
Submitted:
29 November 2024
Posted:
02 December 2024
You are already at the latest version
Abstract
Exploring the cultural dimensions of addiction and recovery among marginalized populations presents significant challenges due to their “hard-to-reach” status and the complexity of measuring “culture.” This paper addresses these challenges by introducing and applying cultural domain analysis, a versatile method for systematically measuring cultural concepts within marginalized groups. Specifically, we use this approach to examine cultural models of addiction. The study was conducted in London, Toronto, and Delhi among reproductive-aged women receiving treatment for substance use disorders. Participants completed a semi-structured questionnaire featuring open-ended and free-list prompts. Findings revealed culturally specific themes at each site, highlighting insights often overlooked by purely quantitative methods. The analysis also uncovered cross-site similarities, such as the role of peer networks in recovery in both India and Toronto. When applied to hybrid data, these results demonstrate how cultural domain analysis provides a structured yet adaptable framework for identifying cultural differences and shared patterns. In conclusion, working with hard-to-reach populations necessitates flexible research methods that authentically amplify participants’ voices while maintaining methodological rigor. Cultural domain analysis achieves this balance, offering a systematic approach to capturing the salience of participants’ perspectives.
Keywords:
culture
; substance use disorders
; hard-to-reach populations
; free-listing
; cultural domains
Introduction
Exploring the cultural dimensions of addiction and recovery among marginalized populations poses significant challenges. The concept of “culture” itself has been widely debated, both within anthropology (Boyd and Richerson 1988; Kleinman and Benson 2006; White 1959) and beyond, particularly in discussions of cultural competence in substance use research and clinical practice (De Kock 2020; Kleinman and Benson 2006; Placek and Wies n.d.). Furthermore, recruiting participants from marginalized populations is challenging due to social (e.g., stigma and discrimination, a history of medical and scientific exploitation), practical (e.g., investment of time, competing responsibilities like work and caregiving), and geographical barriers (e.g., transportation), limiting sample sizes and hindering meaningful findings (Nasser et al., 2011; Placek et al. 2021; Shaghaghi et al., 2011). Nonetheless, examining the role of culture in substance use among these underrepresented groups is essential for developing more equitable and culturally attuned recovery options (Placek and Wies, n.d.).
This paper outlines a process for measuring the cultural domains of recovery among women in recovery from substance use disorders (SUDs), a group that is frequently underrepresented in substance use research (Placek et al. 2021). Women who struggle with drug addiction face several barriers to research participation, including stigma from communities and healthcare institutions, gender biases that emphasize research on men’s substance use, and cultural norms that limit their ability to disclose use (Brady and Randall 1999; Degenhardt et al. 2014; Slabbert et al. 2020; Tuchman 2010). Given the multiple sociocultural barriers preventing women from joining research studies, flexible methodological approaches are needed to document their lived experiences with SUDs and recovery (Placek et al. 2021).
In this study, culture is defined as “shared knowledge and practices that are transmitted non-biologically from generation to generation. It is symbolic, historic, and integrated, shaping how we perceive and respond to the world around us” (Hewlett 2024). Cultural domains, or specific elements of culture, are often measured using free lists and analyzed through salience analysis (Placek et al. 2023; Quinlan 2005). Free-listing is a semi-quantitative method in which participants are asked to list items related to a particular topic, such as “causes of addiction,” to capture collective cultural constructs (Quinlan, 2005; Romney & D’Andrade, 1964; Smith & Borgatti, 1997). Several features highlight the cultural relevance of free-lists: the length of a list typically reflects a participant’s familiarity with the topic, with longer lists indicating greater knowledge (Borgatti, 1998; Gatewood, 1984). Participants also tend to prioritize items based on relevance and familiarity (Quinlan, 2005; Romney & D’Andrade, 1964), while omitted items often reflect a lack of contextual relevance (Quinlan, 2005). Additionally, items listed early tend to recur across other lists within the same cohort, making free-listing a valuable tool for capturing cultural information.
Combining free-listing with open-ended responses provides a richer understanding of cultural domains in marginalized, hard-to-reach populations. This approach helps identify key themes and offers detailed insights into their meanings and significance. This study applies this hybrid method by asking participants to list perceptions of addiction (both their perceptions of addiction as well as those espoused within their community), with opportunities to expand on their reasoning, which enriches the contextual understanding of relevant cultural domains. We refer to this combined approach as “cultural domain analysis,” as it integrates free-listing with open-ended responses and can be adapted to fit the unique needs and characteristics of the population.
Materials and Methods
Data for this study were collected at different times in Toronto, Delhi, and London, regions chosen for their rising rates of substance misuse, particularly opioids including heroin and fentanyl (Avashti and Ghosh 2019; Pierce et al. 2021). The study received approval from Ball State University's Institutional Review Board on 07/28/2023 (#2068016), the Ethics Committee at the Indian Spinal Injuries Centre, and Brunel University’s College of Health, Medicine, and Life Sciences Research Ethics Committee. Data collection in Delhi occurred from 2020 to 2021, while in Toronto it took place from October to December 2023, and in London from January to March 2024.
Participants were initially recruited through directors of treatment centers, who were asked to share study information with eligible individuals. Due to COVID-19 restrictions in Delhi, interviews were conducted primarily online or by phone. For participants in Toronto and London, data collection took place in person or over the phone with women aged 18 and older. The inclusion criteria specified women aged 18 or older who were receiving treatment for a substance use disorder, with a focus on mothers in Toronto and London to explore their recovery experiences. Interviews lasted between 20 and 60 minutes.
Participants responded to open-ended questions covering various topics related to substance addiction and recovery, including the causes of addiction, recovery experiences, harm reduction, community perceptions of mothers who use substances, and barriers mothers face in accessing addiction treatment. All interviews were audio-recorded, and transcribed, and participants received compensation per local norms. This study specifically reports on participants' perceptions regarding the causes of addiction.
Analysis
Data generated from the interviews were a mix of open-ended responses and free-lists. Each transcript initially underwent two iterations of coding; in the first iteration, the theme, "causes of addiction" was identified for questions associated with addiction causes. For the second iteration of coding, the first author recorded sections labeled "causes of addiction" to inductively identify more specific themes associated with perceived causes of addiction, such as "psychological," "interpersonal factors," and "genetics.” Next, themes for causes of addiction were identified in each excerpt in the order they were mentioned, which allowed for the computation of salience analysis (Placek et al. 2023; Quinlan 2005). Themes were recorded for consistency across participants. For example, when asked to free-list the causes of addiction, one participant in Delhi responded:
"Stress; Capability of not coping up with what’s going on around you."
The themes "stress," and "coping" emerged from this excerpt and were placed in a file with participant IDs in the first column, and themes across subsequent columns in the order participants mentioned them (e.g. Column B= “stress” and Column C= “coping”). Then, a salience score was computed for each of the causes of addiction according to order and frequency of mention. Salience analysis is a method used to identify the main items in a domain by computing a score for each item that reflects both the frequency and order of mention (Placek et al. 2023; Quinlan 2005; Weller and Romney 1998). The cut-off for salience in each population is determined by a Smith’s S score of > 0.10 (Purzycki et al. 2018). Below are results with a Smith’s S score > 0.10 across each time point. Data were analyzed using salience analysis with AnthroTools package in R.
Results
A total n=49 women in Delhi, n= 31 women in Toronto, and n= 10 women in London completed the in-depth interview which consisted of free-list prompts and open-ended questions. Of the Canadian participants, 20 were women in recovery and 16 were women who worked at recovery and harm reduction centers but had a past history of substance misuse. Respondents in London and Delhi were all in recovery at treatment centers that ranged from non-residential, drop-in services to residential programs. The average age of women in Delhi was 23.9 (range = 18 to 41), in Toronto, 41.6 (range = 26 to 62), and in London, 42.11 (range = 35 to 52).
The three regions overlapped yet varied in the types of drugs that women reported using. In Delhi, the drugs of choice were cannabis, heroin, and hash. In Toronto, the drugs of choice were alcohol, cannabis, methamphetamine, fentanyl, heroin, benzodiazepines, psilocybin, and crack. In London, the substances included alcohol, cannabis, heroin, cocaine, crack, ecstasy/MDMA, and spice.
- What causes addiction?
- Delhi
In Delhi, the salient perceived causes of addiction for women in treatment were: pleasure (Smith's S= 0.20), stress/tension (Smith's S= 0.19), loneliness (Smith's S= 0.18), habit (Smith's S= 0.16), and peers (Smith's S= 0.10; Figure 1). The excerpts illuminate the complexity of perceived causes of addiction and showcase why cultural domain analysis is a useful tool because it accounts for in-depth responses as well as the frequency and order of mention of a term, which act as an index for the prominence of a given idea or concept within a particular cultural context.
Pleasure (Smith’s S= 0.20) was associated with partying and having fun. For example, one participant, Selma1, described addiction as grounded in pleasure and withdrawal avoidance, “They feel nice and relaxed after doing it, and then when they don’t use it then they feel some pain in their body so they keep using.” Other participants combined pleasure with other feelings; Aayana said, “ 30-40% start because of fun, but then 60% are those in emotional need and support, and then they select the wrong path and eventually get addicted. Max, a person can use for 2 years unless they are rich because after that you get short on money and you get addicted as well so it's a whole spiral situation.” Overall, participants believed that addiction was caused, at least in part, by a desire to feel pleasure and avoid pain.
Stress/tension (Smith’s S= 0.19) was also often mentioned as a cause of addiction and was typically a stand-alone cause. For example, Saanvi said, “By overdoing it. Tensions.” Another participant, Aditi, said, “Because of tension and stress, then you take drugs and you feel de-stressed and then it becomes a habit.” In this example, Aditi acknowledges that habit is a secondary cause of addiction, but is dependent on first the experience of stress. Similarly, another participant, Divya, stated, “Tensions. I had family tensions and I stopped going to school as well.”
Loneliness (Smith’s S = 0.18) was associated with isolation, the death of someone close, separations, break-ups, and divorces; for example, Noor said, “Well, I got addicted due to loneliness, then there was my friend circle.” Another participant, Amya, mentioned loneliness first and then stress, or tension, as a secondary cause: “I think, lack of attention and constant tension.” Similarly, Jiya mentioned, “Everybody has their issues, some people are sad, or alone and that's why they do it.” Within these two cultural domains (stress and loneliness), we can see that substance use as a tool to manage psychological discomfort (caused by a variety of contextual and interpersonal processes), is viewed as precipitating addiction.
Habit (Smith’s S= 0.16) was associated with frequent use of a substance. This is summarized by Amara who said, “When you take it once, and it becomes a habit then it becomes an addiction, it becomes a need, you require it every day to feel what you felt in the first place.” Similarly, Devika said, “Maybe because of regular usage.” As such, frequent use is viewed as a risk for developing unhealthy and addictive patterns of (mis)use.
Peers (Smith’s S= 0.10) was a theme mentioned about friends and acquaintances who introduced the participants to drugs. When Aashvi was asked about the cause of addiction, she said “I think it was because of my friend group.” Peers, however, were not the highest in salience, as is evident from Smith’s S scores. As a result, it was often mentioned after other causes had been highlighted. A good example is from Aachal who said, “I think people who get addicted are the cause of their addiction. They make reasons for themselves to get addicted like break up or divorce or family stress. People find reasons to take drugs. They also get influenced by people around them and what they see around them. Some people want to explore new options. This is what happened with me also.” Overall, participants saw peers (and interpersonal influences) as a key contributor to addiction, but initially placed responsibility at the feet of the individual, attributing their initial patterns of frequent or habitual use to a desire to feel pleasure, avoid pain, or otherwise manage difficult situations or emotions.
- Toronto
In Toronto, the salient terms for the Canadian sample included trauma (Smith’s S= 0.41), mental health (Smith’s S= 0.20), childhood (Smith’s S= 0.14), family (Smith’s S= 0.13), abuse (Smith’s S= 0.12) and peers (Smith’s S= 0.11; Figure 2). The Canadian responses describing addiction were a combination of open responses and lists with many themes overlapping in the same response.
Trauma (Smith’s S= 0.41): According to Jessica, addiction is caused by “Depression, trauma. I feel like if it runs in your family bloodline, that helps. Your brain has a big part of it. Impulse. You have more sporadic impulses medically in your brain. I've learned that. Just different personalities. Like I said, lack of understanding it and boredom.” Others felt that trauma was the sole cause. For example, Maria stated, “I think that addiction is a symptom of trauma.” She then went on to say, “I mean, I guess it could also be like brain chemistry. But most of the time, I feel like it's unresolved trauma or untreated mental health.” Here, we can see that participants perceive addiction as a consequence of the use, and eventual misuse, of substances to manage the psychological/emotional consequences of trauma history. This may be exacerbated by the presence of neurochemical or dispositional vulnerabilities, but the element of trauma is seen as essential.
Mental health (Smith’s S= 0.20): Mental health issues were often mentioned as a secondary cause of addiction. Anna is an example of this. She said,
“So, I think it's just the unreal expectations that society has toward women, especially mothers, and like to be the perfect mother to look perfect to have a job plus, do all the things for your children, like extracurricular activities, to juggle that perfect life. And then, you know, when you have mental health issues like that, that are also, you know, it also I just, I think mental health, causes you to have like, especially like postpartum depression or something like that.”
Similarly, Diana stated,
“Oh, that's a real open-ended question. It could be anything from childhood trauma, abuse, mental illness. It could be physical pain from accidents. It could be homelessness or home insecurity. It could be just neglect in general. All of those. There may be even more. It could be systematic racial problems that they've faced or economic problems. A lot of it is all integrated. I don't think there's one or the-- I don't find one is without another. I think that they're all somehow intertwined.”
Overall, addiction was perceived to be caused by various external stressors (e.g., social expectations, trauma, financial/housing insecurity, discrimination) when combined with individual vulnerabilities, specifically mental illness.
Childhood (Smith’s S= 0.14): Childhood was often mentioned in the middle or toward the end of a list or excerpt, but was mentioned frequently by participants. For example, Emily gave a long response regarding what she thinks causes addiction, and childhood appeared toward the end of her statement:
“Oh, what do we think causes it? You know, I'm not really of the opinion that you have to have some sort of like, trauma, to end up a drug user. You know, I think even just something so simple as bad choices can put you in a situation where you're doing a drug that you have to do every day, even though that's not something that you ever thought you would end up doing, you know, what I think causes it, you know, being a kid being dumb, you know, going out, being with different people, you know, everything could put you in a situation where you're, you know, maybe going to do drugs where you normally wouldn't? What makes you end up a habitual drug user? I think choosing the wrong drug too many times.
Um, I think for some people, you know, maybe they have a really shitty upbringing, and, you know, or they're living on the street. And these would be all good reasons to want to be high every day all day long. And I don't think it's like that for everybody. I think some people really are just functioning addicts. Yeah, sort of late getting high on their time off and they've picked something that you know, maybe it wasn't a good pick.”
In this cultural context, childhood is perceived as contributing to addiction through both external (e.g., traumatic, unstable, and/or neglectful environments) and internal (e.g., being naive, lack of understanding, impulsivity) processes.
Family (Smith’s S= 0.13): Esther combined the themes of family and peers, but this excerpt showcases how family was more salient: “I think a lot of it has to do with your upbringing…Falling into the wrong crowd. If you say, for example, move to another country, city, or neighborhood, you fall into the wrong hands.” Annika also mentioned family as a salient cause of addiction,
“Well, yes, I mean, it starts as you know, like, you just don't even think that because you grow up having it around, or people do or for me, personally, but it's always around, and you don't realize that you use it when you're, you know, I'm also a smoker. So I was reading, you know, a cigarette, you can use when you're happy when you're sad when you're mad like it. It's the cure for everything.”
Abuse (Smith’s S= 0.12): Abuse was another salient cause of addiction. According to Leah, addiction is caused by “Grief, being abused, not feeling accepted, being different.” Similarly, Carla mentioned abuse as an important cause of addiction: “I think it comes from trauma and abusive relationships as well. Bad relationships with your parents feeling like you're an outcast.” Within these two cultural domains (family and abuse), we can see that participants view familial relationships as playing a critical role in addictive processes, through the modeling of substance use and misuse as well as the application of trauma and stress (e.g., abuse, neglect).
Peers (Smith’s S= 0.11): Emily, whose excerpt is included in the childhood section, mentioned peers as an influence, “…you know, being a kid being dumb, you know, going out, being with different people, you know, everything could put you in a situation where you're, you know, maybe going to do drugs where you normally wouldn't?” In other cases, peers were mentioned as a primary cause. According to Anora, “People that are in your circle, and then the way you grew up, and what you see when you grow up. Trauma.” Overall, peers were seen to contribute to addiction through the modeling and normalization of substance use and misuse. Childhood was described as a critical period for this kind of social influence.
- London
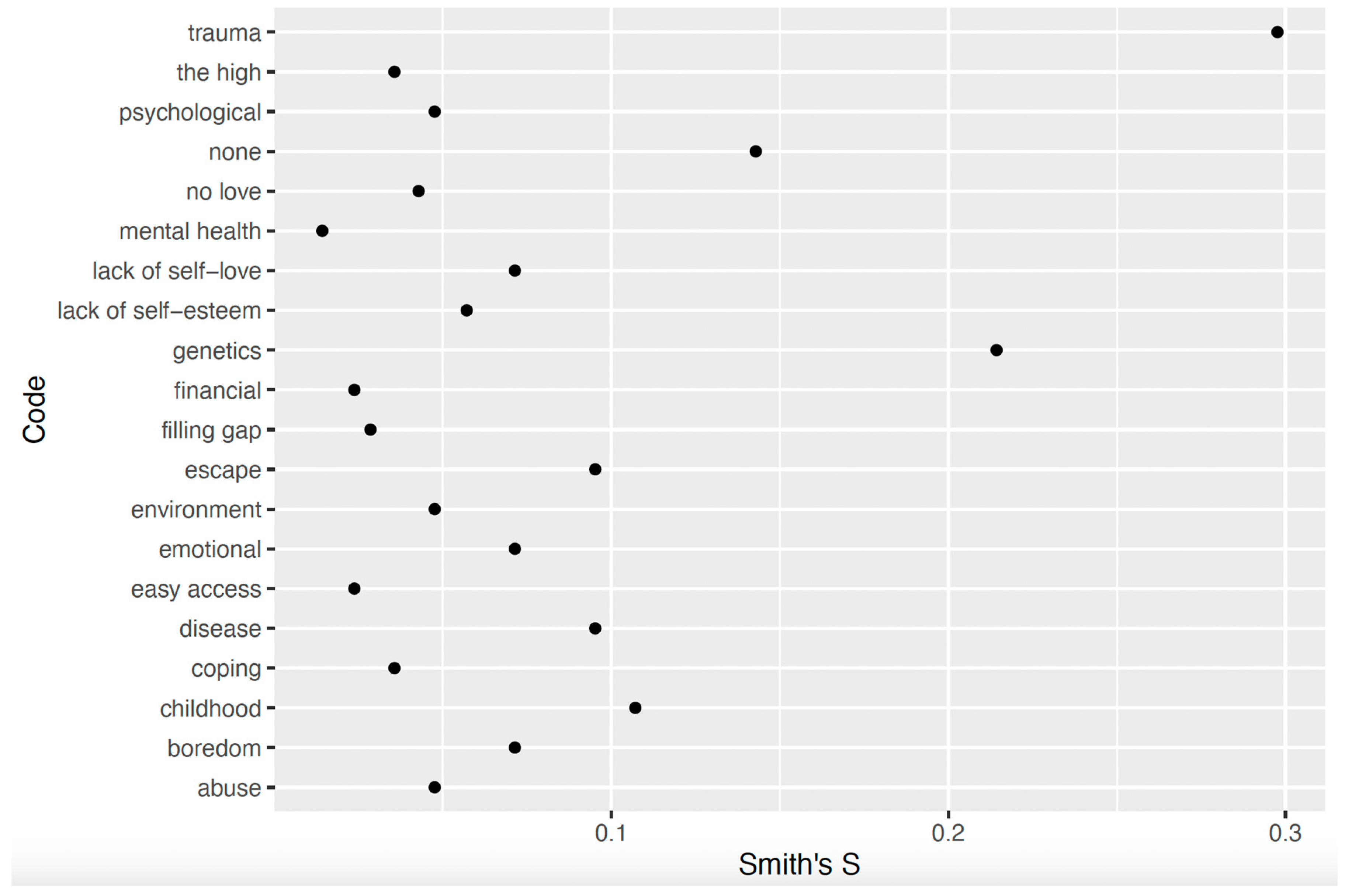
The salient terms for the London sample included trauma (Smith’s S= 0.30), genetics (Smith’s S= 0.21), childhood (Smith’s S= 0.11), and none (Smith’s S= 0.14). Figure 3 displays the Smith’s S scores.
Trauma (Smith’s S= 0.30): Trauma was mentioned early in participants’ lists and often. For example, Elizabeth mentioned trauma first:
“In my opinion, trauma, behaviors copied, learned from what you witness as a child, especially around the age of seven to eight when you're more likely to remember your life. I know for me it is the type of counseling I did and rehabilitation that I was in and what I've learned about myself, I was able to change some behaviors and recognize that and change those.”
For Annabelle, trauma was the sole cause of addiction: “What I noticed, the pattern was that there was always some sort of trauma. It always starts-- A lot of people think-- there's this stereotype that people that take drugs, they're homeless, they've caused this on themselves or whatever. A lot of the time, it actually started when they were younger and something traumatic happened to them. Even the idea, because I always thought there was this idea of like when you start using cannabis and then you want to try something new.”
Overall, it was clear that participants perceived trauma as a key precipitator of substance misuse and addiction, characterizing substance misuse as a strategy to manage the psychological/emotional consequences of trauma (especially trauma in childhood).
Genetics (Smith’s S= 0.21): Genetics was often mentioned first by participants, but fewer times than trauma. From Charlotte’s perspective,
“That's a really tricky question. For me personally, I think it was hereditary. My father and my brother are both alcoholics, so I think I have the addictive gene. Personally, I didn't believe that I could be an alcoholic because I was female, and I didn't think that women could be alcoholics. I think it can also come down to circumstance as well in terms of overuse can just cause you to become addicted to that.”
Diane also mentioned genetics first, but was one of three participants who did so: “In my opinion, I think you are born with it to a certain degree, but I think life traumas contribute to it and a need to escape reality.” While the role that genetics and inheritance plays in addiction is clearly salient for our participants (i.e., patterns of primacy for this factor across participants’ responses), it tended to be mentioned as precipitating addiction when in conjunction with other factors (e.g., traumas, childhood environment, frequent or habitual use)
Childhood (Smith’s S= 0.11): Childhood was mentioned by only two participants. Judy, mentioned childhood as a primary cause:
“I think past life, like childhood or really what's happened to you in your life. You want to forget. Do you understand? Forget things or to cope with stuff that's going to happen.”
For these two participants, childhood seemed to be perceived as a critical period wherein other risk factors (e.g., trauma, social influence via family or peers) were particularly likely to lead to addiction.
Discussion
This study aimed to assess cultural domains through free-listing and open-ended responses among women with substance use disorders. In all locations, findings revealed culturally specific themes that are unlikely to emerge from quantitative approaches to evaluating recovery. For example, the Indian sample mentioned stress/tension as a cause of addiction. “Tension” is a common idiom of distress in India that is linked to chronic conditions, such as reproductive cancers (Van Hollen 2022). This approach also revealed similarities across sites, such as the role of peers in India and Toronto, thereby illustrating how applying cultural domain analysis to hybrid data provides a systematic approach to identifying cross-site similarities and differences. On the other hand, a limitation of this approach is that smaller sample sizes can lead to fewer themes. In London, for example, a smaller sample size generated a smaller list of key terms.
Despite potential limitations, a cultural domain approach to studying addiction in marginalized populations, such as women with substance use disorders, offers several unique advantages. This approach sensitively addresses addiction's complexities, enabling researchers to explore the topic without directly probing potentially traumatic personal experiences. For instance, instead of asking women to discuss their reasons for drug use - questions that could evoke trauma - a cultural domain approach might use prompts like, “What causes addiction among women in your community?” or “What does ‘recovery’ mean to women in your recovery community?” Such questions allow participants to share valuable insights about cultural dimensions of substance use without necessarily recounting personal traumas, although they may choose to draw from personal experience within a broader cultural context, enriching the understanding of shared cultural beliefs.
Additionally, this approach allows women to articulate their perceptions of addiction and recovery without strictly framing these concepts through a biomedical lens, which dominates much of addiction research and treatment. Teaching addiction solely through a biomedical framework, such as the Brain Disease Model of Addiction (BDMA), can miss how individuals in recovery interpret these terms in ways that resonate personally. Biomedical approaches often highlight individual-level factors, overlooking the broader social and structural forces that shape recovery. By focusing on cultural domains, researchers can emphasize aspects of recovery that hold specific significance to women in different contexts. Studies suggest that while addiction and recovery are often viewed as individual processes, such as abstinence for recovery (White, 2007), cultural perspectives reveal that these concepts are cross-culturally diverse and encompass social and structural dimensions (Placek 2024). The findings presented here underscore the social processes that participants in three cultural contexts view as key in shaping addictive processes, such as the role of peers and family members who model and normalize substance (mis)use, or the role of harmful or traumatic interpersonal stressors (particularly in childhood). For instance, “recovery” is inconsistently defined across clinical research, and instruments like the Recovery Capital Scale (Groshkova et al. 2012) reflect Western social and biomedical values (Placek and Wies n.d.). Statements such as “I have an intimate partner supportive of my recovery process” may imply a degree of control over personal relationships that is not universally applicable, potentially leading to culturally biased assessments. This contextualization of recovery as a primarily individual process will also fail to capture the role that relationships (peers, families, etc.) play in both addictive and recovery processes. A culturally competent understanding of addiction and recovery thus requires that participants help define these terms themselves, especially in diverse cultural contexts.
This approach broadens the notion of “culture” beyond race and ethnicity, often the primary focus of cultural competence in substance use research (Kleinman and Benson 2006). Anthropologically, “culture” differs from ethnicity and race. Ethnicity refers to shared identity and feelings of belonging to a "We"-group, often marked by language and religion (Antweiler 2015). However, ethnic identity does not guarantee adherence to cultural norms tied to that ethnicity. Similarly, race is a socially constructed concept based on physical traits like skin color. While race affects biological health due to discrimination and structural violence (Fuentes et al. 2019; Sharif et al. 2022), it does not inherently define cultural practices. Race and ethnicity intersect with gender and substance use in complex ways but do not fully capture “culture.” The cultural domain approach here integrates social, structural, and ecological factors shaping addiction and recovery.
Conclusions
Given the challenges of researching certain populations, we offer several recommendations for conducting cultural domain research that remains sensitive to diversity and promotes equity. First, allow the study to be partially, if not fully, exploratory, with a flexible research design. For example, measuring a cultural domain can vary from open-ended questions with key informants to larger samples where participants systematically respond to structured free-list prompts. Although the London sample was small, we still identified salient themes about addiction, which provided insight into participants’ beliefs on addiction's causes. We also recommend posing open-ended questions about seemingly straightforward concepts. While this study focused primarily on addiction, terms like “drug” and “substance” are also culturally diverse. When asked about commonly used drugs in their communities, some participants quickly cited “alcohol,” while others asked if alcohol counted as a drug. In retrospect, we could have first invited participants to define “drug” and list examples from their communities. Using this inductive approach for key terms in substance use research fosters more culturally competent data and shared understanding between participants and investigators. Finally, we suggest using diverse recruitment methods—from classic anthropological strategies like rapport building and participant observation to social media recruitment.
In conclusion, working with hard-to-reach populations requires adaptable research methods that allow participants’ voices to be authentically represented while upholding research rigor. Cultural domain analysis achieves this balance by systematically assessing the salience of participants’ perspectives.
Author Contributions
Conceptualization, C.P.; Methodology, C.P., V.P., I.J., L.A; Software, C.P.; Formal Analysis, C.P., I.J.; Investigation, C.P., I.J., V.P..; Data Curation, C.P.; Writing – Original Draft Preparation, C.P., L.A.; Writing – Review & Editing, C.P., L.A.; Visualization, C.P..; Supervision, M.S., C.P., V.P.; Project Administration, C.P., V.P.; Funding Acquisition, C.P.
Funding
This study was funded by the Fulbright Global Scholar award and Ball State University’s ASPIRE grant.
Ethics Statement
The study received approval from Ball State University's Institutional Review Board on 07/28/2023 (#2068016), the Ethics Committee at the Indian Spinal Injuries Centre, and Brunel University’s College of Health, Medicine, and Life Sciences Research Ethics Committee.
Acknowledgments
The authors thank the study participants and the recovery centers for their time and efforts.
Conflicts of Interest
The authors report no conflict of interest.
Note
1 All names have been changed to protect the identities of participants.
References
- Antweiler, C. (2015). Ethnicity from an anthropological perspective. In Ethnicity as a Political Resource. University of Cologne Forum.
- Avasthi, A. , & Ghosh, A. (2019). Drug misuse in India: Where do we stand & where to go from here? Indian Journal of Medical Research. [CrossRef]
- Borgatti, S. P. (1998). Elicitation Techniques for Cultural Domain Analysis. In The Ethnographers Toolkit (Vol. 3). Alitmira Press.
- Boyd, R. , & Richerson, P. J. (1988). Culture and the Evolutionary Process.
- Brady, K. , Grice, D., Dustan, L., & Randall, C. (1993). Gender difference in substance use disorders. ( 150, 1707–1711. [CrossRef]
- De Kock, C. (2020). Cultural competence and derivatives in substance use treatment for migrants and ethnic minorities: What’s the problem represented to be? Social Theory & Health. [CrossRef]
- Degenhardt, L. , Charlson, F., Mathers, B., Hall, W. D., Flaxman, A. D., Johns, N., & Vos, T. (2014). The global epidemiology and burden of opioid dependence: Results from the global burden of disease 2010 study. Addiction, 1333. [Google Scholar] [CrossRef]
- Fuentes, A. , Ackermann, R. R., Athreya, S., Bolnick, D., Lasisi, T., Lee, S., McLean, S., & Nelson, R. (2019). AAPA Statement on Race and Racism. ( 169(3), 400–402. [CrossRef]
- Gatewood, J. B. (1984). Familiarity, vocabulary size, and recognition ability in four semantic domains. American Ethnologist. [CrossRef]
- Groshkova, T. , Best, D., & White, W. (2013). The Assessment of Recovery Capital: Properties and psychometrics of a measure of addiction recovery strengths. Drug and Alcohol Review. [CrossRef]
- Hewlett, B. S. (2004). Fathers in Forager, Farmer, and Pastoral Cultures. In The Role of the Father in Child Development, ed. Michael Lamb (pp. 182–195). Wiley.
- Hollen, C. C. V. (2022). Cancer and the Kali Yuga: Gender, Inequality, and Health in South India.
- Kleinman, A. , & Benson, P. (2006). Anthropology in the Clinic: The Problem of Cultural Competency and How to Fix It. PLOS Medicine. [CrossRef]
- Nasser, R. (2005). A Method for Social Scientists to Adapt Instruments From One Culture to Another: The Case of the Job Descriptive Index. Journal of Social Sciences.
- Pierce, M. , van Amsterdam, J., Kalkman, G. A., Schellekens, A., & van den Brink, W. (2021). Is Europe facing an opioid crisis like the United States? An analysis of opioid use and related adverse effects in 19 European countries between 2010 and 2018. European Psychiatry. [CrossRef]
- Placek, C. (2024). Drug Use, Recovery, and Maternal Instinct Bias: A Biocultural and Social-Ecological Approach.
- Placek, C. , Budzielek, E., White, L., & Williams, D. (2023). Anthropology in Evaluation: Free-listing to Generate Cultural Models. American Journal of Evaluation.
- Placek, C. D. , Place, J. M., & Wies, J. (2021). Reflections and Challenges of Pregnant and Postpartum Participant Recruitment in the Context of the Opioid Epidemic. ( 25(7), 1031–1035. [CrossRef] [PubMed]
- Placek, C. , & Wies, J. (n.d.). Cultural Competence for Drug Addiction and Recovery: Considerations for Research and Evaluation. Social Theory & Health.
- Purzycki, B. G. , Pisor, A. C., Apicella, C., Atkinson, Q., Cohen, E., Henrich, J., McElreath, R., McNamara, R. A., Norenzayan, A., Willard, A. K., & Xygalatas, D. (2018). The cognitive and cultural foundations of moral behavior. ( 39(5), 490–501. [CrossRef]
- Quinlan, M. (2005). Considerations for Collecting Freelists in the Field: Examples from Ethobotany. Field Methods. [CrossRef]
- Romney, A. K. , & D’andrade, R. G. (1964). Cognitive Aspects of English Kin Terms. G. ( 66(3), 146–170. [CrossRef]
- Shaghaghi, A. , Bhopal, R. S., & Sheikh, A. (2011). Approaches to Recruiting ‘Hard-To-Reach’ Populations into Re search: A Review of the Literature. Health Promotion Perspectives. [CrossRef]
- Sharif, M. Z. , García, J. J., Mitchell, U., Dellor, E. D., Bradford, N. J., & Truong, M. (2022). Racism and Structural Violence: Interconnected Threats to Health Equity. Frontiers in Public Health. [CrossRef]
- Slabbert, I. , Greene, M. C., Womersley, J. S., Olateju, O. I., Soboka, M., & Lemieux, A. M. (2020). Women and substance use disorders in low- and middle-income countries: A call for advancing research equity in prevention and treatment. Substance Abuse. [CrossRef]
- Smith, J. J. , & Borgatti, S. P. (1997). Salience CountsAnd So Does Accuracy: Correcting and Updating a Measure for Free-List-Item Salience. Journal of Linguistic Anthropology. [CrossRef]
- Tuchman, E. (2010). Women and Addiction: The Importance of Gender Issues in Substance Abuse Research. Journal of Addictive Diseases. [CrossRef]
- White, L. A. (1959). The Concept of Culture. American Anthropologist, /: 227–251. https, 6650. [Google Scholar]
Figure 1.
Smith’s S scores for perceived causes of addiction in Delhi.
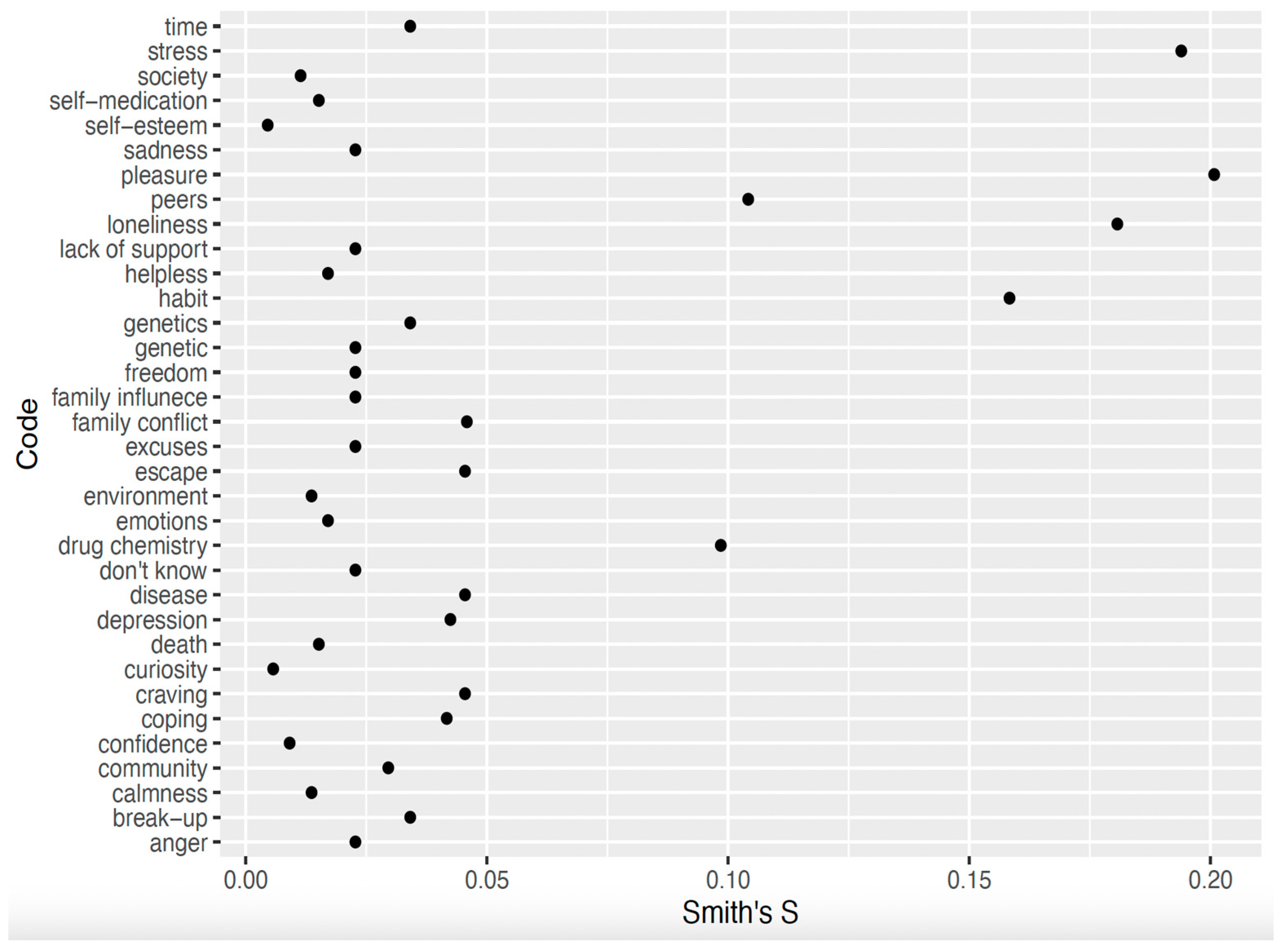
Figure 2.
Smith’s S scores for perceived causes of addiction in Toronto.
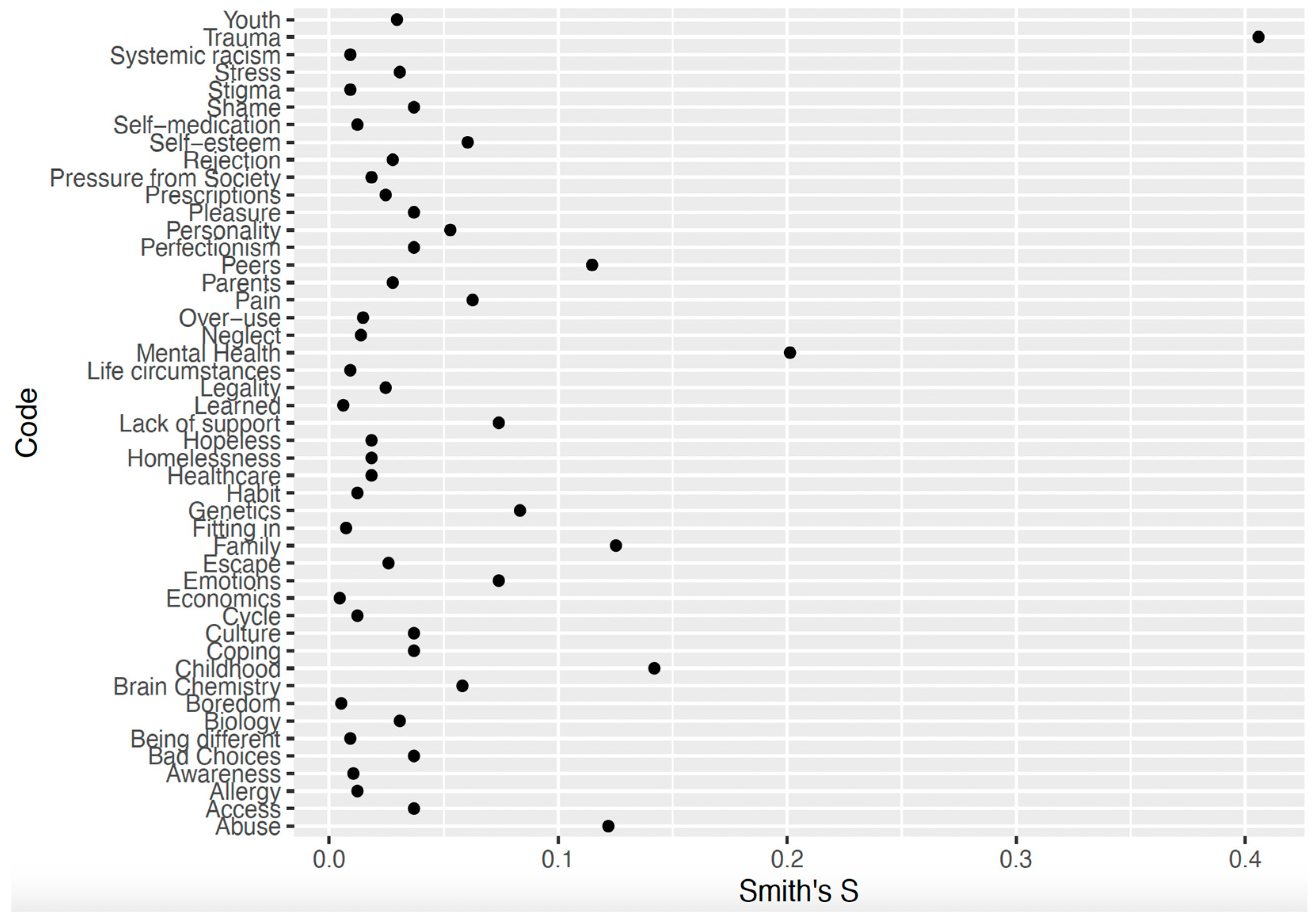
Figure 3.
Smith’s S scores for perceived causes of addiction in London.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



