
Submitted:
05 December 2024
Posted:
06 December 2024
You are already at the latest version
Abstract
Consuming collagen hydrolysate (CH) may improve symptoms of exercise-induced muscle damage (EIMD), however its acute effects have not been compared to dairy protein (DP), the most commonly consumed form of protein supplement. Therefore, this study compared the effects of CH and DP on recovery from EIMD. Thirty-three males consumed either CH (n=11) or DP (n=11), containing 25 g of protein, or an isoenergetic placebo (n=11) immediately post-exercise and once daily for three days. Indices of EIMD were measured before and 30 minutes, 24, 48, and 72 hours after 30 minutes of downhill running on a -15% slope at 80% of VO2max speed. Downhill running induced significant EIMD, with time effects (all P < 0.001) for delayed onset of muscle soreness (visual analogue scale), countermovement jump height, isometric midthigh pull force, maximal voluntary isometric contraction force, running economy, and biomarkers of muscle damage (creatine kinase) and inflammation (interleukin-6, high-sensitivity C-reactive protein). However, no group or interaction effects (all P > 0.05) were observed for any outcome measures. The findings suggest that post-exercise consumption of CH or DP does not improve indices of EIMD during the acute recovery period, in recreationally active males.
Keywords:
collagen hydrolysate
; delayed onset muscle soreness
; exercise-induced muscle damage
; post-exercise recovery
; milk proteins
1. Introduction
Exercise-induced muscle damage (EIMD) is caused by exercise that is strenuous, repetitive, novel, and/or involves eccentric muscle contractions, such as downhill running [1]. Whilst EIMD is temporary, and may be beneficial for future muscle adaptation [2], it can create problems for regular exercisers by impairing performance during subsequent bouts of exercise [3] and/or by causing a disruption to normal daily activities that are not otherwise an issue [4]. Therefore, timely recovery from EIMD is important.
Although significant effort has been made to find nutritional interventions that alleviate the symptoms of EIMD, including omega-3 fatty acids, various amino acids, polphenols and herbal extracts, there is no strong consensus on the best option [5]. One intervention at the forefront of most recommendations is dairy protein (DP) [6], which includes whey, casein, and whole milk. The consumption of DP following EIMD is believed to improve recovery through the delivery of essential amino acids that enhance rates of muscle protein synthesis, thus promoting muscle repair [7]; however, this mechanism has been disputed [8]. Irrespective of the mechanism, whether consuming DP is beneficial for recovery remains unclear, with some studies showing that DP can alter markers of EIMD, including muscle function (for example Brown et al. [9]; Buckley et al. [10]; Cooke et al. [11]), while others, including Gee et al. [12]; Nieman et al. [13]; Ormsbee et al. [14] and Saracino et al. [15], have failed to see an effect. Moreover, the majority of research has shown that supplementing with protein, including DP, does not specifically reduce exercise-induced delayed onset muscle soreness (DOMS) [16]. Despite mixed evidence for its effects on EIMD, and significant environmental footprint [17], DP’s convenience and effects on muscle protein synthesis make it the major contributor to a protein supplement industry that is expected to be worth over US$10B by 2030, in the US alone [18].
In order to improve sustainability, reduce environmental harm, and open up new commercial markets, researchers (and the supplement industry) are increasingly interested in novel protein sources [19] and how they may impact recovery and performance [16,18]. Sourced from the underutilized by-products of the meat industry, bovine collagen is high in the non-essential amino acids used to synthesize collagen and remodel the extra-cellular matrix (ECM) [20]. Once ingested, collagen hydrolysates (CH) are digested in the gastrointestinal tract to yield free amino acids [21], as well as collagen-specific di- and tripeptides, including hydroxyprolylglycine (Hyp-Gly) and prolylhydroxyproline (Pro-Hyp) [22]. These are absorbed intact, via specific transporters on the enterocyte brush border membranes [23], and are increased in circulation following ingestion of CH [22]. Additionally, Pro-Hyp is produced naturally as a product of collagen degradation in damaged tissues [24] where it stimulates proliferation of fibroblasts and subsequent collagen synthesis; collagen-derived Pro-Hyp is therefore considered a fibroblast growth-initiating factor [25]. The effect of endogenous, wound-derived Pro-Hyp appears to be enhanced by Pro-Hyp from dietary CH [24], therefore CH may offer a simple and inexpensive approach to optimizing recovery from connective tissue damage, as occurs with EIMD [2].
Damage to the ECM negatively impacts force transmission [26], storage and utilization of elastic energy during the stretch-shortening cycle [27] and, because of the high density of nociceptors located in the ECM, may be a major contributor to DOMS [28]. As such, enhancing the rate of repair is likely important for recovery. Indeed, there is some, limited, evidence to show that CH attenuates several markers of EIMD, most notably DOMS [29,30] and movements that rely on the stretch-shortening cycle [27,29]. Greater evidence for such benefits may provide economic opportunities and optimize the use of a food industry waste product, thus helping to improve the sustainability and environmental impact of the protein industry by reducing the reliance on DP. Although studies have compared the effects of CH and DP on rates of protein synthesis [31], and a combination of whey and CH on EIMD [6], to date the separate effects of DP and CH have not been directly compared. A greater understanding of whether either protein source is better than the other, or indeed better than a placebo, may help inform consumers who are considering protein supplementation as an aid for muscle recovery. Therefore, we compared the effects of CH and DP on acute recovery from EIMD. It was hypothesised that, when consumed in the days after eccentric exercise, CH would reduce ratings of DOMS, increase recovery of muscle function, and attenuate bloodborne biomarkers of muscle damage and inflammation following EIMD, to an equal or greater extent than an equivalent amount of protein from DP, and that both protein sources would be more effective than an isoenergetic placebo (PLA).
2. Materials and Methods
2.1. Participants
Thirty-three active, healthy males, aged between 18-40 years participated in the study. All participants performed aerobic and resistance exercise at least twice per week in the six months prior to the study and, based on their maximal oxygen uptake (VO2max; Table 1) had fair to good aerobic fitness [32]. Individuals who regularly consumed protein or other potentially ergogenic supplements (e.g., pre-workout products, branched chain amino acids, or creatine monohydrate), consumed more than 1.6 g protein/kg body mass/day, who were vegan or vegetarian, and/or who were participating in other research studies were excluded. Participants completed a 24 hour diet record one week before familiarisation to ascertain their habitual protein consumption, daily energy intake, and if they were consuming any ergogenic supplements. This was analysed by a nutritionist and was used to determine each participant’s suitability for participation. Potential participants who habitually consumed greater than 1.6 g protein/kg body mass/day and/or consumed ergogenic supplements were excluded from the study. If suitable, participants were asked to attend a familiarisation session in the Human Performance Laboratory, School of Sport, Exercise and Nutrition at Massey University, Palmerston North. Participants were instructed to maintain their habitual diet and refrain from strenuous exercise, alcohol, and anti-inflammatory drugs from 48 hours before the main trial and for the duration of the study. All participants were volunteers, recruited by means of public advertisement. The recruitment and data collection process is outlined in Figure 1. Health screening and written informed consent was completed prior to familiarisation. Ethical approval was obtained from the New Zealand Health and Disability Ethics Committee (HDEC EXP 12330) and the study was registered with the Australian and New Zealand Clinical Trials Register (ACTRN12622000529741).
2.2. Experimental Design
A double-blind, placebo controlled, between-subjects design was used to compare the effects of CH, DP and PLA on recovery from 30 minutes of downhill running. Participants were stratified by VO2max then randomly assigned to one of three groups (CH, DP, PLA).
During the familiarisation session, participants completed a health screening questionnaire and provided informed written consent, before individual characteristics were collected (Table 1). They were then familiarised with measures of muscle soreness, muscle function, and the muscle-damaging protocol (downhill running). They then completed a VO2max test to establish running speeds for use in the main trial. Having had an opportunity to ask any further questions, they were then provided with a plastic shaker that contained 61.6 g (1000 kJ) of maltodextrin powder and were instructed to mix this with 250 ml of water and consume it two hours before returning to the laboratory for the main trial. This drink ensured that each participant consumed an equal amount of energy prior to the downhill run and, because each treatment contained 1000 kJ, that energy intake two hours before each measure (pre-downhill run (PRE), 24, 48 and 72 hours post downhill run) was the same.
At least one week after familiarisation, participants returned to the laboratory for the main trial, at a convenient time for them. To understand and compare the effects of the interventions used in this study, and to allow for comparison with other similar studies [6,9,10,27,29,33,34,35,36,37,38,39,40], a series of commonly used, validated measures of EIMD were chosen [41]. PRE indices of EIMD were measured (blood sampling, soreness, muscle function and running economy) and then participants completed 30 minutes of downhill running at 80% of their predetermined VO2max speed. After a 30 minute rest, indices of EIMD were measured again, and participants consumed their first supplement drink (CH, DP or PLA).
For the three subsequent follow up visits (24, 48 and 72 hours post downhill run), participants were instructed to consume their allocated supplement drink two hours before returning to the laboratory.
2.3. Supplements
To ensure double blinding, the supplement powders (CH (bovine collagen hydrolysate; FoodPilot, Massey University, New Zealand, and maltodextrin; Archer Daniels Midland Company, IL, USA), DP (milk protein concentrate 470; Fonterra Cooperative Group Ltd, New Zealand, and maltodextrin), and PLA (maltodextrin)) were sealed in foil packaging and labelled A, B, or C by staff not involved in the study. Prototype spray-dried enzymatic CH was prepared conventionally from frozen, fresh dehaired cow hide in the FoodPilot, Massey University, Palmerston North, New Zealand. Hide was provided by Southern Pastures (NZ) Ltd (New Zealand Business Number 9429031978873). While previous studies have used whey, casein or whole milk, we used milk protein concentrate which contains both whey and casein. It is believed that consuming this has a synergistic effect, where simultaneously there is an immediate effect from faster-acting whey protein and also a sustained effect from slower-acting casein protein (Lacroix et al., 2006). All supplements were isoenergetic and flavour-matched with artificial and natural vanilla flavourings (see Table 2 and Table S1 for supplement details and amino acid profiles, respectively). The CH and DP supplements also contained an equal amount of protein (25 g [42]). Each serving was mixed in a plastic shaker with 250 ml of water and then consumed.
2.4. VO2max
A graded treadmill running test was used to determine participants’ oxygen consumption at four submaximal running speeds and to ascertain VO2max (L/min). Participants were fitted with a silicone mask that covered their nose and mouth, and a heart rate strap (Polar Electro Oy, Finland) was fitted around the chest. Breath-by-breath gas analysis was performed, and heart rate measured continuously throughout the test using a metabolic cart (Quark CPET, Cosmed, Italy). Participants ran continuously on a motorized treadmill (True, MO, USA) at 1% incline for four increasingly faster, predetermined, submaximal speeds, for four minutes per stage. After the last submaximal stage, the speed was increased by 1 km/hour every minute until VO2max was achieved. The relationship between submaximal oxygen consumption and running speed was used to formulate a linear regression equation. This equation, in conjunction with VO2max, was used to calculate running speed at 60% and 80% VO2max for each participant.
2.5. Muscle-Damaging Exercise Protocol
Previous studies investigating the effects of protein supplementation on recovery have used a range of exercise modalities, including maximal eccentric knee extensions [10,15,35,36,40,43], drop jumps [6,27,29,33,38,44], various resistance exercise protocols [7,11,14,30,31,37,39] and downhill running [13,45]. As such, there is no standard methodology used to experimentally cause EIMD. In order to minimse participant burden and avoid the repeated bout effect [46], we asked participants to complete a single bout of downhill running. Bontemps et al. [47] suggest that downhill running has direct applicability to real world exercise scenarios, such as off-road/trail and on-road running, and that it is appropriate for inducing EIMD in participants who are unfamiliar with this mode of exercise, as was the case with our participants. Additionally, downhill running has been shown to specifically alter the measures used in our study [47].
2.6. Muscle Soreness
A visual analogue scale (VAS) was used to assess participants’ self-reported muscle soreness. After holding a bodyweight squat for three seconds at a 90° knee angle, participants were asked to rate the muscle soreness of their lower body on a scale of 0 - 10 (0 being no soreness and 10 being extreme soreness) by marking a vertical line through a 100 mm horizontal line [38]. Using the same VAS, participants also rated muscle soreness of their right quadriceps after performing three maximal voluntary isometric contractions (MVIC) of the right knee extensors [36]. The distance from zero on the VAS was recorded and compared between time points.
2.7. Muscle Function Measures
2.7.1. Counter Movement Jump
Counter movement jump (CMJ) height (cm) was measured using a digital jump mat (SmartSpeed, Australia). Participants stood on the mat, placed their hands on their hips, and used a counter movement to perform a maximal vertical jump, without any tucking of the knees while in flight [27]. Three CMJ attempts were made, with 30 seconds rest in between jumps. The highest jump was used for analysis.
2.7.2. Isometric Midthigh Pull
Peak isometric force of the lower body was determined using an isometric midthigh pull (IMTP [50]). Participants stood on a custom-made platform, bending the hips and knees to 120° and 140°, respectively. Measured with a goniometer at each time point, these joint angles ensured that the bar was positioned at approximately midthigh level [51]. The bar was connected to the platform and a load cell via a chain. After a verbal countdown, participants were told to produce maximal force for three seconds by attempting to extend at the hips and knees. Peak force (N) was then recorded, with the best out of three attempts used for analysis.
2.7.3. MVIC
MVIC of the right knee extensors was assessed using a custom-made isometric dynamometer. Participants were seated upright with hips and knees at 90° flexion and a seat belt was fastened across their lap. A strap was also placed around their right ankle, securing them to a lever arm that was attached to a load cell. The load cell was connected to a custom-made amplifier and data was recorded using a Powerlab data acquisition unit (ADInstruments, Australia) with force (N) recorded in Chart for Windows (v8, ADInstruments, Australia). After being strapped in place, a three second countdown was given, and the participant attempted to maximally extend their right knee for three seconds [52]. They repeated this three times, with 30 seconds rest between attempts. The highest peak force was recorded and used for analysis.
2.8. Running Economy
Participants warmed up for five minutes on a motorised treadmill, set at a 1% incline, at 60% of their previously determined VO2max speed. The speed was then increased to 80% of VO2max speed, an intensity that has been shown to be impacted after downhill running [48], for an additional five minutes. Respiratory gases were sampled and analysed continuously and VO2 (L/min) was averaged over the last minute and used for analysis.
2.9. Blood-Borne Biomarkers
Blood samples were drawn at PRE and 30 minutes, 24, 48, and 72 hours post downhill run from an antecubital vein by a trained phlebotomist and collected into vacutainer tubes (24 ml total per draw). They were then centrifuged and stored at -80°C until analysis. The samples were analysed by Canterbury Health Laboratories (Christchurch, New Zealand) for creatine kinase (CK), high sensitivity C reactive protein (hsCRP) and interleukin-6 (IL-6). Plasma CK and hsCRP were determined on a AU5822 Clinical Chemistry Analyser (Beckman Coulter Inc, CA, USA). IL-6 was analyzed using ELISA (InvitrogenTM, Thermo Fisher Scientific, MA, USA).
2.10. Statistical Analysis
Sample size for repeated measures design was calculated using G*Power software (version 3.1.97; Heinrich-Heine-Universität Düsseldorf, Düsseldorf, Germany). Using 80% power, moderate effect size, and an alpha of 5%, a total of n = 9 participants per group were needed to determine significant differences in responses between groups. However, to account for participant drop out and/or non-compliance, the study aimed to recruit 33 participants as a minimum and 36 participants as a maximum.
All analysis was performed in SPSS (version 28.0.1.1SPSS Inc, IL, USA). Baseline participant characteristics were compared using one-way analysis of variance (ANOVA). Prior to analysis of results, data were examined for normality using the Shapiro-Wilk test. Non-normal data (CK, hsCRP and IL-6) were nlog transformed prior to analysis. Mauchley’s test was used to assess sphericity () and, where the assumption of sphericity was violated, adjustments to the degrees of freedom were made ( > 0.75 = Huynh-Feldt; < 0.75 = Greenhouse-Geisser). After examining for normality, a two-factor mixed ANOVA with repeated measures was used to identify differences between treatments (DP, PLA or CH), time (Pre and 30 minutes, 24, 48 and 72 hours post) and the treatment x time interaction. Where main or interaction effects were identified, post-hoc analysis using the Bonferroni adjustment was carried out. Partial eta squared was used to determine the effect size (small effect: ηp2 = > 0.01, medium effect: ηp2 = > 0.06, large effect: > 0.14). Statistical significance was set to P < 0.05. All data are reported as mean ± SD.
3. Results
3.1. Participant Characteristics
No differences in mean age, height, body mass, aerobic fitness (VO2max), downhill running speed, and energy and protein intake between treatment groups were found (all P > 0.35; Table 1).
3.2. Muscle Soreness
Muscle soreness increased following downhill running across all treatments (Figure 2). Large significant time effects for muscle soreness were observed during the squat (P = < 0.001, ηp2 = 0.514) and during the MVIC (P = < 0.001, ηp2 = 0.424). However, no significant treatment effect for muscle soreness was observed for either measure (during the squat: P = 0.063, ηp2 = 0.168; during the MVIC: P = 0.065, ηp2 = 0.189) and, similarly, no treatment x time interaction effects were found during the squat (P = 0.401, ηp2 = 0.066) or during the MVIC (P = 0.225, ηp2 = 0.94).
3.3. Muscle Function
All measures of muscle function were reduced over time after completion of the downhill run (Figure 3). Large significant time effects were observed across all measures of muscle function (CMJ: P = < 0.001, ηp2 = 0.182; IMTP: P = < 0.001, ηp2 = 0.180; MVIC: P = < 0.001, ηp2 = 0.430; running economy: P = < 0.001, ηp2 = 0.229). Although time effects were observed, we did not find differences between treatments (CMJ: P = 0.332, ηp2 = 0.71; IMTP: P = 0.574, ηp2 = 0.036; MVIC: P = 0.559, ηp2 = 0.038; running economy: P = 0.153, ηp2 = 0.121) and no significant interaction effects were found (CMJ: P = 0.493, ηp2 = 0.059; IMPT: P = 0.994, ηp2 = 0.011; MVIC: P = 0.139, ηp2 = 0.095; running economy P = 0.978, ηp2 = 0.017).
3.4. Blood-Borne Markers
There were large time effects for nlog hsCRP (P = 0.003, ηp2 = 0.143), nlog CK (P = < 0.001, ηp2 = 0.531) and nLog IL-6 (P = 0.013, ηp2 = 0.48) (Figure 4). However, no treatment (hsCRP P = 0.318, ηp2 = 0.084; CK P = 0.488, ηp2 = 0.054; IL-6 P = 0.226, ηp2 = 0.018) or interaction effects (hsCRP P = 0.341, ηp2 = 0.081; CK P = 0.966, ηp2 = 0.022; IL-6 P = 0.261, ηp2 = 0.091) were found. CK and hsCRP peaked 24 hours post-exercise before returning towards baseline levels at 72 hours. IL-6 peaked 30 minutes after exercise; no other time points were significantly different to pre-exercise values.
4. Discussion
EIMD has the potential to reduce performance during subsequent bouts of exercise and/or cause a disruption to normal daily activities [3,4]. According to Robberechts et al. [6], DP has been the standard nutrition intervention used to expedite recovery and minimize the effects of EIMD, and there is a modest body of evidence to suggest that it is beneficial in this context [2]. Additionally, there is growing evidence to suggest that CH may offer similar benefits [27,29,30,53]. However, to the authors’ knowledge, at this time, no one has compared the effects of consuming the two protein sources in the days after damaging exercise. Therefore, this study induced muscle damage to the lower limbs, using downhill running, in order to compare the effects of CH, DP and an isoenergetic PLA on indices of EIMD up to 72 hours post-exercise. All of the indices of EIMD significantly changed over time as a result of 30 minutes of downhill running, suggesting that muscle damage had occurred. However, in contrast to our hypothesis, CH was not equal, nor more beneficial than DP, and neither protein source was better than the PLA.
As expected, the damaging protocol used in our study resulted in large significant changes in muscle function, soreness and blood-borne markers of EIMD over time. However, decrements in muscle function were mostly mild with significant changes in running economy and CMJ limited to 30 minutes and 24 hours post-exercise, respectively, while no significant changes in IMTP were evident at anytime point, for any treatment. Decreases in MVIC force occured with each treatment, albeit at different times and, again, to a mild level [54]. Similarly, measures of soreness changed after exercise with the lowest change occuring with PLA. However, despite treatment effects approaching significance, to say that PLA was more beneficial than either protein source would be speculative. As reported elsewhere CK [55] and hsCRP [56] peaked at 24 hours, before returning towards baseline in the days after exercise, for all treatments. IL-6 increased in response to exercise [57], but does not appear to have been elevated by subsequent muscle damage. Collectively, these results suggest that 30-minutes of downhill running induced a mild to moderate amount of muscle damage.
The proposed mechanisms responsible for any benefit of DP or CH on recovery are theoretically sound, in that DP provides amino acids for the repair and synthesis of skeletal muscle [7,31] and CH provides amino acids and peptides, in particular Pro-Hyp, for the repair of connective tissue [25]. Additionally, both protein sources have anti-inflammatory actions [43,58] which may further benefit recovery. However, despite this, the outcomes of EIMD studies are inconsistent. DP, in its various forms, consumed in the days after damaging exercise has been shown to benefit the recovery of muscle function [9,10,11,35,45], however many more studies have failed to see an effect [12,13,14,15,33,34,37,38,40,59,60,61]. The same is true in regard to DOMS, with only a small number of studies reporting that DP can attenuate acute muscle soreness [36,39,43]. In fact, the majority of studies have failed to observe a benefit [9,10,12,13,14,15,33,34,35,37,38,40,45,59,60,61,62]. Further, of the studies mentioned, none found an effect of DP on inflammation and ony five saw an effect on bloodborne markers of muscle damage [9,13,35,36,39]. In line with this overwhelming evidence, and therefore perhaps not surprising, we also failed to see an effect of DP on any indices of EIMD, at any time point of recovery.
In the studies specifically investigating the influence of CH on EIMD, a positive effect on muscle function has been shown, but only during the counter movement jump [27,29]; a benefit to maximal isometric force recovery has not been observed. Given the potential effect of CH on the ECM, we expected to see some benefit on DOMS [29,30] and muscle performance [27,29]; in particular the counter movement jump and running economy, which both rely on the stretch shortening cycle. However, this was not a given as the results of previous studies are inconsistent [6,27,29,30,53]. The disparate findings may in part be due to the various issues that plague many protein intervention studies [63]. These include, but are not limited to, different modes of exercise used to induce, and criteria used to assess, EIMD; dosing, timing and duration of interventions; participant training history; choice of control/placebo [6,35,36,39]; insufficient levels of damage; studies being under powered [15,27,62]; and perhaps most importantly [61], a lack of control over dietary protein intake [7,12,13,14,33,35,38,60].
Most studies investigating the effects of DP have provided the supplement post-exercise while, conversely, participants in studies using CH have consumed the supplement in varying doses in the days and weeks leading up to and, in some case, also after damaging exercise [6,27,29,30,44,53]. Aussieker et al. [31] appear to be the exception, giving a single dose of CH post-exercise when investigating rates of protein synthesis. Therefore, although the timing used in this study is in line with the majority of studies investigating DP, it is possible that the supplementation period used in our study was insufficient and/or inappropriate to provide any benefit from CH.
It is unclear whether the positive effects CH has on indices of EIMD are the result of a protective effect provided by an increase in intramuscular collagen and/or due to an increased rate of cellular repair in the days after damaging exercise. The timing of our supplemention would only impact the latter, by providing substates to accelerate tissue repair and remodelling. Together with the lack of change in muscle connective protein synthesis reported by Aussieker et al. [31], our results suggest that, when only consumed after eccentric exercise, CH does not enhance recovery. As such, long term supplementation may be required in order to provide a protective effect to connective tissue, prior to eccentric exercise. This benefit was recently suggested by Bishof et al. [44] who found that supplementing concurrent training with CH over 12 weeks enhanced the repeated bout effect, reducing the level of damage occuring after a second bout of eccentric exercise. Additonally, Kuwaba et al. [53] reported that eccentric exercise was easier after 33 days of supplementation with CH. Although the reason for this is unclear, it is possible that adaptation to connective tissue, via an increase in hypoxia-inducible factor alpha 1 (HIF-α), heat shock proteins and other initiators of collagen synthetic pathways [64], reduced stress on the musculotendenous system, and enhanced force transmission and the SSC during repeated squats. As the majority of studies have only compared CH to a placebo [27,29,30,44,53] or they have lacked a placebo [6], it is unclear whether any protective effect is unique to CH, or is provided by protein in general. The findings of Oikawa et al. [65] suggest that increases in intramusuclar collagen are unaffected by CH or whey protein and, additionally, Rindom et al. [42] found that consuming whey protein or CH during a period of intensified training provided similar results on recovery, however they used CH as their low quality protein placebo and did not have a true control, so it is unclear if either protein was beneficial. Studies feeding DP in the days and weeks prior to eccentric exercise do not provide clarity, as results are mixed [6,37,38,39].
It has been suggested that collagen may aid in the repair of the ECM through the delivery of non-essential amino acids glycine, proline, and hydroxyproline, and Pro-Hyp, which are believed to enhance collagen synthesis [66]. However, according to Prowting et al. [27], it is unclear whether the extra provision of non-essential amino acids is required to increase collagen synthesis or that it is possible for the body to sufficiently synthesise them without the need for an exogenous supply. Furthermore, despite CH derived peptides appearing in circulation after ingestion [22], collagen supplementation does not enhance collagen synthesis after EIMD [6,27,29]. The inconsistent views on how CH effects collagen synthesis may stem from the difficulty identifying the synthesis of collagen in skeletal muscle. It is difficult to accurately measure collagen synthesis without performing muscle biopsies [67] and, moreover, commonly used biomarkers of collagen synthesis are not specific to the synthesis of collagen in connective tissue, as they also reflect the synthesis of collagen in bone [27]. Clearly, standardised methods and more invasive measures may be required to fully understand the benefits and mechanisms of CH in the future.
As has been done by others [11,12,34,35,36,40] we used a combination of protein and carbohydrate for our treatments and matched this with an isoenergetic placebo. While carbohydrate may enhance the effect of protein by promoting the uptake of amino acids [68], it is a biologically active nutrient, in its own right. Alone, carbohydrate has been shown to improve recovery by replenishing glycogen and providing energy for cellular recovery [12]. It can also contribute to anabolism in a similar way to the mechanistic actions of DP (e.g., by improving net protein balance [69]). Indeed, some studies have even found it to be more effective than dairy protein for recovery from EIMD [38,62]. As a result, we cannot rule out the effect carbohydrate may have had alone and in combination with DP and CH; perhaps all treatments improved recovery equally.
As noted above, protein intervention studies are not without their limitations and this study is no different. Although we screened participants based on their habitual dietary protein intake, we did not control this during the intervention period. Therefore, it is possible participants consumed higher amounts of protein and, as such, protein from the treatments may not have had any benefit [70]. Additonally, we only recruited recreationally active male participants, and therefore it is unclear whether we would see the same results in individuals with different fitness levels and in females. Further, while downhill running induced significant changes in our measures, an exercise protocol that induces greater damage may provide a stronger stimulus for the interventions to interact with. Based on these limitations, and other gaps in our knowledge, we suggest that future research should control dietary protein intake, investigate different doses and combinations of proteins [71], different supplementation and exercise protocols, and the use of different populations. Additonally, there is a need to better understand the mechanisms responsible for the potential benefits of prolonged CH supplementation, which may require the use of more invasive measures than simply using the common measures of EIMD and changes in muscle function.
5. Conclusions
Our findings suggest that, when consumed for three days after damaging exercise, CH or DP does not expedite the rate of recovery any better than an isoenergetic placebo. Our findings add to the growing evidence that suggests DP has little benefit for recovery from EIMD. For CH to have a beneficial effect on how muscle responds to eccentric exercise, consuming CH for a prolonged period, of at least nine days [29], prior to exercise may be necessary. We propose that individuals specifically wanting to speed up recovery after strenuous, damaging exercise should no longer consider acute, post-exercise protein supplementation as a reliable and valuable strategy.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Amino acid profile of collagen hydrolysate (CH) and milk protein concentrate (DP).
Author Contributions
Conceptualization, J.C. and M.B.; methodology, J.C. and M.B.; formal analysis, R.B. and M.B.; investigation, R.B, K.S, M.B.; writing—original draft preparation, R.B and M.B; writing—review and editing, J.C, K.S.; supervision, M.B.; project administration, R.B.; funding acquisition, J.C and M.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Ministry of Business, Innovation and Employment, New Zealand, grant number HVN1943.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the New Zealand Health and Disability Ethics Committee (HDEC EXP 12330) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.”
Data Availability Statement
Data is available from the corresponding author on request.
Acknowledgments
The authors wish to thank the participants for the time and effort.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Owens DJ, Twist C, Cobley JN, Howatson G, Close GL. Exercise-induced muscle damage: What is it, what causes it and what are the nutritional solutions? European Journal of Sport Science. 2019;19(1):71-85.
- Bongiovanni T, Genovesi F, Nemmer M, Carling C, Alberti G, Howatson G. Nutritional interventions for reducing the signs and symptoms of exercise-induced muscle damage and accelerate recovery in athletes: current knowledge, practical application and future perspectives. European Journal of Applied Physiology. 2020;120:1965-96. [CrossRef]
- Hody S, Croisier J-L, Bury T, Rogister B, Leprince P. Eccentric muscle contractions: risks and benefits. Frontiers in Physiology. 2019;10:442082. [CrossRef]
- Tesarz J, Schuster AK, Hartmann M, Gerhardt A, Eich W. Pain perception in athletes compared to normally active controls: a systematic review with meta-analysis. Pain. 2012;153(6):1253-62. [CrossRef]
- O’Connor E, Mündel T, Barnes MJ. Nutritional compounds to improve post-exercise recovery. Nutrients. 2022;14(23):5069. [CrossRef]
- Robberechts R, Poffé C, Ampe N, Bogaerts S, Hespel P. Partly substituting whey for collagen peptide supplementation improves neither indices of muscle damage nor recovery of functional capacity during eccentric exercise training in fit males. International Journal of Sport Nutrition and Exercise Metabolism. 2023;1(aop):1-10. [CrossRef]
- West DW, Abou Sawan S, Mazzulla M, Williamson E, Moore DR. Whey protein supplementation enhances whole body protein metabolism and performance recovery after resistance exercise: a double-blind crossover study. Nutrients. 2017;9(7):735. [CrossRef]
- avis GF, Jameson TS, Dirks ML, Lee BP, Abdelrahman DR, Murton AJ, et al. Improved recovery from skeletal muscle damage is largely unexplained by myofibrillar protein synthesis or inflammatory and regenerative gene expression pathways. American Journal of Physiology. 2021;320(2):E291-E305. [CrossRef]
- Brown MA, Stevenson EJ, Howatson G. Whey protein hydrolysate supplementation accelerates recovery from exercise-induced muscle damage in females. Applied Physiology, Nutrition, and Metabolism. 2018;43(4):324-30. [CrossRef]
- Buckley JD, Thomson RL, Coates AM, Howe PR, DeNichilo MO, Rowney MK. Supplementation with a whey protein hydrolysate enhances recovery of muscle force-generating capacity following eccentric exercise. Journal of Science and Medicine in Sport. 2010;13(1):178-81. [CrossRef]
- Cooke MB, Rybalka E, Stathis CG, Cribb PJ, Hayes A. Whey protein isolate attenuates strength decline after eccentrically-induced muscle damage in healthy individuals. Journal of the International Society of Sports Nutrition. 2010;7:1-9. [CrossRef]
- Gee TI, Woolrich TJ, Smith MF. Effectiveness of whey protein hydrolysate and milk-based formulated drinks on recovery of strength and power following acute resistance exercise. Journal of Human Kinetics. 2019;68(1):193-202. [CrossRef]
- Nieman DC, Zwetsloot KA, Simonson AJ, Hoyle AT, Wang X, Nelson HK, et al. Effects of whey and pea protein supplementation on post-eccentric exercise muscle damage: a randomized trial. Nutrients. 2020;12(8):2382. [CrossRef]
- Ormsbee MJ, Saracino PG, Morrissey MC, Donaldson J, Rentería LI, McKune AJ. Pre-sleep protein supplementation after an acute bout of evening resistance exercise does not improve next day performance or recovery in resistance trained men. Journal of the International Society of Sports Nutrition. 2022;19(1):164-78. [CrossRef]
- Saracino PG, Saylor HE, Hanna BR, Hickner RC, Kim J-S, Ormsbee MJ. Effects of pre-sleep whey vs. plant-based protein consumption on muscle recovery following damaging morning exercise. Nutrients. 2020;12(7):2049. [CrossRef]
- Pearson AG, Hind K, Macnaughton LS. The impact of dietary protein supplementation on recovery from resistance exercise-induced muscle damage: A systematic review with meta-analysis. European Journal of Clinical Nutrition. 2023;77(8):767-83. [CrossRef]
- Poore J, Nemecek T. Reducing food’s environmental impacts through producers and consumers. Science. 2018;360(6392):987-92. [CrossRef]
- Patel V, Aggarwal K, Dhawan A, Singh B, Shah P, Sawhney A, et al., editors. Protein supplementation: the double-edged sword. Baylor University Medical Center Proceedings; 2024: Taylor & Francis.
- Kurek MA, Onopiuk A, Pogorzelska-Nowicka E, Szpicer A, Zalewska M, Półtorak A. Novel protein sources for applications in meat-alternative products—Insight and challenges. Foods. 2022;11(7):957. [CrossRef]
- Holwerda AM, van Loon LJ. The impact of collagen protein ingestion on musculoskeletal connective tissue remodeling: a narrative review. Nutrition Reviews. 2022;80(6):1497-514.
- Skov K, Oxfeldt M, Thøgersen R, Hansen M, Bertram HC. Enzymatic hydrolysis of a collagen hydrolysate enhances postprandial absorption rate—a randomized controlled trial. Nutrients. 2019;11(5):1064. [CrossRef]
- Taga Y, Kusubata M, Ogawa-Goto K, Hattori S. Stable isotope-labeled collagen: a novel and versatile tool for quantitative collagen analyses using mass spectrometry. Journal of Proteome Research. 2014;13(8):3671-8. [CrossRef]
- Abe M, Hoshi T, Tajima A. Characteristics of transmural potential changes associated with the proton-peptide co-transport in toad small intestine. Journal of Physiology. 1987;394(1):481-99. [CrossRef]
- Sato K, Jimi S, Kusubata M. Generation of bioactive prolyl-hydroxyproline (Pro-Hyp) by oral administration of collagen hydrolysate and degradation of endogenous collagen. International Journal of Food Science & Technology. 2019;54(6):1976-80. [CrossRef]
- Sato K, Asai TT, Jimi S. Collagen-derived di-peptide, prolylhydroxyproline (Pro-Hyp): a new low molecular weight growth-initiating factor for specific fibroblasts associated with wound healing. Frontiers in Cell and Developmental Biology. 2020;8:548975. [CrossRef]
- Tenberg S, Nosaka K, Wilke J. The relationship between acute exercise-induced changes in extramuscular connective tissue thickness and delayed onset muscle soreness in healthy participants: a randomized controlled crossover trial. Sports Medicine-Open. 2022;8(1):57. [CrossRef]
- Prowting JL, Bemben D, Black CD, Day EA, Campbell JA. Effects of collagen peptides on recovery following eccentric exercise in resistance-trained males—A pilot study. International Journal of Sport Nutrition and Exercise Metabolism. 2020;31(1):32-9. [CrossRef]
- Wilke J, Behringer M. Is “delayed onset muscle soreness” a false friend? The potential implication of the fascial connective tissue in post-exercise discomfort. International Journal of Molecular Sciences. 2021;22(17):9482. [CrossRef]
- Clifford T, Ventress M, Allerton DM, Stansfield S, Tang JC, Fraser WD, et al. The effects of collagen peptides on muscle damage, inflammation and bone turnover following exercise: a randomized, controlled trial. Amino Acids. 2019;51:691-704. [CrossRef]
- Lopez HL, Ziegenfuss TN, Park J. Evaluation of the effects of biocell collagen, a novel cartilage extract, on connective tissue support and functional recovery from exercise. Integrative Medicine: A Clinician's Journal. 2015;14(3):30.
- Aussieker T, Hilkens L, Holwerda AM, Fuchs CJ, Houben LH, Senden JM, et al. Collagen protein ingestion during recovery from exercise does not increase muscle connective protein synthesis rates. Medicine and Science in Sports and Exercise. 2023;55(10):1792. [CrossRef]
- Bayles MP. ACSM's exercise testing and prescription: Lippincott Williams & Wilkins; 2023.
- Apweiler E, Wallace D, Stansfield S, Allerton DM, Brown MA, Stevenson EJ, et al. Pre-bed casein protein supplementation does not enhance acute functional recovery in physically active males and females when exercise is performed in the morning. Sports. 2018;7(1):5. [CrossRef]
- Betts JA, Toone RJ, Stokes KA, Thompson D. Systemic indices of skeletal muscle damage and recovery of muscle function after exercise: effect of combined carbohydrate–protein ingestion. Applied Physiology, Nutrition, and Metabolism. 2009;34(4):773-84. [CrossRef]
- Cockburn E, Hayes PR, French DN, Stevenson E, St Clair Gibson A. Acute milk-based protein–CHO supplementation attenuates exercise-induced muscle damage. Applied Physiology, Nutrition, and Metabolism. 2008;33(4):775-83. [CrossRef]
- Cockburn E, Stevenson E, Hayes PR, Robson-Ansley P, Howatson G. Effect of milk-based carbohydrate-protein supplement timing on the attenuation of exercise-induced muscle damage. Applied Physiology, Nutrition, and Metabolism. 2010;35(3):270-7. [CrossRef]
- Davies RW, Bass JJ, Carson BP, Norton C, Kozior M, Wilkinson DJ, et al. The effect of whey protein supplementation on myofibrillar protein synthesis and performance recovery in resistance-trained men. Nutrients. 2020;12(3):845. [CrossRef]
- Hilkens L, Boerboom M, van Schijndel N, Bons J, van Loon LJ, van Dijk J-W. Bone turnover following high-impact exercise is not modulated by collagen supplementation in young men: A randomized cross-over trial. Bone. 2023;170:116705.
- Hirose N, Sato M, Yanagisawa O, Fukubayashi T. Milk peptide intake may decrease muscle damage after eccentric exercise. International Journal of Sport and Health Science. 2013;11:20-8. [CrossRef]
- White JP, Wilson JM, Austin KG, Greer BK, St John N, Panton LB. Effect of carbohydrate-protein supplement timing on acute exercise-induced muscle damage. Journal of the International Society of Sports Nutrition. 2008;5:1-7. [CrossRef]
- Markus I, Constantini K, Hoffman J, Bartolomei S, Gepner Y. Exercise-induced muscle damage: Mechanism, assessment and nutritional factors to accelerate recovery. European Journal of Applied Physiology. 2021;121:969-92. [CrossRef]
- Rindom E, Nielsen M, Kececi K, Jensen M, Vissing K, Farup J. Effect of protein quality on recovery after intense resistance training. European Journal of Applied Physiology. 2016;116:2225-36. [CrossRef]
- raganidis D, Chondrogianni N, Chatzinikolaou A, Terzis G, Karagounis LG, Sovatzidis A, et al. Protein ingestion preserves proteasome activity during intense aseptic inflammation and facilitates skeletal muscle recovery in humans. British Journal of Nutrition. 2017;118(3):189-200. [CrossRef]
- Bischof K, Stafilidis S, Bundschuh L, Oesser S, Baca A, König D. Reduction in systemic muscle stress markers after exercise-induced muscle damage following concurrent training and supplementation with specific collagen peptides–a randomized controlled trial. Frontiers in Nutrition. 2024;11:1384112. [CrossRef]
- Etheridge T, Philp A, Watt PW. A single protein meal increases recovery of muscle function following an acute eccentric exercise bout. Applied Physiology, Nutrition, and Metabolism. 2008;33(3):483-8. [CrossRef]
- Hyldahl RD, Chen TC, Nosaka K. Mechanisms and mediators of the skeletal muscle repeated bout effect. Exercise and sport sciences reviews. 2017;45(1):24-33. [CrossRef]
- Bontemps B, Vercruyssen F, Gruet M, Louis J. Downhill running: what are the effects and how can we adapt? A narrative review. Sports Medicine. 2020;50(12):2083-110. [CrossRef]
- Chen TC, Nosaka K, Tu J-H. Changes in running economy following downhill running. Journal of Sports Sciences. 2007;25(1):55-63. [CrossRef]
- Chrismas BC, Taylor L, Siegler JC, Midgley AW. A reduction in maximal incremental exercise test duration 48 h post downhill run is associated with muscle damage derived exercise induced pain. Frontiers in Physiology. 2017;8:135. [CrossRef]
- Haff GG, Stone M, O'Bryant HS, Harman E, Dinan C, Johnson R, et al. Force-time dependent characteristics of dynamic and isometric muscle actions. Journal of Strength and Conditioning Research. 1997;11(4):269-72.
- Beckham G, Mizuguchi S, Carter C, Sato K, Ramsey M, Lamont H, et al. Relationships of isometric mid-thigh pull variables to weightlifting performance. Journal of Sports Medicine and Physical Fitness. 2013;53(5):573-81.
- Barnes MJ, Mündel T, Stannard SR. The effects of acute alcohol consumption and eccentric muscle damage on neuromuscular function. Applied Physiology, Nutrition, and Metabolism. 2012;37(1):63-71. [CrossRef]
- Kuwaba K, Kusubata M, Taga Y, Igarashi H, Nakazato K, Mizuno K. Dietary collagen peptides alleviate exercise-induced muscle soreness in healthy middle-aged males: a randomized double-blinded crossover clinical trial. Journal of the International Society of Sports Nutrition. 2023;20(1):2206392. [CrossRef]
- Warren GL, Lowe DA, Armstrong RB. Measurement tools used in the study of eccentric contraction-induced injury. Sports medicine. 1999;27:43-59. [CrossRef]
- Brancaccio P, Maffulli N, Limongelli FM. Creatine kinase monitoring in sport medicine. British medical bulletin. 2007;81(1):209-30. [CrossRef]
- Paulsen G, Ramer Mikkelsen U, Raastad T, Peake JM. Leucocytes, cytokines and satellite cells: what role do they play in muscle damage and regeneration following eccentric exercise? Exercise immunology review. 2012;18.
- Nash D, Hughes MG, Butcher L, Aicheler R, Smith P, Cullen T, et al. IL-6 signaling in acute exercise and chronic training: Potential consequences for health and athletic performance. Scandinavian Journal of Medicine & Science in Sports. 2023;33(1):4-19. [CrossRef]
- León-López A, Fuentes-Jiménez L, Hernández-Fuentes AD, Campos-Montiel RG, Aguirre-Álvarez G. Hydrolysed collagen from sheepskins as a source of functional peptides with antioxidant activity. International Journal of Molecular Sciences. 2019;20(16):3931. [CrossRef]
- Burnley ECD, Olson AN, Sharp RL, Baier SM, Alekel DL. Impact of protein supplements on muscle recovery after exercise-induced muscle soreness. Journal of Exercise Science and Fitness. 2010;8(2):89-96. [CrossRef]
- Dahlstrom EC. Impact of protein supplementation on muscle recovery after exercise-induced muscle soreness: Iowa State University; 2007.
- Eddens L, Browne S, Stevenson EJ, Sanderson B, van Someren K, Howatson G. The efficacy of protein supplementation during recovery from muscle-damaging concurrent exercise. Applied Physiology, Nutrition, and Metabolism. 2017;42(7):716-24. [CrossRef]
- Ten Haaf DS, Flipsen MA, Horstman AM, Timmerman H, Steegers MA, De Groot LC, et al. The effect of protein supplementation versus carbohydrate supplementation on muscle damage markers and soreness following a 15-km road race: a double-blind randomized controlled trial. Nutrients. 2021;13(3):858. [CrossRef]
- Pasiakos SM, Lieberman HR, McLellan TM. Effects of protein supplements on muscle damage, soreness and recovery of muscle function and physical performance: a systematic review. Sports Medicine. 2014;44:655-70. [CrossRef]
- Oertzen-Hagemann V, Kirmse M, Eggers B, Pfeiffer K, Marcus K, de Marées M, et al. Effects of 12 weeks of hypertrophy resistance exercise training combined with collagen peptide supplementation on the skeletal muscle proteome in recreationally active men. Nutrients. 2019;11(5):1072. [CrossRef]
- Oikawa SY, Kamal MJ, Webb EK, McGlory C, Baker SK, Phillips SM. Whey protein but not collagen peptides stimulate acute and longer-term muscle protein synthesis with and without resistance exercise in healthy older women: a randomized controlled trial. American Journal of Clinical Nutrition. 2020;111(3):708-18. [CrossRef]
- Shaw G, Lee-Barthel A, Ross ML, Wang B, Baar K. Vitamin C–enriched gelatin supplementation before intermittent activity augments collagen synthesis. American Journal of Clinical Nutrition. 2017;105(1):136-43. [CrossRef]
- Kviatkovsky SA, Hickner RC, Ormsbee MJ. Collagen peptide supplementation for pain and function: is it effective? Current Opinion in Clinical Nutrition & Metabolic Care. 2022;25(6):401-6.
- Starkoff BE, Lenz EK, Mattern CO, Too D, Byrne HK. Protein Supplementation Does Not Enhance Recovery from Exercise-Induced Muscle Damage. Journal of Exercise Physiology Online. 2020;23(1).
- Børsheim E, Cree MG, Tipton KD, Elliott TA, Aarsland A, Wolfe RR. Effect of carbohydrate intake on net muscle protein synthesis during recovery from resistance exercise. Journal of Applied Physiology. 2004;96(2):674-8. [CrossRef]
- Schoenfeld BJ, Aragon AA. How much protein can the body use in a single meal for muscle-building? Implications for daily protein distribution. Journal of the International Society of Sports Nutrition. 2018;15:1-6. [CrossRef]
- Deane CS, Bass JJ, Crossland H, Phillips BE, Atherton PJ. Animal, plant, collagen and blended dietary proteins: effects on musculoskeletal outcomes. Nutrients. 2020;12(9):2670. [CrossRef]
Figure 1.
CONSORT flow diagram for recruitemnt and data collection.
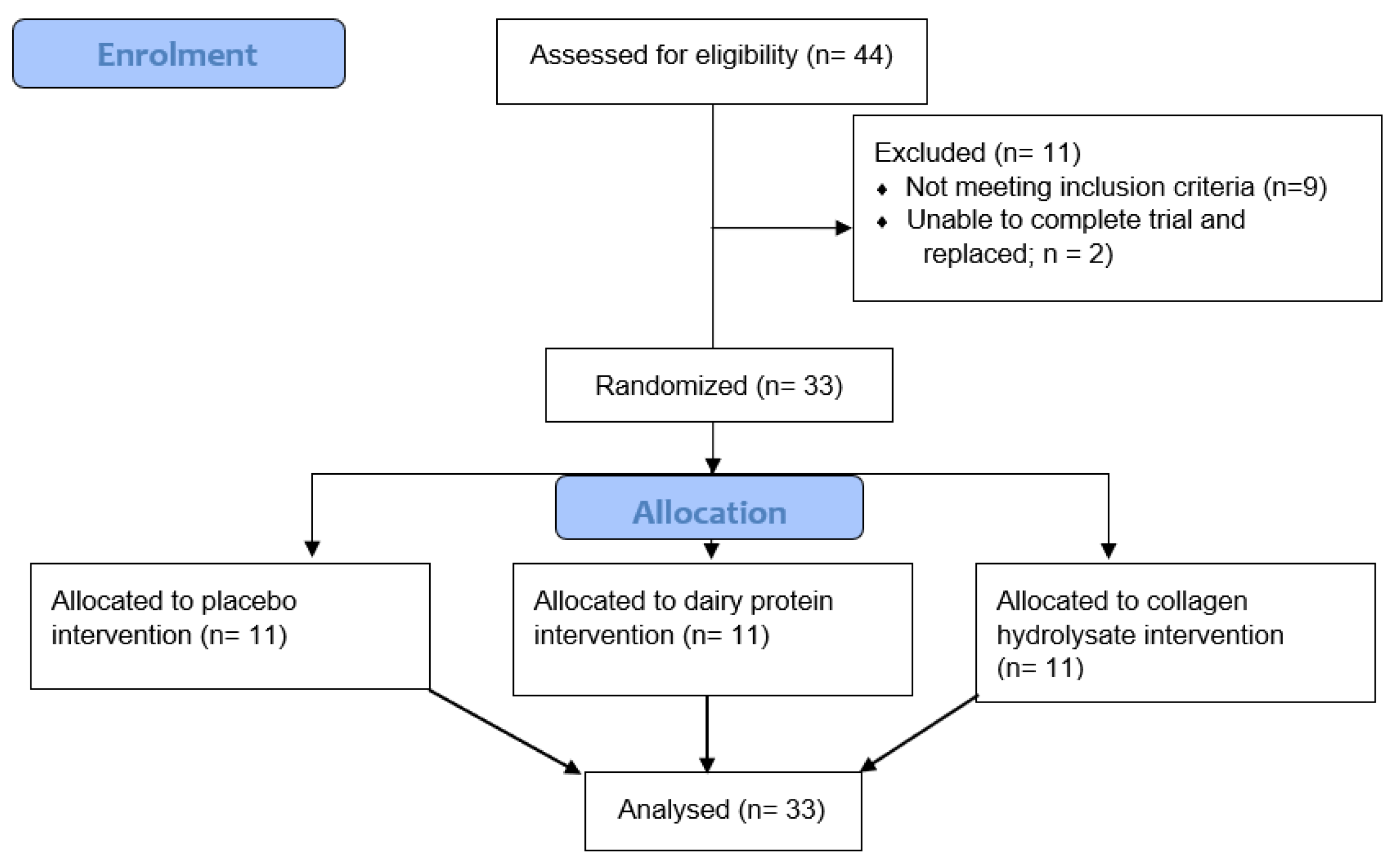
Figure 2.
Muscle soreness, measured on a 100mm visual analogue scale (VAS), during a squat (A) and after three MVICs (B) before (PRE) and after 30 minutes of downhill running. Participants were allocated into dairy protein (n = 11, DP), placebo (n = 11, PLA) or collagen hydrolysate (n = 11, CH) groups. *Different to PRE (P< 0.05); # different to 30 min (P< 0.05); +different to 24h (P< 0.05); ^different to 48h (P< 0.05).
Figure 2.
Muscle soreness, measured on a 100mm visual analogue scale (VAS), during a squat (A) and after three MVICs (B) before (PRE) and after 30 minutes of downhill running. Participants were allocated into dairy protein (n = 11, DP), placebo (n = 11, PLA) or collagen hydrolysate (n = 11, CH) groups. *Different to PRE (P< 0.05); # different to 30 min (P< 0.05); +different to 24h (P< 0.05); ^different to 48h (P< 0.05).
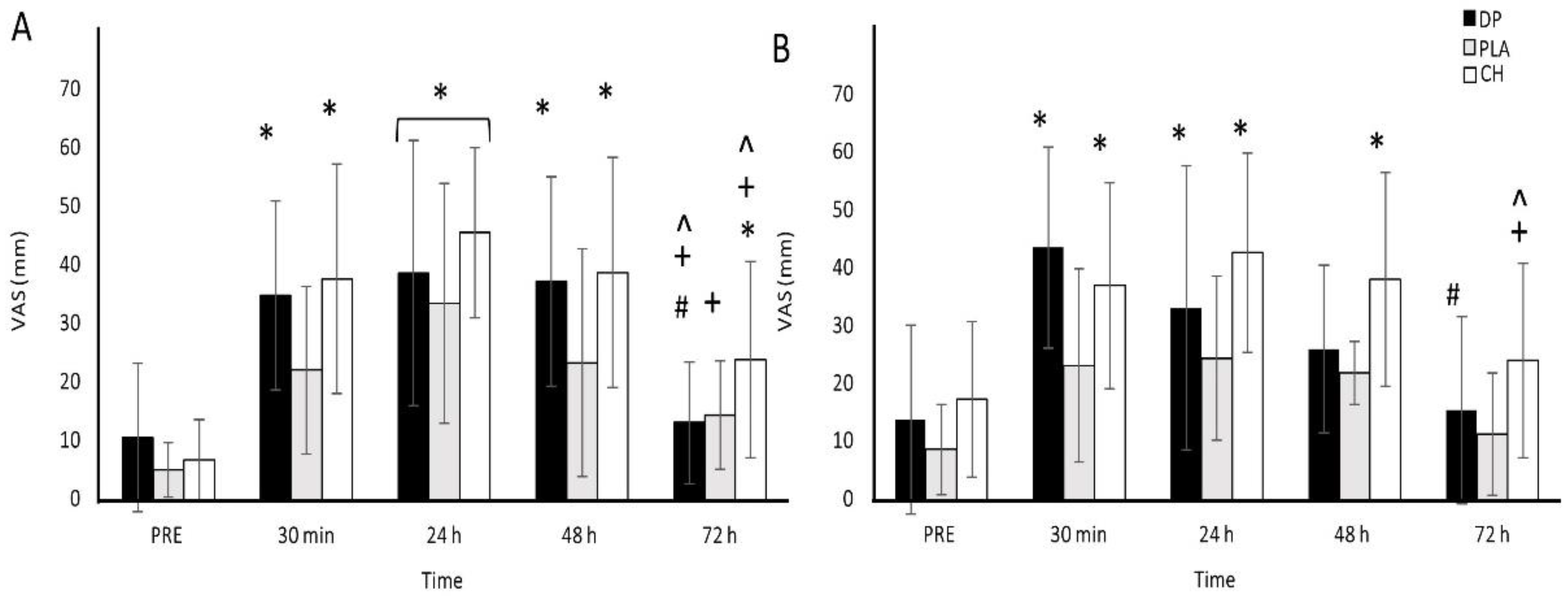
Figure 3.
MVIC (A), IMTP (B), CMJ (C) and running economy (D) before (PRE) and after 30 minutes of downhill running. Participants were allocated into dairy protein (n = 11, DP), placebo (n = 11, PLA) or collagen hydrolysate (n = 11, CH) groups. *Different to PRE (P< 0.05); # different to 30 minutes (P< 0.05).
Figure 3.
MVIC (A), IMTP (B), CMJ (C) and running economy (D) before (PRE) and after 30 minutes of downhill running. Participants were allocated into dairy protein (n = 11, DP), placebo (n = 11, PLA) or collagen hydrolysate (n = 11, CH) groups. *Different to PRE (P< 0.05); # different to 30 minutes (P< 0.05).
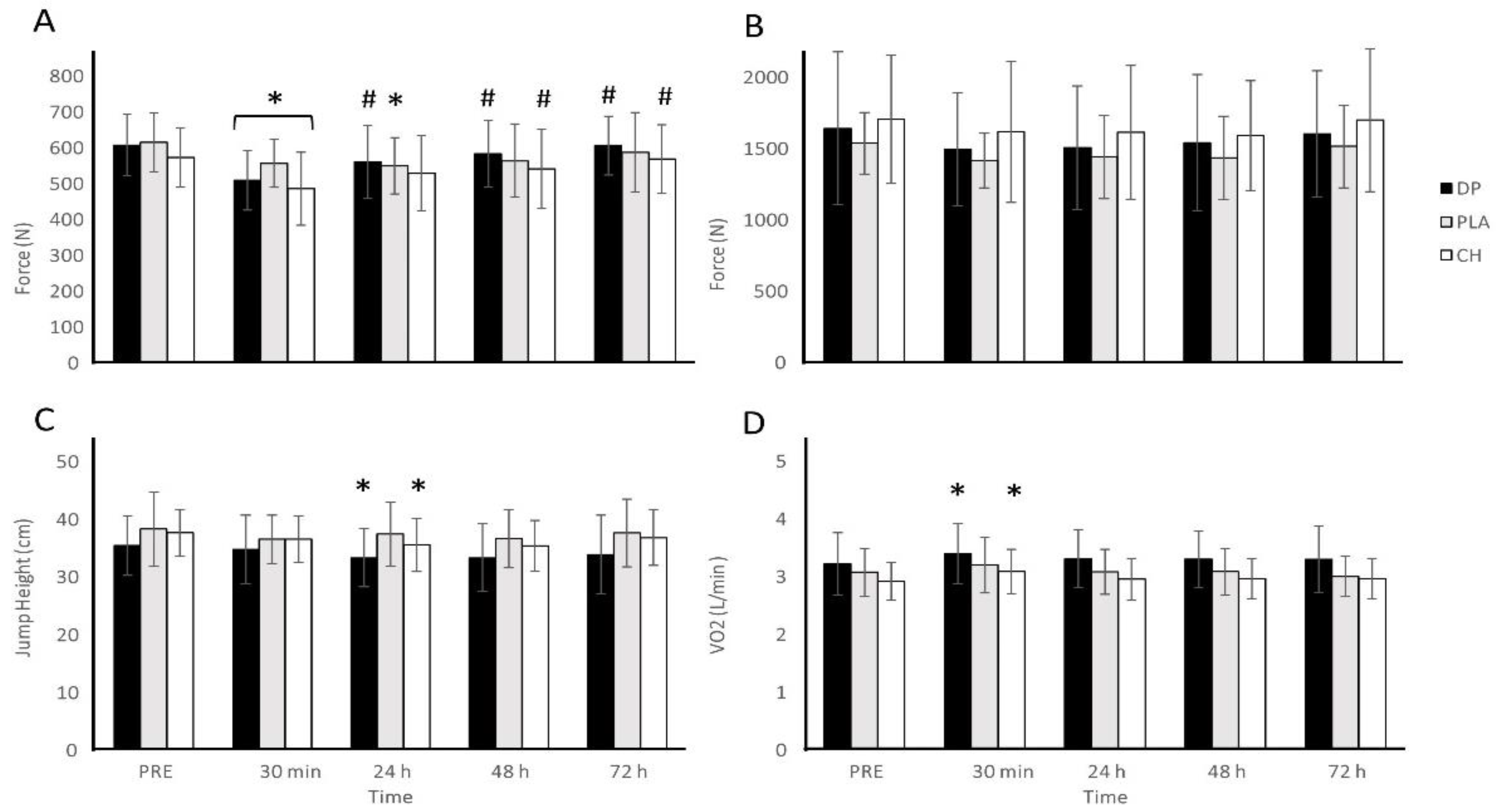
Figure 4.
nLog of high sensitivity C reactive protein (hsCRP; A), interleukin 6 (IL-6; B), and creatine kinase (CK; C) before (PRE) and after 30 minutes of downhill running. Participants were allocated into dairy protein (n = 11, DP), placebo (n = 11, PLA) or collagen hydrolysate (n = 11, CH) groups. *Different to PRE (P< 0.05); # different to 30 min (P< 0.05); +different to 24h (P< 0.05); ^different to 48h (P< 0.05).
Figure 4.
nLog of high sensitivity C reactive protein (hsCRP; A), interleukin 6 (IL-6; B), and creatine kinase (CK; C) before (PRE) and after 30 minutes of downhill running. Participants were allocated into dairy protein (n = 11, DP), placebo (n = 11, PLA) or collagen hydrolysate (n = 11, CH) groups. *Different to PRE (P< 0.05); # different to 30 min (P< 0.05); +different to 24h (P< 0.05); ^different to 48h (P< 0.05).
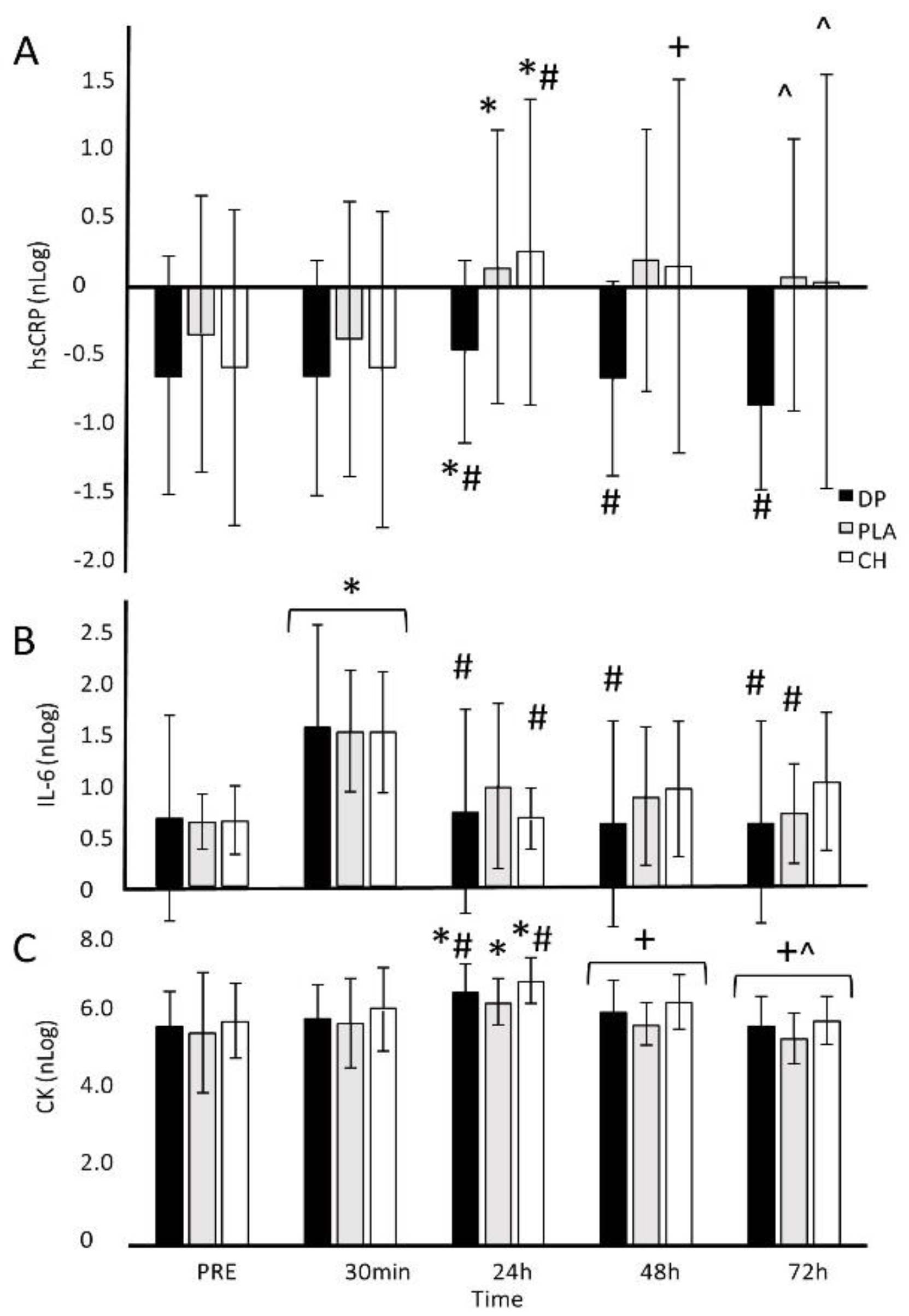

Table 1.
Characteristics of participants in the dairy protein (DP), placebo (PLA) and collagen hydrolysate (CH) groups (mean (SD)). No differences were observed between groups.
Table 1.
Characteristics of participants in the dairy protein (DP), placebo (PLA) and collagen hydrolysate (CH) groups (mean (SD)). No differences were observed between groups.
| DP (n = 11) |
PLA (n = 11) |
CH (n = 11) |
P value | |
|---|---|---|---|---|
| Age (years) | 26.2 ± 7.2 | 23.5 ± 6.1 | 26.6 ± 6.4 | 0.468 |
| Height (cm) | 181.1 ± 11.4 | 182.0 ± 7.6 | 176.0 ± 5.3 | 0.220 |
| Weight (kg) | 87.0 ± 12.6 | 82.3 ± 13.1 | 82.6 ± 9.0 | 0.581 |
| VO2max (ml/kg/min) | 45.8 ± 5.2 | 46.3 ± 5.3 | 45.2 ± 5.7 | 0.896 |
| Protein (g/day)* | 117.9 ± 55.8 | 103.7 ± 38.3 | 102.8 ± 38.4 | 0.697 |
| Protein (g/day/kg BM)* | 1.4 ± 0.6 | 1.3 ± 0.6 | 1.3 ± 0.5 | 0.905 |
| Energy (MJ/day)* | 10.8 ± 5.6 | 8.3 ± 2.1 | 10.0 ± 2.7 | 0.353 |
*Calculated from 24 hr diet diaries recorded one week prior to familiarisation.
Table 2.
Nutritional content of milk protein concentrate (DP), placebo (PLA) and collagen hydrolysate (CH) supplements.
Table 2.
Nutritional content of milk protein concentrate (DP), placebo (PLA) and collagen hydrolysate (CH) supplements.
| Variable | DP | PLA | CH |
|---|---|---|---|
| Serving size (g)Energy (kJ) | 35.8 1000 |
53.2 1000 |
26.9 1000 |
| Protein (g) | 25.0 | 0.0 | 25.0 |
| CHO (g) | 32.9 | 58.8 | 33.8 |
| Fat (g) | 0.42 | 0.0 | 0.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



