
Submitted:
04 February 2025
Posted:
05 February 2025
You are already at the latest version
Abstract
Background: periodontal disease is a multifactorial infectious pathology that affect dental supporting tissues, impacting the health and quality of life of patients. Assessing chewing efficiency before and after periodontal therapy is crucial to better understand its impact on the quality of life of periodontal patients. Aim: to determine whether basic periodontal therapy improves masticatory ability and efficiency in patients with mild to moderate periodontitis.
Methods: a prospective, longitudinal, case series study was carried out in 42 periodontal patients treated at the University Odontology Clinic. Masticatory efficiency before and after basic periodontal treatment was assessed using both objective (HueCheck Gum Test) and subjective (Quality of Masticatory Function questionnaire: QMFq) methods.
Results: significant improvements (P = 0.0001) were observed in periodontal variables like as hygiene index (HI), probing depth (PD), and clinical attachment level (CAL), as well as in the initial and final QMFq total score (P = 0.045). In addition, significant differences were found in post-treatment QMFq scores related to parafunctional habits (P = 0.046) and facial pattern, especially in meat consumption (P = 0.042), fruits and vegetables (P = 0.007, P = 0.044).
Conclusions: basic periodontal treatment does not improve masticatory efficiency of patients with mild-moderate periodontitis objectively, evaluated by means of the test of mixing two chewing gums, but it does subjectively.
Keywords:
Goma de mascar
; Función masticatoria
; Enfermedad periodontal
; Periodontitis
; Calidad de la función masticatoria
1. Introduction
Periodontitis is an irreversible chronic inflammation characterized by the destruction of dental support tissues (periodontal ligament and alveolar bone), the presence of periodontal pockets and gingival bleeding[1]. It can affect up to 50% of the adult population, of which 10-15% suffer the most severe variants [2]. The disease can go through several stages of insertion loss [1] which will affect the aesthetics and masticatory function of the patient and ultimately, their quality of life.
The periodontal ligament is made up of collagen fibres that connect the root of the tooth to the alveolar bone and have mechanoreceptors, responsible for sending signals to the brain about the forces exerted by the teeth when holding, biting or chewing food[3]. The loss of periodontal support as a consequence of periodontitis will alter the sensory function of the mechanoreceptors, generating specific dysfunctions in mastication, which can affect the final product of mastication[4]. In addition, there are studies that indicate that both masticatory muscles [5], as well as the bite force of the molars [6] in periodontal patients, have less activity than patients without periodontitis. All of this may result in patients avoiding tough, fibrous, and hard-to-chew foods, potentially leading to malnutrition and systemic issues [7,8] .
Evaluating the impact of periodontal disease on masticatory function and the patient's quality of life is crucial when diagnosing and treating periodontal patients. For this purpose, there are two types of methods: objective and subjective methods [9]. Objective methods assess the mixing capacity of the food bolus and provide quantitative numerical data, using techniques such as fractional sieving, spectrophotometry, glucose mediators or digital image analysis of the chewed food during a certain number of masticatory cycles. [9]. In contrast, subjective methods allow patients to express their perception of their chewing ability and quality of life, using self-assessment questionnaires, visual analogue scales, or indices based on the perceived difficulty in chewing different types of food. [10]. Although some studies have found a significant correlation between both methods [11,12,13], others determine a weak or non-existent correlation[14,15].
On the other hand, basic periodontal therapy has proven to be effective in treating periodontitis at mild to moderate stages, particularly from a clinical perspective [16], as well as the patient's quality of life (18.) However, there are very few studies that objectively assess the masticatory function of patients with mild to moderate periodontitis and whether it improves after basic periodontal treatment.
The main objective of this study is to determine whether basic periodontal treatment improves masticatory capacity and efficiency in patients with mild-moderate periodontitis, from an objective and/or subjective point of view, and whether there is any type of correlation between both methods. As a secondary objective, we intend to analyze whether variables such as gender, facial patterns or parafunctional habits influence the results obtained in terms of masticatory efficiency.
2. Material and Methods
2.1. Study Population
The present cohort study was comprised of 42 consecutive patients diagnosed with periodontitis stage II or III and grade B. The study period was from September 2023 to May 2024. The sample was selected following a nonprobabilistic sequential model. The sample was comprised of patients that seeked treatment at University Dental Clinic in the Morales Meseguer Hospital in Murcia.
2.2. Ethical Considerations
The study was approved by the research ethics committee of the University of Murcia; M10/2023/117 (ACTA3/2023/CEI). The work described has been carried out in accordance with The Code of Ethics of the World Medical Association (Declaration of Helsinki, 1964) for experiments involving humans. This is a prospective, longitudinal case series study. All patients were informed about the possible risks and benefits of the study and gave their written informed consent. Inclusion criteria included: (a) patients over 18 years old, (b) with Periodontitis Stage II or III and Grade B, (c) having signed the informed consent, (d) having at least 20 teeth in the mouth with antagonist tooth and (e) having completed the basic periodontal treatment and returning one month after the last scaling and root planing. (f) Patients had to understand and correctly complete the Quality of Masticatory Function questionnaire (QMFq). The exclusion criteria were as follows: (a) pregnancy or breastfeeding; (b) systemic disease that could modify the immune response; (c) history of nonsurgical or surgical periodontal treatment in the previous 12 months, (d) history of neoplasm or maxillofacial radiotherapy in the previous 5 years, (e) patients without periodontitis or periodontitis Stage I or IV or Grade A or C, (f) smokers and (g) patients with removable prosthesis.
2.3. Procedures
The clinical procedure was as follows: once the patient went to the Dental Clinic, a complete dental and periodontal anamnesis was performed. The patients were diagnosed as healthy, with gingivitis or periodontitis including their stages, degrees and extent[1]. In the case of periodontitis, the patient was informed of the necessary treatment and the study that we intended to perform. If the patient agreed to participate in the study and underwent nonsurgical periodontal treatment (steps 1 and 2 of the EFP S3 guideline), they received some information sheets and signed the informed consent form. Then, they were asked about the items of the QMFq (pre-treatment). After that, patient carried out the HueCheck Gum test. The recommendations of the EFP guidelines for the treatment of periodontitis stages I–III were followed. The patients were informed of their condition, instructed in oral hygiene techniques and advised on the abandonment of harmful habits (smoking). Subsequently, supragingival cleaning was performed using ultrasonic cleaner, and where pockets larger than 4 mm with bleeding or larger than 6 mm persisted, manual subgingival instrumentation was performed using a reduced set of Gracey curettes (Gracey Mini Five™ Curettes, Hu-Friedy, Chicago, E.E.U.U). The second QMFq and HueCheck Gum test (post-treatment) were completed one month after the last scaling and root planing during their periodontal re-evaluation (Figure 1).
The QMFq consists of 26 questions on the frequency of disfunction for two prior weeks and is grouped into 5 domains: foods-mastication, habits, steak, fruits, vegetables. The answers are recorded on a Likert scale, with values ranging from 0 to 4 coded as follows: 0 ‘never’ or “N/A” (not apply) if the patient had not eaten these foods, 1 ‘hardly ever’, 2 ‘occasionally’, 3 ‘fairly often’ or 4 ‘very often’ (Figure 2). Responses of the QMFq are added to give the total QMFq score and can range from 0 to 104, with a high score indicating a worse QMFq.
For the HueCheck Gum test [18], two pieces of gum, blue and pink, measuring 8x 20 x 12mm were used. These chewing gums were developed and produced by Orophys GmbH (Muri b. Bern, Switzerland). They are sugar-free, uncoated, mint-flavored gums. Their texture is similar to that of commercial chewing gum. The gum was prepared according to the original protocol [19]. Both gums were chewed at once by the patients for 20 chewing cycles. After that, the sample was collected and evaluated by means of optoelectronic analysis performed with the ViewGum® software (Figure 3), https://www.dhal.com/viewgum.htm (dHAL Software, Kifissia, Greece).
Images from the HueCheck Gum test were imported into the ViewGum® software, which analysed the colours of the gum and calculated the Variation in Hue (VOH). The software transformed the images into the HSI colour space and calculated the Hue Value for each pixel. The VOH is the measure that we used to evaluate the masticatory efficiency, and it varied in the interval [0, 1]. Values nearby to 1 corresponded to poor mastication and values closer to 0 indicated adequate mastication.
At the end of the study period, appropriate further periodontal treatment, including periodontal surgery was prescribed for those subjects who still had sites with residual probing more than 6 mm. deep and bleeding upon probing.
2.4. Statistical Analysis
The sample size was determined by previous studies[20] as well as the sample size calculator provided by Elsevier through their primary care support (https://www.fisterra.com/formacion/metodologia-investigacion/determincion-tamanomuestral (accessed on 3 September 2023). The variable used to calculate the sample size was the Hue Value for a precision of 0.15 points of difference. More specifically, for α = 0.05 and a power of 90%, a total sample minimum of 19 patients was needed. An extra 15% was added to this sample of 19 patients, resulting in a final sample size of 22 individuals. Our sample size agrees with that obtained by Halazonetis et al.[20]. Data analysis was conducted in the Statistical Package for the Social Sciences (SPSS) program, version 23.0 (SPSS, Chicago, IL, USA). All outcome variables were adjusted for normality according to the Shapiro-Wilk test. Descriptive and inferential statistics were analysed using Tukey’s exploratory data analysis and Student’s t-test for the 5 variables measured in the questionnaires: foods-mastication, habits, steak, fruits, vegetables, as well as for the total QMFq pre- y post-treatment and the Hue Value obtained by ViewGum® software. In order to assess the behaviour of the variables like as “gender”, “facial pattern” and “parafunction” in the scores on QMFq and the HueCheck Gum test, one-factor analysis of variance (ANOVA) was used. The Pearson correlation test was also applied for continuous scale variables, quantifying the strength and direction of the linear relationship between the QMFq and HueCheck Gum test. The level of significance was p< 0.05, and the mean was adjusted at 5% and 95% confidence intervals.
3. Results
Of the 42 patients initially enrolled in the study, 10 did not complete it due to non-compliance with follow-up appointments.
3.1. Comparison of the sample before and after periodontal treatment.
Statistically significant differences were found between the periodontal variables hygiene index (HI), probing depth (PD) and clinical attachment level (CAL) before and after periodontal treatment, as well as between the total score of the initial and final QMFq. (Table 1).
3.2. Behaviour of the variables “gender”, “facial pattern” and “parafunction” in the scores of QMFq and the HueCheck Gum test.
a) Gender:
No significant differences were found in the QMFq or HueCheck Gum test scores post-treatment according to the “gender” variable.
b) Facial pattern:
In the pre-treatment QMFq, statistically significant differences were found in the food group “fruit” between dolichofacial and brachyfacial patients (Table 2, Figure 4a).
In the post-treatment QMFq, statistically significant differences were found in the items “meat consumption” and “fruit” between dolichofacial patients, mesofacial and brachyfacial patients (Table 3, Figures 4b and 4c).
c) Parafunction:
3.3. Correlation between the QMFq and the HueCheck Gum Test.
No statistically significant correlation was found between the QMFq scores and the HueCheck Gum Test.
4. Discussion
There are several methods for assessing masticatory function in periodontal patients. In this study, Hue-Check Gum® was used as an objective method and the QMFq as a subjective method.
Chewing gum, like other substances used in other studies, such as gelatine gums[21] or silicones[22] allow to standardizer the method due to its specific texture and consistency [18]. In addition, it is easy to recover after chewing, allowing for a complete analysis of the samples. Among its disadvantages we can highlight that the chewing experience can differ from real chewing with natural foods[9] and may require specialized equipment to assess mixability, although free software such as ViewGum® is available for analysis[20].
The chewing gum mixing test we have employed was developed and refined by Schimmel et al[19] (2007) y Halazonetis[20]. Subsequently this test was validated by Buser et al. [18] and Schimmel[23]. It is a gum that maintains its consistency and durability over time [24]. Its hardness guarantees constant conditions in each test, increasing the reliability of the results. In addition, it maintains its properties even after one year of storage.
Schimmel et al. [23] Barbe et al. [24] or Silva et al[25] highlighting its ease of measuring and analyzing the effectiveness of chewing.
On the contrary Kapur et al. [26], Mowlana et al. [27] y Abe R et al. [28] used natural foods such as nuts, raw carrots or rice to assess masticatory function through the sieving method. These studies, although allow a more realistic evaluation of the grinding capacity, the physical properties of these foods can vary and make it difficult to standardize the analysis [9].
The QMFq, used for subjective assessment, was originally developed in French as "Questionnaire D’Alimentation "[29] and adapted by Hilasaca-Mamani et al.[30] for Brazilian teenagers. Barbe et al. [24] and Muller et al.[29] also used this questionnaire and demonstrated its reliability in the evaluation of masticatory function.
Moya-Villaescusa et al.[17] and Nagarajappa et al.[31] used other questionnaires such as 14-ítem Oral Health Impact Profile (OHIP-14) and the Oral Impacts on Daily Performance (OIDP). These questionnaires assess the impact of general oral health on the patient's daily life, but are less specific to the patient's masticatory function compared to the QMFq. Abrahamsson C et al.[32] or Pero AC et al.[33] used the Visual Analogue Scale (VAS) as a measure of the patient's masticatory function, however, it is a very general questionnaire, where no specific type of food is specified.
Regarding the results obtained, we can say that the basic periodontal treatment showed significant improvements (P = 0.0001) in all periodontal variables HI, PD and CAL, except in BoP. The HI decreased from 30.14% ± 32.71% to 13.10% ± 17.28%. The mean PD decreased from 2.46 ± 0.67 mm to 1.88 ± 0.53 mm. The CAL improved from 3.26 ± 1.19 to 2.51 ± 0.74. These results are in agreement with the clinical practice guideline on the treatment of stage I-III [16].
The lack of improvement in BoP could be due to patients improving HI by brushing thoroughly only on the day of re-evaluation, causing gingivitis due to lack of prior brushing [34]. Furthermore, re-evaluation one month after the last scaling may not be sufficient for the reconstruction of periodontal tissues, which may take up to 8 weeks [35].
Masticatory function showed significant differences (P = 0.045) in the total questionnaire scores, decreasing from 25.06 ± 18.44 to 22.63 ± 14.26. This indicated an improvement in the patient's subjective perception of masticatory function after treatment.
Similar results were obtained by Pereira et al. [36] who found significant improvements in the subjective perception of mastication after periodontal treatment. These improvements were attributed to reduced inflammation and pain, dental stabilization and possible regeneration of mechanoreceptors. However, objective data from the HueCheck Gum Test did not show significant differences before (0.59 ± 0.09) and after treatment (0.61 ± 0.11). This indicates that the patient's masticatory efficiency did not objectively improve after basic periodontal treatment.
Like us, Müller et al[29] showed that the subjective perception of chewing can be influenced by factors such as personal adaptability. On the contrary, Barbe et al[24] found a significant correlation between objective masticatory efficiency and QMFq (P = 0.037), with higher values in stage IV of periodontitis.
We consider that a certain “placebo effect” may contribute to the improvement reported by the patients, as they are undergoing treatment aimed at improving their health, which may lead them to perceive some degree of improvement.
Although there are no studies in the current literature that evaluate masticatory efficacy after periodontal treatment from an objective point of view, the results obtained by Barbe et al [24] found associations between periodontal clinical parameters and the HueCheck Gum Test in different stages of periodontitis. In the same way, Kosaka et al[21] also found that periodontal status significantly affected masticatory performance, especially in moderate periodontitis.
Regarding "gender", "facial pattern" and "parafunction", there were statistically significant differences in the variables facial pattern and parafunctional habits from a subjective point of view. In the initial QMFq, dolichofacial patients obtained significantly higher scores (P = 0.047) than brachyfacial patients in the consumption of "fruits". Post-treatment, these differences were observed in the consumption of fruits and meats. Dolichofacial patients perceived a worse chewing of fruits than mesofacial patients (P = 0.007) or brachyifacial patients (P = 0.044). Respect to meats, dolichofacial patients claimed a worse chewing than brachyfacial patients (P = 0.042). These results confirm what has been proven in another study [37], that dolichofacial patients, even if they do not have periodontal disease, are patients with weak muscles. Gomes et al. [38] also observed that dolichofacial patients have a poorer masticatory performance than meso or brachyfacial patients.
With respect to parafunction, after periodontal treatment, patients with parafunctional habits chewed significantly worse (P = 0.046) than those without parafunctional habits. This may be because parafunctional habits, such as bruxism or clenching, can produce wear facets on the teeth, abfractions, and joint and muscle problems in the patient that hinder masticatory function[39]. On the other hand, Sterenborg et al[40] concluded that, although at an individual level there could be an effect of dental wear on mastication, at the patient group level no significant relationship was found. They also suggested the possible influence of other variables such as functional occlusal units and bite force on masticatory performance.
The main limitation of the present study is the scarcity of the initial sample (N=42), which was reduced when 10 patients did not attend the periodontal re-evaluation, preventing them from performing the final QMFq and HueCheck Gum Test. Another limitation was the short follow-up period, only one month, which could be insufficient to perceive significant changes in oral health and masticatory function in patients with moderate stage II to III periodontitis. It should also be considered that many of the patients did not perceive masticatory problems before the treatment, or were not aware of them until completing the questionnaire. Another issue to highlight is that, although the QMFq was used to evaluate masticatory function, it is not validated in Spanish, which could affect the precision and reliability of the answers. In addition, the possible misunderstanding of the questionnaire can also influence the final results.
In conclusion of this work, we can say patients with mild to moderate periodontitis showed poor masticatory function. Basic periodontal treatment does not improve masticatory efficiency objectively in patients with mild to moderate periodontitis, but it does so subjectively. Facial patterns and parafunctional habits influence the patient's masticatory function. Dolichofacial patients have a lower masticatory capacity compared with mesofacial or brachyfacial patterns. There is no correlation between the objective and subjective methods used in this study to assess the masticatory function of patients.
Finally, we can conclude that both the Hue-Check Gum® and the questionnaire are easy to use and administer, do not require highly trained personnel, and the software used is free, making them suitable for use in daily clinical practice and in research.
Author Contributions
Conceptualization: S.-P.A. and M-V.M.J.; methodology: S.-P.A and J-G.A.; investigation: L-L.C. and M-V.M.J.; data curation: S-P.A and J.-G.A; writing—original draft preparation: L-L.C and M-V.M.J.—review and editing, M-V.M.J., L-L.C, S.-P.A, J.-G.A., M-C.J.M.; supervision:. S.-P.A and M.-C.J.M. All authors have contributed substantially to all four categories established by the International Committee of Medical Journal Editors.
Funding
This research did not receive any specific grants from funding agencies in the public, commercial, or not-for-profit sectors.
Conflicts of Interest
The authors declare no conflict of interest, financial or otherwise.
References
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.L.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S.; et al. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Periodontol. 2018, 89 (Suppl. 1), S1–S8. [Google Scholar] [CrossRef]
- Albandar, J.M.; Rams, T.E. Global epidemiology of periodontal diseases: an overview. Periodontology 2000 2002, 29, 7–10. [Google Scholar] [CrossRef] [PubMed]
- Johansson, A.S.; Svensson, K.G.; Trulsson, M. Impaired Masticatory Behavior in Subjects With Reduced Periodontal Tissue Support. J. Periodontol. 2006, 77, 1491–1497. [Google Scholar] [CrossRef]
- Borges, T.d.F.; Regalo, S.C.; Taba, M.; Siéssere, S.; Mestriner, W.; Semprini, M. Changes in Masticatory Performance and Quality of Life in Individuals With Chronic Periodontitis. J. Periodontol. 2013, 84, 325–331. [Google Scholar] [CrossRef] [PubMed]
- Lamba, A.K.; Tandon, S.; Faraz, F.; Garg, V.; Aggarwal, K.; Gaba, V. Effect of periodontal disease on electromyographic activity of muscles of mastication: A cross-sectional study. J. Oral Rehabilitation 2020, 47, 599–605. [Google Scholar] [CrossRef] [PubMed]
- Palinkas, M.; Borges, T.d.F.; Junior, M.T.; Monteiro, S.A.C.; Bottacin, F.S.; Mestriner-Junior, W.; Regalo, I.H.; Siessere, S.; Semprini, M.; Regalo, S.C.H. Alterations in masticatory cycle efficiency and bite force in individuals with periodontitis. Int. J. Health Sci. 2019, 13, 25–29. [Google Scholar]
- Tada, A.; Miura, H. Systematic review of the association of mastication with food and nutrient intake in the independent elderly. Arch. Gerontol. Geriatr. 2014, 59, 497–505. [Google Scholar] [CrossRef]
- Kossioni, A.E. The Association of Poor Oral Health Parameters with Malnutrition in Older Adults: A Review Considering the Potential Implications for Cognitive Impairment. Nutrients 2018, 10, 1709. [Google Scholar] [CrossRef]
- Schott Börger S, Ocaranza Tapia D, Peric Cáceres K, Yévenes López I, Romo Ormazábal F, Schulz Rosales R, et al. Métodos de Evaluación del Rendimiento Masticatorio. Una Revisión. Rev Clínica Periodoncia Implantol Rehabil Oral [Internet]. abril de 2010 [citado 3 de noviembre de 2024];3(1):51-5. Disponible en: http://linkinghub.elsevier.com/retrieve/pii/S0718539110700422.
- Palomares, T.; Montero, J.; Rosel, E.M.; Del-Castillo, R.; Rosales, J.I. Oral health-related quality of life and masticatory function after conventional prosthetic treatment: A cohort follow-up study. J. Prosthet. Dent. 2018, 119, 755–763. [Google Scholar] [CrossRef]
- Page, L.F.; Thomson, W.; Jokovic, A.; Locker, D. Validation of the Child Perceptions Questionnaire (CPQ11-14). J. Dent. Res. 2005, 84, 649–652. [Google Scholar] [CrossRef]
- Hildebrandt, G.H.; Dominguez, B.; Schork, M.; Loesche, W.J. Functional units, chewing, swallowing, and food avoidance among the elderly. J. Prosthet. Dent. 1997, 77, 588–595. [Google Scholar] [CrossRef] [PubMed]
- Hatch, J.; Shinkai, R.; Sakai, S.; Rugh, J.; Paunovich, E. Determinants of masticatory performance in dentate adults. Arch. Oral Biol. 2001, 46, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Owens, S.; Buschang, P.H.; Throckmorton, G.S.; Palmer, L.; English, J. Masticatory performance and areas of occlusal contact and near contact in subjects with normal occlusion and malocclusion. Am. J. Orthod. Dentofac. Orthop. 2002, 121, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Barbosa, T.S.; Tureli, M.C.M.; Gavião, M.B.D. Validity and reliability of the Child Perceptions Questionnaires applied in Brazilian children. BMC Oral Heal. 2009, 9, 13–13. [Google Scholar] [CrossRef]
- Sanz M, Herrera D, Kebschull M, Chapple I, Jepsen S, Berglundh T, et al. Treatment of stage I–III periodontitis—The EFP S3 level clinical practice guideline. J Clin Periodontol [Internet]. julio de 2020 [citado 16 de septiembre de 2024];47(Suppl 22):4-60. Disponible en: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7891343/.
- Moya-Villaescusa, M.J.; Sánchez-Pérez, A.; Esparza-Marín, J.; Jornet-García, A.; Montoya-Carralero, J.M. Periodontal Disease and Nonsurgical Periodontal Therapy on the OHRQoL of the Patient: A Pilot Study of Case Series. Dent. J. 2023, 11, 94. [Google Scholar] [CrossRef]
- Buser, R.; Ziltener, V.; Samietz, S.; Fontolliet, M.; Nef, T.; Schimmel, M. Validation of a purpose-built chewing gum and smartphone application to evaluate chewing efficiency. J. Oral Rehabilitation 2018, 45, 845–853. [Google Scholar] [CrossRef]
- Schimmel, M.; Christou, P.; Herrmann, F.; Müller, F. A two-colour chewing gum test for masticatory efficiency: development of different assessment methods. J. Oral Rehabilitation 2007, 34, 671–678. [Google Scholar] [CrossRef]
- Halazonetis, D.J.; Schimmel, M.; Antonarakis, G.S.; Christou, P. Novel software for quantitative evaluation and graphical representation of masticatory efficiency. J. Oral Rehabilitation 2013, 40, 329–335. [Google Scholar] [CrossRef]
- Kosaka, T.; Ono, T.; Yoshimuta, Y.; Kida, M.; Kikui, M.; Nokubi, T.; Maeda, Y.; Kokubo, Y.; Watanabe, M.; Miyamoto, Y. The effect of periodontal status and occlusal support on masticatory performance: the Suita study. J. Clin. Periodontol. 2014, 41, 497–503. [Google Scholar] [CrossRef]
- van der Bilt, A.; van der Glas, H.; Mowlana, F.; Heath, M. A comparison between sieving and optical scanning for the determination of particle size distributions obtained by mastication in man. Arch. Oral Biol. 1993, 38, 159–162. [Google Scholar] [CrossRef]
- Schimmel, M.; Christou, P.; Miyazaki, H.; Halazonetis, D.; Herrmann, F.R.; Müller, F. A novel colourimetric technique to assess chewing function using two-coloured specimens: Validation and application. J. Dent. 2015, 43, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Barbe, A.G.; Javadian, S.; Rott, T.; Scharfenberg, I.; Deutscher, H.C.D.; Noack, M.J.; Derman, S.H.M. Objective masticatory efficiency and subjective quality of masticatory function among patients with periodontal disease. J. Clin. Periodontol. 2020, 47, 1344–1353. [Google Scholar] [CrossRef]
- Silva, L.C.; Nogueira, T.E.; Rios, L.F.; Schimmel, M.; Leles, C.R. Reliability of a two-colour chewing gum test to assess masticatory performance in complete denture wearers. J. Oral Rehabilitation 2018, 45, 301–307. [Google Scholar] [CrossRef] [PubMed]
- Kapur KK, Soman SD. Masticatory performance and efficiency in denture wearers. 1964. J Prosthet Dent. junio de 2006;95(6):407-11.
- Mowlana, F.; Heath, M.; VAN DER Bilt, A.; VAN DER Glas, H. Assessment of chewing efficiency: a comparison of particle size distribution determined using optical scanning and sieving of almonds. J. Oral Rehabilitation 1994, 21, 545–551. [Google Scholar] [CrossRef]
- Abe, R.; Furuya, J.; Suzuki, T. Videoendoscopic measurement of food bolus formation for quantitative evaluation of masticatory function. J. Prosthodont. Res. 2011, 55, 171–178. [Google Scholar] [CrossRef] [PubMed]
- Muller, K.; Morais, J.; Feine, J. Nutritional and anthropometric analysis of edentulous patients wearing implant overdentures or conventional dentures. Braz. Dent. J. 2008, 19, 145–150. [Google Scholar] [CrossRef]
- Hilasaca-Mamani, M.; Barbosa, T.d.S.; Fegadolli, C.; Castelo, P.M. Validity and reliability of the quality of masticatory function questionnaire applied in Brazilian adolescents. CoDAS 2016, 28, 149–154. [Google Scholar] [CrossRef]
- Nagarajappa, R.; Batra, M.; Sanadhya, S.; Daryani, H.; Ramesh, G. Oral impacts on daily performance: Validity, reliability and prevalence estimates among Indian adolescents. Int. J. Dent. Hyg. 2017, 16, 279–285. [Google Scholar] [CrossRef]
- Abrahamsson C, Henrikson T, Bondemark L, Ekberg E. Masticatory function in patients with dentofacial deformities before and after orthognathic treatment-a prospective, longitudinal, and controlled study. Eur J Orthod. febrero de 2015;37(1):67-72.
- Pero, A.C.; Scavassin, P.M.; Policastro, V.B.; Júnior, N.M.d.O.; Marin, D.O.M.; da Silva, M.D.D.; Cassiano, A.F.B.; Santana, T.d.S.; Compagnoni, M.A. Masticatory function in complete denture wearers varying degree of mandibular bone resorption and occlusion concept: canine-guided occlusion versus bilateral balanced occlusion in a cross-over trial. J. Prosthodont. Res. 2019, 63, 421–427. [Google Scholar] [CrossRef]
- Murakami S, Mealey BL, Mariotti A, Chapple ILC. Dental plaque-induced gingival conditions. J Periodontol. junio de 2018;89 Suppl 1:S17-27.
- Díaz BF, Pomarino SG. Reevaluación del paciente periodontal: intervalo de tiempo adecuado para reevaluar sus parámetros. Acta Odontológica Colomb [Internet]. 1 de julio de 2017 [citado 3 de noviembre de 2024];7(2):65-71. Disponible en: https://revistas.unal.edu.co/index.php/actaodontocol/article/view/66373.
- Pereira, L.J.; Gazolla, C.M.; Magalhães, I.B.; Dominguete, M.H.L.; Vilela, G.R.; Castelo, P.M.; Marques, L.S.; Van Der Bilt, A. Influence of periodontal treatment on objective measurement of masticatory performance. J. Oral Sci. 2012, 54, 151–157. [Google Scholar] [CrossRef]
- Ingervall, B.; Bitsanis, E. A pilot study of the effect of masticatory muscle training on facial growth in long-face children. Eur. J. Orthod. 1987, 9, 15–23. [Google Scholar] [CrossRef] [PubMed]
- Gomes, S.G.F.; Custodio, W.; Faot, F.; Cury, A.A.D.B.; Garcia, R.C.M.R. Masticatory features, EMG activity and muscle effort of subjects with different facial patterns. J. Oral Rehabilitation 2010, 37, 813–819. [Google Scholar] [CrossRef] [PubMed]
- Paulino MR, Moreira VG, Lemos GA, Silva PLP da, Bonan PRF, Batista AUD. Prevalence of signs and symptoms of temporomandibular disorders in college preparatory students: associations with emotional factors, parafunctional habits, and impact on quality of life. Cienc Saude Coletiva. enero de 2018;23(1):173-86.
- Sterenborg, B.A.; Kalaykova, S.I.; Loomans, B.A.; Huysmans, M.-C.D. Impact of tooth wear on masticatory performance. J. Dent. 2018, 76, 98–101. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Outline of the patient visit protocol, treatments performed, and variables recorded. PPD: probing pocket depth; CAL: clinical attachment level; REC: recession; HI: hygiene index; BoP: bleeding on probing; Dx: diagnosis; QMFq: Quality of Masticatory function questionnaire; OHI: oral hygiene instruction.
Figure 1.
Outline of the patient visit protocol, treatments performed, and variables recorded. PPD: probing pocket depth; CAL: clinical attachment level; REC: recession; HI: hygiene index; BoP: bleeding on probing; Dx: diagnosis; QMFq: Quality of Masticatory function questionnaire; OHI: oral hygiene instruction.

Figure 2.
Quality of Masticatory Function questionnaire (QMFq).
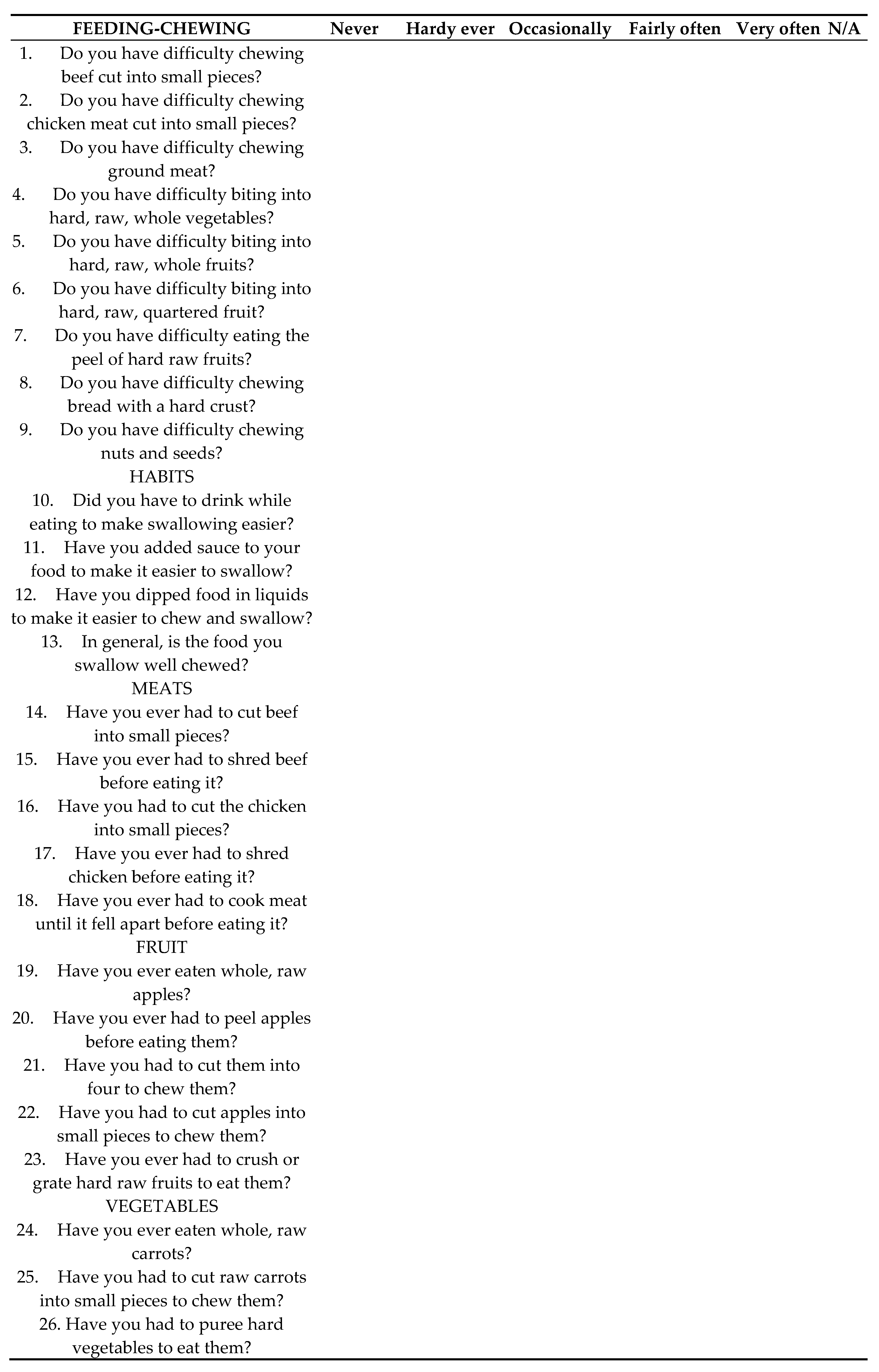
Figure 3.
ViewGum® Software (dHAL Software, Kifissia, Greece) for optoelectronic analysis of the samples.
Figure 3.
ViewGum® Software (dHAL Software, Kifissia, Greece) for optoelectronic analysis of the samples.
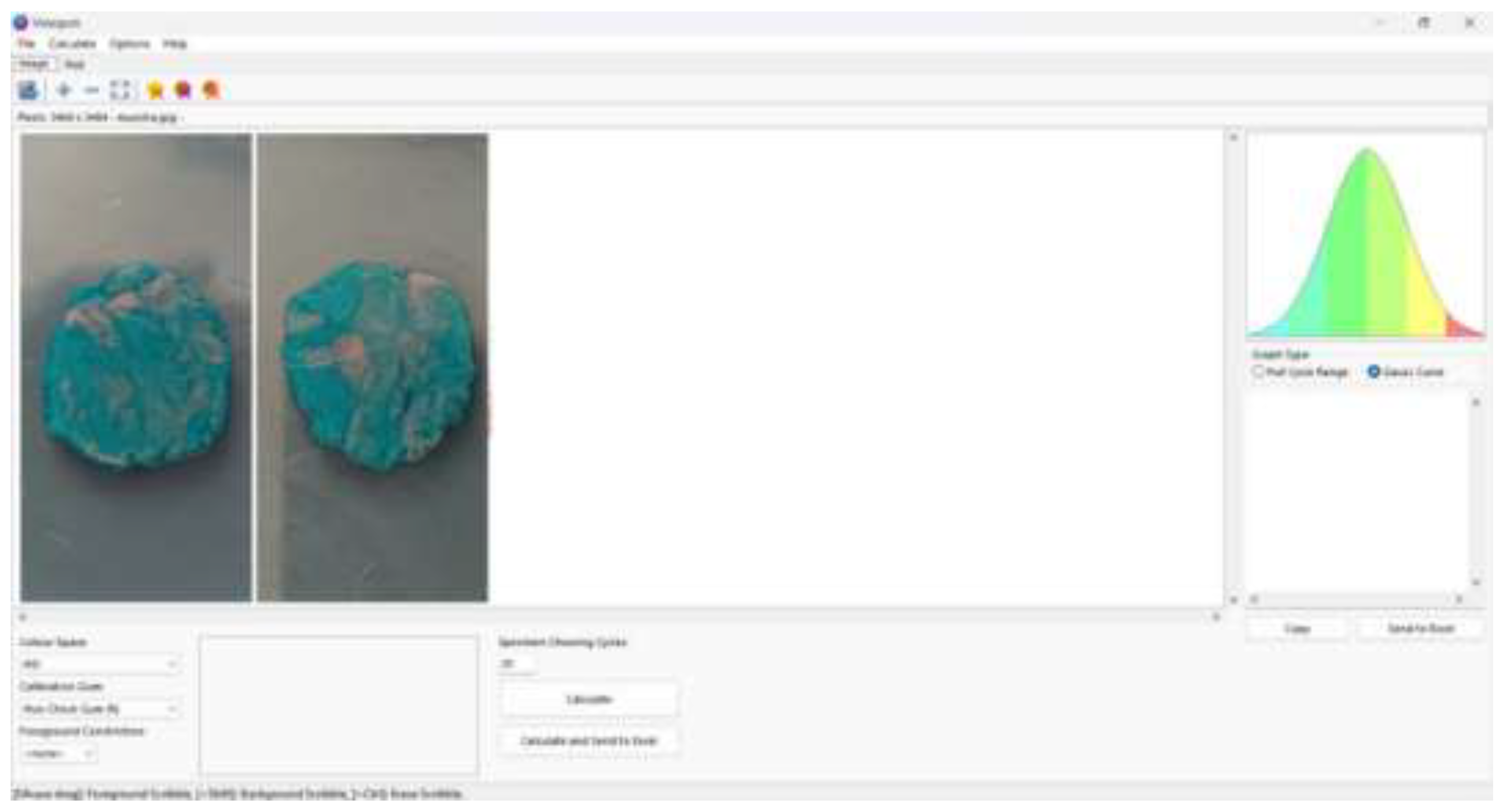
Figure 4.
Graphical representation of the mean scores obtained in the “fruit” items (a) of pre-treatment QMFq and “meats” (b) and “fruits” (c) items of post-treatment QMFq, according to the different facial patterns.
Figure 4.
Graphical representation of the mean scores obtained in the “fruit” items (a) of pre-treatment QMFq and “meats” (b) and “fruits” (c) items of post-treatment QMFq, according to the different facial patterns.
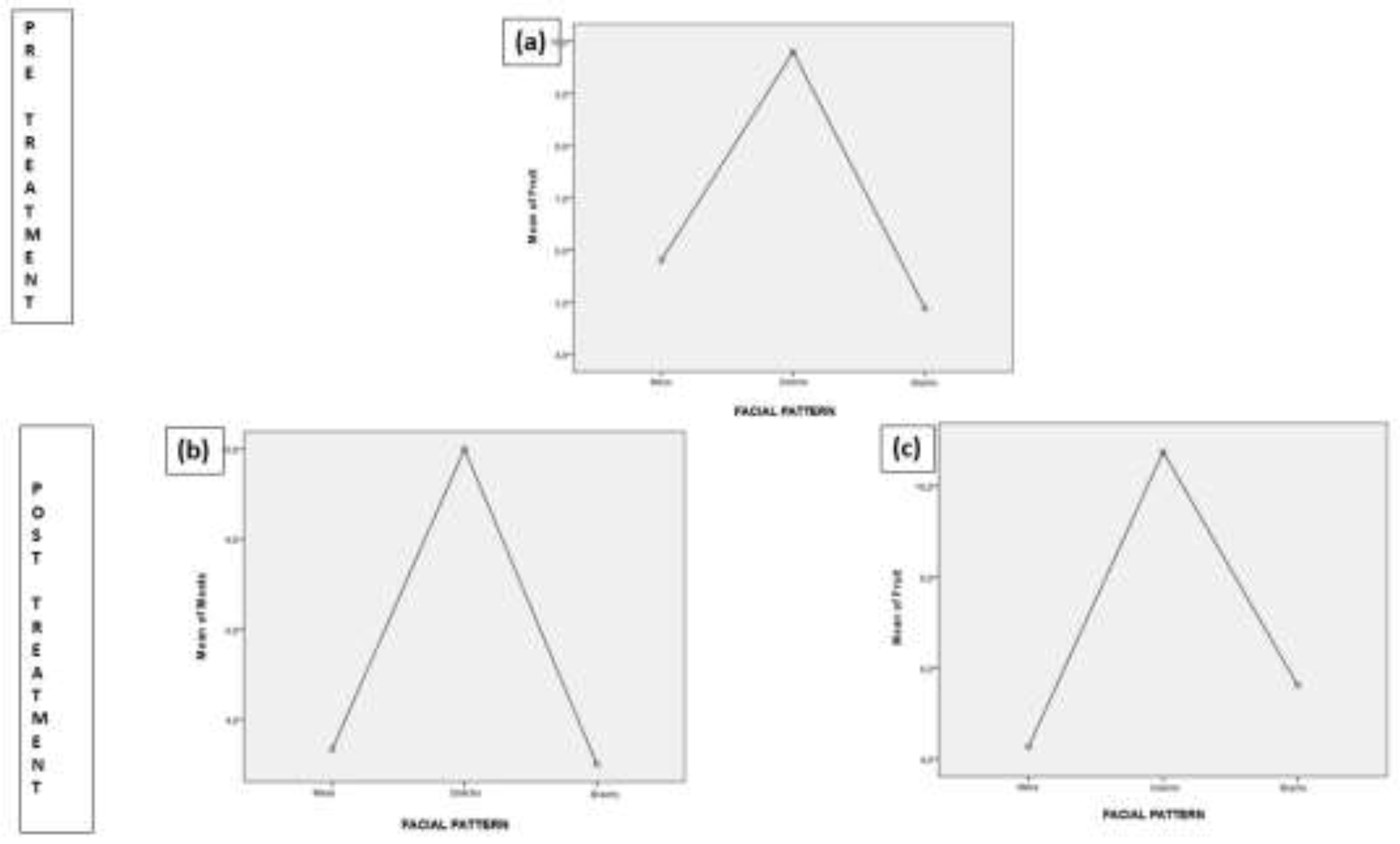
Figure 5.
Graphical representation of the mean scores obtained in “vegetables” items of post-treatment QMFq, according to the presence or absence of parafunction.
Figure 5.
Graphical representation of the mean scores obtained in “vegetables” items of post-treatment QMFq, according to the presence or absence of parafunction.
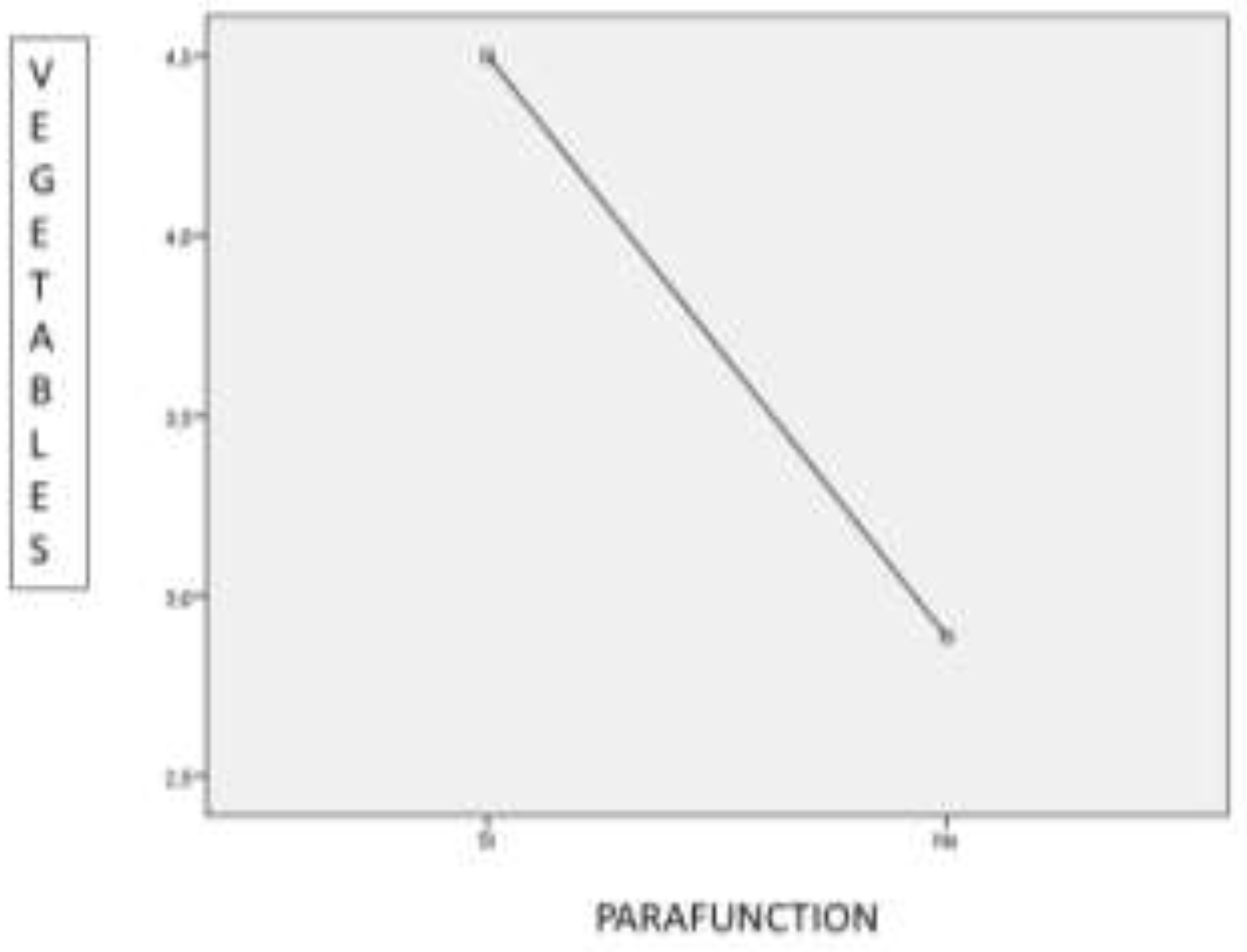

Table 1.
Comparison between periodontal variables and questionnaire before and after periodontal treatment.
Table 1.
Comparison between periodontal variables and questionnaire before and after periodontal treatment.
| Variable. | Initial (Mean ± SD) | Final (Mean ± SD) | Significance (p-value) |
|---|---|---|---|
| HI | 30.1466 ± 32.70924 | 13.0962 ± 17.27574 | 0.0001 |
| PD | 2.4594 ± 0.67493 | 1.8806 ± 0.5332 | 0.0001 |
| CAL | 3.2647 ± 1.18767 | 2.505 ± 0.73897 | 0.0001 |
| Total score QMFq | 25.063 ± 18.4355 | 22.625 ± 14.2574 | 0.045 |
HI: hygiene index; PD: probing depth; CAL: clinical attachment level; QMFq: quality of masticatory function questionnaire.
Table 2.
Degree of significance of the differences between the groups separated by “facial pattern”, with respect to the total pre-treatment sample.
Table 2.
Degree of significance of the differences between the groups separated by “facial pattern”, with respect to the total pre-treatment sample.
| Dependent Variable. | (I) FACIAL PATTERN | (J) FACIAL PATTERN | Mean Difference (I-J) | Standard Error | Sig. | 95% Confidence Interval | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| FRUIT | Dolichofacial | Mesofacial | 4 | 1,9111 | 0,129 | -0,781 | 8,781 |
| Brachyfacial | 4,9176* | 1,9445 | 0,047 | 0,053 | 9,782 | ||
Table 3.
Degree of significance of the differences between the groups separated by “facial pattern” and with respect to the total post-treatment sample.
Table 3.
Degree of significance of the differences between the groups separated by “facial pattern” and with respect to the total post-treatment sample.
| Dependent Variable | (I) FACIAL PATTERN | (J) FACIAL PATTERN | Mean Difference (I-J) | Standard Error | Sig. | 95% Confidence Interval | |
|---|---|---|---|---|---|---|---|
| Lower Bound | Upper Bound | ||||||
| MEATS | Dolichofacial | Mesofacial | 6,6667 | 2,6298 | 0,051 | -0,015 | 13,349 |
| Brachyfacial | 7,0000* | 2,672 | 0,042 | 0,211 | 13,789 | ||
| FRUITS | Dolichofacial | Mesofacial | 6,4833* | 1,9459 | 0,007 | 1,539 | 11,428 |
| Brachyfacial | 5,1346* | 1,9771 | 0,044 | 0,111 | 10,158 | ||
Table 4.
Degree of significance of the differences between the groups separated by “parafunction” and with respect to the total sample in relation to the scores of the QMFq post-treatment.
Table 4.
Degree of significance of the differences between the groups separated by “parafunction” and with respect to the total sample in relation to the scores of the QMFq post-treatment.
| ANOVA | ||||||
|---|---|---|---|---|---|---|
| Sum of Squares | df | Mean Square | F | Sig. | ||
| VEGETABLES | Between Groups | 12,721 | 1 | 12,721 | 4,329 | 0,046 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



