
Submitted:
27 November 2024
Posted:
28 November 2024
You are already at the latest version
Abstract
Background/Objectives: Fibromyalgia is a chronic condition characterized by widespread pain, fatigue, and impaired physical functionality, significantly impacting patients' quality of life. This study aimed to evaluate and compare the effects of two therapeutic interventions—neuromodulation using the EXOPULSE Mollii suit and a structured exercise training program—on the physical and respiratory functionality of female fibromyalgia patients. Methods: A crossover randomized controlled trial was conducted with 10 female fibromyalgia patients (mean age: 51.6 ± 7.18 years). Participants underwent two interventions, each consisting of 16 sessions, with a two-week washout period between treatments. Neuromodulation sessions employed a standardized electrode configuration, while the exercise program included strength training and high-intensity interval training. Outcome measures included respiratory variables (FEV1, FEV6, FEV1/FEV6 ratio, chest perimeter differences) and functional tests (handgrip strength, chair stand, 10-meter up-and-go, and balance tests). Results: Both interventions improved physical and respiratory functionality. Significant gains in the chair stand test (neuromodulation: +6.7 repetitions; exercise: +3.86 repetitions) and FEV1/FEV6 ratio were observed. Neuromodulation yielded greater improvements in balance and handgrip strength, while the exercise intervention demonstrated superior effects on mobility and speed, as evidenced by the 10-meter up-and-go test (final time: neuromodulation 5.4 s vs. exercise 4.97 s). Conclusions: Both neuromodulation and structured exercise programs are effective non-pharmacological interventions for enhancing physical and respiratory functionality in fibromyalgia patients. The complementary effects observed suggest that integrating these therapies could provide a holistic approach to managing fibromyalgia symptoms and improving quality of life.
Keywords:
Fibromyalgia
; Neuromodulation
; Exercise Intervention
; Respiratory Function
; Physical Functionality
; Quality of Life
1. Introduction
Fibromyalgia is recognized as a long-term condition marked by widespread musculoskeletal pain, fatigue, sleep disturbances, autonomic dysfunction, cognitive impairments, heightened sensitivity to stimuli, various somatic symptoms, and psychiatric comorbidities [1,2]. It is one of the three most prevalent musculoskeletal disorders globally, along with lower back pain and osteoarthritis, affecting an estimated 2-3% of the global population [2]. In Western Europe, the prevalence increases to around 4.7% [3]. The condition primarily affects women, with a female-to-male ratio of 3:1 [4], and its incidence tends to rise with age, particularly between the ages of 50 and 60 [5].
The pain experienced by individuals with fibromyalgia varies in terms of nature, location, and intensity, and is influenced by factors such as occupational roles, coexisting conditions, environmental elements like temperature and pressure, and physical or mental stress [6]. Patients commonly endure both physical and mental fatigue, which can range from mild tiredness to severe, fever-like exhaustion [7]. Other frequent symptoms include insomnia [7,8], cognitive impairments like memory loss [9], depression, anxiety [10], headaches [11], gastrointestinal issues [12], genitourinary disorders [13], morning stiffness [14], and autonomic disturbances such as dry mouth and eyes, blurred vision, or light sensitivity [2]. Negative emotions and general distress are also widespread, leading to increased rates of psychiatric disorders, with anxiety affecting 60% of patients and depression rates ranging from 14% to 36%, compared to 6.6% in the general population [15]. Recent research has highlighted mitochondrial dysfunction in fibromyalgia patients, revealing muscle oxygen saturation levels as low as 20%, in contrast to the normal range of approximately 75% [16]. The reason for this reduction, whether due to impaired mitochondrial energy production or heightened energy demand by muscle fibers, remains unclear [17,18].
Managing fibromyalgia requires a comprehensive, multidisciplinary approach that combines pharmacological and psychological therapies, patient education, physical exercise, and dietary adjustments [19]. Pharmacological treatments primarily target pain relief, with some centrally acting medications, such as antidepressants and anticonvulsants, proving effective by influencing pain-inhibitory neurotransmitters, reducing dorsal horn sensitization, and alleviating systemic hyperexcitability [20]. However, only around 25% of patients experience a 30% reduction in pain symptoms with antidepressant therapy [21]. Due to the varied nature of the disease, pharmacological treatments are not standardized, leading to the use of various other medications, including muscle relaxants [22], analgesics [23], hypnotic and antipsychotic drugs [23,24], and cannabinoids [25]. Despite substantial research efforts, no single drug consistently benefits more than half of the treated patients [26]. Cognitive-behavioral therapy, which focuses on helping patients develop effective coping strategies, has shown better outcomes in terms of pain management, physical function, and mood improvement compared to other approaches [27]. Patient education is crucial in helping individuals understand the chronic nature of the condition and take an active role in its management [28]. While pharmacological treatments target specific physiological aspects of the condition, non-pharmacological interventions offer a broader, more holistic impact that is challenging to replicate through medication alone [29].
A variety of non-drug therapies have been studied. Neuromodulation therapies, such as localized transcutaneous electrical nerve stimulation (TENS) [30] or the use of the EXOPULSE Mollii suit [17,18,31], have demonstrated positive effects on pain relief, muscle oxygenation, parasympathetic activity, and overall functionality in fibromyalgia patients. Exercise, including aerobic and strength training, has been consistently shown to alleviate symptoms, improve physical functionality, and enhance overall well-being in fibromyalgia patients [32]. Regular strength training not only improves muscle strength and endurance but also positively impacts pain perception, muscle oxygenation, and autonomic regulation [33]. High-intensity interval training (HIIT) has emerged as an effective approach for enhancing functional performance, including muscle strength, balance, and cardiovascular health [34]. Moreover, in fibromyalgia patients an increase in muscle oxygenation has been reported together with a decrease in pain perception [35]. Additionally, nutritional strategies play a complementary role in managing fibromyalgia symptoms. A balanced diet rich in anti-inflammatory foods, omega-3 fatty acids, and micronutrients like magnesium and vitamin D has been linked to reductions in inflammation, improved energy levels, and better management of pain and fatigue [36]. Emerging evidence highlights the impact of the gut-brain axis on fibromyalgia symptoms, emphasizing the potential benefits of probiotics and dietary interventions in improving mood, cognitive function, and physical health [37]. These non-pharmacological interventions are increasingly recognized as first-line therapies due to their ability to address the multifaceted symptoms of fibromyalgia and promote sustainable improvements without the side effects associated with pharmacological treatments [2,23].
This study seeks to evaluate and compare the impact of a 16-session treatment using the EXOPULSE Mollii suit and a 16-session exercise training program on the physical and respiratory function of female patients with fibromyalgia. The primary hypothesis proposes that notable differences in functionality will be observed between baseline and post-intervention assessments for both treatment approaches.
2. Materials and Methods
2.1. Study Design
This research was carried out at the Faculty of Medicine, University of Badajoz, Spain, utilizing a crossover design following the methodology depicted by Rubio-Zarapuz et al. (2024) in previous research [35,38]. The aim was to evaluate and contrast the extended effects of two different therapeutic interventions in the physical and respiratory function on individuals diagnosed with fibromyalgia, adhering strictly to the 2016 criteria established by the American College of Rheumatology (ACR) [15]. This article is part of a broader research series exploring the efficacy of neuromodulation and exercise interventions in fibromyalgia patients. Previous studies from this series evaluated the effects of these treatments on muscle oxygenation and pain perception [35], as well as autonomic modulation [38]. Together, these articles aim to provide a comprehensive understanding of the physiological and functional adaptations induced by these interventions.
The interventions being evaluated consisted of a treatment plan that included the use of the EXOPULSE Mollii suit (Exoneural Network, Sweden) and a structured exercise program. Participants were recruited from September to December 2022. The intervention phase began in January 2023.
2.2. Participants
After a thorough recruitment and evaluation process, the study enrolled a total of 10 female patients diagnosed with fibromyalgia (mean age: 51.6 ± 7.18 years; mean weight: 68.5 ± 8.26 kg; mean height: 160 ± 3.80 cm; Body Mass Index (BMI): 26.7 ± 2.79 kg/m²). To be eligible, participants needed to meet several criteria: they had to be formally diagnosed with fibromyalgia by a rheumatologist following the ACR guidelines, with the diagnosis confirmed at least three months prior to the study. Only females aged 18 to 67 who could walk independently without assistive devices were considered. Strict exclusion criteria were applied, disqualifying candidates who were participating in other clinical trials, had previously undergone neuromodulation therapy or been involved in structured exercise programs in the past six months, did not provide written consent, or had neurological disorders or conditions affecting pain perception. Additionally, those who had recently undergone surgery, sustained musculoskeletal injuries within the last six months, or had severe cardiovascular or respiratory conditions were excluded, as were individuals undergoing opioid therapy or whose pain management medication had been altered in the previous month. The final cohort size was determined by the availability of scheduling, facilities, and resources. This careful selection process ensured that the participant group met all operational and clinical criteria, allowing for a controlled and scientifically rigorous evaluation of the intervention's effects on fibromyalgia symptoms. The recruitment of 10 patients for this study was based on logistical constraints, including resource availability, scheduling, and the intensive nature of the interventions. While a larger sample size could enhance statistical power and generalizability, the chosen size was sufficient to demonstrate within-subject differences in this crossover randomized controlled trial design. Previous studies in similar populations have effectively utilized small cohorts to explore the efficacy of neuromodulation and exercise interventions [39,40]. The crossover design further mitigates the limitations of a small sample by allowing each participant to act as their own control, reducing inter-individual variability and enhancing statistical robustness.
2.3. Intervention
To achieve the goals of the study, participants randomly started one of the two treatments, having 5 participants doing each treatment at a time. Each participant completed two sessions of their assigned intervention per week for 8 weeks, totaling 16 sessions of treatment. After the 8 weeks of treatment, a 2-week washout period was introduced to clear any lingering treatment effects. The two-week washout period was chosen based on evidence indicating that the physiological effects of neuromodulation and structured exercise interventions diminish within this timeframe [35,38]. This duration ensures the minimization of carryover effects from the first intervention, allowing participants' physiological baselines to reset before initiating the subsequent intervention phase. Similar washout periods have been successfully implemented in studies evaluating therapeutic interventions in populations with chronic conditions [41,42]. Following this break, participants underwent the opposite treatment following the same process 2 sessions of the assigned intervention per week for 8 weeks totaling 16 sessions. Resulting in a total of 18 weeks of intervention (Figure 1).
To address potential biases and limitations in external validity, several methodological controls were implemented. Randomization of treatment order ensured that no systematic bias influenced the outcomes. The use of a two-week washout period minimized carryover effects, resetting physiological baselines before the second intervention phase. Additionally, strict inclusion and exclusion criteria were applied to ensure homogeneity in the study population, reducing confounding factors. Although the small sample size limits generalizability, the findings provide valuable insights into the physiological and functional effects of these interventions, serving as a foundation for larger-scale studies. Future research should expand on this work by including more diverse populations to confirm and broaden these results.
The specific interventions applied to each treatment are outlined as follows:
- Suit: Participants engaged in a 60-minute session with the EXOPULSE Mollii suit, which utilized all 58 electrodes set at an intensity of 2 milliamperes (mA) and a pulse width of 30 milliseconds (ms). This protocol adhered to the treatment procedures established in earlier research [17,18,35,38,43,44]. A certified professional ensured proper placement of the electrodes for each participant. Once the suit was properly fitted and the control unit connected, the participant was positioned lying down on a massage table, after which the session began with the activation of the suit.
- Exercise: Participants attended 1-hour training sessions that began with a mobility warm-up, followed by a main workout consisting of strength exercises and High-Intensity Interval Training (HIIT). The intervention followed a methodology previously described [35,38] being divided into three phases: the first block, comprising sessions 1 and 2, focused on strength training and served as a familiarization phase, essential for building a foundation for the more intense training that followed. This phase helped participants adjust to the exercise routine, ensuring they were comfortable and minimizing the risk of injury. The second block, covering sessions 3 through 8, concentrated on HIIT training; each session included 4 circuits that participants had to complete, with an increasing training volume throughout this phase. The final block focused on strength training using a circuit format, where participants completed all exercises within a circuit before resting and moving on to the next circuit, continuing this pattern until the session was completed.
2.4. Measurements
Outcome measures were assessed both before and after the interventions at three key points: the 1st, 8th, and 16th treatment sessions for each intervention. This multi-phase evaluation approach follows methodologies previously validated in longitudinal research, offering a strong framework for quantifying the effects of the interventions on the participants. The choice of variables for analysis, as well as the assessment methods, were guided by established protocols outlined in earlier academic studies [17,18].
2.4.1. Respiratory Variables
Respiratory variables were assessed using a Vitalograph Asma1 spirometer [45]. Following previously used methodology [18], patients performed the test while seated, where they were instructed to take a deep breath (filling their lungs completely), seal their lips around the mouthpiece, and exhale as quickly and forcefully as possible until their lungs were fully emptied. This maneuver was repeated three times [46], with the best result from the three trials being recorded. Measurements included forced expiratory volume in 1 second (FEV1), 6 seconds (FEV6), and the ratio of these two values (FEV1/FEV6) [47]. Additionally, the difference in chest perimeter between full inhalation and full exhalation was measured using an anthropometric tape by a certified professional. Participants stood upright with feet together, wearing only a sports bra. The tape measure was placed around the chest at the mid-point of the sternum, ensuring that the tape was horizontal and parallel to the ground. Participants were instructed to perform a full inhalation and exhalation, during which both the highest and lowest points were recorded. The measurement of thoracic perimeter reflects thoracic mobility and respiratory function, key factors in assessing the physical functionality of fibromyalgia patients [47]. Reduced thoracic mobility has been linked to shallow breathing patterns and compromised respiratory efficiency, which are common in this population due to musculoskeletal pain and limited physical activity [48]. Assessing changes in thoracic perimeter helps to determine whether the interventions improve thoracic expansion during respiration, thereby supporting overall respiratory health and physical performance [49].
2.4.2. Functional Test
Based on the exercise test battery developed by Carbonell-Baeza et al. (2022) for fibromyalgia patients [50], the following functional tests were utilized implemented by a professional:
- Chair stand test: The patient is instructed to stand beside a chair, and the test involves counting how many times they can move from a seated to a fully standing position within 30 seconds. During the assessment, the patient must keep their back straight, feet flat on the ground, and refrain from using their arms to assist in standing.
- Handgrip strength test: This assessment is carried out using a grip dynamometer (Kuptone, model EH101). The patient completes the test twice with their dominant hand while standing, ensuring the arm is fully extended and held at a 30° angle from the trunk.
- Ten meter up-and-go test: The test begins with the patient seated in a chair. Once given the start signal, the patient is required to stand up and walk 10 meters as fast as possible without breaking into a run.
- One-leg balance: The participant is instructed to balance on one leg for as long as possible with their eyes open. This test is conducted separately on each leg.
2.5. Statistical Analysis
For the statistical analysis, we employed SPSS (Statistical Package for Social Sciences, version 25, IBM, Armonk, NY, USA). Descriptive statistics were reported as mean ± SD, and the Kolmogorov–Smirnov test was used to assess the normality of data distribution. T-tests were performed on parametric variables to assess the intervention effects, while the Wilcoxon test was used for non-parametric variables. A one-way ANOVA was conducted to compare treatment effects. A significance level of p ≤ 0.05 was applied for all tests. Additionally, effect sizes were calculated using Cohen’s d formula.
2.6. Ethical Aspects
The present study adhered to the ethical guidelines outlined in the Declaration of Helsinki. Ethical approval for the study was granted by the University of Évora's Research Ethics Committee (approval number 22033, issued on 31 January 2022). Before the study began, all participants were fully informed about the study's objectives and procedures. Consent was obtained voluntarily from participants through the signing of informed consent forms, confirming their understanding and willingness to take part in the research.
3. Results
In the suit intervention attending to respiratory variables there were only a decrease and an increase in the 1st and 16th sessions respectively for FEV1 (1st pre:2.34 post:2.28; 16th pre: 2.36 post:2.43), and FEV1/FEV6 (1st pre:0.85 post:0.83; 16th pre: 0.86 post:0.87) variables, with no change in the 8th session. While there were changes on FEV6 with a decrease on the 8th and an increase in the 16th sessions (8th pre: 2.77 post:2.73; 16th pre:2.76 post:2.79). Moreover, an increase was observed after the intervention in all sessions measured with this treatment (1st pre: 7.62 post:7.98; 8th pre:7.6 post:7.77; 16th pre: 8.8 post:9.4). Furthermore, changes were observed in all functional variables with the suit interventions. In the handgrip strength test, there was a decrease in the 1st session (pre:24.07 post:23.62) and an increase in the 8th (pre:24.28 post:25.47) and 16th sessions (pre: 23.38 post:24.33). While there was an increase in performance in all three sessions for the chair stand test (1st pre: 18 post:19.9; 8th pre:22.2 post:23.45; 16th pre:24.5 post:26.6), 10m up and go test (1st pre:6.06 post:5.66; 8th pre:5.45 post:5.31; 16th pre: 5.43 post:5.4) as well as the one leg balance test with the left leg (1st pre: 43.94 post:53.54; 8th pre: 59.09 post:67.52) except for the 16th session (pre:63.37 post:58.91) and with the right leg (8th pre:62.45 post:72.52; 16th pre:88.6 post:94.63)except for the 1st session (pre:45.5 post:42.46) were there was a decrease in the mean values of the participants.
In the exercise intervention in respiratory variables there was an increase in the 1st (pre: 2.37 post:2.46) session and a decrease in the 8th (pre:2.38 post:2.35) and 16th (pre:2.36 post:2.27) sessions for FEV1; in FEV6 there was an increase in the 1st (pre:2.75 post:2.82) and 8th (pre:2.71 post:2.72) session while there was a decrease for the 16th session (pre:2.75 post:2.72). Further on, there was a decrease for both the 8th (pre:0.88 post:0.87) and 16th (pre:0.86 post:0.84) session in the FEV1/FEV6 ratio. While there was an increase in all sessions for the chest perimeter (1st pre:7.2 post:7.9; 8th pre:8.7 post:8.85; 16th pre: 7.68 post:8.56). In addition, in functional tests there was an increase in performance in all sessions for the handgrip strength test (1st pre:23.64 post:24.45; 8th pre:23.55 post:24.41; 16th pre:24.24 post:24.72), the chair stand test (1st pre:19.5 post:20.7; 8th pre:21.9 post:23.3; 16th pre:23.56 post:24.56) and the 10m up and go test (1st pre:5.45 post:5.32; 8th pre:5.15 post:5.05; 16th pre:5.2 post:4.97). While there was an increase in the 1st (pre:71.47 post:78.54) and 16th (pre:57.8 post:64.26) session and a decrease in the 8th session (pre: 91.19 post:71.69) for the leg balance test with the right leg and an increase in the 1st (pre:63.51 post:98.07) and 8th (pre:56.84 post:71.03) sessions and a decrease in the 16th session (pre:74.74 post:45.36) for the left leg.

Table 1.
Descriptive statistics.
| Variables | Suit | Exercise | ||||||||||
| 1st session | 8th session | 16th session | 1st session | 8th session | 16th session | |||||||
| pre | post | pre | post | pre | post | pre | post | pre | post | pre | post | |
| FEV 1, L | 2.34 ± 0.52 | 2.28 ± 0.44 | 2.35 ± 0.46 | 2.35 ± 0.55 | 2.36 ± 0.52 | 2.43 ± 0.50 | 2.37 ± 0.49 | 2.46 ± 0.56 | 2.38 ± 0.48 | 2.35 ± 0.46 | 2.36 ± 0.53 | 2.27 ± 0.49 |
| FEV 1, % | 93.33 ± 12.12 | 91.56 ± 9.98 | 96.30 ± 11.81 | 95.70 ± 15.66 | 96.60 ± 12.44 | 99.30 ± 10.91 | 96.70 ± 11.72 | 100.10 ± 13.78 | 97.00 ± 11.51 | 95.70 ± 10.81 | 97.00 ± 13.60 | 94.44 ± 10.96 |
| FEV 6, L | 2.77 ± 0.62 | 2.77 ± 0.65 | 2.77 ± 0.69 | 2.73 ± 0.69 | 2.76 ± 0.66 | 2.79 ± 0.61 | 2.75 ± 0.64 | 2.82 ± 0.67 | 2.71 ± 0.60 | 2.72 ± 0.59 | 2.75 ± 0.61 | 2.72 ± 0.57 |
| FEV 6, % | 93.89 ± 13.12 | 93.11 ± 13.73 | 95.80 ± 17.81 | 84.88 ± 34.40 | 95.80 ± 15.65 | 97.00 ± 12.89 | 95.60 ± 15.01 | 97.80 ± 15.33 | 93.90 ± 13.58 | 94.30 ± 13.99 | 95.78 ± 13.65 | 94.67 ± 11.95 |
| FEV 1/FEV 6, n | 0.85 ± 0.05 | 0.83 ± 0.05 | 0.86 ± 0.06 | 0.86 ± 0.02 | 0.86 ± 0.04 | 0.87 ± 0.04 | 0.87 ± 0.04 | 0.87 ± 0.03 | 0.88 ± 0.03 | 0.87 ± 0.05 | 0.86 ± 0.05 | 0.84 ± 0.07 |
| FEV 1/FEV 6, % | 107.44 ± 6.84 | 106.11 ± 7.36 | 109.40 ± 8.67 | 109.30 ± 4.11 | 109.00 ± 5.10 | 110.20 ± 5.65 | 109.30 ± 6.38 | 110.30 ± 4.81 | 111.40 ± 4.86 | 109.40 ± 6.93 | 108.78 ± 7.79 | 106.00 ± 9.14 |
| Chest perimeter difference, cm | 7.62 ± 1.92 | 7.98 ± 1.79 | 7.60 ± 2.46 | 7.77 ± 2.52 | 8.80 ± 1.93 | 9.40 ± 2.33 | 7.20 ± 1.75 | 7.90 ± 1.91 | 8.70 ± 1.34 | 8.85 ± 1.49 | 7.68 ± 2.90 | 8.56 ± 2.65 |
| Handgrip strength test, kg | 24.07 ± 4.59 | 23.62 ± 4.64 | 24.28 ± 3.58 | 25.47 ± 3.99 | 23.38 ± 5.70 | 24.33 ± 5.28 | 23.64 ± 4.65 | 24.45 ± 2.95 | 23.55 ± 4.24 | 24.41 ± 3.75 | 24.24 ± 1.92 | 24.72 ± 2.29 |
| Chair stand test, n | 18.00 ± 8.46 | 19.90 ± 9.18 | 22.20 ± 9.08 | 23.45 ± 9.16 | 24.50 ± 9.35 | 26.60 ± 10.44 | 19.50 ± 8.87 | 20.70 ± 10.76 | 21.90 ± 8.36 | 23.30 ± 9.02 | 23.56 ± 8.97 | 24.56 ± 9.98 |
| 10 m up and go test, s | 6.06 ± 1.85 | 5.66 ± 1.41 | 5.45 ± 1.29 | 5.31 ± 1.27 | 5.43 ± 1.20 | 5.40 ± 0.97 | 5.45 ± 1.19 | 5.32 ± 1.32 | 5.15 ± 1.22 | 5.05 ± 1.07 | 5.20 ± 0.87 | 4.97 ± 0.85 |
| One leg balance right, s | 45.50 ± 37.85 | 42.46 ± 21.84 | 62.45 ± 36.31 | 72.52 ± 59.97 | 88.60 ± 72.19 | 94.63 ± 77.76 | 71.47 ± 51.97 | 78.54 ± 57.38 | 91.19 ± 92.53 | 71.69 ± 56.66 | 57.80 ± 48.26 | 64.26 ± 37.11 |
| One leg balance left, s | 43.94 ± 33.49 | 53.54 ± 47.97 | 59.09 ± 28.84 | 67.52 ± 55.92 | 63.37 ± 53.37 | 58.91 ± 48.58 | 63.51 ± 50.20 | 98.07 ± 91.49 | 56.84 ± 36.52 | 71.03 ± 45.05 | 74.74 ± 98.84 | 45.36 ± 27.95 |
* Data are expressed as means ± SD for quantitative variables. FEV1: forced expiratory volume in 1 s. FEV6: forced expiratory volume in 6 s.
Table 2, Table 3, Table 4, Table 5 and Table 6 display the comparative statistics for the sample. Table 2 shows one-way ANOVA results, highlighting significant differences in pre- and post-intervention measurements for the Chair Stand Test in both interventions. In the suit intervention, notable differences were found in post-session measurements for the FEV1/FEV6 ratio and the One-Leg Balance Test (left leg), as well as pre-session measurements for the 10 Meter Up-and-Go Test. In contrast, the exercise intervention revealed significant differences in pre-session chest perimeter difference measures and post-session results for the 10 Meter Up-and-Go Test. No significant differences were detected between the two interventions for any measurement except for the FEV1/FEV6 ratio after the first session (Table 3).
Table 4 highlights the comparative statistics between baseline and post-session measurements for each intervention. In the suit intervention, significant differences were found for the 10 Meter Up-and-Go Test in the 1st session, the Handgrip Strength Test in the 8th session, and both the FEV1/FEV6 ratio and Chair Stand Test in the 16th session. On the other hand, the exercise intervention showed significant pre- and post-intervention differences in FEV1 during the 1st session, the One-Leg Balance Test on the left leg, and the FEV1/FEV6 ratio in the 16th session.
Table 5 and Table 6 shows the comparative statistics between different measurements. In the suit intervention (Table 5), significant changes in respiratory variables were observed for FEV1 between the 1st and 16th post-session measurements, as well as in the FEV1/FEV6 ratio between the 1st and 8th, and the 1st and 16th post-session measurements. Additionally, significant differences in chest perimeter measurements were identified in the suit intervention between the 8th pre-session and 16th post-session measurements. In functional test outcomes, significant differences were found in the handgrip strength test between the 1st and 8th post-session measurements in the suit intervention. In the 10 Meter Up-and-Go Test, notable differences were observed between the 1st pre- and 8th pre- and post-session measurements for the suit intervention. Additionally, significant differences in the One-Leg Balance Test (right leg) were identified between the 1st and 16th post-session measurements, as well as between the 1st pre- and 16th post-session measurements. Significant changes were also seen in all comparisons for the Chair Stand Test. For the exercise intervention (Table 6), notable differences in the FEV1/FEV6 ratio were found between the 1st and 8th pre-session measurements, between the 1st pre-session and 16th post-session measurements, and between the 8th pre-session and 16th post-session measurements. For chest perimeter differences, significant changes were detected between the 1st and 8th pre-session measurements, the 1st and 8th post-session measurements, the 1st pre-session and 8th post-session measurements, and the 1st pre-session and 16th post-session measurements. In functional test outcomes significant differences were found in the 10m up and go test between the 1st pre-session and 16th post-session measurements for the exercise intervention. Significant changes were also seen in all comparisons for the Chair Stand Test across both interventions, except between the 1st and 8th pre-session measurements, the 8th and 16th pre-session measurements, and between the 8th pre- and 16th post-session measurements.
4. Discussion
This study aimed to investigate the effects of different therapeutic approaches on the functionality of female patients with fibromyalgia. The analysis of the collected data supports the primary hypothesis, indicating statistically significant differences in the patients' functionality assessments. Regarding respiratory functionality, we observed a significant increase in FEV1 values during the first session of the exercise intervention, as well as in the FEV1/FEV6 ratio by the 16th session in both interventions. These findings contrast with previous studies on fibromyalgia patients, which reported no significant changes in FEV1, FEV6, or FEV1/FEV6 ratios for either neuromodulation or strength exercise during 60-minute sessions [18]. The observed difference in the FEV1/FEV6 ratio may be attributed to an accumulative effect of the treatment across sessions, as evidenced by the clear increasing trend in FEV1 values during the suit treatment, while FEV6 remained stable. This resulted in a significant difference in the FEV1/FEV6 ratio by the 16th session.
Furthermore, significant differences were noted between post-session measurements in the suit intervention and between post-intervention FEV1 values in the 1st and 16th sessions. The increase in forced expiration observed in fibromyalgia patients could be attributed to the analgesic effects of neuromodulation [17,18,31], which potentially enhanced expiratory muscle activation and functioning. Conversely, the significant decrease in the FEV1/FEV6 ratio during the 16th session of the exercise intervention could be attributed to fatigue induced by the incremental nature of the training sessions. This last session, being the most intense, likely caused subsequent fatigue, thereby reducing forced expiratory capacity.
Additionally, the increased FEV1 value observed during the first session of the exercise intervention can be ascribed to bronchodilation and greater expiratory muscle activation induced by exercise, allowing patients to have a greater forced expiratory capacity. No significant differences in chest perimeter values were observed before and after sessions for any of the treatments studied, which contradicts previous findings [18]. Despite this, significant differences were noted between session measurements, indicating an increase in chest perimeter values after both interventions, represented by significant differences between basal values and the 16th post-session measurement. This increase was 1.78 cm for neuromodulation and 1.36 cm for exercise interventions. In addition, statistically significant differences were found between pre-intervention chest perimeter measures for the exercise treatment, suggesting exercise-induced adaptation in this variable for fibromyalgia patients. This finding highlights the potential for improved respiratory functionality through exercise interventions in this patient population.
Fibromyalgia is characterized by musculoskeletal pain and fatigue, significantly hindering physical function and quality of life for patients [1,2]. Consequently, the primary objective of fibromyalgia treatment should be to enhance physical functionality, as this directly impacts patients' quality of life. In this context, our study revealed varying results in functionality assessments. In the handgrip strength test, significant differences were observed only between the pre- and post-measures for the 8th session and when comparing the 1st and 8th post-session measurements in the suit treatment. These findings align with previous research, which reported no significant differences in handgrip strength after a single session of either exercise or neuromodulation [18]. The results suggest that significant improvements in handgrip strength are evident by the 8th session of neuromodulation treatment, though this improvement does not extend to the 16th session. The lack of influence of the exercise intervention on handgrip strength may be due to the absence of specific exercises targeting handgrip strength in the treatment plan.
Additionally, previous studies reported significant differences in the Chair Stand Test after a single 60-minute session with both treatments [18]; however, we did not find any significant intrasession differences. Notwithstanding, significant differences were noted between all pre- and post-session values when compared using a one-way ANOVA for both treatments. Moreover, a t-test revealed significant changes in different session measurements for the suit intervention and nearly all for the exercise intervention. These findings indicate substantial improvements in this test for both treatments, with a gain of 6.5 repetitions in pre-session measures between the 1st and 16th sessions and 6.7 repetitions in post-session conditions for the suit treatment. The exercise treatment exhibited a 4.06 increase in pre-session measures and 3.86 repetitions increase in post-session measurements. Thus, both treatments enhanced lower limb functionality, though neuromodulation demonstrated a slightly greater effect. In the 10-meter Up and Go Test, significant differences were observed after one session of the neuromodulation treatment, whereas no significant differences were found after a single exercise session, contradicting previous findings [18]. Additionally, significant differences were noted between different session measurements, indicating performance improvements in this test for both treatments. These results suggest enhanced strength, power, and velocity, with the exercise intervention yielding a greater impact. Patients achieved a mean time of 4.97 seconds after the 16th session in the exercise intervention compared to 5.4 seconds in the neuromodulation intervention.
Balance was also assessed throughout both treatments, with no significant variations observed in the 1st session, consistent with previous findings [18]. However, significant differences were noted between pre- and post-session measurements on the left leg in the 8th session of the exercise intervention and between session comparisons on the right leg in the suit intervention when comparing basal and 16th post-session measurements. These findings suggest an adaptation and subsequent improvement in balance with successive neuromodulation sessions, likely due to enhanced muscle coordination, reduced pain, and corrected muscle stimulation. The dominant leg showed the most improvement, possibly due to the preferential activation of neural pathways on the dominant side. Conversely, a decrease in balance means values after the 8th and 16th exercise interventions, though not statistically significant, may be attributed to fatigue induced by the training sessions. Pre-intervention measurements, however, indicated improved balance, suggesting an adaptation induced by the exercise intervention through better muscle coordination and increased lower limb muscle force capacity. Overall, the findings suggest enhanced physical functionality for patients undergoing both treatments, demonstrating improvements in strength, velocity, power, and balance. These enhancements can be attributed to the analgesic effects and improved muscle function associated with both treatments, highlighting their potential to enhance the quality of life for fibromyalgia patients.
4.1. Limitations and Future Research
This study has several limitations that should be considered when interpreting the results. The small sample size of 10 participants limits the generalizability of the findings. Future studies should include a larger and more diverse sample to enhance external validity. Additionally, the study duration was relatively short, spanning only 16 sessions over a few months. Longitudinal studies with extended follow-up periods are needed to assess the long-term efficacy and sustainability of the interventions. Another limitation is the reliance on self-reported measures, which may introduce bias. Future research should incorporate objective measures of physical functionality and pain. Lastly, the study focused exclusively on female patients; hence, the findings may not be applicable to male fibromyalgia patients. Future research should include both genders to explore potential sex differences in response to these treatments.
4.2. Practical Applications
The findings of this study have important practical implications for the management of fibromyalgia. The significant improvements observed in respiratory and physical functionality suggest that both neuromodulation using the EXOPULSE Mollii suit and structured exercise programs can be effective non-pharmacological interventions for enhancing the quality of life in fibromyalgia patients. Clinicians can consider incorporating these interventions into multidisciplinary treatment plans to address the multifaceted symptoms of fibromyalgia. Specifically, the neuromodulation suit showed potential for improving muscle oxygenation and pain perception, while exercise programs enhanced overall physical strength and endurance. Implementing these interventions in clinical practice could help reduce reliance on pharmacological treatments, thereby minimizing potential side effects and promoting a more holistic approach to fibromyalgia management.
5. Conclusions
We can conclude that Neuromodulation and Exercise Interventions have the potential to enhance the functionality of Fibromyalgia patients as shown by the increase in FEV1/FEV6 ratio in respiratory functionality as well as the increase in FEV 1 and chest perimeter references, and physical functionality shown by the increase in performance in the Chair stand test, 10m up and go test and balance in the right leg.
Author Contributions
Conceptualization, V.J.C.-S., J.A.P. and M.D.A.-A.; methodology, V.J.C.-S., J.A.P., M.D.A.-A., A.R.-Z.; formal analysis, A.R.-Z., M.D.A.-A. and J.A.P.; investigation, A.R.-Z., M.D.A.-A. and J.A.P.; resources, V.J.C.-S., J.A.P., M.D.A.-A.; data curation, V.J.C.-S., J.A.P. and A.R.-Z.; writing—original draft preparation, V.J.C.-S., J.A.P., A.R.-Z. and J.F.T.-A.; writing— review and editing, V.J.C.-S., J.A.P., A.R.-Z. and J.F.T.-A.; visualization, V.J.C.-S., J.A.P., M.D.A.-A., A.R.-Z., and J.F.T.-A.; supervision, V.J.C.-S., J.A.P. and M.D.A.-A.; project administration, V.J.C.-S., J.A.P. and M.D.A.-A.; funding acquisition, J.A.P. and M.D.A.-A. All authors have read and agreed to the published version of the manuscript.
Funding
This work is funded by national funds through the Foundation for Science and Technology, under the project UIDP/04923/2020 and funds from the contract/convention art.83 LOU. Reference UEx083/23.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the University of Évora research ethics committee, approval nr. 22033 (31 January 2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
Data are contained within the article.
Acknowledgments
We would like to thank the undergraduate and predoctoral students who assisted during the intervention and data collection.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Bair, M.J.; Krebs, E.E. Fibromyalgia. Ann Intern Med 2020, 172, ITC33–ITC48. [Google Scholar] [CrossRef] [PubMed]
- Sarzi-Puttini, P.; Giorgi, V.; Marotto, D.; Atzeni, F. Fibromyalgia: An Update on Clinical Characteristics, Aetiopathogenesis and Treatment. Nat Rev Rheumatol 2020, 16, 645–660. [Google Scholar] [CrossRef] [PubMed]
- Branco, J.C.; Bannwarth, B.; Failde, I.; Abello Carbonell, J.; Blotman, F.; Spaeth, M.; Saraiva, F.; Nacci, F.; Thomas, E.; Caubère, J.P.; Le Lay, K.; Taieb, C.; Matucci-Cerinic, M. Prevalence of Fibromyalgia: A Survey in Five European Countries. Seminars in Arthritis and Rheumatism 2010. [Google Scholar] [CrossRef] [PubMed]
- Queiroz, L.P. Worldwide Epidemiology of Fibromyalgia Topical Collection on Fibromyalgia. Curr Pain Headache Rep 2013, 17. [Google Scholar] [CrossRef]
- Rossi, A.; Di Lollo, A.C.; Guzzo, M.P.; Giacomelli, C.; Atzeni, F.; Bazzichi, L.; Di Franco, M. Fibromyalgia and Nutrition: What News? Clinical and Experimental Rheumatology. 2015. [Google Scholar]
- Lacasse, J.R.; Leo, J. Serotonin and Depression: A Disconnect between the Advertisements and the Scientific Literature. PLoS Med 2005, 2, e392. [Google Scholar] [CrossRef]
- Overman, C.L.; Kool, M.B.; Da Silva, J.A.P.; Geenen, R. The Prevalence of Severe Fatigue in Rheumatic Diseases: An International Study. Clin Rheumatol 2016, 35. [Google Scholar] [CrossRef]
- Kleinman, L.; Mannix, S.; Arnold, L.M.; Burbridge, C.; Howard, K.; McQuarrie, K.; Pitman, V.; Resnick, M.; Roth, T.; Symonds, T. Assessment of Sleep in Patients with Fibromyalgia: Qualitative Development of the Fibromyalgia Sleep Diary. Health Qual Life Outcomes 2014, 12. [Google Scholar] [CrossRef]
- Too, L.S.; Leach, L.; Butterworth, P. Mental Health Problems and Internet Access: Results from an Australian National Household Survey. JMIR Mental Health. 2020. [Google Scholar] [CrossRef]
- Yepez, D.; Grandes, X.A.; Talanki Manjunatha, R.; Habib, S.; Sangaraju, S.L. Fibromyalgia and Depression: A Literature Review of Their Shared Aspects. Cureus 2022. [Google Scholar] [CrossRef]
- Whealy, M.; Nanda, S.; Vincent, A.; Mandrekar, J.; Cutrer, F.M. Fibromyalgia in Migraine: A Retrospective Cohort Study. Journal of Headache and Pain 2018, 19. [Google Scholar] [CrossRef] [PubMed]
- Erdrich, S.; Hawrelak, J.A.; Myers, S.P.; Harnett, J.E. A Systematic Review of the Association between Fibromyalgia and Functional Gastrointestinal Disorders. Therapeutic Advances in Gastroenterology. 2020. [Google Scholar] [CrossRef] [PubMed]
- Jones, K.D.; Maxwell, C.; Mist, S.D.; King, V.; Denman, M.A.; Gregory, W.T. Pelvic Floor and Urinary Distress in Women with Fibromyalgia. Pain Management Nursing 2015, 16. [Google Scholar] [CrossRef] [PubMed]
- Arnold, L.M.; Bennett, R.M.; Crofford, L.J.; Dean, L.E.; Clauw, D.J.; Goldenberg, D.L.; Fitzcharles, M.-A.; Paiva, E.S.; Staud, R.; Sarzi-Puttini, P.; Buskila, D.; Macfarlane, G.J. AAPT Diagnostic Criteria for Fibromyalgia. J Pain 2019, 20, 611–628. [Google Scholar] [CrossRef] [PubMed]
- Salaffi, F.; Farah, S.; Beci, G.; Schettino, M.; Carotti, M.; Di Carlo, M. Development and Validation of the Simple Fibromyalgia Screening Questionnaire for Improving the Recognition of Fibromyalgia in Daily Practice. Clin Exp Rheumatol 2020, 38. [Google Scholar]
- Villafaina, S.; Collado-Mateo, D.; Fuentes, J.P.; Rohlfs-Domínguez, P.; Gusi, N. Effects of Exergames on Brain Dynamics in Women with Fibromyalgia: A Randomized Controlled Trial. J Clin Med 2019, 8. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Zarapuz, A.; Apolo-Arenas, M.D.; Clemente-Suárez, V.J.; Costa, A.R.; Pardo-Caballero, D.; Parraca, J.A. Acute Effects of a Session with The EXOPULSE Mollii Suit in a Fibromyalgia Patient: A Case Report. Int J Environ Res Public Health 2023, 20. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Zarapuz, A.; Apolo-Arenas, M.D.; Tomas-Carus, P.; Tornero-Aguilera, J.F.; Clemente-Suárez, V.J.; Parraca, J.A. Comparative Analysis of Psychophysiological Responses in Fibromyalgia Patients: Evaluating Neuromodulation Alone, Neuromodulation Combined with Virtual Reality, and Exercise Interventions. Medicina (B Aires) 2024, 60, 404. [Google Scholar] [CrossRef]
- Rhodes, C.E.; Denault, D.; Varacallo, M. Physiology, Oxygen Transport; 2023.
- Nakazawa, M.S.; Keith, B.; Simon, M.C. Oxygen Availability and Metabolic Adaptations. Nature Reviews Cancer. 2016. [Google Scholar] [CrossRef]
- Prabhakar, N.R.; Semenza, G.L. Oxygen Sensing and Homeostasis. Physiology. 2015. [Google Scholar] [CrossRef]
- Littlejohn, G.O.; Guymer, E.K.; Ngian, G.S. Is There a Role for Opioids in the Treatment of Fibromyalgia? Pain Manag 2016, 6. [Google Scholar] [CrossRef] [PubMed]
- Macfarlane, G.J.; Kronisch, C.; Dean, L.E.; Atzeni, F.; Häuser, W.; Fluß, E.; Choy, E.; Kosek, E.; Amris, K.; Branco, J.; Dincer, F.; Leino-Arjas, P.; Longley, K.; McCarthy, G.M.; Makri, S.; Perrot, S.; Sarzi-Puttini, P.; Taylor, A.; Jones, G.T. EULAR Revised Recommendations for the Management of Fibromyalgia. Ann Rheum Dis 2017, 76, 318–328. [Google Scholar] [CrossRef] [PubMed]
- Walitt, B.; Klose, P.; Üçeyler, N.; Phillips, T.; Häuser, W. Antipsychotics for Fibromyalgia in Adults. Cochrane Database of Systematic Reviews. 2016. [Google Scholar] [CrossRef] [PubMed]
- Anaya, H.J.M.; Ortiz, M.P.T.; Valencia, D.H.F.; Ribero, O.F.G. Efficacy of Cannabinoids in Fibromyalgia: A Literature Review. Colombian Journal of Anesthesiology. 2021. [Google Scholar] [CrossRef]
- Boomershine, C.S.; Crofford, L.J. A Symptom-Based Approach to Pharmacologic Management of Fibromyalgia. Nat Rev Rheumatol 2009, 5. [Google Scholar] [CrossRef]
- Bernardy, K.; Klose, P.; Welsch, P.; Häuser, W. Efficacy, Acceptability and Safety of Cognitive Behavioural Therapies in Fibromyalgia Syndrome – A Systematic Review and Meta-Analysis of Randomized Controlled Trials. European Journal of Pain (United Kingdom) 2018. [Google Scholar] [CrossRef]
- García-Ríos, M.C.; Navarro-Ledesma, S.; Tapia-Haro, R.M.; Toledano-Moreno, S.; Casas-Barragán, A.; Correa-Rodríguez, M.; Aguilar-Ferrándiz, M.E. Effectiveness of Health Education in Patients with Fibromyalgia: A Systematic Review. European Journal of Physical and Rehabilitation Medicine. 2019. [Google Scholar] [CrossRef]
- Perrot, S.; Russell, I.J. More Ubiquitous Effects from Non-Pharmacologic than from Pharmacologic Treatments for Fibromyalgia Syndrome: A Meta-Analysis Examining Six Core Symptoms. Eur J Pain 2014, 18, 1067–1080. [Google Scholar] [CrossRef]
- Cheng, Y.C.; Hsiao, C.Y.; Su, M.I.; Chiu, C.C.; Huang, Y.C.; Huang, W.L. Treating Fibromyalgia with Electrical Neuromodulation: A Systematic Review and Meta-Analysis. Clinical Neurophysiology 2023, 148. [Google Scholar] [CrossRef]
- Riachi, N.; Chalah, M.A.; Ahdab, R.; Arshad, F.; Ayache, S.S. Effects of the TENS Device, Exopulse Mollii Suit, on Pain Related to Fibromyalgia: An Open-Label Study. Neurophysiologie Clinique 2023, 53. [Google Scholar] [CrossRef]
- Rodríguez-Mansilla, J.; Mejías-Gil, A.; Garrido-Ardila, E.M.; Jiménez-Palomares, M.; Montanero-Fernández, J.; González-López-Arza, M.V. Effects of an Exercise for Well-Being and Physical Training Programme on Muscle Strength, Range of Movement, Respiratory Capacity and Quality of Life in Women with Fibromyalgia: A Randomized Controlled Trial. J Clin Med 2023, 12. [Google Scholar] [CrossRef] [PubMed]
- Besnier, F.; Labrunée, M.; Pathak, A.; Pavy-Le Traon, A.; Galès, C.; Sénard, J.M.; Guiraud, T. Exercise Training-Induced Modification in Autonomic Nervous System: An Update for Cardiac Patients. Annals of Physical and Rehabilitation Medicine. 2017. [Google Scholar] [CrossRef] [PubMed]
- Ballesta-García, I.; Martínez-González-moro, I.; Rubio-Arias, J.; Carrasco-Poyatos, M. High-Intensity Interval Circuit Training versus Moderate-Intensity Continuous Training on Functional Ability and Body Mass Index in Middle-Aged and Older Women: A Randomized Controlled Trial. Int J Environ Res Public Health 2019, 16. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Zarapuz, A.; Apolo-Arenas, M.D.; Tornero-Aguilera, J.F.; Parraca, J.A.; Clemente-Suárez, V.J. Comparative Efficacy of Neuromodulation and Structured Exercise Program on Pain and Muscle Oxygenation in Fibromyalgia Patients: A Randomized Crossover Study. Front Physiol 2024, 15. [Google Scholar] [CrossRef] [PubMed]
- Haß, U.; Herpich, C.; Norman, K. Anti-Inflammatory Diets and Fatigue. Nutrients. 2019. [Google Scholar] [CrossRef] [PubMed]
- Roman, P.; Estévez, A.F.; Miras, A.; Sánchez-Labraca, N.; Cañadas, F.; Vivas, A.B.; Cardona, D. A Pilot Randomized Controlled Trial to Explore Cognitive and Emotional Effects of Probiotics in Fibromyalgia. Sci Rep 2018, 8. [Google Scholar] [CrossRef]
- Rubio-Zarapuz, A.; Apolo-Arenas, M.D.; Fernandes, O.; Tornero-Aguilera, J.F.; Clemente-Suárez, V.J.; Parraca, J.A. Comparative Efficacy of Neuromodulation and Structured Exercise Program on Autonomic Modulation in Fibromyalgia Patients: Pilot Study. J Clin Med 2024, 13, 4288. [Google Scholar] [CrossRef]
- Jamison, R.N.; Edwards, R.R.; Curran, S.; Wan, L.; Ross, E.L.; Gilligan, C.J.; Gozani, S.N. Effects of Wearable Transcutaneous Electrical Nerve Stimulation on Fibromyalgia: A Randomized Controlled Trial. J Pain Res 2021, 14. [Google Scholar] [CrossRef]
- Izquierdo-Alventosa, R.; Inglés, M.; Cortés-Amador, S.; Gimeno-Mallench, L.; Sempere-Rubio, N.; Serra-Añó, P. Effectiveness of High-Frequency Transcranial Magnetic Stimulation and Physical Exercise in Women with Fibromyalgia: A Randomized Controlled Trial. Phys Ther 2021, 101. [Google Scholar] [CrossRef]
- Baeken, C.; Vanderhasselt, M.A.; Remue, J.; Herremans, S.; Vanderbruggen, N.; Zeeuws, D.; Santermans, L.; De Raedt, R. Intensive HF-RTMS Treatment in Refractory Medication-Resistant Unipolar Depressed Patients. J Affect Disord 2013, 151. [Google Scholar] [CrossRef]
- Muthulingam, J.A.; Hansen, T.M.; Olesen, S.S.; Drewes, A.M.; Frøkjær, J.B. Two-Week Cervical Vagus Nerve Stimulation in Chronic Pancreatitis Patients Induces Functional Connectivity Changes of Limbic Structures. Neuromodulation 2022, 25. [Google Scholar] [CrossRef] [PubMed]
- Pennati, G.V.; Bergling, H.; Carment, L.; Borg, J.; Lindberg, P.G.; Palmcrantz, S. Effects of 60 Min Electrostimulation With the EXOPULSE Mollii Suit on Objective Signs of Spasticity. Front Neurol 2021, 12, 706610. [Google Scholar] [CrossRef] [PubMed]
- Raffalt, P.C.; Bencke, J.; Mortensen, K.; Torabi, T.P.; Wong, C.; Speedtsberg, M.B. Electro-Suit Treatment of Children with Unilateral Cerebral Palsy Alters Nonlinear Dynamics of Walking. Clinical Biomechanics 2022, 98, 105714. [Google Scholar] [CrossRef] [PubMed]
- Meier, T.; Rummey, C.; Leinonen, M.; Voit, T.; Schara, U.; Straathof, C.; D’Angelo, M.; Bernert, G.; Cuisset, J.-M.; Finkel, R.; Goemans, N.; McDonald, C.; Buyse, G. The Use of a Hand-Held Device (ASMA-1) for Home-Based Monitoring of Respiratory Function Changes in Pediatric and Adolescent Patients with Duchenne Muscular Dystrophy. Neuromuscular Disorders 2015, 25, S201. [Google Scholar] [CrossRef]
- Sener, U.; Ucok, K.; Ulasli, A.M.; Genc, A.; Karabacak, H.; Coban, N.F.; Simsek, H.; Cevik, H. Evaluation of Health-Related Physical Fitness Parameters and Association Analysis with Depression, Anxiety, and Quality of Life in Patients with Fibromyalgia. Int J Rheum Dis 2016, 19, 763–772. [Google Scholar] [CrossRef]
- Forti, M.; Zamunér, A.R.; Andrade, C.P.; Silva, E. Lung Function, Respiratory Muscle Strength, and Thoracoabdominal Mobility in Women With Fibromyalgia Syndrome. Respir Care 2016, 61, 1384–1390. [Google Scholar] [CrossRef]
- Jonsson, K.; Peterson, M. Peak Expiratory Flow Rate and Thoracic Mobility in People with Fibromyalgia. A Cross Sectional Study. Scand J Pain 2019, 19. [Google Scholar] [CrossRef]
- Padkao, T.; Boonla, O. Relationships between Respiratory Muscle Strength, Chest Wall Expansion, and Functional Capacity in Healthy Nonsmokers. J Exerc Rehabil 2020, 16. [Google Scholar] [CrossRef]
- Carbonell-Baeza, A.; Álvarez-Gallardo, I.C.; Segura-Jiménez, V.; Castro-Piñero, J.; Ruiz, J.R.; Delgado-Fernández, M.; Aparicio, V.A. Reliability and Feasibility of Physical Fitness Tests in Female Fibromyalgia Patients. Int J Sports Med 2015, 36, 157–162. [Google Scholar] [CrossRef]
Figure 1.
Experimental Crossover Design.
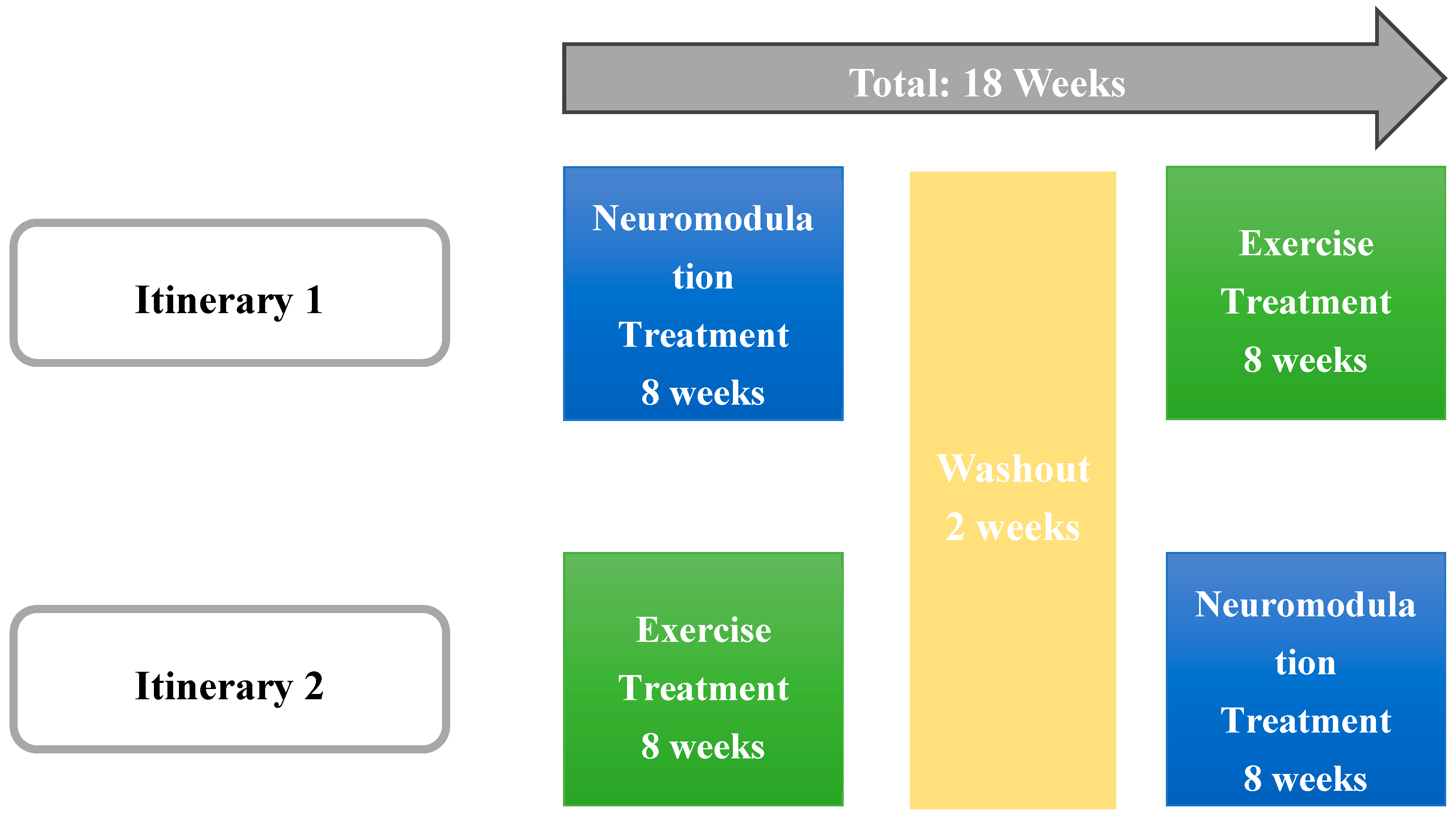
Table 2.
One-way ANOVA results.
| Variables | Suit | Exercise | ||
| Pre (p) | Post (p) | Pre (p) | Post (p) | |
| FEV 1, L | 0.926 | 0.082 | 0.895 | 0.347 |
| FEV 1, % | 0.969 | 0.124 | 0.895 | 0.562 |
| FEV 6, L | 0.926 | 0.584 | 0.49 | 1 |
| FEV 6, % | 0.971 | 0.391 | 0.625 | 0.889 |
| FEV 1/FEV 6, n | 0.905 | 0.045* | 0.717 | 0.121 |
| FEV 1/FEV 6, % | 0.581 | 0.1 | 0.405 | 0.093 |
| Chest perimeter difference, cm | 0.402 | 0.318 | 0.035* | 0.326 |
| Handgrip strength test, kg | 0.767 | 0.202 | 0.641 | 0.459 |
| Chair stand test, n | 0.005* | <.001* | 0.002* | 0.006* |
| 10 m up and go test, s | 0.007* | 0.273 | 0.117 | 0.045* |
| One leg balance right, s | 0.301 | 0.273 | 0.459 | 0.895 |
| One leg balance left, s | 0.264 | 0.0025* | 0.882 | 0.135 |
* Table presents one-way ANOVA test results. *p<0.05. FEV1: forced expiratory volume in 1 s. FEV6: forced expiratory volume in 6 s.
Table 3.
Comparative statistics between treatments.
| Variables | Pre 1st session | Post 1st session | Pre 8th session | Post 8th session | Pre 16th session | Post 16th session | ||||||
| p | ε² | p | ε² | p | ε² | p | ε² | p | ε² | p | ε² | |
| FEV 1, L | 0.762 | 0.005 | 0.545 | 0.019 | 0.88 | 0.001 | 0.821 | 0.003 | 0.775 | 0.005 | 0.235 | 0.078 |
| FEV 1, % | 0.513 | 0.024 | 0.19 | 0.095 | 0.85 | 0.002 | 0.91 | 0.001 | 0.838 | 0.002 | 0.165 | 0.107 |
| FEV 6, L | 1 | 0.000 | 0.88 | 0.001 | 0.791 | 0.004 | 0.88 | 0.001 | 0.838 | 0.002 | 0.713 | 0.008 |
| FEV 6, % | 0.683 | 0.009 | 0.513 | 0.024 | 0.734 | 0.006 | 0.545 | 0.019 | 0.902 | 0.001 | 0.623 | 0.013 |
| FEV 1/FEV 6, n | 0.406 | 0.036 | 0.034* | 0.236 | 0.151 | 0.109 | 0.199 | 0.087 | 0.683 | 0.009 | 0.288 | 0.063 |
| FEV 1/FEV 6, % | 0.437 | 0.034 | 0.083 | 0.167 | 0.363 | 0.043 | 0.79 | 0.004 | 0.902 | 0.001 | 0.461 | 0.030 |
| Chest perimeter difference, cm | 0.591 | 0.015 | 1 | 0.000 | 0.117 | 0.129 | 0.393 | 0.038 | 0.385 | 0.042 | 0.385 | 0.042 |
| Handgrip strength test, kg | 0.88 | 0.001 | 0.406 | 0.036 | 0.762 | 0.005 | 0.82 | 0.003 | 0.93 | 0.000 | 0.967 | 0.000 |
| Chair stand test, n | 0.733 | 0.006 | 0.939 | 0.000 | 0.88 | 0.001 | 0.82 | 0.003 | 0.87 | 0.001 | 0.713 | 0.008 |
| 10 m up and go test, s | 0.597 | 0.015 | 0.597 | 0.015 | 0.406 | 0.036 | 0.597 | 0.015 | 0.744 | 0.006 | 0.165 | 0.107 |
| One leg balance right, s | 0.326 | 0.051 | 0.199 | 0.087 | 0.65 | 0.011 | 0.762 | 0.005 | 0.624 | 0.013 | 0.744 | 0.006 |
| One leg balance left, s | 0.597 | 0.015 | 0.226 | 0.077 | 0.757 | 0.006 | 0.683 | 0.009 | 1 | 0.000 | 0.935 | 0.000 |
* Table presents comparisons between both treatments for each measurement. *p<0.05. FEV1: forced expiratory volume in 1 s. FEV6: forced expiratory volume in 6 s.
Table 4.
Intrasession Comparative Statistics.
| Variables | Suit | Exercise | ||||
| 1st session | 8th session | 16th session | 1st session | 8th session | 16th session | |
| Effect Size | Effect Size | Effect Size | Effect Size | Effect Size | Effect Size | |
| FEV 1, L | -0.365 | -0.024 | 0.570 | 0.798* | -0.376 | -0.6608 |
| FEV 1, % | -0.280 | -0.074 | 0.614 | 0.755* | -0.337 | -0.489 |
| FEV 6, L | -0.032 | -0.145 | 0.281 | 0.596 | 0.097 | -0.319 |
| FEV 6, % | -0.257 | -0.164 | 0.273 | 0.5546 | 0.087 | -0.298 |
| FEV 1/FEV 6, n | -0.241 | 0.046 | 1.021* | 0.217 | -0.501 | -0.919* |
| FEV 1/FEV 6, % | -0.175 | -0.017 | 0.813* | 0.139 | -0.500 | -0.970* |
| Chest perimeter difference, cm | 0.184 | 0.111 | 0.444 | 0.559 | 0.106 | 0.467 |
| Handgrip strength test, kg | -0.152 | 0.858* | 0.402 | 0.234 | 0.473 | 0.342 |
| Chair stand test, n | 0.650 | 0.628 | 0.917* | 0.425 | 0.515 | 0.577 |
| 10 m up and go test, s | -0.746* | -0.527 | -0.055 | -0.400 | -0.182 | -0.556 |
| One leg balance right, s | -0.127 | 0.127 | 0.200 | 0.309 | -0.127 | 0.200 |
| One leg balance left, s | 0.442 | 0.200 | -0.200 | 0.673 | 0.883* | -0.600 |
* Table presents t-test results comparing baseline and post-session measurement for each session and treatment. *p<0.05. FEV1: forced expiratory volume in 1 s. FEV6: forced expiratory volume in 6 s.
Table 5.
Neuromodulation Intersession Comparative Statistics.
| Variables | 1st vs 8th pre session | 8th vs 16th pre session | 1st vs 16th pre session | 1st vs 8th post session | 8th vs 16th post session | 1st vs 16th post session | 1st pre vs 8th post session | 1st pre vs 16th post session | 8th pre vs 16th post session |
| Effect Size | Effect Size | Effect Size | Effect Size | Effect Size | Effect Size | Effect Size | Effect Size | Effect Size | |
| FEV 1, L | -0.0361 | -0.0717 | -0.126 | -0.388 | -0.413 | -0.851* | -0.00798 | -0.471 | -0.361 |
| FEV 1, % | -0.203 | -0.0534 | -0.124 | -0.198 | -0.442 | -0.902* | -0.0673 | -0.462 | -0.407 |
| FEV 6, L | 0.0103 | 0.0797 | 0.0743 | -0.00512 | -0.344 | -0.248 | 0.165 | -0.233 | -0.147 |
| FEV 6, % | 0.0759 | 0 | 0.121 | 0.393 | -0.4 | -0.343 | 0.356 | -0.177 | -0.191 |
| FEV 1/FEV 6, n | -0.208 | -0.0195 | -0.257 | -0.834* | -0.273 | -1.01* | -0.255 | -0.458 | -0.268 |
| FEV 1/FEV 6, % | -0.417 | 0.0831 | -0.272 | -0.816* | -0.22 | -0.934* | -0.342 | -0.419 | -0.146 |
| Chest perimeter difference, cm | 0.139 | -0.75 | -0.422 | -0.111 | -0.778 | -0.529 | -0.0556 | -0.522 | -0.86* |
| Handgrip strength test, kg | -0.0689 | 0.246 | 0.147 | -0.848* | 0.286 | -0.229 | -0.54 | -0.0486 | -0.012 |
| Chair stand test, n | -0.973* | -0.889* | -0.945* | -0.863* | -1.48* | -1.28* | -1.1* | -1.38* | -1.47* |
| 10 m up and go test, s | 1* | 0.236 | 0.6 | 0.673 | -0.164 | 0.345 | 1* | 0.573 | 0.145 |
| One leg balance right, s | -0.402 | -0.6 | -0.636 | -0.273 | -0.345 | -0.747* | -0.564 | -0.745* | -0.66 |
| One leg balance left, s | -0.364 | -0.0222 | -0.527 | -0.636 | 0.455 | -0.0182 | -0.481 | -0.127 | -0.093 |
* Table presents t-test results comparing baseline and post-session measurements between different sessions in the neuromodulation treatment. *p<0.05. FEV1: forced expiratory volume in 1 s. FEV6: forced expiratory volume in 6 s.
Table 6.
Exercise Intersession Comparative Statistics.
| 1st vs 8th pre session | 8th vs 16th pre session | 1st vs 16th pre session | 1st vs 8th post session | 8th vs 16th post session | 1st vs 16th post session | 1st pre vs 8th post session | 1st pre vs 16th post session | 8th pre vs 16th post session | |
| Effect Size | Effect Size | Effect Size | Effect Size | Effect Size | Effect Size | Effect Size | Effect Size | Effect Size | |
| FEV 1, L | -0.0765 | -0.107 | -0.128 | 0.537 | 0.17 | 0.582 | 0.111 | 0.266 | 0.299 |
| FEV 1, % | -0.031 | -0.172 | -0.172 | 0.499 | -0.111 | 0.5 | 0.121 | 0.156 | 0.056 |
| FEV 6, L | 0.211 | -0.554 | -0.213 | 0.415 | -0.211 | 0.302 | 0.148 | -0.005 | -0.35 |
| FEV 6, % | 0.198 | -0.537 | -0.252 | 0.414 | -0.309 | 0.211 | 0.16 | -0.071 | -0.395 |
| FEV 1/FEV 6, n | -0.839* | 0.732 | 0.223 | 0.0899 | 0.689 | 0.662 | -0.135 | 0.709 | 1* |
| FEV 1/FEV 6, % | -0.738* | 0.698 | 0.295 | -0.127 | 0.678 | 0.786 | -0.035 | 0.776* | 0.998* |
| Chest perimeter difference, cm | -0.789* | 0.395 | -0.434 | -0.65* | 0.077 | -0.36 | -1,28* | -1.03* | 0.095 |
| Handgrip strength test, kg | 0.0505 | -0.145 | -0.037 | 0.0208 | -0.08 | -0.091 | -0.267 | -0.186 | -0.368 |
| Chair stand test, n | -0.692 | -0.62 | -1.35* | -0.683* | -0.84* | -1.06* | -1.28* | -1.36* | -0.664 |
| 10 m up and go test, s | 0.673 | -0.0556 | 0.583 | 0.6 | 0.378 | 0.733 | 0.673 | 0.867* | 0.378 |
| One leg balance right, s | -0.345 | 0.6 | -0.111 | -0.018 | -0.067 | 0.216 | -0.091 | -0.2 | 0.022 |
| One leg balance left, s | 0.609 | -0.333 | -0.378 | 0.6 | 0.5 | 0.511 | -0.1 | 0.333 | 0.167 |
*Table presents t-test results comparing baseline and post-session measurements between different sessions in the exercise treatment. *p<0.05. FEV1: forced expiratory volume in 1 s. FEV6: forced expiratory volume in 6 s.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



