
Submitted:
31 December 2024
Posted:
03 January 2025
You are already at the latest version
Abstract
Type 2 diabetes mellitus (T2DM) is a common, lifelong metabolic disorder. Adults with T2DM bear a greater burden of cardiometabolic risk factors than the general popula-tion. T2DM presents as a spectrum of clinical manifestations, where uncontrolled dia-betes leads to progressive or irreparable damage to various organs. Neurologic end-organ damage due to uncontrolled diabetes may include neuropathy, nephropa-thy, and retinopathy. T2DM can be categorized into three levels: (1) prediabetes, with a blood sugar level between 110 and 125 mg/dL, (2) T2DM, with a blood sugar level higher than 126 mg/dL, and (3) uncontrolled T2DM, with a blood sugar level exceeding 180 mg/dL despite multiple medications. If blood sugar remains consistently high in level 1, it may cause pathological and functional changes in healthy vascular tissues and various systems, often without noticeable clinical symptoms. However, the latter two levels are important for identifying individuals at high risk of nerve damage, kid-ney damage, and cardiovascular (CV) events. Research shows that reducing modifia-ble risk factors can help prevent the progression from prediabetes to T2DM, while an-tidiabetic drugs can help prevent long-term complications of hyperglycemia in indi-viduals with T2DM. Considerable effort is being made to increase diabetes awareness and develop new pharmacological interventions to better treat the underlying causes of T2DM. This review provides a comprehensive overview of current knowledge in common genetic variants and novel targets for potential therapeutic use in T2DM and discusses recent advances in the pharmaceutical management of uncontrolled T2DM, including those currently in phase II and III development.
Keywords:
diabetes mellitus
; etiology
; genetics
; treatment
; inflammation
; new targets
1. Introduction
Metabolic mechanisms are a complex network of biochemical reactions that ensure proper nutrition consumption, energy production, and energy balance within a range that optimizes the structural integrity and function of cells, tissues, and the organism [1,2]. The hepatopancreatic unit plays a fundamental role in adjusting metabolism and the flow of energy across various tissues, activating complex regulatory genes, cells, and mediators to achieve this balance (Figure 1). A similar level of dynamic complexity is observed across vertebrates in order to coordinate the diverse cell types and functions. Consequently, metabolic networks are highly interconnected to sustain homeostasis [3].
An individual's metabolism, which consists of life-sustaining biochemical reactions, is influenced by genetic factors to maintain an evolutionarily stable strategy. Accumulating evidence demonstrates that factors such as age, nutrition, physical activity, and environmental influences impact an individual's metabolic processes [4,5,6,7]. Thus, the set point for metabolism is molded not only by genetic factors but also by extrinsic variables [8,9].
Glucose, the body's primary source of energy, is tightly regulated. While normal fasting blood glucose levels typically range between 70 and 80 mg/dL in most individuals, there is considerable variability in glucose levels even among healthy people. This biological variation is largely genetically determined. In general, when glucose disturbances are mild, the glucose homeostatic system helps resolve these perturbations, maintaining glucose levels within a narrow range to meet the body's needs [10]. However, when the disturbance in glucose homeostasis is significant and sustained, the homeostatic response may develop into a pathological process, resulting in abnormal glucose accumulation. Over time, this can lead to insulin resistance, insulin deficiency, and ultimately T2DM.
We conducted an electronic search in October 2024 using PubMed, Medline, U.S. Food and Drug Administration (FDA, fda.gov), ClinicalTrials.gov, and Scopus databases, with keywords and MeSH (medical subject headings) terms such as genetic polymorphisms in DNA coding regions and the prevalence of specific polymorphisms across different ethnic groups.
This review aims to summarize current knowledge on the gene and the most common epigenetic variants and their relationship to diabetes risk and prevention, particularly among patients with uncontrolled diabetes. Additionally, it outlines newly approved therapies, and those under investigation (Phase 2 and Phase 3) as novel options for treating T2DM. Although high proportion of individuals with T2DM is on treamtent for their condition, only a small fraction of T2DM patients achieve glycemic control with existing treatments, making uncontrolled T2DM a major clinical isuue. Therefore, new treatment strategies are urgently needed to prevent serious complications and reduce the need for hospitalization.
2. Definition of Uncontrolled T2DM
Plasma glycosylated hemoglobin A1C (HbA1C) levels serve as a key indicator of long-term blood glucose control [11], playing a central role in both diagnosis [12] and monitoring of individuals with diabetes. According to the American Diabetes Association (ADA) [13], the American College of Physicians (ACP) [14], the Association of Clinical Endocrinologists [15], the American College of Endocrinology [16], and the World Health Organization (WHO), uncontrolled diabetes is defined as chronic hyperglycemia, with HbA1C levels exceeding 7.9%.
3. Heterogeneity of Uncontrolled T2DM
T2DM is a polygenic disorder [17,18], with multiple genetic risk alleles contributing to an individual’s susceptibility [19]. While hundreds of genomic sites are associated with an increased risk of T2DM, only a small fraction are located in protein-coding regions of DNA. Interestingly, many polymorphisms identified through genome-wide association studies (GWAS) are found in noncoding regions, which often play a significant role in human diseases [20]. In contrast, rare familial forms of diabetes, caused by mutations in a single gene (monogenic diabetes), can lead to hyperglycemia and a diabetic phenotype due to alterations in protein sequences [21].
T2DM arises from a complex interaction between genetic and environmental factors [22]. Risk factors such as poor diet, lack of physical activity, and surprisingly noise and air pollution [23,24,25] contribute significantly to its onset. Genetic factors account for approximately 20% to 80% of the population's risk for T2DM [26].
Monogenic forms of diabetes, which are caused by mutations in a single gene [27,28], include conditions such as neonatal diabetes [29], maternally inherited diabetes with deafness [30,31], and syndromic forms like Bardet-Biedl syndrome and Wolfram syndrome [32,33]. Below, we summariz the key findings on T2DM-associated monogenic genes that influence insulin secretion, inflammation, and insulin sensitivity, which are emerging as key targets for developing novel antidiabetic therapies.
Among the T2DM-associated monogenic genes, we explore the preproinsulin gene, mutations of which can lead to hyperinsulinemia, hyperproinsulinemia, and neonatal diabetes mellitus. This review focuses on specific gene variants such as PPARγ, TCF7L2, KCNJ11, HNF4α, p.Arg114Trp, GLIS3, and LEP, as these variants represent strong candidates because of their roles in insulin regulation and insulin signaling. They are well-supported by replication studies and play significant roles in pancreatic beta-cell function and energy metabolism in the context of T2DM pathogenesis (Table 1). Moreover, these genes endode proteins that are the recent emerging targets that already in the focus for developing new therapies in the treatment of uncontrolled diabetes.
3.1. Peroxisome Proliferator-Activated Receptor Gamma (PPARγ)
PPARs (PPARα, PPARγ, PPARβ) belong to the nuclear hormone receptor superfamily of ligand-activated transcription factors [48]. PPARα is predominantly expressed in adipose tissue [49] and plays a crucial role in regulating adipocyte differentiation [50], free fatty acid uptake, and storage. PPARγ is highly expressed in monocytes and macrophages, where it inhibits inflammatory responses by modulating the nuclear factor-κB (NF-κB) signaling pathway [50,51,52]. In addition to its anti-inflammatory functions, PPARγ activation is essential for macrophage differentiation, polarization, and lipid metabolism [50].
PPARγ regulates glucose homeostasis [50]. PPARγ agonists have been shown to reduce fibrosis in organs like the pancreas and liver [53], which play a crucial role in regulating the rate of glucose metabolism and controlling glucose homeostasis. Deficiencies in PPARγ and leptin are associated with metabolic syndrome, characterized by dyslipidemia, renal hypertrophy, and elevated levels of the profibrotic cytokine transforming growth factor beta (TGFβ) in the kidneys [54]. Notably, studies have demonstrated that deletion of the PPARγ gene in the epiblast of mice leads to the development of T2DM and renal fibrosis [55]. Similarly, macrophage-specific deletion of PPARγ results in lupus-like autoimmune glomerulonephritis [56], emphasizing the critical role of PPARγ in inflammation. Inflammation, reactive oxygen species, and diabetes have a bi-directional relationship [57].
Several studies have extensively examined the role of PPARγ [55,58,59,60]. Disease-associated mutations in PPARγ can result in either complete or partial loss of function [61], depending on their impact on the residual activity of the encoded mutant PPARγ. Variants in the PPARγ gene have been linked to severe obesity [60], insulin resistance [61], a decreased risk of T2DM in certain ancestries [62] or increased risk of T2DM [45], hypercholesterolemia [63], and systemic sclerosis characterized by diffuse fibrosis and vascular abnormalities [64]. Taken together, these studies provide irrefutable evidence of the pathogenicity of several common PPARγ variants when inherited and their influences on glycemic physiology.
3.2. Maturity-Onset Diabetes of the Young (MODY)
Maturity-Onset Diabetes of the Young (MODY) is a heterogeneous genetic disorder caused by mutations in genes involved in beta-cell dysfunction, leading to insulin deficiency [65,66]. MODY can be classified into at least 14 various types based on clinical presentation, two of which will be discussed here. MODY 1 and MODY 13 are associated with increased risk of T2DM in several studies and large-scale meta-analyses [67,68,69].
MODY is characterized by inherited beta-cell dysfunction, leading to reduced insulin secretion and elevated blood glucose levels. The severity of hyperglycemia and beta-cell dysfunction varies depending on the type of MODY. The global prevalence of MODY is estimated to range from 1-5% of diabetic patients [70], with a mutation carrier rate of approximately 1-5 in 10,000 individuals in the general population.
3.2.1. HNF4α and Its Role in Diabetes
Obesity and hyperinsulinemia are observed in MODY 1 [71]. The most common causes of MODY are mutations in hepatocyte nuclear factor 4-α (HNF4α, p.Arg114Trp) [72,73] with reduced penetrance [39,40], which exhibits autosomal dominant inheritance. HNF4α regulates hepatic genes [38]. HNF4α (p.Arg114Trp) is characterized by pancreatic β-cell dysfunction. Evidence suggests that HNF4α regulates glucose transport and metabolism [74]. Mutations in HNF4α are generally associated with a progressive decline in pancreatic beta cell function and a vascular risk profile similar to that of T2DM [75]. However, the individuals with MODY do not have either ketoacidosis or pancreatic autoantibodies. They are nonobese individuals who have diabetes at young age, but it can occur at any age. Mutations in HNF4α are the most common cause of MODY in the European countries [76]. Notably, HNF4α variants do not appear to contribute significantly in the European American population [40]. HNF4α (p.Arg114Trp) variant is associated with an approximate eight-fold increased T2DM risk in T2DM genome-wide association studies [77]. These patients with this disease should receive a stronger β cell-preserving therapy.
3.2.2. KCNJ11 and Its Role in Diabetes
KCNJ11 is a member of the potassium channel genes [41]. The protein encoded by KCNJ11 is an inward-rectifying channel (Kir6.2), which is characterized by allowing the efflux of potassium into the cell [78]. The elevation of cytosolic potassium levels depolarizes the cell membrane and subsequently activates calcium ion channel, leading to the elevation of calcium levels. Increased intracellular free calcium levels are essential for insulin secretion from pancreatic β-cells [79]. These calcium channels trigger the voltage-dependent potassium channels to repolarize the cell membrane. Kir 6.2 protein (consists of 4 subunits) is controlled by G-protein and is associated with the sulfonylurea receptor (made of 4 subunits) encoded by the ABCC8 gene [35]. Kir6.2 is implicated in the regulation of cellular metabolism and contribute to the mechanisms by which hypoglycemia stimulates glucagon release from pancreatic α-cells. Several reviews can provide the readers with a more detailed understanding of the structure, function, and regulation of potassium inward-rectifying channel superfamily [41,78,80].
Mutations in KCNJ11 typically occur de novo during gametogenesis or embryogenesis [81]. While genome-wide association studies on KCNJ11 gene have identified over 180 single nucleotide polymorphisms (SNPs) [82,83], three of which are located in the coding regions and are associated with increased risk of diabetes [41]. These three SNPs include rs5215, rs5218, and rs5219 [42], which will be discussed here.
KCNJ11 rs5218 variant is associated with the pathogenesis of T2DM, whereas rs5215 and rs5219 are found in individuals with T1DM, T2DM. The KCNJ11 gene variant (rs5219) is strongly related to the levels of the circulating HbA1c in this disease [84] and can cause transient neonatal diabetes or permanent neonatal diabetes. Both rs5215 and rs5219 polymorphism were associated with blood pressure levels among patients with T2DM [85,86,87]. The correlation between rs5219 in patients with T2DM and the medication response is controversial. KCNJ11 rs5219 gene polymorphism also is found to be implicated in gestational diabetes mellitus in people in China [88] but not in individuals from Sweden [89,90]. These studies suggest that background polygenic risk in the population in China differ greatly with respect to disease prevalence and incidence. A meta-analysis showed that the KCNJ11 rs5219 polymorphism is a risk factor for developing T2DM in Caucasians and in populations from East Asia [91], and an independent predictor of T2DM in the Iraqi population in the Middle East [92]. Another study provides no evidence supporting a relationship between rs5219 and the risk of diabetes in Iranian [93]. The lack of association could potentially be due to the absence of other environmental elements such as obesity [94] and hypertension [85]. Rs5219 is found to be associated with several diseases including hyperinsulinemic hypoglycemia [95], familial 2 [82], and MODY 13.
The role of rs5219 in medication response remains contentious. While the KCNJ11 gene polymorphism (rs5219) is associated with hepatitis insulin sensitivity [96], it is not associated with diabetic peripheral neuropathy [97]. Several studies provide evidence that the diabetic patients with KCNJ11 rs5219 variant are susceptible to metformin therapy [98], metformin and sulfonylurea combination therapy [99], metformin and gliclazide therapy [100] in different ethnic groups [98]. Patients with KCNJ11 gene polymorphism (rs5219) are more responsive to glimepiride and glibenclamide than those being treated with gliclazide [84]. However, another study indicates that patients with rs5219 variant exhibit the impairment of glibenclamide-induced insulin release, highlighting an example of pharmacogenetics in T2DM [101].
These findings highlight the importance of genetic variability in drug response, underscoring the potential for personalized treatment strategies to reduce healthcare disparities and enhance precision medicine.
3.2.3. GLIS3 and Its Role in Diabetes
Gli-similar 3 (GIS3), a key transcription factor in insulin production, is a compensatory β-cell proliferation in adults [102,103,104]. GLIS family of proteins (GLIS 1, GLIS 2, GLIS 3) carry significant role in the regulation of a number of physiological processes [105,106]. Mutations in GLIS proteins have been implicated in several pathologies such as neonatal diabetes mellitus, congenital hypothyroidism, congenital glaucoma, and cystic kidneys [107,108].
Defective GLIS3 results in impaired insulin function, which may arise abnormal pancreatic development [109], dysfunctional β-cells, or β-cell destruction [105,108,110]. In vitro deficiency of GLIS3 in β-cells triggers the activation of the intrinsic pathway of apoptosis [111], thereby susceptibility to diabetes. Individuals with P/LP GLIS3 variants are associated with increased T2DM risk [37]. Rare missense mutations in GLIS3 are linked to elevated HbA1c levels and an increased risk of T2DM [112]. GLIS3 rs10758593 variant is associated with T2DM in an Egyptian population [36]. Polymorphism of the GLIS3 gene is found to be associated with the development of MODY in a Russian population sample [113].
Given its role in insulin production and β-cell function, GLIS3 is emerging as a potential therapeutic target. Inhibiting the apoptotic effects of GLIS3 could help reduce complications from neonatal diabetes and improve β-cell function, making it a promising avenue for future T2DM treatments.
3.3. LEP Variant and Its Role in T2DM and Obesity
While the genetic causes of T2DM remain complex, certain rare genetic variants have been identified that increase the risk of developing the disease. A recent study identified a rare enhancer variant near the LEP gene (rs147287548), particularly prevalent in African and African American populations, which increases the risk of diabetes by four-fold [43]. The LEP gene encodes leptin, a hormone primarily produced by adipose tissue that regulates body weight. Leptin levels are positively correlated with body mass index (BMI) and fat mass [114].
Diet in high fat, carbohydrate, fructose, and low in protein reduce leptin secretion, known as leptin resistance [115]. A high-protein diet triggers sustained reduction in appetite and reduced plasma leptin [116]. Congenital leptin deficiency is associated with excessive hunger and weight gain, while increased leptin levels are linked to T2DM [117]. Interestingly, recombinant leptin treatment in children with leptin deficiency has shown a sustained reduction in body weight, particularly through fat loss [118]. These findings underscore the role of leptin in body weight regulation and highlight its potential as a therapeutic target for obesity and T2DM.
3.4. OPG Gene
Recent genetic evidence indicates that monogenic rare variants and SNPs are responsible for susceptibility to high blood pressure via alterations in the components of renin-angiotensin system, including natriuretic peptides, the sympathetic neuronal system, endothelial dysfunction, and inflammation [119,120]. Notably, 50% of people with insulin resistance are susceptible to develop hypertension, in the early phase of the disease [121,122]. This suggests that insulin resistance leads to genetic and epigenetic perturbations that results in hypertension. Both diabetes and hypertension are recognized as the major risk factors for CV disease [123], and have substantial overlap in the CV disease complications, including atherosclerosis, dyslipidemia, and obesity (Figure 2). Needless to say, prevalence of diabetes associated complications varies among different ethnic population [124], leading to the notion that disparities in the variant allele frequencies among different ethnic regions may play a role in disease susceptibility [125].
Vascular calcification, an age related phenomenon, is common to both diabetes [126] and hypertension [127]. The intimal calcification not only contributes to a reduction in vascular compliance [127] but also is linked to vessel stiffness. Arterial stiffening, a hallmark of atherosclerosis, is a known pathophysiological mechanism of hypertension [128]. Although the underlying mechanisms of diabetes-induced atherosclerosis remain a dilemma, higher levels of arterial calcification are observed in patients with diabetes at the clinical and pathological level [129]. Osteoprotegerin (OPG), a biomarker of vascular calcification, is a decoy receptor for receptor-activator for NF-κB ligand (RANKL), which has been implicated in pathophysiology of vascular calcification [126]. OPG is also found to be associated with myocardial stiffness [130], hypertension, and diabetes [47,131,132]. Recent genetic evidence indicates that CV risks are higher in T2DM patients with hypertensions expressing OPG rs2073618 gene polymorphism [47] (Table 1).
In conclusion, T2DM is influenced by a complex interplay between genetic predisposition and epigenetic factors.
4. Diabetes Inheritance and Personalized Treatment Approaches
4.1. Current Treatment Guidelines for Diabetes
The ADA recommends a stepwise approach for managing diabetes, with metformin as the first-line treatment, followed by other agents like sulfonylureas, glucagon-like peptide-1 (GLP-1) receptor agonists, or sodium-glucose co-transporter-2 (SGLT2) inhibitors (Figure 2). These guidelines emphasize individual patient factors such as CV, kidney, and liver health, along with comorbidities, preferences, and risk of hypoglycemia [133].
However, emerging data suggest that this "one-size-fits-all" approach may not be effective for all patients. Diabetes is a multifactorial disease, with endothelial dysfunction, inflammation, oxidative stress, insulin resistance, and chronic hyperglycemia-induced coagulation [134] and fibrinolysis impairment [135] all contributing to thrombotic diseases in T2DM patients [57,136,137] . Genetic variability, particularly in different ethnic groups, can significantly influence drug efficacy, often leading to suboptimal outcomes.
4.2. Genetic Variability and Ethnic Differences in Drug Response
Genetic differences influence responses to common antidiabetic medications [138]. For example, the PPARγ gene, a susceptibility locus for T2DM [139], is also the molecular target of thiazolidinediones [140]. Similarly, KCNJ11, which encodes a potassium channel involved in insulin secretion, is a target for sulfonylureas, with genetic variation influencing medication responses, as seen in changes to fasting glucose and HbA1c levels [140]. Furthermore, TCF7L2 polymorphisms have been associated with insulin secretion and response to GLP-1 receptor agonists and sulfonylureas [140,141].
Additionally, SLC2A2 gene, encodes the facilitated glucose transporter GLUT2, variations affect hepatic metformin uptake, influencing its therapeutic effectiveness [142]. It is suggested that SLC2A2 rs8192675 can serve as a potential biomarker for stratified medicine [142]. Research also shows that African Americans exhibit a stronger glycemic response to metformin compared to European Americans [143].
The implications of these findings are significant. Integrating pharmacogenomic testing into diabetes care could pave the way for personalized treatment strategies that maximize efficacy and minimize adverse effects. Developing genotype-guided treatment protocols, supported by evidence from diverse, large-scale studies, could transform diabetes care into a precision medicine framework. Such an approach not only has the potential to improve individual outcomes but also to address disparities in treatment effectiveness across different population groups, promoting equity in healthcare delivery.
5. Obesity and Its Association with Insulin Resistance
Obesity is a medical condition characterized by the excessive accumulation of body fat, which poses significant health risks, including reduced life expectancy and an increased incidence of various diseases [144]. The most common measure of obesity is BMI, which classifies individuals based on their weight relative to height. According to the WHO, a BMI of 25 or higher is classified as overweight, and a BMI of 30 or higher is considered obese. The prevalence of overweight and obesity has been steadily increasing in both children and adults from 1990 to 2022 [145].
Several factors contribute to obesity, including the consumption of energy-dense, nutrient-poor foods, poor eating habits, lack of physical activity, hormonal imbalances, genetic predisposition, and certain illnesses and medications [146,147]. As a highly complex condition, obesity involves multiple genetic loci and pathways that regulate energy balance, appetite, and metabolism. Among the most prominent complications of obesity are metabolic syndrome, stroke, osteoarthritis, and certain types of cancer (such as endometrial, colon, and gall bladder cancer) [148,149].
Unfortunately, most current treatments for obesity, including pharmacological agents, are associated with serious side effects and variable clinical outcomes [150].
Obesity is closely associated with insulin resistance [151], making it a significant risk factor for the development of T2DM. Genetic studies have identified several genes linked to both obesity and insulin resistance, such as Pro12Ala PPAR-γ, fat mass and obesity-associated (FTO), and retinol binding protein. Research has uncovered hundreds of genetic loci associated with obesity, revealing its heterogeneous nature across different populations. Variants in genes like FTO and melanortin-4 receptor (MC4R) have been consistently linked to BMI and fat distribution, highlighting the genetic underpinnings of obesity [152,153]. However, the interaction between genetic susceptibility and environmental factors like diet and physical activity is still not fully understood, leading to significant variability in obesity-related outcomes.
Importantly, many of the genetic loci implicated in obesity also overlap with pathways involved in glucose metabolism, suggesting a shared genetic foundation between obesity and metabolic disorders like T2DM. For example, FTO gene variants not only influence BMI but also affect insulin sensitivity and glucose regulation [152]. Similarly, MC4R polymorphisms, which are key regulators of appetite and energy expenditure, have been linked to impaired glycemic control alongside obesity [154]. These findings underscore the interrelated nature of genetic pathways governing both conditions, which can manifest differently depending on an individual's genetic profile and environmental influences.
5.1. Gene-Environment Interactions in Obesity
The heterogeneity observed in obesity can be further amplified by gene-environment interactions. For instance, the PPARγ gene, which plays a critical role in lipid metabolism and adipogenesis, exhibits variable effects on obesity risk depending on factors such as dietary fat intake [155]. Furthermore, epigenetic modifications, including DNA methylation and histone acetylation, regulate gene expression in response to environmental influences, contributing to obesity [156]. These epigenetic mechanisms also play a role in metabolic outcomes, highlighting the dynamic interplay between genetic predisposition and environmental factors in shaping the health risks associated with obesity.
These findings suggest that the heterogeneity of obesity is not determined by genetics alone but is also influenced by external factors, including diet and lifestyle. For example, transient hyperglycemia has been shown to induce p65 gene, a regulator of inflammation [157], expression in endothelial cells, which can persist for several days [158]. Additionally, obesity risk alleles, such as those in the FTO gene [159] and LEPR gene [160], are influenced by diet composition and physical activity levels [159].
5.2. Implications for Personalized Medicine and Obesity Management
Understanding the genetic heterogeneity of obesity has profound implications for both clinical practice and public health. Environmental factors can interact with genetically determined glucose homeostasis in genetically susceptible individuals, contributing to the development of obesity and diabetes. For instance, evidence suggests that hyperglycemia can activate genes that perpetuate endothelial dysfunction, a key feature of metabolic disorders [158]. By leveraging insights from genomic studies, clinicians can develop more targeted strategies for managing obesity and its associated complications, such as T2DM.
Genetic profiling could help identify individuals at higher risk for obesity-related metabolic disorders, allowing for earlier and more personalized interventions. Moreover, integrating genomic and epigenetic data into obesity research could offer new therapeutic targets and inform precision medicine approaches. This personalized approach could provide more effective treatments tailored to an individual’s genetic makeup and environmental exposure, ultimately improving health outcomes.
By addressing the genetic diversity of obesity, we can better understand the complex factors that contribute to its development and its association with metabolic diseases, such as T2DM. This understanding is critical for reducing the global burden of obesity-related diseases and improving overall health.
6. Need for New Treatments
Despite the availability of a variety of pharmacotherapies for glycemic control in T2DM, including biguanides, thiazolidinediones, and sulfonylureas, their major limitation is that they often tend to lose effectiveness after a few years. This suggests that T2DM management remains difficult and challenging, in part due to the genetic variability among patients. These genetic variants are key factors that influence disease susceptibility, response to therapy, and clinical outcomes. Other significant barriers to effective diabetes management include the side effects of current treatments, such as weight gain, hypoglycemia, fluid retention, and gastrointestinal discomfort.
The rising incidence of diabetes, coupled with the limitations of existing medications and their adverse effects, has driven the FDA to approve new antidiabetic drugs almost every year in recent years. This reflects a growing need for more effective, sustainable, and safer treatment options for T2DM (Table 2).
6.1. Novel Pharmacological Therapies in T2DM
Several novel pharmacological treatments have recently been developed and approved to improve the management of T2DM:
6.1.1. Brenzavvy (Bexagliflozin)
Brenzavvy is an FDA-approved oral SGLT2 inhibitor [161] designed for use in adult patients with T2DM to help improve blood sugar control alongside diet and exercise (Table 2). The kidneys play a crucial role in glucose homeostasis by reabsorbing glucose through the SGLT2 protein in the renal proximal convoluted tubules. Bexagliflozin reduces glucose reabsorption, lowers the renal threshold for glucose, and promotes urinary glucose excretion, significantly lowering blood sugar levels. It is particularly beneficial for T2DM patients with chronic kidney disease (CKD) [162] (eGFR between 30-60 mL/min/1.73 m²). In addition to improving glycemic control [162], brenzavvy also helps reduce CV and renal complications in these patients. However, common side effects include yeast infections, diabetic ketoacidosis, kidney or bladder infections, and increased urination (Table 2).
6.1.2. Tirzepatide
Tirzepatide is considered a novel medication recently approved for treating T2DM in the USA (Table 2). Tirzepatide is a synthetic polypeptide and acts as dual agonists for the GLP-1 and glucose-dependent insulinotropic polypeptide (GIP) receptors, key mediators of insulin secretion that are also expressed in certain brain regions that regulate food intake [163]. Tirzepatide is shown to significantly improve glycemic control and promote weight loss similar to GLP-1 medications such as semaglutide [164]. It is reported that tirzepatide outperforms dulaglutide, semaglutide (Ozempic, Figure 3), degludec, and glargine in terms of glycemic control [165], which may help reduce microvascular complications. It is feasible to assume that if tirzepatide is implemented shortly after the diagnosis of T2DM, it might potentially cause a long-term reduction in microvascular disease. Tirzepatide is currently used as a second-line diabetes medication to maintain glycemic levels in the recommended range in order to delay or prevent diabetes-related complications [166].
6.1.3. Kerendia (finerenone)
Kerendia is an FDA-approved mineralocorticoid receptor antagonist [167]. Compared to other antagonists, finerenone is more potent and selective for the mineralocorticoid receptor [168]. It has been shown to reduce CV and renal complications, particularly in patients with diabetes and kidney disease [167] (Table 2). Finerenone is an adjunctive medication, that provides a promising option for managing T2DM in individuals with comorbid conditions affecting both the heart and kidneys. It is not an essential part of treatment but may help offer a dual benefit in reducing adverse CV and renal outcomes [169].
These novel therapies represent significant advances in the treatment of T2DM, addressing not only glycemic control but also reducing comorbidities such as CV and renal complications, thus improving patient outcomes and quality of life.
6.2. Clinical Trial of Antidiabetic Therapy in Patients T2DM
Our search yielded 33 eligible clinical trials. Among these studies, we identified 15 new compounds. In the clinical studies, compared with placebo, dipeptidyl peptidase 4 (DPP-4) inhibitors, new SGLT2 inhibitors, insulin secretion inducer (Exenatide)/ SGLT2 inhibitor combination, oral small-molecule glucagon-like peptide-1 receptor agonist (GLP1 RA), and GLP1 RA are found to be more effective in improving glycemic control and appear to have no or minimal side effects for most participants. The summary of these potential new treatments is shown in (Table 3).
7. Future Perspectives
The impact of human genetic variation on metabolic homeostasis is becoming increasingly evident, particularly in T2DM. Rare genetic variants play a significant role in altering the metabolic phenotype of individuals with T2DM. Understanding these genetic variations and their role in energy homeostasis, as well as the regulation of food intake, could pave the way for developing more targeted and effective treatments for T2DM.
The etiology of T2DM is influenced by several complex factors, including the central nervous system (CNS), which regulates glucose metabolism, and a combination of genetic and environmental factors. Key hormones involved in metabolic regulation, such as insulin, glucagon, GLP-1, and GIP, also play pivotal roles in disease development. Lifestyle factors, including glucolipotoxicity diets and sedentary behavior, as well as altered islet architecture, vascular endothelial dysfunction, immune system changes, and pancreatic islet behavior, all contribute to the pathogenesis of T2DM.
Due to the intricate and interconnected systems that govern metabolism, the pathogenesis of T2DM remains mechanistically complex and not yet fully understood. Future therapeutic research will need to consider how these diverse networks of systems and processes interact synergistically to produce the altered metabolic phenotype in T2DM. Additionally, research must explore how new treatments, such as bexagliflozin, tirzepatide, and finerenone, can influence the hormones involved in metabolic homeostasis, ultimately striving to produce a metabolic profile that closely resembles that of a healthy individual.
Both bexagliflozin and tirzepatide have shown considerable promise as novel agents that provide more effective therapies for T2DM, while also offering beneficial effects on multiple organs involved in disease pathology. However, the genetic profile of each patient can significantly influence their response to these drugs. Gene variants may lead to variations in drug efficacy and potential side effects, signifying the need for a personalized approach to treatment. Enormous progress has been made in identifying and cataloging the genetic basis of T2DM based on GWAS. However, we should continue to improve our understanding of the genetic basis of T2DM and elucidate how these variants influence cellular pathways, leading to the observed disease trait. Our newly gained knowledge would immensely help improve patient management by helping clinicians predict which treatments will be most effective for individual patients.
8. Conclusions
Uncontrolled T2DM often progresses into a multisystemic illness that encompasses micro- and macrovascular dysfunction, clotting abnormalities, renal injury, inflammation, retinopathy, and peripheral neuronal damage. These complications have already caused significant morbidity and debilitation in a large fraction of patients with T2DM worldwide. Despite our growing understanding of the genetic drivers of disease heterogeneity and advancements in treatment strategies, uncontrolled T2DM remains a significant global health challenge.
Recent advancements in T2DM treatment, such as new DPP-4 inhibitors, oral small-molecule GLP1-RAs, new SGLT2 inhibitors, and oral insulin, show considerable promise in managing hyperglycemia, particularly in patients with uncontrolled T2DM or hypertensive patients with T2DM. However, diagnostic and treatment options for this subset of patients are currently insufficient. While positive results have been reported in a limited number of clinical trials, there is still a need for rigorous further research to assess the efficacy and potential side effects of these treatments.
Moreover, new clinical trials are required to evaluate treatments that address the underlying physiological mechanisms of uncontrolled T2DM, including persistent hyperglycemia, as well as the etiological heterogeneity that drives the disease's development and progression. Only through a more comprehensive understanding of both the genetic and environmental factors at play, together with advancements in precision medicine, will we be able to address the challenges posed by T2DM in order to improve patient outcomes worldwide.
Author Contributions
Conceptualization, Z.SM., and F.M.; writing—original draft preparation, F.M., S.B., Z.SM.; writing—review and editing, Z.SM., S.B., F.M.; supervision, F.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
The original contributions in the study are included in the article, further inquiries can be directed to the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| ADA | American Diabetes Association |
| BMI | Body mass index |
| CV | Cardiovascular |
| CNS | Central nervous system |
| DPP-4 | dipeptidyl peptidase-4 |
| FTO | Fat mass and obesity-associated |
| FDA | Food and Drug Administration |
| GLIS3 | Gli-similar 3 |
| GLP-1 | Glucagon-like peptide-1 |
| GIP | Glucose-dependent insulinotropic polypeptide |
| GWAS | Genome-wide association studies |
| HNF4α | hepatocyte nuclear factor 4-alpha |
| HbA1C | Plasma glycosylated hemoglobin A1C |
| MC4R | Melanortin-4 receptor |
| MeSH | Medical subject headings |
| MODY | Maturity-onset diabetes of the young |
| NF-κB | Nuclear factor-κB |
| OPG | Osteoprotegerin |
| PPARγ | Peroxisome proliferator-activated receptor Gamma |
| SNPs | Single nucleotide polymorphisms |
| SGLT2 | Sodium-glucose co-transporter-2 |
| T2DM | Type 2 diabetes mellitus |
| TGFβ | Transforming growth factor beta |
| WHO | World Health Organization |
References
- Hollstein, T.; Basolo, A.; Ando, T.; Votruba, S.B.; Walter, M.; Krakoff, J.; Piaggi, P. , Recharacterizing the Metabolic State of Energy Balance in Thrifty and Spendthrift Phenotypes. The Journal of Clinical Endocrinology & Metabolism 2020, 105, 1375–1392. [Google Scholar]
- Heilbronn, L.K.; de Jonge, L.; Frisard, M.I.; DeLany, J.P.; Larson-Meyer, D.E.; Rood, J.; Nguyen, T.; Martin, C.K.; Volaufova, J.; Most, M.M.; Greenway, F.L.; Smith, S.R.; Deutsch, W.A.; Williamson, D.A.; Ravussin, E.; Pennington CALERIE Team, f. t. , Effect of 6-Month Calorie Restriction on Biomarkers of Longevity, Metabolic Adaptation, and Oxidative Stress in Overweight IndividualsA Randomized Controlled Trial. Jama 2006, 295, 1539–1548. [Google Scholar] [CrossRef]
- Chia, C.W.; Egan, J.M.; Ferrucci, L. , Age-Related Changes in Glucose Metabolism, Hyperglycemia, and Cardiovascular Risk. Circulation research 2018, 123, 886–904. [Google Scholar] [CrossRef]
- Sun, J.; Fang, R.; Wang, H.; Xu, D.-X.; Yang, J.; Huang, X.; Cozzolino, D.; Fang, M.; Huang, Y. , A review of environmental metabolism disrupting chemicals and effect biomarkers associating disease risks: Where exposomics meets metabolomics. Environment international 2022, 158, 106941. [Google Scholar] [CrossRef]
- Virolainen, S.J.; VonHandorf, A.; Viel, K.C.M.F.; Weirauch, M.T.; Kottyan, L.C. , Gene–environment interactions and their impact on human health. Genes & Immunity 2023, 24, 1–11. [Google Scholar]
- Xu, F.; Liu, J.; Na, L.; Chen, L. , Roles of Epigenetic Modifications in the Differentiation and Function of Pancreatic β-Cells. Frontiers in cell and developmental biology 2020, 8, 748. [Google Scholar] [CrossRef]
- Snykers, S.; Henkens, T.; De Rop, E.; Vinken, M.; Fraczek, J.; De Kock, J.; De Prins, E.; Geerts, A.; Rogiers, V.; Vanhaecke, T. , Role of epigenetics in liver-specific gene transcription, hepatocyte differentiation and stem cell reprogrammation. Journal of hepatology 2009, 51, 187–211. [Google Scholar] [CrossRef]
- Trexler, E.T.; Smith-Ryan, A.E.; Norton, L.E. , Metabolic adaptation to weight loss: implications for the athlete. Journal of the International Society of Sports Nutrition 2014, 11, 7. [Google Scholar] [CrossRef]
- Hyde, P.N.; Sapper, T.N.; Crabtree, C.D.; LaFountain, R.A.; Bowling, M.L.; Buga, A.; Fell, B.; McSwiney, F.T.; Dickerson, R.M.; Miller, V.J.; Scandling, D.; Simonetti, O.P.; Phinney, S.D.; Kraemer, W.J.; King, S.A.; Krauss, R.M.; Volek, J.S. , Dietary carbohydrate restriction improves metabolic syndrome independent of weight loss. JCI insight 2019, 4. [Google Scholar] [CrossRef]
- Park, C.; Pagnini, F.; Langer, E. , Glucose metabolism responds to perceived sugar intake more than actual sugar intake. Scientific reports 2020, 10, 15633. [Google Scholar] [CrossRef]
- Nathan, D.M.; Singer, D.E.; Hurxthal, K.; Goodson, J.D. , The clinical information value of the glycosylated hemoglobin assay. The New England journal of medicine 1984, 310, 341–6. [Google Scholar] [CrossRef] [PubMed]
- Cohen, R.M.; Haggerty, S.; Herman, W.H. , HbA1c for the Diagnosis of Diabetes and Prediabetes: Is It Time for a Mid-Course Correction? The Journal of Clinical Endocrinology & Metabolism 2010, 95, 5203–5206. [Google Scholar]
- Association, A.D., 6. Glycemic Targets: Standards of Medical Care in Diabetes—2019. Diabetes care 2018, 42, (Supplement_1), S61-S70.
- Glycemic Control and Type 2 Diabetes Mellitus: The Optimal Hemoglobin A1c Targets. A Guidance Statement from the American College of Physicians. Annals of internal medicine 2007, 147, 417–422. [Google Scholar] [CrossRef] [PubMed]
- Blonde, L.; Umpierrez, G.E.; Reddy, S.S.; McGill, J.B.; Berga, S.L.; Bush, M.; Chandrasekaran, S.; DeFronzo, R.A.; Einhorn, D.; Galindo, R.J.; Gardner, T.W.; Garg, R.; Garvey, W.T.; Hirsch, I.B.; Hurley, D.L.; Izuora, K.; Kosiborod, M.; Olson, D.; Patel, S.B.; Pop-Busui, R.; Sadhu, A.R.; Samson, S.L.; Stec, C.; Tamborlane, W.V., Jr.; Tuttle, K.R.; Twining, C.; Vella, A.; Vellanki, P.; Weber, S.L. , American Association of Clinical Endocrinology Clinical Practice Guideline: Developing a Diabetes Mellitus Comprehensive Care Plan—2022 Update. Endocrine Practice 2022, 28, 923–1049. [Google Scholar]
- Garber, A.J.; Moghissi, E.S.; Bransome, E.D., Jr.; Clark, N.G.; Clement, S.; Cobin, R.H.; Furnary, A.P.; Hirsch, I.B.; Levy, P.; Roberts, R.; Van den Berghe, G.; Zamudio, V. , American College of Endocrinology position statement on inpatient diabetes and metabolic control. Endocrine practice : official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists 2004, 10, 77–82. [Google Scholar] [CrossRef]
- Yun, J.-S.; Jung, S.-H.; Shivakumar, M.; Xiao, B.; Khera, A.V.; Won, H.-H.; Kim, D. , Polygenic risk for type 2 diabetes, lifestyle, metabolic health, and cardiovascular disease: a prospective UK Biobank study. Cardiovascular diabetology 2022, 21, 131. [Google Scholar] [CrossRef]
- Laakso, M.; Fernandes Silva, L. , Genetics of Type 2 Diabetes: Past, Present, and Future. Nutrients 2022, 14, 3201. [Google Scholar] [CrossRef]
- Yajnik, C.S.; Wagh, R.; Kunte, P.; Asplund, O.; Ahlqvist, E.; Bhat, D.; Shukla, S.R.; Prasad, R.B. , Polygenic scores of diabetes-related traits in subgroups of type 2 diabetes in India: a cohort study. The Lancet Regional Health - Southeast Asia.
- Praetorius, C.; Grill, C.; Stacey, Simon N. ; Metcalf, Alexander M.; Gorkin, David U.; Robinson, Kathleen C.; Van Otterloo, E.; Kim, Reuben S. Q.; Bergsteinsdottir, K.; Ogmundsdottir, Margret H.; Magnusdottir, E.; Mishra, Pravin J.; Davis, Sean R.; Guo, T.; Zaidi, M.R.; Helgason, Agnar S.; Sigurdsson, Martin I.; Meltzer, Paul S.; Merlino, G.; Petit, V.; Larue, L.; Loftus, Stacie K.; Adams, David R.; Sobhiafshar, U.; Emre, N.C.T.; Pavan, William J.; Cornell, R.; Smith, Aaron G.; McCallion, Andrew S.; Fisher, David E.; Stefansson, K.; Sturm, Richard A.; Steingrimsson, E., A Polymorphism in IRF4 Affects Human Pigmentation through a Tyrosinase-Dependent MITF/TFAP2A Pathway. Cell 2013, 155, 1022–1033. [Google Scholar]
- Fajans, S.S.; Bell, G.I.; Polonsky, K.S. , Molecular mechanisms and clinical pathophysiology of maturity-onset diabetes of the young. The New England journal of medicine 2001, 345, 971–80. [Google Scholar] [CrossRef]
- Wu, Y.; Ding, Y.; Tanaka, Y.; Zhang, W. , Risk Factors Contributing to Type 2 Diabetes and Recent Advances in the Treatment and Prevention. International journal of medical sciences 2014, 11, 1185–1200. [Google Scholar] [CrossRef]
- Dzhambov, A.M. , Long-term noise exposure and the risk for type 2 diabetes: a meta-analysis: Erratum. Noise & health 2015, 17, 123. [Google Scholar]
- Marcadenti, A. , Diet, Cardiometabolic Factors and Type-2 Diabetes Mellitus: The Role of Genetics. Current diabetes reviews 2016, 12, 322–330. [Google Scholar] [CrossRef] [PubMed]
- Kuntić, M.; Hahad, O.; Münzel, T.; Daiber, A. , Crosstalk between Oxidative Stress and Inflammation Caused by Noise and Air Pollution—Implications for Neurodegenerative Diseases. Antioxidants 2024, 13, 266. [Google Scholar] [CrossRef] [PubMed]
- Ali, O. , Genetics of type 2 diabetes. World journal of diabetes 2013, 4, 114–23. [Google Scholar] [CrossRef]
- Todd, J.N.; Kleinberger, J.W.; Zhang, H.; Srinivasan, S.; Tollefsen, S.E.; Levitsky, L.L.; Levitt Katz, L.E.; Tryggestad, J.B.; Bacha, F.; Imperatore, G.; Lawrence, J.M.; Pihoker, C.; Divers, J.; Flannick, J.; Dabelea, D.; Florez, J.C.; Pollin, T.I. , Monogenic Diabetes in Youth With Presumed Type 2 Diabetes: Results From the Progress in Diabetes Genetics in Youth (ProDiGY) Collaboration. Diabetes care 2021, 44, 2312–9. [Google Scholar] [CrossRef]
- Salguero, M.V.; Arosemena, M.; Pollin, T.; Greeley, S.A.W.; Naylor, R.N.; Letourneau-Freiberg, L.; Bowden, T.L.; Wei, D.; Philipson, L.H., Monogenic Forms of Diabetes. In Diabetes in America, Lawrence, J.M.; Casagrande, S.S.; Herman, W.H.; Wexler, D.J.; Cefalu, W.T., Eds. National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK): Bethesda (MD), 2023.
- Blonde, L.; Umpierrez, G.E.; Reddy, S.S.; McGill, J.B.; Berga, S.L.; Bush, M.; Chandrasekaran, S.; DeFronzo, R.A.; Einhorn, D.; Galindo, R.J.; Gardner, T.W.; Garg, R.; Garvey, W.T.; Hirsch, I.B.; Hurley, D.L.; Izuora, K.; Kosiborod, M.; Olson, D.; Patel, S.B.; Pop-Busui, R.; Sadhu, A.R.; Samson, S.L.; Stec, C.; Tamborlane, W.V., Jr.; Tuttle, K.R.; Twining, C.; Vella, A.; Vellanki, P.; Weber, S.L. , American Association of Clinical Endocrinology Clinical Practice Guideline: Developing a Diabetes Mellitus Comprehensive Care Plan-2022 Update. Endocrine practice : official journal of the American College of Endocrinology and the American Association of Clinical Endocrinologists 2022, 28, 923–1049. [Google Scholar]
- Ali, A.S.; Ekinci, E.I.; Pyrlis, F. , Maternally inherited diabetes and deafness (MIDD): An uncommon but important cause of diabetes. Endocrine and Metabolic Science 2021, 2, 100074. [Google Scholar] [CrossRef]
- Donovan, L.E.; Severin, N.E. , Maternally Inherited Diabetes and Deafness in a North American Kindred: Tips for Making the Diagnosis and Review of Unique Management Issues. The Journal of Clinical Endocrinology & Metabolism 2006, 91, 4737–4742. [Google Scholar]
- Urano, F. , Wolfram Syndrome: Diagnosis, Management, and Treatment. Current diabetes reports 2016, 16, 6. [Google Scholar] [CrossRef]
- Shoemaker, A., Bardet-Biedl syndrome: A clinical overview focusing on diagnosis, outcomes and best-practice management. Diabetes, Obesity and Metabolism 2024, 26, (S2), 25-33.
- Baier, L.J.; Muller, Y.L.; Remedi, M.S.; Traurig, M.; Piaggi, P.; Wiessner, G.; Huang, K.; Stacy, A.; Kobes, S.; Krakoff, J.; Bennett, P.H.; Nelson, R.G.; Knowler, W.C.; Hanson, R.L.; Nichols, C.G.; Bogardus, C. , ABCC8 R1420H Loss-of-Function Variant in a Southwest American Indian Community: Association With Increased Birth Weight and Doubled Risk of Type 2 Diabetes. Diabetes 2015, 64, 4322–32. [Google Scholar] [CrossRef]
- Riveline, J.P.; Rousseau, E.; Reznik, Y.; Fetita, S.; Philippe, J.; Dechaume, A.; Hartemann, A.; Polak, M.; Petit, C.; Charpentier, G.; Gautier, J.F.; Froguel, P.; Vaxillaire, M. , Clinical and metabolic features of adult-onset diabetes caused by ABCC8 mutations. Diabetes care 2012, 35, 248–51. [Google Scholar] [CrossRef] [PubMed]
- Farid, M.M.M.; Abdel-Mageed, A.I.; El-sherbini, A.; Mohamed, N.R.; Mohsen, M. , Study of the association between GLIS3 rs10758593 and type 2 diabetes mellitus in Egyptian population. Egyptian Journal of Medical Human Genetics 2022, 23, 44. [Google Scholar] [CrossRef]
- Meulebrouck, S.; Scherrer, V.; Boutry, R.; Toussaint, B.; Vaillant, E.; Dechaume, A.; Loiselle, H.; Balkau, B.; Charpentier, G.; Franc, S.; Marre, M.; Baron, M.; Vaxillaire, M.; Derhourhi, M.; Boissel, M.; Froguel, P.; Bonnefond, A. , Pathogenic monoallelic variants in GLIS3 increase type 2 diabetes risk and identify a subgroup of patients sensitive to sulfonylureas. Diabetologia 2024, 67, 327–332. [Google Scholar] [CrossRef] [PubMed]
- Hayhurst, G.P.; Lee, Y.H.; Lambert, G.; Ward, J.M.; Gonzalez, F.J. , Hepatocyte nuclear factor 4alpha (nuclear receptor 2A1) is essential for maintenance of hepatic gene expression and lipid homeostasis. Molecular and cellular biology 2001, 21, 1393–403. [Google Scholar] [CrossRef]
- Billings, L.K.; Jablonski, K.A.; Warner, A.S.; Cheng, Y.C.; McAteer, J.B.; Tipton, L.; Shuldiner, A.R.; Ehrmann, D.A.; Manning, A.K.; Dabelea, D.; Franks, P.W.; Kahn, S.E.; Pollin, T.I.; Knowler, W.C.; Altshuler, D.; Florez, J.C. , Variation in Maturity-Onset Diabetes of the Young Genes Influence Response to Interventions for Diabetes Prevention. The Journal of clinical endocrinology and metabolism 2017, 102, 2678–2689. [Google Scholar] [CrossRef]
- Hellwege, J.N.; Hicks, P.J.; Palmer, N.D.; Ng, M.C.; Freedman, B.I.; Bowden, D.W. , Examination of Rare Variants in HNF4 alpha in European Americans with Type 2 Diabetes. Journal of diabetes & metabolism 2011, 2. [Google Scholar]
- Haghvirdizadeh, P.; Mohamed, Z.; Abdullah, N.A.; Haghvirdizadeh, P.; Haerian, M.S.; Haerian, B.S. , KCNJ11: Genetic Polymorphisms and Risk of Diabetes Mellitus. Journal of diabetes research 2015, 2015, 908152. [Google Scholar] [CrossRef]
- Rizvi, S.; Raza, S.T.; Mahdi, F.; Singh, S.P.; Rajput, M.; Rahman, Q. , Genetic polymorphisms in KCNJ11 (E23K, rs5219) and SDF-1β (G801A, rs1801157) genes are associated with the risk of type 2 diabetes mellitus. British journal of biomedical science 2018, 75, 139–144. [Google Scholar] [CrossRef]
- Huerta-Chagoya, A.; Schroeder, P.; Mandla, R.; Li, J.; Morris, L.; Vora, M.; Alkanaq, A.; Nagy, D.; Szczerbinski, L.; Madsen, J.G.S.; Bonàs-Guarch, S.; Mollandin, F.; Cole, J.B.; Porneala, B.; Westerman, K.; Li, J.H.; Pollin, T.I.; Florez, J.C.; Gloyn, A.L.; Carey, D.J.; Cebola, I.; Mirshahi, U.L.; Manning, A.K.; Leong, A.; Udler, M.; Mercader, J.M. , Rare variant analyses in 51,256 type 2 diabetes cases and 370,487 controls reveal the pathogenicity spectrum of monogenic diabetes genes. Nature genetics 2024, 56, 2370–2379. [Google Scholar] [CrossRef]
- Claussnitzer, M.; Dankel, S.N.; Klocke, B.; Grallert, H.; Glunk, V.; Berulava, T.; Lee, H.; Oskolkov, N.; Fadista, J.; Ehlers, K.; Wahl, S.; Hoffmann, C.; Qian, K.; Ronn, T.; Riess, H.; Muller-Nurasyid, M.; Bretschneider, N.; Schroeder, T.; Skurk, T.; Horsthemke, B.; Spieler, D.; Klingenspor, M.; Seifert, M.; Kern, M.J.; Mejhert, N.; Dahlman, I.; Hansson, O.; Hauck, S.M.; Bluher, M.; Arner, P.; Groop, L.; Illig, T.; Suhre, K.; Hsu, Y.H.; Mellgren, G.; Hauner, H.; Laumen, H. , Leveraging cross-species transcription factor binding site patterns: from diabetes risk loci to disease mechanisms. Cell, 2014; 156, 343–358. [Google Scholar]
- Majithia, A.R.; Flannick, J.; Shahinian, P.; Guo, M.; Bray, M.-A.; Fontanillas, P.; Gabriel, S.B.; Consortium, G.D.; Project, N.J.F.A.S.; Consortium, S.T.D.; Consortium, T.D.-G.; Rosen, E.D.; Altshuler, D.; Flannick, J.; Manning, A.K.; Hartl, C.; Agarwala, V.; Fontanillas, P.; Green, T.; Banks, E.; DePristo, M.; Poplin, R.; Shakir, K.; Fennell, T.; Njølstad, P.R.; Altshuler, D.; Burtt, N.; Gabriel, S.; Fuchsberger, C.; Kang, H.M.; Sim, X.; Ma, C.; Locke, A.; Blackwell, T.; Jackson, A.; Teslovich, T.M.; Stringham, H.; Chines, P.; Kwan, P.; Huyghe, J.; Tan, A.; Jun, G.; Stitzel, M.; Bergman, R.N.; Bonnycastle, L.; Tuomilehto, J.; Collins, F.S.; Scott, L.; Mohlke, K.; Abecasis, G.; Boehnke, M.; Strom, T.; Gieger, C.; Nurasyid, M.M.; Grallert, H.; Kriebel, J.; Ried, J.; Hrabé de Angelis, M.; Huth, C.; Meisinger, C.; Peters, A.; Rathmann, W.; Strauch, K.; Meitinger, T.; Kravic, J.; Algren, P.; Ladenvall, C.; Toumi, T.; Isomaa, B.; Groop, L.; Gaulton, K.; Moutsianas, L.; Rivas, M.; Pearson, R.; Mahajan, A.; Prokopenko, I.; Kumar, A.; Perry, J.; Howie, B.; van de Bunt, M.; Small, K.; Lindgren, C.; Lunter, G.; Robertson, N.; Rayner, W.; Morris, A.; Buck, D.; Hattersley, A.; Spector, T.; McVean, G.; Frayling, T.; Donnelly, P.; McCarthy, M.; Gupta, N.; Taylor, H.; Fox, E.; Cheh, C.N.; Wilson, J.G.; O'Donnell, C.J.; Kathiresan, S.; Hirschhorn, J.; Seidman, J.G.; Gabriel, S.; Seidman, C.; Altshuler, D.; Williams, A.L.; Jacobs, S.B.R.; Macías, H.M.; Chagoya, A.H.; Churchhouse, C.; Luna, C.M.; Ortíz, H.G.; Vázquez, M.J.G.; Burtt, N.P.; Estrada, K.; Mercader, J.M.; Ripke, S.; Manning, A.K.; Neale, B.; Stram, D.O.; López, J.C.F.; Hidalgo, S.R.; Delfín, I.A.; Hernández, A.M.; Cruz, F.C.; Caamal, E.M.; Monsalve, C.R.; Andrade, S.I.; Córdova, E.; Arellano, E.R.; Soberón, X.; Villalpando, M.E.G.; Monroe, K.; Wilkens, L.; Kolonel, L.N.; Le Marchand, L.; Riba, L.; Sánchez, M.L.O.; Guillén, R.R.; Bautista, I.C.; Torres, M.R.; Hernández, L.L.M.; Sáenz, T.; Gómez, D.; Alvirde, U.; Onofrio, R.C.; Brodeur, W.M.; Gage, D.; Murphy, J.; Franklin, J.; Mahan, S.; Ardlie, K.; Crenshaw, A.T.; Winckler, W.; Fennell, T.; MacArthur, D.G.; Altshuler, D.; Florez, J.C.; Haiman, C.A.; Henderson, B.E.; Salinas, C.A.A.; Villalpando, C.G.; Orozco, L.; Luna, T.T.; Abecasis, G.; Almeida, M.; Altshuler, D.; Asimit, J.L.; Atzmon, G.; Barber, M.; Beer, N.L.; Bell, G.I.; Below, J.; Blackwell, T.; Blangero, J.; Boehnke, M.; Bowden, D.W.; Burtt, N.; Chambers, J.; Chen, H.; Chen, P.; Chines, P.S.; Choi, S.; Churchhouse, C.; Cingolani, P.; Cornes, B.K.; Cox, N.; Williams, A.G.D.; Duggirala, R.; Dupuis, J.; Dyer, T.; Feng, S.; Tajes, J.F.; Ferreira, T.; Fingerlin, T.E.; Flannick, J.; Florez, J.; Fontanillas, P.; Frayling, T.M.; Fuchsberger, C.; Gamazon, E.R.; Gaulton, K.; Ghosh, S.; Gloyn, A.; Grossman, R.L.; Grundstad, J.; Hanis, C.; Heath, A.; Highland, H.; Hirokoshi, M.; Huh, I.-S.; Huyghe, J.R.; Ikram, K.; Jablonski, K.A.; Kim, Y.J.; Jun, G.; Kato, N.; Kim, J.; King, C.R.; Kooner, J.; Kwon, M.-S.; Im, H.K.; Laakso, M.; Lam, K.K.-Y.; Lee, J.; Lee, S.; Lee, S.; Lehman, D.M.; Li, H.; Lindgren, C.M.; Liu, X.; Livne, O.E.; Locke, A.E.; Mahajan, A.; Maller, J.B.; Manning, A.K.; Maxwell, T.J.; Mazoure, A.; McCarthy, M.I.; Meigs, J.B.; Min, B.; Mohlke, K.L.; Morris, A.; Musani, S.; Nagai, Y.; Ng, M.C.Y.; Nicolae, D.; Oh, S.; Palmer, N.; Park, T.; Pollin, T.I.; Prokopenko, I.; Reich, D.; Rivas, M.A.; Scott, L.J.; Seielstad, M.; Cho, Y.S.; Tai, E.-S.; Sim, X.; Sladek, R.; Smith, P.; Tachmazidou, I.; Teslovich, T.M.; Torres, J.; Trubetskoy, V.; Willems, S.M.; Williams, A.L.; Wilson, J.G.; Wiltshire, S.; Won, S.; Wood, A.R.; Xu, W.; Teo, Y.Y.; Yoon, J.; Lee, J.-Y.; Zawistowski, M.; Zeggini, E.; Zhang, W.; Zöllner, S. , Rare variants in <i>PPARG</i> with decreased activity in adipocyte differentiation are associated with increased risk of type 2 diabetes. Proceedings of the National Academy of Sciences 2014, 111, 13127–13132. [Google Scholar]
- Chan, K.H.; Niu, T.; Ma, Y.; You, N.C.; Song, Y.; Sobel, E.M.; Hsu, Y.H.; Balasubramanian, R.; Qiao, Y.; Tinker, L.; Liu, S. , Common genetic variants in peroxisome proliferator-activated receptor-gamma (PPARG) and type 2 diabetes risk among Women's Health Initiative postmenopausal women. The Journal of clinical endocrinology and metabolism 2013, 98, E600–E604. [Google Scholar] [CrossRef] [PubMed]
- Sailaja, A.N.; Nanda, N.; Suryanarayana, B.S.; Pal, G.K. , Association of rs2073618 polymorphism and osteoprotegerin levels with hypertension and cardiovascular risks in patients with type 2 diabetes mellitus. Scientific reports 2023, 13, 17451. [Google Scholar] [CrossRef] [PubMed]
- Kliewer, S.A.; Forman, B.M.; Blumberg, B.; Ong, E.S.; Borgmeyer, U.; Mangelsdorf, D.J.; Umesono, K.; Evans, R.M. , Differential expression and activation of a family of murine peroxisome proliferator-activated receptors. Proceedings of the National Academy of Sciences of the United States of America 1994, 91, 7355–9. [Google Scholar] [CrossRef] [PubMed]
- Tontonoz, P.; Hu, E.; Graves, R.A.; Budavari, A.I.; Spiegelman, B.M. , mPPAR gamma 2: tissue-specific regulator of an adipocyte enhancer. Genes & development 1994, 8, 1224–34. [Google Scholar]
- Ricote, M.; Huang, J.; Fajas, L.; Li, A.; Welch, J.; Najib, J.; Witztum, J.L.; Auwerx, J.; Palinski, W.; Glass, C.K. , Expression of the peroxisome proliferator-activated receptor γ (PPARγ) in human atherosclerosis and regulation in macrophages by colony stimulating factors and oxidized low density lipoprotein. Proceedings of the National Academy of Sciences 1998, 95, 7614–7619. [Google Scholar] [CrossRef]
- Yu, L.; Gao, Y.; Aaron, N.; Qiang, L. , A glimpse of the connection between PPARγ and macrophage. Frontiers in pharmacology 2023, 14, 1254317. [Google Scholar] [CrossRef]
- Chawla, A. , Control of macrophage activation and function by PPARs. Circulation research 2010, 106, 1559–69. [Google Scholar] [CrossRef]
- Lakatos, H.F.; Thatcher, T.H.; Kottmann, R.M.; Garcia, T.M.; Phipps, R.P.; Sime, P.J. , The Role of PPARs in Lung Fibrosis. PPAR research 2007, 2007, 71323. [Google Scholar] [CrossRef]
- Martínez-García, C.; Izquierdo, A.; Velagapudi, V.; Vivas, Y.; Velasco, I.; Campbell, M.; Burling, K.; Cava, F.; Ros, M.; Oresic, M.; Vidal-Puig, A.; Medina-Gomez, G. , Accelerated renal disease is associated with the development of metabolic syndrome in a glucolipotoxic mouse model. Disease models & mechanisms 2012, 5, 636–48. [Google Scholar]
- Kökény, G.; Calvier, L.; Hansmann, G. , PPARγ and TGFβ-Major Regulators of Metabolism, Inflammation, and Fibrosis in the Lungs and Kidneys. International journal of molecular sciences 2021, 22. [Google Scholar] [CrossRef]
- Roszer, T.; Menéndez-Gutiérrez, M.P.; Lefterova, M.I.; Alameda, D.; Núñez, V.; Lazar, M.A.; Fischer, T.; Ricote, M. , Autoimmune kidney disease and impaired engulfment of apoptotic cells in mice with macrophage peroxisome proliferator-activated receptor gamma or retinoid X receptor alpha deficiency. J Immunol 2011, 186, 621–31. [Google Scholar] [CrossRef] [PubMed]
- Arabshomali, A.; Bazzazzadehgan, S.; Mahdi, F.; Shariat-Madar, Z. , Potential Benefits of Antioxidant Phytochemicals in Type 2 Diabetes. Molecules 2023, 28, 7209. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.; Wang, L.; Wang, M.; Zhou, S.; Lu, Y.; Cui, H.; Racanelli, A.C.; Zhang, L.; Ye, T.; Ding, B.; Zhang, B.; Yang, J.; Yao, Y. , Targeting fibrosis: mechanisms and clinical trials. Signal Transduction and Targeted Therapy 2022, 7, 206. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.; Birerdinc, A.; Younossi, Z.M. , Host Genetic Variants in Obesity-Related Nonalcoholic Fatty Liver Disease. Clinics in liver disease 2014, 18, 249–267. [Google Scholar] [CrossRef]
- Semple, R.K.; Chatterjee, V.K.K.; O’Rahilly, S. , PPARγ and human metabolic disease. The Journal of clinical investigation 2006, 116, 581–589. [Google Scholar] [CrossRef]
- Majithia, A.R.; Flannick, J.; Shahinian, P.; Guo, M.; Bray, M.A.; Fontanillas, P.; Gabriel, S.B.; Rosen, E.D.; Altshuler, D. , Rare variants in PPARG with decreased activity in adipocyte differentiation are associated with increased risk of type 2 diabetes. Proceedings of the National Academy of Sciences of the United States of America 2014, 111, 13127–32. [Google Scholar] [CrossRef]
- Sarhangi, N.; Sharifi, F.; Hashemian, L.; Hassani Doabsari, M.; Heshmatzad, K.; Rahbaran, M.; Jamaldini, S.H.; Aghaei Meybodi, H.R.; Hasanzad, M. , PPARG (Pro12Ala) genetic variant and risk of T2DM: a systematic review and meta-analysis. Scientific reports 2020, 10, 12764. [Google Scholar] [CrossRef]
- Li, S.; He, C.; Nie, H.; Pang, Q.; Wang, R.; Zeng, Z.; Song, Y. , G Allele of the rs1801282 Polymorphism in PPARgamma Gene Confers an Increased Risk of Obesity and Hypercholesterolemia, While T Allele of the rs3856806 Polymorphism Displays a Protective Role Against Dyslipidemia: A Systematic Review and Meta-Analysis. Frontiers in endocrinology 2022, 13, 919087. [Google Scholar] [CrossRef]
- Marangoni, R.G.; Korman, B.D.; Allanore, Y.; Dieude, P.; Armstrong, L.L.; Rzhetskaya, M.; Hinchcliff, M.; Carns, M.; Podlusky, S.; Shah, S.J.; Ruiz, B.; Hachulla, E.; Tiev, K.; Cracowski, J.-L.; Varga, J.; Hayes, M.G. , A candidate gene study reveals association between a variant of the Peroxisome Proliferator-Activated Receptor Gamma (PPAR-γ) gene and systemic sclerosis. Arthritis research & therapy 2015, 17, 128. [Google Scholar]
- Kant, R.; Davis, A.; Verma, V. , Maturity-Onset Diabetes of the Young: Rapid Evidence Review. American family physician 2022, 105, 162–167. [Google Scholar]
- Lemelman, M.B.; Letourneau, L.; Greeley, S.A.W. , Neonatal Diabetes Mellitus: An Update on Diagnosis and Management. Clinics in perinatology 2018, 45, 41–59. [Google Scholar] [CrossRef]
- Barroso, I.; Luan, J.; Middelberg, R.P.; Harding, A.H.; Franks, P.W.; Jakes, R.W.; Clayton, D.; Schafer, A.J.; O'Rahilly, S.; Wareham, N.J. , Candidate gene association study in type 2 diabetes indicates a role for genes involved in beta-cell function as well as insulin action. PLoS biology 2003, 1, E20. [Google Scholar]
- Gloyn, A.L.; Weedon, M.N.; Owen, K.R.; Turner, M.J.; Knight, B.A.; Hitman, G.; Walker, M.; Levy, J.C.; Sampson, M.; Halford, S.; McCarthy, M.I.; Hattersley, A.T.; Frayling, T.M. , Large-scale association studies of variants in genes encoding the pancreatic beta-cell KATP channel subunits Kir6.2 (KCNJ11) and SUR1 (ABCC8) confirm that the KCNJ11 E23K variant is associated with type 2 diabetes. Diabetes 2003, 52, 568–72. [Google Scholar] [CrossRef]
- Fajans, S.S.; Bell, G.I. , MODY: History, genetics, pathophysiology, and clinical decision making. Diabetes care 2011, 34, 1878–1884. [Google Scholar] [CrossRef]
- Thanabalasingham, G.; Pal, A.; Selwood, M.P.; Dudley, C.; Fisher, K.; Bingley, P.J.; Ellard, S.; Farmer, A.J.; McCarthy, M.I.; Owen, K.R. , Systematic assessment of etiology in adults with a clinical diagnosis of young-onset type 2 diabetes is a successful strategy for identifying maturity-onset diabetes of the young. Diabetes care 2012, 35, 1206–12. [Google Scholar] [CrossRef]
- Fajans, S.S.; Bell, G.I.; Paz, V.P.; Below, J.E.; Cox, N.J.; Martin, C.; Thomas, I.H.; Chen, M. , Obesity and hyperinsulinemia in a family with pancreatic agenesis and MODY caused by the IPF1 mutation Pro63fsX60. Translational research : the journal of laboratory and clinical medicine 2010, 156, 7–14. [Google Scholar] [CrossRef]
- Tattersall, R.B. , Mild familial diabetes with dominant inheritance. Q J Med 1974, 43, 339–57. [Google Scholar]
- Shields, B.M.; Hicks, S.; Shepherd, M.H.; Colclough, K.; Hattersley, A.T.; Ellard, S. , Maturity-onset diabetes of the young (MODY): how many cases are we missing? Diabetologia 2010, 53, 2504–8. [Google Scholar] [CrossRef]
- Stoffel, M.; Duncan, S.A. , The maturity-onset diabetes of the young (MODY1) transcription factor HNF4alpha regulates expression of genes required for glucose transport and metabolism. Proceedings of the National Academy of Sciences of the United States of America 1997, 94, 13209–14. [Google Scholar] [CrossRef]
- Kavvoura, F.K.; Owen, K.R. , Maturity onset diabetes of the young: clinical characteristics, diagnosis and management. Pediatric endocrinology reviews : PER 2012, 10, 234–42. [Google Scholar]
- Costa, A.; Bescos, M.; Velho, G.; Chevre, J.; Vidal, J.; Sesmilo, G.; Bellanne-Chantelot, C.; Froguel, P.; Casamitjana, R.; Rivera-Fillat, F. , Genetic and clinical characterisation of maturity-onset diabetes of the young in Spanish families. European journal of endocrinology 2000, 142, 380–386. [Google Scholar] [CrossRef]
- Voight, B.F.; Scott, L.J.; Steinthorsdottir, V.; Morris, A.P.; Dina, C.; Welch, R.P.; Zeggini, E.; Huth, C.; Aulchenko, Y.S.; Thorleifsson, G. , Twelve type 2 diabetes susceptibility loci identified through large-scale association analysis. Nature genetics 2010, 42, 579–589. [Google Scholar] [CrossRef]
- Hibino, H.; Inanobe, A.; Furutani, K.; Murakami, S.; Findlay, I.; Kurachi, Y. , Inwardly Rectifying Potassium Channels: Their Structure, Function, and Physiological Roles. Physiological reviews 2010, 90, 291–366. [Google Scholar] [CrossRef]
- McTaggart, J.S.; Clark, R.H.; Ashcroft, F.M. , The role of the KATP channel in glucose homeostasis in health and disease: more than meets the islet. The Journal of physiology 2010, (Pt 17) Pt 17, 3201–9. [Google Scholar] [CrossRef]
- Gloyn, A.L.; Diatloff-Zito, C.; Edghill, E.L.; Bellanné-Chantelot, C.; Nivot, S.; Coutant, R.; Ellard, S.; Hattersley, A.T.; Robert, J.J. , KCNJ11 activating mutations are associated with developmental delay, epilepsy and neonatal diabetes syndrome and other neurological features. European Journal of Human Genetics 2006, 14, 824–830. [Google Scholar] [CrossRef]
- Edghill, E.L.; Gloyn, A.L.; Goriely, A.; Harries, L.W.; Flanagan, S.E.; Rankin, J.; Hattersley, A.T.; Ellard, S. , Origin of de Novo KCNJ11 Mutations and Risk of Neonatal Diabetes for Subsequent Siblings. The Journal of Clinical Endocrinology & Metabolism 2007, 92, 1773–1777. [Google Scholar]
- Phani, N.M.; Guddattu, V.; Bellampalli, R.; Seenappa, V.; Adhikari, P.; Nagri, S.K.; D′Souza, S.C.; Mundyat, G.P.; Satyamoorthy, K.; Rai, P.S. , Population Specific Impact of Genetic Variants in KCNJ11 Gene to Type 2 Diabetes: A Case-Control and Meta-Analysis Study. PloS one 2014, 9, e107021. [Google Scholar] [CrossRef]
- Gallardo-Blanco, H.L.; Villarreal-Perez, J.Z.; Cerda-Flores, R.M.; Figueroa, A.; Sanchez-Dominguez, C.N.; Gutierrez-Valverde, J.M.; Torres-Muñoz, I.C.; Lavalle-Gonzalez, F.J.; Gallegos-Cabriales, E.C.; Martinez-Garza, L.E. , Genetic variants in KCNJ11, TCF7L2 and HNF4A are associated with type 2 diabetes, BMI and dyslipidemia in families of Northeastern Mexico: A pilot study. Experimental and therapeutic medicine 2017, 13, 523–529. [Google Scholar] [CrossRef]
- Javorsky, M.; Klimcakova, L.; Schroner, Z.; Zidzik, J.; Babjakova, E.; Fabianova, M.; Kozarova, M.; Tkacova, R.; Salagovic, J.; Tkac, I. , KCNJ11 gene E23K variant and therapeutic response to sulfonylureas. European journal of internal medicine 2012, 23, 245–9. [Google Scholar] [CrossRef]
- Sakamoto, Y.; Inoue, H.; Keshavarz, P.; Miyawaki, K.; Yamaguchi, Y.; Moritani, M.; Kunika, K.; Nakamura, N.; Yoshikawa, T.; Yasui, N.; Shiota, H.; Tanahashi, T.; Itakura, M. , SNPs in the KCNJ11-ABCC8 gene locus are associated with type 2 diabetes and blood pressure levels in the Japanese population. Journal of human genetics 2007, 52, 781–793. [Google Scholar] [CrossRef]
- Koo, B.K.; Cho, Y.M.; Park, B.L.; Cheong, H.S.; Shin, H.D.; Jang, H.C.; Kim, S.Y.; Lee, H.K.; Park, K.S. , Polymorphisms of KCNJ11 (Kir6.2 gene) are associated with Type 2 diabetes and hypertension in the Korean population. Diabetic medicine : a journal of the British Diabetic Association 2007, 24, 178–86. [Google Scholar] [CrossRef]
- Moazzam-Jazi, M.; Najd-Hassan-Bonab, L.; Masjoudi, S.; Tohidi, M.; Hedayati, M.; Azizi, F.; Daneshpour, M.S. , Risk of type 2 diabetes and KCNJ11 gene polymorphisms: a nested case-control study and meta-analysis. Scientific reports 2022, 12, 20709. [Google Scholar] [CrossRef]
- Mao, H.; Li, Q.; Gao, S. , Meta-analysis of the relationship between common type 2 diabetes risk gene variants with gestational diabetes mellitus. PloS one 2012, 7, e45882. [Google Scholar] [CrossRef] [PubMed]
- Lauenborg, J.; Grarup, N.; Damm, P.; Borch-Johnsen, K.; Jørgensen, T.; Pedersen, O.; Hansen, T. , Common type 2 diabetes risk gene variants associate with gestational diabetes. The Journal of Clinical Endocrinology & Metabolism 2009, 94, 145–150. [Google Scholar]
- Majcher, S.; Ustianowski, P.; Malinowski, D.; Czerewaty, M.; Tarnowski, M.; Safranow, K.; Dziedziejko, V.; Pawlik, A. , KCNJ11 and KCNQ1 Gene Polymorphisms and Placental Expression in Women with Gestational Diabetes Mellitus. Genes 2022, 13, 1315. [Google Scholar] [CrossRef] [PubMed]
- Qiu, L.; Na, R.; Xu, R.; Wang, S.; Sheng, H.; Wu, W.; Qu, Y. , Quantitative assessment of the effect of KCNJ11 gene polymorphism on the risk of type 2 diabetes. PloS one 2014, 9, e93961. [Google Scholar] [CrossRef] [PubMed]
- Muftin, N.Q.; Jubair, S. , KCNJ11 polymorphism is associated with type 2 diabetes mellitus in Iraqi patients. Gene Reports 2019, 17, 100480. [Google Scholar] [CrossRef]
- Keshavarz, P.; Habibipour, R.; Ghasemi, M.; Kazemnezhad, E.; Alizadeh, M.; Omami, M.H. , Lack of genetic susceptibility of KCNJ11 E23K polymorphism with risk of type 2 diabetes in an Iranian population. Endocrine research 2014, 39, 120–5. [Google Scholar] [CrossRef]
- Makhzoom, O.; Kabalan, Y.; Al-Quobaili, F. , Association of KCNJ11 rs5219 gene polymorphism with type 2 diabetes mellitus in a population of Syria: a case-control study. BMC medical genetics 2019, 20, 107. [Google Scholar] [CrossRef]
- Zhou, D.; Zhang, D.; Liu, Y.; Zhao, T.; Chen, Z.; Liu, Z.; Yu, L.; Zhang, Z.; Xu, H.; He, L. , The E23K variation in the KCNJ11 gene is associated with type 2 diabetes in Chinese and East Asian population. Journal of human genetics 2009, 54, 433–5. [Google Scholar] [CrossRef]
- Gonen, M.S.; Arikoglu, H.; Erkoc Kaya, D.; Ozdemir, H.; Ipekci, S.H.; Arslan, A.; Kayis, S.A.; Gogebakan, B. , Effects of single nucleotide polymorphisms in K(ATP) channel genes on type 2 diabetes in a Turkish population. Archives of medical research 2012, 43, 317–23. [Google Scholar] [CrossRef] [PubMed]
- Elzehery, R.; El-Hafez, H.A.; Elsehely, I.; Barakat, A.; Foda, E.A.E.; Hendawy, S.R.; Gameil, M.A.; Nada, H.S.; El-Sebaie, A. , Association of the E23K (rs5219) polymorphism in the potassium channel (KCNJ11) gene with diabetic neuropathy in type 2 diabetes. Gene 2024, 921, 148525. [Google Scholar] [CrossRef] [PubMed]
- Shorokhova, P.; Baranov, V.; Vorokhobina, N. , Abstract #1001320: Effects of KCNJ11 RS5219 Variant on Metformin Pharmacodynamics in Patients With Newly Diagnosed Type 2 Diabetes Mellitus. Endocrine Practice 2021, 27, S39. [Google Scholar]
- Ahmed, A.; Elsadek, H.M.; Shalaby, S.M.; Elnahas, H.M. , Association of SLC22A1, SLC47A1, and KCNJ11 polymorphisms with efficacy and safety of metformin and sulfonylurea combination therapy in Egyptian patients with type 2 diabetes. Research in pharmaceutical sciences 2023, 18, 614–625. [Google Scholar] [CrossRef]
- Lie, X.; Fang, Y.A.O.; Limin, J.I.N.; Fan, N.; Hanqiang, S.H.I.; Shuqin, D.U.; Yanbo, S.H.I. , Study of <i>KCNJ11</i> rs5219 Gene Polymorphism on the Efficacy of Metformin Combined with Gliclazide in Newly Diagnosed Diabetes Mellitus Type 2 Patients. Chinese Journal of Modern Applied Pharmacy 2023, 40, 3431–3438. [Google Scholar]
- Sesti, G.; Laratta, E.; Cardellini, M.; Andreozzi, F.; Del Guerra, S.; Irace, C.; Gnasso, A.; Grupillo, M.; Lauro, R.; Hribal, M.L.; Perticone, F.; Marchetti, P. , The E23K Variant of KCNJ11 Encoding the Pancreatic β-Cell Adenosine 5′-Triphosphate-Sensitive Potassium Channel Subunit Kir6.2 Is Associated with an Increased Risk of Secondary Failure to Sulfonylurea in Patients with Type 2 Diabetes. The Journal of Clinical Endocrinology & Metabolism 2006, 91, 2334–2339. [Google Scholar]
- Dupuis, J.; Langenberg, C.; Prokopenko, I.; Saxena, R.; Soranzo, N.; Jackson, A.U.; Wheeler, E.; Glazer, N.L.; Bouatia-Naji, N.; Gloyn, A.L.; Lindgren, C.M.; Mägi, R.; Morris, A.P.; Randall, J.; Johnson, T.; Elliott, P.; Rybin, D.; Thorleifsson, G.; Steinthorsdottir, V.; Henneman, P.; Grallert, H.; Dehghan, A.; Hottenga, J.J.; Franklin, C.S.; Navarro, P.; Song, K.; Goel, A.; Perry, J.R.; Egan, J.M.; Lajunen, T.; Grarup, N.; Sparsø, T.; Doney, A.; Voight, B.F.; Stringham, H.M.; Li, M.; Kanoni, S.; Shrader, P.; Cavalcanti-Proença, C.; Kumari, M.; Qi, L.; Timpson, N.J.; Gieger, C.; Zabena, C.; Rocheleau, G.; Ingelsson, E.; An, P.; O'Connell, J.; Luan, J.; Elliott, A.; McCarroll, S.A.; Payne, F.; Roccasecca, R.M.; Pattou, F.; Sethupathy, P.; Ardlie, K.; Ariyurek, Y.; Balkau, B.; Barter, P.; Beilby, J.P.; Ben-Shlomo, Y.; Benediktsson, R.; Bennett, A.J.; Bergmann, S.; Bochud, M.; Boerwinkle, E.; Bonnefond, A.; Bonnycastle, L.L.; Borch-Johnsen, K.; Böttcher, Y.; Brunner, E.; Bumpstead, S.J.; Charpentier, G.; Chen, Y.D.; Chines, P.; Clarke, R.; Coin, L.J.; Cooper, M.N.; Cornelis, M.; Crawford, G.; Crisponi, L.; Day, I.N.; de Geus, E.J.; Delplanque, J.; Dina, C.; Erdos, M.R.; Fedson, A.C.; Fischer-Rosinsky, A.; Forouhi, N.G.; Fox, C.S.; Frants, R.; Franzosi, M.G.; Galan, P.; Goodarzi, M.O.; Graessler, J.; Groves, C.J.; Grundy, S.; Gwilliam, R.; Gyllensten, U.; Hadjadj, S.; Hallmans, G.; Hammond, N.; Han, X.; Hartikainen, A.L.; Hassanali, N.; Hayward, C.; Heath, S.C.; Hercberg, S.; Herder, C.; Hicks, A.A.; Hillman, D.R.; Hingorani, A.D.; Hofman, A.; Hui, J.; Hung, J.; Isomaa, B.; Johnson, P.R.; Jørgensen, T.; Jula, A.; Kaakinen, M.; Kaprio, J.; Kesaniemi, Y.A.; Kivimaki, M.; Knight, B.; Koskinen, S.; Kovacs, P.; Kyvik, K.O.; Lathrop, G.M.; Lawlor, D.A.; Le Bacquer, O.; Lecoeur, C.; Li, Y.; Lyssenko, V.; Mahley, R.; Mangino, M.; Manning, A.K.; Martínez-Larrad, M.T.; McAteer, J.B.; McCulloch, L.J.; McPherson, R.; Meisinger, C.; Melzer, D.; Meyre, D.; Mitchell, B.D.; Morken, M.A.; Mukherjee, S.; Naitza, S.; Narisu, N.; Neville, M.J.; Oostra, B.A.; Orrù, M.; Pakyz, R.; Palmer, C.N.; Paolisso, G.; Pattaro, C.; Pearson, D.; Peden, J.F.; Pedersen, N.L.; Perola, M.; Pfeiffer, A.F.; Pichler, I.; Polasek, O.; Posthuma, D.; Potter, S.C.; Pouta, A.; Province, M.A.; Psaty, B.M.; Rathmann, W.; Rayner, N.W.; Rice, K.; Ripatti, S.; Rivadeneira, F.; Roden, M.; Rolandsson, O.; Sandbaek, A.; Sandhu, M.; Sanna, S.; Sayer, A.A.; Scheet, P.; Scott, L.J.; Seedorf, U.; Sharp, S.J.; Shields, B.; Sigurethsson, G.; Sijbrands, E.J.; Silveira, A.; Simpson, L.; Singleton, A.; Smith, N.L.; Sovio, U.; Swift, A.; Syddall, H.; Syvänen, A.C.; Tanaka, T.; Thorand, B.; Tichet, J.; Tönjes, A.; Tuomi, T.; Uitterlinden, A.G.; van Dijk, K.W.; van Hoek, M.; Varma, D.; Visvikis-Siest, S.; Vitart, V.; Vogelzangs, N.; Waeber, G.; Wagner, P.J.; Walley, A.; Walters, G.B.; Ward, K.L.; Watkins, H.; Weedon, M.N.; Wild, S.H.; Willemsen, G.; Witteman, J.C.; Yarnell, J.W.; Zeggini, E.; Zelenika, D.; Zethelius, B.; Zhai, G.; Zhao, J.H.; Zillikens, M.C.; Borecki, I.B.; Loos, R.J.; Meneton, P.; Magnusson, P.K.; Nathan, D.M.; Williams, G.H.; Hattersley, A.T.; Silander, K.; Salomaa, V.; Smith, G.D.; Bornstein, S.R.; Schwarz, P.; Spranger, J.; Karpe, F.; Shuldiner, A.R.; Cooper, C.; Dedoussis, G.V.; Serrano-Ríos, M.; Morris, A.D.; Lind, L.; Palmer, L.J.; Hu, F.B.; Franks, P.W.; Ebrahim, S.; Marmot, M.; Kao, W.H.; Pankow, J.S.; Sampson, M.J.; Kuusisto, J.; Laakso, M.; Hansen, T.; Pedersen, O.; Pramstaller, P.P.; Wichmann, H.E.; Illig, T.; Rudan, I.; Wright, A.F.; Stumvoll, M.; Campbell, H.; Wilson, J.F.; Bergman, R.N.; Buchanan, T.A.; Collins, F.S.; Mohlke, K.L.; Tuomilehto, J.; Valle, T.T.; Altshuler, D.; Rotter, J.I.; Siscovick, D.S.; Penninx, B.W.; Boomsma, D.I.; Deloukas, P.; Spector, T.D.; Frayling, T.M.; Ferrucci, L.; Kong, A.; Thorsteinsdottir, U.; Stefansson, K.; van Duijn, C.M.; Aulchenko, Y.S.; Cao, A.; Scuteri, A.; Schlessinger, D.; Uda, M.; Ruokonen, A.; Jarvelin, M.R.; Waterworth, D.M.; Vollenweider, P.; Peltonen, L.; Mooser, V.; Abecasis, G.R.; Wareham, N.J.; Sladek, R.; Froguel, P.; Watanabe, R.M.; Meigs, J.B.; Groop, L.; Boehnke, M.; McCarthy, M.I.; Florez, J.C.; Barroso, I. , New genetic loci implicated in fasting glucose homeostasis and their impact on type 2 diabetes risk. Nature genetics 2010, 42, 105–16. [Google Scholar] [CrossRef]
- Yang, Y.; Chang, B.H.; Samson, S.L.; Li, M.V.; Chan, L. , The Krüppel-like zinc finger protein Glis3 directly and indirectly activates insulin gene transcription. Nucleic acids research 2009, 37, 2529–38. [Google Scholar] [CrossRef]
- Yang, Y.; Chan, L. , Monogenic Diabetes: What It Teaches Us on the Common Forms of Type 1 and Type 2 Diabetes. Endocrine reviews 2016, 37, 190–222. [Google Scholar] [CrossRef]
- Kang, H.S.; ZeRuth, G.; Lichti-Kaiser, K.; Vasanth, S.; Yin, Z.; Kim, Y.S.; Jetten, A.M. , Gli-similar (Glis) Krüppel-like zinc finger proteins: insights into their physiological functions and critical roles in neonatal diabetes and cystic renal disease. Histology and histopathology 2010, 25, 1481–96. [Google Scholar]
- London, S.; De Franco, E.; Elias-Assad, G.; Barhoum, M.N.; Felszer, C.; Paniakov, M.; Weiner, S.A.; Tenenbaum-Rakover, Y. , Case Report: Neonatal Diabetes Mellitus Caused by a Novel GLIS3 Mutation in Twins. Frontiers in endocrinology 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Pinto, K.; Chetty, R. , Gene of the month: GLIS1-3. Journal of clinical pathology 2020, 73, 527–530. [Google Scholar] [CrossRef] [PubMed]
- Kang, H.S.; Kim, Y.S.; ZeRuth, G.; Beak, J.Y.; Gerrish, K.; Kilic, G.; Sosa-Pineda, B.; Jensen, J.; Pierreux, C.E.; Lemaigre, F.P.; Foley, J.; Jetten, A.M. , Transcription factor Glis3, a novel critical player in the regulation of pancreatic beta-cell development and insulin gene expression. Molecular and cellular biology 2009, 29, 6366–79. [Google Scholar] [CrossRef] [PubMed]
- Scoville, D.W.; Jetten, A.M. , GLIS3: A Critical Transcription Factor in Islet β-Cell Generation. Cells 2021, 10, 3471. [Google Scholar] [CrossRef]
- De Franco, E.; Flanagan, S.E.; Houghton, J.A.L.; Allen, H.L.; Mackay, D.J.G.; Temple, I.K.; Ellard, S.; Hattersley, A.T. , The effect of early, comprehensive genomic testing on clinical care in neonatal diabetes: an international cohort study. The Lancet 2015, 386, 957–963. [Google Scholar] [CrossRef]
- Nogueira, T.C.; Paula, F.M.; Villate, O.; Colli, M.L.; Moura, R.F.; Cunha, D.A.; Marselli, L.; Marchetti, P.; Cnop, M.; Julier, C.; Eizirik, D.L. , GLIS3, a Susceptibility Gene for Type 1 and Type 2 Diabetes, Modulates Pancreatic Beta Cell Apoptosis via Regulation of a Splice Variant of the BH3-Only Protein Bim. PLoS genetics 2013, 9, e1003532. [Google Scholar] [CrossRef]
- Sun, J.; Have, C.T.; Hollensted, M.; Grarup, N.; Linneberg, A.; Pedersen, O.; Nielsen, J.S.; Rungby, J.; Christensen, C.; Brandslund, I.; Kristiansen, K.; Jun, W.; Hansen, T.; Gjesing, A.P. , Sequencing reveals protective and pathogenic effects on development of diabetes of rare GLIS3 variants. PloS one 2019, 14, e0220805. [Google Scholar] [CrossRef]
- Shakhtshneider, E.V.; Mikhailova, S.V.; Ivanoshchuk, D.E.; Orlov, P.S.; Ovsyannikova, A.K.; Rymar, O.D.; Ragino, Y.I.; Voevoda, M.I. , Polymorphism of the GLIS3 gene in a Caucasian population and among individuals with carbohydrate metabolism disorders in Russia. BMC research notes 2018, 11, 211. [Google Scholar] [CrossRef]
- Considine, R.V.; Sinha, M.K.; Heiman, M.L.; Kriauciunas, A.; Stephens, T.W.; Nyce, M.R.; Ohannesian, J.P.; Marco, C.C.; McKee, L.J.; Bauer, T.L. , Serum immunoreactive-leptin concentrations in normal-weight and obese humans. New England Journal of Medicine 1996, 334, 292–295. [Google Scholar] [CrossRef]
- Mendoza-Herrera, K.; Florio, A.A.; Moore, M.; Marrero, A.; Tamez, M.; Bhupathiraju, S.N.; Mattei, J. , The Leptin System and Diet: A Mini Review of the Current Evidence. Frontiers in endocrinology 2021, 12, 749050. [Google Scholar] [CrossRef]
- Weigle, D.S.; Breen, P.A.; Matthys, C.C.; Callahan, H.S.; Meeuws, K.E.; Burden, V.R.; Purnell, J.Q. , A high-protein diet induces sustained reductions in appetite, ad libitum caloric intake, and body weight despite compensatory changes in diurnal plasma leptin and ghrelin concentrations. The American journal of clinical nutrition 2005, 82, 41–48. [Google Scholar] [CrossRef] [PubMed]
- Katsiki, N.; Mikhailidis, D.P.; Banach, M. , Leptin, cardiovascular diseases and type 2 diabetes mellitus. Acta pharmacologica Sinica 2018, 39, 1176–1188. [Google Scholar] [CrossRef] [PubMed]
- Farooqi, I.S.; Jebb, S.A.; Langmack, G.; Lawrence, E.; Cheetham, C.H.; Prentice, A.M.; Hughes, I.A.; McCamish, M.A.; O'Rahilly, S. , Effects of Recombinant Leptin Therapy in a Child with Congenital Leptin Deficiency. New England Journal of Medicine 1999, 341, 879–884. [Google Scholar] [CrossRef] [PubMed]
- Padmanabhan, S.; Dominiczak, A.F. , Genomics of hypertension: the road to precision medicine. Nature reviews. Cardiology 2021, 18, 235–250. [Google Scholar] [CrossRef]
- Pandey, K.N. , Genetic and Epigenetic Mechanisms Regulating Blood Pressure and Kidney Dysfunction. Hypertension 2024, 81, 1424–1437. [Google Scholar] [CrossRef]
- Wilmot, E.; Idris, I. , Early onset type 2 diabetes: risk factors, clinical impact and management. Therapeutic advances in chronic disease 2014, 5, 234–44. [Google Scholar] [CrossRef]
- Qi, Q.; Forman, J.P.; Jensen, M.K.; Flint, A.; Curhan, G.C.; Rimm, E.B.; Hu, F.B.; Qi, L. , Genetic predisposition to high blood pressure associates with cardiovascular complications among patients with type 2 diabetes: two independent studies. Diabetes 2012, 61, 3026–32. [Google Scholar] [CrossRef]
- Petrie, J.R.; Guzik, T.J.; Touyz, R.M. , Diabetes, Hypertension, and Cardiovascular Disease: Clinical Insights and Vascular Mechanisms. The Canadian journal of cardiology 2018, 34, 575–584. [Google Scholar] [CrossRef]
- Shoily, S.S.; Ahsan, T.; Fatema, K.; Sajib, A.A. , Common genetic variants and pathways in diabetes and associated complications and vulnerability of populations with different ethnic origins. Scientific reports 2021, 11, 7504. [Google Scholar] [CrossRef]
- Huang, T.; Shu, Y.; Cai, Y.D. , Genetic differences among ethnic groups. BMC genomics 2015, 16, 1093. [Google Scholar] [CrossRef]
- Harper, E.; Forde, H.; Davenport, C.; Rochfort, K.D.; Smith, D.; Cummins, P.M. , Vascular calcification in type-2 diabetes and cardiovascular disease: Integrative roles for OPG, RANKL and TRAIL. Vascular pharmacology 2016, 82, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Kalra, S.S.; Shanahan, C.M. , Vascular calcification and hypertension: cause and effect. Annals of medicine 2012, 44 Suppl 1, S85–92. [Google Scholar] [CrossRef]
- Duan, P.; Tu, P.; Si, L.; Hu, W.; Liu, M.; Liu, J.; Xue, Y. , Gene Polymorphisms in the RANKL/RANK/OPG Pathway Are Associated with Type 2 Diabetes Mellitus in Southern Han Chinese Women. Genetic testing and molecular biomarkers 2016, 20, 285–90. [Google Scholar] [CrossRef] [PubMed]
- Yahagi, K.; Kolodgie, F.D.; Lutter, C.; Mori, H.; Romero, M.E.; Finn, A.V.; Virmani, R. , Pathology of Human Coronary and Carotid Artery Atherosclerosis and Vascular Calcification in Diabetes Mellitus. Arteriosclerosis, thrombosis, and vascular biology 2017, 37, 191–204. [Google Scholar] [CrossRef] [PubMed]
- Kamimura, D.; Suzuki, T.; Furniss, A.L.; Griswold, M.E.; Kullo, I.J.; Lindsey, M.L.; Winniford, M.D.; Butler, K.R.; Mosley, T.H.; Hall, M.E. , Elevated serum osteoprotegerin is associated with increased left ventricular mass index and myocardial stiffness. Journal of Cardiovascular Medicine 2017, 18, 954–961. [Google Scholar] [CrossRef] [PubMed]
- Blazquez-Medela, A.M.; Garcia-Ortiz, L.; Gomez-Marcos, M.A.; Recio-Rodriguez, J.I.; Sanchez-Rodriguez, A.; Lopez-Novoa, J.M.; Martinez-Salgado, C. , Osteoprotegerin is associated with cardiovascular risk in hypertension and/or diabetes. European journal of clinical investigation 2012, 42, 548–56. [Google Scholar] [CrossRef]
- Jasmine, M.R.; Nanda, N.; Sahoo, J.; Velkumary, S.; Pal, G.K. , Increased osteoprotegerin level is associated with impaired cardiovagal modulation in type-2 diabetic patients treated with oral antidiabetic drugs. BMC cardiovascular disorders 2020, 20, 453. [Google Scholar] [CrossRef]
- Committee, A.D.A.P.P., 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Care in Diabetes—2025. Diabetes care 2024, 48, (Supplement_1), S181-S206.
- Lemkes, B.A.; Hermanides, J.; Devries, J.H.; Holleman, F.; Meijers, J.C.; Hoekstra, J.B. , Hyperglycemia: a prothrombotic factor? Journal of thrombosis and haemostasis : JTH 2010, 8, 1663–9. [Google Scholar] [CrossRef]
- Bryk, A.H.; Prior, S.M.; Plens, K.; Konieczynska, M.; Hohendorff, J.; Malecki, M.T.; Butenas, S.; Undas, A. , Predictors of neutrophil extracellular traps markers in type 2 diabetes mellitus: associations with a prothrombotic state and hypofibrinolysis. Cardiovascular diabetology 2019, 18, 49. [Google Scholar] [CrossRef]
- Salavati, M.; Arabshomali, A.; Nouranian, S.; Shariat-Madar, Z. , Overview of Venous Thromboembolism and Emerging Therapeutic Technologies Based on Nanocarriers-Mediated Drug Delivery Systems. Molecules 2024, 29, 4883. [Google Scholar] [CrossRef]
- Picard, F.; Adjedj, J.; Varenne, O. , [Diabetes Mellitus, a prothrombotic disease]. Annales de cardiologie et d'angeiologie 2017, 66, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Baye, A.M.; Fanta, T.G.; Siddiqui, M.K.; Dawed, A.Y. , The Genetics of Adverse Drug Outcomes in Type 2 Diabetes: A Systematic Review. Frontiers in genetics 2021, 12, 675053. [Google Scholar] [CrossRef] [PubMed]
- Altshuler, D.; Hirschhorn, J.N.; Klannemark, M.; Lindgren, C.M.; Vohl, M.C.; Nemesh, J.; Lane, C.R.; Schaffner, S.F.; Bolk, S.; Brewer, C.; Tuomi, T.; Gaudet, D.; Hudson, T.J.; Daly, M.; Groop, L.; Lander, E.S. , The common PPARgamma Pro12Ala polymorphism is associated with decreased risk of type 2 diabetes. Nature genetics 2000, 26, 76–80. [Google Scholar] [CrossRef] [PubMed]
- Vella, A. , Pharmacogenetics for type 2 diabetes: practical considerations for study design. Journal of diabetes science and technology 2009, 3, 705–9. [Google Scholar] [CrossRef]
- Vella, A.; Camilleri, M. , Pharmacogenetics: potential role in the treatment of diabetes and obesity. Expert opinion on pharmacotherapy 2008, 9, 1109–19. [Google Scholar] [CrossRef]
- Zhou, K.; Yee, S.W.; Seiser, E.L.; van Leeuwen, N.; Tavendale, R.; Bennett, A.J.; Groves, C.J.; Coleman, R.L.; van der Heijden, A.A.; Beulens, J.W.; de Keyser, C.E.; Zaharenko, L.; Rotroff, D.M.; Out, M.; Jablonski, K.A.; Chen, L.; Javorský, M.; Židzik, J.; Levin, A.M.; Williams, L.K.; Dujic, T.; Semiz, S.; Kubo, M.; Chien, H.-C.; Maeda, S.; Witte, J.S.; Wu, L.; Tkáč, I.; Kooy, A.; van Schaik, R.H.N.; Stehouwer, C.D.A.; Logie, L.; Sutherland, C.; Klovins, J.; Pirags, V.; Hofman, A.; Stricker, B.H.; Motsinger-Reif, A.A.; Wagner, M.J.; Innocenti, F.; Hart, L.M. t.; Holman, R.R.; McCarthy, M.I.; Hedderson, M.M.; Palmer, C.N.A.; Florez, J.C.; Giacomini, K.M.; Pearson, E.R.; MetGen, I.; Investigators, D.P.P.; Investigators, A. , Variation in the glucose transporter gene SLC2A2 is associated with glycemic response to metformin. Nature genetics 2016, 48, 1055–1059. [Google Scholar] [CrossRef]
- Williams, L.K.; Padhukasahasram, B.; Ahmedani, B.K.; Peterson, E.L.; Wells, K.E.; González Burchard, E.; Lanfear, D.E. , Differing effects of metformin on glycemic control by race-ethnicity. The Journal of clinical endocrinology and metabolism 2014, 99, 3160–8. [Google Scholar] [CrossRef]
- www.who.int/nutrition/topics/obesity/en.
- Fruh, S.M. , Obesity: Risk factors, complications, and strategies for sustainable long-term weight management. J Am Assoc Nurse Pract 2017, (S1), S3–s14. [Google Scholar] [CrossRef]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.-P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; St-Onge, M.-P.; Lifestyle, O. b. o. t. A. H. A. C. o.; Health, C.; Cardiovascular, C. o.; Nursing, S.; Cardiology, C. o. C.; Epidemiology, C. o.; Prevention; Council, S. , Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation 2021, 143, e984–e1010. [Google Scholar] [CrossRef]
- Lin, X.; Li, H. , Obesity: Epidemiology, Pathophysiology, and Therapeutics. Frontiers in endocrinology 2021, 12, 706978. [Google Scholar] [CrossRef]
- Moini, J.; Ahangari, R.; Miller, C.; Samsam, M. , Chapter 18 - Perspective on economics and obesity. In Global Health Complications of Obesity, Moini, J.; Ahangari, R.; Miller, C.; Samsam, M., Eds. Elsevier: 2020; pp 411-423.
- Evans, M.; de Courcy, J.; de Laguiche, E.; Faurby, M.; Haase, C.L.; Matthiessen, K.S.; Moore, A.; Pearson-Stuttard, J. , Obesity-related complications, healthcare resource use and weight loss strategies in six European countries: the RESOURCE survey. International Journal of Obesity 2023, 47, 750–757. [Google Scholar] [CrossRef] [PubMed]
- Haslam, D.W.; James, W.P. , Obesity. Lancet 2005, 366, 1197–209. [Google Scholar] [CrossRef] [PubMed]
- Kahn, B.B.; Flier, J.S. , Obesity and insulin resistance. The Journal of clinical investigation 2000, 106, 473–81. [Google Scholar] [CrossRef] [PubMed]
- Ewens, K.G.; Jones, M.R.; Ankener, W.; Stewart, D.R.; Urbanek, M.; Dunaif, A.; Legro, R.S.; Chua, A.; Azziz, R.; Spielman, R.S.; Goodarzi, M.O.; Strauss, J.F. , 3rd, FTO and MC4R gene variants are associated with obesity in polycystic ovary syndrome. PloS one 2011, 6, e16390. [Google Scholar] [CrossRef]
- Wojciechowski, P.; Lipowska, A.; Rys, P.; Ewens, K.G.; Franks, S.; Tan, S.; Lerchbaum, E.; Vcelak, J.; Attaoua, R.; Straczkowski, M.; Azziz, R.; Barber, T.M.; Hinney, A.; Obermayer-Pietsch, B.; Lukasova, P.; Bendlova, B.; Grigorescu, F.; Kowalska, I.; Goodarzi, M.O.; Consortium, G.; Strauss, J.F., 3rd; McCarthy, M.I.; Malecki, M.T. , Impact of FTO genotypes on BMI and weight in polycystic ovary syndrome: a systematic review and meta-analysis. Diabetologia 2012, 55, 2636–2645. [Google Scholar] [CrossRef]
- Cauchi, S.; Stutzmann, F.; Cavalcanti-Proenca, C.; Durand, E.; Pouta, A.; Hartikainen, A.L.; Marre, M.; Vol, S.; Tammelin, T.; Laitinen, J.; Gonzalez-Izquierdo, A.; Blakemore, A.I.; Elliott, P.; Meyre, D.; Balkau, B.; Jarvelin, M.R.; Froguel, P. , Combined effects of MC4R and FTO common genetic variants on obesity in European general populations. J Mol Med (Berl) 2009, 87, 537–46. [Google Scholar] [CrossRef]
- Castillo, J.J.; Orlando, R.A.; Garver, W.S. , Gene-nutrient interactions and susceptibility to human obesity. Genes & nutrition 2017, 12, 29. [Google Scholar]
- Trang, K.; Grant, S.F.A. , Genetics and epigenetics in the obesity phenotyping scenario. Reviews in endocrine & metabolic disorders 2023, 24, 775–793. [Google Scholar]
- Lalle, G.; Lautraite, R.; Bouherrou, K.; Plaschka, M.; Pignata, A.; Voisin, A.; Twardowski, J.; Perrin-Niquet, M.; Stéphan, P.; Durget, S.; Tonon, L.; Ardin, M.; Degletagne, C.; Viari, A.; Belgarbi Dutron, L.; Davoust, N.; Postler, T.S.; Zhao, J.; Caux, C.; Caramel, J.; Dalle, S.; Cassier, P.A.; Klein, U.; Schmidt-Supprian, M.; Liblau, R.; Ghosh, S.; Grinberg-Bleyer, Y. , NF-κB subunits RelA and c-Rel selectively control CD4+ T cell function in multiple sclerosis and cancer. Journal of Experimental Medicine 2024, 221. [Google Scholar] [CrossRef]
- El-Osta, A.; Brasacchio, D.; Yao, D.; Pocai, A.; Jones, P.L.; Roeder, R.G.; Cooper, M.E.; Brownlee, M. , Transient high glucose causes persistent epigenetic changes and altered gene expression during subsequent normoglycemia. The Journal of experimental medicine 2008, 205, 2409–17. [Google Scholar] [CrossRef]
- Huang, C.; Chen, W.; Wang, X. , Studies on the fat mass and obesity-associated (FTO) gene and its impact on obesity-associated diseases. Genes Dis 2023, 10, 2351–2365. [Google Scholar] [CrossRef] [PubMed]
- Saqlain, M.; Khalid, M.; Fiaz, M.; Saeed, S.; Mehmood Raja, A.; Mobeen Zafar, M.; Fatima, T.; Bosco Pesquero, J.; Maglio, C.; Valadi, H.; Nawaz, M.; Kaukab Raja, G. , Risk variants of obesity associated genes demonstrate BMI raising effect in a large cohort. PloS one 2022, 17, e0274904. [Google Scholar] [CrossRef] [PubMed]
- Allegretti, A.S.; Zhang, W.; Zhou, W.; Thurber, T.K.; Rigby, S.P.; Bowman-Stroud, C.; Trescoli, C.; Serusclat, P.; Freeman, M.W.; Halvorsen, Y.C. , Safety and Effectiveness of Bexagliflozin in Patients With Type 2 Diabetes Mellitus and Stage 3a/3b CKD. American journal of kidney diseases : the official journal of the National Kidney Foundation 2019, 74, 328–337. [Google Scholar] [CrossRef]
- Bassett, R.L.; Gallo, G.; Le, K.-P. N.; Volino, L.R. , Bexagliflozin: a comprehensive review of a recently approved SGLT2 inhibitor for the treatment of type 2 diabetes mellitus. Medicinal Chemistry Research 2024, 33, 1354–1367. [Google Scholar] [CrossRef]
- Nauck, M.A.; D‘Alessio, D.A. , Tirzepatide, a dual GIP/GLP-1 receptor co-agonist for the treatment of type 2 diabetes with unmatched effectiveness regrading glycaemic control and body weight reduction. Cardiovascular diabetology 2022, 21, 169. [Google Scholar] [CrossRef]
- Tirzepatide (Mounjaro) for type 2 diabetes. The Medical letter on drugs and therapeutics 2022, 64, 105–107.
- Dutta, P.; Kumar, Y.; Babu, A.T.; Giri Ravindran, S.; Salam, A.; Rai, B.; Baskar, A.; Dhawan, A.; Jomy, M. , Tirzepatide: A Promising Drug for Type 2 Diabetes and Beyond. Cureus 2023, 15, e38379. [Google Scholar] [CrossRef]
- Collins, L.; Costello, R.A., Glucagon-Like Peptide-1 Receptor Agonists. In StatPearls, StatPearls Publishing.
- Copyright © 2024, StatPearls Publishing LLC.: Treasure Island (FL), 2024.
- Frampton, J.E. , Finerenone: First Approval. Drugs 2021, 81, 1787–1794. [Google Scholar] [CrossRef]
- Rico-Mesa, J.S.; White, A.; Ahmadian-Tehrani, A.; Anderson, A.S. , Mineralocorticoid Receptor Antagonists: a Comprehensive Review of Finerenone. Current cardiology reports 2020, 22, 140. [Google Scholar] [CrossRef]
- Escobar Vasco, M.A.; Fantaye, S.H.; Raghunathan, S.; Solis-Herrera, C. , The potential role of finerenone in patients with type 1 diabetes and chronic kidney disease. Diabetes, Obesity and Metabolism 2024, 26, 4135–4146. [Google Scholar] [CrossRef]
- AstraZeneca. Study of BMS-477118 as Monotherapy With Titration in Subjects With Type 2 Diabetes Who Are Not Controlled With Diet and Exercise. ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT00316082?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=9&page=1&limit=10. (accessed on 10 December 2024).
- AstraZeneca. A Phase 3 Study of BMS-477118 in Combination With Metformin in Subjects With Type 2 Diabetes Who Are Not Controlled With Diet and Exercise. ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT00327015?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=14&page=2&limit=10. (accessed on 10 December 2024).
- AstraZeneca. A Pilot Study of BMS-512148 in Subjects With Type 2 Diabetes. ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT00357370?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=3. (accessed on 10 December 2024).
- AstraZeneca. A Study of BMS-512148 (Dapagliflozin) in Patients With Type 2 Diabetes With Inadequately Controlled Hypertension on an ACEI or ARB and an Additional Antihypertensive Medication. ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT01195662?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=13&page=2&limit=10. (accessed on 10 December 2024).
- Cadila Pharnmaceuticals. Effect of CPL-2009-0031 in the Treatment of Patients With Uncontrolled Type 2 Diabetes Mellitus. ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT04801199?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=1. (accessed on 10 December 2024).
- University of Florida. Effect of a Basal/Pre-Meal Insulin Strategy (Detemir/Aspart) on Insulin Secretion and Action in Type 2 Diabetes. ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT00998335?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=24&page=3&limit=10. (accessed on 10 December 2024).
- Soo Lim. Effect of Ertugliflozin on Cardiac Function in Diabetes (ERTU-GLS). ClinicalTrials.Gov. [];2024 Available online:https://clinicaltrials.gov/study/NCT03717194?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=2. (accessed on 10 December 2024).
- Weill Medical College of Cornell University. Efficacy of Exenatide-LAR and Dapagliflozin in Overweight/Obese, Insulin Treated Patients With Type 2 Diabetes (Dexlar). ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT02811484?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=6. (accessed on 10 December 2024).
- Medical University of Vienna. Effects of Combined Dapagliflozin and Exenatide Versus Dapagliflozin and Placebo on Ectopic Lipids in Patients With Uncontrolled Type 2 Diabetes Mellitus. (EXENDA). ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT03007329?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=17&page=2&limit=10. (accessed on 10 December 2024).
- Ross, S.A.; Caballero, A.E.; Del Prato, S.; Gallwitz, B.; Lewis-D'Agostino, D.; Bailes, Z.; Thiemann, S.; Patel, S.; Woerle, H.J.; von Eynatten, M. , Linagliptin plus metformin in patients with newly diagnosed type 2 diabetes and marked hyperglycemia. Postgraduate medicine 2016, 128, 747–754. [Google Scholar] [CrossRef]
- Boehringer Ingelheim. Linagliptin and Metformin Versus Linagliptin in Newly Diagnosed, Untreated Type 2 Diabetes. ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT01512979?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=27&page=3&limit=10. (accessed on 10 December 2024).
- Roger New. Study to Evaluate the Safety and Efficacy of Oral Insulin Formulation in Type 2 Diabetes Mellitus Subjects. ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT06473662?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=15&page=2&limit=10. (accessed on 10 December 2024).
- Pfizer. Trial to Learn About the Study Medicine (PF-07081532) and Rybelsus in People With Type 2 Diabetes and Separately PF-07081532 in People With Obesity. ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT05579977?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=20&page=2&limit=10. (accessed on 10 December 2024).
- AstraZeneca. A Study Assessing Saxagliptin Treatment in Type 2 Diabetic Subjects Who Are Not Controlled With TZD Therapy Alone. ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT00295633?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=12&page=2&limit=10. (accessed on 10 December 2024).
- AstraZeneca. Study Assessing Saxagliptin Treatment In Type 2 Diabetic Subjects Who Are Not Controlled With Metformin Alone. ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT00121667?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=19&page=2&limit=10. (accessed on 10 December 2024).
- AstraZeneca. Study Assessing Saxagliptin Treatment in Subjects With Type 2 Diabetes Who Are Not Controlled With Diet and Exercise. ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT00374907?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=21&page=3&limit=10. (accessed on 10 December 2024).
- Sanofi. Effect of Soliqua 100/33 on Time in Range From Continuous Glucose Monitoring in Insulin-naive Patients With Very Uncontrolled Type 2 Diabetes Mellitus (Soli-CGM). ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT05114590?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=4. (accessed on 10 December 2024).
- Novartis Pharmaceuticals. Safety and Efficacy of Vildagliptin vs. Thiazolidinedione as add-on Therapy to Metformin in Patients With Type 2 Diabetes Not Controlled With Metformin Alone. ClinicalTrials.Gov. [];2024 Available online: https://clinicaltrials.gov/study/NCT00396227?term=New%20Antidiabetic%20Drugs,%20uncontrolled%20diabetes&rank=11&page=2&limit=10. (accessed on 10 December 2024).
Figure 1.
Spectrum of diseases can induce blood glucose alteration and lead to the development of diabetes, which plays roles in pathology.
Figure 1.
Spectrum of diseases can induce blood glucose alteration and lead to the development of diabetes, which plays roles in pathology.
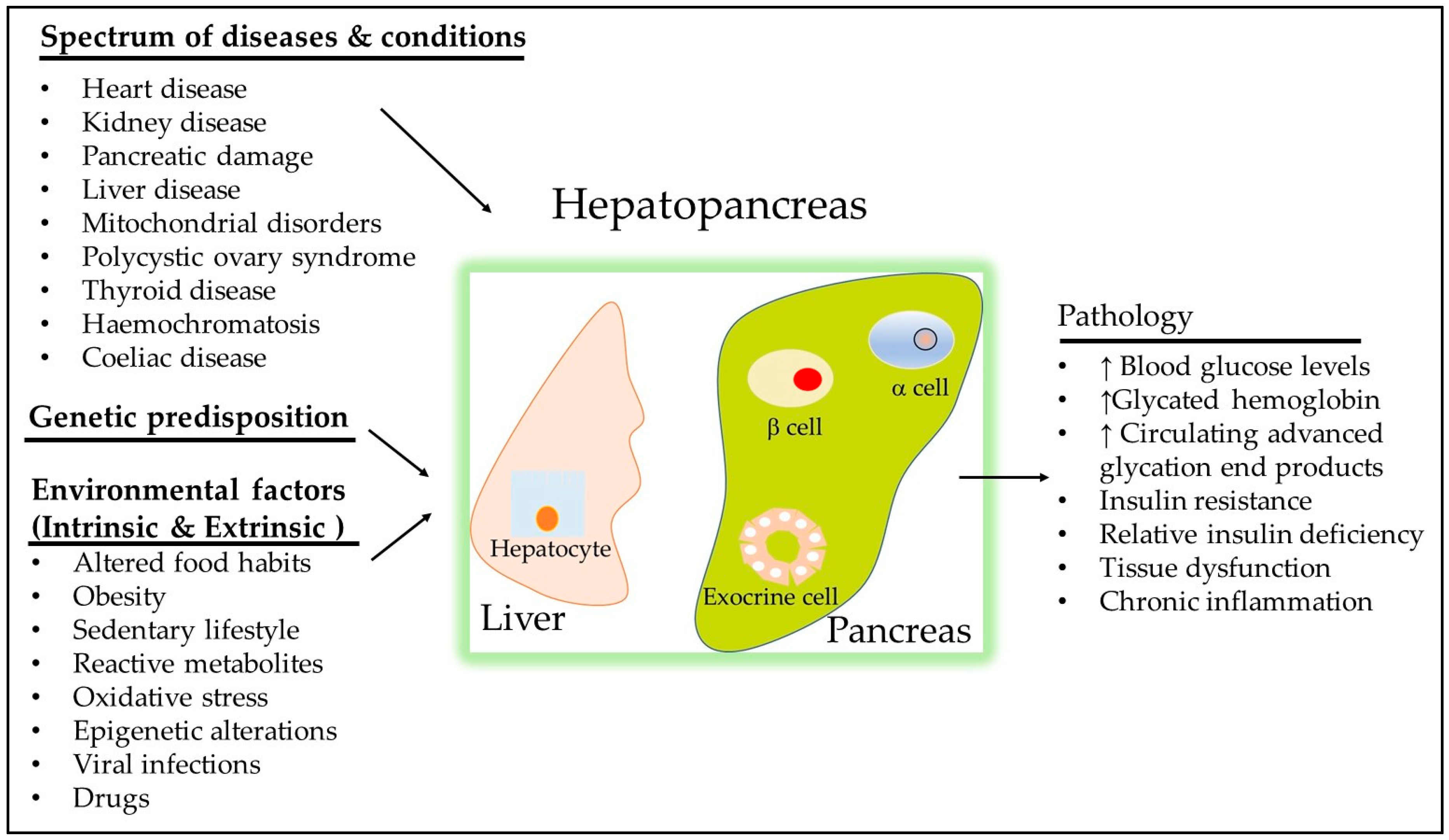
Figure 2.
Diabetes and hypertension and their common complications appear to be due a complex interaction between genetic predisposition and epigenetic factors.
Figure 2.
Diabetes and hypertension and their common complications appear to be due a complex interaction between genetic predisposition and epigenetic factors.
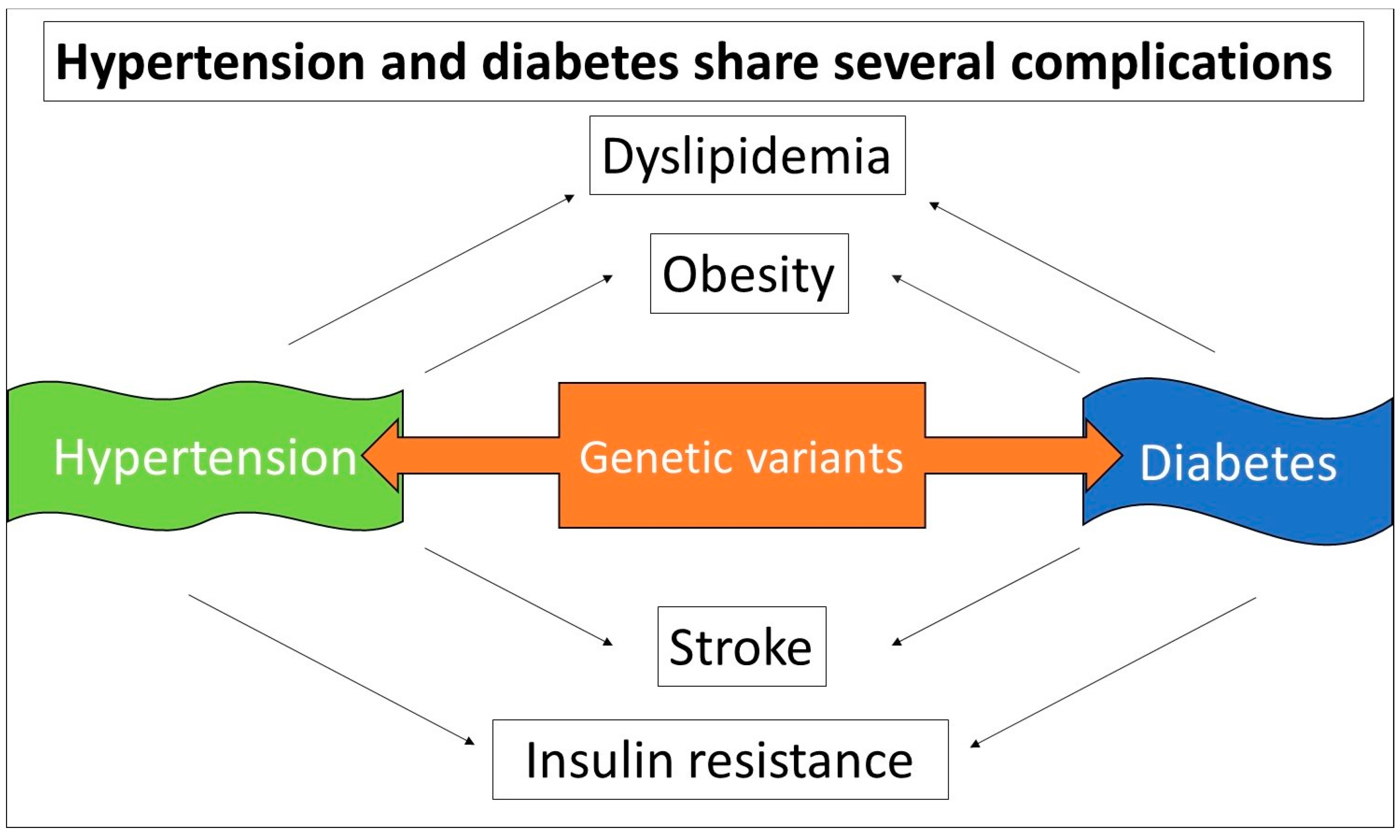
Figure 3.
Current strategies to target uncontrolled diabetic patients primarily focus on lifestyle modification combined with medications to achieve target glucose, blood pressure, and cholesterol.
Figure 3.
Current strategies to target uncontrolled diabetic patients primarily focus on lifestyle modification combined with medications to achieve target glucose, blood pressure, and cholesterol.
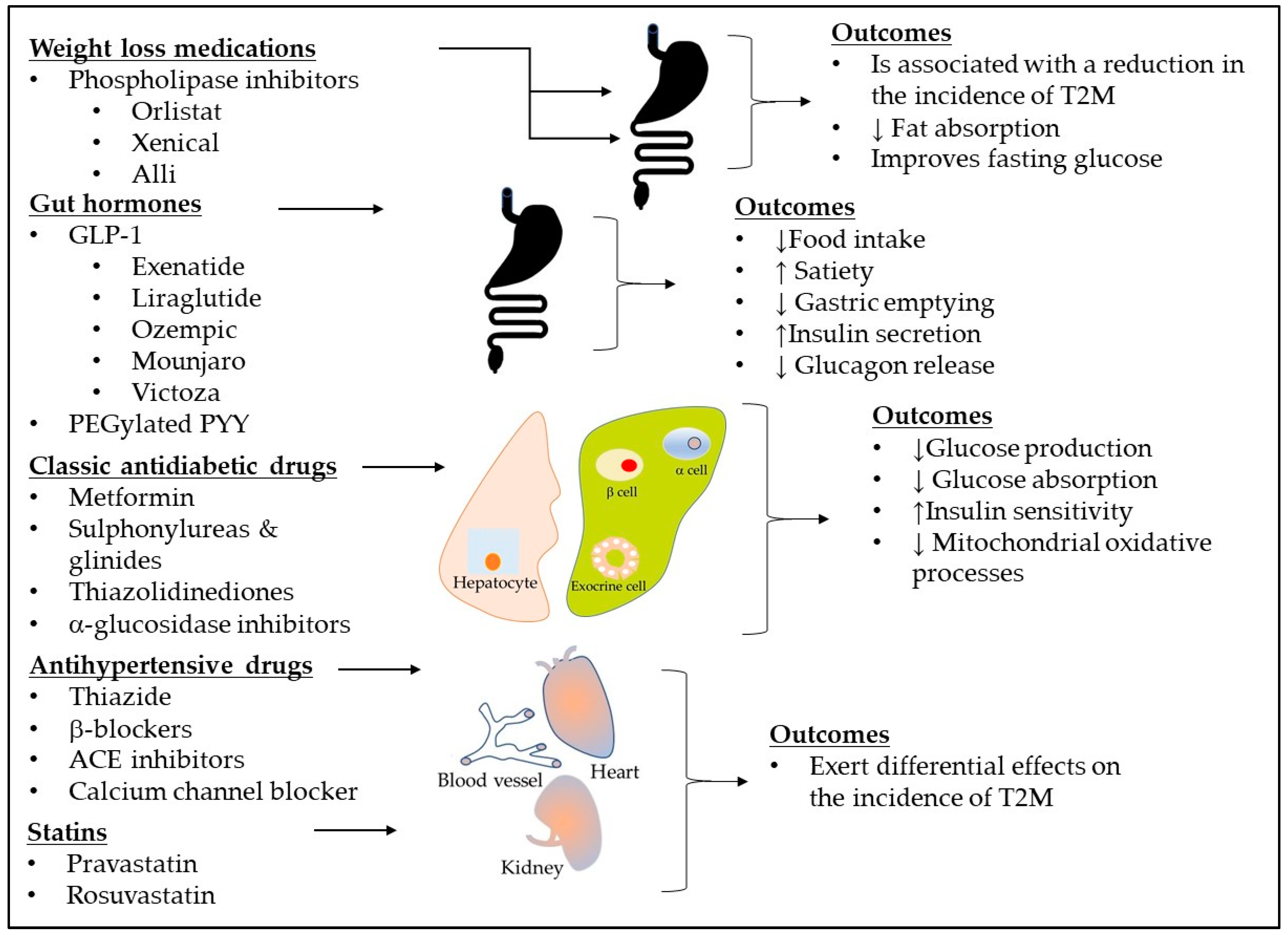

Table 1.
Diabetes genes and variants associated with T2DM based on GWAS.
|
Genes |
Major function |
Mutations or variants associated with T2DM |
References |
|---|---|---|---|
| ABCC8 | Encodes regulatory SUR1 subunits | R1420H, rare occurrence in adult | [34,35] |
| GLIS3 | A transcription factor: Regulator of islet development, insulin gene transcription, and obesity-induced compensatory β-cell proliferation |
P/LP GLIS3, rs10758593 |
[36,37] |
| HNF4A | Transcription factor for early fetal development | p.Arg114Trp | [38,39,40] |
| KCNJ11 | Encodes pore-forming inwardly-rectifying potassium channel subunits (Kir6.2) | E23K rs5215, rs5218, and rs5219 |
[41,42] |
| LEP | A regulator of appetite and energy balance | rs147287548 | [43] |
| PPAR | A transcription factor: master regulator of adipogenesis, energy balance, lipid biosynthesis, and insulin sensitivity; cellular target of TZDs |
rs4684847 rs1801282 |
[44] [45,46] |
| OPG | A decoy receptor for receptor-activator for NF-B ligand (RANKL) | rs2073618 | [47] |
Table 2.
FDA novel drug therapy approval for T2DM between 2020 and 2025.
| Conditions | Medicines | MAO | Outcomes | Side effects | Comments |
|---|---|---|---|---|---|
| T2DM | Brenzavvy (bexagliflozin) | A dual agonist for the glucagon-like peptide-1 (GLP-1) and glucose-dependent insulinotropic polypeptide (GIP) receptors | Improves hyperglycemia | It may cause ketoacidosis, a serious, potentially life-threatening complication that occurs when the body produces high levels of acids in the blood | It works similarly in Asians, Black or African Americans, and Whites adults |
| T2DM | Mounjaro (tirzepatide) | Improves blood sugar control | It may cause serious side effects including inflammation of the pancreas (pancreatitis), low blood sugar, allergic reactions, kidney problems (kidney failure), severe stomach problems, and complications of diabetes-related eye disease (diabetic retinopathy) | It works similarly in Asians, Black or African Americans, and Whites adults | |
| CKD associated T2DM | Kerendia (finerenone) | It reduced the risk of kidney failure associated with T2DM, having a heart attack or stroke, being hospitalized for heart failure, and dying from cardiovascular disease | The most common side effects included high potassium levels in the blood (hyperkalemia), low blood pressure (hypotension), and low sodium levels in the blood (hyponatremia). | No notable difference in side effects was observed by racial subgroups. |
Table 3.
New compounds and novel drugs for uncontrolled T2DM from recent clinical trials.
|
Conditions |
Compounds |
Mechanism of action |
Clinical outcomes |
Stage |
Trial registration no. |
Sponsor |
Ref. |
|---|---|---|---|---|---|---|---|
| T2DM | BMS-477118 | DPP-4 inhibitor | Phase 3 | NCT00316082 | AstraZeneca | [170,171] | |
| Diabetes | BMS-512148 (Dapagliflozin) |
A new SGLT2 inhibitor | Phase 2| Phase 3 | NCT00357370 | AstraZeneca | [172,173] | |
| Uncontrolled T2DM | CPL2009-0031 | DPP-4 inhibitor | Phase 3 | NCT04801199 | Cadila Pharnmaceuticals | [174] | |
| Uncontrolled T2DM | Detemir/Aspart | Insulin | Improved glycemic control | Phase 4 | NCT00998335 | University of Florida | [175] |
| Cardiac function in diabetes | Ertugliflozin | A new SGLT2 inhibitor | Phase 3 | NCT03717194 | Soo Lim | [176] | |
| Uncontrolled T2DM | Exenatide-LAR and Dapagliflozin | Insulin secretion/ SGLT2 inhibitor | Improved glycemic control, weight, SBP | Phase 4 | NCT0281184, NCT03007329 | Weill Medical College of Cornell University, Medical University of Vienna | [177,178] |
| Uncontrolled T2DM | Linagliptin plus metformin | DPP-4 inhibitor/ inhibiting hepatic gluconeogenesis | Improved glycemic control | Phase 4 | NCT01512979 | Boehringer Ingelheim | [179,180] |
| T2DM | Oral insulin | Insulin | Phase 2 | NCT06473662 | Roger New | [181] | |
| T2DM/Obesity | PF-07081532 | Oral small-molecule glucagon-like peptide-1 receptor agonist | Phase 2 | NCT05579977 | Pfizer | [182] | |
| T2DM | Saxagliptin | DPP-4 inhibitor | Phase 3 | NCT00295633, NCT00121667, NCT00374907 | AstraZeneca | [183,184,185] | |
| Very Uncontrolled T2DM | Soliqua 100/33 | GLP1 RA | Improved glycemic control as an adjunct to diet and exercise | Phase 4 | NCT05114590 | Sanofi | [186] |
| T2DM | Vildagliptin | DPP-4 inhibitor | Phase 3 | NCT00396227 | Novartis Pharmaceuticals | [187] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



