
Submitted:
05 December 2024
Posted:
06 December 2024
You are already at the latest version
Abstract
Toxic metal exposure is a pervasive global health concern, with significant implications for human health. Toxic metals such as lead, mercury, arsenic, and cadmium are widely distributed in the environment due to natural processes and human activities. Industrial emissions, mining, smelting, and agricultural practices contribute to environmental contamination, while consumer products, food, water, and air serve as common exposure pathways for humans. Exposure to toxic metals can occur through inhalation, ingestion, and dermal contact. Inhalation is a significant route for metals like lead and cadmium, primarily through occupational settings and environmental pollution. Ingestion of contaminated food, water, and beverages is a primary route for mercury and arsenic exposure, while dermal contact with contaminated soil, water, or consumer products can also contribute to exposure. Toxic metals exert their adverse effects through various mechanisms, including oxidative stress, disruption of cellular function, and interference with enzymatic processes. These metals can enter cells and tissues, where they bind to biomolecules such as proteins and DNA, leading to cellular damage, inflammation, and apoptosis. The health effects of toxic metal exposure are diverse and can affect multiple organ systems. Neurological effects, including neurodevelopmental deficits in children and cognitive impairment in adults, are well-documented for metals such as lead and mercury. Cardiovascular effects, such as hypertension and increased risk of cardiovascular disease, are associated with cadmium exposure. Renal toxicity, manifested as kidney damage and renal dysfunction, is a common consequence of exposure to metals like cadmium and lead. Additionally, certain toxic metals, including arsenic and cadmium, are classified as carcinogens and have been linked to various cancers, including lung, bladder, and liver cancer. Prevention of toxic metal exposure requires a multi-faceted approach, including regulatory measures, environmental monitoring, and public education. Regulation of industrial emissions, implementation of pollution control measures, and promotion of safer alternatives are essential for reducing environmental contamination. Monitoring programs for environmental and human biomarkers of exposure are critical for assessing exposure levels and identifying at-risk populations. Efforts to mitigate these risks require collaborative action at the local, national, and global levels to implement effective preventive measures and safeguard public health. This comprehensive overview will provide valuable insights into the complex interplay between toxic metal exposure and human health, highlighting the importance of proactive measures to address this global health challenge.
Keywords:
Toxic Metal
; Exposure of toxic metals
; Public Health
; Health Effects
Introduction:
Toxic metal exposure represents a significant public health concern with far-reaching consequences for human health and well-being. [1] Metals such as lead, mercury, arsenic, cadmium, and others, once considered valuable commodities for industrial and technological purposes, are now recognized for their harmful effects on human health even at low levels of exposure. [2] The ubiquity of toxic metals in our environment stems from both natural processes and anthropogenic activities. Industrial operations, including mining, smelting, and manufacturing, contribute to the release of metals into the air, water, and soil, leading to environmental contamination. [3] For instance, lead, a pervasive environmental toxin, has historically been used in lead-based paints, gasoline additives, and plumbing materials, resulting in widespread contamination of soil and water sources. [4] Similarly, mercury emissions from coal-fired power plants and industrial processes contaminate aquatic ecosystems, leading to bioaccumulation in fish and seafood consumed by humans. Agricultural practices, such as the use of metal-containing pesticides and fertilizers, also contribute to environmental metal contamination, with metals leaching into soil and groundwater. Additionally, consumer products such as electronics, batteries, and cosmetics may contain toxic metals, posing a risk of exposure through direct contact or inhalation of airborne particles. [5]
Toxic metals can enter the human body through multiple routes, including inhalation, ingestion, and dermal contact. Inhalation represents a significant route of exposure for metals such as lead, cadmium, and mercury, particularly in occupational settings where workers may be exposed to metal-containing dust, fumes, or vapours. [6] Industrial processes, including welding, smelting, and soldering, can generate airborne metal particles that are easily inhaled, leading to systemic absorption and distribution within the body. Ingestion of contaminated food and water is another common route of exposure for certain metals, including arsenic and mercury. Arsenic contamination of groundwater, often resulting from natural geological sources or anthropogenic pollution, poses a significant risk to human health, particularly in regions reliant on groundwater for drinking and irrigation purposes. [7] Similarly, mercury bioaccumulates in fish and seafood, posing a risk of exposure to individuals consuming these contaminated foods. Dermal contact with contaminated soil, water, or consumer products represents a less common but nonetheless significant route of exposure to toxic metals. For example, individuals working in industries involving the handling of metal-containing materials may be at risk of dermal exposure, particularly if proper personal protective equipment is not utilized. Similarly, cosmetic products containing heavy metals such as lead or mercury may pose a risk of dermal absorption upon application to the skin. [8]
Toxic metals exert their adverse effects on human health through a variety of mechanisms, including oxidative stress, disruption of cellular function, and interference with enzymatic processes. These metals possess the ability to bind to cellular components such as proteins, lipids, and nucleic acids, leading to structural and functional alterations within cells. For instance, lead binds to sulfhydryl groups in proteins, disrupting enzymatic activity and cellular signaling pathways. Oxidative stress represents a common mechanism underlying the toxic effects of many metals, whereby metals generate reactive oxygen species (ROS) and free radicals, leading to oxidative damage to cellular macromolecules such as DNA, proteins, and lipids. [9] Additionally, certain metals, such as arsenic and cadmium, have been shown to induce epigenetic modifications, altering gene expression patterns and contributing to the development of various diseases. [10]
The health effects of toxic metal exposure are diverse and can manifest across multiple organ systems, ranging from neurological and cardiovascular disorders to renal dysfunction and carcinogenesis. [11] Neurological effects, including impaired cognitive function, developmental delays, and behavioral abnormalities, are well-documented consequences of lead and mercury exposure, particularly in children whose developing brains are more susceptible to the neurotoxic effects of these metals. [12] Cardiovascular effects, such as hypertension, atherosclerosis, and increased risk of cardiovascular disease, have been associated with chronic exposure to metals such as cadmium and lead. [13] Cadmium, in particular, has been implicated in the development of peripheral arterial disease and endothelial dysfunction, contributing to the pathogenesis of cardiovascular disorders. Renal toxicity represents another significant health concern associated with certain toxic metals, including cadmium and lead. [14] Chronic exposure to these metals can result in nephrotoxicity, characterized by tubular dysfunction, proteinuria, and ultimately, renal failure. Additionally, certain metals, such as arsenic and cadmium, have been classified as carcinogens by international agencies, with evidence linking them to various cancers, including lung, bladder, and liver cancer. [15] Toxic metal exposure poses a significant threat to human health, with adverse effects that extend across multiple organ systems. Understanding the sources, routes of exposure, mechanisms of toxicity, and health effects associated with toxic metals is essential for developing effective prevention and intervention strategies to mitigate the risks posed by these environmental contaminants. By addressing the root causes of metal contamination and implementing measures to reduce exposure, we can safeguard public health and promote a healthier environment for current and future generations. This review will provide a comprehensive overview of toxic metal exposure, exploring its sources, routes of exposure, mechanisms of toxicity, and associated health effects, while emphasizing the critical importance of addressing this global health challenge.
Common Toxic Metals and Their Sources:
Toxic metals are ubiquitous environmental contaminants with sources ranging from natural geological processes to anthropogenic activities. Understanding the sources of these metals is crucial for identifying potential exposure pathways and implementing effective mitigation strategies. Various sources of heavy metals include soil erosion, natural weathering of the earth's crust, mining, industrial effluents, urban runoff, sewage discharge, insect or disease control agents applied to crops, and many others. Some common toxic metals, including lead, mercury, arsenic, and cadmium, along with their primary sources of exposure are mentioned here: Figure 1
Lead: Lead is a highly toxic metal that has been used for centuries in various industrial applications, including lead-based paints, gasoline additives, plumbing materials, and batteries. Lead is a bright silvery metal, slightly bluish in a dry atmosphere. It begins to tarnish on contact with air, thereby forming a complex mixture of compounds, depending on the given conditions. Despite efforts to reduce lead exposure in recent decades, it remains a significant environmental and public health concern, particularly in urban areas with a legacy of lead contamination. [16] Lead toxicity from anthropogenic activities like industrial emissions contaminates the environment. Natural sources contribute to pollution too. Lead exposure damages the renal system, causing nephropathy and renal failure. It disrupts kidney function, leading to hypertension and impaired filtration. Long-term exposure exacerbates renal ailments, posing serious health risks. (Figure 2) Plants with increased in lead concentration fastens the production of reactive oxygen species (ROS), and lead to the cause of lipid membrane damage that ultimately results in damage of chlorophyll and photosynthetic processes and suppresses the overall growth of the plant [17]. Research also revealed that lead is capable of inhibiting the growth of tea plant by reducing biomass and debases the quality of tea by changing the quality of its components. [18] Contamination of lead in soil and dust from deteriorating lead-based paint and leaded gasoline residues continues to pose a risk of exposure, especially in older housing stock and industrial sites. Additionally, lead pipes and plumbing fixtures can leach lead into drinking water, contributing to lead exposure in certain communities. [19]
Mercury: The metallic mercury metal occurs naturally; it’s a shiny silver-white, odorless liquid and becomes colorless and odorless gas when it is heated. It is very toxic and exceedingly bio-accumulative. Presence of mercury adversely affects the marine environment and hence many studies are directed towards the distribution of mercury in water environment. Major sources of mercury pollution include anthropogenic activities such as agriculture, municipal wastewater discharges, mining, incineration, and discharges of industrial wastewater [20] Mercury is a potent neurotoxin that exists in various forms, including elemental mercury (found in thermometers and dental amalgams), inorganic mercury compounds (used in industrial processes), and organic mercury compounds (such as methylmercury, found in fish and seafood). [21] Coal-fired power plants are a major source of mercury emissions, releasing elemental mercury into the atmosphere, where it can be deposited into water bodies and undergo bioaccumulation in aquatic ecosystems. As a result, fish and seafood consumption represent a significant route of exposure to methylmercury, particularly for vulnerable populations such as pregnant women and young children. [22] (Figure 3)
Arsenic: Arsenic is one of the most toxic heavy metals causing disquiet from ecological and individual health standpoints. [23] Arsenic has a semi-metallic property, and it is prominently toxic and carcinogenic, and is extensively available in the form of oxides or sulfides or as a salt of iron, sodium, calcium, copper, etc. [24]. It is a naturally occurring metalloid found in soil, rocks, and minerals, with both geological and anthropogenic sources of contamination. Inorganic arsenic compounds can leach into groundwater from natural geological formations or be released into the environment through mining, smelting, and agricultural practices. [25] Arsenic contamination of drinking water is a major public health concern in many regions worldwide, particularly in areas with high levels of naturally occurring arsenic in groundwater. Additionally, arsenic-based pesticides and herbicides were historically used in agriculture, contributing to environmental contamination and human exposure. [26]
Cadmium: Cadmium is the seventh most toxic heavy metal that is primarily released into the environment through industrial processes such as mining, smelting, and manufacturing. It is a by-product of zinc production which humans or animals get exposed to at work or in the environment. [27] When this metal gets absorbed by humans, it gets accumulated inside the body throughout the life. Cadmium was first used in World War I as a substitute for tin and in paint industries as a pigment. It is widely used in the production of batteries, coatings of metal, pigments, and in plastics (toys, bottles etc), resulting in the release of cadmium-containing effluents and airborne emissions. Three-fourths of cadmium is used in alkaline batteries as an electrode component, and the remaining part is utilized in coatings, pigments and platings and as a plastic stabilizer. Plants take up these metals which get accumulated in them and concentrate along the food chain, ultimately reaching human body. [28] In America, more than 500,000 workers get exposed to toxic cadmium every year as per The Agency for Toxic Substances and Disease Registry Board [29]. Tobacco smoking is another significant source of cadmium exposure, with tobacco plants accumulating cadmium from soil contaminated with cadmium-containing fertilizers. As a result, smokers and individuals exposed to environmental tobacco smoke are at an increased risk of cadmium exposure and associated health effects. [30] Cadmium is predominantly found in most of the fruits and vegetables due to its high content of soil-to-plant transfer [31]. It is a highly toxic nonessential heavy metal that is well recognized for its adverse influence on the enzymatic systems of cells, oxidative stress and for inducing nutritional deficiency in plants. [32] (Figure 4)
Other Common Toxic Metals: In addition to lead, mercury, arsenic, and cadmium, several other metals have toxicological significance and can pose risks to human health. These include metals such as chromium, nickel, and aluminum, which are used in various industrial processes and consumer products. Chromium, for example, is widely used in stainless steel production and can contaminate soil and water sources near industrial sites. [33] Nickel is commonly used in alloys, batteries, and electronic devices, with potential exposure occurring through occupational settings and consumer products; it is strongly associated with high apoptosis rates, and causes pulmonary fibrosis. [34] Aluminum exposure can occur through food, water, and pharmaceuticals, with concerns regarding its neurotoxic effects and potential links to neurodegenerative diseases. [35] Common toxic metals pose significant risks to human health and the environment, with sources of exposure ranging from industrial emissions and mining activities to consumer products and agricultural practices. Identifying and mitigating sources of metal contamination is essential for reducing human exposure and preventing adverse health effects. [36] Heavy metals discharged by industries contaminate soil, bioaccumulate in the food chain, and harm living organisms. Bioremediation employs physical, chemical, and biological strategies to mitigate this. Physical methods include soil washing or electrokinetic treatment. Chemical methods involve using chelating agents to bind metals for removal. Biological methods utilize microorganisms or plants to metabolize or absorb contaminants. These approaches aid in reducing heavy metal concentrations, restoring ecosystem balance, and safeguarding human health. However, efficacy varies depending on metal type, soil characteristics, and environmental conditions, requiring careful implementation and monitoring for sustainable remediation. Public health interventions, regulatory measures, and pollution control strategies play a crucial role in minimizing metal exposure and safeguarding human health in communities worldwide. By addressing the root causes of metal contamination and promoting sustainable practices, we can mitigate the risks posed by toxic metals and create a safer and healthier environment for current and future generations.
Routes of Exposure to Toxic Metals:
Exposure to toxic metals occurs through various routes, each presenting unique risks to human health. Understanding these pathways is essential for assessing exposure levels, identifying vulnerable populations, and implementing effective preventive measures. This section provides an in-depth exploration of the routes of exposure to toxic metals, including inhalation, ingestion, and dermal contact, along with their associated health risks and mitigation strategies.
1-Inhalation Exposure: Human health is threatened by significant emissions of heavy metals toxicity into the urban environment due to various man made activities. Inhalation is a significant route of exposure to toxic metals, particularly in occupational settings where workers may encounter airborne contaminants during industrial processes such as mining, smelting, welding, and metal fabrication. Inhalable particles containing metals can be generated through mechanical processes, combustion, and thermal decomposition, leading to respiratory exposure and systemic absorption. Similarly, potential health risk of heavy metals in urban population is through ingestion of heavy metals on road dust of < 63-μm diameter, via incidental ingestion, dermal contact, and inhalation exposure routes by children and adults. [37]
A)-Health Risks by inhalation: Inhaled toxic metals can bypass the body's natural defense mechanisms and enter the bloodstream directly through the lungs, resulting in systemic distribution and potential toxicity to various organs. Chronic exposure to airborne metals such as lead, cadmium, and arsenic has been linked to respiratory disorders, cardiovascular diseases, neurological impairments, and cancer. Additionally, certain metals, such as nickel and chromium, are respiratory sensitizers, capable of inducing allergic reactions and respiratory conditions such as asthma and chronic obstructive pulmonary disease (COPD). [38].
b)-Mitigation Strategies to minimize inhalation: Effective control measures to minimize inhalation exposure include engineering controls such as ventilation systems, local exhaust ventilation, and enclosed processes to capture and remove airborne contaminants at the source. Personal protective equipment (PPE), including respiratory protection such as masks, respirators, and air-supplied helmets, should be provided to workers in high-risk environments. Occupational health and safety regulations, regular monitoring of airborne metal concentrations and employee training programs are essential for reducing the risks associated with inhalation exposure in the workplace. [39]
2- Health Risks from Ingestion Exposure: Ingested toxic metals can be absorbed through the gastrointestinal tract and distributed throughout the body, where they can accumulate in organs such as the liver, kidneys, and brain, leading to systemic toxicity. Chronic exposure to metals such as lead and cadmium has been associated with neurological impairments, developmental delays, renal dysfunction, cardiovascular diseases, and cancer. Additionally, prenatal exposure to certain metals, such as methylmercury and lead, can result in developmental abnormalities and long-term health effects in infants and children. [41]
A)- Mitigation Strategies: Preventive measures to reduce ingestion exposure include ensuring the safety and quality of food and drinking water through regulatory standards, monitoring programs, and pollution control measures. Public health interventions, such as education campaigns, dietary guidelines, and nutritional interventions, can help raise awareness about the risks of metal contamination in food and promote healthier dietary habits. Water treatment technologies, such as filtration, ion exchange, and reverse osmosis, can be employed to remove metals from drinking water sources and reduce exposure levels in communities at risk. [42]
3. Dermal Contact Exposure: Dermal contact represents another route of exposure to toxic metals, particularly through direct skin contact with contaminated soil, water, consumer products, and occupational materials. Metals such as lead, mercury, arsenic, and cadmium can adhere to the skin and be absorbed through the epidermal barrier, leading to systemic distribution and potential health effects.
A)- Health Risks: Dermal exposure to toxic metals can result in localized irritation, dermatitis, and allergic reactions, as well as systemic toxicity depending on the metal and exposure duration. Chronic exposure to metals such as arsenic and cadmium has been associated with skin disorders, including hyperpigmentation, keratosis, and skin cancer. Additionally, occupational exposure to metals such as nickel and chromium can lead to occupational dermatoses, contact dermatitis, and skin sensitization. [43]
B)- Mitigation Strategies: Preventive measures to reduce dermal contact exposure include wearing appropriate protective clothing, gloves, and footwear in occupational settings where contact with metal-containing materials is likely. Personal hygiene practices, such as handwashing and showering after potential exposure, can help minimize skin contact with contaminated substances. Regulatory measures, such as the restriction of hazardous substances in consumer products and occupational safety standards, are essential for reducing the risks associated with dermal exposure in various settings, exposure to toxic metals occurs through multiple routes, each presenting unique risks to human health. Inhalation, ingestion, and dermal contact are the primary pathways of exposure, with occupational, environmental, and consumer-related activities contributing to human exposure levels. Understanding these routes of exposure is essential for assessing health risks, identifying vulnerable populations, and implementing effective preventive measures to mitigate the adverse effects of metal toxicity. [44] By addressing the root causes of exposure and implementing targeted interventions, we can reduce the burden of metal-related diseases and create healthier environments for current and future generations. (Figure 5)
Mechanisms of Toxicity: Understanding How Toxic Metals Impact Human Health
Toxic metals exert their adverse effects on human health through a variety of mechanisms, disrupting normal cellular function and leading to a range of physiological and pathological responses. This section explores the mechanisms by which toxic metals exert their toxicity, including oxidative stress, interference with cellular processes, and disruption of essential biochemical pathways.
1. Toxic metals induce Oxidative Stress:
Oxidative stress induced by toxic metals is a significant mechanism underlying their toxicity in biological systems. Toxic metals such as lead, mercury, cadmium, and arsenic have been shown to promote oxidative stress, leading to damage of cellular components including lipids, proteins, and DNA. Toxic metals induce reactive oxygen species (ROS) generation by disrupting cellular redox balance. They can directly stimulate ROS production via Fenton or Haber-Weiss reactions, or indirectly by inhibiting antioxidant enzymes. ROS cause oxidative damage to biomolecules, leading to cellular dysfunction, DNA damage, and ultimately contributing to metal toxicity. (Figure 6) This oxidative damage can contribute to various adverse health effects, ranging from neurotoxicity and cardiovascular disease to cancer and reproductive dysfunction. [45] One of the primary ways toxic metals induce oxidative stress is through the generation of reactive oxygen species (ROS) and reactive nitrogen species (RNS). Metals such as cadmium and arsenic can directly generate ROS through redox cycling reactions, while others like lead and mercury can disrupt cellular antioxidant defenses, leading to increased ROS production. [46] ROS and RNS are highly reactive molecules that can oxidize cellular macromolecules, resulting in cellular dysfunction and tissue damage. Furthermore, toxic metals can impair the activity of antioxidant enzymes such as superoxide dismutase (SOD), catalase (CAT), and glutathione peroxidase (GPx). [47]
These enzymes play crucial roles in scavenging ROS and maintaining cellular redox homeostasis. For instance, lead has been shown to inhibit SOD and GPx activity, leading to increased oxidative stress and cellular damage. Mercury can also bind to thiol groups in antioxidant enzymes, rendering them inactive and further exacerbating oxidative stress. The mitochondria, known as the powerhouse of the cell, are particularly susceptible to oxidative damage induced by toxic metals. [48] Mitochondrial dysfunction resulting from oxidative stress can disrupt energy production and lead to the generation of more ROS, creating a vicious cycle of oxidative damage. This can have profound effects on cellular function, especially in highly metabolically active tissues such as the brain and heart. Accumulating evidence suggests that oxidative stress induced by toxic metals plays a key role in the development of various diseases. For example, chronic exposure to lead has been linked to neurodegenerative disorders such as Alzheimer's disease and Parkinson's disease, partly due to its ability to induce oxidative stress and neuronal damage. [49] Similarly, mercury exposure has been associated with cardiovascular diseases, with oxidative stress playing a central role in endothelial dysfunction and atherosclerosis. Oxidative stress is a critical mechanism underlying the toxicity of toxic metals in biological systems. By promoting the generation of ROS and impairing antioxidant defenses, these metals can induce oxidative damage to cellular components, leading to a wide range of adverse health effects. [50]
Excessive ROS production can damage cellular macromolecules such as DNA, proteins, and lipids, leading to oxidative damage, inflammation, and cell death. Chronic oxidative stress has been implicated in the pathogenesis of various diseases, including neurodegenerative disorders, cardiovascular diseases, renal dysfunction, and cancer. Additionally, oxidative stress induced by prenatal exposure to toxic metals can result in developmental abnormalities and long-term health effects in infants and children. [51] Strategies to mitigate oxidative stress associated with metal toxicity include enhancing antioxidant defenses through dietary supplementation, promoting healthy lifestyle habits such as regular exercise and balanced nutrition, and reducing exposure to environmental pollutants and pro-oxidant factors. Antioxidant compounds such as vitamins C and E, glutathione, and polyphenols have been shown to mitigate the adverse effects of oxidative stress and protect against metal-induced toxicity in experimental studies. [50]
2. Interference of toxic metals with Cellular Processes:
Toxic metals can interfere with essential cellular processes, including DNA synthesis and repair, protein synthesis, and signal transduction pathways, leading to cellular dysfunction and pathological changes. Metals such as lead, mercury, and cadmium can bind to cellular components such as proteins, enzymes, and nucleic acids, disrupting their structure and function. [52] Interference with DNA synthesis and repair can lead to genetic mutations, chromosomal abnormalities, and increased susceptibility to cancer. Disruption of protein synthesis and folding can impair cellular function and contribute to the development of neurodegenerative diseases, cardiovascular disorders, and renal dysfunction. Metal-induced alterations in signal transduction pathways can dysregulate cellular responses to environmental stimuli, leading to aberrant cell growth, inflammation, and apoptosis. [53]
Mitigating the adverse effects of metal-induced interference with cellular processes requires a multifaceted approach, including the development of targeted therapeutics, the identification of biomarkers of cellular toxicity, and the implementation of preventive measures to reduce exposure levels. Strategies to enhance DNA repair mechanisms, restore protein homeostasis, and modulate signal transduction pathways may offer potential avenues for intervention in metal-induced toxicity. [54] Furthermore, understanding the interplay between genetic susceptibility and metal toxicity is crucial for identifying individuals at heightened risk and tailoring personalized interventions. Integrating advanced technologies such as high-throughput screening assays and omics approaches (e.g., genomics, proteomics, metabolomics) can provide valuable insights into the molecular mechanisms underlying metal-induced cellular dysfunction.
3. Disruption of Essential Biochemical Pathways:
Toxic metals can disrupt essential biochemical pathways within cells, leading to metabolic dysregulation and functional impairment of vital organs and systems. Metals such as arsenic, cadmium, and mercury can interfere with enzymatic processes, metal ion homeostasis, and cellular energy metabolism, leading to a cascade of deleterious effects. Disruption of essential biochemical pathways can lead to metabolic disorders, endocrine disruption, and organ dysfunction. For example, cadmium-induced inhibition of metallothionein synthesis and zinc ion binding can lead to renal tubular dysfunction and impaired renal clearance of toxicants. [55] Mercury-induced inhibition of mitochondrial respiration and ATP synthesis can impair cellular energy metabolism and contribute to neurological deficits and cognitive impairments. [56]
Addressing the disruption of essential biochemical pathways associated with metal toxicity requires targeted interventions aimed at restoring metabolic homeostasis, enhancing detoxification processes, and promoting organ function. Strategies such as chelation therapy, which involves the administration of chelating agents to bind and remove toxic metals from the body, may be employed to mitigate the adverse effects of metal-induced metabolic dysfunction. [57] Additionally, nutritional interventions aimed at replenishing essential nutrients and cofactors may help support cellular function and mitigate the toxic effects of metal exposure. Toxic metals exert their adverse effects on human health through a variety of mechanisms, including oxidative stress, interference with cellular processes, and disruption of essential biochemical pathways. Understanding these mechanisms is essential for elucidating the pathogenesis of metal-induced toxicity and developing targeted interventions to mitigate the adverse effects of metal exposure. By addressing the underlying mechanisms of toxicity and implementing preventive measures to reduce exposure levels, we can minimize the burden of metal-related diseases and promote human health and well-being.
Health Effects from Toxic Metals: Understanding the Risks and Implications
Adverse effects of toxic metals can manifest across multiple organ systems and physiological processes. Understanding the health effects associated with exposure to these metals is essential for assessing risk, identifying vulnerable populations, and implementing preventive measures. This section provides an overview of the health effects associated with exposure to common toxic metals, including lead, mercury, arsenic, and cadmium, along with their physiological mechanisms and implications for human health.
Lead: Exposure to toxic metals, such as lead, poses significant health risks, with deleterious effects on various organ systems and physiological processes. Understanding the mechanisms underlying lead toxicity is essential for elucidating its health effects and developing strategies to mitigate its adverse impact on human health. Lead exerts its toxic effects primarily by interfering with essential biological processes at the cellular and molecular levels. One of the primary mechanisms of lead toxicity involves its ability to mimic essential divalent cations, particularly calcium (Ca2+), and interfere with critical cellular functions reliant on calcium signaling. [58] Lead ions can infiltrate calcium channels and disrupt intracellular calcium homeostasis, leading to dysregulation of cellular signaling pathways and impaired neurotransmitter release. Moreover, lead interferes with the activity of enzymes and proteins crucial for cellular function and metabolism. Lead ions can bind to sulfhydryl groups on enzymes, inhibiting their activity and disrupting essential biochemical pathways. For instance, lead inhibits the activity of delta-aminolevulinic acid dehydratase (ALAD), an enzyme involved in heme synthesis, leading to the accumulation of toxic intermediates and impairing red blood cell function. [59]
Another mechanism by which lead exerts its toxic effects is through the generation of oxidative stress and the production of reactive oxygen species (ROS). Lead-induced oxidative stress results from the imbalance between the production of ROS and the antioxidant defense mechanisms, leading to oxidative damage to lipids, proteins, and DNA. This oxidative damage can disrupt cellular membranes, compromise mitochondrial function, and induce inflammation, contributing to tissue injury and organ dysfunction. Furthermore, lead disrupts the integrity of the blood-brain barrier (BBB) and facilitates its entry into the central nervous system (CNS), where it exerts neurotoxic effects. Once in the brain, lead interferes with neurotransmitter release, impairs synaptic function, and disrupts neuronal signaling pathways. These neurotoxic effects can manifest as cognitive deficits, behavioral abnormalities, learning disabilities, and developmental delays, particularly in children, whose developing brains are more vulnerable to lead exposure. Lead exposure also adversely affects the cardiovascular system, contributing to hypertension, atherosclerosis, and cardiovascular disease. Lead-induced oxidative stress and inflammation promote endothelial dysfunction, impair vascular tone regulation, and promote the formation of atherosclerotic plaques, increasing the risk of heart attacks and strokes. [60] Lead toxicity stems from its ability to disrupt essential cellular processes, interfere with enzyme function, induce oxidative stress, and exert neurotoxic effects. These mechanisms underlie the diverse health effects associated with lead exposure, including neurological impairment, cardiovascular disease, developmental abnormalities, and reproductive dysfunction. Recognizing the mechanisms of lead toxicity is critical for implementing effective preventive measures, such as reducing environmental lead exposure, implementing public health interventions, and promoting early detection and treatment of lead poisoning to mitigate its adverse health effects and protect public health. Lead exposure in children has been associated with developmental delays, learning disabilities, and reduced IQ scores. The neurotoxic effects of lead are thought to result from its ability to interfere with synaptic transmission, disrupt neurotransmitter function, and impair neuronal connectivity in the developing brain. (61,62) Chronic lead exposure has been linked to hypertension, increased risk of cardiovascular disease, and adverse effects on cardiac function. [63] Lead-induced hypertension is thought to result from alterations in vascular tone, renal function, and the renin-angiotensin system, leading to increased peripheral resistance and elevated blood pressure. [64] Lead is known to accumulate in the kidneys and interfere with renal function, leading to tubular damage, proteinuria, and impaired glomerular filtration. Chronic lead exposure has been associated with chronic kidney disease, renal insufficiency, and end-stage renal disease, particularly in adults with occupational or environmental exposure. (65,66) (Figure 7) Lead toxicity adversely affects the heart by increasing blood pressure, causing arrhythmias, and impairing cardiac function. Neurologically, it damages the brain, leading to developmental delays, cognitive impairment, and behavioral disorders. These effects stem from lead's interference with enzyme function, neurotransmitter signaling, and cellular integrity, posing serious health risks.
2. Mercury: Mercury, a toxic metal found in various environmental sources, including air, water, and soil, poses significant health risks to human populations worldwide. Understanding the mechanisms by which mercury exerts its toxic effects is essential for elucidating its health impacts and developing strategies to mitigate exposure and prevent adverse outcomes. One of the primary mechanisms of mercury toxicity involves its ability to bind to sulfhydryl groups (-SH) on proteins and enzymes, disrupting their structure and function. Mercury forms stable complexes with sulfhydryl-containing molecules, such as cysteine residues in proteins, leading to inhibition of enzyme activity and impairment of critical biological processes. This interference with enzymatic function can disrupt essential biochemical pathways, including those involved in cellular metabolism, antioxidant defense, and neurotransmitter regulation. [67] Moreover, mercury disrupts cellular membrane integrity and function, leading to increased permeability and altered membrane fluidity. Mercury ions can incorporate into cell membranes, interfering with lipid bilayer structure and compromising membrane integrity. This disruption of membrane function can impair cellular signaling, ion transport, and nutrient uptake, contributing to cellular dysfunction and tissue damage. Another mechanism by which mercury exerts its toxic effects is through the generation of oxidative stress and the production of reactive oxygen species (ROS). Mercury-induced oxidative stress results from the imbalance between ROS production and antioxidant defense mechanisms, leading to oxidative damage to lipids, proteins, and DNA. This oxidative damage can disrupt cellular function, promote inflammation, and contribute to tissue injury and organ dysfunction. [68]
Furthermore, mercury has a high affinity for binding to sulfur-containing molecules, such as glutathione (GSH), an essential antioxidant molecule. Mercury binds to GSH, depleting cellular antioxidant reserves and impairing the cell's ability to neutralize ROS and protect against oxidative damage. [69] This depletion of antioxidants further exacerbates oxidative stress and contributes to cellular injury and dysfunction. In addition to its direct effects on cellular function and oxidative stress, mercury also exerts neurotoxic effects by interfering with neurotransmitter regulation and synaptic function. [70] Mercury disrupts neurotransmitter release and uptake, impairs synaptic transmission, and alters neuronal signaling pathways. [71] These neurotoxic effects can manifest as cognitive deficits, memory impairment, and behavioral abnormalities, particularly in developing fetuses and young children, whose developing nervous systems are more vulnerable to mercury exposure. [72] Mercury toxicity arises from its ability to disrupt essential cellular processes, impair enzymatic function, induce oxidative stress, and exert neurotoxic effects. The diverse health effects associated with mercury exposure, including neurological impairment, cardiovascular disease, immune dysfunction, and reproductive abnormalities cause deleterious effects on human body. Methylmercury is a potent neurotoxin that can cross the blood-brain barrier and accumulate in the central nervous system, leading to neurodevelopmental deficits, cognitive impairments, and motor dysfunction. [73] Prenatal exposure to methylmercury through maternal consumption of contaminated fish has been linked to adverse effects on fetal brain development, resulting in reduced cognitive function and increased risk of neurodevelopmental disorders such as autism and attention deficit hyperactivity disorder (ADHD). [72] Chronic exposure to mercury has been associated with cardiovascular disease, including hypertension, myocardial infarction, and arrhythmias. Mercury-induced endothelial dysfunction, oxidative stress, and inflammation are thought to contribute to the pathogenesis of cardiovascular disorders, leading to impaired vascular function and increased risk of adverse cardiovascular events. [74] Mercury toxicity harms the heart by causing hypertension, arrhythmias, and myocardial damage. Neurologically, it induces tremors, cognitive deficits, and motor dysfunction. These adverse effects arise from mercury's interference with cellular signaling, enzyme function, and neurotransmitter release, posing significant health risks. (Figure 8) Mercury exposure has been linked to reproductive toxicity, including adverse effects on fertility, pregnancy outcomes, and fetal development. Mercury can accumulate in the placenta and fetal tissues, leading to developmental abnormalities, preterm birth, and low birth weight. Additionally, mercury exposure has been associated with impaired sperm quality and reduced fertility in men. [75]
3. Arsenic: Arsenic, a naturally occurring toxic metalloid found in soil, water, and various industrial products, poses significant health risks to human populations worldwide. Understanding the mechanisms underlying arsenic toxicity is essential for elucidating its health impacts and developing strategies to mitigate exposure and prevent adverse outcomes. Arsenic exerts its toxic effects primarily through its ability to interfere with essential biological processes at the cellular and molecular levels. One of the primary mechanisms of arsenic toxicity involves its interaction with cellular thiols, such as glutathione (GSH), which plays a crucial role in maintaining cellular redox balance and detoxification. Arsenic binds to sulfhydryl groups (-SH) on proteins and enzymes, disrupting their structure and function.[76] This interference with enzymatic activity can impair critical biochemical pathways, including those involved in cellular metabolism, DNA repair, and antioxidant defense mechanisms. Moreover, arsenic disrupts cellular signaling pathways and gene expression by interacting with transcription factors and modulating gene expression patterns. [77] Arsenic can interfere with the activity of transcription factors such as NF-κB and AP-1, which regulate the expression of genes involved in inflammation, cell proliferation, and apoptosis. Dysregulation of these signaling pathways can contribute to oxidative stress, inflammation, and cellular damage, leading to tissue injury and organ dysfunction. [77] Another mechanism by which arsenic exerts its toxic effects is through the generation of reactive oxygen species (ROS) and induction of oxidative stress. Arsenic exposure leads to the production of ROS, including superoxide anion (O2•−) and hydrogen peroxide (H2O2), which can cause oxidative damage to lipids, proteins, and DNA. This oxidative damage disrupts cellular function, impairs mitochondrial respiration, and activates stress-responsive signaling pathways, leading to cellular injury and apoptosis. [78] Furthermore, arsenic interferes with DNA repair mechanisms and promotes the formation of DNA adducts and chromosomal abnormalities. Arsenic exposure can induce DNA strand breaks, cross-linking, and base modifications, leading to genomic instability and increased susceptibility to mutations and carcinogenesis. Chronic exposure to arsenic has been associated with an elevated risk of various cancers, including skin, lung, bladder, and liver cancer, due to its genotoxic effects. In addition to its direct effects on cellular function and oxidative stress, arsenic also disrupts immune function and promotes inflammation. [79] Arsenic exposure can impair immune cell function, alter cytokine production, and suppress immune responses, leading to increased susceptibility to infections and autoimmune diseases. Chronic inflammation associated with arsenic exposure contributes to tissue damage, organ dysfunction, and the development of chronic diseases. [80] Toxicity arises from its ability to interfere with essential cellular processes, disrupt signaling pathways, induce oxidative stress, and promote genotoxicity and inflammation. Arsenic is classified as a Group 1 carcinogen by the International Agency for Research on Cancer (IARC), with evidence linking arsenic exposure to various cancers, including skin, lung, bladder, and liver cancer. Chronic arsenic exposure has been associated with increased cancer incidence, particularly in regions with high levels of arsenic contamination in groundwater. [81] Arsenic exposure has also been linked to cardiovascular disease, including hypertension, atherosclerosis, and peripheral vascular disease. Arsenic-induced endothelial dysfunction, oxidative stress, and inflammation are thought to contribute to the pathogenesis of cardiovascular disorders, leading to impaired vascular function and increased risk of adverse cardiovascular events. [82] Exposure of arsenic can lead to dermatological effects, including hyperpigmentation, keratosis, and skin cancer. Arsenic-induced skin lesions, known as arsenical keratoses, are a hallmark feature of chronic arsenic poisoning and can progress to squamous cell carcinoma in severe cases. [83] Arsenic exposure increases the risk of various cancers including skin, lung, bladder, liver, and kidney cancers. It induces carcinogenesis by disrupting DNA repair mechanisms, promoting oxidative stress, and altering gene expression. Arsenic's ability to activate oncogenes and inhibit tumor suppressor genes contributes to its carcinogenic effects across multiple cell types. Arsenic exposure increases breast cancer risk by disrupting DNA repair mechanisms and promoting oxidative stress and inflammation. (Figure 9)
4. Cadmium: Cadmium, a heavy metal widely distributed in the environment due to industrial activities and natural processes, poses significant health risks to human populations worldwide. Understanding the mechanisms underlying cadmium toxicity is essential for elucidating its health impacts and developing strategies to mitigate exposure and prevent adverse outcomes. Cadmium exerts its toxic effects primarily through its ability to interfere with essential biological processes at the cellular and molecular levels. One of the primary mechanisms of cadmium toxicity involves its high affinity for sulfhydryl groups (-SH) on proteins and enzymes, leading to the disruption of their structure and function. [84] Cadmium ions bind to sulfhydryl-containing molecules, such as cysteine residues in proteins, altering their conformation and inhibiting enzymatic activity. This interference with enzymatic function can impair critical biochemical pathways, including those involved in cellular metabolism, DNA repair, and antioxidant defense mechanisms. Moreover, cadmium disrupts cellular signaling pathways and gene expression by activating stress-responsive signaling cascades and modulating the activity of transcription factors. Cadmium exposure induces the activation of mitogen-activated protein kinases (MAPKs), such as p38 MAPK and c-Jun N-terminal kinase (JNK), which regulate gene expression patterns associated with inflammation, apoptosis, and oxidative stress. [85] Dysregulation of these signaling pathways can lead to the production of reactive oxygen species (ROS), activation of pro-inflammatory cytokines, and promotion of cellular damage and apoptosis. [85]
Another mechanism by which cadmium exerts its toxic effects is through the induction of oxidative stress and the generation of ROS. Cadmium exposure leads to the production of ROS, including superoxide anion (O2•−) and hydroxyl radicals (•OH), which can cause oxidative damage to lipids, proteins, and DNA. This oxidative damage disrupts cellular function, impairs mitochondrial respiration, and activates stress-responsive signaling pathways, leading to cellular injury and apoptosis. [86] Furthermore, cadmium interferes with DNA repair mechanisms and promotes the formation of DNA adducts and chromosomal abnormalities. Cadmium exposure can induce DNA strand breaks, cross-linking, and base modifications, leading to genomic instability and increased susceptibility to mutations and carcinogenesis. [87] Chronic exposure to cadmium has been associated with an elevated risk of various cancers, including lung, prostate, and kidney cancer, due to its genotoxic effects. In addition to its direct effects on cellular function and oxidative stress, cadmium disrupts immune function and promotes inflammation. [87] Cadmium exposure can impair immune cell function, alter cytokine production, and suppress immune responses, leading to increased susceptibility to infections and autoimmune diseases. [88] Chronic inflammation associated with cadmium exposure contributes to tissue damage, organ dysfunction, and the development of chronic diseases. Cadmium is known to accumulate in the kidneys and interfere with renal function, leading to tubular damage, proteinuria, and impaired glomerular filtration.
Chronic cadmium exposure has been associated with chronic kidney disease, renal insufficiency, and end-stage renal disease, particularly in individuals with occupational or environmental exposure. [89] Cadmium exposure has been linked to osteotoxicity, including decreased bone mineral density, osteoporosis, and increased risk of fractures. Cadmium-induced bone damage is thought to result from its ability to interfere with calcium metabolism, disrupt osteoblast function, and stimulate osteoclast activity, leading to bone resorption and skeletal fragility. [90] It has also been associated with reproductive toxicity, including adverse effects on fertility, pregnancy outcomes, and fetal development. Cadmium can accumulate in the testes and ovaries, leading to impaired sperm quality, reduced fertility, and increased risk of adverse pregnancy outcomes such as spontaneous abortion and low birth weight. [91] Exposure to toxic metals such as lead, mercury, arsenic, and cadmium can have profound effects on human health, with adverse effects that can manifest across multiple organ systems and physiological processes. Cadmium toxicity arises from its ability to interfere with essential cellular processes, disrupt signaling pathways, induce oxidative stress, and promote genotoxicity and inflammation. These mechanisms underlie the diverse health effects associated with cadmium exposure, including cancer, cardiovascular disease, neurotoxicity, and immune dysfunction.
Vulnerable Populations from Toxic metal exposure:
Exposure to toxic metals can affect individuals of all ages and backgrounds, but certain populations are particularly vulnerable to the adverse health effects associated with metal exposure. Vulnerable populations may include children, pregnant women, the elderly, individuals with pre-existing health conditions, and marginalized communities. (Figure 10)
1. Children: Children are especially susceptible to the adverse effects of toxic metals due to their developing organ systems, higher rates of exposure, and increased sensitivity to environmental toxins. Lead exposure, in particular, poses significant risks to children's health and development, as even low levels of lead exposure can impair cognitive function, learning ability, and behavior. Children may be exposed to lead through lead-based paint in older housing, contaminated soil and dust, lead pipes, and certain consumer products such as toys and cosmetics. [92] Prenatal exposure to toxic metals can also have lifelong implications for children's health and development. Maternal exposure to metals such as mercury and arsenic during pregnancy can lead to developmental abnormalities, neurological deficits, and increased risk of neurodevelopmental disorders in offspring. Additionally, exposure to metals such as cadmium and lead during critical periods of fetal development can result in adverse pregnancy outcomes, including preterm birth, low birth weight, and developmental delays. (93,94)
2. Pregnant Women: Pregnant women are particularly vulnerable to the adverse effects of toxic metals due to the potential for transplacental transfer of metals to the developing fetus. [95] Exposure to metals such as mercury, lead, and arsenic during pregnancy can have serious consequences for maternal and fetal health, including increased risk of miscarriage, preterm birth, and birth defects. Additionally, prenatal exposure to toxic metals has been linked to long-term health effects in offspring, including cognitive impairments, behavioral disorders, and developmental delays. (96,97) Certain cultural practices and dietary habits may also increase pregnant women's risk of metal exposure. For example, consumption of certain types of fish and seafood high in mercury, such as swordfish and shark, can lead to elevated mercury levels in pregnant women and their unborn babies. [98] Similarly, exposure to lead through contaminated water, soil, or occupational settings can pose risks to maternal and fetal health, highlighting the importance of environmental monitoring and public health interventions to protect vulnerable populations during pregnancy. [99]
3. Elderly Individuals: Elderly individuals are another vulnerable population at increased risk of adverse health effects from toxic metal exposure. Age-related changes in physiology, including decreased renal function, impaired detoxification pathways, and compromised immune function, can make older adults more susceptible to the toxic effects of metals such as lead, cadmium, and arsenic. [100] Additionally, comorbidities such as hypertension, diabetes, and cardiovascular disease can exacerbate the health effects of metal exposure in elderly individuals, leading to increased morbidity and mortality. [101] Chronic exposure to toxic metals over a lifetime can also contribute to the development of age-related diseases and cognitive decline in elderly individuals. For example, lead exposure has been linked to increased risk of neurodegenerative disorders such as Alzheimer's disease and Parkinson's disease, [101] while cadmium exposure has been associated with decreased bone mineral density and increased risk of osteoporosis and fractures in older adults. [102]
4. Individuals with Pre-existing Health Conditions: Individuals with pre-existing health conditions, such as respiratory disorders, cardiovascular disease, and renal dysfunction, may be at increased risk of adverse health effects from toxic metal exposure. [103] Metals such as lead, cadmium, and arsenic can exacerbate existing health conditions and increase the risk of disease progression in vulnerable populations. For example, individuals with asthma or chronic obstructive pulmonary disease (COPD) may be more susceptible to the respiratory effects of metal exposure, including exacerbation of symptoms and increased risk of respiratory infections, [104] similarly, individuals with cardiovascular disease may be at increased risk of adverse cardiovascular events from metal exposure, including hypertension, myocardial infarction, and arrhythmias. [105] Chronic kidney disease patients are particularly vulnerable to the renal effects of metals such as lead and cadmium, as impaired renal function can lead to decreased clearance of metals and increased accumulation in the body, exacerbating renal dysfunction and increasing the risk of adverse outcomes. [106]
5. Marginalized Communities: Marginalized communities, including low-income populations, minority groups, and indigenous communities, may face disproportionate exposure to toxic metals due to socioeconomic factors, environmental injustice, and lack of access to resources and healthcare services. Environmental racism and discrimination can contribute to disparities in exposure to environmental pollutants, including toxic metals, leading to higher rates of adverse health effects in marginalized communities. [107] Industrial facilities, hazardous waste sites, and polluting industries are often located in low-income and minority neighborhoods, leading to increased exposure to environmental contaminants such as lead, mercury, arsenic, and cadmium. Additionally, lack of access to clean drinking water, nutritious food, and healthcare services can exacerbate the health effects of metal exposure in marginalized communities, further widening health disparities and perpetuating cycles of poverty and environmental injustice, [108] these populations are particularly vulnerable to the adverse health effects associated with exposure to toxic metals, including children, pregnant women, the elderly.
Epidemiological Evidence of Health Effects from Toxic Metal Exposure
Epidemiological studies play a crucial role in elucidating the relationship between toxic metal exposure and adverse health outcomes in human populations. By examining patterns of exposure and disease occurrence across different populations, these studies provide valuable insights into the magnitude of the health risks posed by toxic metals and inform public health policies and interventions. [109]
1. Lead Exposure: Epidemiological evidence has consistently demonstrated the detrimental effects of lead exposure on neurological development, cognitive function, and cardiovascular health. Longitudinal studies of children exposed to lead have shown associations between elevated blood lead levels and reduced IQ scores, learning disabilities, and behavioral problems. [110] The landmark Dunedin Multidisciplinary Health and Development Study, for example, followed a cohort of individuals from birth to adulthood and found that childhood lead exposure was associated with lower cognitive function, poorer educational attainment, and increased risk of criminal behavior in adulthood. In addition to its effects on neurodevelopment, lead exposure has been linked to increased risk of cardiovascular disease, hypertension, and renal dysfunction in adults. (111,112,113) Epidemiological studies have shown associations between higher blood lead levels and elevated blood pressure, increased risk of myocardial infarction, and impaired renal function. The Normative Aging Study, a longitudinal cohort study of elderly men, found that higher bone lead levels were associated with increased risk of hypertension and decreased renal function, independent of other cardiovascular risk factors. [114]
2. Mercury Exposure: Epidemiological research has provided compelling evidence of the health effects of mercury exposure, particularly methylmercury, on neurological development, cardiovascular health, and reproductive outcomes. Prospective cohort studies of pregnant women and their offspring have demonstrated associations between maternal methylmercury exposure from fish consumption and adverse neurodevelopmental outcomes in children, including reduced IQ scores, impaired cognitive function, and increased risk of developmental delays. [115] In addition to its neurotoxic effects, mercury exposure has been linked to cardiovascular disease and adverse pregnancy outcomes. Epidemiological studies have shown associations between higher mercury exposure and increased risk of hypertension, myocardial infarction, and stroke in adults. Similarly, prenatal mercury exposure has been associated with increased risk of preterm birth, low birth weight, and developmental abnormalities in offspring. [116]
3. Arsenic Exposure: Epidemiological evidence has highlighted the health risks associated with arsenic exposure, particularly through contaminated drinking water, including increased risk of cancer, cardiovascular disease, and skin lesions. Longitudinal studies of populations exposed to high levels of arsenic in drinking water have shown elevated risks of various cancers, including skin, lung, bladder, and liver cancer. [117] The Health Effects of Arsenic Longitudinal Study (HEALS), conducted in Bangladesh, found dose-response relationships between arsenic exposure and increased mortality from cancers of the lung, bladder, and kidney. In addition to its carcinogenic effects, arsenic exposure has been associated with increased risk of cardiovascular disease and skin lesions. [118] Epidemiological studies have shown associations between higher arsenic exposure and elevated risk of hypertension, atherosclerosis, and peripheral vascular disease. Similarly, chronic arsenic exposure has been linked to the development of skin lesions, including hyperpigmentation, keratosis, and skin cancer, particularly in regions with high levels of arsenic contamination in groundwater.
4. Cadmium Exposure: Epidemiological research has documented the health effects of cadmium exposure on renal function, bone health, and cardiovascular disease. Longitudinal studies of populations exposed to cadmium through occupational settings or environmental contamination have shown associations between higher urinary cadmium levels and increased risk of renal dysfunction, including proteinuria, decreased glomerular filtration rate, and chronic kidney disease. In addition to its renal effects, cadmium exposure has been linked to adverse bone outcomes and cardiovascular disease. [119] Epidemiological studies have shown associations between higher cadmium exposure and increased risk of osteoporosis, fractures, and decreased bone mineral density, particularly in postmenopausal women. Similarly, chronic cadmium exposure has been associated with elevated risk of hypertension, peripheral arterial disease, and myocardial infarction, independent of other cardiovascular risk factors.[120] Epidemiological evidence from studies examining the health effects of toxic metal exposure provides critical insights into the magnitude of the risks posed by these environmental contaminants. By identifying associations between exposure levels and disease outcomes, epidemiological research informs public health policies and interventions aimed at reducing exposure and mitigating the adverse health effects of toxic metals.
Prevention and Intervention Strategies for Mitigating Toxic Metal Exposure
Preventing and mitigating exposure to toxic metals is essential for protecting public health and reducing the burden of metal-related diseases. Effective prevention and intervention strategies encompass a range of approaches, including regulatory measures, environmental monitoring, public health interventions, and community outreach. (Figure 11)
1. Regulatory Measures: Regulatory measures play a critical role in controlling and reducing exposure to toxic metals by establishing standards, guidelines, and regulations to limit environmental contamination and protect human health. Government agencies such as the Environmental Protection Agency (EPA), the Food and Drug Administration (FDA), and the Occupational Safety and Health Administration (OSHA) set standards for permissible levels of toxic metals in air, water, food, consumer products, and occupational settings. For example, regulations such as the Clean Air Act and the Clean Water Act impose emissions standards on industrial sources to reduce air and water pollution from toxic metals such as lead, mercury, and arsenic. Similarly, the FDA establishes maximum allowable levels of mercury in seafood to protect consumers from methylmercury exposure. Occupational safety regulations set by OSHA mandate the use of engineering controls, personal protective equipment, and workplace monitoring to minimize worker exposure to toxic metals in industrial settings. [121]
2. Environmental Monitoring: Environmental monitoring programs are essential for assessing the extent of metal contamination in air, water, soil, and food sources and identifying high-risk areas and populations. Monitoring efforts involve collecting and analyzing samples from environmental media and biomonitoring studies to measure metal concentrations and track trends over time. [122] Government agencies, academic institutions, and environmental organizations collaborate to conduct monitoring programs and provide data to inform regulatory decisions and public health interventions. For example, the EPA's National Ambient Air Quality Standards (NAAQS) program monitors air quality across the United States to assess compliance with standards for air pollutants, including lead, mercury, and arsenic. Similarly, the FDA conducts routine monitoring of seafood products to assess mercury levels and ensure compliance with safety standards. Biomonitoring studies measure metal levels in human tissues and biological fluids to assess exposure levels and identify at-risk populations, informing targeted interventions and preventive measures.[123]
3. Public Health Interventions: Public health interventions aim to raise awareness about the risks of metal exposure, promote healthy behaviors, and provide resources and support to affected communities. [124] Education campaigns, outreach programs, and community engagement efforts play a crucial role in empowering individuals and communities to take proactive steps to reduce exposure and protect their health. For example, public health agencies collaborate with healthcare providers, community organizations, and schools to educate the public about sources of lead exposure, such as lead-based paint and contaminated drinking water, and provide guidance on preventive measures, such as regular testing of water and soil, and safe practices for home renovation and remodeling. Similarly, educational materials and outreach events raise awareness about the risks of mercury exposure from fish consumption and provide guidance on selecting safe seafood options and limiting exposure. (125,126)
4. Environmental Remediation: Environmental remediation efforts aim to clean up contaminated sites and reduce exposure pathways to toxic metals in affected communities. Remediation strategies may include soil and water remediation, containment measures, and site redevelopment to restore land use and prevent ongoing exposure to contaminants. For example, remediation efforts in communities with legacy lead contamination from industrial sources may involve soil excavation, encapsulation, or phytoremediation techniques to reduce soil lead levels and prevent exposure to residents, particularly children. Similarly, cleanup efforts in mercury-contaminated water bodies may involve dredging, sediment removal, or wetland restoration to reduce mercury levels and restore aquatic ecosystems. [127] Bioremediation reduces metal poisoning by using plants, like sunflowers, for phytoremediation, and bacteria for microbial bioremediation, transforming heavy metals into less toxic forms in soil and water. Preventing and mitigating exposure to toxic metals requires a comprehensive approach that encompasses regulatory measures, environmental monitoring, public health interventions, and community engagement efforts. [128] (Figure 12) By implementing targeted strategies to reduce environmental contamination, raise awareness about the risks of metal exposure, and empower individuals and communities to take proactive measures to protect their health, we can reduce the burden of metal-related diseases and create healthier environments for current and future generations. [129] Continued collaboration between government agencies, healthcare providers, community organizations, and the public is essential for achieving meaningful progress in addressing the challenges posed by toxic metal exposure and promoting human health and well-being.
Monitoring and Surveillance of Toxic Metals: Safeguarding Public Health through Vigilance:
Monitoring and surveillance of toxic metals are crucial components of public health efforts aimed at identifying, assessing, and mitigating the risks posed by environmental contaminants. By systematically collecting and analyzing data on metal concentrations in air, water, soil, food, and biological samples, monitoring and surveillance programs provide valuable insights into exposure levels, trends, and distribution patterns, enabling informed decision-making and targeted interventions. [130] (Figure 13)
1. Importance of Monitoring and Surveillance: Monitoring and surveillance of toxic metals serve several critical functions in protecting public health. Monitoring programs measure metal concentrations in environmental media and biological samples to assess exposure levels and identify populations at risk. By quantifying exposure levels and trends over time, monitoring data inform risk assessments and guide the development of targeted interventions to reduce exposure. [131] Surveillance efforts identify geographic areas with elevated metal contamination levels and prioritize resources for intervention and remediation. By mapping metal concentrations and identifying hotspots of environmental contamination, surveillance data inform decision-making and resource allocation to protect vulnerable populations. [132] Monitoring programs assess compliance with regulatory standards and guidelines for permissible levels of toxic metals in air, water, food, and consumer products. By enforcing environmental regulations and monitoring compliance, surveillance efforts ensure that protective measures are in place to safeguard public health. [133] Surveillance systems track trends in metal-related diseases and health outcomes to detect emerging threats and inform public health responses. By monitoring disease incidence, mortality rates, and biomarker data, surveillance efforts identify health disparities and guide preventive measures to reduce the burden of metal-related diseases. [134]
2. Methodologies for Monitoring and Surveillance: Monitoring and surveillance of toxic metals employ a variety of methodologies to collect, analyse, and interpret data. Monitoring programs collect samples of air, water, soil, and food from environmental media to measure metal concentrations using analytical techniques such as atomic absorption spectrometry, inductively coupled plasma mass spectrometry, and X-ray fluorescence spectroscopy. Sampling strategies may include grab sampling, passive sampling, and continuous monitoring to capture spatial and temporal variability in metal levels. (135,136) Surveillance efforts measure metal levels in biological samples, such as blood, urine, hair, and nails, to assess internal exposure levels and biomarker responses in human populations. Biomonitoring studies provide direct measures of internal dose and enable comparisons with reference values and health-based guidelines to assess risks and inform public health interventions. Surveillance systems track disease incidence, prevalence, and mortality rates associated with metal exposure to identify trends and patterns in health outcomes. Epidemiological studies examine associations between metal exposure and disease outcomes using cohort studies, case-control studies, and ecological analyses to elucidate causal relationships and guide preventive measures. [138]
3. Challenges and Emerging Trends: Despite the importance of monitoring and surveillance efforts, several challenges exist in effectively managing the risks associated with toxic metal exposure. Limited funding, personnel, and infrastructure constrain the capacity of monitoring programs to collect comprehensive data on metal concentrations and health outcomes, particularly in low-resource settings and underserved communities. Integration of data from multiple sources, including environmental monitoring, biomonitoring, and health surveillance, poses challenges in harmonizing methodologies, standardizing measurements, and synthesizing findings to inform decision-making and policy development. Rapid industrialization, urbanization, and technological advancements introduce new contaminants and exposure pathways, necessitating ongoing surveillance efforts to monitor emerging threats and adapt preventive measures to address evolving risks. Meaningful engagement with communities, stakeholders, and policymakers is essential for building trust, fostering collaboration, and promoting transparency in monitoring and surveillance efforts to address community concerns and priorities. Monitoring and surveillance of toxic metals are essential components of public health efforts to identify, assess, and mitigate the risks posed by environmental contaminants. By systematically collecting and analyzing data on metal concentrations, exposure levels, and health outcomes, monitoring and surveillance programs provide valuable insights into the spatial and temporal distribution of metal contamination, enabling informed decision-making and targeted interventions to protect public health. Continued investment in monitoring and surveillance infrastructure, capacity-building initiatives, and community engagement efforts is essential for addressing emerging threats, reducing health disparities, and promoting environmental justice in vulnerable communities. [139]
Treatment and Management of Toxic Metal Poisoning: Strategies for Minimizing Health Risks and Promoting Recovery
Toxic metal poisoning poses significant health risks, requiring prompt and effective treatment and management strategies to mitigate adverse effects and promote recovery. While prevention remains the cornerstone of addressing metal exposure, individuals who have been exposed to toxic metals may require medical intervention to address acute toxicity and prevent long-term health consequences. (Figure 14)
1. Chelation Therapy: Chelation therapy is a medical intervention used to remove toxic metals from the body by administering chelating agents that bind to metal ions and facilitate their excretion through urine or feces. Chelating agents such as dimercaprol, EDTA (ethylene diamine tetra-acetic acid), DMSA (dimercaptosuccinic acid), and DMPS (2,3-dimercapto-1-propanesulfonic acid) are commonly used in clinical practice to treat acute metal poisoning and chronic metal toxicity. Chelation therapy is the primary treatment for lead poisoning, particularly in cases of severe toxicity or symptomatic lead encephalopathy. EDTA and DMSA are FDA-approved chelating agents for lead poisoning, administered intravenously or orally to enhance lead excretion and reduce blood lead levels. Chelation therapy may be indicated in children with blood lead levels ≥45 µg/dL or adults with blood lead levels ≥70 µg/dL, according to CDC guidelines. [140] Chelation therapy may be considered in cases of acute mercury poisoning or chronic mercury exposure with elevated urine mercury levels. DMPS and DMSA are FDA-approved chelating agents for mercury toxicity, administered orally or intravenously to enhance mercury excretion and reduce body burden. Chelation therapy may be combined with supportive care measures, such as fluid replacement and electrolyte balance, to manage symptoms of mercury toxicity. [141] Chelation therapy may be used in cases of acute arsenic poisoning or chronic arsenic exposure with elevated urine arsenic levels. Dimercaprol and DMSA are FDA-approved chelating agents for arsenic toxicity, administered intramuscularly or orally to enhance arsenic excretion and reduce body burden. Chelation therapy may be supplemented with supportive measures, such as gastric lavage and activated charcoal, to remove arsenic from the gastrointestinal tract. [142] Chelation therapy may be considered in cases of acute cadmium poisoning or chronic cadmium exposure with elevated urine cadmium levels. EDTA and DMPS are FDA-approved chelating agents for cadmium toxicity, administered intravenously or orally to enhance cadmium excretion and reduce body burden. Chelation therapy may be combined with supportive care measures, such as respiratory support and hemodialysis, to manage symptoms of cadmium toxicity. [143]
2. Supportive Care: In addition to chelation therapy, supportive care measures play a crucial role in managing toxic metal poisoning and addressing associated symptoms and complications. Supportive care interventions includes Intravenous fluids, that may be administered to maintain hydration and electrolyte balance in patients with dehydration or electrolyte imbalances resulting from metal poisoning. (144,145) Medications may be prescribed to alleviate symptoms of metal poisoning, such as pain relievers for headache and abdominal pain, antiemetics for nausea and vomiting, and antihypertensives for hypertension. Gastric lavage, activated charcoal, and cathartics may be used to remove ingested metals from the gastrointestinal tract and prevent systemic absorption. Mechanical ventilation may be required in cases of severe respiratory distress or acute respiratory failure resulting from metal fume inhalation or pulmonary edema. [146]
3. Long-term Monitoring and Follow-up: After initial treatment for toxic metal poisoning, patients may require long-term monitoring and follow-up to assess recovery, monitor residual metal levels, and address potential health effects. Long-term monitoring may involve: Blood and urine tests may be performed periodically to monitor metal levels and assess response to treatment. Serial monitoring of metal biomarkers can help evaluate the effectiveness of chelation therapy and guide adjustments in treatment regimens. [147] Children exposed to lead or mercury may undergo neurodevelopmental assessment to evaluate cognitive function, learning ability, and behavioral outcomes. Longitudinal follow-up may be recommended to monitor developmental progress and identify any delays or deficits. Individuals exposed to cadmium or arsenic may undergo renal function testing to assess kidney function and detect early signs of renal dysfunction. [148] Long-term follow-up may be necessary to monitor renal health and identify any deterioration in kidney function.Patients with a history of chronic lead or arsenic exposure may undergo cardiovascular evaluation to assess cardiovascular risk factors, such as hypertension, atherosclerosis, and peripheral vascular disease. Longitudinal monitoring may be recommended to monitor cardiovascular health and manage any complications. [149] Treatment and management of toxic metal poisoning require a multifaceted approach that encompasses chelation therapy, supportive care, and long-term monitoring. Prompt recognition of metal poisoning, initiation of appropriate treatment, and close follow-up are essential for minimizing health risks, promoting recovery, and preventing long-term complications.
Future Directions in the Management of Toxic Metal Exposure: As we look ahead, several key areas warrant attention and exploration to advance the management of toxic metal exposure and protect public health. These future directions encompass research, technology, policy, and community engagement initiatives aimed at enhancing our understanding of metal toxicity, improving prevention and intervention strategies, and promoting environmental sustainability. [150] Continued advancements in monitoring technologies, such as sensor-based systems, remote sensing platforms, and portable analytical devices, hold promise for enhancing real-time detection and mapping of metal contamination in air, water, soil, and food sources. These technologies enable rapid response to environmental emergencies, early warning systems for at-risk populations, and targeted interventions to mitigate exposure risks. Tailored interventions based on individual susceptibility factors, genetic predisposition, and biomarker profiles offer opportunities for personalized medicine approaches to the management of metal toxicity. (151,152) Precision medicine strategies, including pharmacogenomics, metabolomics, and molecular imaging techniques, may help identify high-risk individuals, optimize treatment regimens, and improve health outcomes for affected populations. Embracing principles of green chemistry, sustainable manufacturing, and pollution prevention can reduce the environmental burden of toxic metals and minimize exposure risks throughout the product lifecycle. [153] Innovations in eco-friendly materials, waste management technologies, and clean production processes contribute to a circular economy and promote environmental sustainability while safeguarding human health. Engaging communities, stakeholders, and affected populations in participatory research initiatives fosters collaboration, empowers local decision-making, and promotes environmental justice in addressing metal contamination issues. Community-based participatory research approaches, including citizen science projects, environmental health assessments, and participatory action research, enhance community resilience, build trust, and promote equitable solutions to environmental challenges.
Integrated Risk Assessment Frameworks: Developing integrated risk assessment frameworks that consider cumulative exposures, synergistic effects, and vulnerable populations' susceptibility can improve our understanding of the complex interactions between multiple metals and other environmental stressors. Integrated approaches, such as exposome analysis, systems toxicology, and multi-stressor modeling, enable comprehensive risk assessment and inform evidence-based decision-making for preventive interventions. Strengthening regulatory frameworks, updating exposure guidelines, and implementing evidence-based policies are essential for addressing emerging threats and protecting public health from metal exposure risks. Policy initiatives, such as pollution prevention strategies, green procurement policies, and environmental justice legislation, promote equitable access to clean air, water, and soil, and hold polluters accountable for environmental contamination.
Global Collaboration and Knowledge Sharing: Promoting international collaboration, knowledge sharing, and capacity-building efforts fosters a collective response to global challenges associated with toxic metal exposure. Collaborative initiatives, such as research networks, data-sharing platforms, and international partnerships, facilitate cross-border cooperation, harmonize standards, and strengthen resilience to environmental threats on a global scale. Future efforts to manage toxic metal exposure require a multidisciplinary and collaborative approach that integrates scientific innovation, policy reform, community engagement, and global cooperation. By investing in research, technology, and policy initiatives aimed at preventing exposure, improving treatment outcomes, and promoting environmental sustainability, we can address the complex challenges posed by toxic metal contamination and create healthier, more resilient communities for future generations.
Conclusion:
In conclusion, the management of toxic metal poisoning requires a multi-pronged approach that integrates preventive measures, prompt treatment, and long-term monitoring. Toxic metals such as lead, mercury, arsenic, and cadmium pose significant health risks, with adverse effects ranging from neurological impairment and cardiovascular disease to renal dysfunction and developmental abnormalities. Prevention remains paramount in reducing exposure to these contaminants, with regulatory measures, environmental monitoring, and public health interventions playing critical roles in controlling contamination levels and protecting human health. Once exposure has occurred, timely intervention is essential to mitigate acute toxicity and prevent long-term health consequences. Chelation therapy serves as a cornerstone of treatment for severe cases of metal poisoning, facilitating the removal of toxic metals from the body and reducing body burden. Chelating agents such as EDTA, DMSA, DMPS, and dimercaprol are commonly used in clinical practice to enhance metal excretion and promote recovery. Supportive care measures, including fluid replacement, symptomatic treatment, and gastrointestinal decontamination, complement chelation therapy by addressing associated symptoms and complications. Furthermore, long-term monitoring and follow-up are crucial components of managing toxic metal poisoning, enabling healthcare providers to assess recovery, monitor residual metal levels, and identify potential health effects.
Periodic blood and urine testing, neurodevelopmental assessment, renal function monitoring, and cardiovascular evaluation facilitate ongoing surveillance of affected individuals and guide interventions to optimize health outcomes. By implementing comprehensive management strategies and fostering collaboration between healthcare providers, public health agencies, and community stakeholders, we can minimize the adverse effects of toxic metal exposure and promote health and well-being for affected individuals and communities. However, challenges remain in addressing the complexities of toxic metal poisoning, including resource limitations, data integration issues, emerging contaminants, and the need for community engagement. Continued investment in surveillance infrastructure, capacity-building initiatives, and research efforts is essential for enhancing our understanding of metal exposure risks and developing targeted interventions to address evolving threats. By prioritizing prevention, early intervention, and long-term monitoring, we can mitigate the health risks associated with toxic metal exposure and create healthier environments for current and future generations. In essence, the management of toxic metal poisoning requires a comprehensive and collaborative approach that encompasses prevention, treatment, and ongoing surveillance. By leveraging scientific knowledge, regulatory frameworks, and community partnerships, we can mitigate the adverse effects of metal contamination and safeguard public health for generations to come.
Conflict of Interest
None Declared
Acknowledgement
We extend our sincere gratitude to Era University for their generous provision of logistics support, which greatly facilitated the execution of this Article.
Funding
None
References
- Khlifi, R.; Hamza-Chaffai, A. Head and neck cancer due to heavy metal exposure via tobacco smoking and professional exposure: A review. Toxicol. Appl. Pharmacol. 2010, 248, 71–88. [Google Scholar] [CrossRef] [PubMed]
- Jarup, L. Hazards of heavy metal contamination. Br. Med. Bull. 2003, 68, 167–182. [Google Scholar] [CrossRef] [PubMed]
- Nagajyoti, P.C.; Lee, K.D.; Sreekanth, T.V.M. Heavy metals, occurrence and toxicity for plants: a review. Environ. Chem. Lett. 2010, 8, 199–216. [Google Scholar] [CrossRef]
- Lambert, M.; Leven BA, Green RM. New methods of cleaning up heavy metal in soils and water; Environmental science and technology briefs for citizens; Manhattan, KS: Kansas State University; 2000.
- Morais, S.; Costa, F.G.; Pereira, M.L. Heavy metals and human health. In: Oosthuizen, J.; editor. Environmental health – emerging issues and practice. 2012. pp. 227–246.
- Nriagu, J.O. A History of Global Metal Pollution. Science 1996, 272, 223–223. [Google Scholar] [CrossRef]
- Hughes, J.P.; Polissar, L.; VAN Belle, G. Evaluation and Synthesis of Health Effects Studies of Communities Surrounding Arsenic Producing Industries. Leuk. Res. 1988, 17, 407–413. [Google Scholar] [CrossRef]
- Chen, C.W.; Chen, C.F.; Dong, C.D. Distribution and Accumulation of Mercury in Sediments of Kaohsiung River Mouth, Taiwan. APCBEE Procedia. 2012, 1, 153–158. [Google Scholar] [CrossRef]
- Valko, M.; Morris, H.; Cronin, M.T. Metals, toxicity and oxidative stress. Curr Med Chem. 2005, 12, 1161–208. [Google Scholar] [CrossRef]
- Jomova, K.; Valko, M. Advances in metal-induced oxidative stress and human disease. Toxicology 2011, 283, 65–87. [Google Scholar] [CrossRef]
- Jarup, L. Hazards of heavy metal contamination. Br. Med. Bull. 2003, 68, 167–182. [Google Scholar] [CrossRef]
- Sanders, T.; Liu, Y.; Buchner, V.; Tchounwou, P. Neurotoxic Effects and Biomarkers of Lead Exposure: A Review. Rev. Environ. Heal. 2009, 24, 15–46. [Google Scholar] [CrossRef]
- Chowdhury, R.; Ramond, A.; O’keeffe, L.M.; Shahzad, S.; Kunutsor, S.K.; Muka, T.; Gregson, J.; Willeit, P.; Warnakula, S.; Khan, H.; et al. Environmental toxic metal contaminants and risk of cardiovascular disease: systematic review and meta-analysis. BMJ 2018, 362, k3310. [Google Scholar] [CrossRef] [PubMed]
- Jin, T.; Lu, J.; Nordberg, M. Toxicokinetics and biochemistry of cadmium with special emphasis on the role of metallothionein. Neurotoxicology 1998, 19, 529–535. [Google Scholar] [PubMed]
- Valko M, Morris H, Cronin MT. Metals, toxicity and oxidative stress. Curr Med Chem. 2005, 12, 1161–1208. [CrossRef] [PubMed]
- Sharma, P.; Dubey, RS. Lead toxicity in plants. Brazilian Journal of Plant Physiology 2005, 17, 35–52. [Google Scholar] [CrossRef]
- Najeeb, U.; Ahmad, W.; Zia, M.H.; Zaffar, M.; Zhou, W. Enhancing the lead phytostabilization in wetland plant Juncus effusus L. through somaclonal manipulation and EDTA enrichment. Arab. J. Chem. 2017, 10, S3310–S3317. [Google Scholar] [CrossRef]
- Yongsheng, W.; Qihui, L.; Qian, T. Effect of Pb on growth, accumulation and quality component of tea plant. Procedia Eng. 2011, 18, 214–219. [Google Scholar] [CrossRef]
- Goyer, R.A. Lead Toxicity: From Overt to Subclinical to Subtle Health Effects. Environ. Heal. Perspect. 1990, 86, 177. [Google Scholar] [CrossRef]
- Chen CW, Chen CF, Dong CD. Distribution and Accumulation of Mercury in Sediments of Kaohsiung River Mouth, Taiwan. APCBEE Procedia 2012, 1, 153–158. [Google Scholar] [CrossRef]
- Yang, L.; Zhang, Y.; Wang, F.; Luo, Z.; Guo, S.; Strähle, U. Toxicity of mercury: Molecular evidence. Chemosphere 2019, 245, 125586. [Google Scholar] [CrossRef]
- Trasande, L.; Landrigan, P.J.; Schechter, C. Public Health and Economic Consequences of Methyl Mercury Toxicity to the Developing Brain. Environ. Heal. Perspect. 2005, 113, 590–596. [Google Scholar] [CrossRef]
- Hughes, J.P.; Polissar, L.; VAN Belle, G. Evaluation and Synthesis of Health Effects Studies of Communities Surrounding Arsenic Producing Industries. Leuk. Res. 1988, 17, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Singh, N.; Kumar, D.; Sahu, A.P. Arsenic in the environment: effects on human health and possible prevention. Journal of Environmental Biology 2007, 28, 359–365. [Google Scholar] [PubMed]
- Kaur, S.; Kamli, M.R.; Ali, A. Role of arsenic and its resistance in nature. Can. J. Microbiol. 2011, 57, 769–774. [Google Scholar] [CrossRef] [PubMed]
- Byeon, E.; Kang, H.-M.; Yoon, C.; Lee, J.-S. Toxicity mechanisms of arsenic compounds in aquatic organisms. Aquat. Toxicol. 2021, 237, 105901. [Google Scholar] [CrossRef]
- Satarug, S.; Garrett, S.H.; Sens, M.A.; Sens, D.A. Cadmium, environmental exposure, and health outcomes. Environ Health Perspect. 2010, 118, 182–90. [Google Scholar] [CrossRef]
- Fatima, G.; Raza, A.M.; Hadi, N.; Nigam, N.; Mahdi, A.A. Cadmium in Human Diseases: It’s More than Just a Mere Metal. Indian J. Clin. Biochem. 2019, 34, 371–378. [Google Scholar] [CrossRef]
- Mutlu, A.; Lee, B.-K.; Park, G.-H.; Yu, B.-G.; Lee, C.-H. Long-term concentrations of airborne cadmium in metropolitan cities in Korea and potential health risks. Atmospheric Environ. 2012, 47, 164–173. [Google Scholar] [CrossRef]
- Ganguly, K.; Levänen, B.; Palmberg, L.; Åkesson, A.; Lindén, A. Cadmium in tobacco smokers: a neglected link to lung disease? Eur Respir Rev. 2018, 27, 170122. [Google Scholar] [CrossRef]
- Satarug, S.; Garrett, S.H.; Sens, M.A.; Sens, D.A. Cadmium, environmental exposure, and health outcomes. Ciência & Saúde Coletiva. 2011, 16, 2587–2602. [Google Scholar]
- Irfan, M.; Hayat, S.; Ahmad, A.; Alyemeni, M.N. Soil cadmium enrichment: Allocation and plant physiological manifestations. Saudi J. Biol. Sci. 2012, 20, 1–10. [Google Scholar] [CrossRef]
- Hossini, H.; Shafie, B.; Niri, A.D.; Nazari, M.; Esfahlan, A.J.; Ahmadpour, M.; Nazmara, Z.; Ahmadimanesh, M.; Makhdoumi, P.; Mirzaei, N.; et al. A comprehensive review on human health effects of chromium: insights on induced toxicity. Environ. Sci. Pollut. Res. 2022, 29, 70686–70705. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Lin, Z.; Wang, Y.; Li, C.; Xu, W.; Li, Q.; Yao, W.; Song, Z.; Liu, G. Nickle(II) ions exacerbate bleomycin-induced pulmonary inflammation and fibrosis by activating the ROS/Akt signaling pathway. Environ. Sci. Pollut. Res. 2017, 25, 4406–4418. [Google Scholar] [CrossRef] [PubMed]
- Colomina MT, Peris-Sampedro, F. Aluminum and Alzheimer's Disease. Adv Neurobiol. 2017, 18, 183–197. [Google Scholar]
- Rehman, K.; Fatima, F.; Waheed, I.; Akash, M.S.H. Prevalence of exposure of heavy metals and their impact on health consequences. J. Cell. Biochem. 2018, 119, 157–184. [Google Scholar] [CrossRef]
- Shabanda, I.S.; Koki, I.B.; Low, K.H.; Zain, S.M.; Khor, S.M.; Abu Bakar, N.K. Daily exposure to toxic metals through urban road dust from industrial, commercial, heavy traffic, and residential areas in Petaling Jaya, Malaysia: a health risk assessment. Environ. Sci. Pollut. Res. 2019, 26, 37193–37211. [Google Scholar] [CrossRef]
- Lafta, M.H.; Afra, A.; Patra, I.; Jalil, A.T.; Mohammadi, M.J.; Al-Dhalimy, A.M.B.; Ziyadullaev, S.; Kiani, F.; Ekrami, H.A.; Asban, P. Toxic effects due to exposure heavy metals and increased health risk assessment (leukemia). Rev. Environ. Heal. 2022, 39, 351–362. [Google Scholar] [CrossRef]
- Occupational Safety and Health Administration (OSHA) - Respiratory Protection Standard (29 CFR 1910.134)" https://www.osha.gov/laws-regs/regulations/standardnumber/1910/1910.134.
- Charkiewicz, A.E.; Backstrand, J.R. Lead Toxicity and Pollution in Poland. Int. J. Environ. Res. Public Heal. 2020, 17, 4385. [Google Scholar] [CrossRef]
- Al Osman, M.; Yang, F.; Massey, I.Y. Exposure routes and health effects of heavy metals on children. BioMetals 2019, 32, 563–573. [Google Scholar] [CrossRef]
- Landrigan PJ, Stegeman JJ, Fleming LE, Allemand D, Anderson DM, Backer LC, Brucker-Davis F et al Human Health and Ocean Pollution. Ann Glob Health. 2020, 86, 151.
- Filon, F.L.; Bello, D.; Cherrie, J.W.; Sleeuwenhoek, A.; Spaan, S.; Brouwer, D.H. Occupational dermal exposure to nanoparticles and nano-enabled products: Part I—Factors affecting skin absorption. Int. J. Hyg. Environ. Heal. 2016, 219, 536–544. [Google Scholar] [CrossRef]
- Anderson, S.E.; Meade, B.J. Potential Health Effects Associated with Dermal Exposure to Occupational Chemicals. Environ. Heal. Insights 2014, 8, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Jomova, K.; Valko, M. Advances in metal-induced oxidative stress and human disease. Toxicology 2011, 283, 65–87. [Google Scholar] [CrossRef] [PubMed]
- Fu, Z.; Xi, S. The effects of heavy metals on human metabolism. Toxicol. Mech. Methods 2019, 30, 167–176. [Google Scholar] [CrossRef] [PubMed]
- Birla, H.; Minocha, T.; Kumar, G.; Misra, A.; Singh, S.K. Role of Oxidative Stress and Metal Toxicity in the Progression of Alzheimer’s Disease. Curr. Neuropharmacol. 2020, 18, 552–562. [Google Scholar] [CrossRef]
- Nowicka, B. Heavy metal–induced stress in eukaryotic algae—mechanisms of heavy metal toxicity and tolerance with particular emphasis on oxidative stress in exposed cells and the role of antioxidant response. Environ. Sci. Pollut. Res. 2022, 29, 16860–16911. [Google Scholar] [CrossRef]
- Valko, M.; Rhodes, C.J.; Moncol, J.; Izakovic, M.; Mazur, M. Free radicals, metals and antioxidants in oxidative stress-induced cancer. Chem. Biol. Interact. 2006, 160, 1–40. [Google Scholar] [CrossRef]
- Flora, S.J.S. Structural, Chemical and Biological Aspects of Antioxidants for Strategies Against Metal and Metalloid Exposure. Oxidative Med. Cell. Longev. 2009, 2, 191–206. [Google Scholar] [CrossRef]
- Farina, M.; Avila, D.S.; da Rocha, J.B.T.; Aschner, M. Metals, oxidative stress and neurodegeneration: A focus on iron, manganese and mercury. Neurochem. Int. 2013, 62, 575–594. [Google Scholar] [CrossRef]
- Haidar, Z.; Fatema, K.; Shoily, S.S.; Sajib, A.A. Disease-associated metabolic pathways affected by heavy metals and metalloid. Toxicol. Rep. 2023, 10, 554–570. [Google Scholar] [CrossRef]
- Morales ME, Derbes RS, Ade CM, Ortego JC, Stark J, Deininger PL, Roy-Engel AM. Heavy Metal Exposure Influences Double Strand Break DNA Repair Outcomes. PLoS One 2016, 11, e0151367. [Google Scholar]
- Huang, R.; Zhou, P.-K. DNA damage repair: historical perspectives, mechanistic pathways and clinical translation for targeted cancer therapy. Signal Transduct. Target. Ther. 2021, 6, 1–35. [Google Scholar] [CrossRef] [PubMed]
- Genchi, G.; Sinicropi, M.S.; Lauria, G.; Carocci, A.; Catalano, A. The Effects of Cadmium Toxicity. Int. J. Environ. Res. Public Health 2020, 17, 3782. [Google Scholar] [CrossRef] [PubMed]
- Jacob, S.; Thangarajan, S. Fisetin impedes developmental methylmercury neurotoxicity via downregulating apoptotic signalling pathway and upregulating Rho GTPase signalling pathway in hippocampus of F1 generation rats. Int. J. Dev. Neurosci. 2018, 69, 88–96. [Google Scholar] [CrossRef] [PubMed]
- Flora, S.J.S.; Pachauri, V. Chelation in Metal Intoxication. Int. J. Environ. Res. Public Health 2010, 7, 2745–2788. [Google Scholar] [CrossRef]
- Ashraf U, Kanu AS, Mo Z, Hussain S, Anjum SA, Khan I, Abbas RN, Tang, X. Lead toxicity in rice: effects, mechanisms, and mitigation strategies--a mini review. Environ Sci Pollut Res Int. 2015, 22, 18318–18332. [Google Scholar] [CrossRef]
- Jonasson, M.; Afshari, R. Historical documentation of lead toxicity prior to the 20th century in English literature. Hum. Exp. Toxicol. 2017, 37, 775–788. [Google Scholar] [CrossRef]
- Bellinger, DC. Lead. Pediatrics 2004, 113(4 Suppl), 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- Grandjean, P.; Landrigan, P.J. Neurobehavioural effects of developmental toxicity. Lancet Neurol. 2014, 13, 330–338. [Google Scholar] [CrossRef]
- van de Bor, M. Fetal toxicology. Handb Clin Neurol. 2019, 162, 31–55. [Google Scholar]
- Huang, Z. Association Between Blood Lead Level With High Blood Pressure in US (NHANES 1999–2018). Front. Public Heal. 2022, 10, 836357. [Google Scholar] [CrossRef]
- Scinicariello, F.; Abadin, H.G.; Murray, H.E. Association of low-level blood lead and blood pressure in NHANES 1999–2006. Environ. Res. 2011, 111, 1249–1257. [Google Scholar] [CrossRef] [PubMed]
- Howard, S.C.; McCormick, J.; Pui, C.-H.; Buddington, R.K.; Harvey, R.D. Preventing and Managing Toxicities of High-Dose Methotrexate. Oncologist 2016, 21, 1471–1482. [Google Scholar] [CrossRef] [PubMed]
- Perazella, M.A. Drug-induced acute kidney injury: diverse mechanisms of tubular injury. Curr. Opin. Crit. Care 2019, 25, 550–557. [Google Scholar] [CrossRef] [PubMed]
- Yang, L.; Zhang, Y.; Wang, F.; Luo, Z.; Guo, S.; Strähle, U. Toxicity of mercury: Molecular evidence. Chemosphere 2019, 245, 125586. [Google Scholar] [CrossRef]
- Sakamoto, M.; Nakamura, M.; Murata, K. Mercury as a Global Pollutant and Mercury Exposure Assessment and Health Effects. Nippon. Eiseigaku Zasshi (Japanese J. Hyg. 2018, 73, 258–264. [Google Scholar] [CrossRef]
- Zhao, Y.; Zhou, C.; Guo, X.; Hu, G.; Li, G.; Zhuang, Y.; Cao, H.; Li, L.; Xing, C.; Zhang, C.; et al. Exposed to Mercury-Induced Oxidative Stress, Changes of Intestinal Microflora, and Association between them in Mice. Biol. Trace Element Res. 2020, 199, 1900–1907. [Google Scholar] [CrossRef]
- Carocci, A.; Rovito, N.; Sinicropi, M.S.; Genchi, G. Mercury Toxicity and Neurodegenerative Effects. Rev. Environ. Contam. Toxicol. 2014, 229, 1–18. [Google Scholar] [CrossRef]
- Ke, T.; A Tinkov, A.; Skalny, A.V.; Bowman, A.B.; Rocha, J.B.T.; Santamaria, A.; Aschner, M. Developmental exposure to methylmercury and ADHD, a literature review of epigenetic studies. Environ. Epigenetics 2021, 7, dvab014. [Google Scholar] [CrossRef]
- Landrigan, P.J.; Wright, R.O.; Birnbaum, L.S. Mercury Toxicity in Children. Science 2013, 342, 1447–1447. [Google Scholar] [CrossRef]
- Raposo RS, Pinto DV, Moreira R, Dias RP, Fontes Ribeiro CA, Oriá RB and Malva JO. Methylmercury Impact on Adult Neurogenesis: Is the Worst Yet to Come From Recent Brazilian Environmental Disasters? Front. Aging Neurosci. 2020, 12, 59160.
- Genchi G, Sinicropi MS, Carocci A, Lauria G, Catalano, A. Mercury Exposure and Heart Diseases. Int J Environ Res Public Health. 2017, 14, 74. [Google Scholar] [CrossRef] [PubMed]
- McCue, K.; DeNicola, N. Environmental Exposures in Reproductive Health. Obstet. Gynecol. Clin. North Am. 2019, 46, 455–468. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Li, J.; Lou, B.; Wu, R.; Wang, G.; Lu, C.; Wang, H.; Pi, J.; Xu, Y. The Role of Reactive Oxygen Species in Arsenic Toxicity. Biomolecules 2020, 10, 240. [Google Scholar] [CrossRef] [PubMed]
- Ratnaike, R.N. Acute and chronic arsenic toxicity. Postgrad. Med J. 2003, 79, 391–396. [Google Scholar] [CrossRef]
- Zargari, F.; Rahaman, S.; KazemPour, R.; Hajirostamlou, M. Arsenic, Oxidative Stress and Reproductive System. J. Xenobiotics 2022, 12, 214–222. [Google Scholar] [CrossRef]
- Huang, H.-W.; Lee, C.-H.; Yu, H.-S. Arsenic-Induced Carcinogenesis and Immune Dysregulation. Int. J. Environ. Res. Public Heal. 2019, 16, 2746. [Google Scholar] [CrossRef]
- Attreed, S.E.; Navas-Acien, A.; Heaney, C.D. Arsenic and Immune Response to Infection During Pregnancy and Early Life. Curr. Environ. Heal. Rep. 2017, 4, 229–243. [Google Scholar] [CrossRef]
- Martinez, V.D.; Vucic, E.A.; Becker-Santos, D.D.; Gil, L.; Lam, W.L. Arsenic Exposure and the Induction of Human Cancers. J. Toxicol. 2011, 2011, 1–13. [Google Scholar] [CrossRef]
- Kononenko, M.; Frishman, W.H. Association Between Arsenic Exposure and Cardiovascular Disease. Cardiol. Rev. 2020, 29, 217–221. [Google Scholar] [CrossRef]
- Paul, S.; Majumdar, S.; Giri, A.K. Genetic susceptibility to arsenic-induced skin lesions and health effects: a review. Genes Environ. 2015, 37, 1–7. [Google Scholar] [CrossRef]
- Charkiewicz, A.E.; Omeljaniuk, W.J.; Nowak, K.; Garley, M.; Nikliński, J. Cadmium Toxicity and Health Effects—A Brief Summary. Molecules 2023, 28, 6620. [Google Scholar] [CrossRef] [PubMed]
- Wieland, M.; Levin, M.K.; Hingorani, K.S.; Biro, F.N.; Hingorani, M.M. Mechanism of Cadmium-Mediated Inhibition of Msh2-Msh6 Function in DNA Mismatch Repair. Biochemistry 2009, 48, 9492–9502. [Google Scholar] [CrossRef] [PubMed]
- Ma, Y.; Su, Q.; Yue, C.; Zou, H.; Zhu, J.; Zhao, H.; Song, R.; Liu, Z. The Effect of Oxidative Stress-Induced Autophagy by Cadmium Exposure in Kidney, Liver, and Bone Damage, and Neurotoxicity. Int. J. Mol. Sci. 2022, 23, 13491. [Google Scholar] [CrossRef] [PubMed]
- Park, S.S.; A Skaar, D.; Jirtle, R.L.; Hoyo, C. Epigenetics, Obesity and Early-Life Cadmium or Lead Exposure. Epigenomics 2016, 9, 57–75. [Google Scholar] [CrossRef]
- Wang, Z.; Sun, Y.; Yao, W.; Ba, Q.; Wang, H. Effects of Cadmium Exposure on the Immune System and Immunoregulation. Front. Immunol. 2021, 12, 695484. [Google Scholar] [CrossRef]
- Fujiki, K. Involvement of Notch1 and ALK4/5 Signaling Pathways in Renal Tubular Cell Death: Their Application to Clarification of Cadmium Toxicity. Nippon. Eiseigaku Zasshi (Japanese J. Hyg.) 2020, 75, 20007. [Google Scholar] [CrossRef]
- Bhattacharyya, M.H. Cadmium osteotoxicity in experimental animals: Mechanisms and relationship to human exposures. Toxicol. Appl. Pharmacol. 2009, 238, 258–265. [Google Scholar] [CrossRef]
- Ragan HA, Mast TJ. Cadmium inhalation and male reproductive toxicity. Rev Environ Contam Toxicol. 1990, 114, 1–22. [Google Scholar]
- Yazdanfar, N.; Saatloo, N.V.; Sadighara, P. Contamination of potentially toxic metals in children’s toys marketed in Iran. Environ. Sci. Pollut. Res. 2022, 29, 68441–68446. [Google Scholar] [CrossRef]
- Al Osman, M.; Yang, F.; Massey, I.Y. Exposure routes and health effects of heavy metals on children. BioMetals 2019, 32, 563–573. [Google Scholar] [CrossRef]
- Ma, J.; Geng, S.; Sun, Q.; Zhang, X.; Han, L.; Yao, X.; Zhang, B.; Zhu, L.; Wen, J. Exposure to metal mixtures and young children’s growth and development: A biomonitoring-based study in Eastern China. Ecotoxicol. Environ. Saf. 2023, 268, 115726. [Google Scholar] [CrossRef] [PubMed]
- Gundacker, C.; Hengstschläger, M. The role of the placenta in fetal exposure to heavy metals. Wien. Med. Wochenschr. 2012, 162, 201–206. [Google Scholar] [CrossRef] [PubMed]
- Wai, K.M.; Mar, O.; Kosaka, S.; Umemura, M.; Watanabe, C. Prenatal Heavy Metal Exposure and Adverse Birth Outcomes in Myanmar: A Birth-Cohort Study. Int. J. Environ. Res. Public Health 2017, 14, 1339. [Google Scholar] [CrossRef] [PubMed]
- Lawn JE, Cousens S, Zupan, J. 4 million neonatal deaths: When? Where? Why? Lancet, 2005; 365, 891–900.
- Oken, E.; Bellinger, D.C. Fish consumption, methylmercury and child neurodevelopment. Curr. Opin. Pediatr. 2008, 20, 178–183. [Google Scholar] [CrossRef]
- Zajac, L.; Kobrosly, R.W.; Ericson, B.; Caravanos, J.; Landrigan, P.J.; Riederer, A.M. Probabilistic estimates of prenatal lead exposure at 195 toxic hotspots in low- and middle-income countries. Environ. Res. 2020, 183, 109251–109251. [Google Scholar] [CrossRef]
- Kamel, F.; Umbach, D.; Hu, H.; Munsat, T.; Shefner, J.; Taylor, J.; Sandler, D. Lead Exposure as a Risk Factor for Amyotrophic Lateral Sclerosis. Neurodegener. Dis. 2005, 2, 195–201. [Google Scholar] [CrossRef]
- Weisskopf, M.G.; Weuve, J.; Nie, H.; Saint-Hilaire, M.-H.; Sudarsky, L.; Simon, D.K.; Hersh, B.; Schwartz, J.; Wright, R.O.; Hu, H. Association of Cumulative Lead Exposure with Parkinson’s Disease. Environ. Heal. Perspect. 2010, 118, 1609–1613. [Google Scholar] [CrossRef]
- Engström, A.; Michaëlsson, K.; Vahter, M.; Julin, B.; Wolk, A.; Åkesson, A. Associations between dietary cadmium exposure and bone mineral density and risk of osteoporosis and fractures among women. Bone 2012, 50, 1372–1378. [Google Scholar] [CrossRef]
- Mordukhovich, I.; Wright, R.O.; Hu, H.; Amarasiriwardena, C.; Baccarelli, A.; Litonjua, A.; Sparrow, D.; Vokonas, P.; Schwartz, J. Associations of Toenail Arsenic, Cadmium, Mercury, Manganese, and Lead with Blood Pressure in the Normative Aging Study. Environ. Heal. Perspect. 2012, 117, 1532–1538. [Google Scholar]
- Münzel, T.; Gori, T.; Al-Kindi, S.; Deanfield, J.; Lelieveld, J.; Daiber, A.; Rajagopalan, S. Effects of gaseous and solid constituents of air pollution on endothelial function. Eur. Heart J. 2018, 39, 3543–3550. [Google Scholar] [CrossRef]
- Navas-Acien, A.; Guallar, E.; Silbergeld, E.K.; Rothenberg, S.J. Lead Exposure and Cardiovascular Disease—A Systematic Review. Environ. Heal. Perspect. 2007, 115, 472–482. [Google Scholar] [CrossRef] [PubMed]
- Kim, N.H.; Hyun, Y.Y.; Lee, K.B.; Chang, Y.; Ryu, S.; Oh, K.H.; Ahn, C. Environmental heavy metal exposure and chronic kidney disease in the general population. J. Korean Med. Sci. 2014, 29, 1491–1498. [Google Scholar]
- Mohai, P.; Saha, R. Reassessing racial and socioeconomic disparities in environmental justice research. Demography 2006, 43, 383–399. [Google Scholar] [CrossRef] [PubMed]
- Morello-Frosch, R.; Jesdale, B.W. Separate and Unequal: Residential Segregation and Estimated Cancer Risks Associated with Ambient Air Toxics in U.S. Metropolitan Areas. Environ. Health Perspect. 2006, 114, 386–393. [Google Scholar] [CrossRef]
- Saha, D.; Alam, S.; Haque, M.A.; Alam, M.S.; Islam, M.S.; Rahman, M.S. . & Khan, M.H. Association of blood lead level with hypertension and renal function in a Bangladeshi adult population: A cross-sectional study. Chemosphere 2022, 287, 132041. [Google Scholar]
- Bellinger, D.C. Lead neurotoxicity and socioeconomic status: Conceptual and analytical issues. NeuroToxicology 2008, 29, 828–832. [Google Scholar] [CrossRef]
- Poulton, R.; Moffitt, T.E.; Silva, P.A. The Dunedin Multidisciplinary Health and Development Study: overview of the first 40 years, with an eye to the future. Chest 2015, 50, 679–693. [Google Scholar] [CrossRef]
- Caspi, A.; Houts, R.M.; Belsky, D.W.; Goldman-Mellor, S.J.; Harrington, H. The p factor: One general psychopathology factor in the structure of psychiatric disorders? Clin. Psychol. Sci. 2014, 2, 119–137. [Google Scholar] [CrossRef]
- Vaziri, N.D. Mechanisms of lead-induced hypertension and cardiovascular disease. Am. J. Physiol. Circ. Physiol. 2008, 295, H454–H465. [Google Scholar] [CrossRef]
- Hu, H.; Shih, R.; Rothenberg, S.; Schwartz, B.S. The Epidemiology of Lead Toxicity in Adults: Measuring Dose and Consideration of Other Methodologic Issues. Environ. Heal. Perspect. 2007, 115, 455–462. [Google Scholar] [CrossRef]
- Grandjean, P.; Landrigan, P.J. Developmental neurotoxicity of industrial chemicals: A silent pandemic. Lancet 2006, 368, 2167–2178. [Google Scholar] [CrossRef] [PubMed]
- Roman, H.A.; Walsh, T.L.; Coull, B.A.; Dewailly, É.; Guallar, E.; Hattis, D.; Mariën, K.; Schwartz, J.; Stern, A.H.; Virtanen, J.K.; et al. Evaluation of the Cardiovascular Effects of Methylmercury Exposures: Current Evidence Supports Development of a Dose–Response Function for Regulatory Benefits Analysis. Environ. Heal. Perspect. 2011, 119, 607–614. [Google Scholar] [CrossRef] [PubMed]
- Bakulski, K.M.; Feinberg, J.I.; Andrews, S.V.; Yang, J.; Brown, S.; McKenney, S.L.; Martin, E. DNA methylation signatures of prenatal exposure to arsenic and associations with developmental and health outcomes in childhood. Environ. Int. 2020, 134, 105289. [Google Scholar]
- Chen, Y.; Graziano, J.H.; Parvez, F.; Liu, M.; Slavkovich, V.; Kalra, T.; Argos, M.; Islam, T.; Ahmed, A.; Rakibuz-Zaman, M.; et al. Arsenic exposure from drinking water and mortality from cardiovascular disease in Bangladesh: prospective cohort study. BMJ 2011, 342, d2431–d2431. [Google Scholar] [CrossRef]
- Wu, H.; Lai, Y.; Zhu, G.; Wang, X.; Ding, X.; Huang, S. Relationship between cadmium exposure and renal outcomes in a Chinese population: a cross-sectional study. Environ. Health Prev. Med. 2020, 25, 1–10. [Google Scholar]
- Kwak, K.M.; Paek, D.; Hwang, S.J.; Kim, Y.; Choi, Y.H.; Chung, H.K. Association of blood cadmium with hypertension in the Korean general population: analysis of the 2008-2013 Korean National Health and Nutrition Examination Survey data. Environ. Health Toxicol. 2019, 34, e2019007. [Google Scholar]
- Bland, J.M.; Baker, G.; Rees, M. An overview of regulatory aspects of toxic metals in food and dietary supplements. Foods 2021, 10, 1068. [Google Scholar]
- Sharma, S.; Nagpal, A.; Maurya, R. Environmental monitoring and health risk assessment of heavy metals using leafy vegetables. Environ. Sci. Pollut. Res. 2020, 27, 37991–38004. [Google Scholar]
- Monikh, F.A.; Hadipour, M.; Karami, M. Monitoring and health risk assessment of heavy metals in seafood from the Persian Gulf. Environ. Sci. Pollut. Res. 2021, 28, 50482–50493. [Google Scholar]
- Kriegel, A.M.; Soliman, A.S.; Zhang, Q. Mercury exposure: a neglected public health problem. J. Environ. Health 2021, 84, 16–24. [Google Scholar]
- Xue, J.; Zartarian, V.; Wang, S.W.; Liu, S.V. Lead exposure reduction efforts and declining blood lead levels among US children. J. Environ. Health 2020, 82, 20–27. [Google Scholar]
- Schober, S.E.; Mirel, L.B.; Grainger, J.; Dye, B.A.; Caudill, S.P.; Belson, M. Blood lead levels and death from all causes, cardiovascular disease, and cancer: results from the NHANES III mortality study. Environ. Health Perspect. 2012, 120, 518–524. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Chen, S.; Wu, X.; Sun, H. Recent advances in heavy metal removal from water and wastewater by graphene-based nanomaterials: Mechanisms, influencing factors, and environmental implications. J. Hazard. Mater. 2022, 429, 128069. [Google Scholar]
- Praveena, S.M.; Shaari, N.; Aris, A.Z. Heavy metals removal from soil and water using agricultural waste-based adsorbents: A review. J. Environ. Manag. 2022, 306, 114565. [Google Scholar]
- Tong, J.; Zhu, R. Immobilization remediation of heavy metal-contaminated soil: A review. J. Hazard. Mater. 2021, 411, 124983. [Google Scholar]
- Alves, M.A.; Mota, J.P.; Rosa, R. Heavy metals in marine invertebrates: monitoring and biomarker responses. Rev. Environ. Contam. Toxicol. 2020, 249, 1–30. [Google Scholar]
- Lin, C.C.; Chen, Y.C.; Su, F.C.; Lin, C.M. Exposure to heavy metals and its association with chronic kidney disease: A nationwide population-based study in Taiwan. Sci. Total Environ. 2022, 804, 150085. [Google Scholar]
- Wang, X.; Sato, T.; Xing, B.; Tao, S. Assessing and mapping regional mercury contamination using tree bark as bio-indicator: A case study in China. Environ. Pollut. 2020, 267, 115637. [Google Scholar]
- Babamale, O.A.; Olawale, O.B.; Ayanda, I.O.; Taiwo, A.M. Regulatory compliance and health risk assessment of heavy metals in drinking water sources and bottled water within Ibadan metropolis, Nigeria. Environ. Geochem. Health Advance online publication. 2022. [Google Scholar] [CrossRef]
- Barceloux, D.G. (2021). Clinical and public health aspects of cadmium toxicity in humans. In Cadmium Toxicity and Tolerance in Plants (pp. 145–175). Springer, Cham. [CrossRef]
- Gardea-Torresdey, J.L.; Tiemann, K.J.; Armendariz, R.; Rodriguez, O.; Gamez, G.; Webb, R. Characterization of trace metal particulates found on playgrounds in the El Paso, Texas, USA-Mexico border region. Int. J. Environ. Health Res. 2003, 13, 19–28. [Google Scholar] [CrossRef]
- USEPA. (2017). Compendium of methods for the determination of inorganic compounds in ambient air. United States Environmental Protection Agency.
- Holland, M.G.; Carrington, C.D. (2020). Biomonitoring of metals in urine and blood in the general population. In Trace Metals and Other Contaminants in the Environment (pp. 207–244). Academic Press. [CrossRef]
- Navas-Acien, A.; Sharrett, A.R.; Silbergeld, E.K.; Schwartz, B.S.; Nachman, K.E.; Burke, T.A.; Guallar, E. Arsenic Exposure and Cardiovascular Disease: A Systematic Review of the Epidemiologic Evidence. Am. J. Epidemiology 2005, 162, 1037–1049. [Google Scholar] [CrossRef] [PubMed]
- Sudhakar, V.; Rai, P.; Choudhury, S.R. Current trends and challenges in environmental health risk assessment of heavy metals: A review. J. Environ. Manag. 2021, 290, 112675. [Google Scholar]
- Rogan, W.J.; Dietrich, K.N.; Ware, J.H.; Dockery, D.W.; Salganik, M.; Radcliffe, J.; Jones, R.L.; Ragan, N.B.; Chisolm, J.J.J.; Rhoads, G.G. The Effect of Chelation Therapy with Succimer on Neuropsychological Development in Children Exposed to Lead. New Engl. J. Med. 2001, 344, 1421–1426. [Google Scholar] [CrossRef] [PubMed]
- Geier, D.A.; Geier, M.R. A Prospective Study of Mercury Toxicity Biomarkers in Autistic Spectrum Disorders∗. J. Toxicol. Environ. Heal. Part A 2007, 70, 1723–1730. [Google Scholar] [CrossRef]
- Yoshida, T.; Yamauchi, H.; Sun, G.F. Chronic health effects in people exposed to arsenic via the drinking water: dose?response relationships in review. Toxicol. Appl. Pharmacol. 2004, 198, 243–252. [Google Scholar] [CrossRef]
- Vaziri, N.D.; Gonick, H.C.; Wedeen, R.P. Experimental cadmium nephropathy: Effect of chelation therapy with succimer. Arch. Environ. Health: Int. J. 1982, 37, 178–184. [Google Scholar]
- Velez, L.I.; O'Connell, E.J.; Jean, J. Lead toxicity. In StatPearls [Internet]. StatPearls Publishing. [PubMed]
- Goldfrank, L.R.; Nelson, L.S.; Howland, M.A. Goldfrank's Toxicologic Emergencies. McGraw Hill Professional.
- Wong, O. (2014). Metals. In LaDou, J. (Ed.), Current Occupational & Environmental Medicine (5th ed.; pp. 448-476).
- Liu, J.; Zhang, H.; Lin, L. The application of metal ions in the diagnosis and treatment of osteoarthritis. Bioinorg. Chem. Appl. 2019, 5467428. [Google Scholar]
- Bellinger, D.C. Neurological and behavioral toxicity of lead. Neurol. Clin. 2016, 34, 445–455. [Google Scholar]
- Moon, K.A.; Oberoi, S.; Barchowsky, A.; Chen, Y. Challenging the hypothesis of an inverse stage-association between arsenic in drinking water and prevalence of hypertension in the United States. Int. J. Hyg. Environ. Health 2018, 221, 79–88. [Google Scholar]
- Navas-Acien, A.; Silbergeld, E.K.; Pastor-Barriuso, R.; Guallar, E. Arsenic Exposure and Prevalence of Type 2 Diabetes in US Adults. JAMA 2008, 300, 814–822. [Google Scholar] [CrossRef]
- Shah, A.S.V.; Langrish, J.P.; Nair, H.; McAllister, D.A.; Hunter, A.L.; Donaldson, K.; Newby, D.E.; Mills, N.L. Global association of air pollution and heart failure: a systematic review and meta-analysis. Lancet 2013, 382, 1039–1048. [Google Scholar] [CrossRef] [PubMed]
- Zheng, J.S.; Xu, W.; Yang, J.; Ye, Q.; Zhou, M.; Xie, L. . & Shu, X.O. Plasma selenium biomarkers in association with risk of different cancers: a population-based nested case-control study. Lancet 2017, 389, S86. [Google Scholar] [CrossRef]
- Crespo-Otero, R.; Vega-Hernandez, E.; Sanchez-Gonzalez, J. Computational drug discovery: Where are we now? Drug Discovery Today 2021, 26, 600–613. [Google Scholar]
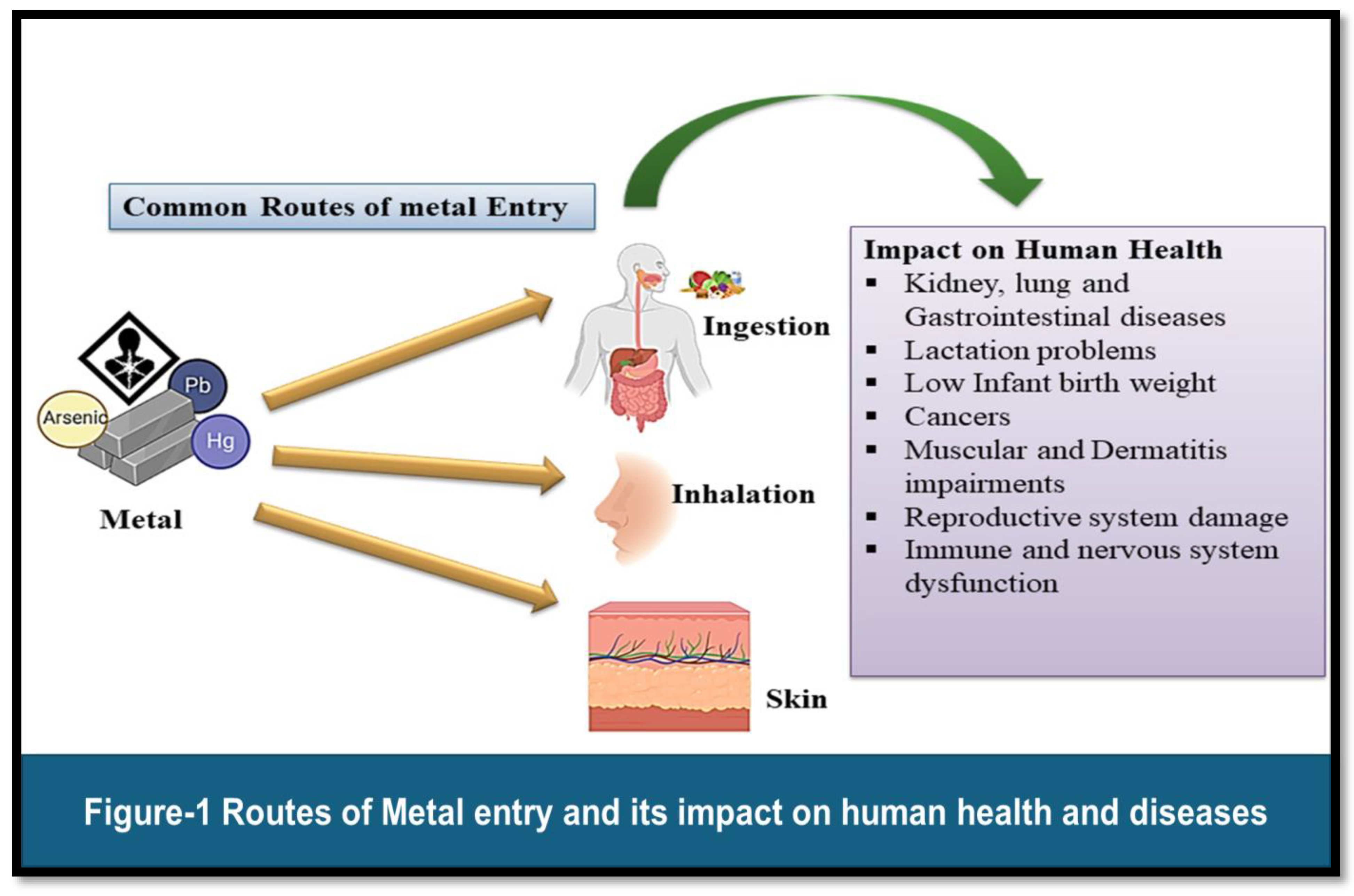
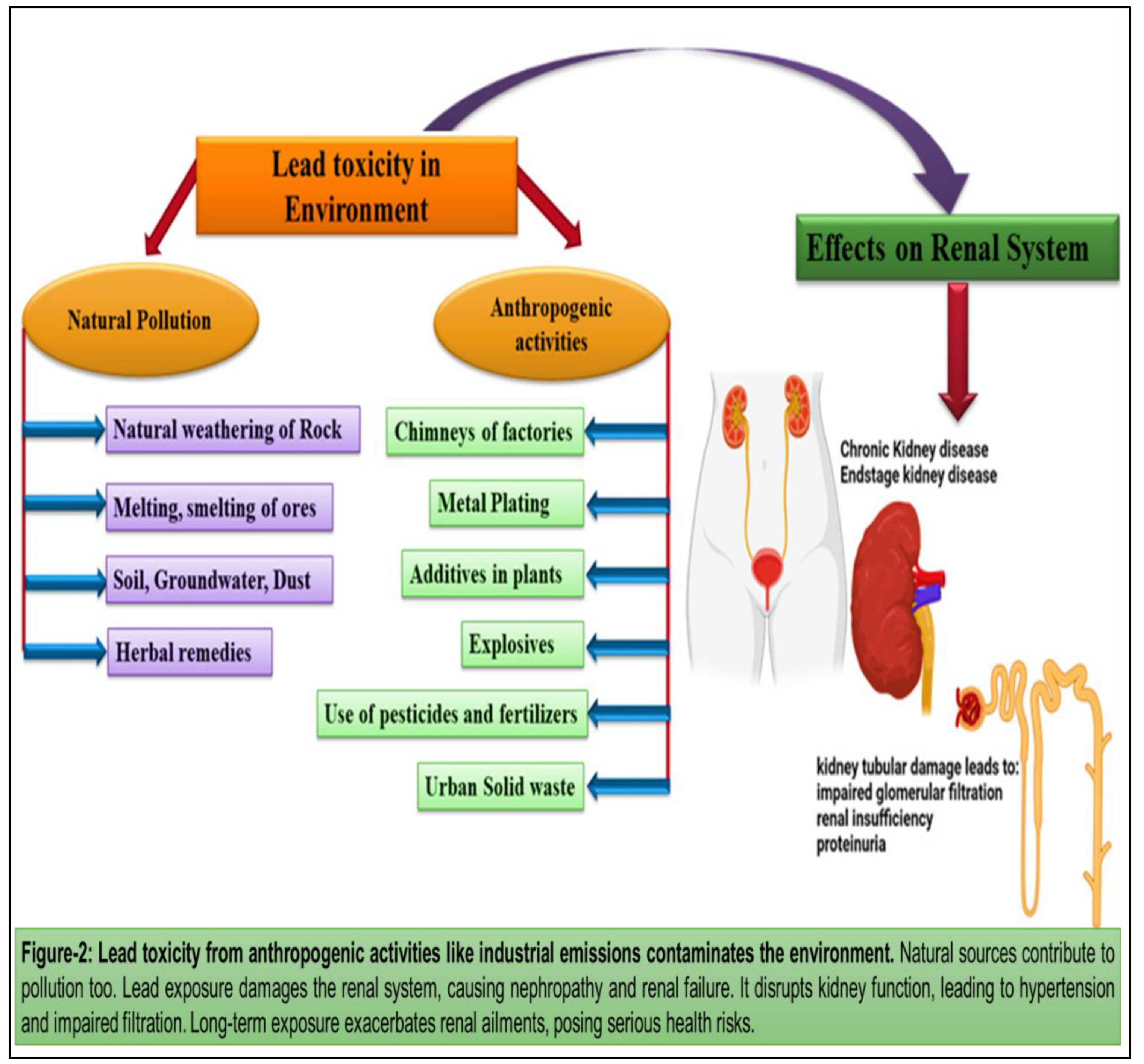
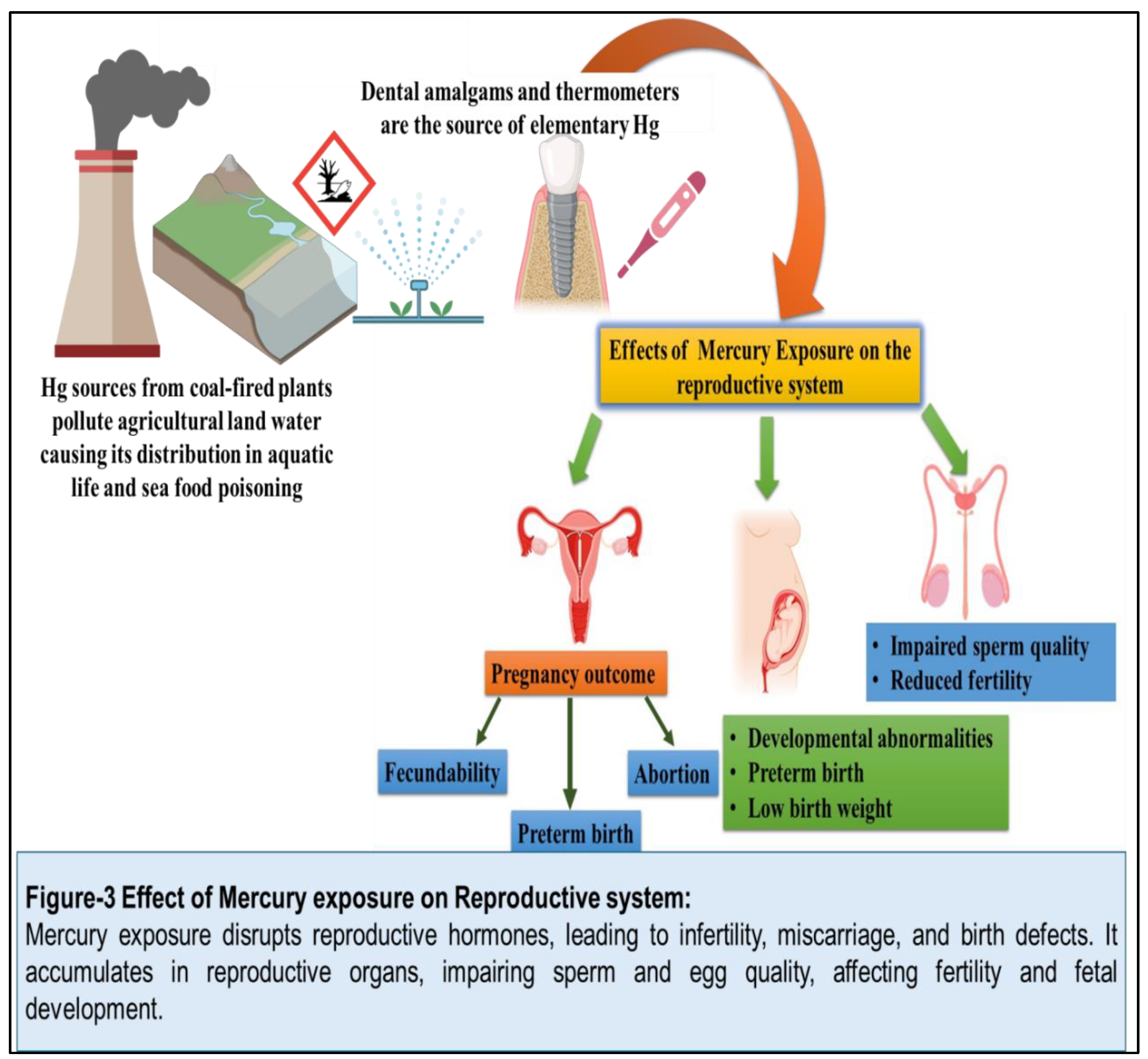
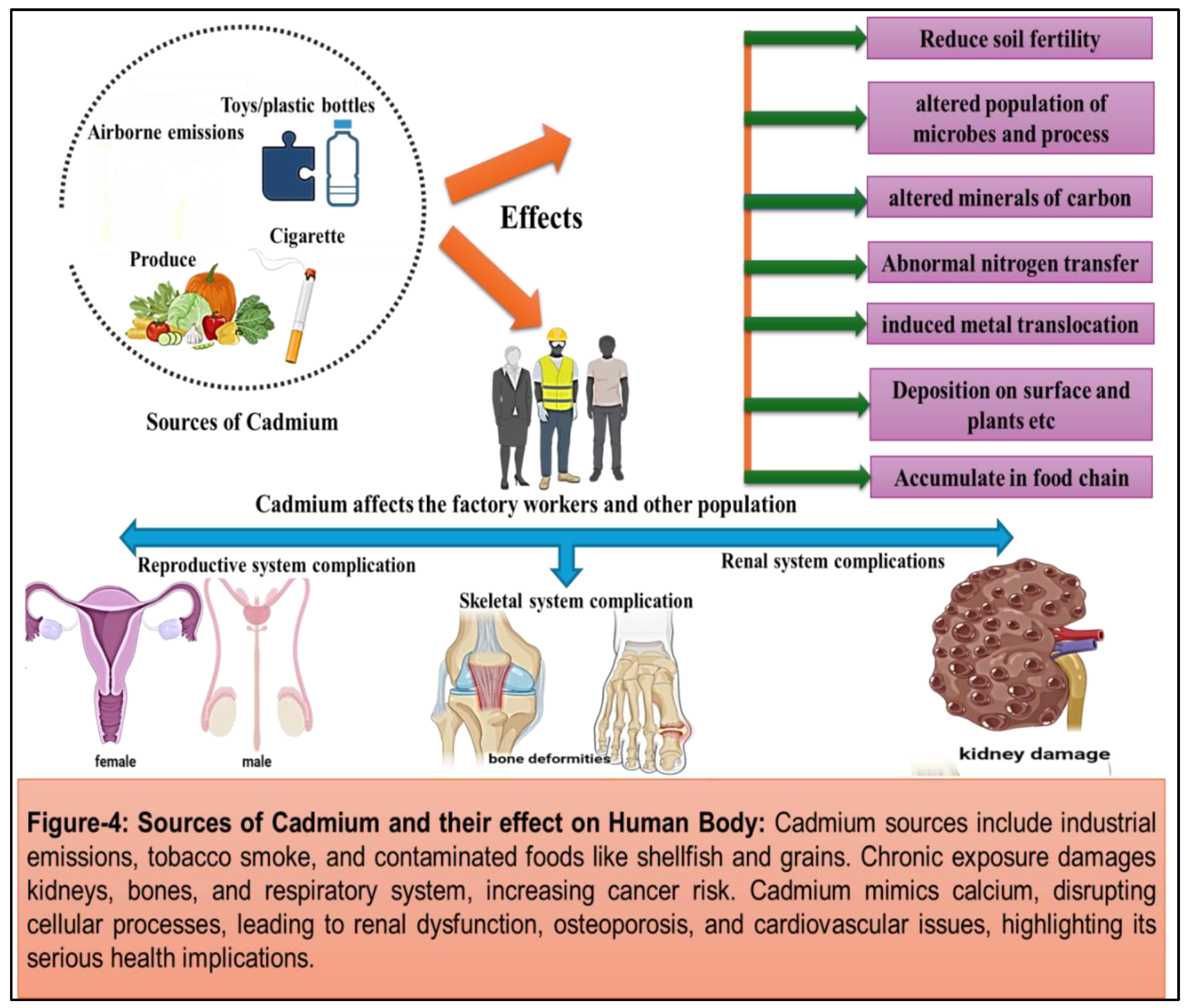
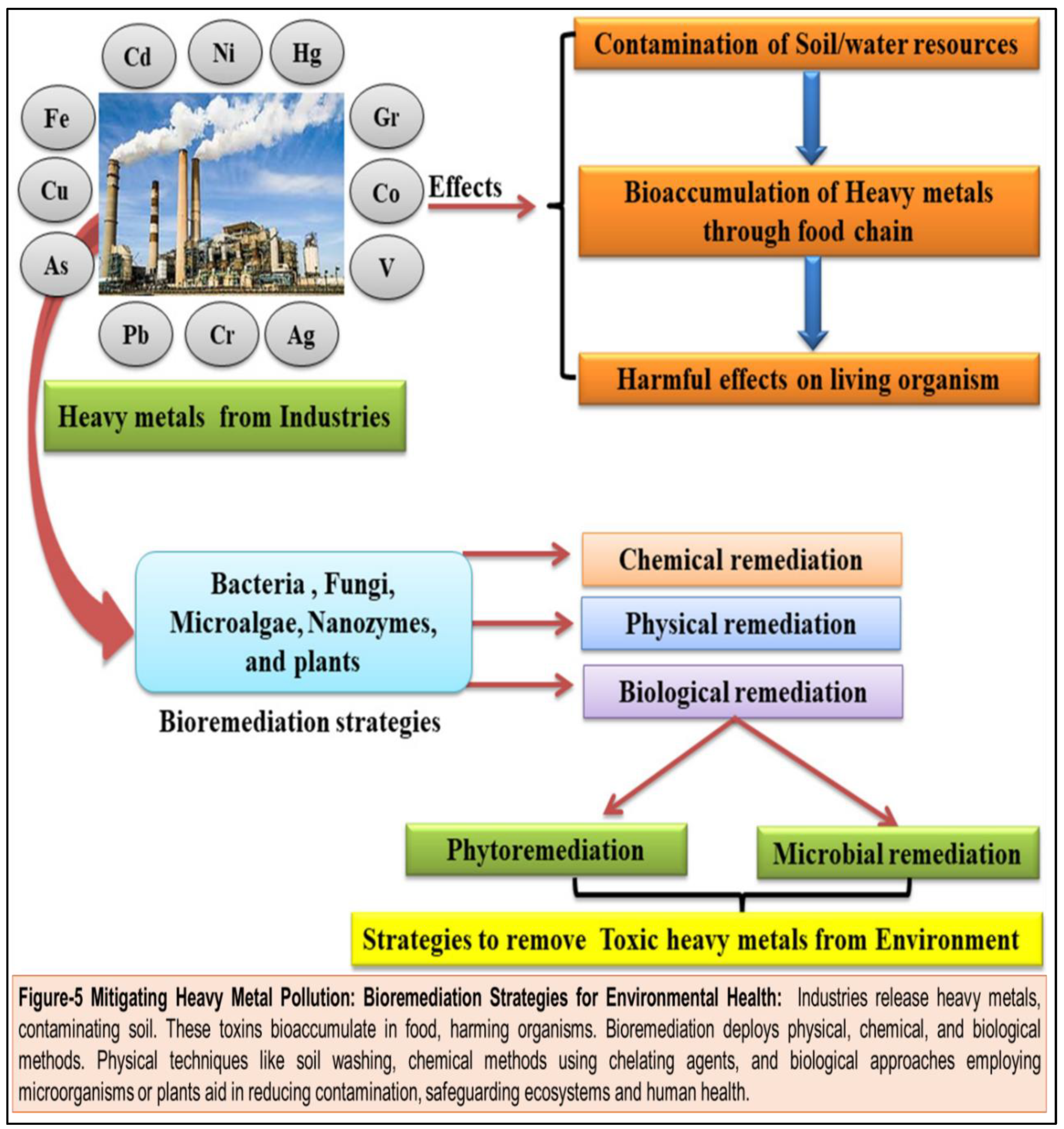
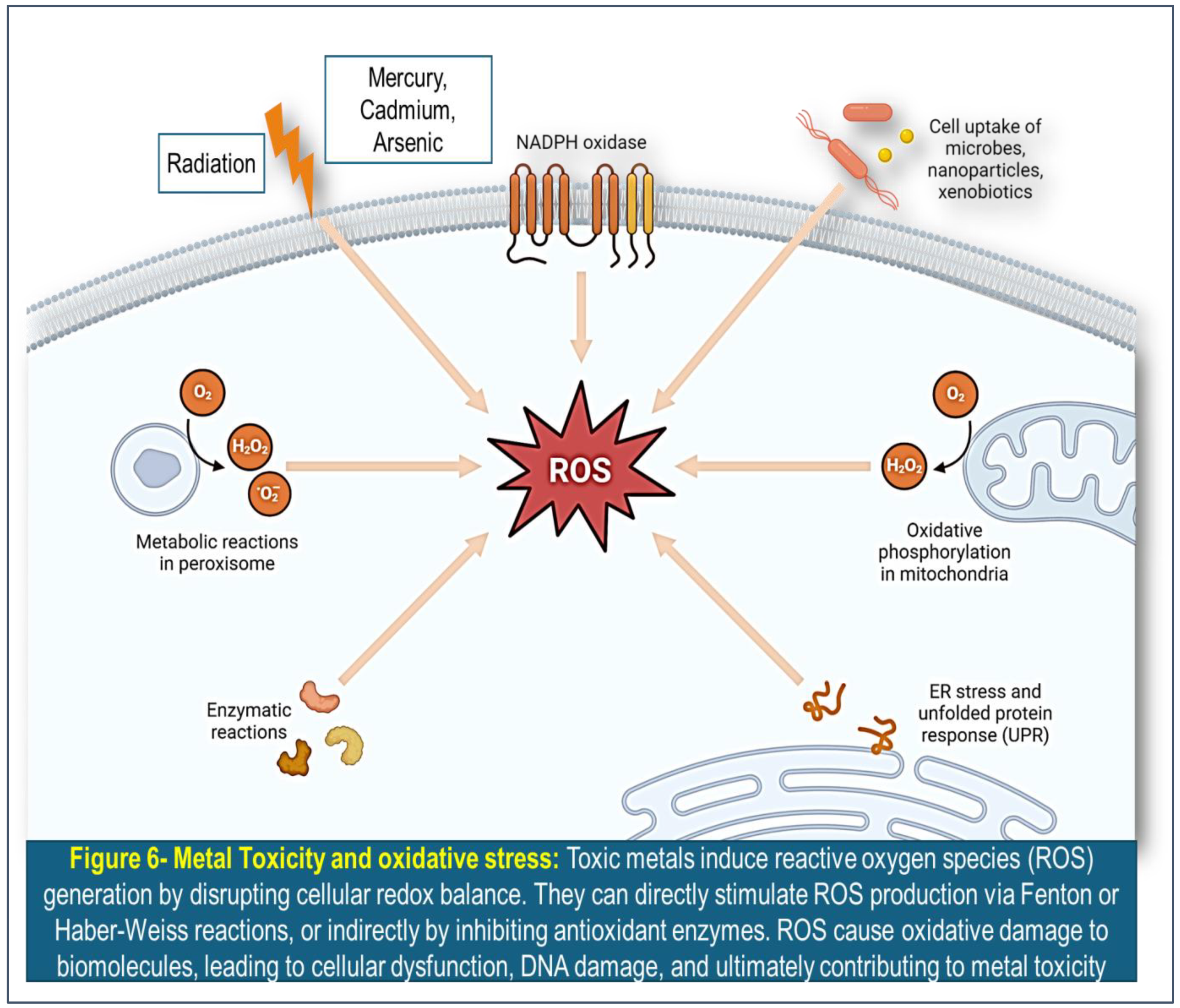
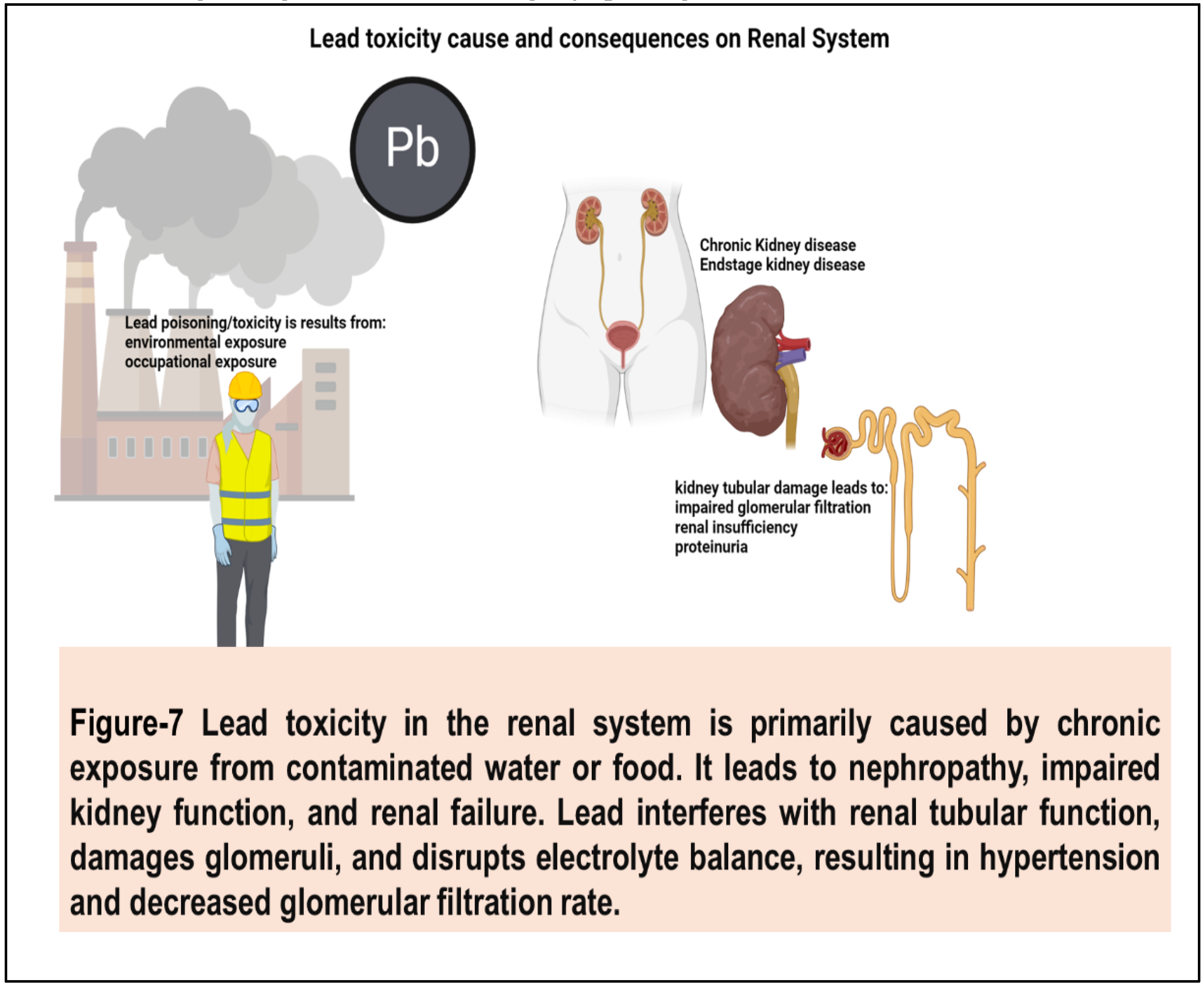
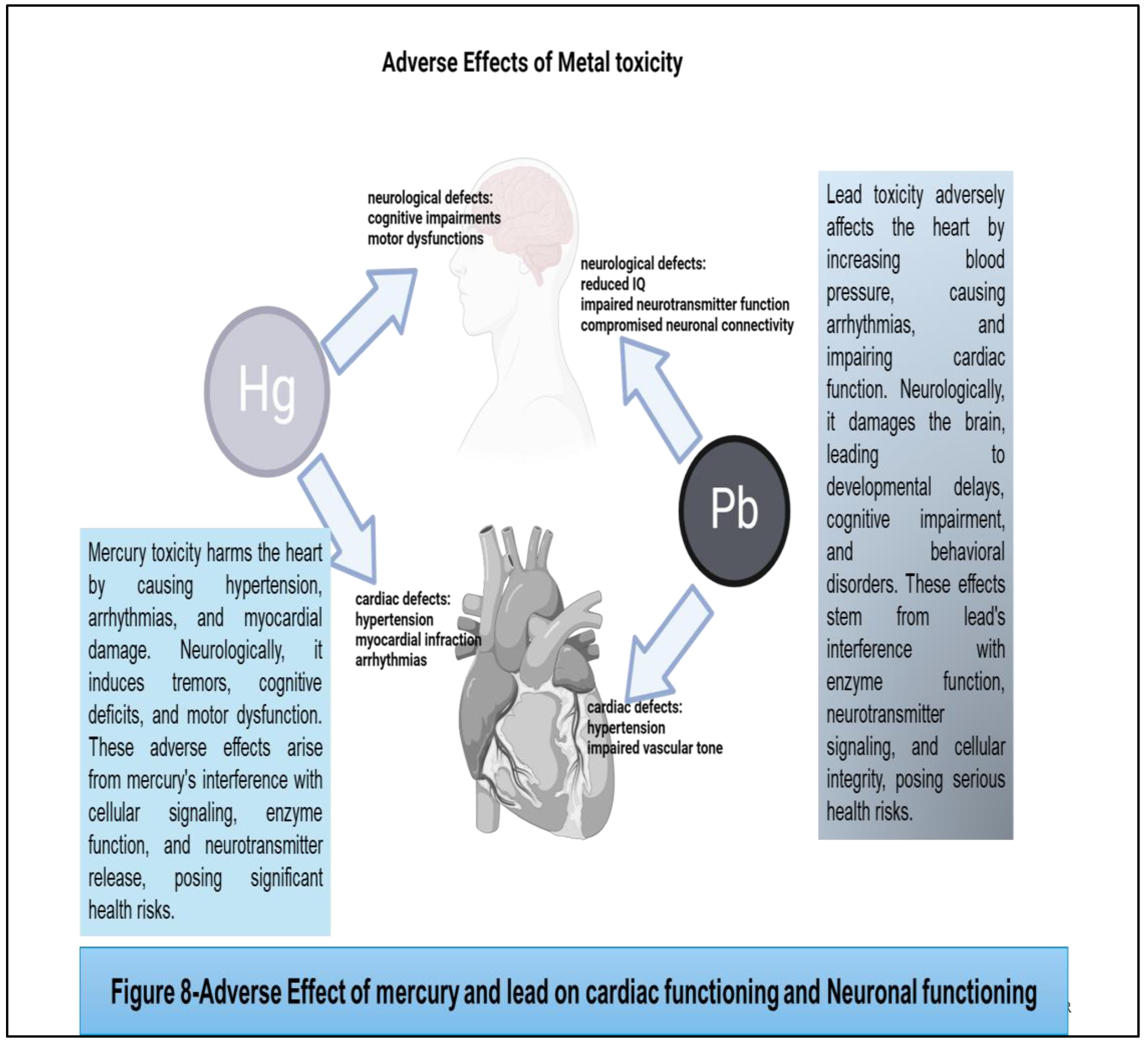
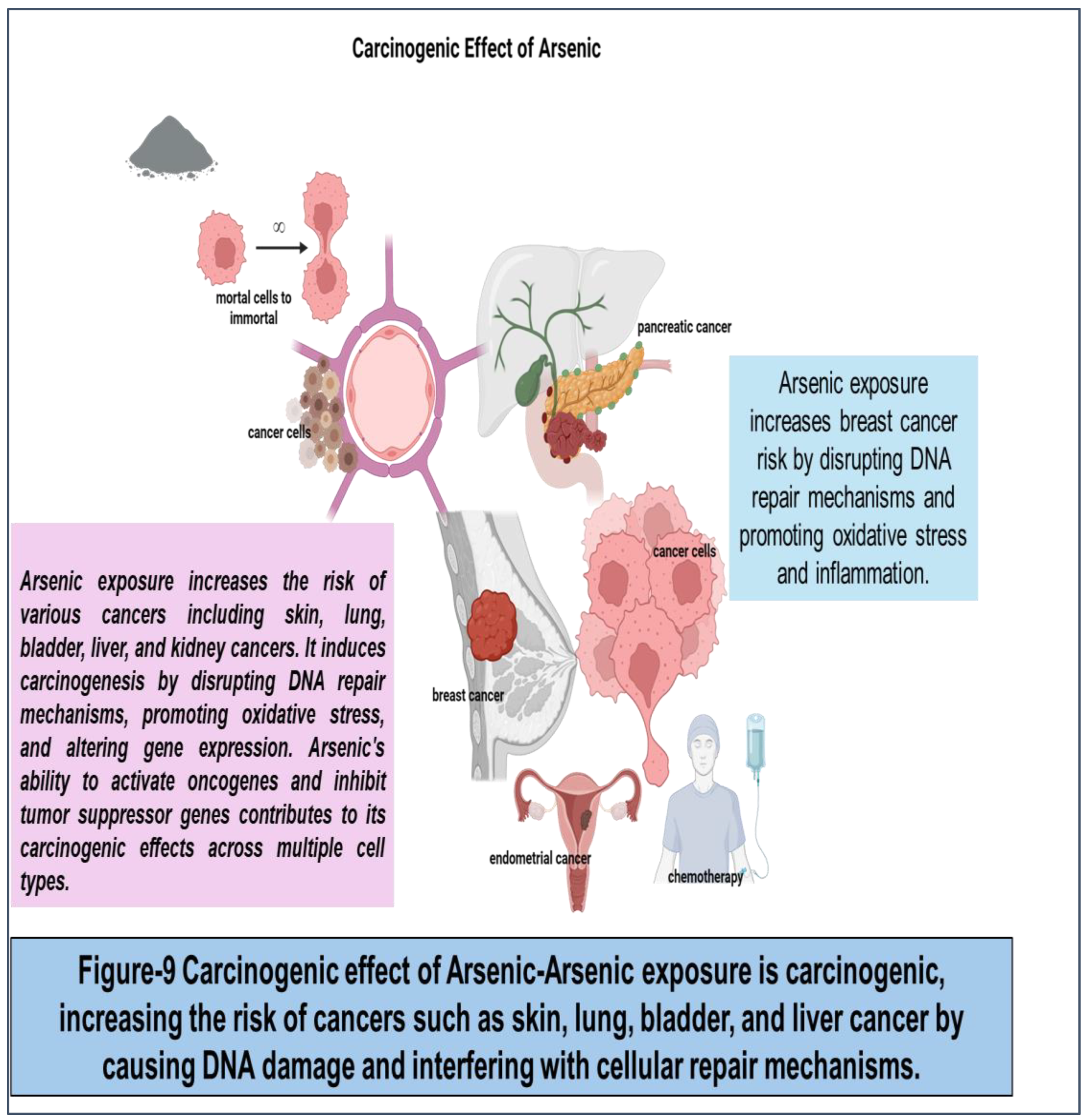
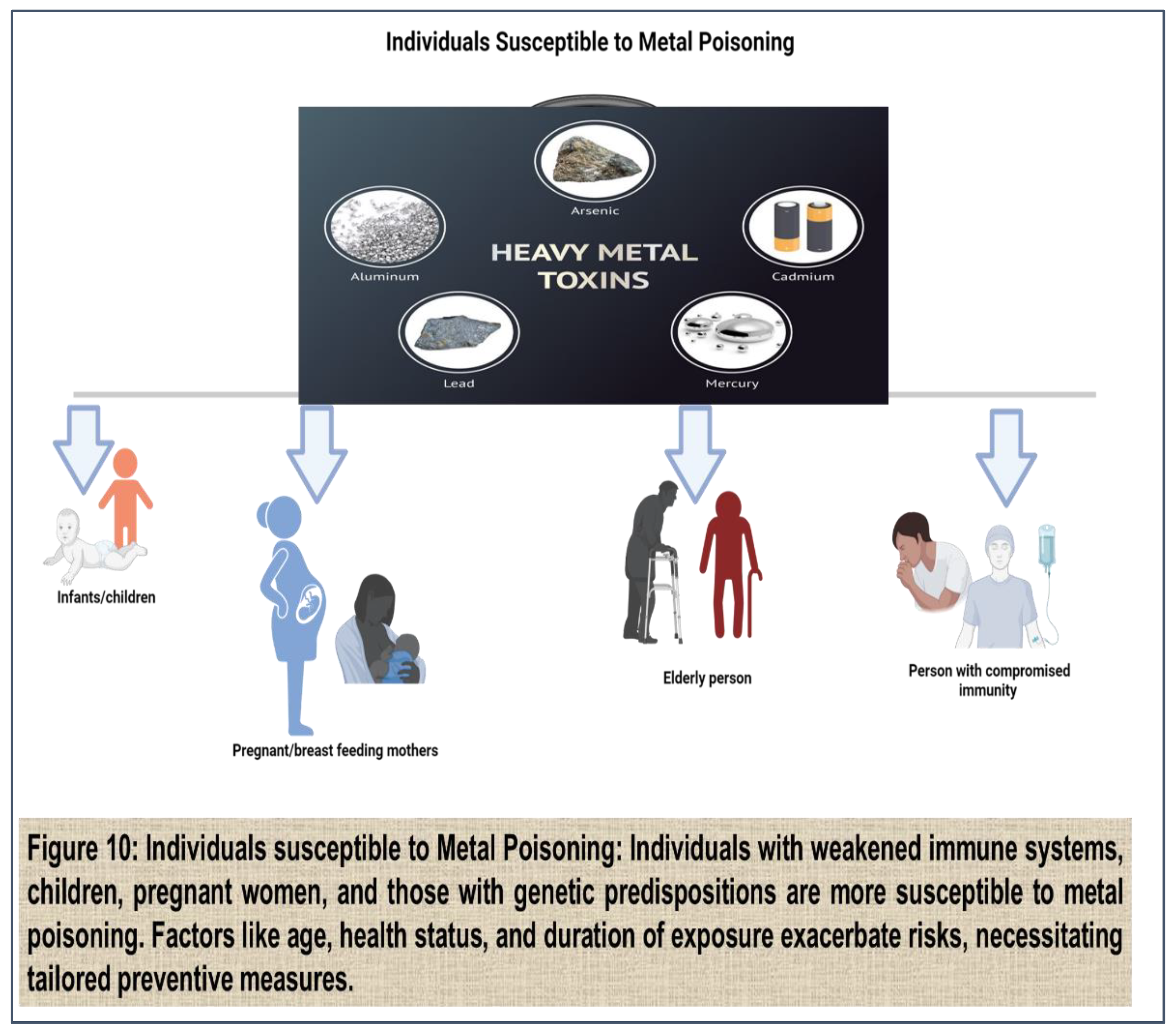
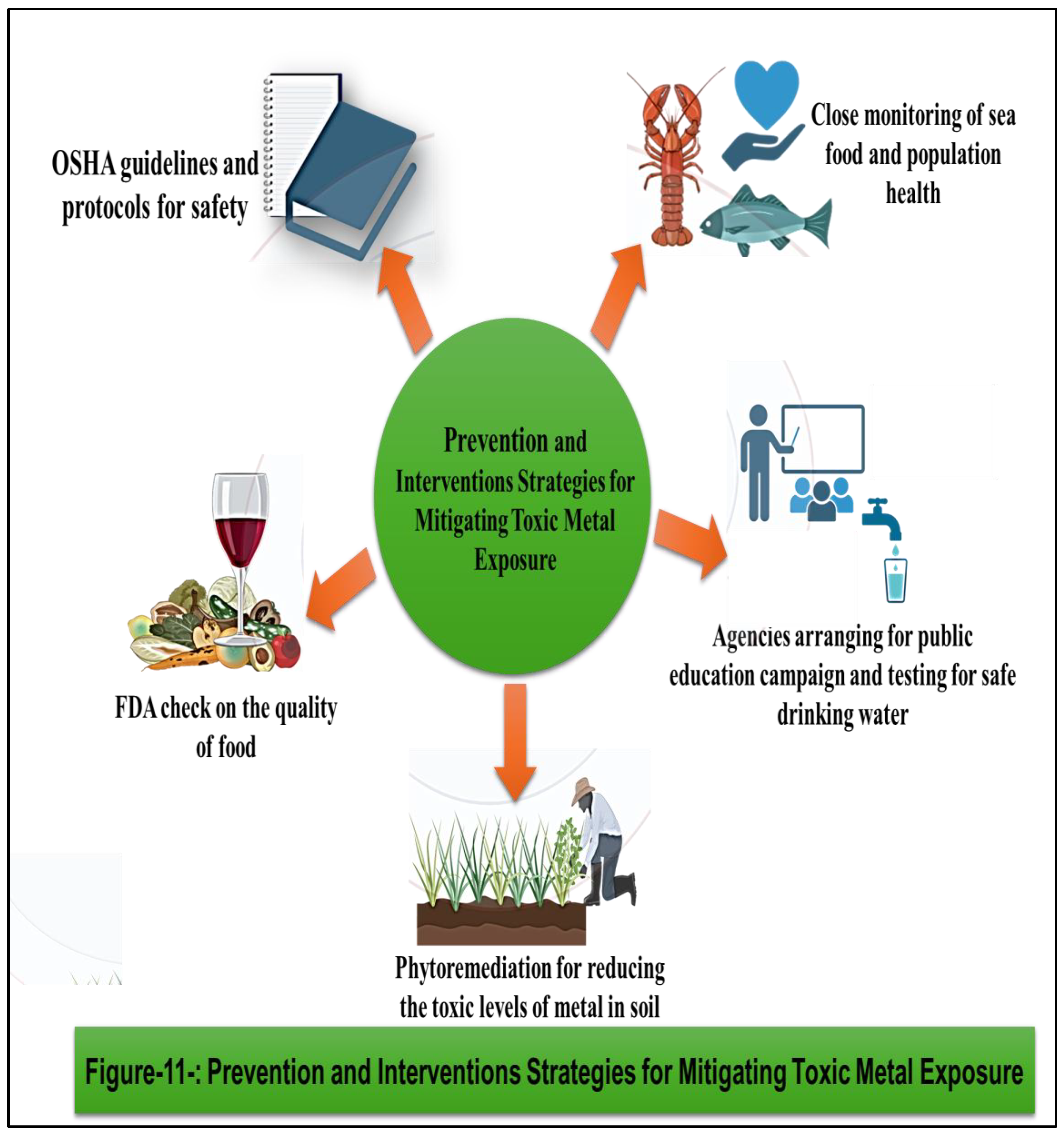
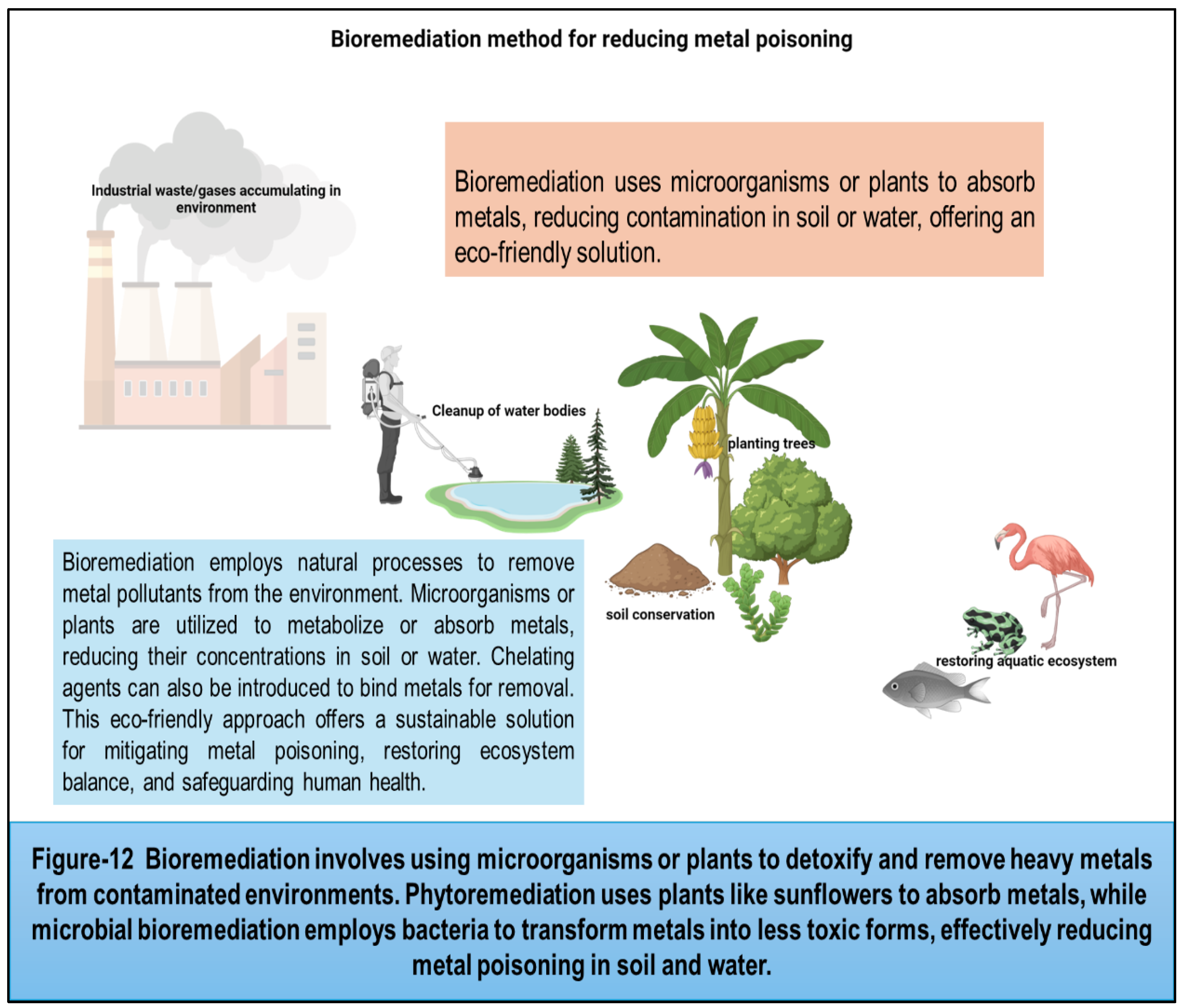
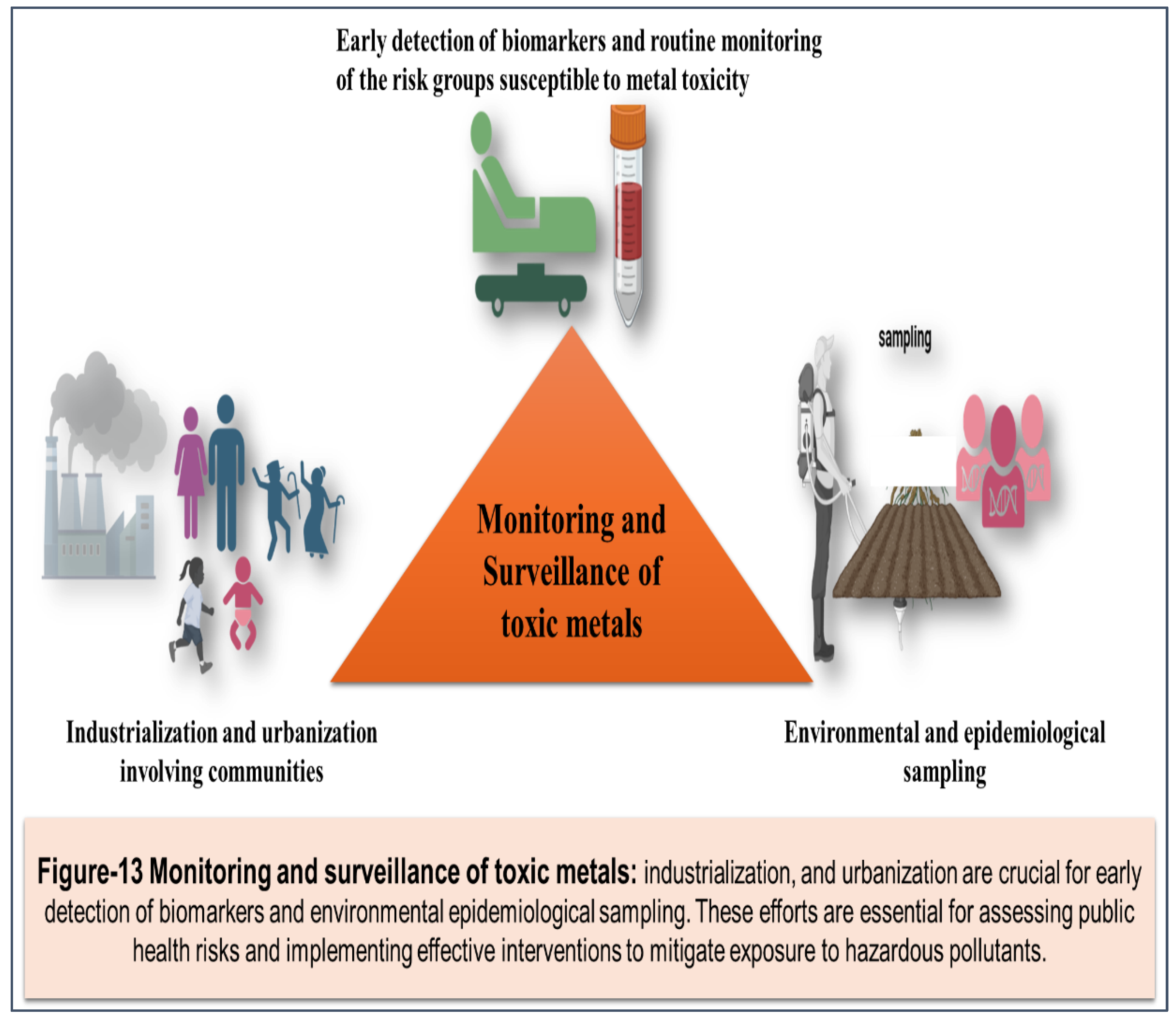
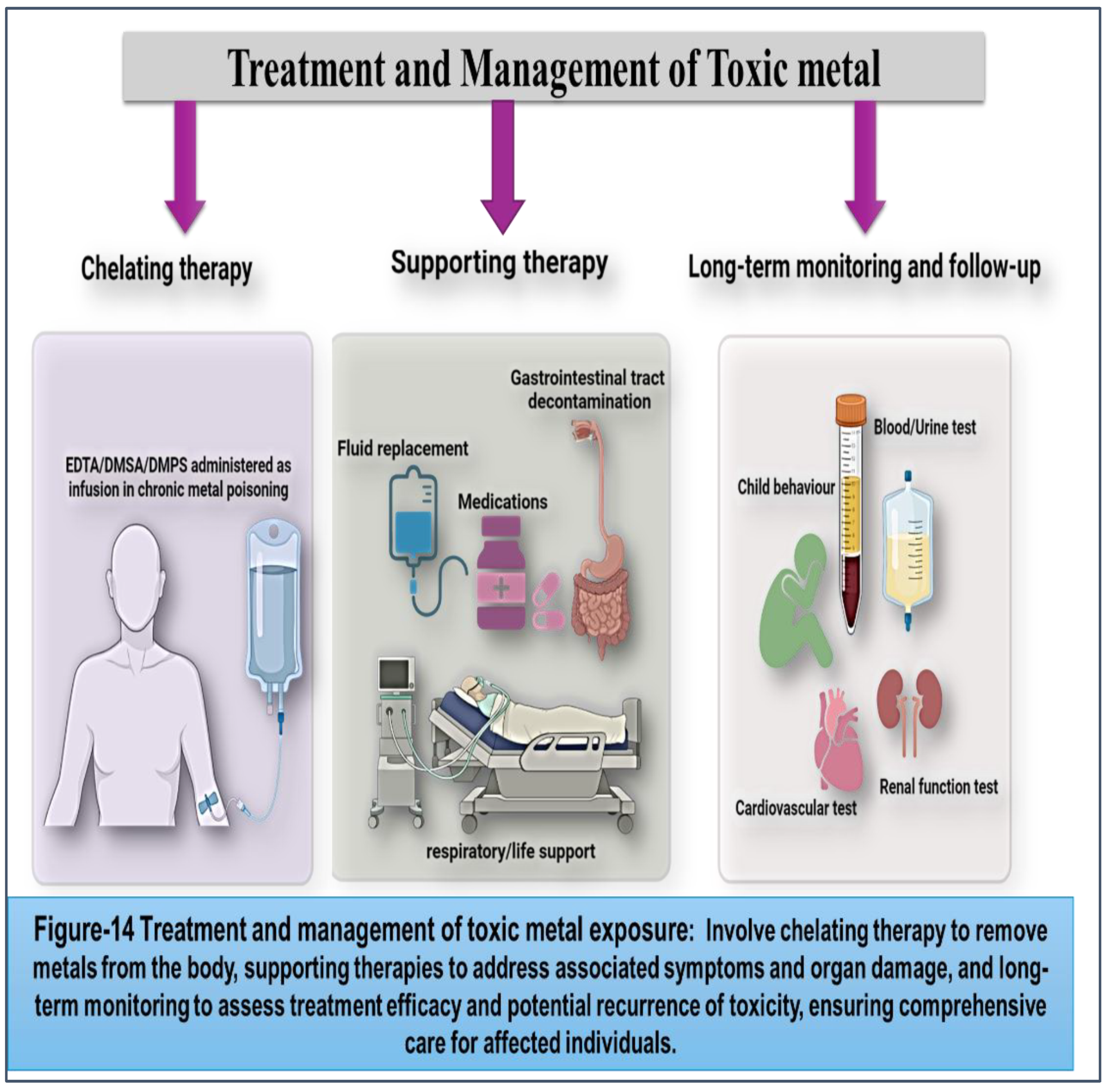
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



