
Submitted:
05 December 2024
Posted:
05 December 2024
You are already at the latest version
Abstract
Prosthetic joint infections (PJIs) remain a significant challenge, occurring in 1% to 2% of joint arthroplasties and potentially leading to a 20% to 30% mortality rate within 5 years. The primary pathogens responsible for PJIs include Staphylococcus aureus, coagulase-negative staphylococci, and various gram-negative bacteria, typically treated with intravenous antibiotic drugs. However, this conventional approach fails to effectively eradicate biofilms or the microbial burden in affected tissues. As a result, innovative strategies are being explored to enhance the efficacy of infection prevention, through the development of antibacterial coated implants. These coatings are required to demonstrate broad-spectrum antimicrobial activity, minimal local and systemic toxicity, favourable cost-effectiveness, and support for bone healing. In the present review, the analysis of various methodologies for developing antibacterial coatings was performed, emphasizing studies that conducted in vivo tests to advance potential clinical applications. A diversity of techniques employed for the development of coatings incorporating antimicrobial agents, highlight promising avenues for reducing infection-related surgical failures.
Keywords:
Antibacterial coatings
; Antimicrobial Coatings
; Surface Treatments
; Antibacterial Surfaces
; Implants
; Biomedical Implants
1. Introduction
Improvements in routine perioperative antibiotic administration have been shown to be effective in reducing the incidence of infection after orthopedic surgery. However, infections after knee and total hip arthroplasty are still one of the main causes of implanted biomaterial failure [1,2]. Prosthetic joint infection (PJI) occurs in 1% to 2% of all joint arthroplasties and can lead to death within 5 years in 20% to 30% of cases [3,4]. Infections also occur in patients who have undergone elective procedures (0.7 to 4.2%) or with exposed fractures (5 to 33%) [5,6].
Furthermore, the costs of treating PJI are very high. Data indicate that the costs of treating PJI after hip and knee replacements can exceed $80,000 and $100,000, respectively [7,8,9]. The graph in Figure 1 displays data from literature about the costs of treating PJI after Total Hip Arthroplasty (THA) and Total Knee Arthroplasty (TKA) in several countries between 2008 and 2019 [7,10,11]. Likewise, some estimates show that the annual cost of treating PJI of the knee and hip will exceed $1.85 billion in the US [12,13].
Most prosthetic joint infections are caused by Staphylococcus aureus, coagulase-negative staphylococci, or gram-negative strains and are treated with intravenous cefazolin [3,14,15,16]. However, this strategy is not effective in eradicating biofilms from the materials or the S. aureus bioburden from the affected tissues [3]. PJI cases are more common immediately after surgery. However, they can develop months or even years after the new material is implanted [17]. Therefore, strategies for obtaining materials with long-lasting antimicrobial activity must also be considered [9,18].
Thus, new strategies are being proposed to reduce the failure rate of surgeries caused by infections. These strategies involve promoting bactericidal properties to implant surfaces passively or actively [19]. Passive surface modifications aim to control bacterial adhesion by modifying surface topography, such as wettability and roughness [19,20]. On the other hand, active strategies aim to load the surface of implants with antibiotic or antiseptic agents [1]. Furthermore, the coatings would have to act against a broad spectrum of microorganisms, not present local or systemic toxicity, have excellent cost-benefit, and ensure bone healing [21].
Therefore, this review aims to analyze the literature on various strategies for developing bactericidal surfaces - an area of paramount importance for clinical applications, particularly in orthopaedics. Our primary focus was on studies that report in vivo results, as these represent a critical step toward the clinical translation of newly developed materials. Given the relatively limited number of in vivo studies, our reference list includes 102 selected sources, prioritizing those with direct relevance to clinical outcomes.
The current literature addresses predominantly coatings and surface-modified implants. To organize our review, we divided the review into sections related to coatings and surface-treated implants with antibacterial properties. The first chapter is structured according to the types of bactericidal agents used in coatings, specifically antibiotics and disinfectants. The second chapter provides an in-depth overview of both in vitro and in vivo tests performed on implants with functionalized surfaces. Finally, we explore future perspectives, focusing on potential developments and emerging trends in the field.
2. Antibacterial Strategies Applied on Coatings
Bactericidal coatings have emerged as a promising solution to prevent infections in hip and joint arthroplasty procedures, where bacterial contamination is a significant complication. In vivo studies are crucial to evaluating these coatings' effectiveness in biological environments, offering better information about their ability to combat bacterial infections and promote implant osseointegration.
Therefore, this section focused on the literature review of implant coatings used in arthroplasties to determine their in vivo bactericidal efficacy. Figure 2 categorizes the collected papers based on the bactericidal agent and types of microorganisms tested.
Among antibiotics, ten articles studied the use of gentamicin [20,22,23,24,25,26,27,28,29,30], six used vancomycin [29,31,32,33,34,35], four worked with rifampicin [31,36,37,38], four with linezolid [31,36,37,39], and two with tobramycin [29,36]. The drugs daptomycin [31], berberine [40], ceftriaxone [36], cefazolin [36], cefepime [36], piperacillin [36], tazobactam [36], clindamycin [36], minocycline [38] and tigecycline [32] were used in only 1 study.
Another group of papers investigated the use of certain disinfectants in coatings as part of the bactericidal strategy. Twelve of them used silver [20,41,42,43,44,45,46,47,48,49,50,51], four studied the use of copper [52,53,54,55], two added magnesium oxide (MgO) [55,56], chlorhexidine [9,22] or iodine [57,58] to the coatings, and one paper used Cationic Steroidal Antimicrobial-13 (CSA13) [59], phage [39], Mouse Beta-Defensin-14 (MBD-14) [60], selenium[61], or XPerience (XP) [12].
The microorganisms used in the analyzed papers include Staphylococcus aureus [12,20,23,25,26,28,30,31,32,34,35,36,38,40,42,43,54,55,56,57,60,62], Methicillin-Resistant Staphylococcus aureus (MRSA) [9,22,33,37,39,48,49,51,52,59], Escherichia coli [9,12,22,28,30,42,57], Staphylococcus epidermidis [9,12,22,40,51], Pseudomonas aeruginosa [12,22,60], Methicillin-Resistant Staphylococcus epidermidis (MRSE) [9], Enterococcus faecalis [12], Cutibacterium acnes [12], Streptococcus pyogenes [22], Staphylococcus capitis [53], Enterobacter cloacae [12], Acinetobacter baumannii [9], Candida albicans [12], and Candida tropicalis [12].
Finally, Figure 3 illustrates that, among the selected articles, 56% of the coatings were made of polymers and 44% of ceramics. Furthermore, among polymeric coatings, most bactericidal agents used were antibiotics (82%), while for ceramic coatings, more disinfectants were utilized (68%).
2.1. Use of Different Bactericidal Agents
2.1.1. Antibiotics
The use of antibiotics before, during, and after surgery is a standard practice in orthopedic procedures [63]. Furthermore, research is being conducted on techniques for local antibiotic application to reduce the surgical infection rate. However, the presence of antibiotics around the implant is short-lived and may not be as effective against biofilm formation [32].
Using antibiotics loaded in coatings is advantageous as it reduces systemic toxicity [64]. However, using low doses of drugs for prolonged periods can be harmful, causing the development of drug-resistant strains [64]. Therefore, one strategy to prevent post-surgical infection is to improve the loading and release of drugs from the implant coatings.
Every antibiotic has a specific mechanism of action and targets different parts or processes of the bacterial cell, as illustrated in Figure 4 [65,66].
Gentamicin is an antibiotic known for its thermostability and efficacy in a broad bacterial spectrum, covering gram-positive and gram-negative bacteria [23,28,67,68]. Furthermore, it has good bone penetration [64] and helps prevent infections shortly after surgery [69], which makes it favorable for local antibiotic applications in orthopedic surgeries.
Another antibiotic used in biomedical implant coatings is vancomycin. It has bactericidal efficiency against many bacteria, including MRSE and MRSA [70]. Consequently, it is normally used to treat more serious infections caused by gram-positive bacteria and prevent and treat osteomyelitis cases [71,72]. Furthermore, vancomycin is also widely used to treat osteoarthritis [35,73].
The third most used antibiotic among the selected papers was Rifampicin. According to the literature, it is effective against Staphylococcus species [74,75] and is commonly used to treat early infections [76,77]. However, there is concern about the development of bacteria resistant to Rifampicin when this antibiotic is used alone [31,37]. Therefore, one solution is to apply a combination of Rifampicin and another type of antibiotic to the coatings [31,37].
Linezolid is a bacteriostatic agent that inhibits the formation of the initiation complex during bacteria's protein synthesis phase [39]. Its use against infections after joint prosthesis placement is favored by its great efficacy against Gram-positive and drug-resistant strains, good tissue and bone penetration, and high bioavailability (it can be taken orally or intravenously) [39,78,79,80,81].
Min et al. [25] studied Polyetheretherketone (PEEK) implants coated with multilayers containing gentamicin and osteoinductive growth factor (BMP-2). The implants were placed in the tibias of adult male rats and tested against S. aureus Xen 29, which is 20 times more resistant to gentamicin than general strains. The antibiotic-treated group manifested little or no expression of S. aureus after 8 weeks post-revision. Furthermore, the growth factor led to over 80% bone coverage after 3 weeks of revision.
Matsuno et al. [26] investigated coating Ti-6Al-4V, CoCrMo, and stainless steel with a hyaluronic acid gel containing gentamicin. The gel was chosen because it is bioabsorbable and biocompatible. In vivo studies showed a bactericidal effect up to 2 weeks after surgery. The authors presented results relating to 2 animal models. The mouse model results showed that the fractures were healed, and the gentamicin-containing material prevented osteomyelitis. In the rabbit model, the osseointegration of the implant was not impaired by the coating. However, the material did not appear to be effective against forming biofilms and other more serious cases of infection.
Alt et al. [27,82] studied the effects of gentamicin on hydroxyapatite coatings produced on steel implants by an electrochemically assisted process. Rabbit model studies showed that the coatings effectively reduced S. aureus infection rates in 19 animals up to 4 weeks after surgery [82]. The authors also showed no significant difference in bone formation between the implant without and with gentamicin [27]. However, they observed a trend towards decreased new bone formation after 4 and 12 weeks of surgery with coatings containing gentamicin [27]. This may be because antibiotics, such as gentamicin, have been associated with impairments in the functioning of osteoblasts, influencing the osseointegration of implants [83,84,85,86].
Stavrakis et al. [32] developed a biodegradable poly(ethylene glycol)-poly(propylene sulfide) (PEG-PPS) coating that can be used for antibiotic delivery. The authors tested vancomycin and tigecycline as antibiotics loaded in the produced coating and used titanium as the material to be coated. The in vivo results showed the great efficiency of the coatings in preventing the colonization of S. aureus on the implant's surface and the surrounding bone and joint tissue after surgery. However, the results presented were better when using tigecycline. Furthermore, the bactericidal efficacy of this coating is limited to a short period after implantation. This is because the coating was designed to be biodegradable within 14 days. This way, it does not interfere with the osseointegration of the implant and does not provide an additional surface for bacteria to lodge.
Giavaresi et al. [33] studied the bactericidal efficacy of a bioresorbable hydrogel coating loaded with vancomycin. In vitro results determined that over 80% of the vancomycin was released in the first 24 h. In vivo tests showed that the coating significantly reduced the MRSA bacterial load at the implant/bone interface after 7 days of surgery.
Boot et al. [34] analyzed the bactericidal efficiency of a hydrogel coating loaded with vancomycin and two other non-antibiotic agents (bioactive glass (BAG) and N-acetyl-L-cysteine (NAC)) against S. aureus. This study placed hydrogel coatings on the surface of titanium implants. In vivo results showed that vancomycin-loaded coatings reduced the severity of infections and improved bone-to-implant contact. Compared to the hydrogel-implanted group, the BAG- and NAC-loaded coatings did not significantly reduce infection after surgery. However, applying local antibiotics was insufficient to eliminate the entire bacterial load.
Fang et al. [35] produced a hybrid layer on the surface of an acetabular cup made of ultra-high molecular weight polyethylene (UHMWPE), using the traditional hot-pressing process and acid treatment to bond with a porous titanium layer loaded with vancomycin. to evaluate the method's efficiency against the bacterial activity of S. aureus for 7 days after subcutaneous implantation in rats (Figure 5.a). The authors demonstrated that the number of bacteria following the in vivo testing period was two orders of magnitude lower when the implant contained vancomycin than when it did not (Figure 5.b). Furthermore, parallel set of tests conducted on Labrador dogs demonstrated biocompatibility and new bone formation capability after 3 months. The authors highlighted that this biofunctionalized polymer can produce promising benefits when used in artificial joint prostheses at long-term implantation.
Ashbaugh et al. [31] developed a polymeric coating of poly(lactic-coglycolic acid) (PLGA) and poly(ε-caprolactone) (PCL) loaded with different combinations of antibiotics (rifampicin + vancomycin or rifampicin + linezolid or rifampicin + daptomycin) via electrospinning and applied to titanium wires. All combinations effectively prevented biofilm formation on the implant and inhibited bone changes caused by infections. Nevertheless, the combinations of rifampicin + linezolid and rifampicin + daptomycin had better efficacy due to a possible reduction in the bactericidal activity of vancomycin in biofilms with increased cell wall thickness.
Miller et al. [37] produced a PLGA and PCL nanofiber coating loaded with a combination of rifampicin and linezolid via electrospinning. Nanofibers were used to coat titanium implants and used in rabbit surgeries. The authors measured the width of the mice's knees 7 days after surgery to determine infection-induced inflammation. There were no changes in the animals treated with the implant loaded with antibiotics, while the group without antibiotics showed a 36% increase in the knee. They also found that the bioluminescence signals of MRSA were significantly greater when using implants without antibiotic loading.
2.1.2. Disinfectants
Another strategy for manufacturing bactericidal coatings is the release of bioactive ions, such as magnesium, silver, copper, zinc, and strontium. These ions help promote osseointegration, tissue regeneration, and vascularization [42,87,88,89].
In general, metal ions and nanoparticles penetrate and destroy the cell membrane, which can lead to the formation of reactive oxygen species (ROS), which damage proteins and DNA and induce oxidative stress [90,91], as illustrated in Figure 6.
Silver ions can neutralize the colonization of microorganisms on the surface of implants, which results in the non-formation of biofilm [92]. This occurs due to the interaction of ions with the DNA and metabolic enzymes of microorganisms, leading to difficulty in replication and cell death [93,94,95,96]. Silver has high toxicity to a wide spectrum of bacteria and a low risk of developing resistance [42,97,98]. Therefore, very small amounts of this agent are sufficient for the bactericidal effect to be manifested, which reduces the risk of toxic effects against human cells [92,97,99].
Copper is another metal widely used for its bactericidal effects against both gram-positive and gram-negative bacteria [100,101]. It has already been reported that copper has a “contact-killing” effect on bacteria, leading to cytoplasmic membrane damage and DNA degradation [52,100,102]. Furthermore, copper stimulates osteogenesis and angiogenesis, making it a good bone-formation agent [52,103].
Magnesium is an essential element for the human body, contributing to the formation of new bones [56,104]. However, magnesium is also important for bacterial metabolism, making its use difficult in implants whose bactericidal properties are required [56]. One way forward is the use of magnesium oxides, which are alkaline and thus induce bacterial oxidative stress, killing microorganisms [105,106]. Furthermore, MgO increases osteogenesis and bone remodeling processes [55].
Yang et al. [42] incorporated silver and manganese ions into the surface of a PEEK material. Two weeks after implantation of the material into S. aureus-infected mice, the interface of the PEEK material containing manganese and silver contained the greatest amount of new bone compared to materials containing only manganese or without any metallic components. Furthermore, histological analysis using Masson's trichrome staining (Figure 7.a) and Giemsa staining (Figure 7.b) revealed that no infection occurred around the silver-containing implant, and fewer fibrous tissues appeared at the interface with the bone.
Zeng et al. [43] tested the bactericidal effect of a TiO2 nanotube coating containing Ag2O nanoparticles on animals infected by S. aureus after artificial joint replacement surgery. The results showed that the silver-containing implants were effective in controlling the infection and presented excellent bactericidal properties.
Eto et al. [46], Akiyama et al. [48], and Shimazakiet et al. [49] prepared silver-containing hydroxyapatite coatings on titanium via the thermal-spray method. The results showed low osteoconductivity of the uncoated implant surface after two weeks of implantation, unlike the coated surfaces [46]. Furthermore, the number of viable MRSA was significantly lower for silver-containing implants after 72 h of surgery [48,49].
Devlin-Mullin et al. [51] developed titanium scaffolds using selective laser melting (SLM) and covered them with a silver nanolayer via atomic layer deposition (ALD). Their in vivo results show that the implants induced osteogenesis and angiogenesis, showing no evidence of toxicity.
Huo et al. [52] developed a coating via electrophoretic deposition (EPD) composed of chitosan and a bioactive copper-doped glass. The authors also used titanium implants to be covered by the material. All groups of rats implanted with copper-containing materials showed less destruction of the femur after 3 weeks of surgery. Copper implants also reduced the severity of implant-related infections observed in rats implanted with pure titanium. Finally, the bacterial load in rat femurs was also reduced when copper-containing implants were used.
Mauerer et al. [54] investigated the bactericidal properties of a Ti-6Al-4V spacer coated, via dip coating, with TiO2 doped with copper. After revision surgery, the insertion of copper-containing spacers demonstrated good results against MRSA infection.
Tan et al. [56] developed a coating on titanium via magnetron sputtering, containing Ca-O-Ti in the inner layer and MgO in the outer layer. After 6 weeks of implantation, the MgO-containing materials showed no obvious bone destruction and only a small amount of bacteria adhered to the coating. On the other hand, femurs implanted with uncoated titanium showed clear signs of infection. Finally, the MgO-coated implants were almost completely covered by new bone.
The literature reviewed in this section highlights the number of bactericidal agents used in implant coatings, including antibiotics such as gentamicin, vancomycin, and rifampicin, as well as disinfectants like silver, copper, and magnesium oxide. The microorganisms tested in these studies span a wide spectrum, with a particular focus on common pathogens such as Staphylococcus aureus, Escherichia coli, and Methicillin-Resistant Staphylococcus aureus, underscoring the need for coatings that can effectively combat both Gram-positive and Gram-negative bacteria.
Additionally, the analysis of polymeric and ceramic coatings reveals distinct trends in bactericidal strategies. Polymeric coatings predominantly utilized antibiotics (82%), while ceramic coatings were more likely to incorporate disinfectants (68%), suggesting different approaches to achieving long-lasting antimicrobial effects based on the material properties of the coatings.
In conclusion of this section, while significant progress has been made in the development of antibacterial coatings for joint arthroplasty, further research, particularly in clinical trials and more advanced in vivo models, is essential to optimize these coatings for both infection prevention and enhanced implant integration. Future studies should continue to explore novel bactericidal agents and material combinations to improve the overall effectiveness of these coatings in clinical practice.
3. In-Vitro and In-Vivo Experimental Approaches for Surface-Treated Implants with Antibacterial Properties
3.1. In-Vitro
New strategies for antimicrobial surface coating and treatment of biomaterials have been extensively reported in the literature. Being the studies mainly focused on metallic materials for use as implants and using conventional commercial techniques, such as those evolving mechanical, electrochemical, physical, or plasma methods, to produce bacteriostatic or bactericidal surfaces. Furthermore, the in vitro antimicrobial activity and biofilm formation testing have been the first choice for an initial screening of the bacteria and surface interaction.
Yoda et al. [107] investigated the adhesion ability of S. Epidermidis as distinct levels of surface roughness by using in vitro tests. The study grouped distinct commercial metallic biomaterials, such as oxidized zirconium-niobium (Oxinium), cobalt-chromium-molybdenum alloy (Co-Cr-Mo), Ti-6Al-4V alloy, commercially pure titanium grade 2 (CP-Ti), and stainless steel (SUS316L). The surface roughness was altered by polishing with diamond slurry, being the samples later divided into fine (Ra ~ 10 nm) and coarse (Ra ~ 30 nm) groups. The in vitro tests conducted after 48 hours of incubation demonstrated that S. Epidermidis tended to have better adhesion in the course group than the fine one. However, the hydrophobic behavior of the Co-Cr-Mo sample contributed to providing lesser bacteria adhesion when compared to the other biomaterials. The authors pointed out that this study shed some light on the minimal level of roughness needed to provide a reasonable impact on the bacteria adhesion in metallic implants. While Ma et al. [108] studied the potential usage of TiO2 nanotubes for drug delivery system of antimicrobial peptides (AMPs). The nanotubes were grown on CP-Ti grade 2 by using anodizing treatment at 30 V, for 6 hours, in an ethylene glycol (C2H6O2) solution with 0.27M of ammonium fluoride (NH4F). Then, the AMPs were incorporated into the nanotubes by immersion of the anodized titanium samples in a phosphate buffer solution enriched with the AMPs. The results indicated that the anatase TiO2 had better efficiency for the AMP loading, having drug releasing a significant effect on reducing the activity and adhesion of S. Aureus in the in vitro tests. And Guastaldi et al. [109] investigated the biological effects of the Ti-15Mo (wt.%) alloy surface after laser-beam irradiation. The surface was treated by using a Yb:YAG laser beam, operating with a density power of 1.9 J·cm-2, pulse frequency in the range of 20 and 35 kHz, and exposure area of 14 mm2. The in vitro tests indicated an expressive effect on the adhesion of methicillin-resistant Staphylococcus Aureus (S. Aureus) when compared to the commercially pure titanium (CP-Ti) grade 2 treated under the same conditions. The authors stated that the laser-beam irradiation produced a homogeneous micro-roughness on the surface which affected the physicochemical properties and antibacterial performance of the materials. Finally, Zaatreh et al. [16] investigated the antibacterial ability of Mg-based coatings on the biomedical Ti-6Al-4V alloy produced by magnetron sputtering. The results indicated that the level of biofilm and colony-forming units of Staphylococcus Epidermidis (S. Epidermidis) significantly decreased while the human osteoblastic cells had a pronounceable growth after 7 days of in vitro co-culture.
3.1. In-Vivo
All the studies evolving in vitro testing have a consensus that further in vivo tests are needed for a better view of the benefits of these innovative surfaces for the next generation of biomedical implants. In this scenario, the scarce papers reporting in vivo antimicrobial testing are mainly focused on metals and polymers coated with a combination of bactericidal ions or antibiotics and their interaction with gram-positive bacteria lineages.
For example, Ständert et al. [20] investigated the in vitro cytocompatibility, as well as the in vivo biocompatibility and antimicrobial ability of CP-Ti grade 5 samples submitted to a laser treatment and enrichment of Ag particles and gentamicin. The authors produced a micro-scaled porous surface by using a Nd:YAG laser, at 100 W, then used a sputtering chamber to embed Ag particles on the top of the pores, and finally loaded the inner region of the pores with gentamicin. The in vitro results indicated the surface-treated samples possessed a unique combination of proper cell viability and differentiation of primary human osteoblastic cells, evaluated after 3 to 4 days of incubation, and enhanced osteointegration ability, drug releasing ability, and antimicrobial effectivity against S. Aureus after 3 days of culturing. While the in vivo tests, performed in Sprague Dawley rats after 28 days of surgery, indicated a clear reduction of histopathological bone destruction signs and the absence of bacteria colonization or infection of S. Aureus. The authors pointed out that this surface treatment methodology can also be applied to other kinds of antibiotics, being a useful tool to fight against the implant-associated infections of orthopedical implants and artificial prostheses.
Liu et al. [23] exploited the antibacterial effect and bone cell biocompatibility of nanotubular anodized titanium loaded with gentamicin by using in vivo tests. The nanotube array was prepared by electrochemical anodization method performed in 0.09 M NH4F added to ethylene glycol with 10% of water, at 60 V, for 30 minutes. The in vivo tests were conducted in New Zealand White rabbits during 6 weeks of implantation. The results indicated that the surface-treated samples diminished implant-related osteomyelitis and improved bone biocompatibility. Furthermore, the surface-treated samples depicted less bacterial growth of S. Aureus than the bare material, having the potential to prevent local infections for joint replacement surgeries.
Considering now the biopolymers, there are also outstanding contributions regarding in vivo testing of antimicrobial surfaces. As example, Sang et al. [28] coated the surface of polyetheretherketone (PEEK) with silk protein-gentamicin and enriched the bulk with SrCO3 nanoparticles, using traditional processing methods of chemical immersion. In vivo tests in Sprague Dawley rats indicated strong osteogenic activity and antibacterial abilities against S. Aureus, being further confirmed by in vitro tests. The authors noticed that this new innovative approach for surface modification of the PEEK can be useful for the processing of a novel generation of orthopedic implants. In the study of Sang et al. [40], the same strategy was used to coat PEEK with silk fibroin and load the bulk with osthole and berberine compounds. The in vivo tests performed in Sprague Dawley rats for 10 weeks indicated that the samples possessed adequate osteogenesis, prevented endophytic infection, avoided bacterial adhesion of S. Aureus, and exhibited a significant killing effect of suspended bacteria around it. The authors concluded that this biofunctionalized PEEK also has potential for use in orthopedy.
Li et al. [110] produced a novel hydrogel, with a multi-hydrogen bond network structure, enriched with polyvinyl alcohol, N-carboxyethyl chitosan, agarose, and silver nanowires (Figure 8). The material was produced by conventional sol-gel synthesis with the aim to provide innovative drug release and bone regeneration. After that, the hydrogel was embedded in a 3D printed porous titanium alloy and evaluated in vivo in New Zealand White rabbits, under the osteoporosis model, after 3 months. The results were supported by in vitro tests, which confirmed the positive effect on cell proliferation, survival, osteogenic differentiation of bone mesenchymal cells, and also the antibacterial effect against normal and methicillin-resistant S. Aureus. The authors pointed out that this novel processing route can be an efficient strategy to produce novel prosthetic interfaces to avoid complications in patients with osteoporosis submitted to arthroplasty surgery.
Furthermore, some ongoing studies have also focused on the in vivo testing of hybrid materials produced by advanced processing methods. To cite, Ciliveri and Bandyopadhyay [55] pioneering employed metal additive manufacturing techniques (directed energy deposition and selective laser melting) to produce Ti-based samples enriched with MgO and Cu. Then, the authors evaluated the in vitro and in vivo biological aspects of the samples, focusing on their biocompatibility, osteogenesis, and antimicrobial aspects. The in vivo tests, conducted in Sprague Dawley rats during 2 weeks of implantation, indicated that the MgO addition promptly stimulated that bone mineralization and bone-implant strength, while the Cu presence promoted a pronounceable efficacy against S. Aureus without evident cytotoxic effect. The authors highlighted that the designed samples can be useful for the manufacturing of advanced biomedical implants, with superior osseointegration and antimicrobial capabilities.
It is possible to point out that the reduced number of in vivo antimicrobial testing studies has some drawbacks to be surpassed. For example, the studies are mainly focused on bactericidal strategies based on ion or drug releasing, despite bacteriostatic ones. Furthermore, they are restricted to small animal models (rat and rabbit) that still do not reproduce entirely the complex biological nature of the human body. And also, the studies only focused on gram-positive bacteria, without evaluation of gram-negative lineages, or even other microorganisms (viruses and fungi). In this sense, it is important to know the current clinical needs in the experiment design of novel biomaterials., Alaee et al. [1] reported some important consensus related to orthopedic infections during the surgical procedure. The report details clinical issues related to the changing knife blade, surgical duration, operational room, antibiotic-coated implants, implant size and volume, C-arm contamination, robotics and computer-assisted surgeries, and also patient-specific instrumentation. This kind of report is crucial to summarize the current understanding for prevention of bacterial infection in patients submitted to implantation surgeries and should be considered in further research in the field.
To summarize this chapter, in vitro studies focused on various surface treatments, including mechanical, electrochemical, and plasma methods, aimed to create bactericidal surfaces. In vivo studies, however, remain limited but essential for validating these surface treatments. More in vivo studies, particularly in terms of using a wider range of bacteria, including also resistant hospital strains, are needed. Current studies predominantly use small animal models, which may not fully reproduce human conditions. Moving forward, these issues should be taken into account.
4. Conclusions and Future Prospectives
The growing concern about infections associated with biomedical implants has driven the development of new antimicrobial coating and treatment strategies for biomaterials.
Although in vitro studies have significantly advanced our understanding of the interaction between surfaces and microorganisms, the limited number of in vivo studies hinders the full validation of these innovations. In vivo testing is crucial for assessing the effectiveness of these coatings, offering valuable insights into their antibacterial properties and their ability to facilitate successful implant osseointegration.
The data obtained in this review suggests that, while the current focus is on conventional techniques and metallic materials, a more comprehensive approach should include the exploration of biopolymers and advanced hybrids. Recent research indicates that the use of TiO2 nanotubes, laser treatments, and coatings with biofunctionalized polymers, such as PEEK, offer promising antimicrobial properties and biocompatibility, although most investigations still focus on Gram-positive bacteria, such as S. aureus.
Furthermore, integrating clinical knowledge into biomaterials research is crucial for developing effective solutions that meet real-world needs in the surgical environment. Collecting data on operational factors and clinical complications associated with infections should guide the design of experiments that target both antimicrobial efficacy and long-term implant safety and functionality. Therefore, for new antimicrobial surfaces to be effectively implemented in clinical practice, a concerted effort to overcome the current limitations of biomaterials research is necessary, establishing a continuous dialogue between material science, clinical applications, and patient needs.
To advance this field, future research should focus on developing multidisciplinary approaches that integrate materials engineering, microbiology, and biomedicine. It is essential to investigate new combinations of antimicrobial agents and explore innovative surface modification methods that can inhibit bacterial adhesion without compromising biocompatibility. In addition, using more complex animal models representative of human physiology can provide more robust data on the efficacy and safety of new biomaterials. The application of emerging technologies, such as 3D printing and nanotechnology, can also open new frontiers in the design of personalized implants that meet the specific needs of patients. Finally, continued collaboration between industry, academia, and healthcare institutions will be essential to translate scientific discoveries into practical and innovative solutions for preventing infections in biomedical implants.
Author Contributions
For research articles with several authors, a short paragraph specifying their individual contributions must be provided. The following statements should be used “Conceptualization, G.C.C., D.R.N.C., M.F., E.V.P.. and J.V.R..; formal analysis, G.C.C., D.R.N.C.; resources, C.R.G., AND J.V.R.; data curation, G.C.C., D.R.N.C., and M.F.; writing—original draft preparation, G.C.C., D.R.N.C., and J.V.R.; writing—review and editing, M.F., E.V.P. I.V.A., C.R.G., and J.V.R.; visualization, G.C.C.; supervision, C.R.G., J.V.R.; project administration, J.V.R.; funding acquisition, D.R.N.C, and C.R.G. All authors have read and agreed to the published version of the manuscript.”.
Funding
Please add: This study was funded by the Coordination of Superior Level Staff Improvement (CAPES; grants #88887.716787/2022-00 and #88887.898681/2023-00), National Council for Scientific and Technological Research (CNPq; grant #404020/2023-2), and São Paulo Research Foundation (FAPESP; grants #2021/15018-9 and #2024/03148-3) funding agencies.
Data Availability Statement
The obtained data are available upon a reasonable request to the corresponding author.
Conflicts of Interest
The authors declare that they are not aware of competition for financial interest or personal relationships that may have influenced the work reported in this paper.
References
- Alaee, F.; Angerame, M.; Bradbury, T.; Blackwell, R.; Booth, R.E.; Brekke, A.C.; Courtney, P.M.; Frenkel, T.; Silva, F.R.G.; Heller, S. General assembly, prevention, operating room-surgical technique: proceedings of international consensus on orthopedic infections. The Journal of Arthroplasty 2019, 34, S139–S146. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Osman, K.; Green, G.; Haddad, F.S. The epidemiology of failure in total knee arthroplasty. The Bone & Joint Journal 2016, 98-B, 105–112. [Google Scholar] [CrossRef]
- Irwin, S.; Wang, T.; Bolam, S.M.; Alvares, S.; Swift, S.; Cornish, J.; Williams, D.L.; Ashton, N.N.; Matthews, B.G. Rat model of recalcitrant prosthetic joint infection using biofilm inocula. Journal of Orthopaedic Research 2023, 41, 2462–2473. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Lau, E.C.; Son, M.-S.; Chang, E.T.; Zimmerli, W.; Parvizi, J. Are We Winning or Losing the Battle With Periprosthetic Joint Infection: Trends in Periprosthetic Joint Infection and Mortality Risk for the Medicare Population. The Journal of Arthroplasty 2018, 33, 3238–3245. [Google Scholar] [CrossRef] [PubMed]
- Barger, J.; Fragomen, A.T.; Rozbruch, S.R. Antibiotic-Coated Interlocking Intramedullary Nail for the Treatment of Long-Bone Osteomyelitis. JBJS Reviews 2017, 5, e5. [Google Scholar] [CrossRef] [PubMed]
- Schmidmaier, G.; Lucke, M.; Wildemann, B.; Haas, N.P.; Raschke, M. Prophylaxis and treatment of implant-related infections by antibiotic-coated implants: a review. Injury 2006, 37, S105–S112. [Google Scholar] [CrossRef]
- Szymski, D.; Walter, N.; Hierl, K.; Rupp, M.; Alt, V. Direct Hospital Costs per Case of Periprosthetic Hip and Knee Joint Infections in Europe — A Systematic Review. The Journal of Arthroplasty 2024, 39, 1876–1881. [Google Scholar] [CrossRef] [PubMed]
- Kurtz, S.M.; Lau, E.; Schmier, J.; Ong, K.L.; Zhao, K.; Parvizi, J. Infection Burden for Hip and Knee Arthroplasty in the United States. The Journal of Arthroplasty 2008, 23, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Perni, S.; Alotaibi, H.F.; Yergeshov, A.A.; Dang, T.; Abdullin, T.I.; Prokopovich, P. Long acting anti-infection constructs on titanium. Journal of Controlled Release 2020, 326, 91–105. [Google Scholar] [CrossRef]
- Dal-Paz, K.; Oliveira, P.R.D.; Paula, A.P.d.; Emerick, M.C.d.S.; Pécora, J.R.; Lima, A.L.L.M. Economic impact of treatment for surgical site infections in cases of total knee arthroplasty in a tertiary public hospital in Brazil. Brazilian Journal of Infectious Diseases 2010, 14. [Google Scholar]
- Kurtz, S.M.; Higgs, G.B.; Lau, E.; Iorio, R.R.; Courtney, P.M.; Parvizi, J. Hospital Costs for Unsuccessful Two-Stage Revisions for Periprosthetic Joint Infection. The Journal of Arthroplasty 2022, 37, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Bashyal, R.K.; Mathew, M.; Bowen, E.; James, G.A.; Stulberg, S.D. A Novel Irrigant to Eliminate Planktonic Bacteria and Eradicate Biofilm Superstructure With Persistent Effect During Total Hip Arthroplasty. The Journal of Arthroplasty 2022, 37, S647–S652. [Google Scholar] [CrossRef] [PubMed]
- Premkumar, A.; Kolin, D.A.; Farley, K.X.; Wilson, J.M.; McLawhorn, A.S.; Cross, M.B.; Sculco, P.K. Projected Economic Burden of Periprosthetic Joint Infection of the Hip and Knee in the United States. The Journal of Arthroplasty 2021, 36, 1484–1489.e1483. [Google Scholar] [CrossRef] [PubMed]
- Guo, G.; Wang, J.; You, Y.; Tan, J.; Shen, H. Distribution characteristics of Staphylococcus spp. in different phases of periprosthetic joint infection: A review (Review). Exp Ther Med 2017, 13, 2599–2608. [Google Scholar] [CrossRef] [PubMed]
- Ravi, S.; Zhu, M.; Luey, C.; Young, S.W. Antibiotic resistance in early periprosthetic joint infection. ANZ Journal of Surgery 2016, 86, 1014–1018. [Google Scholar] [CrossRef] [PubMed]
- Zaatreh, S.; Haffner, D.; Strauss, M.; Dauben, T.; Zamponi, C.; Mittelmeier, W.; Quandt, E.; Kreikemeyer, B.; Bader, R. Thin magnesium layer confirmed as an antibacterial and biocompatible implant coating in a co-culture model. Mol Med Rep 2017, 15, 1624–1630. [Google Scholar] [CrossRef]
- Huotari, K.; Peltola, M.; Jämsen, E. The incidence of late prosthetic joint infections. Acta Orthopaedica 2015, 86, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Al Thaher, Y.; Perni, S.; Prokopovich, P. Nano-carrier based drug delivery systems for sustained antimicrobial agent release from orthopaedic cementous material. Advances in Colloid and Interface Science 2017, 249, 234–247. [Google Scholar] [CrossRef] [PubMed]
- Damiati, L.; Eales, M.G.; Nobbs, A.H.; Su, B.; Tsimbouri, P.M.; Salmeron-Sanchez, M.; Dalby, M.J. Impact of surface topography and coating on osteogenesis and bacterial attachment on titanium implants. Journal of Tissue Engineering 2018, 9, 2041731418790694. [Google Scholar] [CrossRef] [PubMed]
- Ständert, V.; Borcherding, K.; Bormann, N.; Schmidmaier, G.; Grunwald, I.; Wildemann, B. Antibiotic-loaded amphora-shaped pores on a titanium implant surface enhance osteointegration and prevent infections. Bioactive Materials 2021, 6, 2331–2345. [Google Scholar] [CrossRef] [PubMed]
- Romanò, C.L.; Scarponi, S.; Gallazzi, E.; Romanò, D.; Drago, L. Antibacterial coating of implants in orthopaedics and trauma: a classification proposal in an evolving panorama. Journal of Orthopaedic Surgery and Research 2015, 10, 157. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Yergeshov, A.A.; Al-Thaher, Y.; Avdokushina, S.; Statsenko, E.; Abdullin, T.I.; Prokopovich, P. Nanocomposite orthopaedic bone cement combining long-acting dual antimicrobial drugs. Biomaterials Advances 2023, 153, 213538. [Google Scholar] [CrossRef]
- Liu, D.; He, C.; Liu, Z.; Xu, W. Gentamicin coating of nanotubular anodized titanium implant reduces implant-related osteomyelitis and enhances bone biocompatibility in rabbits. International Journal of Nanomedicine 2017, 5461–5471. [Google Scholar] [CrossRef]
- Tan, H.; Ao, H.; Ma, R.; Tang, T. Quaternised chitosan-loaded polymethylmethacrylate bone cement: Biomechanical and histological evaluations. Journal of Orthopaedic Translation 2013, 1, 57–66. [Google Scholar] [CrossRef]
- Min, J.; Choi, K.Y.; Dreaden, E.C.; Padera, R.F.; Braatz, R.D.; Spector, M.; Hammond, P.T. Designer Dual Therapy Nanolayered Implant Coatings Eradicate Biofilms and Accelerate Bone Tissue Repair. ACS Nano 2016, 10, 4441–4450. [Google Scholar] [CrossRef] [PubMed]
- Matsuno, H.; Yudoh, K.; Hashimoto, M.; Himeda, Y.; Miyoshi, T.; Yoshida, K.; Kano, S. A new antibacterial carrier of hyaluronic acid gel. Journal of Orthopaedic Science 2006, 11, 497–504. [Google Scholar] [CrossRef]
- Alt, V.; Bitschnau, A.; Böhner, F.; Heerich, K.E.; Magesin, E.; Sewing, A.; Pavlidis, T.; Szalay, G.; Heiss, C.; Thormann, U.; et al. Effects of gentamicin and gentamicin–RGD coatings on bone ingrowth and biocompatibility of cementless joint prostheses: An experimental study in rabbits. Acta biomaterialia 2011, 7, 1274–1280. [Google Scholar] [CrossRef] [PubMed]
- Sang, S.; Yang, C.; Chai, H.; Yuan, X.; Liu, W.; Zhang, X. The sulfonated polyetheretherketone with 3D structure modified by two bio-inspired methods shows osteogenic and antibacterial functions. Chemical Engineering Journal 2021, 420, 130059. [Google Scholar] [CrossRef]
- McKenna, P.B.; O’Shea, K.; Masterson, E.L. Two-stage revision of infected hip arthroplasty using a shortened post-operative course of antibiotics. Archives of Orthopaedic and Trauma Surgery 2009, 129, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Sang, S.; Guo, G.; Yu, J.; Zhang, X. Antibacterial application of gentamicin–silk protein coating with smart release function on titanium, polyethylene, and Al2O3 materials. Materials Science and Engineering: C 2021, 124, 112069. [Google Scholar] [CrossRef]
- Ashbaugh, A.G.; Jiang, X.; Zheng, J.; Tsai, A.S.; Kim, W.-S.; Thompson, J.M.; Miller, R.J.; Shahbazian, J.H.; Wang, Y.; Dillen, C.A.; et al. Polymeric nanofiber coating with tunable combinatorial antibiotic delivery prevents biofilm-associated infection in vivo. Proceedings of the National Academy of Sciences 2016, 113, E6919–E6928. [Google Scholar] [CrossRef] [PubMed]
- Stavrakis, A.I.; Zhu, S.; Hegde, V.; Loftin, A.H.; Ashbaugh, A.G.; Niska, J.A.; Miller, L.S.; Segura, T.; Bernthal, N.M. In Vivo Efficacy of a “Smart” Antimicrobial Implant Coating. JBJS 2016, 98, 1183–1189. [Google Scholar] [CrossRef] [PubMed]
- Giavaresi, G.; Meani, E.; Sartori, M.; Ferrari, A.; Bellini, D.; Sacchetta, A.C.; Meraner, J.; Sambri, A.; Vocale, C.; Sambri, V.; et al. Efficacy of antibacterial-loaded coating in an in vivo model of acutely highly contaminated implant. International Orthopaedics 2014, 38, 1505–1512. [Google Scholar] [CrossRef] [PubMed]
- Boot, W.; Vogely, H.C.; Jiao, C.; Nikkels, P.G.; Pouran, B.; van Rijen, M.H.; Ekkelenkamp, M.B.; Hänsch, G.M.; Dhert, W.J.; Gawlitta, D. Prophylaxis of implant-related infections by local release of vancomycin from a hydrogel in rabbits. European cells & materials 2020, 39, 108–120. [Google Scholar] [CrossRef]
- Fang, Y.; Xiao, Y.; Zhao, Y.; Golodok, R.P.; Savich, V.V.; Ilyushchanka, A.P.; Chen, X.; Wang, R. Porous titanium layer co-immobilized with bone morphogenetic protein-2 and vancomycin for biofunctionalization of ultra high molecular weight polyethylene. Materials & Design 2023, 232, 112131. [Google Scholar] [CrossRef]
- Xi, W.; Hegde, V.; Zoller, S.D.; Park, H.Y.; Hart, C.M.; Kondo, T.; Hamad, C.D.; Hu, Y.; Loftin, A.H.; Johansen, D.O.; et al. Point-of-care antimicrobial coating protects orthopaedic implants from bacterial challenge. Nature Communications 2021, 12, 5473. [Google Scholar] [CrossRef]
- Miller, R.J.; Thompson, J.M.; Zheng, J.; Marchitto, M.C.; Archer, N.K.; Pinsker, B.L.; Ortines, R.V.; Jiang, X.; Martin, R.A.; Brown, I.D.; et al. In Vivo Bioluminescence Imaging in a Rabbit Model of Orthopaedic Implant-Associated Infection to Monitor Efficacy of an Antibiotic-Releasing Coating. JBJS 2019, 101. [Google Scholar] [CrossRef] [PubMed]
- Bernthal, N.M.; Stavrakis, A.I.; Billi, F.; Cho, J.S.; Kremen, T.J.; Simon, S.I.; Cheung, A.L.; Finerman, G.A.; Lieberman, J.R.; Adams, J.S.; et al. A Mouse Model of Post-Arthroplasty Staphylococcus aureus Joint Infection to Evaluate In Vivo the Efficacy of Antimicrobial Implant Coatings. PLOS ONE 2010, 5, e12580. [Google Scholar] [CrossRef]
- Kaur, S.; Harjai, K.; Chhibber, S. In Vivo Assessment of Phage and Linezolid Based Implant Coatings for Treatment of Methicillin Resistant S. aureus (MRSA) Mediated Orthopaedic Device Related Infections. PLOS ONE 2016, 11, e0157626. [Google Scholar] [CrossRef] [PubMed]
- Sang, S.; Wang, S.; Yang, C.; Geng, Z.; Zhang, X. Sponge-inspired sulfonated polyetheretherketone loaded with polydopamine-protected osthole nanoparticles and berberine enhances osteogenic activity and prevents implant-related infections. Chemical Engineering Journal 2022, 437, 135255. [Google Scholar] [CrossRef]
- Kawano, S.; Sonohata, M.; Eto, S.; Kitajima, M.; Mawatari, M. Bone ongrowth of a cementless silver oxide-containing hydroxyapatite-coated antibacterial acetabular socket. Journal of Orthopaedic Science 2019, 24, 658–662. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Wang, Q.; Zhang, Y.; He, H.; Xiong, S.; Chen, P.; Li, C.; Wang, L.; Lu, G.; Xu, Y. A dual-functional PEEK implant coating for anti-bacterial and accelerated osseointegration. Colloids and Surfaces B: Biointerfaces 2023, 224, 113196. [Google Scholar] [CrossRef]
- Zeng, Z.; He, X.; Tan, B.; Dai, C.; Zheng, W. Titanium oxide nanotubes embedded with silver dioxide nanoparticles for Staphylococcus aureus infections after prosthetic joint replacement in animal models. Int. J. Clin. Exp. Med 2018, 11, 7392–7399. [Google Scholar]
- Hashimoto, A.; Sonohata, M.; Kitajima, M.; Kawano, S.; Eto, S.; Mawatari, M. First experience with a thermal-sprayed silver oxide-containing hydroxyapatite coating implant in two-stage total hip arthroplasty for the treatment of septic arthritis with hip osteoarthritis: A case report. International Journal of Surgery Case Reports 2020, 77, 434–437. [Google Scholar] [CrossRef] [PubMed]
- Eto, S.; Kawano, S.; Someya, S.; Miyamoto, H.; Sonohata, M.; Mawatari, M. First Clinical Experience With Thermal-Sprayed Silver Oxide–Containing Hydroxyapatite Coating Implant. The Journal of Arthroplasty 2016, 31, 1498–1503. [Google Scholar] [CrossRef]
- Eto, S.; Miyamoto, H.; Shobuike, T.; Noda, I.; Akiyama, T.; Tsukamoto, M.; Ueno, M.; Someya, S.; Kawano, S.; Sonohata, M.; et al. Silver oxide-containing hydroxyapatite coating supports osteoblast function and enhances implant anchorage strength in rat femur. Journal of Orthopaedic Research 2015, 33, 1391–1397. [Google Scholar] [CrossRef]
- Nakashima, T.; Morimoto, T.; Hashimoto, A.; Kii, S.; Tsukamoto, M.; Miyamoto, H.; Todo, M.; Sonohata, M.; Mawatari, M. Osteoconductivity and neurotoxicity of silver-containing hydroxyapatite coating cage for spinal interbody fusion in rats. JOR SPINE 2023, 6, e1236. [Google Scholar] [CrossRef] [PubMed]
- Akiyama, T.; Miyamoto, H.; Yonekura, Y.; Tsukamoto, M.; Ando, Y.; Noda, I.; Sonohata, M.; Mawatari, M. Silver oxide-containing hydroxyapatite coating has in vivo antibacterial activity in the rat tibia. Journal of Orthopaedic Research 2013, 31, 1195–1200. [Google Scholar] [CrossRef] [PubMed]
- Shimazaki, T.; Miyamoto, H.; Ando, Y.; Noda, I.; Yonekura, Y.; Kawano, S.; Miyazaki, M.; Mawatari, M.; Hotokebuchi, T. In vivo antibacterial and silver-releasing properties of novel thermal sprayed silver-containing hydroxyapatite coating. Journal of Biomedical Materials Research Part B: Applied Biomaterials 2010, 92B, 386–389. [Google Scholar] [CrossRef] [PubMed]
- Kawano, S.; Ueno, M.; Fujii, M.; Mawatari, D.; Mawatari, M. Case Series of Silver Oxide–Containing Hydroxyapatite Coating in Antibacterial Cementless Total Hip Arthroplasty: Clinical Results of 50 Cases at 5-Year Follow-Up. Arthroplasty Today 2023, 19, 101067. [Google Scholar] [CrossRef] [PubMed]
- Devlin-Mullin, A.; Todd, N.M.; Golrokhi, Z.; Geng, H.; Konerding, M.A.; Ternan, N.G.; Hunt, J.A.; Potter, R.J.; Sutcliffe, C.; Jones, E.; et al. Atomic Layer Deposition of a Silver Nanolayer on Advanced Titanium Orthopedic Implants Inhibits Bacterial Colonization and Supports Vascularized de Novo Bone Ingrowth. Advanced Healthcare Materials 2017, 6, 1700033. [Google Scholar] [CrossRef]
- Huo, S.; Lyu, Z.; Su, X.; Wang, F.; Liu, J.; Liu, S.; Liu, X.; Bao, X.; Zhang, J.; Zheng, K.; et al. Formation of a novel Cu-containing bioactive glass nano-topography coating with strong bactericidal capability and bone regeneration. Composites Part B: Engineering 2023, 253, 110521. [Google Scholar] [CrossRef]
- Ellenrieder, M.; Haenle, M.; Lenz, R.; Bader, R.; Mittelmeier, W. Titanium-copper-nitride coated spacers for two-stage revision of infected total hip endoprostheses. GMS Krankenhaushygiene interdisziplinar 2011, 6, Doc16. [Google Scholar] [CrossRef] [PubMed]
- Mauerer, A.; Stenglein, S.; Schulz-Drost, S.; Schoerner, C.; Taylor, D.; Krinner, S.; Heidenau, F.; Adler, W.; Forst, R. Antibacterial Effect of a 4x Cu-TiO2 Coating Simulating Acute Periprosthetic Infection—An Animal Model. Molecules 2017, 22, 1042. [Google Scholar] [CrossRef] [PubMed]
- Ciliveri, S.; Bandyopadhyay, A. Enhanced osteogenesis and bactericidal performance of additively manufactured MgO-and Cu-added CpTi for load-bearing implants. IJB 2023, 9. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.; Wang, C.; Wang, D.; Jiang, H.; Qiao, Y.; Zhang, D.; Zhang, X.; Xu, R.; Liu, C.; Su, J.; et al. Tailoring time-varying alkaline microenvironment on titanium for sequential anti-infection and osseointegration. Chemical Engineering Journal 2022, 431, 133940. [Google Scholar] [CrossRef]
- Shirai, T.; Shimizu, T.; Ohtani, K.; Zen, Y.; Takaya, M.; Tsuchiya, H. Antibacterial iodine-supported titanium implants. Acta biomaterialia 2011, 7, 1928–1933. [Google Scholar] [CrossRef]
- Taga, T.; Kabata, T.; Kajino, Y.; Inoue, D.; Ohmori, T.; Yamamoto, T.; Takagi, T.; Tsuchiya, H. Comparison with the osteoconductivity and bone-bonding ability of the iodine supported titanium, titanium with porous oxide layer and the titanium alloy in the rabbit model. Journal of Orthopaedic Science 2018, 23, 585–591. [Google Scholar] [CrossRef]
- Sinclair, K.D.; Pham, T.X.; Williams, D.L.; Farnsworth, R.W.; Loc-Carrillo, C.M.; Bloebaum, R.D. Model development for determining the efficacy of a combination coating for the prevention of perioperative device related infections: A pilot study. Journal of Biomedical Materials Research Part B: Applied Biomaterials 2013, 101, 1143–1153. [Google Scholar] [CrossRef]
- Yuan, X.; Ouyang, L.; Luo, Y.; Sun, Z.; Yang, C.; Wang, J.; Liu, X.; Zhang, X. Multifunctional sulfonated polyetheretherketone coating with beta-defensin-14 for yielding durable and broad-spectrum antibacterial activity and osseointegration. Acta biomaterialia 2019, 86, 323–337. [Google Scholar] [CrossRef] [PubMed]
- Hu, H.; Cui, R.; Mei, L.; Ni, S.; Sun, H.; Zhang, C.; Ni, S. Cytocompatibility and Bone-Formation Potential of Se-Coated 316L Stainless Steel with Nano-Pit Arrays. Journal of Biomedical Nanotechnology 2018, 14, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Bai, X.; Yu, J.; Xiao, J.; Wang, Y.; Li, Z.; Wang, H. Antibacterial intraosseous implant surface coating that responds to changes in the bacterial microenvironment. Frontiers in Bioengineering and Biotechnology 2023, 10, 1016001. [Google Scholar] [CrossRef] [PubMed]
- Blackburn Jr., W. D.; Alarcón, G.S. Prosthetic joint infections. A role for prophylaxis. Arthritis & Rheumatism 1991, 34, 110–117. [Google Scholar] [CrossRef]
- Lucke, M.; Schmidmaier, G.; Sadoni, S.; Wildemann, B.; Schiller, R.; Haas, N.P.; Raschke, M. Gentamicin coating of metallic implants reduces implant-related osteomyelitis in rats. Bone 2003, 32, 521–531. [Google Scholar] [CrossRef]
- Commission, E.; Centre, J.R.; Sanseverino, I.; Loos, R.; Navarro Cuenca, A.; Marinov, D.; Lettieri, T. State of the art on the contribution of water to antimicrobial resistance; Publications Office: 2018.
- Babutan, I.; Lucaci, A.-D.; Botiz, I. Antimicrobial Polymeric Structures Assembled on Surfaces. Polymers 2021, 13, 1552. [Google Scholar] [CrossRef] [PubMed]
- Shaygani, H.; Seifi, S.; Shamloo, A.; Golizadeh, M.; Rahnamaee, S.Y.; Alishiri, M.; Ebrahimi, S. Novel bilayer coating on gentamicin-loaded titanium nanotube for orthopedic implants applications. International Journal of Pharmaceutics 2023, 636, 122764. [Google Scholar] [CrossRef]
- Mohan Raj, R.; Priya, P.; Raj, V. Gentamicin-loaded ceramic-biopolymer dual layer coatings on the Ti with improved bioactive and corrosion resistance properties for orthopedic applications. Journal of the mechanical behavior of biomedical materials 2018, 82, 299–309. [Google Scholar] [CrossRef] [PubMed]
- Ballarre, J.; Aydemir, T.; Liverani, L.; Roether, J.A.; Goldmann, W.H.; Boccaccini, A.R. Versatile bioactive and antibacterial coating system based on silica, gentamicin, and chitosan: Improving early stage performance of titanium implants. Surface and Coatings Technology 2020, 381, 125138. [Google Scholar] [CrossRef]
- Zhang, L.; Yan, J.; Yin, Z.; Tang, C.; Guo, Y.; Li, D.; Wei, B.; Xu, Y.; Gu, Q.; Wang, L. Electrospun vancomycin-loaded coating on titanium implants for the prevention of implant-associated infections. International Journal of Nanomedicine 2014, 9, 3027–3036. [Google Scholar] [CrossRef]
- Ordikhani, F.; Tamjid, E.; Simchi, A. Characterization and antibacterial performance of electrodeposited chitosan–vancomycin composite coatings for prevention of implant-associated infections. Materials Science and Engineering: C 2014, 41, 240–248. [Google Scholar] [CrossRef]
- Pon-On, W.; Charoenphandhu, N.; Teerapornpuntakit, J.; Thongbunchoo, J.; Krishnamra, N.; Tang, I.M. In vitro study of vancomycin release and osteoblast-like cell growth on structured calcium phosphate-collagen. Materials Science and Engineering: C 2013, 33, 1423–1431. [Google Scholar] [CrossRef] [PubMed]
- Thanyaphoo, S.; Kaewsrichan, J. Potential of bone scaffolds containing vancomycin and bone morphogenetic protein-2 in a rat model of osteomyelitis. Asian Biomedicine 2017, 8, 651–658. [Google Scholar] [CrossRef]
- Hirschfeld, J.; Akinoglu, E.M.; Wirtz, D.C.; Hoerauf, A.; Bekeredjian-Ding, I.; Jepsen, S.; Haddouti, E.-M.; Limmer, A.; Giersig, M. Long-term release of antibiotics by carbon nanotube-coated titanium alloy surfaces diminish biofilm formation by Staphylococcus epidermidis. Nanomedicine: Nanotechnology, Biology and Medicine 2017, 13, 1587–1593. [Google Scholar] [CrossRef] [PubMed]
- Aboltins, C.A.; Page, M.A.; Buising, K.L.; Jenney, A.W.J.; Daffy, J.R.; Choong, P.F.M.; Stanley, P.A. Treatment of staphylococcal prosthetic joint infections with debridement, prosthesis retention and oral rifampicin and fusidic acid. Clinical Microbiology and Infection 2007, 13, 586–591. [Google Scholar] [CrossRef]
- Cao, X.-Y.; Tian, N.; Dong, X.; Cheng, C.-K. Implant Coating Manufactured by Micro-Arc Oxidation and Dip Coating in Resorbable Polylactide for Antimicrobial Applications in Orthopedics. Coatings 2019, 9, 284. [Google Scholar] [CrossRef]
- Kastoris, A.C.; Rafailidis, P.I.; Vouloumanou, E.K.; Gkegkes, I.D.; Falagas, M.E. Synergy of fosfomycin with other antibiotics for Gram-positive and Gram-negative bacteria. European Journal of Clinical Pharmacology 2010, 66, 359–368. [Google Scholar] [CrossRef] [PubMed]
- Dryden, M.S. Linezolid pharmacokinetics and pharmacodynamics in clinical treatment. Journal of Antimicrobial Chemotherapy 2011, 66, iv7–iv15. [Google Scholar] [CrossRef] [PubMed]
- Ament, P.W.; Jamshed, N.; Horne, J.P. Linezolid: its role in the treatment of gram-positive, drug-resistant bacterial infections. American family physician 2002, 65, 663–670. [Google Scholar] [PubMed]
- Toirac, B.; Aguilera-Correa, J.J.; Mediero, A.; Esteban, J.; Jiménez-Morales, A. The Antimicrobial Activity of Micron-Thin Sol–Gel Films Loaded with Linezolid and Cefoxitin for Local Prevention of Orthopedic Prosthesis-Related Infections. Gels 2023, 9, 176. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Lai, Y.; Zheng, X.; Yang, Y. Facile Fabrication of Linezolid/Strontium Coated Hydroxyapatite/Graphene Oxide Nanocomposite for Osteoporotic Bone Defect. Heliyon 2024. [Google Scholar] [CrossRef]
- Alt, V.; Bitschnau, A.; Österling, J.; Sewing, A.; Meyer, C.; Kraus, R.; Meissner, S.A.; Wenisch, S.; Domann, E.; Schnettler, R. The effects of combined gentamicin–hydroxyapatite coating for cementless joint prostheses on the reduction of infection rates in a rabbit infection prophylaxis model. Biomaterials 2006, 27, 4627–4634. [Google Scholar] [CrossRef] [PubMed]
- Miclau, T.; Edin, M.L.; Lester, G.E.; Lindsey, R.W.; Dahners, L.E. Bone Toxicity of Locally Applied Aminoglycosides. Journal of Orthopaedic Trauma 1995, 9, 401–406. [Google Scholar] [CrossRef]
- Edin, M.L.; Miclau, T.; Lester, G.E.; Lindsey, R.W.; Dahners, L.E. Effect of Cefazolin and Vancomycin on Osteoblasts In Vitro. Clinical Orthopaedics and Related Research® 1996, 333, 245–251. [Google Scholar] [CrossRef]
- Isefuku, S.; Joyner, C.J.; Simpson, A.H.R.W. Gentamicin May Have an Adverse Effect on Osteogenesis. Journal of Orthopaedic Trauma 2003, 17, 212–216. [Google Scholar] [CrossRef] [PubMed]
- Duewelhenke, N.; Krut, O.; Eysel, P. Influence on Mitochondria and Cytotoxicity of Different Antibiotics Administered in High Concentrations on Primary Human Osteoblasts and Cell Lines. Antimicrobial Agents and Chemotherapy 2007, 51, 54–63. [Google Scholar] [CrossRef] [PubMed]
- Mouriño, V.; Cattalini, J.P.; Boccaccini, A.R. Metallic ions as therapeutic agents in tissue engineering scaffolds: an overview of their biological applications and strategies for new developments. Journal of The Royal Society Interface 2012, 9, 401–419. [Google Scholar] [CrossRef] [PubMed]
- Brokesh, A.M.; Gaharwar, A.K. Inorganic Biomaterials for Regenerative Medicine. ACS Applied Materials & Interfaces 2020, 12, 5319–5344. [Google Scholar] [CrossRef]
- Cardoso, G.C.; Barbaro, K.; Kuroda, P.A.B.; Imperatori, L.; De Bonis, A.; Teghil, R.; Curcio, M.; Innocenzi, E.; Grigorieva, V.Y.; Vadalà, G.; et al. Incorporation of Ca, P, Mg, and Zn Elements in Ti-30Nb-5Mo Alloy by Micro-Arc Oxidation for Biomedical Implant Applications: Surface Characterization, Cellular Growth, and Microorganisms' Activity. Coatings 2023, 13, 1577. [Google Scholar] [CrossRef]
- Rahman, S.; Rahman, L.; Khalil, A.T.; Ali, N.; Zia, D.; Ali, M.; Shinwari, Z.K. Endophyte-mediated synthesis of silver nanoparticles and their biological applications. Applied Microbiology and Biotechnology 2019, 103, 2551–2569. [Google Scholar] [CrossRef]
- Godoy-Gallardo, M.; Eckhard, U.; Delgado, L.M.; de Roo Puente, Y.J.D.; Hoyos-Nogués, M.; Gil, F.J.; Perez, R.A. Antibacterial approaches in tissue engineering using metal ions and nanoparticles: From mechanisms to applications. Bioactive Materials 2021, 6, 4470–4490. [Google Scholar] [CrossRef]
- Burtscher, S.; Krieg, P.; Killinger, A.; Al-Ahmad, A.; Seidenstücker, M.; Latorre, S.H.; Bernstein, A. Thin Degradable Coatings for Optimization of Osteointegration Associated with Simultaneous Infection Prophylaxis. Materials 2019, 12, 3495. [Google Scholar] [CrossRef]
- He, X.; Zhang, X.; Bai, L.; Hang, R.; Huang, X.; Qin, L.; Yao, X.; Tang, B. Antibacterial ability and osteogenic activity of porous Sr/Ag-containing TiO2 coatings. Biomedical Materials 2016, 11, 045008. [Google Scholar] [CrossRef]
- Yang, W.; Shen, C.; Ji, Q.; An, H.; Wang, J.; Liu, Q.; Zhang, Z. Food storage material silver nanoparticles interfere with DNA replication fidelity and bind with DNA. Nanotechnology 2009, 20, 085102. [Google Scholar] [CrossRef]
- Feng, Q.L.; Wu, J.; Chen, G.Q.; Cui, F.Z.; Kim, T.N.; Kim, J.O. A mechanistic study of the antibacterial effect of silver ions on Escherichia coli and Staphylococcus aureus. Journal of Biomedical Materials Research 2000, 52, 662–668. [Google Scholar] [CrossRef]
- Cardoso, G.C.; Barbaro, K.; Kuroda, P.A.B.; De Bonis, A.; Teghil, R.; Monteleone, V.; Imperatori, L.; Ortenzi, M.; Antoniac, I.; Grandini, C.R.; et al. Silver Containing Antimicrobial Coatings on Innovative Ti-30Nb-5Mo β-Alloy Prepared by Micro-Arc Oxidation for Biomedical Implant Applications. Coatings 2024, 14, 214. [Google Scholar] [CrossRef]
- Percival, S.L.; Bowler, P.; Russell, D. Bacterial resistance to silver in wound care. Journal of hospital infection 2005, 60, 1–7. [Google Scholar] [CrossRef]
- Cardoso, G.C.; Grandini, C.R.; Rau, J.V. Comprehensive review of PEO coatings on titanium alloys for biomedical implants. Journal of Materials Research and Technology 2024, 31, 311–328. [Google Scholar] [CrossRef]
- Gosheger, G.; Hardes, J.; Ahrens, H.; Streitburger, A.; Buerger, H.; Erren, M.; Gunsel, A.; Kemper, F.H.; Winkelmann, W.; von Eiff, C. Silver-coated megaendoprostheses in a rabbit model—an analysis of the infection rate and toxicological side effects. Biomaterials 2004, 25, 5547–5556. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Li, J.; Wang, X.; Wang, Y.; Hang, R.; Huang, X.; Tang, B.; Chu, P.K. Effects of copper nanoparticles in porous TiO2 coatings on bacterial resistance and cytocompatibility of osteoblasts and endothelial cells. Materials Science and Engineering: C 2018, 82, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Cardoso, G.C.; Barbaro, K.; Kuroda, P.A.B.; De Bonis, A.; Teghil, R.; Krasnyuk, I.I.; Imperatori, L.; Grandini, C.R.; Rau, J.V. Antimicrobial Cu-Doped TiO2 Coatings on the β Ti-30Nb-5Mo Alloy by Micro-Arc Oxidation. Materials 2024, 17, 156. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Li, X.; Elkhooly, T.A.; Liu, X.; Zhang, R.; Wu, H.; Feng, Q.; Liu, Y. The Cu-containing TiO2 coatings with modulatory effects on macrophage polarization and bactericidal capacity prepared by micro-arc oxidation on titanium substrates. Colloids and Surfaces B: Biointerfaces 2018, 170, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, A.; Renaudin, G.; Forestier, C.; Nedelec, J.-M.; Descamps, S. Biological properties of copper-doped biomaterials for orthopedic applications: A review of antibacterial, angiogenic and osteogenic aspects. Acta biomaterialia 2020, 117, 21–39. [Google Scholar] [CrossRef] [PubMed]
- O’Neill, E.; Awale, G.; Daneshmandi, L.; Umerah, O.; Lo, K.W.H. The roles of ions on bone regeneration. Drug Discovery Today 2018, 23, 879–890. [Google Scholar] [CrossRef]
- Tan, J.; Wang, D.; Cao, H.; Qiao, Y.; Zhu, H.; Liu, X. Effect of Local Alkaline Microenvironment on the Behaviors of Bacteria and Osteogenic Cells. ACS Applied Materials & Interfaces 2018, 10, 42018–42029. [Google Scholar] [CrossRef]
- Tan, J.; Liu, Z.; Wang, D.; Zhang, X.; Qian, S.; Liu, X. A facile and universal strategy to endow implant materials with antibacterial ability via alkalinity disturbing bacterial respiration. Biomaterials Science 2020, 8, 1815–1829. [Google Scholar] [CrossRef] [PubMed]
- Yoda, I.; Koseki, H.; Tomita, M.; Shida, T.; Horiuchi, H.; Sakoda, H.; Osaki, M. Effect of surface roughness of biomaterials on Staphylococcus epidermidis adhesion. BMC Microbiology 2014, 14, 234. [Google Scholar] [CrossRef] [PubMed]
- Ma, M.; Kazemzadeh-Narbat, M.; Hui, Y.; Lu, S.; Ding, C.; Chen, D.D.Y.; Hancock, R.E.W.; Wang, R. Local delivery of antimicrobial peptides using self-organized TiO2 nanotube arrays for peri-implant infections. Journal of Biomedical Materials Research Part A 2012, 100A, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Guastaldi, F.P.S.; Foggi, C.C.d.; Santana, L.C.L.; Vaz, L.G.; Vergani, C.E.; Guastaldi, A.C. Lower Susceptibility of Laser-irradiated Ti-15Mo Surface to Methicillin-resistant <i>Staphylococcus aureus</i> Cells Adhesion. Materials Research 2019, 22. [Google Scholar] [CrossRef]
- Li, Z.; Zhao, Y.; Wang, Z.; Ren, M.; Wang, X.; Liu, H.; Lin, Q.; Wang, J. Engineering Multifunctional Hydrogel-Integrated 3D Printed Bioactive Prosthetic Interfaces for Osteoporotic Osseointegration. Advanced Healthcare Materials 2022, 11, 2102535. [Google Scholar] [CrossRef]
Figure 1.
Costs associated with prosthetic joint infections treatment. TKA: Total Knee Arthroplasty; THA: Total Hip Arthroplasty [7,10,11].
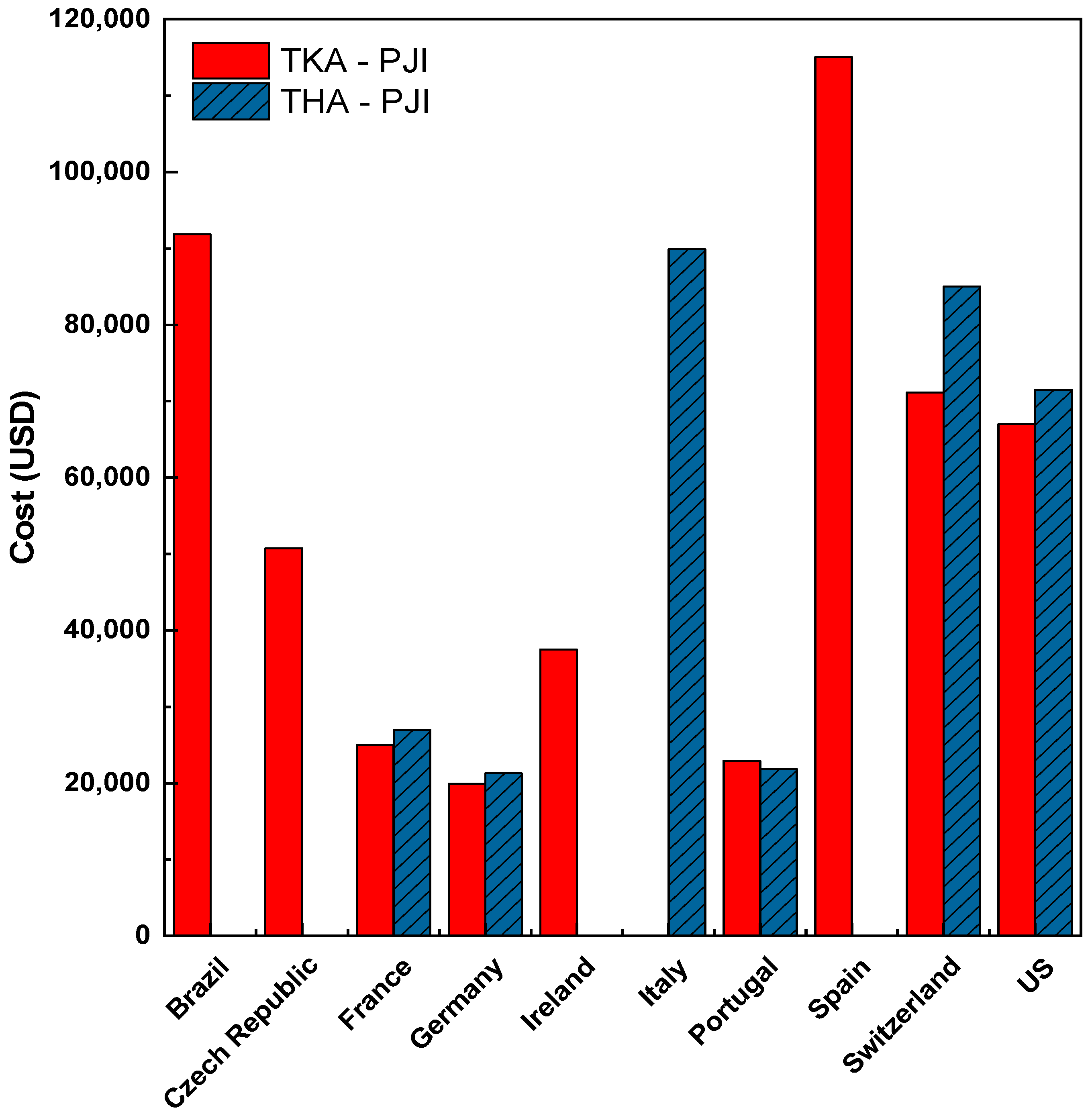
Figure 2.
Organization of articles on bactericidal coatings for arthroplasties.
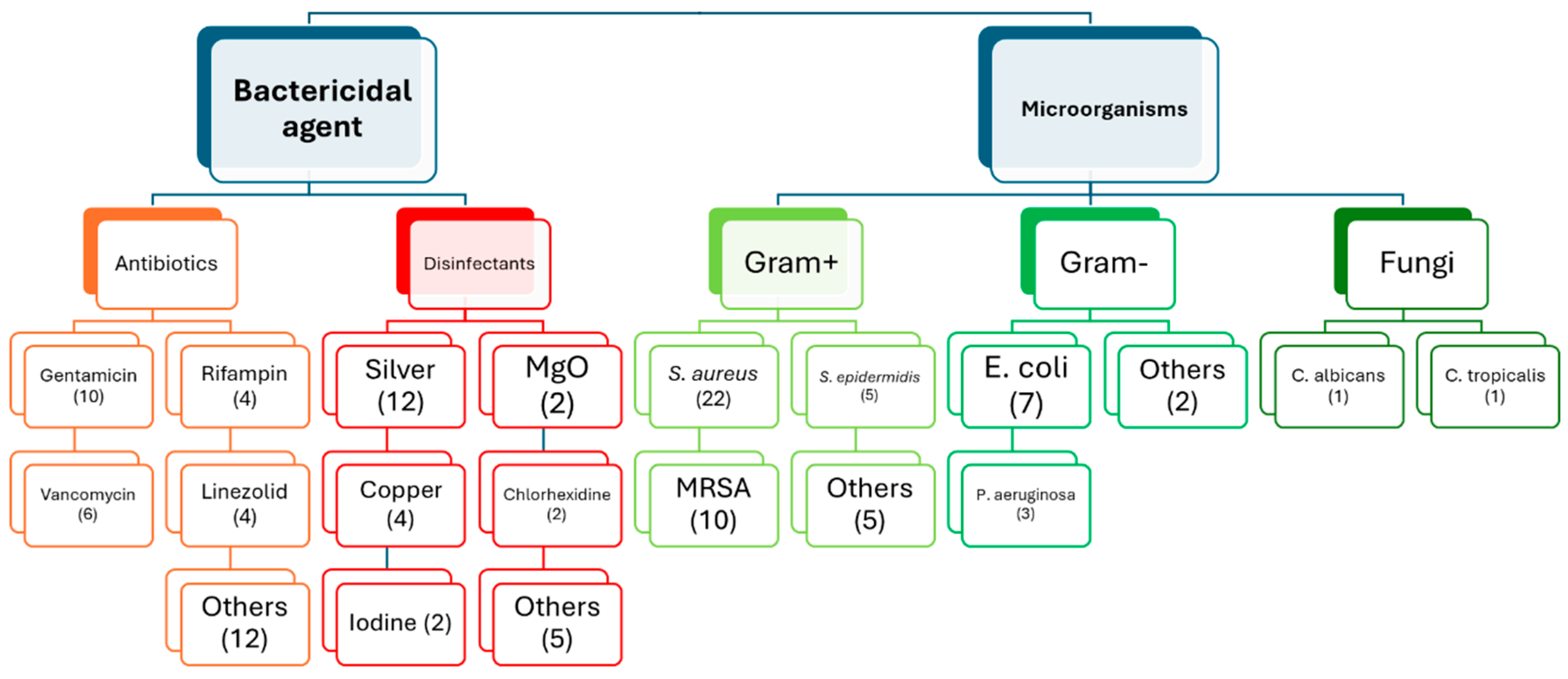
Figure 3.
Quantification of articles relating to polymeric and ceramic coatings, and the most used bactericidal agents.
Figure 3.
Quantification of articles relating to polymeric and ceramic coatings, and the most used bactericidal agents.
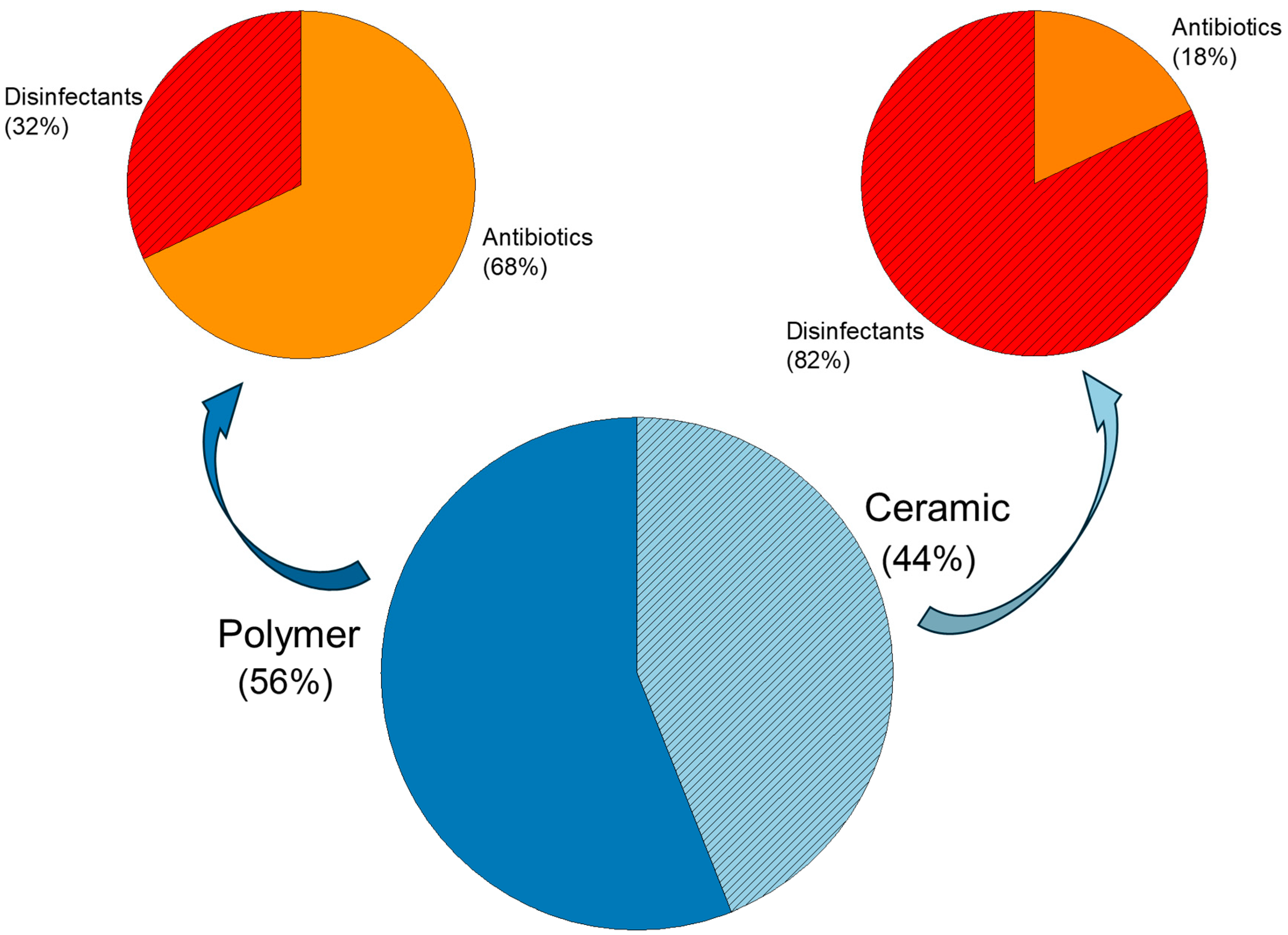
Figure 4.
Mechanisms of action of different antibiotics. Parts of the figure were drawn using pictures from Server Medical Art. Servier Medical Art by Servier is licensed under a Creative Commons Attribution 3.0 Unported License.
Figure 4.
Mechanisms of action of different antibiotics. Parts of the figure were drawn using pictures from Server Medical Art. Servier Medical Art by Servier is licensed under a Creative Commons Attribution 3.0 Unported License.
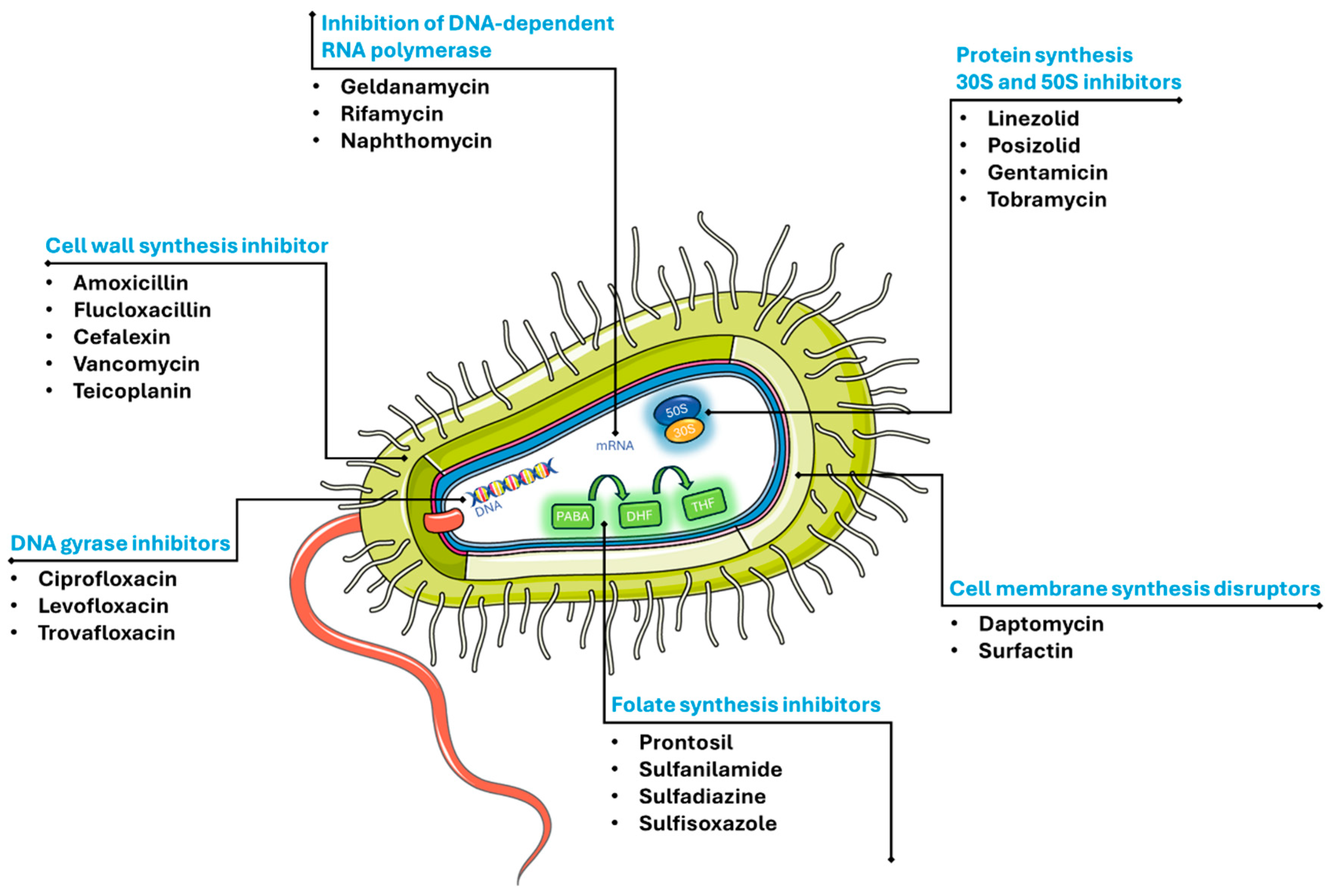
Figure 5.
Illustration of the implantation of the materials (a), and number of viable S. aureus in tissues around the implant after 7 days (b). *: p<0.05; UHMWPE-Ti-Ta-B/V: UHMWPE samples coated with Ti powders, activated by tannic acid (TA) treatment, and loaded with BMP-2 and vancomycin [35]. Reproduced with permission from Materials & Design, 2023, 232, 112131, Elsevier.
Figure 5.
Illustration of the implantation of the materials (a), and number of viable S. aureus in tissues around the implant after 7 days (b). *: p<0.05; UHMWPE-Ti-Ta-B/V: UHMWPE samples coated with Ti powders, activated by tannic acid (TA) treatment, and loaded with BMP-2 and vancomycin [35]. Reproduced with permission from Materials & Design, 2023, 232, 112131, Elsevier.
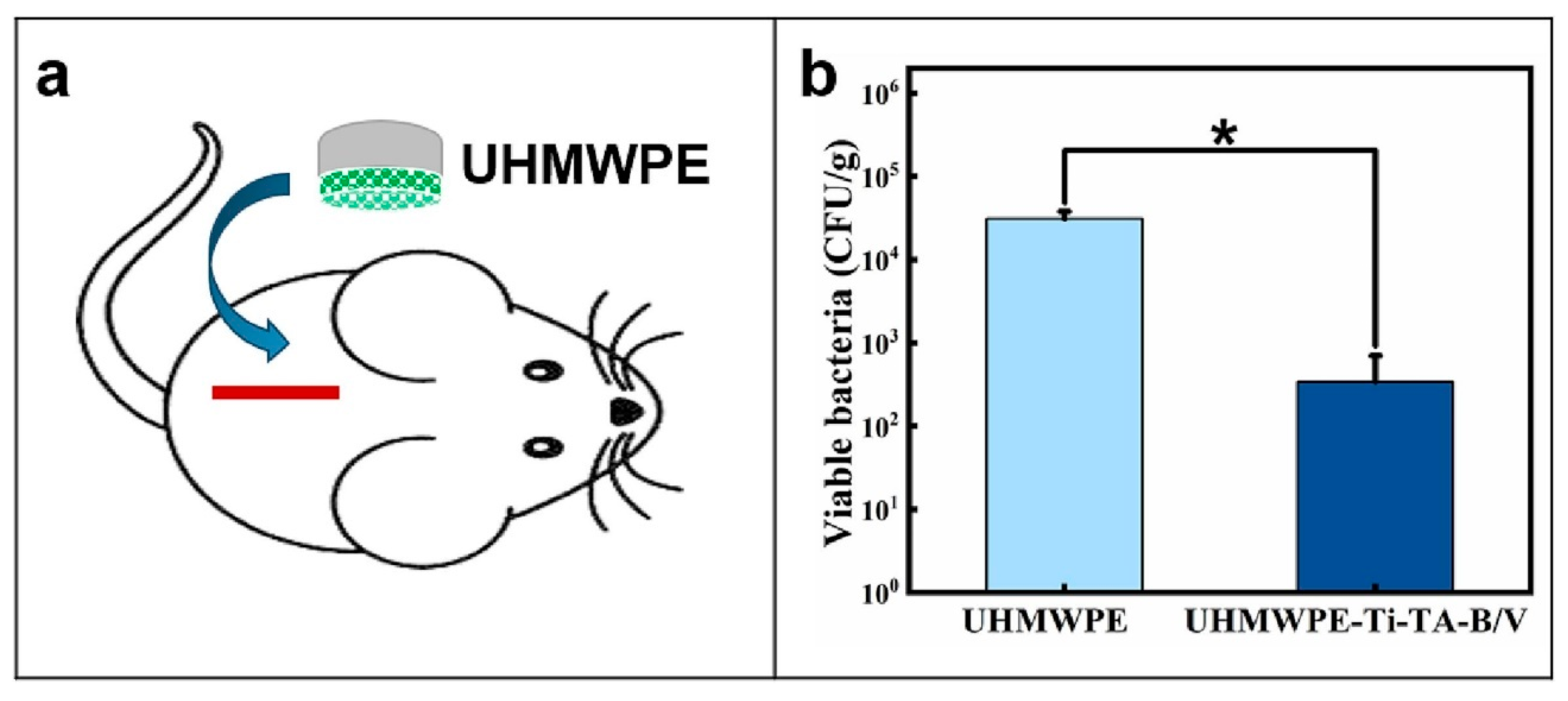
Figure 6.
Mechanisms of action of bactericidal metal ions and metals nanoparticles. Parts of the figure were drawn using pictures from Server Medical Art. Servier Medical Art by Servier is licensed under a Creative Commons Attribution 3.0 Unported License.
Figure 6.
Mechanisms of action of bactericidal metal ions and metals nanoparticles. Parts of the figure were drawn using pictures from Server Medical Art. Servier Medical Art by Servier is licensed under a Creative Commons Attribution 3.0 Unported License.

Figure 7.
Masson (a) and Giemsa (b) stainings of tissues around the implants after 2 and 4 weeks of implantation. In (a), the red arrows indicate the new generated bones with low fibrous tissue, and in (b) indicates the chronic inflammatory cells in the interface of PEEK without Ag [42]. Reproduced with permission from Colloids and Surfaces B: Biointerfaces, 2023, 224, 113196, Elsevier.
Figure 7.
Masson (a) and Giemsa (b) stainings of tissues around the implants after 2 and 4 weeks of implantation. In (a), the red arrows indicate the new generated bones with low fibrous tissue, and in (b) indicates the chronic inflammatory cells in the interface of PEEK without Ag [42]. Reproduced with permission from Colloids and Surfaces B: Biointerfaces, 2023, 224, 113196, Elsevier.
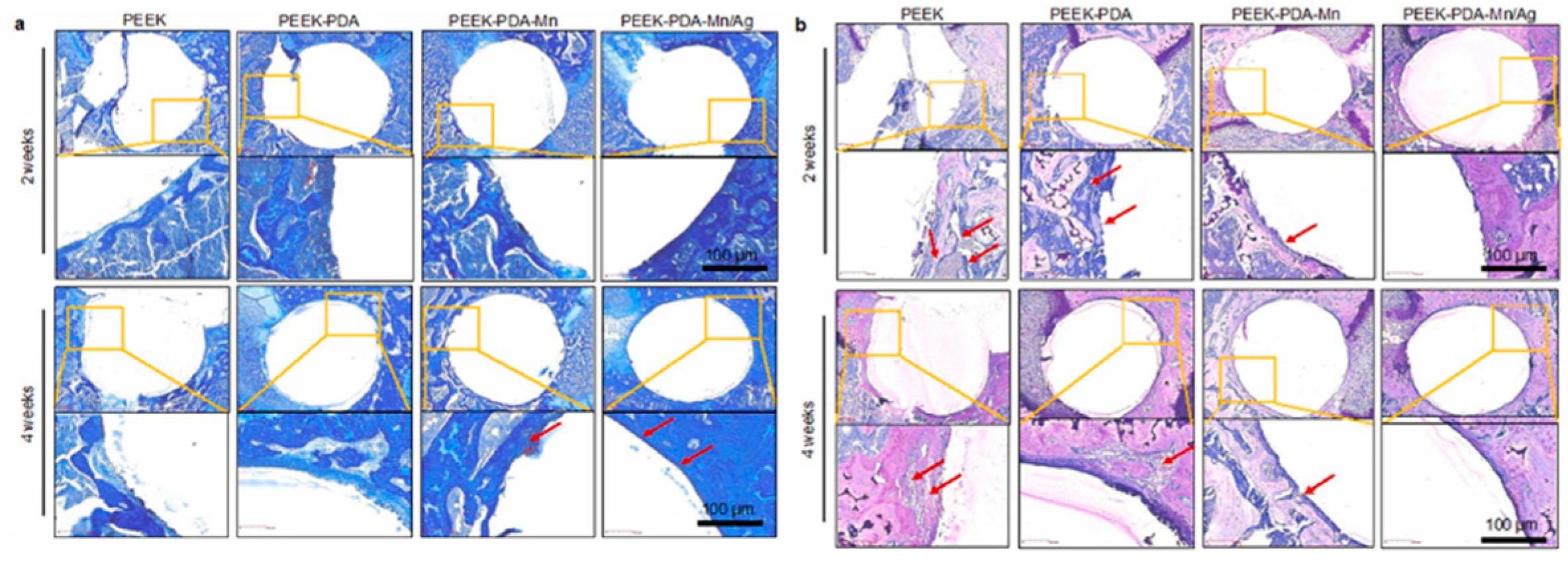
Figure 8.
Illustrations of the bioactive and anti-infection 3D-printed titanium scaffold sample [110]. Reproduced with permission from Advanced Healthcare Materials, 2022, 11, 2102535, Wiley.
Figure 8.
Illustrations of the bioactive and anti-infection 3D-printed titanium scaffold sample [110]. Reproduced with permission from Advanced Healthcare Materials, 2022, 11, 2102535, Wiley.

Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



