
Submitted:
02 December 2024
Posted:
03 December 2024
You are already at the latest version
Abstract
With a new vitamin on the horizon, it is first necessary to clarify what the basic definition of vitamins is. What is a vitamin? Which institutions are generally responsible for officially recognizing the status of a vitamin and which legal basis should be used if necessary? How were other vitamins identified and established as essential nutrients in the last century? And specifically in this case: What is vitamin A? What are the defined biological functions of vitamin A? In this article, the basics and definitions are summarized in a historical context, with relevance for the discovery, establishment and categorization of a new vitamin concept.
Keywords:
retinoids
; carotenoids
; vitamin
; retinoid
1. How Do You “Discover” and Establish a Vitamin? A Brief Historical Review
Vitamins are typically associated with specific deficiency symptoms. Historically, however, the precise timing of vitamin deficiency symptoms and the identification of the factors responsible have not always been easy and transparent. For this reason, the considerations in this work begin with the best-documented example of vitamin C, isolated by Albert Szent-Györgyi. A researcher who, as in the case of vitamin A5 to be described later (Banati et al., 2024), carried out his work mainly in Hungary (Waugh & King, 1976; Zilva, 1935).
It often begins with a theory of how a physiological dysfunction or even existing pathological signs can be reversibly prevented by food components. In the case of vitamin C, this was scurvy, which was particularly prevalent among sailors. It was discovered relatively quickly that a low intake of fresh fruit and vegetables increased the incidence of scurvy (Waugh & King, 1976). This finding was followed by what was probably the world's first described clinical trial, conducted and described by James Lind 1747, summarized in Dresen et al. (2023). The other questions that arose came from the field of applied instrumental science, namely what active constituents were present in these foods, how the active constituents could be enriched and isolated, and how these enriched extracts or isolated compounds worked (Waugh & King, 1976; Zilva, 1935). The major challenge has been to isolate and determine the exact structure of the active compounds using currently available preparative and analytical methods.
Such extracts or, ideally, isolated compounds, and later organochemically synthesised substances, were then studied in animal models (Haworth & Hirst, 1933). In the case of vitamin C, this was the guinea pig, in which scurvy-like symptoms were induced. Initially, these test animals were treated with extracts from lemons or peppers and later with isolated substances (Waugh & King, 1976; Zilva, 1935). The animals were also examined for the symptoms described above. Initially, different extraction methods were used to obtain different extracts to study and develop ideas about the physico-chemical properties of the active ingredient in these extracts (Waugh & King, 1976; Zilva, 1935). The final result in 1933 was an identified, physico-chemically characterized and isolated substance -ascorbic acid / vitamin C- which prevented the existing physiological dysfunctions in the model animal or even reversibly cured a disease.
Later experiments on humans could be carried out quite quickly and easily. On a "let's get started" basis, one simply "recruited" some "volunteers" and/or patients and treated them with laboratory extracts (Letondal, 1936). Targeted clinical interventions in humans, whether to a) induce a specific vitamin deficiency, b) investigate a correlation between the intake or concentration of a specific vitamin in the organism with markers of dysfunction, or c) supplement vitamin-deficient "volunteers" or patients, were not carried out in detail until much later. The reason for this was the lack of analytical methods to specifically identify specific deficiencies by laboratory methods and to determine the effect of substitutions analytically and mechanistically in detail, summarized in Maxfield and Maxfield (2024).
Summary: In the 1930s, many aspects of vitamin discovery were supposedly simpler: no animal experiments, no ethical applications for clinical trials, peer review in very rare cases, no months of communication with journals, no legal advice, no clinics with high overheads and no restrictive government agencies. However, there were similar problems then as there are now, such as a lack of funding to carry out trials. Clinical interventions with targeted nutritional deficiencies and supplementation experiments were carried out 'en passant' on patients, prisoners of war or prison inmates (Creamer, 2018; Joost, 2012). All these experiments, which now seem bizarre, were later uncritically incorporated into national and international vitamin and food references (WHO, 1998) (WHO/FAOExpertgroup, 1967). The problem is that the existing national and international vitamin references contain many inconsistencies, which are inviolable from a historical perspective, but not necessarily from a scientific one.
Only much later, after the discovery of additional vitamins and the establishment of vitamin concepts, i.e. from the 1960s (WHO/FAOExpertgroup, 1967), were uniform criteria and definitions for vitamins and micronutrients established by the WHO/FAO Expert Groups (WHO, 1998) and reference intakes proposed (EFSA Panel on Dietetic Products & Allergies, 2010; European Food Safety, 2017). Later, after the establishment of the European Food Safety Authority (EFSA) in 2002, regulations on novel foods (Commission, 2017) and on substance-specific health claims were also developed (European Commission, 2006).
2. What Is a Vitamin as Defined by the World Health Organisation (WHO) and EFSA? (Figure 1)
The WHO writes: “Definition of terms: The following definitions relate to the micronutrient intake from food and water required to promote optimal health, that is, prevent vitamin and mineral deficiency and avoid the consequences of excess” (WHO, 1998) (Figure 1).
EFSA's definition of a vitamin is as follows: "Dietary substance needed in very small amounts to support normal growth and maintenance of health in humans and animals. Most vitamins are 'essential' as they are not made within the body" (EFSA Panel on Dietetic Products & Allergies, 2015). The definition is somewhat softened by the addition of the word 'most' before the word 'vitamins', presumably to avoid having to withdraw the status of a vitamin from the non-essential 'vitamin' (Glerup et al., 2000), vitamin D, based on an overly strict vitamin definition.
Summary: Four criteria are used to define a vitamin. A vitamin must be a) a micronutrient, b) a component of the diet, c) perform a physiologically important function, and d) be essential (according to EFSA, "as they are not made in the body" (Figure 1).
3. What Is the Definition of Vitamin A? (Figure 2)
a) Vitamin A definitions from EFSA, the British National Health Service (NHS) and the French Agency for Food, Environmental and Occupational Safety (Agence nationale de sécurité sanitaire de l'alimentation, ANSES):
“Vitamin A is a fat soluble vitamin obtained from the diet either as preformed vitamin A (mainly retinol and retinyl esters) in foods of animal origin, or as provitamin A carotenoids in plant-derived foods. Foods rich in vitamin A include meat, butter, retinol-enriched margarine, dairy products, eggs, and vegetables and fruits such as sweet potatoes, carrots, pumpkins, dark green leafy vegetables, sweet red peppers, mangoes and melons.”(EFSA Panel on Dietetic Products & Allergies, 2015):
The term “vitamin A” therefore includes the substances retinol, various retinyl esters, and various provitamin A carotenoids (Böhm et al., 2021; T. Bohn et al., 2021). This definition is also used by the NHS in the United Kingdom (NHS, 2020) and the ANSES in France (ANSES, 2013).
b) Vitamin A-definition of the German Nutrition Society (Deutsche Gesellschaft für Ernährung, DGE):
The DGE defines the term vitamin A as follows: “Vitamin A is a vital (essential), fat-soluble nutrient that is necessary for many biological processes such as vision, immune function, cell differentiation and embryonic development. The term vitamin A describes a group of compounds that have a vitamin A effect. The main active form is retinol” and “Plants contain a number of provitamin A carotenoids that can be converted to vitamin A to varying degrees. The most important provitamin A for human vitamin A intake is β-carotene, as it has a high rate of conversion to retinol and is the most abundand. Provitamin A carotenoids are not essential, but are particularly important for maintaining an adequate vitamin A status, especially in predominantly vegetarian or vegan diets.”
The term "vitamin A" as defined by the DGE includes only retinol and retinyl esters, and does not include provitamin A carotenoids. According to the DGE definition, this creates a paradox based on the following contradictory statements: a) "vitamin A describes a group of compounds that have vitamin A effects" and b) "provitamin A carotenoids can be converted to vitamin A". However, as provitamin A carotenoids mediate vitamin A effects directly - i.e. without direct conversion to retinol - and thus have them, based on dozens of scientific studies (Böhm et al., 2021; Bohn, de Lera, Landrier, & Rühl, 2022; Bohn et al., 2017; Bohn et al., 2019), provitamin A carotenoids belong to the vitamin A family as defined by the WHO, EFSA and DGE. Therefore, the conversion of "vitamin A" (in the form of provitamin A) to "vitamin A" is a paradox. We suspect that the terms "retinol", "vitamin A" and "vitamin A1" have been equated by the DGE, although they describe different things. A further statement by the DGE that provitamin A carotenoids are not essential, although they belong to the vitamin A family and are therefore vitamin A, is therefore another paradox in the above formulations.
c) Vitamin definition of the WHO and the International Union of Pure and Applied Chemistry (IUPAC):
According to the IUPAC definition (IUPAC-IUB, 1982), the vitamin A family includes the substance groups vitamin A1 and vitamin A2. In the early FAO / WHO communications of 1967 (WHO/FAOExpertgroup, 1967) also clearly stated that: “The term 'retinol' refers to vitamin A1 alcohol. The term 'vitamin A' includes all compounds with vitamin A activity.”, which provided a clear definition of vitamin A and vitamin A1 and clearly distinguished these two terms from each other. A definition for vitamin A2 was also provided: “Vitamin A2 refers to 3,4-dehydroretinol.” (Figure 3).
This definition was not officially changed subsequent FAO / WHO communications from 1988 onwards (WHO/FAOExpertgroup, 1988), but in the WHO communications from 1988 onwards the term “vitamin A” was equated with the terms “retinol” and “vitamin A1”.
From a legal and general point of view, the 1967 WHO definition was never been revoked, but simply "optimized" and simplified by the WHO from a certain point in time, in 1988. This new optimized definition of vitamin A was then partially adopted by other national organizations.
Summary: According to the IUPAC and WHO definitions, in addition to retinol, retinyl esters and provitamin A, there are vitamin A subgroups, namely vitamin A1 and A2, with the possibility of adding other relevant subgroups. These subgroups, vitamin A1 and A2, have not been further differentiated or included in other dietary guidelines based on the EFSA and WHO guidelines. Only the IUPAC definition did not follow this simplification (IUPAC-IUB, 1982).
d) Vitamin A2 forgotten and banned?
Vitamin A2 (3,4-dehydroretinol, Figure 3), first found in fish oils, was discovered in the late 1920s (La Frano, Cai, Burri, & Thilsted, 2018; Morton, Salah, & Stubbs, 1947) and can functionally replace vitamin A1 to prevent general vitamin A deficiency (Shantz, Embree, & et al., 1946). With only 30 publications listed in the scientific database PubMed in the last 20 years with the search term “vitamin A2” compared to >60,000 publications with the search term “vitamin A”, it has seemingly become insignificant and was probably simply “banned” from the current vitamin A definition. It is also suspected that this was done for the sake of simplification and because of the minor role of vitamin A2 in the food chain.
Summary: Unfortunately, to date, the term “vitamin A1” has been and continues to be partially equated with the term “vitamin A”, which is incorrect but has not seemed to be problematic to date (Banati et al., 2024; Banati & Rühl, 2024; Bohn, Hellman-Regen, de Lera, Böhm, & Rühl, 2023; de Lera, Krezel, & Rühl, 2016; Krezel, Rühl, & de Lera, 2019; Rühl, Krezel, & de Lera, 2018).
e) Vitamin A(1) aldehyde and vitamin A(1) acid
The substance retinal is also defined by the EFSA as vitamin A (EFSA Panel on Nutrition et al., 2024) because retinal can be metabolized to retinol (all-trans-) and is therefore also defined as vitamin A. It also seemed to be recognized that retinal, which is mainly found in eyes, is a relevant dietary component.
Retinoic acid (all-trans-), also known as vitamin A / A(1) acid, is another substance that does not occur significantly in relevant food components and concentrations and cannot be metabolized to retinol (all-trans-) in the human organism. An important function of vitamin A, which is mediated by retinal in the visual cycle, cannot therefore be mediated. Therefore, two criteria for being defined as vitamin A are not met.
f) Summary of the definition of vitamins in general and vitamin A in particular
The problem is that different national and international professional societies do not describe the definition of “vitamin A” consistently and sometimes present it in a paradoxical manner.
The following three problems of the current situation with different definitions are summarized here:
i) Based on the information provided by EFSA and WHO and the current state of science, the latter of which can be read in many publications and reviews (Böhm et al., 2021; T. Bohn et al., 2021; T. Bohn et al., 2019), provitamin A is part of the vitamin A family and therefore vitamin A and vitamin A IS essential. These facts are based on the general vitamin definition of the WHO and EFSA (EFSA Panel on Dietetic Products & Allergies, 2015; WHO/FAOExpertgroup, 1967, 1988) and numerous scientific studies (Böhm et al., 2021; Bohn et al., 2022; Bohn et al., 2017; Bohn et al., 2019).
ii) Another problem in optimising and simplifying the term vitamin A is also the equation of the terms “retinol” with “vitamin A” and “vitamin A1”, which prevents a differentiation between vitamin A subgroups such as vitamin A1 and vitamin A2 and other possible subclasses.
iii) An additional problem is that vitamin A alcohol / retinol is mistakenly used as the reference for vitamin A-mediated activity and subsequent dietary recommendations, rather than the major "active" form, all-trans-retinoic acid (ATRA), and further ATRA - retinoic acid receptor (RAR) mediated signalling.
A clear definition of vitamin A is important for a further evaluation of whether a new vitamin A subclass should be included in the vitamin A group. For this, all criteria (Figure 1) should be met: a vitamin must be a) a micronutrient, b) a dietary component, c) provide a physiologically important function and d) being essential (according to EFSA, “as they are not made within the body”). These three problems with the definition of vitamin A lead to serious problems of interpretation. A publication by Prof. Diana Banati, from the University of Szeged, Hungary, a former chair of EFSA, summarizes the problems of the different definitions (Banati & Rühl, 2024), shown in Figure 3.
g) Need for optimization and action:
There is currently an urgent need for optimization and therefore a direct need for action at national and international level by national societies and international authorities (EFSA and WHO), but also for the EU legislators, whose draft laws will be further implemented in the respective EU member states and associated third countries.
The problem is the false equivalence of the term “vitamin A” with the terms “vitamin A1” and “retinol”, which now, after decades, is now widespread in many national and international organizations and also forms the basis for legally binding food labeling in national and international legislation.
A scientifically correct presentation of scientific facts, based on WHO and EFSA definitions in the area of vitamin A, therefore also has direct legal consequences for free science, popular science communication, scientifically correct dietary recommendations, but also for the commercial implementation of scientific findings in the area of food and its declaration. European consumer protection organizations are currently pushing for the communication of scientifically incorrect data in food labeling based solely on the basis on given, partly paradoxical foundations of EU food law and the EU Food Declaration (Commission, 2011; European Commission, 2024).
In order to ensure correct, legally binding food labeling, also with relevance for new vitamin A subclasses, a correct, uniform and non-paradoxical reorganization and disentangling of the term vitamin A must be sought. This correct presentation of the term vitamin A could be initiated by a national nutrition association such as the DGE, although further persuasion work will probably be required to overcome the initial activation energy. But constant dripping wears away the stone and sooner or later international and national organizations will have to take action.
4. The Biological/Physiological Mechanisms of Action of Vitamin A
The biological mechanisms of action for optimal health and prevention of vitamin A deficiency include three biological / physiological vital / essential mechanisms:
a) The action of retinal as a component of the pigment Rhodopsin in the visual process.
b) Activation of the retinoic acid receptor (RAR) and subsequent RAR-mediated signalling initiated by all-trans-retinoic acid. This RAR-mediated signalling involves important physiological functions of vitamin A in the immune system, embryonic development, cellular differentiation and proliferation, and other biochemical processes.
c) Activation of the retinoid X receptor (RXR) and subsequent RXR-mediated signaling. The RXR is the respective partner for the RAR, so RXR-mediated signaling is also an important criterion for RAR-mediated signaling. It is also a partner in signaling of vitamin D via the vitamin D receptor (VDR), of thyroid hormones via the thyroid hormone receptor (TR), of cholesterol derivatives via the liver X receptors (LXRs), of fatty acids and lipid mediators via the peroxisome proliferator-activated receptors (PPARs) and other signaling such as via alternative nuclear hormone receptors, e.g. the “nuclear receptor subfamily 4 group A member 2” (NR4A2), see Figure 4.
Summary: The RXR is probably THE most important physiological master switch, enabling a multitude of signalling pathways via numerous nuclear hormone receptors (Mangelsdorf & Evans, 1995). An endogenous RXR ligand is therefore the most important dietary substance that enables and controls all these signaling cascades (Evans, 2005; Evans & Mangelsdorf, 2014).
5. The Missing Piece of the Vitamin A Puzzle, the Vitamin A-Controlled RXR-Mediated Signaling
Based on experiments in animal models, this most important part of a vitamin A-mediated effect is the vitamin A - RXR-mediated signaling (Balmer & Blomhoff, 2002; Mangelsdorf & Evans, 1995). This vitamin A - RXR-mediated signaling effect includes not only the vitamin A - RXR - RAR-mediated effect, with is important for general and embryonic development, but also the control of physiological processes such as differentiation, apoptosis and proliferation with essential importance for the immune system, and the maintenance of skin, bones and other organs.
The importance of vitamin A - RXR signalling extends much further, to the general control of processes mediated by other nuclear hormone receptors, such as VDR, TR, LXRs, PPARs and NR4A2, which are responsible for, among other things, the general maintenance and control of our body's metabolism (Evans & Mangelsdorf, 2014). Some of these mechanisms are vital to our bodies, while others are not immediately essential. Using the example of the control of insulin secretion mediated by vitamin A - RXR signalling (Kane et al., 2010; Mangelsdorf & Evans, 1995), long-term dysregulation of vitamin A-RXR signalling can have serious consequences that only occur after a long period of dysregulation, as in the case of diabetes mellitus (Khunti et al., 2023). This disease is a chronic, treatable disease that severely limits the quality of life but is not fatal and immediately leading to death. In this case, vitamin A - RXR signaling would not be essential. These consequences therefore only occur after a long (very long) period of dysregulation, i.e. not immediately, in other known chronic diseases of the Western lifestyle, such as cardiovascular disease, diabetes, atherosclerosis, suboptimal mental health and an increased prevalence of a variety of neurological diseases with a focus on neurodegenerative diseases (NIH, 2024; Wilson, Cookson, Van Den Bosch, Zetterberg, Holtzman, & Dewachter, 2023).
These disorders are different from those caused by a deficiency of B vitamins. These water-soluble B vitamins are not stored in the body in significant quantities (with the exception of vitamin B12) and must therefore be taken in daily. In the case of vitamin A and vitamin A - RXR signaling, an acute effect is difficult to determine and difficult to correlate with a current daily vitamin intake. In the area of vitamin A and vitamin A deficiency, long-term effects relevant to chronic diseases must also be considered, even if these chronic diseases are not immediately fatal and can be explained by an essential, vital vitamin effect.
The important question is: how does vitamin A mediate this RXR activation and subsequent RXR signalling?
a) The controversial phantom ligand for RXR, 9-cis-retinoic acid.
9-Cis-retinoic acid (9CRA) was independently "identified" by two working groups and described as THE endogenous ligand for the activation of the RXR (Heyman et al., 1992; Levin et al., 1992). This work was carried out in the early 1990s using the most up-to-date analytical techniques available at the time. These techniques are considered to be rather unselective and insensitive analytical methods based on the current state of the art. In the years that followed, numerous experts in the field of vitamin A analysis, including the working group led by Dr. Heinz Nau (†) at the Free University of Berlin and later at the University of Veterinary Medicine in Hanover, conducted studies on this topic. Dr. Rühl, one of the discoverers of the vitamin A5 concept, carried out his diploma and doctoral theses with this working group. This working group, like other groups worldwide, attempted to detect 9CRA endogenously in animals and also in humans. The detection of endogenous 9CRA in humans could not be carried out or at least not clearly, summarized in (T. Bohn et al., 2022). Only decades later was a working group able to identify “9CRA” in humans using liquid chromatography coupled to mass spectrometry (LC-MS), but again not unambiguously and only at concentrations that are far below the level required for RXR activation (Arnold, Amory, Walsh, & Isoherranen, 2012). Another problem was that many alternative substances co-elute with 9CRA in the analytical chromatographic methods used (de Lera et al., 2016; Rühl, 2006; Rühl et al., 2018; Rühl et al., 2015) and a clear identification and quantification of the analytical peak as 9CRA was not yet clearly possible (Rühl, 2006).
To unambiguously detect an endogenous substance, ideally two or more independent analytical detection methods should be performed in parallel. In the case of 9CRA, separation by HPLC should be followed by detection, e.g. by selective MS/MS methodology and a diode array detector (Rühl, 2006). Based on this need for parallel detection of 9CRA by two independent methods, many publications that have detected and quantified 9CRA must be questioned (Heyman et al., 1992; Wang, Krinsky, Benotti, & Russell, 1994). The interpretation that 9CRA has not been unambiguously identified and that 9CRA is not THE endogenously occurring RXR ligand is currently accepted by experts in the field of retinoid analysis, reviewed in (Bohn et al., 2022; de Lera et al., 2016; Krezel et al., 2019; Rühl et al., 2018).
The questions of whether a) 9CRA is definitely present in the human organism and whether b) there is a controlled enzymatic synthesis in the human organism (again based on inadequate analysis) have not yet been clearly clarified, are speculative and therefore not a proven scientific fact. Unfortunately, this "shaky" "9CRA - endogenous RXR ligand" hypothesis is still being promoted by many nutritional experts with no experience in the field of retinoid analysis and no involvement in this complex subject.
Dr. Ron M. Evans (H-index 232) and Dr. Pierre Chambon (H-index 211) are the pioneers in the field of nuclear hormone receptors and highly decorated scientists and multiple nominees for the Nobel Prize. Ron Evans was the research supervisor of Dr Rühl's former postdoctoral supervisor and later collaborator (Dr Laszlo Nagy, University of Debrecen, Hungary and John´s Hopkins University, St Petersburg, USA) in Hungary and Pierre Chambon is the PhD supervisor of Dr Wojtek Krezel, who is also the discoverer of vitamin A5.
In 1992, Ron Evans identified 9CRA as THE endogenous RXR ligand (Heyman et al., 1992) and later described 9CRA as the “BIG BANG” in nuclear hormone receptor research (Giguère & Evans, 2022). In a review article in 2022, Evans revised his statement based on the work of Krezel et al. ( Krezel et al., 2021): “A search for a higher affinity retinoid for RXR led to the identification of the 9-cis isomer of RA (9-cis-RA) as a suitable ligand (Heyman et al., 1992; Levin et al., 1992). Given its low abundance in tissues and high affinity of the RARs, the exact role that endogenous 9-cis-RA plays as an RXR ligand in retinoid signaling in vivo has remained elusive. However, it has recently been reported that a retinoid related to 9-cis-RA present at high endogenous levels in mice, namely 9-cis-13,14-dihydroretinoic acid, binds and transactivates all three RXRs at physiological concentrations (Rühl et al., 2015),” see Figure 5.
Summary: The status of 9CRA as THE physiological ligand for the RXR with an enzymatically regulated metabolic pathway is still very present in the nutritional research literature, but this hypothesis remains very fragile and has been revised by Dr. Ron Evans (Giguère & Evans, 2022), based on the later work of Krezel, Rühl and de Lera (Krezel et al., 2021), around the discovery of the 9CDHRA-RXR-mediated pathway (Rühl et al., 2018; Rühl et al., 2015).
b) The new vitamin A5 concept and vitamin A - RXR-mediated signaling
This new vitamin concept describes the unique concept of a nutritionally relevant precursor of an endogenous RXR ligand, 9CDHRA, and the subsequent mediation of vitamin A – RXR-mediated signaling (de Lera et al., 2016; Krężel et al., 2021; Krezel et al., 2019; Rühl et al., 2018; Rühl et al., 2015). Physiological relevance (Krężel et al., 2021; Rühl et al., 2018), essentiality of an RXR ligand (Mascrez, Ghyselinck, Chambon, & Mark, 2009; Mascrez, Mark, Dierich, Ghyselinck, Kastner, & Chambon, 1998), occurrence as a micronutrient in the human food chain (Bohn, Despotovic, Vahid, & Rühl, 2024; Bohn et al., 2023; Krężel et al., 2021), occurrence in the human organism (Krężel et al., 2021; Lucas, Szklenar, Mihály, Szegedi, Töröcsik, & Rühl, 2022), the relevance of vitamin A5 to mediated RXR-mediated signaling in humans (Shaish et al., 2006) and the calculated occurrence in the diet of Western society (Bohn et al., 2024), as well as the relevance of vitamin A5 for human health and in particular for brain and nerve health, have already been described in numerous publications and are summarized in detail in another chapter (Bohn et al., 2025).
6. A General Summary
In order to discover and identify a vitamin, it was logical to first identify a disease that could be "cured" or whose symptoms could be significantly reduced by certain foods. The substances responsible for this were extracted, isolated, identified and then tested for their effects in non-human models. The result made it possible to declare it a vitamin.
It was only years / decades later that clinical trials with dose-response relationships and mechanistic analyses, as well as accompanying metabolic analyses, were carried out, i.e. usually decades after a vitamin was considered to have been "discovered". Further decades later, the regulatory basis was established, additional health claims were created and intake levels for these vitamins were proposed. These reference values and health claims were then anchored in sometimes paradoxical legal frameworks on the use of health claims and reference values for legal food labeling.
Based on existing definitions for the terms “vitamin” and “vitamin A”, improvements and global standardization in the field of vitamin A are proposed, which can and must be easily and quickly implemented by national and international organizations.
References
- ANSES. (2013). Vitamin A and provitamin A carotenoids. https://www.anses.fr/en/content/vitamin-provitamin-carotenoids ), accessed June 28, 2024 .
- Arnold, S.L., Amory, JK, Walsh, TJ, & Isoherranen, N. (2012). A sensitive and specific method for measurement of multiple retinoids in human serum with UHPLC-MS/MS. J Lipid Res, 53 (3), 587-598. [CrossRef]
- Balmer, J.E., & Blomhoff, R. (2002). Gene expression regulation by retinoic acid. J Lipid Res, 43 (11), 1773-1808. http://www.jlr.org/content/43/11/1773.full.pdf .
- Banati, D., Hellmann-Regen, J., Mack, I., Young, HA, Benton, D., Eggerdorfer, M., . . . Rühl, R. (2024). Defining a vitamin A5/X specific deficiency–vitamin A5/X as a critical dietary factor for mental health. Int J Vitam Nutr Res, 94 (5-6), 443-475.
- Banati, D., & Rühl, R. (2024). Analysis of the current vitamin A terminology and dietary regulations from vitamin A1 to vitamin A5. International Journal of Vitamin and Nutrion Research, 94 (5-6), 326-333.
- Böhm, V., Borel, P., Corte-Real, J., de Lera, A., Desmarchelier, C., Dulinska-Litewka, J., . . . Bohn, T. (2021). From carotenoid intake to carotenoid blood and tissue concentrations – implications for dietary intake recommendations. Nutr Rev, 79 , 544–573.
- Bohn, T., Bonet, ML, Borel, P., Keijer, J., Landrier, JF, Milisav, I., . . . Dulińska-Litewka, J. (2021). Mechanistic aspects of carotenoid health benefits - where are we now? Nutr Res Rev , 1-27. [CrossRef]
- Bohn, T., de Lera, AR, Landrier, JF, & Rühl, R. (2022). Carotenoid metabolites, their tissue and blood concentrations in humans and further bioactivity via retinoid receptor-mediated signaling. Nutr Res Rev , 1-14. [CrossRef]
- Bohn, T., Desmarchelier, C., Dragsted, LO, Nielsen, CS, Stahl, W., Ruhl, R., . . . Borel, P. (2017). Host-related factors explaining interindividual variability of carotenoid bioavailability and tissue concentrations in humans. Mol Nutr Food Res, 61 , 1600685. [CrossRef]
- Bohn, T., Desmarchelier, C., El, SN, Keijer, J., van Schothorst, E., Ruhl, R., & Borel, P. (2019). Beta-Carotene in the human body: metabolic bioactivation pathways - from digestion to tissue distribution and excretion. Proc Nutr Soc, 78 (1), 68-87. [CrossRef]
- Bohn, T., Despotovic, M., Vahid, F., & Rühl, R. (2024). Estimated Dietary Intakes of Vitamin A5. Nutrients (Vol. 16).
- Bohn, T., Hellman-Regen, J., de Lera, AR, Böhm, V., & Rühl, R. (2023). Human nutritional relevance and suggested nutritional guidelines for vitamin A5/X and provitamin A5/X. Nutr Metab (Lond), 20 (1), 34. [CrossRef]
- Bohn, T., Rohn, S., Böhm, V., Despotovic, M., de Lera Á, R., Krezel, W., . . . Rühl, R. (2025). Chapter 2: Vitamin A5, a newly identified micronutrient for the brain and nerves: What is fact, what is still missing? Nutritional review, in preparation .
- Commission, E. (2011). Regulation (EU) No 1169/2011 of the European Parliament and of the Council of 25 October 2011 on the provision of food information to consumers, amending Regulations (EC) No 1924/2006 and (EC) No 1925/2006 of the European Parliament and of the Council, and repealing Commission Directive 87/250/EEC, Council Directive 90/496/EEC, Commission Directive 1999/10/EC, Directive 2000/13/EC of the European Parliament and of the Council, Commission Directives 2002/67/EC and 2008/5/EC and Commission Regulation (EC) No 608/2004 Text with EEA relevance. Official Journal of the European Union L304/18 .
- Commission, E. (2017). Commission Implementing Regulation (EU) 2017/2470 of 20 December 2017 establishing the Union list of novel foods in accordance with Regulation (EU) 2015/2283 of the European Parliament and of the Council on novel foods (Text with EEA relevance. ). Official Journal of the European Union , L 351/372.
- Creamer, D. (2018). Malnutrition and skin disease in Far East prisoners-of-war in World War II. Clin Exp Dermatol, 43 (7), 766-769. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=29855062 .
- de Lera, AR, Krezel, W., & Rühl, R. (2016). An endogenous mammalian retinoid X receptor ligand, at last! ChemMedChem, 11 (10), 1027-1037. [CrossRef]
- Dresen, E., Lee, ZY, Hill, A., Notz, Q., Patel, JJ, & Stoppe, C. (2023). History of scurvy and use of vitamin C in critical illness: A narrative review. Nutr Clin Pract, 38 (1), 46-54. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=36156315 .
- EFSA Panel on Dietetic Products, N., & Allergies. (2010). Scientific Opinion on principles for deriving and applying Dietary Reference Values. EFSA Journal, 8 (3), 1458. [CrossRef]
- EFSA Panel on Dietetic Products, N., & Allergies. (2015). Scientific Opinion on Dietary Reference Values for vitamin A. EFSA Journal, 13 (3), 4028. [CrossRef]
- Efsa Panel on Nutrition, NF, Food, A., Turck, D., Bohn, T., Castenmiller, J., de Henauw, S., . . . Naska, A. (2024). Scientific opinion on the tolerable upper intake level for preformed vitamin A and β-carotene. EFSA Journal, 22 (6), e8814. [CrossRef]
- European Commission. (2006). REGULATION (EC) No 1924/2006 OF THE EUROPEAN PARLIAMENT AND OF THE COUNCIL of 20 December 2006 on nutrition and health claims made on foods. Official Journal of the European Union, L404/9 .
- European Commission. (2024). Food safety in the EU. https://european-union.europa.eu/priorities-and-actions/actions-topic/food-safety_en . accessed 31.10.2024 2024.
- European Food Safety, A. (2017). Dietary Reference Values for nutrients Summary report. EFSA Supporting Publications, 14 (12), e15121E. [CrossRef]
- Evans, R.M. (2005). The nuclear receptor superfamily: a rosetta stone for physiology. Mol Endocrinol, 19 (6), 1429-1438. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=15914712 .
- Evans, RM, & Mangelsdorf, DJ (2014). Nuclear receptors, RXR, and the big bang. Cell, 157 (1), 255-266. [CrossRef]
- Giguère, V., & Evans, RM (2022). Chronicle of a discovery: the retinoic acid receptor. J Mol Endocrinol, 69 (4), T1-t11. [CrossRef]
- Glerup, H., Mikkelsen, K., Poulsen, L., Hass, E., Overbeck, S., Thomsen, J., . . . Eriksen, E. F. (2000). Commonly recommended daily intake of vitamin D is not sufficient if sunlight exposure is limited. Journal of Internal Medicine, 247 (2), 260-268. [CrossRef]
- Haworth, W., & Hirst, E. (1933). Synthesis of ascorbic acid. J Soc Chem Ind, 52 , 645-647.
- Heyman, RA, Mangelsdorf, DJ, Dyck, JA, Stein, RB, Eichele, G., Evans, RM, & Thaller, C. (1992). 9-cis retinoic acid is a high affinity ligand for the retinoid X receptor. Cell, 68 (2), 397-406.
- IUPAC-IUB. (1982). Nomenclature of retinoids. Recommendations. Eur J Biochem, 129 , 1-5.
- Joost, HG (2012). Carl Arthur Scheunert's nutritional experiments on humans 1938–1943: A scientist's transgressions during National Socialism. Medical History Journal, 47 , 296-334.
- Kane, MA, Folias, AE, Pingitore, A., Perri, M., Obrochta, KM, Krois, CR, . . . Napoli, J.L. (2010). Identification of 9-cis-retinoic acid as a pancreas-specific autacoid that attenuates glucose-stimulated insulin secretion. Proceedings of the National Academy of Sciences of the United States of America, 107 (50), 21884-21889. [CrossRef]
- Khunti, K., Chudasama, YV, Gregg, EW, Kamkuemah, M., Misra, S., Suls, J., . . . Valabhji, J. (2023). Diabetes and Multiple Long-term Conditions: A Review of Our Current Global Health Challenge. Diabetes Care, 46 (12), 2092-2101. [CrossRef]
- Krezel, W., Rivas, A., Szklenar, M., Ciancia, M., Alvarez, R., de Lera, AR, & Ruhl, R. (2021). Vitamin A5/X, a New Food to Lipid Hormone Concept for a Nutritional Ligand to Control RXR-Mediated Signaling. Nutrients, 13 (3). http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=33809241 .
- Krężel, W., Rivas, A., Szklenar, M., Ciancia, M., Alvarez, R., de Lera, AR, & Rühl, R. (2021). Vitamin A5/X, a New Food to Lipid Hormone Concept for a Nutritional Ligand to Control RXR-Mediated Signaling. Nutrients, 13 (3), 925. [CrossRef]
- Krezel, W., Rühl, R., & de Lera, AR (2019). Alternative retinoid X receptor (RXR) ligands. Mol Cell Endocrinol, 491 , 110436. [CrossRef]
- La Frano, MR, Cai, Y., Burri, BJ, & Thilsted, SH (2018). Discovery and biological relevance of 3,4-didehydroretinol (vitamin A(2)) in small indigenous fish species and its potential as a dietary source for addressing vitamin A deficiency. Int J Food Sci Nutr, 69 (3), 253-261. [CrossRef]
- Letondal, P. (1936). The Treatment of Infantile Scurvy with Ascorbic Acid: (Preliminary Report). Can Med Assoc J, 35 (6), 646-647. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=20320471 .
- Levin, AA, Rumpfenbecker, LJ, Kazmer, S., Bosakowski, T., Huselton, C., Allenby, G., . . . et al. (1992). 9-cis retinoic acid stereoisomer binds and activates the nuclear receptor RXR alpha. Nature, 355 (6358), 359-361. [CrossRef]
- Lucas, R., Szklenar, M., Mihály, J., Szegedi, A., Töröcsik, D., & Rühl, R. (2022). Plasma Levels of Bioactive Vitamin D and A5 Ligands Positively Correlate with Clinical Atopic Dermatitis Markers. Dermatology , 1-8. [CrossRef]
- Mangelsdorf, DJ, & Evans, RM (1995). The RXR heterodimers and orphan receptors. Cell, 83 (6), 841-850. [CrossRef]
- Mascrez, B., Ghyselinck, N.B., Chambon, P., & Mark, M. (2009). A transcriptionally silent RXRalpha supports early embryonic morphogenesis and heart development. Proceedings of the National Academy of Sciences of the United States of America, 106 (11), 4272-4277. [CrossRef]
- Mascrez, B., Mark, M., Dierich, A., Ghyselinck, NB, Kastner, P., & Chambon, P. (1998). The RXRalpha ligand-dependent activation function 2 (AF-2) is important for mouse development. Development, 125 (23), 4691-4707. [CrossRef]
- Maxfiled, L., SF, D., & JS, C. (2024). Vitamin C Deficiency : StaPearls Publishing.
- Morton, RA, Salah, MK, & Stubbs, AL (1947). Retinene2 and vitamin A2. Nature, 159 (4048), 744. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=20241598 .
- NHS. (2020). Vitamin A. https://www.nhs.uk/conditions/vitamins-and-minerals/vitamin-a/ , accessed June 28, 2024 .
- NIH. (2024). Neurodegenerative diseases. https://www.niehs.nih.gov/research/supported/health/neurodegenerative , accessed October 31, 2024 .
- Rühl, R. (2006). Method to determine 4-oxo-retinoic acids, retinoic acids and retinol in serum and cell extracts by liquid chromatography/diode-array detection atmospheric pressure chemical ionization tandem mass spectrometry. Rapid Commun Mass Spectrom, 20 (16), 2497-2504. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=16862622 .
- Rühl, R., Krezel, W., & de Lera, AR (2018). 9-Cis-13,14-dihydroretinoic acid, a new endogenous mammalian ligand of retinoid X receptor and the active ligand of a potential new vitamin A category: Vitamin A5. Nutrition Reviews, 76 (12), 929-941.
- Rühl, R., Krzyzosiak, A., Niewiadomska-Cimicka, A., Rochel, N., Szeles, L., Vaz, B., . . . Krezel, W. (2015). 9-cis-13,14-dihydroretinoic acid is an endogenous retinoid acting as RXR ligand in mice. PLoS Genet, 11 (6), e1005213. [CrossRef]
- Shaish, A., Harari, A., Hananshvili, L., Cohen, H., Bitzur, R., Luvish, T., . . . Harats, D. (2006). 9-cis beta-carotene-rich powder of the alga Dunaliella bardawil increases plasma HDL-cholesterol in fibrate-treated patients. Atherosclerosis, 189 (1), 215-221. [CrossRef]
- Shantz, EM, Embree, ND, & et al. (1946). The replacement of vitamin A1 by vitamin A2 in the retina of the rat. J Biol Chem, 163 , 455-464. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=21024915 .
- Wang, XD, Krinsky, NI, Benotti, PN, & Russell, RM (1994). Biosynthesis of 9-cis-retinoic acid from 9-cis-beta-carotene in human intestinal mucosa in vitro. Arch Biochem Biophys, 313 (1), 150-155. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=8053676 .
- Waugh, W.A., & King, C.G. (1976). Nutrition classics. The Journal of Biological Chemistry, Volume XCVII, 1932, pages 325-331. Isolation and identification of vitamin C by WA Waugh and CG King. Nutr Rev, 34 (3), 81-83. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=768830 .
- WHO. (1998). Vitamin and mineral requirements in human nutrition; report of a joint FAO/WHO expert consultation . Bankok, Thailand: WHO / FAO of the UN.
- WHO/FAO Expert Group. (1967). Requirements of Vitamin A, Thiamine, Riboflavins and Niacin . Geneva.
- WHO/FAO Expert Group. (1988). Requirements of Vitamin A, Iron, Folate and Vitamin B12 : Food and Agriculture Organization of the United Nations.
- Wilson, DM, III, Cookson, MR, Van Den Bosch, L., Zetterberg, H., Holtzman, DM, & Dewachter, I. (2023). Hallmarks of neurodegenerative diseases. Cell, 186 (4), 693-714. [CrossRef]
- Zilva, SS (1935). The isolation and identification of vitamin C. Arch Dis Child, 10 (58), 253-264. http://www.ncbi.nlm.nih.gov/entrez/query.fcgi?cmd=Retrieve&db=PubMed&dopt=Citation&list_uids=21032000 .
Figure 1.
Summary of the criteria that define a vitamin (WHO, 1998) .
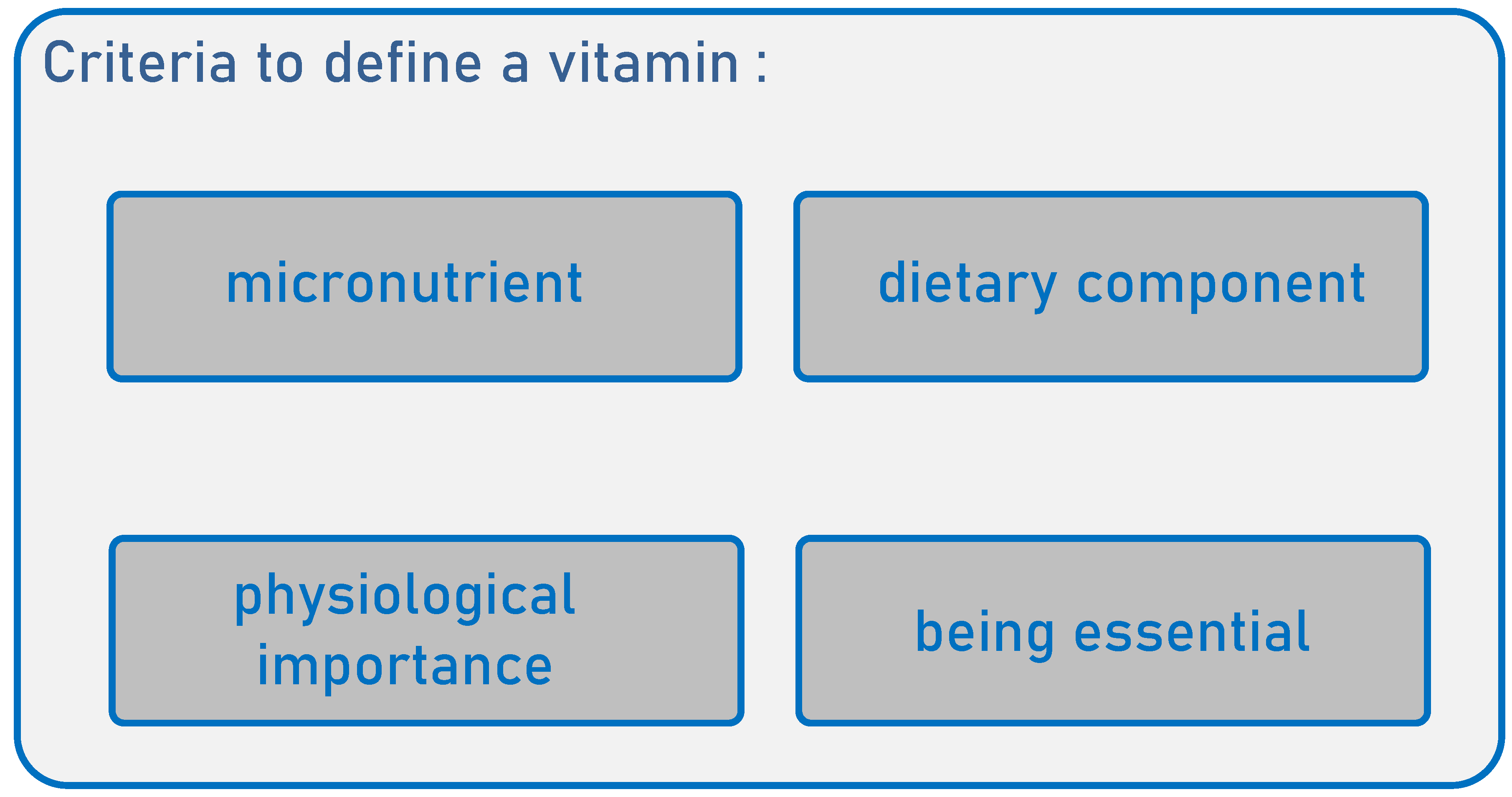
Figure 2.
The definition of vitamin A by various organizations: World Health Organization (WHO), International Union of Pure and Applied Chemistry (IUPAC) , European Food Safety Authority (EFSA), German Nutrition Society (Deutsche Gesellschaft für Ernährung, DGE), British National Health Service (NHS) and the French Agency for Food, Environmental and Occupational Safety (Agence nationale de sécurité sanitaire de l'alimentation, ANSES).
Figure 2.
The definition of vitamin A by various organizations: World Health Organization (WHO), International Union of Pure and Applied Chemistry (IUPAC) , European Food Safety Authority (EFSA), German Nutrition Society (Deutsche Gesellschaft für Ernährung, DGE), British National Health Service (NHS) and the French Agency for Food, Environmental and Occupational Safety (Agence nationale de sécurité sanitaire de l'alimentation, ANSES).
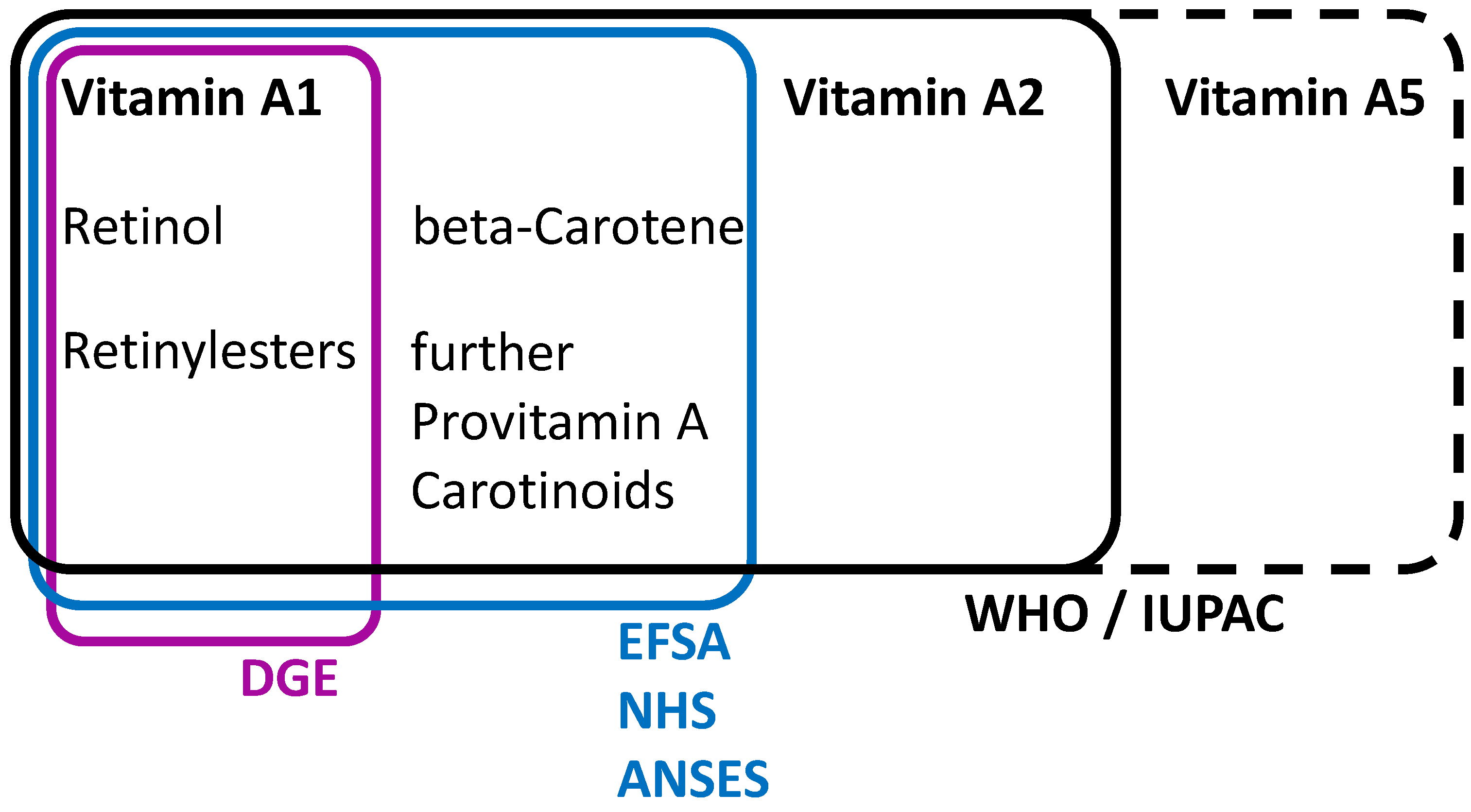
Figure 3.
Which substances belong to the categories vitamin A, vitamin A1 and vitamin A2 (modified from (Banati & Rühl, 2024) ).
Figure 3.
Which substances belong to the categories vitamin A, vitamin A1 and vitamin A2 (modified from (Banati & Rühl, 2024) ).
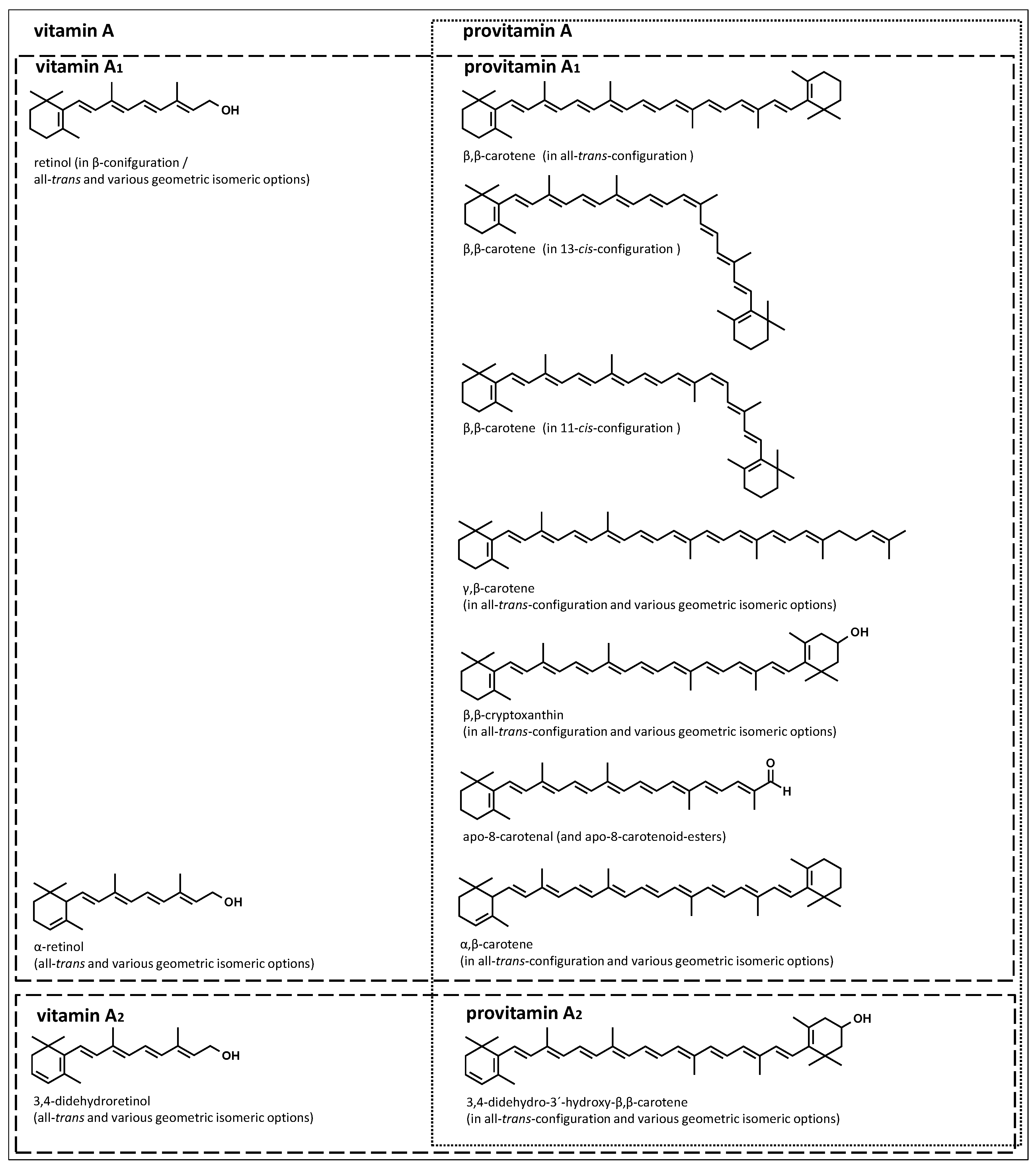
Figure 4.
Summary of RXR-controlled signaling, modified from (Banati et al., 2024) . Abbreviations: Nuclear hormone receptor (NHR), peroxisome proliferator-activated receptors (PPAR), vitamin D receptor (VDR), liver X receptor (LXR), “nuclear receptor subfamily 4 Group A Member 2" (NR4A2), retinoid X receptor (RXR), provitamin A1 (proVitA1), vitamin (Vit), all-trans-retinoic acid (ATRA) and 1,25-dihydroxy-vitamin D3 (1,25VD3).
Figure 4.
Summary of RXR-controlled signaling, modified from (Banati et al., 2024) . Abbreviations: Nuclear hormone receptor (NHR), peroxisome proliferator-activated receptors (PPAR), vitamin D receptor (VDR), liver X receptor (LXR), “nuclear receptor subfamily 4 Group A Member 2" (NR4A2), retinoid X receptor (RXR), provitamin A1 (proVitA1), vitamin (Vit), all-trans-retinoic acid (ATRA) and 1,25-dihydroxy-vitamin D3 (1,25VD3).
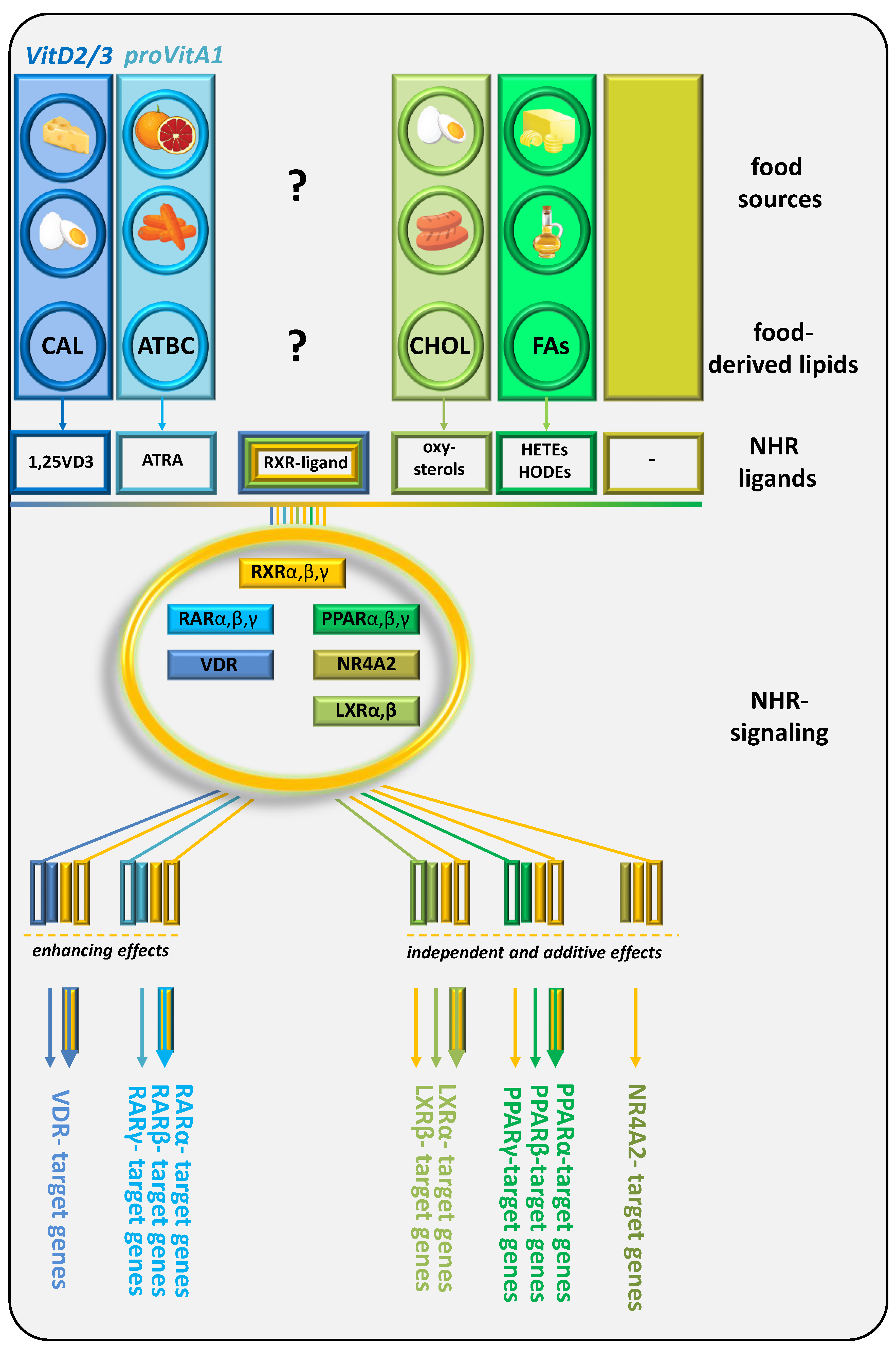
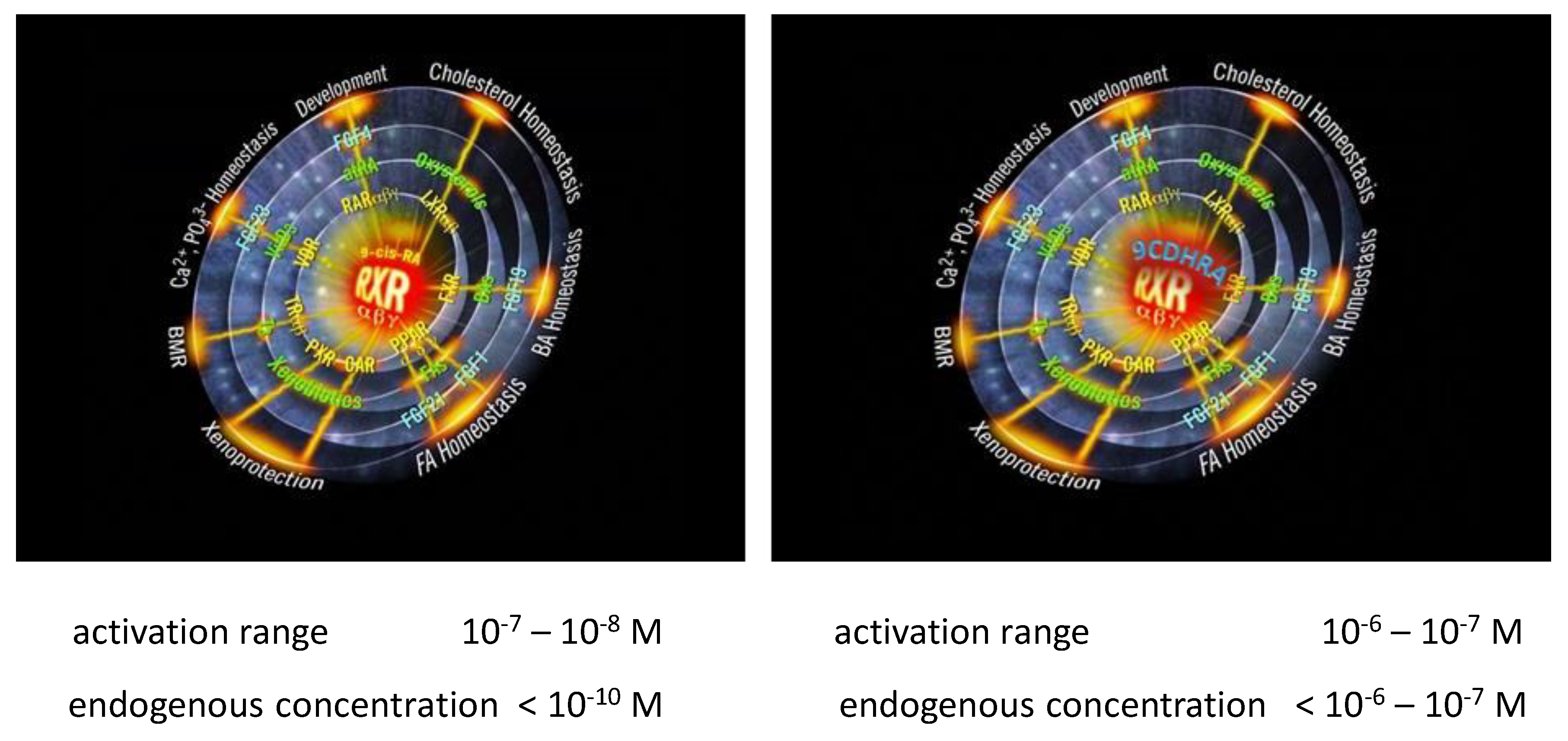
Figure 5.
Left figure, 9CRA as “BIG BANG” and right figure, 9CDHRA as “BIG BANG” for the physiologically important RXR signaling mediated by interaction with a variety of nuclear hormone receptors and their important physiological functions in the human organism (Bohn et al., 2023; Evans & Mangelsdorf, 2014).
Figure 5.
Left figure, 9CRA as “BIG BANG” and right figure, 9CDHRA as “BIG BANG” for the physiologically important RXR signaling mediated by interaction with a variety of nuclear hormone receptors and their important physiological functions in the human organism (Bohn et al., 2023; Evans & Mangelsdorf, 2014).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



