
Submitted:
06 December 2024
Posted:
06 December 2024
You are already at the latest version
Abstract
Background: The relationship between hemoglobin and serum iron levels and mortality risk in patients with coronary artery disease (CAD) is not well understood.
Methods: We analyzed data from 3,224 patients with CAD using Cox proportional hazards regression models to assess the association of hemoglobin and serum iron levels with cardiovascular and all-cause mortality.
Results: Over a median follow-up period of 8.9 years, 636 patients died, including 403 from cardiovascular causes. Higher hemoglobin and serum iron levels were linked to a reduced risk of cardiovascular and all-cause mortality. Patients in the highest quartiles of hemoglobin and serum iron levels had multivariable-adjusted hazard ratios (HRs) of 0.62 (95% CI, 0.46–0.85) and 0.51 (95% CI, 0.37–0.69) for cardiovascular mortality, and 0.64 (95% CI, 0.50–0.83) and 0.67 (95% CI, 0.53–0.85) for all-cause mortality, compared to those in the lowest quartile. A one-standard deviation increase in hemoglobin and serum iron levels corresponded to a 19% and 24% reduction in cardiovascular mortality risk and a 19% reduction in all-cause mortality risk for both factors. Restricted cubic spline analysis revealed L-shaped and U-shaped associations between hemoglobin and serum iron levels and cardiovascular and all-cause mortality, respectively. These associations were consistent across various age groups, sex, and CAD types.
Conclusions: Hemoglobin and serum iron levels are significantly associated with lower risks of cardiovascular and all-cause mortality in patients with CAD. Further research is needed to evaluate the effects of iron supplementation in these patients.
Keywords:
coronary artery disease
; iron
; hemoglobin
; mortality
; prospective cohort study
Introduction
Iron is a vital trace element found predominantly in hemoglobin and is essential for oxygen transport in red blood cells. Maintaining adequate iron levels is crucial for preventing anemia, which can result from insufficient dietary intake or inflammation that impairs iron absorption [1]. Conversely, iron overload due to abnormal erythropoiesis or genetic disruptions in iron homeostasis can increase the risk of organ damage and infections, significantly affecting liver and heart function [2].
While the role of iron in red blood cell formation is well-established, its involvement in other aspects of blood cell biology and broader metabolic processes is still emerging. Beyond erythropoiesis, iron plays key roles in oxygen and lipid metabolism, protein synthesis, and DNA replication [1]. Serum iron levels, along with transferrin, total iron-binding capacity (TIBC), and transferrin saturation, provide insights into an individual’s iron status, whereas ferritin levels primarily indicate iron stores [3].
The "iron hypothesis," introduced by Sullivan in the early 1980s, suggested that elevated body iron levels might increase the risk of coronary artery disease (CAD), based on the observation of reduced CAD prevalence in populations with lower iron stores [4]. However, subsequent research on the relationship between iron status and CAD mortality has yielded inconclusive results. Some studies, such as those by Corti et al. [5] suggest that higher serum iron levels may have a protective effect against mortality. In contrast, others like Grammer et al. [6] have found that low hemoglobin and iron depletion are associated with an increased risk of CAD. Iron deficiency has been linked to adverse cardiovascular outcomes. For example, Parikh et al. [7] found an association between low hemoglobin levels and cardiovascular mortality in heart failure patients. Conversely, Bagheri et al. [8] reported high serum iron levels in patients with severe CAD, underscoring the complexity of iron's impact on cardiovascular health. Further investigations by Salonen et al. [9] and Magnusson et al. [10] examined iron overload and its correlation with CAD, yielding mixed conclusions about the roles of TIBC and ferritin in CAD. Despite numerous studies, including meta-analyses [11], the definitive association between iron parameters and CAD risk remains unclear, highlighting a significant gap in current understanding.
Despite these conflicting findings, iron homeostasis is recognized as a critical determinant of heart function, with both deficiency and overload linked to CAD and heart failure [12,13]. The potential toxicity of iron in CAD patients remains contentious, with hypotheses suggesting that oxidative stress, catalytic oxidation of low density lipoprotein particles, and excessive reactive oxygen species production may contribute to vessel wall damage and atherosclerosis [1,14,15].
Studies investigating the association of iron status markers with CAD risk have been limited by conflicting results and the complexity of iron metabolism. A single marker may provide inadequate or misleading information. Therefore, this study aims to explore the association between hemoglobin, serum iron, transferrin, TIBC, transferrin saturation, ferritin, and mortality risk among CAD patients. This paper will examine how variations in these iron-related parameters influence mortality rates among patients diagnosed with CAD, contributing valuable insights into managing iron levels in this patient population.
Methods
Study Population
The Guangdong Coronary Artery Disease Cohort (GCADC) is a prospective study of individuals aged 40 to 85 years from Guangdong province. The detailed cohort design and methodology have been previously published [16]. We initially recruited 1,977 patients diagnosed with CAD from three hospitals between 2008 and 2011 using standardized selection, inclusion, and diagnostic criteria. In 2014, we expanded the cohort by identifying an additional 1,622 CAD patients from hospital electronic medical records who were not previously included, bringing the total number of recruited CAD patients in the GCADC to 3,599. All patients were diagnosed with CAD according to the International Classification of Diseases, 10th revision (codes I20‒I25). After excluding 375 subjects with missing data, we included 3,224 CAD subjects in the primary analysis, focusing on serum iron and hemoglobin levels. Supplementary subgroup analyses were conducted with available data on serum ferritin, transferrin, and TIBC for 1,190, 1,473, and 1,470 patients, respectively. A flowchart of participant recruitment in the GCADC is summarized in Figure 1. Written informed consent was obtained from the initial 1,977 participants, and anonymous data from electronic medical records were used for the 2014 recruits. The research protocol was approved by the ethics committee of Sun Yat-Sen University, and all clinical investigations followed the principles of the Helsinki Declaration.
Clinical Data Collection and Biological Measurements
Demographic information, smoking and alcohol consumption habits, medical histories, and additional risk factors were collected through a standardized questionnaire administered during face-to-face interviews or extracted from electronic hospitalization records. Trained personnel measured participants' heights, weights, and blood pressures according to established protocols. After an overnight fast of at least 12 hours post-admission, venous blood samples were collected and stored at -80°C. Biochemical variables, including serum iron, hemoglobin, transferrin, TIBC, triglycerides (TG), total cholesterol (TC), Low-density lipoprotein cholesterol (LDL-C), High-density lipoprotein cholesterol (HDL-C), fasting plasma glucose (FPG), and creatinine levels, were measured using a Hitachi 7600-020 Automatic Analyzer following clinical laboratory guidelines. Plasma ferritin levels were measured via electrochemiluminescence immunoassay using the Architect i4000 system. C-reactive protein (CRP) was measured using flow cytometry. Estimated glomerular filtration rates (eGFR) were calculated to assess renal function and were categorized as <60 mL/min per 1.73 m2 or ≥60 mL/min per 1.73 m2.
Prospective Follow-Up
The primary outcomes were cardiovascular and all-cause mortality. Follow-up data were collected from hospital records, telephone conversations with patients or their family members, and the death registration system at the Guangdong Provincial Centers for Disease Control and Prevention. The follow-up period extended from the date of blood sample collection to the date of death or until November 30, 2019.
Statistical Analyses
Continuous variables with normal distributions are presented as means and standard deviations, while non-normally distributed variables are presented as medians with 25th and 75th percentiles. Categorical data are represented as numbers and percentages. Analysis of variance was used for continuous normally distributed data, and log-transformation was applied to non-normally distributed continuous data prior to analysis. Categorical variables were analyzed using the chi-square test. Serum iron and hemoglobin were analyzed as continuous variables and categorized into quartiles by sex. Spearman’s correlation and partial correlation coefficients were used to analyze relationships between serum iron, hemoglobin, and cardiovascular risk factors. Cox proportional hazards models evaluated the associations between serum iron, hemoglobin, and the risks of cardiovascular and all-cause mortality, with adjustments for confounding factors. Models were adjusted sequentially for age, sex, alcohol consumption status, smoking status, body mass index (BMI), systolic blood pressure (SBP), diastolic blood pressure, FPG, non-HDL-C, TG, CAD duration, CAD type (acute and chronic), eGFR, CRP, use of anti-diabetic, anti-platelet, cholesterol-lowering and anti-hypertensive drugs, hemoglobin (except for serum iron) and serum iron (except for hemoglobin) levels. Subgroup analyses were conducted based on variables such as CAD type, sex, BMI (≥24 or <24), history of diabetes, and the use of lipid-lowering drugs. Statistical analyses were performed using IBM® SPSS® software, version 22.0, with a two-tailed P-value <0.05 considered statistically significant.
Results
Baseline Characteristics
The cohort consisted of 3,224 patients (63.6% male) diagnosed with CAD, with a median follow-up duration of 8.9 years. Table 1 summarizes the baseline characteristics. Men had higher levels of serum iron, hemoglobin, and CRP, as well as higher rates of smoking, alcohol use, and acute coronary syndrome compared to women. Women had higher mean ages, SBP, TC, LDL-C, HDL-C, TG, a longer history of CAD, and a higher prevalence of comorbidities such as reduced eGFR (< 60 mL/min/1.73 m²), along with more frequent use of antihypertensive and antidiabetic medications.
Serum iron levels were positively correlated with hemoglobin, BMI, SBP, TC, LDL-C, HDL-C, and TG levels (all P < 0.05) and negatively correlated with sex, age, CRP, and FPG (all P < 0.05). These correlations remained after adjusting for age, sex, and BMI, except for TG. Hemoglobin levels also positively correlated with BMI, TC, LDL-C, and TG, and inversely with sex, age, CRP, and FPG (all P < 0.05), with stronger correlations after adjustment (Supplemental Table 1).
Hemoglobin Concentrations and Mortality Risks
During the follow-up period, 636 all-cause deaths and 403 cardiovascular deaths were recorded. Multivariable adjustment (model 3) revealed hazard ratios (HRs) for cardiovascular mortality of 0.64 (95% confidence intervals [CI], 0.50–0.83), 0.58 (95% CI, 0.44–0.77), and 0.62 (95% CI, 0.46–0.85) for the second, third, and fourth quartiles of hemoglobin levels, respectively. Similarly, for all-cause mortality, HRs were 0.64 (95% CI, 0.52–0.79), 0.66 (95% CI, 0.53–0.82), and 0.64 (95% CI, 0.50–0.83) for the second, third, and fourth quartiles, respectively (Table 2). For each one-standard deviation (SD) increase in hemoglobin concentrations, the HRs for cardiovascular and all-cause mortality risks were 0.81 (95% CI, 0.73–0.90) and 0.81 (95% CI, 0.74–0.88), respectively. Restricted cubic splines in Cox models showed that low hemoglobin levels (< 130 g/L) were significantly associated with increased mortality risk (Figure 1). These results indicate that higher hemoglobin levels are associated with reduced risks of cardiovascular and all-cause mortality among CAD patients.
Multivariable subgroup analyses, stratified by age, type of CAD, sex, BMI, and history of diabetes, demonstrated consistent associations between hemoglobin levels and both cardiovascular and all-cause mortality. However, a significant interaction between hemoglobin levels and CAD type was found for all-cause mortality, as well as between hemoglobin levels and a history of diabetes for both cardiovascular and all-cause mortality. No statistically significant interaction was found between hemoglobin levels and other variables (Supplementary Table 2).
Serum Iron Concentrations and Mortality Risks
Following multivariable adjustment in model 3, the HRs for cardiovascular mortality across the four quartiles of serum iron levels were 1.00, 0.72 (95% CI, 0.56–0.92), 0.44 (95% CI, 0.33–0.59), and 0.51 (95% CI, 0.37–0.69). Similarly, the HRs for all-cause mortality were 1.00, 0.84 (95% CI, 0.69–1.03), 0.51 (95% CI, 0.40–0.64), and 0.67 (95% CI, 0.53–0.85) (Table 3). For each one-SD increase in serum iron levels, there was a 24% reduction in the risk of cardiovascular mortality and a 19% reduction in the risk of all-cause mortality (all P < 0.05) (Table 3). Notably, low serum iron levels were associated with increased mortality risks, as indicated by the U-shaped curves observed in the Cox models (Figure 2). Separate analyses demonstrated that high iron levels had an independent protective effect on mortality risk, regardless of hemoglobin levels (Supplementary Figure S1).
Subgroup analyses, stratified by age, CAD type, sex, BMI, and history of diabetes, confirmed consistent associations between serum iron levels and mortality risks, with the exception of an interaction with diabetes history affecting cardiovascular mortality risk (Supplementary Table S3). Specifically, in CAD patients with diabetes, each one-SD increase in serum iron levels corresponded to a 37% reduction in cardiovascular mortality risk and a 29% reduction in all-cause mortality risk (Supplementary Table 3).
Serum Ferritin and Mortality Risks
After multivariable adjustments in model 3, each one-SD increase in plasma ferritin levels was associated with a 25% increase in cardiovascular mortality risk and a 21% increase in all-cause mortality risk (all P < 0.05), as presented in Supplementary Table S4. HRs for individuals in the highest versus lowest quartile of serum ferritin levels were 1.55 (95% CI, 1.04–2.31) for cardiovascular mortality and 1.45 (95% CI, 1.05–2.01) for all-cause mortality, respectively. Restricted cubic splines in Cox models also showed that higher plasma ferritin levels were associated with higher mortality risk (Supplementary Figures S2 and S3).
Serum Transferrin and Mortality Risks
Multivariable adjustments revealed U-shaped associations between serum transferrin levels and both cardiovascular and all-cause mortality among CAD patients, as illustrated in Supplementary Figures S2 and S3. The third quartile of serum transferrin levels exhibited the lowest HRs for cardiovascular mortality (HR: 0.51; 95% CI: 0.30–0.86) and all-cause mortality (HR: 0.66; 95% CI: 0.44–0.98) compared to the first quartile, as documented in Supplementary Table S5. These findings suggest an optimal range of transferrin levels that may confer protective effects against mortality in this patient population.
TIBC and Mortality Risks
The restricted cubic splines in Cox models, after multivariable adjustment, demonstrated U-shaped associations between TIBC levels and both cardiovascular and all-cause mortality among CAD patients, as depicted in Supplementary Figures S2 and S3. The third quartile of TIBC levels showed the lowest hazard ratios for cardiovascular mortality (HR: 0.59; 95% CI: 0.35–0.99) and all-cause mortality (HR: 0.66; 95% CI: 0.45–0.99) compared to the first quartile, as noted in Supplementary Table S6. This suggests an optimal range of TIBC that may offer protection against mortality in CAD patients.
Transferrin saturation and Mortality Risks
Each one-SD increase in transferrin saturation was associated with a 17% reduction in cardiovascular mortality risk and a 21% reduction in all-cause mortality risk in model 3 (all P < 0.05), as detailed in Supplementary Table S7. This suggests that an optimal range of transferrin saturation may provide protective effects against mortality risks in CAD patients. However, the U-shaped curve observed implies that excessively high or low transferrin saturation levels could be detrimental, highlighting the importance of maintaining iron levels within a moderate range (30–40%), as shown in Supplementary Figures S2 and S3.
Discussion
Our study indicates that among Chinese patients with CAD, higher levels of hemoglobin and serum iron are associated with significantly lower risks of cardiovascular and all-cause mortality. The observed U-shaped associations suggest that both iron deficiency and overload can negatively impact cardiovascular health. Additionally, we found that moderate transferrin saturation (30–40%) was associated with the lowest risk of mortality, with deviations from this range linked to higher mortality. In contrast, high plasma ferritin levels were associated with increased risks of cardiovascular and all-cause mortality among CAD patients after adjusting for other biomarkers associated with cardiovascular. Hence, iron status markers may serve as independent predictors of mortality risk among patients with CAD.
Previous epidemiological studies investigating the association of hemoglobin and CAD have yielded conflicting results regarding associations with CVD [6,17] and mortality [18,19,20]. The UK Biobank study observed a J-shaped association between hemoglobin levels and CAD risk among European adults, where both extremely low and high hemoglobin levels were detrimental. Additionally, Mendelian randomization showed a linear positive correlation, indicating an 8% increase in CAD risk per standard deviation increase in genetically predicted hemoglobin levels [17]. The Ludwigshafen Risk and Cardiovascular Health Study showed that low hemoglobin levels were independently associated with CAD [6], but had only a marginal association with cardiovascular and total mortality in patients with stable CAD [20]. Low or high hemoglobin concentrations were associated with elevated cardiovascular and all-cause mortality [19], emphasizing the importance of maintaining hemoglobin levels within the normal range. However, a large cohort study of 39,922 patients with acute coronary syndrome found a highly statistically significant and independent association between low hemoglobin levels and adverse cardiovascular outcomes [18]. This is consistent with our findings that low hemoglobin is an independent predictor of cardiovascular and all-cause mortality in CAD patients.
In addition to hemoglobin concentrations, the present study also evaluated the associations of iron status biomarkers with mortality. Our findings support the beneficial effects of higher serum iron and hemoglobin levels on reducing mortality risks in CAD patients. Mendelian randomization analysis suggests a protective effect of higher iron status against CAD [21], specifically indicating that increased levels of serum iron, transferrin saturation, and ferritin are associated with a reduced risk of CAD. Conversely, higher levels of transferrin, which indicate lower iron status, appeared to increase CAD risk [21]. Similarly, Corti et al. [5] found that higher serum iron levels were linked to lower all-cause and cardiovascular mortality in older adults, aligning with our findings on the risks associated with iron levels. These observations are supported by Jankowska et al. [22], who noted that optimal transferrin saturation levels could discriminate iron deficiency and protect against heart disease. Furthermore, the research by Grammer et al. [6] and Kiechl et al. [23] suggests that maintaining adequate iron status is crucial for preventing the progression of atherosclerosis and improving cardiovascular outcomes. Moreover, our observation of moderate transferrin saturation levels (30–40%) offering the lowest risk of mortality is supported by Guedes et al. [24], who found similar beneficial effects at a 40% transferrin saturation level for all-cause mortality and major adverse cardiovascular events. Recent studies, such as those by Zhang et al. [25], discuss the dual nature of iron in the cardiovascular system, emphasizing that both deficiency and overload can significantly impact heart health, particularly in heart failure patients. This aligns with our observations of a beneficial range for transferrin saturation and the detrimental effects of iron overload indicated by high plasma ferritin levels [25]. Moreover, research by Lupu et al. [26] explores the therapeutic implications of iron modulation in cardiovascular disease, suggesting that controlled iron supplementation could offer protective benefits in chronic cardiovascular conditions, thus supporting our findings of reduced mortality with higher serum iron and hemoglobin levels [26]. However, these findings contrast with the results of a meta-analysis that indicated no significant association between serum iron, TIBC, serum ferritin, and CAD, but found a significant negative association between transferrin saturation and CAD [27]. The meta-analysis compared the top and bottom tertiles of body iron status, which may have masked the different effects of mild iron deficiency and mild iron overload on CAD risk [27].
The protective role of moderate transferrin saturation observed in our study may be related to its balance in making iron available for erythropoiesis and other cellular functions without reaching toxic levels that catalyze the production of reactive oxygen species which can exacerbate oxidative stress, leading to endothelial dysfunction, a critical factor in the pathogenesis of atherosclerosis [23,28]. By avoiding both iron deficiency and overload, moderate transferrin saturation might optimize cellular function and minimize oxidative stress.
Furthermore, the relationship between higher ferritin levels and increased mortality could be explained by ferritin’s role as an acute-phase reactant. Elevated ferritin levels might not only reflect increased iron stores but also systemic inflammation, which is a known risk factor for atherosclerosis and subsequent cardiovascular events [29,30]. This inflammation can lead to increased vascular instability and plaque vulnerability, contributing to higher mortality rates.
The discrepancies observed could stem from methodological differences in measuring and defining iron status across studies, variations in population characteristics like age, sex, and baseline health conditions, and the interaction of iron with other risk factors such as inflammation, diabetes, and lipid profiles. These factors necessitate a cautious interpretation of the relationship between iron status and cardiovascular health, as the influence of iron may differ substantially based on individual and demographic factors.
The field of cardiovascular research presents varied findings regarding the impact of iron status on heart disease, illustrating the complexity of iron metabolism and its interaction with cardiovascular health. Some studies suggest a role for iron in promoting atherosclerosis, where elevated iron stores may contribute to the formation of atherosclerotic plaques [23,31]. Conversely, Tuomainen et al. [15] indicated a potential oxidative role of iron in cardiovascular disease, which could explain the increased cardiovascular risk with higher iron levels. Further, studies found no significant relationship between serum ferritin and cardiovascular events, challenging the hypothesis that iron overload heightens cardiovascular risk [32,33]. The importance of managing iron metabolism to prevent dysregulation that can lead to severe cardiovascular conditions, which may arise from both iron deficiency and overload [34]. More recent studies found no conclusive evidence linking iron status with CAD [11,35], suggesting that factors like sex, population genetics, dietary influences, or methodological differences across studies may play roles in these varied outcomes.
Iron metabolism plays a complex role in cardiovascular health, influencing processes ranging from oxygen transport and mitochondrial function to inflammation and oxidative stress [36,37]. Moreover, the U-shaped curves observed for iron and transferrin saturation suggest that both deficiency and excess of iron could be harmful, emphasizing the need for a delicate balance in iron homeostasis [4,38]. This balance is crucial, as iron overload can lead to toxic effects, including the promotion of lipid peroxidation and foam cell formation, both key processes in atherogenesis [31,39]. In summary, the associations between iron metabolism markers and cardiovascular outcomes likely involve a complex interplay of metabolic, oxidative, and inflammatory pathways, each contributing to the overall cardiovascular risk profile in individuals with CAD. The interplay between iron metabolism and cardiovascular health is intricate and multifaceted. Maintaining appropriate iron levels within a specific therapeutic window may be key to optimizing treatment strategies for CAD, as both iron deficiency and overload pose significant risks. Future research should continue to explore these dynamics, particularly in diverse populations and under varying health conditions to better understand and exploit iron's potential in cardiovascular disease management.
A significant strength of our study is the comprehensive evaluation of multiple iron markers and their association with mortality in a large cohort of patients with CAD. Our analysis of the independent effects of hemoglobin, serum iron, transferrin, transferrin saturation, TIBC, and ferritin on mortality provides valuable insights into the complex interactions between iron metabolism and cardiovascular health. Furthermore, utilizing a well-defined cohort with long-term follow-up enhances the reliability of our findings. However, our study does have several limitations. The observational nature of our research precludes drawing causal inferences between iron status and mortality. Additionally, our cohort was hospital-based, potentially limiting the generalizability of our findings to the broader population. The absence of data on iron supplementation and dietary iron intake could also have influenced our results. Another potential limitation is the influence of confounding factors such as inflammation and chronic disease states, which can affect ferritin levels independently of iron status. Addressing these confounding factors in future research could help clarify the relationships between iron parameters and cardiovascular outcomes.
Conclusions
Our study highlights the significant impact of hemoglobin, serum iron, transferrin, transferrin saturation, TIBC, and ferritin on mortality risks in patients with CAD. We found that optimal levels of serum iron and hemoglobin are associated with reduced mortality, whereas high ferritin levels correlate with increased mortality risk. These findings underscore the importance of balanced iron management in cardiovascular health.
Author Contributions
Conceptualization, Q.L. and W.L.; Methodology, Q.C.; Validation, Q.L., Q.C. and W.L.; Formal Analysis, Z.P. and Y.Z.; Investigation, X.W., D.L., T.Y., Z.P., Q.L., Q.C., and Y.Z.; Resources, W.L.; Data Curation, Q.L., Q.C. and W.L.; Writing – Original Draft Preparation, Q.L.; Writing – Review & Editing, Q.C. and W.L.; Visualization, Q.L. and W.L.; Supervision, W.L.; Project Administration, W.L.; Funding Acquisition, Q.C. and W.L.
Funding
This work was supported by the National Natural Science Foundation of China (grant No. U22A20360 and No. 82204012) and Guangzhou Science and Technology Plan Project (grant No. 202201011146).
Conflicts of Interest
The authors declare that there was no conflict of interest regarding the publication of this paper.
Abbreviations
| BMI | Body mass index |
| CAD | Coronary artery disease |
| CVD | Cardiovascular disease |
| CRP | C-reactive protein |
| eGFR | Estimated glomerular filtration rate |
| FPG | Fasting plasma glucose |
| HDL-C | High-density lipoprotein cholesterol |
| HRs | Hazard ratios |
| LDL-C | Low-density lipoprotein cholesterol |
| SBP | Systolic blood pressure |
| SD | standard deviation |
| TC | Total cholesterol |
| TG | Total triglycerides |
| TIBC | Total iron-binding capacity |
References
- Kobayashi, M.; Suhara, T.; Baba, Y.; Kawasaki, N.K.; Higa, J.K.; Matsui, T. Pathological Roles of Iron in Cardiovascular Disease. Curr. Drug Targets 2018, 19, 1068–1076. [CrossRef]
- Bi, Y.; Ajoolabady, A.; Demillard, L.J.; Yu, W.; Hilaire, M.L.; Zhang, Y.; Ren, J. Dysregulation of iron metabolism in cardiovascular diseases: From iron deficiency to iron overload. Biochem. Pharmacol. 2021, 190, 114661. [CrossRef]
- Semenova, Y.; Bjørklund, G.; Butnariu, M.; Peana, M. Iron-related Biomarkers in the Diagnosis and Management of Iron Disorders. Curr. Med. Chem. 2024. [CrossRef]
- Sullivan, J.L. Iron and the sex difference in heart disease risk. Lancet 1981, 1, 1293–1294. [CrossRef]
- Corti, M.-C.; Guralnik, J.M.; Salive, M.E.; Ferrucci, L.; Pahor, M.; Wallace, R.B.; Hennekens, C.H. Serum Iron Level, Coronary Artery Disease, and All-Cause Mortality in Older Men and Women. The American Journal of Cardiology 1997, 79, 120–127. [CrossRef]
- Grammer, T.B.; Kleber, M.E.; Silbernagel, G.; Pilz, S.; Scharnagl, H.; Tomaschitz, A.; König, W.; März, W. Hemoglobin, iron metabolism and angiographic coronary artery disease (The Ludwigshafen Risk and Cardiovascular Health Study). Atherosclerosis 2014, 236, 292–300. [CrossRef]
- Parikh, A.; Natarajan, S.; Lipsitz, S.R.; Katz, S.D. Iron deficiency in community-dwelling US adults with self-reported heart failure in the National Health and Nutrition Examination Survey III: prevalence and associations with anemia and inflammation. Circ. Heart Fail. 2011, 4, 599–606. [CrossRef]
- Bagheri, B.; Shokrzadeh, M.; Mokhberi, V.; Azizi, S.; Khalilian, A.; Akbari, N.; Habibi, V.; Yousefnejad, K.; Tabiban, S.; Nabati, M. Association between Serum Iron and the Severity of Coronary Artery Disease. Int. Cardiovasc. Res. J. 2013, 7, 95–98.
- Salonen, J.T.; Nyyssönen, K.; Korpela, H.; Tuomilehto, J.; Seppänen, R.; Salonen, R. High stored iron levels are associated with excess risk of myocardial infarction in eastern Finnish men. Circulation 1992, 86, 803–811. [CrossRef]
- Magnusson, M.K.; Sigfusson, N.; Sigvaldason, H.; Johannesson, G.M.; Magnusson, S.; Thorgeirsson, G. Low iron-binding capacity as a risk factor for myocardial infarction. Circulation 1994, 89, 102–108. [CrossRef]
- Danesh, J.; Appleby, P. Coronary heart disease and iron status: meta-analyses of prospective studies. Circulation 1999, 99, 852–854. [CrossRef]
- Cleland, J.G.F.; Zhang, J.; Pellicori, P.; Dicken, B.; Dierckx, R.; Shoaib, A.; Wong, K.; Rigby, A.; Goode, K.; Clark, A.L. Prevalence and Outcomes of Anemia and Hematinic Deficiencies in Patients With Chronic Heart Failure. JAMA Cardiol. 2016, 1, 539–547. [CrossRef]
- Paterek, A.; Mackiewicz, U.; Mączewski, M. Iron and the heart: A paradigm shift from systemic to cardiomyocyte abnormalities. J. Cell. Physiol. 2019, 234, 21613–21629. [CrossRef]
- Shah, S.V.; Alam, M.G. Role of iron in atherosclerosis. Am. J. Kidney Dis. 2003, 41, S80-3. [CrossRef]
- Tuomainen, T.-P.; Diczfalusy, U.; Kaikkonen, J.; Nyyssönen, K.; Salonen, J.T. Serum ferritin concentration is associated with plasma levels of cholesterol oxidation products in man. Free Radical Biology and Medicine 2003, 35, 922–928. [CrossRef]
- Chen, Q.; Li, Q.; Li, D.; Chen, X.; Liu, Z.; Hu, G.; Wang, J.; Ling, W. Association between liver fibrosis scores and the risk of mortality among patients with coronary artery disease. Atherosclerosis 2020, 299, 45–52. [CrossRef]
- Liu, Y.; Clarke, R.; Bennett, D.A.; Zong, G.; Gan, W. Iron Status and Risk of Heart Disease, Stroke, and Diabetes: A Mendelian Randomization Study in European Adults. J. Am. Heart Assoc. 2024, 13, e031732. [CrossRef]
- Sabatine, M.S.; Morrow, D.A.; Giugliano, R.P.; Burton, P.B.J.; Murphy, S.A.; McCabe, C.H.; Gibson, C.M.; Braunwald, E. Association of hemoglobin levels with clinical outcomes in acute coronary syndromes. Circulation 2005, 111, 2042–2049. [CrossRef]
- Lee, G.; Choi, S.; Kim, K.; Yun, J.-M.; Son, J.S.; Jeong, S.-M.; Kim, S.M.; Park, S.M. Association of Hemoglobin Concentration and Its Change With Cardiovascular and All-Cause Mortality. J. Am. Heart Assoc. 2018, 7. [CrossRef]
- Grammer, T.B.; Scharnagl, H.; Dressel, A.; Kleber, M.E.; Silbernagel, G.; Pilz, S.; Tomaschitz, A.; Koenig, W.; Mueller-Myhsok, B.; März, W.; et al. Iron Metabolism, Hepcidin, and Mortality (the Ludwigshafen Risk and Cardiovascular Health Study). Clin. Chem. 2019, 65, 849–861. [CrossRef]
- Gill, D.; Del Greco M, F.; Walker, A.P.; Srai, S.K.S.; Laffan, M.A.; Minelli, C. The Effect of Iron Status on Risk of Coronary Artery Disease: A Mendelian Randomization Study-Brief Report. Arterioscler. Thromb. Vasc. Biol. 2017, 37, 1788–1792. [CrossRef]
- Jankowska, E.A.; Wojtas, K.; Kasztura, M.; Mazur, G.; Butrym, A.; Kalicinska, E.; Rybinska, I.; Skiba, J.; Haehling, S. von; Doehner, W.; et al. Bone marrow iron depletion is common in patients with coronary artery disease. Int. J. Cardiol. 2015, 182, 517–522. [CrossRef]
- Kiechl, S.; Willeit, J.; Egger, G.; Poewe, W.; Oberhollenzer, F. Body iron stores and the risk of carotid atherosclerosis: prospective results from the Bruneck study. Circulation 1997, 96, 3300–3307. [CrossRef]
- Guedes, M.; Muenz, D.G.; Zee, J.; Bieber, B.; Stengel, B.; Massy, Z.A.; Mansencal, N.; Wong, M.M.Y.; Charytan, D.M.; Reichel, H.; et al. Serum Biomarkers of Iron Stores Are Associated with Increased Risk of All-Cause Mortality and Cardiovascular Events in Nondialysis CKD Patients, with or without Anemia. J. Am. Soc. Nephrol. 2021, 32, 2020–2030. [CrossRef]
- Zhang, H.; Zhabyeyev, P.; Wang, S.; Oudit, G.Y. Role of iron metabolism in heart failure: From iron deficiency to iron overload. Biochim. Biophys. Acta Mol. Basis Dis. 2019, 1865, 1925–1937. [CrossRef]
- Lupu, M.; Tudor, D.; Filip, A. Iron metabolism and cardiovascular disease: Basic to translational purviews and therapeutical approach. Rev. Port. Cardiol. 2022, 41, 1037–1046. [CrossRef]
- Das De, S.; Krishna, S.; Jethwa, A. Iron status and its association with coronary heart disease: systematic review and meta-analysis of prospective studies. Atherosclerosis 2015, 238, 296–303. [CrossRef]
- Duffy, S.J.; Biegelsen, E.S.; Holbrook, M.; Russell, J.D.; Gokce, N.; Keaney, J.F.; Vita, J.A. Iron chelation improves endothelial function in patients with coronary artery disease. Circulation 2001, 103, 2799–2804. [CrossRef]
- Gillum, R.F.; Sempos, C.T.; Makuc, D.M.; Looker, A.C.; Chien, C.Y.; Ingram, D.D. Serum transferrin saturation, stroke incidence, and mortality in women and men. The NHANES I Epidemiologic Followup Study. National Health and Nutrition Examination Survey. Am. J. Epidemiol. 1996, 144, 59–68. [CrossRef]
- Zheng, H.; Cable, R.; Spencer, B.; Votto, N.; Katz, S.D. Iron stores and vascular function in voluntary blood donors. Arterioscler. Thromb. Vasc. Biol. 2005, 25, 1577–1583. [CrossRef]
- You, S.-A.; Archacki, S.R.; Angheloiu, G.; Moravec, C.S.; Rao, S.; Kinter, M.; Topol, E.J.; Wang, Q. Proteomic approach to coronary atherosclerosis shows ferritin light chain as a significant marker: evidence consistent with iron hypothesis in atherosclerosis. Physiol. Genomics 2003, 13, 25–30. [CrossRef]
- Baer, D.M.; Tekawa, I.S.; Hurley, L.B. Iron stores are not associated with acute myocardial infarction. Circulation 1994, 89, 2915–2918. [CrossRef]
- Knuiman, M.W.; Divitini, M.L.; Olynyk, J.K.; Cullen, D.J.; Bartholomew, H.C. Serum ferritin and cardiovascular disease: a 17-year follow-up study in Busselton, Western Australia. Am. J. Epidemiol. 2003, 158, 144–149. [CrossRef]
- Sawicki, K.T.; Jesus, A. de; Ardehali, H. Iron Metabolism in Cardiovascular Disease: Physiology, Mechanisms, and Therapeutic Targets. Circ. Res. 2023, 132, 379–396. [CrossRef]
- Sun, Q.; Ma, J.; Rifai, N.; Franco, O.H.; Rexrode, K.M.; Hu, F.B. Excessive body iron stores are not associated with risk of coronary heart disease in women. J. Nutr. 2008, 138, 2436–2441. [CrossRef]
- Carpenter, J.-P.; He, T.; Kirk, P.; Roughton, M.; Anderson, L.J.; Noronha, S.V. de; Sheppard, M.N.; Porter, J.B.; Walker, J.M.; Wood, J.C.; et al. On T2* magnetic resonance and cardiac iron. Circulation 2011, 123, 1519–1528. [CrossRef]
- Haehling, S. von; Jankowska, E.A.; van Veldhuisen, D.J.; Ponikowski, P.; Anker, S.D. Iron deficiency and cardiovascular disease. Nat. Rev. Cardiol. 2015, 12, 659–669. [CrossRef]
- Ponikowska, B.; Suchocki, T.; Paleczny, B.; Olesinska, M.; Powierza, S.; Borodulin-Nadzieja, L.; Reczuch, K.; Haehling, S. von; Doehner, W.; Anker, S.D.; et al. Iron status and survival in diabetic patients with coronary artery disease. Diabetes Care 2013, 36, 4147–4156. [CrossRef]
- Syrovatka, P.; Kraml, P.; Potockova, J.; Fialova, L.; Vejrazka, M.; Crkovska, J.; Andel, M. Relationship between increased body iron stores, oxidative stress and insulin resistance in healthy men. Ann. Nutr. Metab. 2009, 54, 268–274. [CrossRef]
Figure 1.
Restricted cubic splines in Cox models of hemoglobin levels with cardiovascular (A) and all-cause (B) mortality risk. Adjustments were made for age, sex, drinking alcohol status, smoking status, body mass index, systolic blood pressure, diastolic blood pressure, fasting plasma glucose, non-high-density lipoprotein cholesterol, triglycerides, duration of coronary artery disease, estimated glomerular filtration rate, type of coronary artery disease (acute and chronic), C-reactive protein, use of anti-diabetic, anti-platelet, cholesterol-lowering and anti-hypertensive drugs, and serum iron levels.
Figure 1.
Restricted cubic splines in Cox models of hemoglobin levels with cardiovascular (A) and all-cause (B) mortality risk. Adjustments were made for age, sex, drinking alcohol status, smoking status, body mass index, systolic blood pressure, diastolic blood pressure, fasting plasma glucose, non-high-density lipoprotein cholesterol, triglycerides, duration of coronary artery disease, estimated glomerular filtration rate, type of coronary artery disease (acute and chronic), C-reactive protein, use of anti-diabetic, anti-platelet, cholesterol-lowering and anti-hypertensive drugs, and serum iron levels.
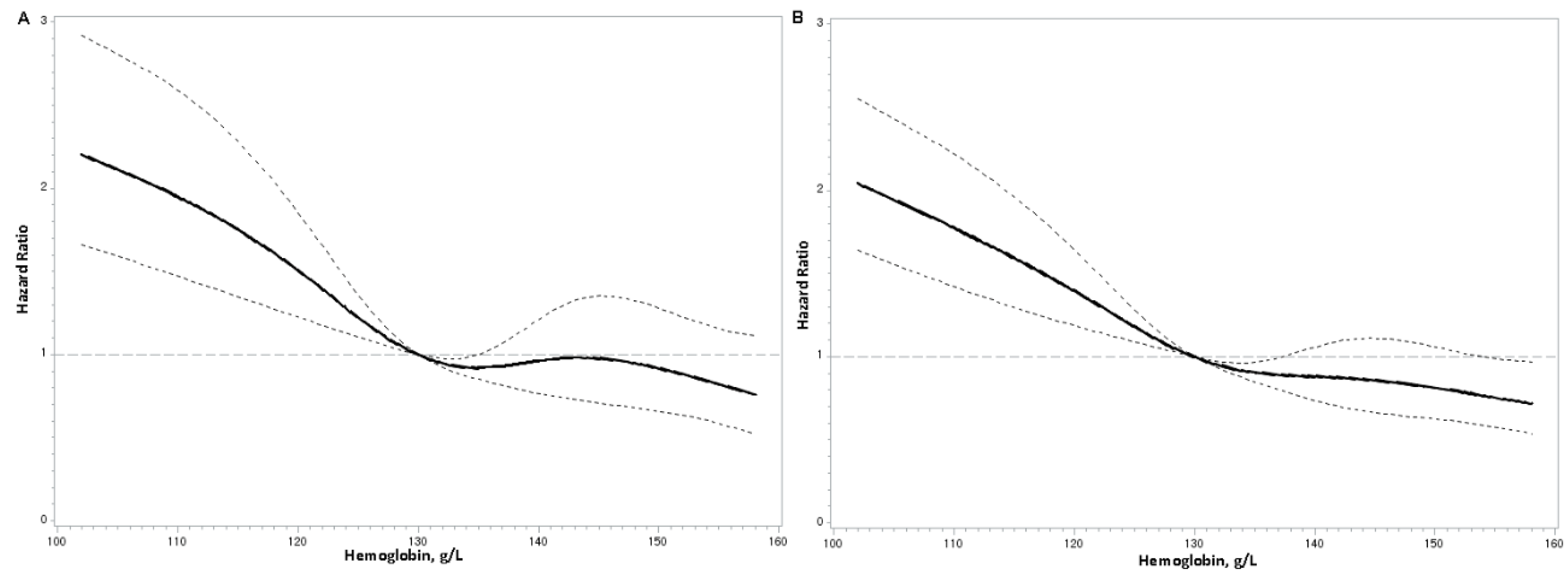
Figure 2.
Restricted cubic splines in Cox models of serum iron levels with cardiovascular (A) and all-cause (B) mortality risk. Adjustments were made for age, sex, drinking alcohol status, smoking status, body mass index, systolic blood pressure, diastolic blood pressure, fasting plasma glucose, non-high-density lipoprotein cholesterol, triglycerides, duration of coronary artery disease, estimated glomerular filtration rate, type of coronary artery disease (acute and chronic), C-reactive protein, use of anti-diabetic, anti-platelet, cholesterol-lowering and anti-hypertensive drugs, and hemoglobin levels.
Figure 2.
Restricted cubic splines in Cox models of serum iron levels with cardiovascular (A) and all-cause (B) mortality risk. Adjustments were made for age, sex, drinking alcohol status, smoking status, body mass index, systolic blood pressure, diastolic blood pressure, fasting plasma glucose, non-high-density lipoprotein cholesterol, triglycerides, duration of coronary artery disease, estimated glomerular filtration rate, type of coronary artery disease (acute and chronic), C-reactive protein, use of anti-diabetic, anti-platelet, cholesterol-lowering and anti-hypertensive drugs, and hemoglobin levels.
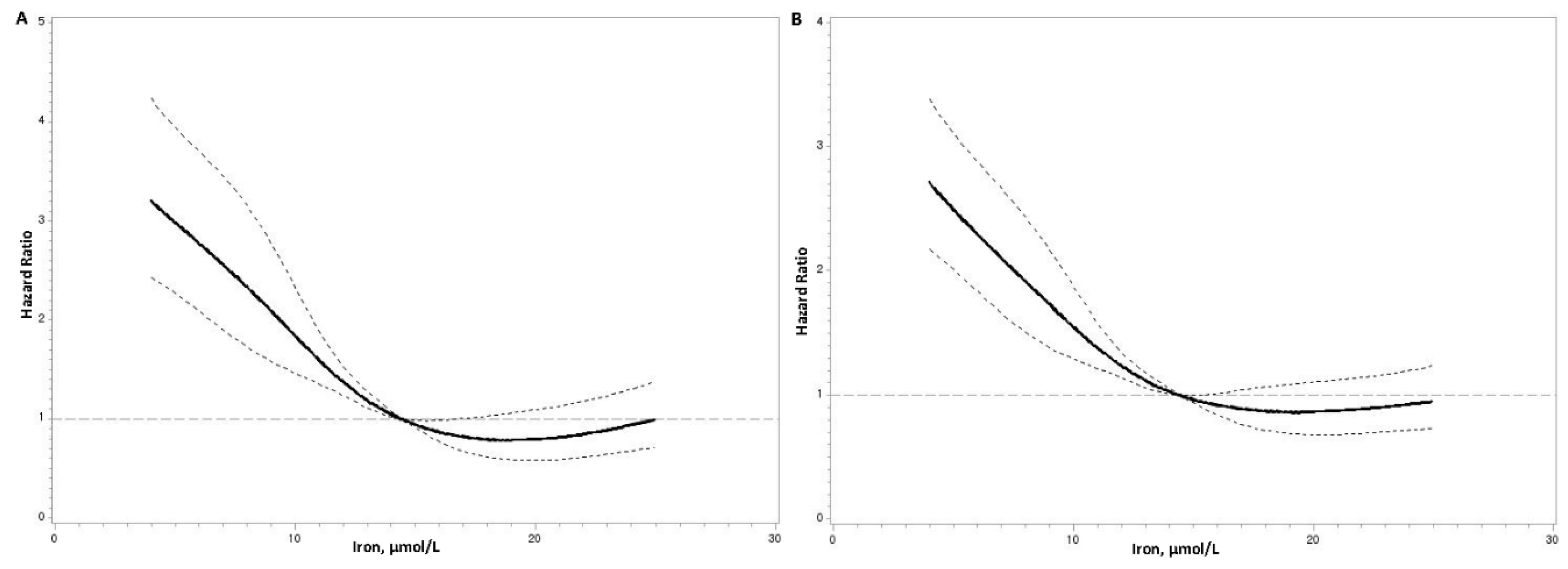

Table 1.
Baseline characteristics of subjects with coronary artery disease according to sex.
| Variables | Total (n=3224) |
Male (n=2052) |
Female (n=1172) |
P value |
|---|---|---|---|---|
| Serum Iron (μmol/L) | 13.1 (9.1–17.5) | 13.2 (9.2–18.2) | 12.9 (9.1–16.5) | 0.001 |
| Hemoglobin (g/L) | 133.0 (121.0–143.0) | 138.0 (127.0–147.0) | 125.0 (115.0–133.0) | <0.001 |
| Age, year | 64.2 (11.1) | 62.4 (11.6) | 67.3 (9.5) | <0.001 |
| Body mass index, kg/m2 | 24.0 (3.4) | 24.0 (3.2) | 24.0 (3.6) | 0.968 |
| Systolic blood pressure, mmHg | 135.4 (22.4) | 133.4 (22.4) | 138.7 (22.0) | <0.001 |
| Diastolic blood pressure, mmHg | 78.1 (12.7) | 78.3 (13.1) | 77.8 (12.0) | 0.301 |
| Fasting plasma glucose, mmol/L | 6.62 (2.84) | 6.55 (2.61) | 6.74 (3.20) | 0.060 |
| Total cholesterol, mmol/L | 4.80 (1.15) | 4.65 (1.12) | 5.05 (1.16) | <0.001 |
| Low-density lipoprotein cholesterol, mmol/L | 2.99 (0.98) | 2.93 (0.97) | 3.09 (1.00) | <0.001 |
| High-density lipoprotein cholesterol, mmol/L | 1.14 (0.31) | 1.08 (0.28) | 1.25 (0.33) | <0.001 |
| Triglycerides, mmol/L | 1.53 (1.09–2.17) | 1.51 (1.07–2.14) | 1.56 (1.12–2.21) | 0.036 |
| C-reactive protein*, mg/L | 3.11 (1.11–11.16) | 3.39 (1.11–13.28) | 2.70 (1.10–8.26) | <0.001 |
| Estimated glomerular filtration rate, ml/min per 1.73 m2, % | <0.001 | |||
| < 60 | 28.7 | 24.5 | 35.8 | |
| ≥ 60 | 71.3 | 75.5 | 64.2 | |
| Duration of coronary artery disease, year | ||||
| First diagnosed coronary artery disease (n = 2114) | - | - | - | - |
| History of coronary artery disease (n = 1110) | 3.00 (0.86–7.16) | 2.34 (0.73–6.34) | 4.00 (1.00–9.80) | <0.001 |
| Smoking status, % | <0.001 | |||
| Never | 60.8 | 41.2 | 95.2 | |
| Current | 29.1 | 43.9 | 3.2 | |
| Past | 10.1 | 15.0 | 1.6 | |
| Alcohol drinking status, % | <0.001 | |||
| Never | 83.9 | 75.3 | 98.7 | |
| Current | 11.7 | 17.8 | 1.1 | |
| Past | 4.4 | 6.8 | 0.2 | |
| Type of coronary artery disease, % | <0.001 | |||
| Acute coronary syndrome (n = 1823) | 56.5 | 61.5 | 47.9 | |
| Chronic coronary artery disease (n = 1401) | 43.5 | 38.5 | 52.1 | |
| History of diseases (Yes), % | ||||
| Hypertension | 76.2 | 74.5 | 79.4 | 0.002 |
| Dyslipidemia | 19.3 | 18.7 | 20.4 | 0.232 |
| Diabetes | 23.7 | 21.7 | 27.0 | 0.001 |
| Use of medication before admission (Yes), % | ||||
| Anti-hypertensive drugs | 48.6 | 44.2 | 57.2 | <0.001 |
| Cholesterol-lowering drugs | 12.3 | 12.5 | 11.8 | 0.668 |
| Anti-diabetic drugs | 16.7 | 14.7 | 20.5 | 0.002 |
| Anti-platelet drugs | 19.9 | 20.7 | 18.2 | 0.202 |
Data are presented as mean (standard deviation) for the continuous variables, median [25th, 75th] for non-normally distributed variables or percent for categorical variables. # Log transformed before analysis.
Table 2.
Hazard ratios of cardiovascular and all-cause mortality according to baseline hemoglobin levels.
Table 2.
Hazard ratios of cardiovascular and all-cause mortality according to baseline hemoglobin levels.
| Hemoglobin levels | |||||||
|---|---|---|---|---|---|---|---|
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | P value | Hazard Ratio per 1-SD Increment | P value | |
| Cardiovascular mortality | |||||||
| Model 1 | 1.00 | 0.61 (0.47–0.78) | 0.50 (0.38–0.66) | 0.51 (0.38–0.69) | <0.001 | 0.74 (0.68–0.82) | <0.001 |
| Model 2 | 1.00 | 0.61 (0.47–0.79) | 0.52 (0.39–0.69) | 0.53 (0.39–0.72) | <0.001 | 0.76 (0.68–0.84) | <0.001 |
| Model 3 | 1.00 | 0.64 (0.50–0.83) | 0.58 (0.44–0.77) | 0.62 (0.46–0.85) | <0.001 | 0.81 (0.73–0.90) | <0.001 |
| All–cause mortality | |||||||
| Model 1 | 1.00 | 0.59 (0.48–0.72) | 0.55 (0.45–0.69) | 0.51 (0.41–0.65) | <0.001 | 0.74 (0.68–0.79) | <0.001 |
| Model 2 | 1.00 | 0.61 (0.50–0.75) | 0.60 (0.48–0.75) | 0.56 (0.44–0.72) | <0.001 | 0.77 (0.71–0.83) | <0.001 |
| Model 3 | 1.00 | 0.64 (0.52–0.79) | 0.66 (0.53–0.82) | 0.64 (0.50–0.83) | <0.001 | 0.81 (0.74–0.88) | <0.001 |
Model 1 was adjusted for age, sex, drinking alcohol status, and smoking status. Model 2 was adjusted for model 1 covariates plus body mass index, systolic blood pressure, diastolic blood pressure, fasting plasma glucose, non-high-density lipoprotein cholesterol, triglycerides, duration of coronary artery disease, estimated glomerular filtration rate, type of coronary artery disease (acute and chronic), C-reactive protein, use of anti-diabetic, anti-platelet, cholesterol-lowering and anti-hypertensive drugs. Model 3 was adjusted for model 2 covariates plus serum iron levels.
Table 3.
Hazard ratios of cardiovascular and all-cause mortality according to baseline serum iron levels.
Table 3.
Hazard ratios of cardiovascular and all-cause mortality according to baseline serum iron levels.
| Serum iron levels | |||||||
|---|---|---|---|---|---|---|---|
| Quartile 1 | Quartile 2 | Quartile 3 | Quartile 4 | P value | Hazard Ratio per 1-SD Increment | P value | |
| Cardiovascularmortality | |||||||
| Model 1 | 1.00 | 0.63 (0.50–0.81) | 0.37 (0.27–0.49) | 0.40 (0.29–0.53) | <0.001 | 0.67 (0.60–0.75) | <0.001 |
| Model 2 | 1.00 | 0.68 (0.53–0.87) | 0.41 (0.30–0.55) | 0.46 (0.34–0.62) | <0.001 | 0.72 (0.64–0.81) | <0.001 |
| Model 3 | 1.00 | 0.72 (0.56–0.92) | 0.44 (0.33–0.59) | 0.51 (0.37–0.69) | <0.001 | 0.76 (0.67–0.85) | <0.001 |
| All–cause mortality | |||||||
| Model 1 | 1.00 | 0.74 (0.61–0.90) | 0.42 (0.33–0.53) | 0.51 (0.41–0.64) | <0.001 | 0.72 (0.65–0.78) | <0.001 |
| Model 2 | 1.00 | 0.79 (0.65–0.97) | 0.47 (0.37–0.59) | 0.59 (0.47–0.75) | <0.001 | 0.77 (0.70–0.84) | <0.001 |
| Model 3 | 1.00 | 0.84 (0.69–1.03) | 0.51 (0.40–0.64) | 0.67 (0.53–0.85) | <0.001 | 0.81 (0.74–0.89) | <0.001 |
Model 1 was adjusted for age, sex, drinking alcohol status, and smoking status. Model 2 was adjusted for model 1 covariates plus body mass index, systolic blood pressure, diastolic blood pressure, fasting plasma glucose, non-high-density lipoprotein cholesterol, triglycerides, duration of coronary artery disease, estimated glomerular filtration rate, type of coronary artery disease (acute and chronic), C-reactive protein, use of anti-diabetic, anti-platelet, cholesterol-lowering and anti-hypertensive drugs. Model 3 was adjusted for model 2 covariates plus hemoglobin levels.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



