial costs in terms of healthcare resources and medical care, especially during the first year.
Keywords:
hyperkalemia
; costs
; economic impact
; heart failure
; reduced ejection fraction
1. INTRODUCTION
Hyperkalemia is a common electrolyte disorder in patients with heart failure and reduced ejection fraction (HFrEF)[1]. It is defined as an increase in plasma potassium concentration to > 5.0 mEq/l, although the clinical guides consider cut-off points of up to 5.5 mEq/l to be acceptable and safe, with no need to modify neurohormonal treatment [2]. Higher plasma potassium values, especially > 6 mEq/l, are associated with alterations in cell action potential and cardiac conduction and excitability [3], which can result in increased arrhythmias and mortality [4,5].
Although the results of the different studies are very heterogeneous, the prevalence of hyperkalemia is estimated to be about 3% in the general population [6]. These figures can reach 20% in patients with chronic heart failure [7], mainly because of the concomitant presence of comorbidities such as chronic kidney disease and diabetes mellitus, as well as neurohormonal treatment [8,9].
In patients with HFrEF, the use of renin-angiotensin-aldosterone system inhibitors (RAASi), which include the combination of neprilysin and angiotensin II receptor inhibitors (ARNi), angiotensin converting enzyme inhibitors (ACEi) or angiotensin II receptors inhibitors (ARBi), together with mineralocorticoid receptor antagonists (MRAs), at the maximum tolerated doses, has been shown to improve survival and reduce the hospital admission rates (2,10,11). However, these drugs also contribute to increase the serum potassium levels through different mechanisms of action [12], thus limiting their use or resulting in a decrease in dose or even suspension of treatment - with the consequent loss of prognostic benefit [13,14]. In a recent study, the presence of hyperkalemia prevented the reaching of target doses in up to 9.3% of the patients jointly treated with ACEi / ARBs and MRAs and was moreover responsible for 8.9% of the contraindications or intolerances to some of these drugs [1].
The prevention and treatment of hyperkalemia requires a multidisciplinary approach. In the case of life-threatening hyperkalemia, the main aim is to avoid fatal arrhythmias by adopting measures that allow stabilization of the myocardial cell membrane, the transport of extracellular potassium into the cells, and elimination of the cation from the body as quickly as possible. If these measures do not prove effective, hemodialysis may be required in some cases. In the rest of patients, the initial measures consist of a low-potassium diet, the withdrawal of potassium supplements and nephrotoxic drugs, and the start or titration of loop or thiazide diuretics. The prolonged use of binding agents such as ion exchange resins is not advised, due to the possible associated adverse effects and lack of safety and efficacy studies [15,16,17,18].
In many cases, the absence of adequate treatment alternatives for potassium control ultimately leads to the suspension or dose reduction of RAASi drugs, which can worsen the patient prognosis and increase mortality. According to the clinical guides, if short term suspension of these drugs is required, it should be minimized and the treatment should be carefully reintroduced as soon as possible, with close monitoring of the serum potassium levels [19]. The new potassium binding agents such as patiromer or sodium zirconium cyclosilicate constitute novel therapeutic options allowing the maintenance of RAASi drugs in those patients that need them despite the development of hyperkalemia [2]. The pivotal studies have demonstrated efficacy and safety in terms of the normalization of elevated potassium levels, the maintenance of normokalemia over time, and the prevention of recurrence of hyperkalemia in these patients. Such drugs therefore can be considered for the treatment of this disorder under certain circumstances [20,21,22].
Hyperkalemia is therefore associated to important clinical and economic consequences, with an increase in the use of healthcare resources: more visits to the emergency room or specialist care, an increase in hospital admissions, and a rise in mortality [23]. In this context, the need arises to know the management of hyperkalemia and its impact in terms of the use of RAASi drugs in real clinical practice, and to quantify the associated resources and costs in a cohort of patients with HFrEF.
The main objective of the present study was to analyze the management of hyperkalemia in a cohort of patients with HFrEF, and its clinical and economic impact. Evaluation was made of the modifications in RAASi treatment, the number of visits to the emergency room, hospitalizations, and the need for additional consultations correction of the electrolyte imbalance was achieved. In addition, the economic impact and medical costs associated with the management of hyperkalemia were examined.
3. MATERIAL AND METHODS
3.1. Study Design and Screening Criteria
An observational, longitudinal, retrospective, single-center retrospective study was made of consecutive patients starting follow-up in the Specialized Heart Failure Unit of the Department of Cardiology of a secondary hospital between January 2010 and December 2021.
The study included patients with HFrEF defined according to the criteria of the 2021 clinical practice guide of the European Society of Cardiology (ESC) [2]. All patients were Caucasian, over 18 years of age, and were referred from the Hospitalization Unit or other Cardiology clinics. None of them presented decompensated heart failure.
3.2. Intervention and Data Collection
The collection of data referred to demographic, clinical, laboratory test, electrocardiographic and echocardiographic parameters, as well as the information referred to treatment, hospital admissions, visits to the emergency room or successive controls by the specialist, was carried out by the cardiologists of the Unit, based on reviews of the electronic case histories of the patients. The study variables were entered in a statistical database previously designed for the purpose of the study.
Patient management abided with the heart failure guides applicable at the time of patient assessment in the clinic.
Hyperkalemia was defined as a serum potassium concentration of > 5.5 mEq/l. The plasma potassium levels were determined before each patient visit, with none being determined during hospital admission. Hyperkalemia was considered to be present at the first measurement meeting the diagnostic criterion.
The corresponding cost of consumables and laboratory materials was assigned to each laboratory test, along with the cost of the extraction visit and the cost of the telephone contact (to report the result to the patient and modify treatment, program another test, or confirm a follow-up visit).
All the patients presented an electrocardiogram (ECG) prior to consultation.
The follow-up starting date for this study was that of the first outpatient visit to our Heart Failure Unit.
The economic costs were calculated based on Spanish Royal Decree 56/2014, of 30 April [24], establishing the healthcare service rates for centers dependent upon the Galician Health Service and public healthcare foundations of Galicia.
3.3. Ethical Particulars
The study was carried out following the Good Clinical Practice (GCP) guidelines, ethical principles, and the Spanish legal specifications referred to research in force at the time of the study. Approval was obtained from the local Regional Research Ethics Committee (protocol code 2022/343; date of approval 21 September 2022) before starting the study.
3.4. Statistical Analysis
Quantitative variables were reported as the mean and standard deviation (SD), or median and interquartile range (IQR), and qualitative variables were reported as frequencies and percentages.
Quantification was made of the costs of the emergency room visits, stays in the hospital ward, admission to the Intensive Care Unit (ICU) and follow-up laboratory tests. The costs of the consumables and laboratory materials (€9.91), the cost of the extraction visit (€14.52), and the cost of the subsequent telephone contact (€34.52) were quantified. Table 2 shows the cost of each of these items according to Spanish Royal Decree 56/2014, of 30 April [24].
The SPSS version 19 statistical package (IBM, Armonk, NY, USA) was used throughout.
4. RESULTS
4.1. Baseline and Clinical Characteristics of the Study Sample
Of the patients followed-up on in our Heart Failure Unit, 1181 met the criteria for participation in this study. The mean patient age was 66.6 years, and 22.7% were females. Mean creatinine clearance (MDRD) was 72.0 ± 24.7 ml/min/1.73 m2, and 31.3% of the patients presented creatinine clearance (MDRD) < 60 ml/min/1.73 m2. The rest of the baseline characteristics of the study sample are shown in Table 1.
The mean duration of follow-up was 64.6 ± 38.8 months (median 56; IQR 30.5-97.5), during which a total of 11,059 control visits took place. These visits documented 438 hyperkalemia episodes in 262 patients (Figure 1, flow chart). Of these 262 patients, 163 (62.0%) presented a single episode, while 99 (38.0%) suffered more than one hyperkalemia episode.
The mean potassium concentration of the 438 hyperkalemia episodes was 5.76 ± 0.30 mEq/l.
4.2. Management of Hyperkalemia and Need for Medical Care
The pharmacological treatment was modified in 341 hyperkalemia episodes (77.9%), and one of the essential drug groups was reduced or suspended in 306 episodes (69.9%). In the 35 hyperkalemia episodes in which treatment was modified but without reducing the essential drug groups, the loop diuretic was modified in 16 episodes, potassium binders were added in 17, and the binder drug doses were increased on 2 occasions.
With regard to the essential drug groups, ACEi/ARBi or ARNi were withdrawn in 65 episodes (14.8% of the hyperkalemia episodes), and could be reintroduced in 48 cases, with a median of 11.5 days (IQR 6.0-50.3). In turn, the MRAs were withdrawn in 129 hyperkalemia episodes and could be reintroduced in only 31.5% of the cases, with a median of 111 days (IQR 11-1191). Resins or potassium binders were started in 10.6% of the hyperkalemia episodes.
Emergency room care in hospital was required in 13 episodes (3.0%). Of these cases, 6 (1.4%) required hospital ward admission and 1 required admission to the ICU. In no case was renal replacement therapy needed due to hyperkalemia. The mean stay in the hospital ward was 7.2 ± 3.2 days.
In the days after the visit on which hyperkalemia was detected, a total of 953 laboratory tests were performed on an ambulatory basis, followed by additional telephone contacts to monitor the evolution of the potassium levels.
4.3. Hyperkalemia Episodes During the First Year of Follow-Up
A total of 196 hyperkalemia episodes (44.7%) occurred during the first year (Figure 2). Of these episodes, 8 required emergency care (4.1%) and 3 (1.5%) required conventional hospital ward admission. No admissions to the ICU or use of renal replacement therapy proved necessary. Neurohormonal treatment was modified in 164 of the 196 hyperkalemia episodes (83.7%) during the first year of follow-up. In 22.0% of the cases ACEi/ARBi or ARNi were suspended, and in 48.8% of the cases MRAs were withdrawn. Resins or potassium binders were prescribed in 11.0% of the patients.
4.4. Resource Utilization and Associated Costs
An average of 4.21 ± 3.71 laboratory tests were made in the period between the visit prior to the hyperkalemia episode and the episode.
After determining the maximum hyperkalemia value, an average of 2.18 ± 1.30 subsequent laboratory tests were made until normokalemia was confirmed.
With regard to the costs, Table 2 shows that at the end of follow-up, the cost related to conventional hospital ward stay was €25,918.56, while the cost of ICU stay was €2284.95. The cost of care in the emergency room was €4700.65. The cost associated with the laboratory tests and posterior clinical monitoring totaled €56,274.65. Over an average follow-up of 64 months, the calculated total cost related to healthcare resource utilization and the clinical management of hyperkalemia was €89,178.83.
During the first year of follow-up, the total cost corresponding to the 196 recorded hyperkalemia episodes was €43,508.17, representing 48.8% of the hyperkalemia-related costs over 4.5 years of follow-up.
5. DISCUSSION
Our study has two main findings. On one hand, most of the costs derived from the hyperkalemia episodes in a cohort of patients with HFrEF are concentrated in the course of the first year. On the other hand, the main cost is associated with the laboratory tests and successive visits to monitor the evolution of plasma potassium and introduce the opportune treatment optimizations. The number of admissions to hospital is low.
In our study the incidence of hyperkalemia during follow-up of the patients with HFrEF was high (22.0%) and consistent with the data reported by other series [7,25]. As our group has previously reported [25], a relevant finding was that there is an increased incidence of hyperkalemia in the first year of follow-up, which could be explained by the fact that it is in the first months after patient referral to the Heart Failure Unit when the progressive titration of neurohormonal treatment with RAASi takes place. In our case, at one year of follow-up, 97.2% of the patients were under treatment with ACEi/ARBi/ARNi at higher doses than at the start; 67.3% were receiving MRAs at doses similar to those at the start; and a lesser proportion (55.2%) of subjects were treated with diuretics at lower doses than at the start. This initial increase in the incidence of hyperkalemia caused the costs of the disorder to be concentrated in the first year. In effect, 48.8% of the total cost corresponded to this period.
In addition, half of the visits to the emergency room and hospital ward admissions occurred during the first year of follow-up, which is precisely when the greatest percentage of hyperkalemia episodes was detected. These results contrast with those of other studies [26,27], where greater incidences of hospitalization, emergency room visits and hospital visits were recorded than in our series. However, it should be noted that these studies did not involve only patients with heart failure.
In the 11,059 visits during follow-up, we detected 438 hyperkalemia episodes in 262 patients, and of these, 40% experienced more than one episode over time. This observation is consistent with the data published by Thomsen et al. [28], who found the recurrence of hyperkalemia to be frequent in patients with heart failure, resulting in an increase in hospital admissions and thus of healthcare resource utilization.
In our sample, the mean potassium concentration was 5.76 ± 0.30 mEq/l. According to the expert opinions included in the KDIGO guides [29], and in the absence of electrocardiographic changes, this potassium level would be regarded as corresponding to mild hyperkalemia. The close monitoring of these patients after the optimization of RAASi treatment, with periodic laboratory tests (4.21 ± 3.71 on average), could explain the early detection of the hyperkalemia episodes. Likewise, the need for fewer subsequent laboratory tests (2.18 ± 1.30 on average) until normokalemia is confirmed could be justified.
In line with the above, the fact that most of the hyperkalemia episodes involved potassium levels of < 6 mEq/l, could explain why emergency room care was only required in 3.0% of the cases, with admission to the hospital ward in 1.4% and admission to the ICU in only 0.2%. In no case did renal replacement therapy prove necessary. This also explains why the main cost observed in our study was centered on the outpatient monitoring of potassium elevation, with frequent laboratory tests and telephone visits.
At present, the clinical practice guides (2,30,31) recommend different measures in application to patients with chronic hyperkalemia involving potassium levels > 5.5 mEq/l. These include a low-potassium diet, the withdrawal of potassium supplements and nephrotoxic drugs, or the start of non-potassium sparing diuretics. Furthermore, and given the prognostic benefits of RAASi in patients with HFrEF, those patients who develop hyperkalemia could also benefit from potassium-reducing drugs to introduce or increase neurohormonal treatment [2,32].
However, in the same way as previously described in other observational studies [1], the suspension or reduction of RAASi treatment is common practice in the control of hyperkalemia in patients with HFrEF - with the consequent impact in terms of morbidity and mortality. In our study, RAASi treatment was modified (drug reduction or withdrawal) in almost 70% of the hyperkalemia episodes. Specifically, ACEi/ARBi or ARNi were suspended in 65 episodes, and could be reintroduced relatively early during follow-up (after about 10 days) in 73.8% of the cases, once the potassium levels were controlled. In turn, the MRAs were withdrawn in 149 hyperkalemia episodes, but could only be reintroduced much later (after > 3 months) and in much lower proportion than with ACEi/ARBi or ARNi (in only 31.5% of the cases). Ion exchange resins or potassium binders were prescribed in only 10.6% of the cases. In the case of the ion exchange resins, this low percentage could be explained by the lack of scientific evidence of their efficacy and the possible adverse effects that might result from their prolonged use [33], and which limit their prescription. In the case of the potassium binders, both patiromer [34] and sodium zirconium cyclosilicate [35] have been postulated as new therapeutic alternatives. On one hand, these drugs would make it possible to maintain RAASi in those patients who need them despite hyperkalemia, and on the other hand they could protect these same patients against hyperkalemia recurrence, with a good efficacy, tolerability and safety profile even at long term - thus exerting a positive impact upon the clinical course of patients with HFrEF [36,37,38,39]. In effect, the current clinical practice guides [2] for the first time offer different recommendations to facilitate the management of hyperkalemia in patients with HFrEF combining potassium binders. However, the strict requirements for authorizing their use [40] complicate and largely limit their prescription, as reflected in our study.
As previously commented, hyperkalemia has important clinical consequences, with a very significant economic impact. In our study, the mean cost per assisted hyperkalemia episode at the end of follow-up was €203.60, with a total hyperkalemia episodes cost of €89,178.83. It is important to note that during the first year of follow-up, the total cost was €43,508.17, representing almost half of the total cost at the end of the 5 years of follow-up. In our series it was during the first year when RAASi drug titration took place, with a low prescription of concomitant potassium binders, and thus with the largest observed number of hyperkalemia episodes. As a result, it seems logical for this to be the time when most laboratory tests were made and more visits to the emergency room or hospital admissions took place, giving rise to increased healthcare expenditure. Mention also should be made of the important cost of the laboratory test controls and posterior monitoring at the end of follow-up (€56,274.65) in our series, as previously mentioned. Perhaps the close monitoring of these patients, with periodic laboratory tests, allows for the early detection of hyperkalemia episodes that are largely mild, with early treatment modifications, avoiding subsequent emergency care and hospital admissions, and with clear minimization of the costs at this level. Few studies have addressed the economic impact of chronic hyperkalemia, particularly in a cohort of patients with HFrEF [27,41]. However, as in our case, the existing studies all highlight the important added costs involved, due not only to the direct complications of hyperkalemia but also to the modification in neurohormonal treatment, which is associated with an increased number of cardiovascular events, progression of cardiorenal disease, and increased mortality [42]. Based on the above, the healthcare cost generated by the management of hyperkalemia in patients with HFrEF appears to clearly exceed the cost derived from the new potassium binders, as is reflected in the current clinical practice guides [2].
6. CONCLUSIONS
Hyperkalemia is a common finding in patients with HFrEF. It is usually accompanied by a modification in RAASi treatment, which results in a loss of prognostic benefit for the patients. The new potassium binding agents such as patiromer or sodium zirconium cyclosilicate constitute therapeutic options allowing the maintenance of neurohormonal treatment despite the presence of hyperkalemia, though their use is still largely limited due to the strict authorization conditions applied in Spain. Furthermore, hyperkalemia episodes generate substantial costs in terms of healthcare resources and medical care, particularly during the first year. Close clinical monitoring, with periodic laboratory tests, as well as the sustained and early use of the new binding agents, would allow for the early detection of hyperkalemia episodes and the introduction of timely modifications capable of improving the patient prognosis and reducing healthcare costs.
7. STUDY LIMITATIONS
Our study has limitations. Firstly, this is a retrospective observational study, with the inherent limitations this implies. In addition, the definition of hyperkalemia differs from that used in the clinical practice guides and in most previous studies (potassium > 5 mEq/l)[2]. Nevertheless, as mentioned previously, a potassium concentration of up to 5.5 mEq/l represents the cut-off level up to which neurohormonal treatment can be maintained without requiring modification. Mention also must be made of the low percentage of patients in our cohort treated with sodium-glucose cotransporter 2 inhibitors (SGLT2i), since their use was not indicated in the clinical practice guides in force at the start of the study [19]. Furthermore, the study was designed to determine the management and costs of hyperkalemia, but we did not contemplate the costs derived from progression of the disorder or mortality derived from the modification of neurohormonal treatment. Lastly, it should be noted that the economic cost was estimated for the Galician Health Service (Spain), and cannot be generalized to other Spanish or European health systems.
Despite this, the characterization and long follow-up period of our cohort of patients with HFrEF is one of the strong points of the study. In addition, an extensive evaluation has been made of the economic impact of hyperkalemia in patients with HFrEF, considering different clinical parameters (hospital stay, emergency care visits, the use of drugs and the cost associated to each of them).
Author Contributions
Individual contributions: A.L.-L. developed the conceptualization, methodology, investigation and writing—original draft preparation. M.R.-A performed data collection and collaborated with in-depth investigation. E.P.-G. performed the formal analysis as well as the writing—review and editing. C.A.-J.-C., J.M.V.-F, J.E.-T. and J.A.-R. performed data collection and collaborated with in-depth investigation. R.F.-G. performed the formal analysis as well as the writing—review and editing. R.R.-V. performed data collection and collaborated with in-depth investigation. C.G.-J. developed the visualization, writing—original draft preparation, supervision and validation of the research article. All authors have read and agreed to the published version of the manuscript.
Funding
This research received a grant of ASTRA-ZENECA (ESR-20-20731).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by Ethics Committee of Santiago-Lugo (protocol code 2022/343 and date of approval 21 September 2022).
Informed Consent Statement
Patient consent was waived due to the study being conducted under additional provision 17 of Organic Law 3/2018 of 5 December on the Protection of Personal Data and the guarantee of digital rights in Spain.
Data Availability Statement
Data will be available after reasonable request to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Crespo-Leiro MG, Barge-Caballero E, Segovia-Cubero J, González-Costello J, López-Fernández S, García-Pinilla JM, et al. Hyperkalemia in heart failure patients in Spain and its impact on guidelines and recommendations: ESC-EORP-HFA Heart Failure Long-Term Registry. Revista Española de Cardiología (English Edition) 2020, 73, 313–323. [Google Scholar] [CrossRef] [PubMed]
- McDonagh TA, Metra M, Adamo M, Gardner RS, Baumbach A, Böhm M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef] [PubMed]
- Fisch C, Knoebel SB, Feigenbaum H, Greenspan K. Potassium and the monophasic action potential, electrocardiogram, conduction and arrhythmias. Prog Cardiovasc Dis 1966, 8, 387–418. [Google Scholar] [CrossRef] [PubMed]
- Gorriz JL, D’Marco L, Pastor-González A, Molina P, Gonzalez-Rico M, Puchades MJ, et al. Long-term mortality and trajectory of potassium measurements following an episode of acute severe hyperkalaemia. Nephrology Dialysis Transplantation 2022, 37, 522–530. [Google Scholar] [CrossRef] [PubMed]
- Ingelfinger, JR. A New Era for the Treatment of Hyperkalemia? New England Journal of Medicine 2015, 372, 275–277. [Google Scholar] [CrossRef]
- Hughes-Austin JM, Rifkin DE, Beben T, Katz R, Sarnak MJ, Deo R, et al. The Relation of Serum Potassium Concentration with Cardiovascular Events and Mortality in Community-Living Individuals. Clinical Journal of the American Society of Nephrology 2017, 12, 245–252. [Google Scholar] [CrossRef]
- Savarese G, Xu H, Trevisan M, Dahlström U, Rossignol P, Pitt B, et al. Incidence, Predictors, and Outcome Associations of Dyskalemia in Heart Failure With Preserved, Mid-Range, and Reduced Ejection Fraction. JACC Heart Fail 2019, 7, 65–76. [Google Scholar] [CrossRef]
- Desai, AS. Hyperkalemia in patients with heart failure: Incidence, prevalence, and management. Curr Heart Fail Rep 2009, 6, 272–280. [Google Scholar] [CrossRef]
- Sarwar CMS, Papadimitriou L, Pitt B, Piña I, Zannad F, Anker SD, et al. Hyperkalemia in Heart Failure. J Am Coll Cardiol 2016, 68, 1575–1589. [Google Scholar] [CrossRef]
- Burnett H, Earley A, Voors AA, Senni M, McMurray JJV, Deschaseaux C, et al. Thirty Years of Evidence on the Efficacy of Drug Treatments for Chronic Heart Failure With Reduced Ejection Fraction. Circ Heart Fail 2017, 10. [Google Scholar]
- Bao J, Kan R, Chen J, Xuan H, Wang C, Li D, et al. Combination pharmacotherapies for cardiac reverse remodeling in heart failure patients with reduced ejection fraction: A systematic review and network meta-analysis of randomized clinical trials. Pharmacol Res 2021, 169, 105573. [Google Scholar] [CrossRef] [PubMed]
- Weir MR, Rolfe M. Potassium Homeostasis and Renin-Angiotensin-Aldosterone System Inhibitors. Clinical Journal of the American Society of Nephrology 2010, 5, 531–548. [Google Scholar] [CrossRef] [PubMed]
- Ouwerkerk W, Voors AA, Anker SD, Cleland JG, Dickstein K, Filippatos G, et al. Determinants and clinical outcome of uptitration of ACE-inhibitors and beta-blockers in patients with heart failure: a prospective European study. Eur Heart J 2017, 38, 1883–1890. [Google Scholar] [CrossRef] [PubMed]
- Epstein M, Reaven NL, Funk SE, McGaughey KJ, Oestreicher N, Knispel J. Evaluation of the treatment gap between clinical guidelines and the utilization of renin-angiotensin-aldosterone system inhibitors. Am J Manag Care 2015, 21 (11 Suppl), S212–S220.
- Rosano GMC, Tamargo J, Kjeldsen KP, Lainscak M, Agewall S, Anker SD, et al. Expert consensus document on the management of hyperkalaemia in patients with cardiovascular disease treated with renin angiotensin aldosterone system inhibitors: coordinated by the Working Group on Cardiovascular Pharmacotherapy of the European Society of Cardiology. Eur Heart J Cardiovasc Pharmacother 2018, 4, 180–188. [Google Scholar]
- Elliott MJ, Ronksley PE, Clase CM, Ahmed SB, Hemmelgarn BR. Management of patients with acute hyperkalemia. Can Med Assoc J 2010, 182, 1631–1635. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes CKD Work Group. KDIGO 2012 clinical practice guideline for the evaluation and management of chronic kidney disease. Kidney Int Suppl 2013, 3, 1. [Google Scholar]
- Sterns RH, Rojas M, Bernstein P, Chennupati S. Ion-Exchange Resins for the Treatment of Hyperkalemia. Journal of the American Society of Nephrology 2010, 21, 733–735. [Google Scholar] [CrossRef]
- Ponikowski A del G de TP, Voors AA, Anker SD, Bueno H, Cleland JGF, Coats AJS, et al. Guía ESC 2016 sobre el diagnóstico y tratamiento de la insuficiencia cardiaca aguda y crónica. Rev Esp Cardiol 2016, 69, e1–e1167. [Google Scholar]
- Rosano GMC, Spoletini I, Agewall S. Pharmacology of new treatments for hyperkalaemia: patiromer and sodium zirconium cyclosilicate. European Heart Journal Supplements 2019, 21 (Supplement_A), A28–A33. [CrossRef]
- Anker SD, Kosiborod M, Zannad F, Piña IL, McCullough PA, Filippatos G, et al. Maintenance of serum potassium with sodium zirconium cyclosilicate ( <scp>ZS</scp> -9) in heart failure patients: results from a phase 3 randomized, double-blind, placebo-controlled trial. Eur J Heart Fail 2015, 17, 1050–1056. [Google Scholar]
- Pitt B, Bakris GL, Bushinsky DA, Garza D, Mayo MR, Stasiv Y, et al. Effect of patiromer on reducing serum potassium and preventing recurrent hyperkalaemia in patients with heart failure and chronic kidney disease on <scp>RAAS</scp> inhibitors. Eur J Heart Fail 2015, 17, 1057–1065. [Google Scholar]
- Kim K, Thomsen RW, Nicolaisen SK, Hasvold LP, Palaka E, Sørensen HT. Healthcare resource utilisation and cost associated with elevated potassium levels: a Danish population-based cohort study. BMJ Open 2019, 9, e026465. [Google Scholar] [CrossRef] [PubMed]
- https://www.xunta.gal/dog/Publicados/2014/20140521/AnuncioC3K1-140514-0001_es.html.
- Lopez-López A, Franco-Gutiérrez R, Pérez-Pérez AJ, Regueiro-Abel M, Elices-Teja J, Abou-Jokh-Casas C, et al. Impact of Hyperkalemia in Heart Failure and Reduced Ejection Fraction: A Retrospective Study. J Clin Med 2023, 12. [Google Scholar]
- Jiménez-Marrero S, Cainzos-Achirica M, Monterde D, Vela E, Cleries M, García-Eroles L, et al. Impact on clinical outcomes and health costs of deranged potassium levels in patients with chronic cardiovascular, metabolic, and renal conditions. Revista Española de Cardiología (English Edition) 2021, 74, 312–320. [Google Scholar] [CrossRef]
- Olry de Labry Lima A, Díaz Castro Ó, Romero-Requena JM, García Díaz-Guerra M de los R, Arroyo Pineda V, de la Hija Díaz MB, et al. Hyperkalaemia management and related costs in chronic kidney disease patients with comorbidities in Spain. Clin Kidney J 2021, 14, 2391–2400. [Google Scholar] [CrossRef]
- Thomsen RW, Nicolaisen SK, Hasvold P, Garcia-Sanchez R, Pedersen L, Adelborg K, et al. Elevated Potassium Levels in Patients With Congestive Heart Failure: Occurrence, Risk Factors, and Clinical Outcomes. J Am Heart Assoc 2018, 7. [Google Scholar]
- Clase CM, Carrero JJ, Ellison DH, Grams ME, Hemmelgarn BR, Jardine MJ, et al. Potassium homeostasis and management of dyskalemia in kidney diseases: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 2020, 97, 42–61. [Google Scholar] [CrossRef]
- House AA, Wanner C, Sarnak MJ, Piña IL, McIntyre CW, Komenda P, et al. Heart failure in chronic kidney disease: conclusions from a Kidney Disease: Improving Global Outcomes (KDIGO) Controversies Conference. Kidney Int 2019, 95, 1304–1317. [Google Scholar] [CrossRef]
- Ortiz A, del Arco Galán C, Fernández-García JC, Gómez Cerezo J, Ibán Ochoa R, Núñez J, et al. Documento de consenso sobre el abordaje de la hiperpotasemia. Nefrología 2023, 43, 765–782. [Google Scholar] [CrossRef]
- Rosano GMC, Tamargo J, Kjeldsen KP, Lainscak M, Agewall S, Anker SD, et al. Expert consensus document on the management of hyperkalaemia in patients with cardiovascular disease treated with renin angiotensin aldosterone system inhibitors: coordinated by the Working Group on Cardiovascular Pharmacotherapy of the European Society of Cardiology. Eur Heart J Cardiovasc Pharmacother 2018, 4, 180–188. [Google Scholar]
- Sterns RH, Rojas M, Bernstein P, Chennupati S. Ion-Exchange Resins for the Treatment of Hyperkalemia. Journal of the American Society of Nephrology 2010, 21, 733–735. [Google Scholar] [CrossRef] [PubMed]
- Weir MR, Bakris GL, Bushinsky DA, Mayo MR, Garza D, Stasiv Y, et al. Patiromer in Patients with Kidney Disease and Hyperkalemia Receiving RAAS Inhibitors. New England Journal of Medicine. 2015, 372, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Packham DK, Kosiborod M. Potential New Agents for the Management of Hyperkalemia. American Journal of Cardiovascular Drugs 2016, 16, 19–31. [Google Scholar] [CrossRef] [PubMed]
- Weir MR, Bakris GL, Bushinsky DA, Mayo MR, Garza D, Stasiv Y, et al. Patiromer in Patients with Kidney Disease and Hyperkalemia Receiving RAAS Inhibitors. New England Journal of Medicine 2015, 372, 211–221. [Google Scholar] [CrossRef]
- Spinowitz BS, Fishbane S, Pergola PE, Roger SD, Lerma E V. , Butler J, et al. Sodium Zirconium Cyclosilicate among Individuals with Hyperkalemia. Clinical Journal of the American Society of Nephrology 2019, 14, 798–809. [Google Scholar] [CrossRef]
- Agiro A, AN A, Cook EE, Mu F, Chen J, Desai P, et al. Real-World Modifications of Renin-Angiotensin-Aldosterone System Inhibitors in Patients with Hyperkalemia Initiating Sodium Zirconium Cyclosilicate Therapy: The OPTIMIZE I Study. Adv Ther 2023, 40, 2886–2901. [Google Scholar] [CrossRef]
- Rastogi A, Pollack C V, Sánchez Lázaro IJ, Lesén E, Arnold M, Franzén S, et al. Maintained renin–angiotensin–aldosterone system inhibitor therapy with sodium zirconium cyclosilicate following a hyperkalaemia episode: a multicountry cohort study. Clin Kidney J 2024, 17. [Google Scholar]
- https://www.aemps.gob.es/medicamentosUsoHumano/informesPublicos/docs/IPT-patiromer-Veltassa-hiperpotasemia.pdf.
- Sharma A, Alvarez PJ, Woods SD, Fogli J, Dai D. Healthcare resource utilization and costs associated with hyperkalemia in a large managed care population. Journal of Pharmaceutical Health Services Research 2021, 12, 35–41. [Google Scholar] [CrossRef]
- Epstein M, Alvarez PJ, Reaven NL, Funk SE, McGaughey KJ, Brenner MS, et al. Evaluation of clinical outcomes and costs based on prescribed dose level of renin-angiotensin-aldosterone system inhibitors. Am J Manag Care 2016, 22 (11 Suppl), s311–s324.
Figure 1.
Flow chart.
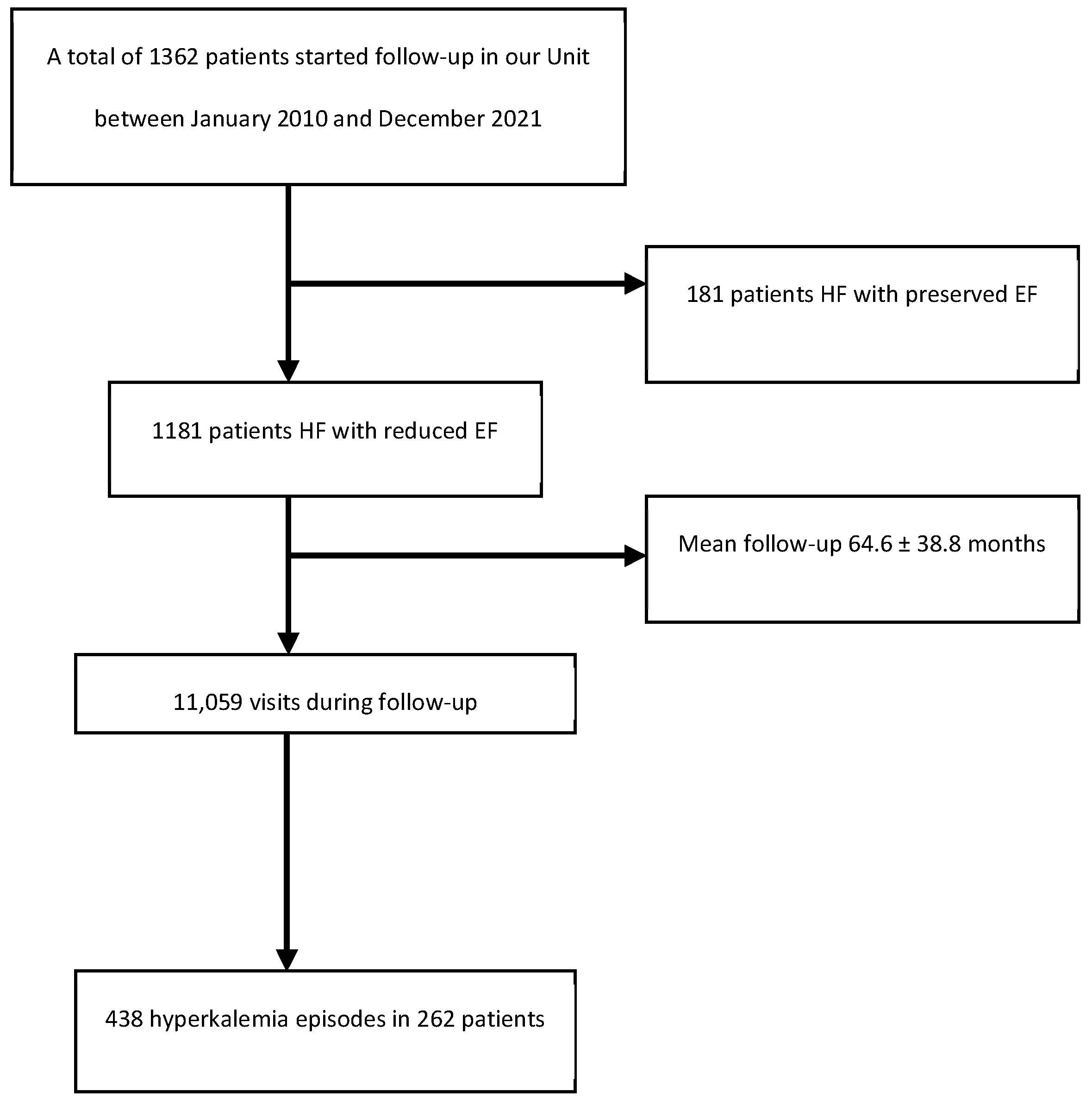
Figure 2.
Hyperkalemia episodes over the course of follow-up.
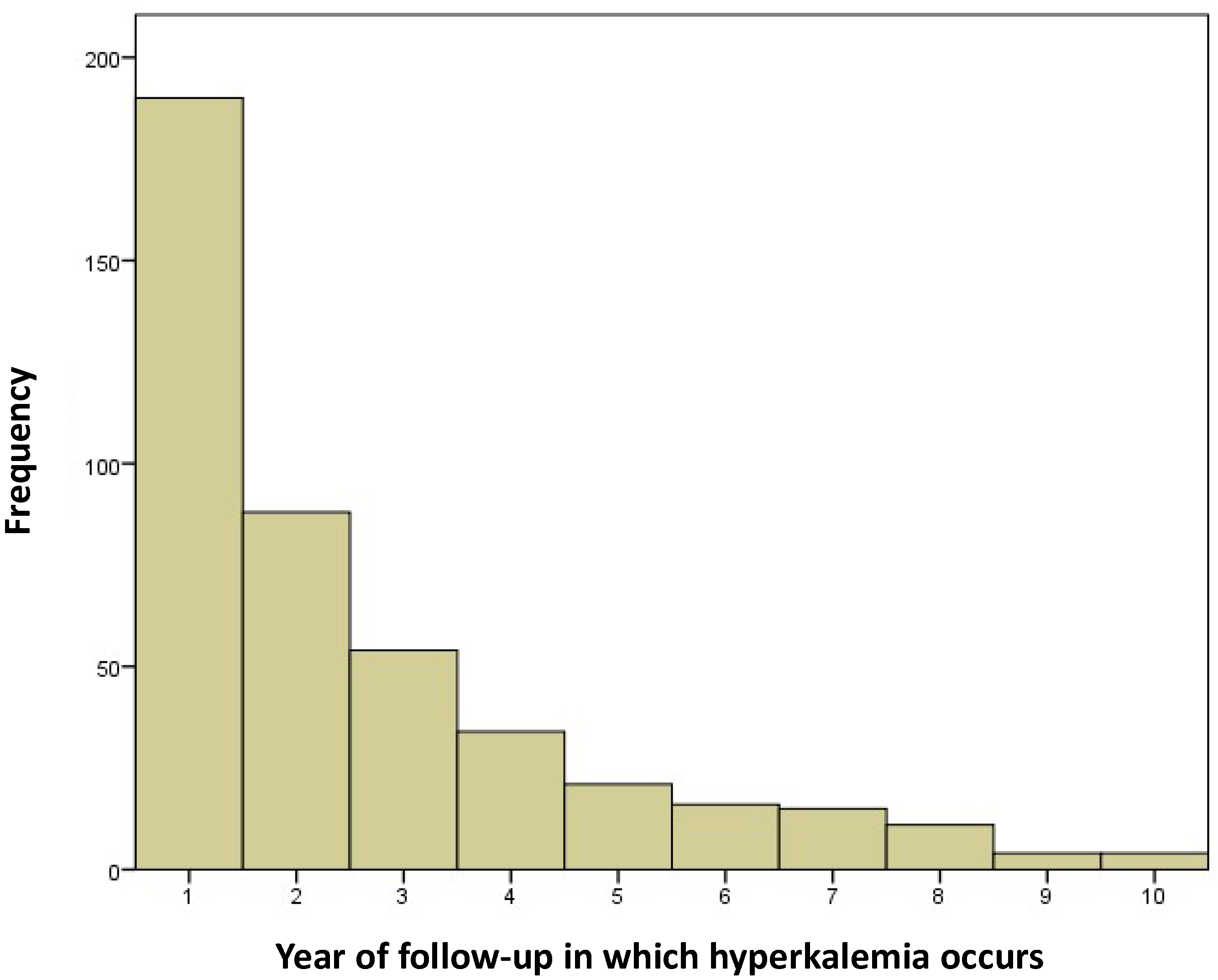

Table 1.
Baseline characteristics of the study population.
| Characteristics | N = 1181 | |
| Males, n (%) | 913 (77.3%) | |
| Age (years) | 66.6 ± 11.0 | |
| Arterial hypertension, n (%) | 721 (61.0%) | |
| Diabetes mellitus, n (%) | 448 (37.9%) | |
| Smoking (ex-smoker and active smoker), n (%) | 631(53.5%) | |
| Alcohol abuse (previous and current consumption: > 2 alcoholic beverage equivalents per day in males and > 1 in females), n (%) | 494(41.8%) | |
| Body mass index (kg/m2) | 28.8 ± 5.1 | |
| NYHA functional class ≥ 2, n (%) | 843 (71.4%) | |
| Systolic blood pressure (mmHg) | 128.2 ± 20.8 | |
| Diastolic blood pressure (mmHg) | 70.2 ± 11.2 | |
| Primary cause, n (%) | ||
| Ischemic | 467 (39.8%) | |
| Idiopathic | 204(17.4%) | |
| Alcoholic | 101 (8.6%) | |
| Tachycardia-induced cardiomyopathy | 100 (8.5%) | |
| Hypertensive | 88 (7.5%) | |
| Others | 221(18.2%) | |
| Left ventricular ejection fraction (%) | 31.5 ± 7.0 | |
| Hematocrit (%) | 41.7 ± 5.3 | |
| Creatinine clearance, MDRD (ml/min/1.73 m2) | 72.0 ± 24.7 | |
| Creatinine clearance < 60 ml/min/1.73 m2, n (%) | 371(31.3%) | |
| Basal potassium (mEq/l) | 4.66 ± 0.4 | |
| Basal potassium > 5.5(mEq/l), n (%) | 24 (2.0%) | |
| Treatment (first consultation), n (%) | ||
| ARNi/ACEi/ARBi | 1149 (97.3%) | |
| BB | 1143 (97.8%) | |
| MRAs | 699 (59.1%) | |
| SGLT2i | 132 (11.2%) | |
| Loop diuretics | 703 (67.3%) | |
| Potassium supplements | 2(0.2%) | |
| Drug doses at first consultation (over 1, maximum dose according to ESC guidelines) | ||
| ARNi/ACEi/ARBi | 0.64 ± 0.49 | |
| BB | 0.77 ± 0.34 | |
| MRAs | 0.31 ± 0.26 | |
| Loop diuretics | 0.74 ± 0.77 | |
| Treatment (at 1 year), n (%) | ||
| ARNi/ACEi/ARBi | 955 (97.2%) | |
| BB | 947 (97.8%) | |
| MRAs SGLT2i |
622 (67.3%) 171 (17.4%) |
|
| Loop diuretics | 492 (55.2%) | |
| Drug doses at one year (over 1, maximum dose according to ESC guidelines) | ||
| ARNi/ACEi/ARBi | 0.88 ± 0.56 | |
| BB | 0.80 ± 0.34 | |
| MRAs Loop diuretics |
0.32 ± 0.28 0.63 ± 0.78 |
|
1 Abbreviations: ACEIs: angiotensin-converting enzyme inhibitors; ARAIIs: angiotensin II receptor antagonists; ARNi: neprilysin and angiotensin II receptor inhibitor; IAD: implantable automatic defibrillator; SGLT2i: sodium glucose co-transporter-2 inhibitor; BB: beta-blocker; ESC: European Society of Cardiology; MDRD: Modification of diet in renal disease; MRA: mineralocorticoid receptor antagonist; NYHA: New York Heart Association.
Table 2.
Summary of general costs due to hospital services in patients with hyperkalemia episodes.
| Item | Health Service assigned cost | Total number | Total cost | Number, first year | Cost, first year |
|---|---|---|---|---|---|
| Emergency care | €361.59 | 13 | €4700.65 | 8 | €2892.72 |
| Stay in ward (days) | €528.95 | 49 | €25,918.56 |
28 | €14,810.6 |
| Stay in ICU (days) | €1142.48 | 2 | €2284.95 | 0 | 0 |
| Follow-up laboratory test* | €14.52 + €34.52 + €9.91 | 953 | €56,274.65 | 437 | €25,804.85 |
| Total cost | €89,178.83 | €43,508.17 |
*Follow-up laboratory test includes the costs related to the extraction visit, the material used in testing, and the physician telephone contact.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



