
Submitted:
11 February 2025
Posted:
12 February 2025
You are already at the latest version
Abstract
An abnormal accumulation of misfolded proteins is a common feature shared by most neurodegenerative disorders. Olfactory dysfunction (OD) is common in elderly population and is present in 90% of patients with Alzheimer’s or Parkinson’s disease, usually preceding the cognitive and motor symptoms onset by several years. Early Aβ, tau and α-synuclein protein aggregates have been observed in brain structures involved in odor processing (olfactory bulb and tract, piriform cortex, amygdala, entorhinal cortex, and hippocampus) and seem to underly OD. Glymphatic system is a glial-associated fluid transport system that facilitates the movement of CSF and ISF and removes brain waste during specific brain waste sleep stages. Noteworthy, glymphatic system became less functional in aging and is impaired in several conditions, including neurodegenerative diseases. As the nasal pathway has been recently described as the main outflow pathway of cerebrospinal fluid and solutes, we hypothesized that OD may be indeed a clinical marker of early glymphatic dysfunction that entails abnormal accumulation of pathological proteins in olfactory structures. Here we review the physiological, anatomical, and chronological evidence supporting this suggestion. If this hypothesis is confirmed, olfactory dysfunction could be considered as a clinical proxy of glymphatic dysfunction in neurodegenerative diseases.
Keywords:
1. Introduction
2. Olfactory Dysfunction in Neurodegenerative Diseases
2.1. OD in Preclinical Alzheimer's Disease
2.2. OD in Prodromal Lewy Bodies Diseases
3. Glymphatic System and Its Failure in Neurodegenerative Diseases
4. Menopause, Olfactory Dysfunction, and Glymphatic Failure
5. Olfactory Dysfunction as a Clinical Marker of Glymphatic Failure in Neurodegenerative Disease
- 1)
- Olfactory structures show early protein aggregation. Early Aβ, tau and α-synuclein protein aggregates have been observed in the olfactory bulb, olfactory epithelium, piriform cortex, the glomerular layer, anterior olfactory nucleus, and olfactory tubercle [74,75,76]. In LBD, the olfactory bulbs are an initial site of α- synuclein aggregation [34]. Neuropil threads and neurofibrillary tangles of tau protein have been observed in the olfactory bulb and olfactory nerve in all cases of definite AD, as well as in many cases of probable AD, MCI, and even cognitively normal aging [77,78]. Moreover, in healthy elderly population, primary age-related tauopathy typically concentrates in the medial temporal lobe and olfactory regions, including the olfactory bulb, transentorhinal region, and entorhinal cortex [79,80].
- 2)
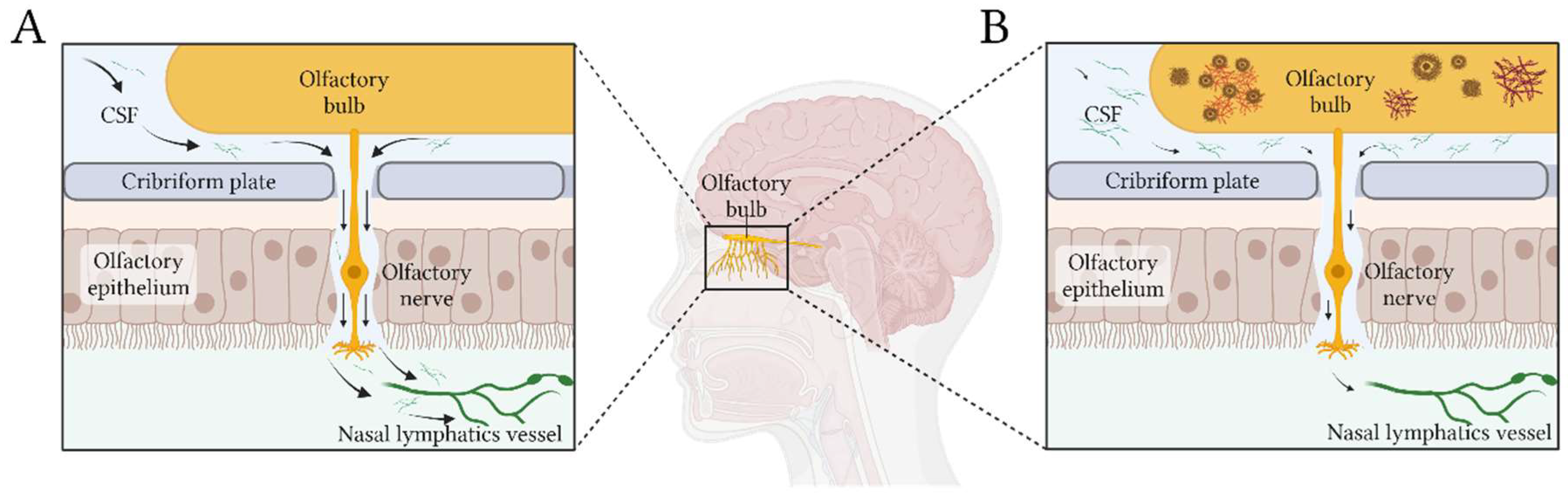
- Nasal pathway is the main CSF egress from the brain. CSF is primarily cleared along olfactory nerves that traverse the cribriform plate, draining into lymphatic vessels in the nasal mucosa [81]. De Leon and colleagues demonstrated using dynamic PET that, as in other mammals, human nasal turbinates are part of the CSF egress system [82]. They also observed that such clearance measures were 66% lower in AD patients. Using a different technique -serial MRI after an intrathecal contrast injection- Zhou et al found concordant results [4]. They observed drainage of CSF to the turbinates via the cribriform plate along olfactory nerve, this being the main egress pathway. Moreover, clearance function through the peri-olfactory inferior turbinate pathway was diminished with aging, and was associated with cognitive function and reported sleep quality. Figure 1 depicts the physiological CSF egress through perineural olfactory pathway (1A), and the pathological protein aggregation associated with diminished clearance (1B).
- 3)
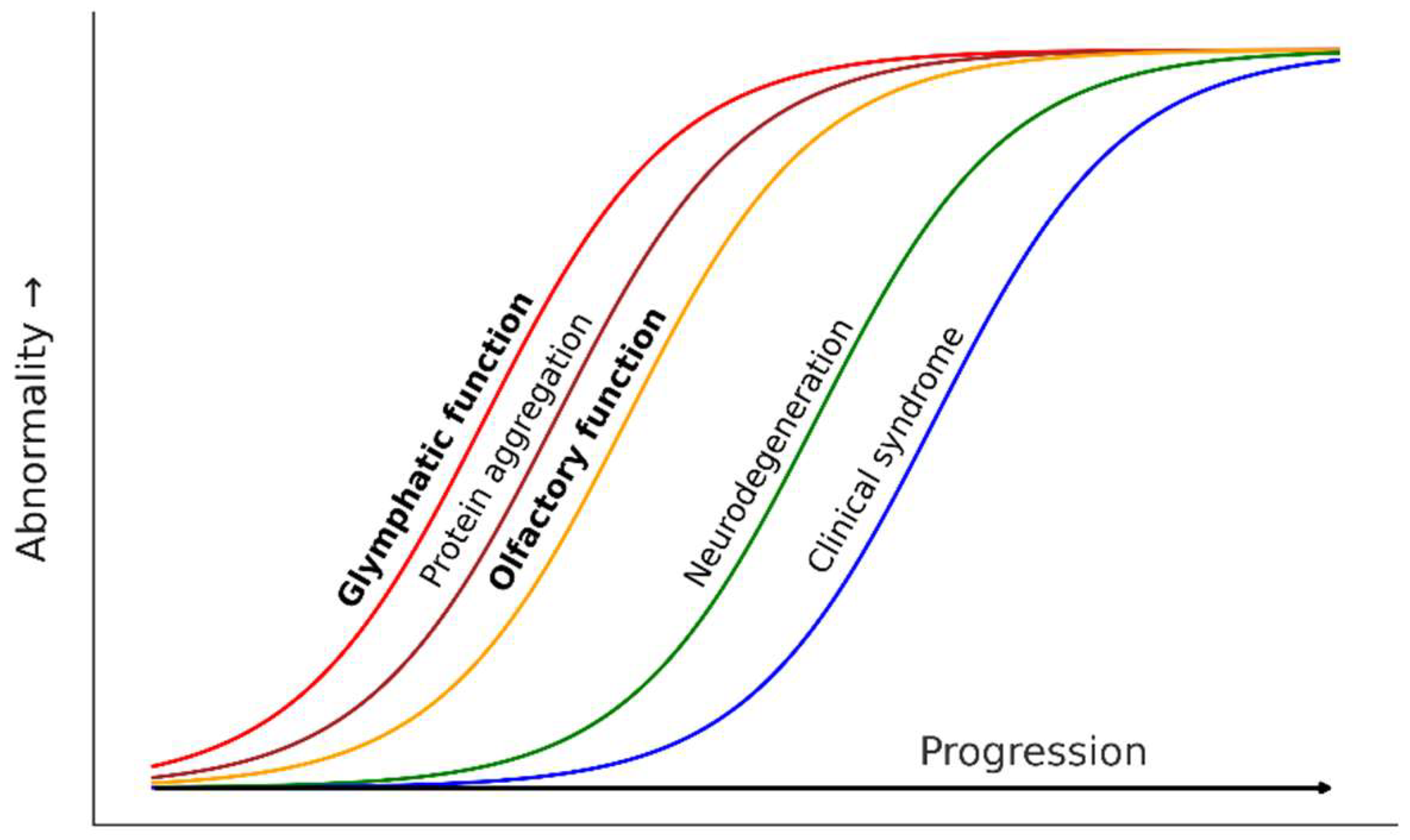
- Glymphatic failure seems to be a very early event in neurodegenerative diseases. Recent evidence suggested that glymphatic function is affected very early in AD. Using DTI along perivascular spaces (ALPS), a neuroimaging proxy of glymphatic function, two large longitudinal studies found that ALPS index becomes abnormal in individuals with subjective cognitive decline (SCD), before objective cognitive impairment can be detected [83,84]. Moreover, lower ALPS index predicts accelerated Aβ PET burden and AD signature ROI thinning, higher risk of amyloid-positive transition, and faster cognitive decline [83]. Based on such evidence, Huang et al proposed a hypothetical cascade model of pathological events in AD, in which reduction of ALPS index would be the first biomarker to change. The evidence in LBD is similar. Using also DTI-ALPS index, Bae et al found that glymphatic function was diminished in RBD patients, and that lower ALPS index predicted phenoconversion to PD [85]. Accordingly, they concluded that glymphatic impairment is presumed to start at the preclinical stage of PD.
- 4)
- Olfactory dysfunction is associated with loss of estrogen after menopause and parallels glymphatic-related events. Olfactory dysfunction in postmenopausal women seems linked to estrogen loss, paralleling glymphatic dysfunction. Estrogen influences LC-NA regulation, sleep, and vascular function, all of which are critical for glymphatic clearance[59]. Sleep disturbances and abnormal blood pressure patterns, both prevalent after menopause, further compromise glymphatic efficiency and may contribute to AD risk. Experimental and neuroimaging studies support estrogen’s role in olfactory function, suggesting that its decline may accelerate neurodegenerative processes.
6. Concluding Remarks
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Iliff, J.J.; Wang, M.; Liao, Y.; Plogg, B.A.; Peng, W.; Gundersen, G.A.; Benveniste, H.; Vates, G.E.; Deane, R.; Goldman, S.A.; et al. A Paravascular Pathway Facilitates CSF Flow through the Brain Parenchyma and the Clearance of Interstitial Solutes, Including Amyloid β. Sci Transl Med 2012, 4. [Google Scholar] [CrossRef]
- Nedergaard, M.; Goldman, S.A. Glymphatic Failure as a Final Common Pathway to Dementia. Science (1979) 2020, 370, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Fatuzzo, I.; Niccolini, G.F.; Zoccali, F.; Cavalcanti, L.; Bellizzi, M.G.; Riccardi, G.; de Vincentiis, M.; Fiore, M.; Petrella, C.; Minni, A.; et al. Neurons, Nose, and Neurodegenerative Diseases: Olfactory Function and Cognitive Impairment. Int J Mol Sci 2023, 24, 2117. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Ran, W.; Luo, Z.; Wang, J.; Fang, M.; Wei, K.; Sun, J.; Lou, M. Impaired Peri-Olfactory Cerebrospinal Fluid Clearance Is Associated with Ageing, Cognitive Decline and Dyssomnia. EBioMedicine 2022, 86, 104381. [Google Scholar] [CrossRef] [PubMed]
- Doty, R.L.; Kamath, V. The Influences of Age on Olfaction: A Review. Front Psychol 2014, 5. [Google Scholar] [CrossRef]
- Schubert, C.R.; Cruickshanks, K.J.; Fischer, M.E.; Huang, G.-H.; Klein, B.E.K.; Klein, R.; Pankow, J.S.; Nondahl, D.M. Olfactory Impairment in an Adult Population: The Beaver Dam Offspring Study. Chem Senses 2012, 37, 325–334. [Google Scholar] [CrossRef]
- Man, R.E.K.; Wong, C.M.J.; Gupta, P.; Fenwick, E.K.; Aravindhan, A.; Teo, N.W.Y.; Charn, T.C.; Forde, C.; Lamoureux, E.L. Understanding the Prevalence and Risk Factor Profile of Olfactory Impairment and Its Impact on Patient Health Indicators and Economic Outcomes in Community-Dwelling Older Asian Adults. Innov Aging 2024, 8. [Google Scholar] [CrossRef]
- Murphy, C.; Schubert, C.R.; Cruickshanks, K.J.; Klein, B.E.K.; Klein, R.; Nondahl, D.M. Prevalence of Olfactory Impairment in Older Adults. JAMA 2002, 288, 2307–2312. [Google Scholar] [CrossRef]
- Attems, J.; Walker, L.; Jellinger, K.A. Olfaction and Aging: A Mini-Review. Gerontology 2015, 61, 485–490. [Google Scholar] [CrossRef]
- Uchida, S.; Shimada, C.; Sakuma, N.; Kagitani, F.; Kan, A.; Awata, S. The Relationship between Olfaction and Cognitive Function in the Elderly. J Physiol Sci 2020, 70, 48. [Google Scholar] [CrossRef]
- Doty, R.L.; Hawkes, C.H.; Good, K.P.; Duda, J.E. 2015.
- Ross, G.W.; Petrovitch, H.; Abbott, R.D.; Tanner, C.M.; Popper, J.; Masaki, K.; Launer, L.; White, L.R. Association of Olfactory Dysfunction with Risk for Future Parkinson’s Disease. Ann Neurol 2008, 63, 167–173. [Google Scholar] [CrossRef] [PubMed]
- Doty, R.L. Olfactory Dysfunction in Neurodegenerative Diseases: Is There a Common Pathological Substrate? Lancet Neurol 2017, 16, 478–488. [Google Scholar] [CrossRef]
- Murphy, C. Olfactory and Other Sensory Impairments in Alzheimer Disease. Nat Rev Neurol 2019, 15, 11–24. [Google Scholar] [CrossRef]
- Jack, C.R.; Bennett, D.A.; Blennow, K.; Carrillo, M.C.; Dunn, B.; Haeberlein, S.B.; Holtzman, D.M.; Jagust, W.; Jessen, F.; Karlawish, J.; et al. NIA-AA Research Framework: Toward a Biological Definition of Alzheimer’s Disease. Alzheimer’s and Dementia 2018, 14, 535–562. [Google Scholar] [CrossRef] [PubMed]
- Hassenstab, J.; Ruvolo, D.; Jasielec, M.; Xiong, C.; Grant, E.; Morris, C.; Hassenstab, J.; Ruvolo, D.; Jasielec, M.; Xiong, C.; et al. Absence of Practice Effects in Preclinical Alzheimer’ s Disease. Neuropsychology 2015. [Google Scholar] [CrossRef] [PubMed]
- Mowrey, W.B.; Lipton, R.B.; Katz, M.J.; Ramratan, W.S.; Loewenstein, D.A.; Zimmerman, M.E.; Buschke, H. Memory Binding Test Predicts Incident Amnestic Mild Cognitive Impairment. Journal of Alzheimer’s Disease 2016, 53, 1585–1595. [Google Scholar] [CrossRef]
- Graves, A.B.; Larson, E.B.; Edland, S.D.; Bowen, J.D.; McCormick, W.C.; McCurry, S.M.; Rice, M.M.; Wenzlow, A.; Uomoto, J.M. Prevalence of Dementia and Its Subtypes in the Japanese American Population of King County, Washington State. The Kame Project. Am.J Epidemiol. 1996, 144, 760–771. [Google Scholar] [CrossRef]
- Calhoun-Haney, R.; Murphy, C. Apolipoprotein Epsilon4 Is Associated with More Rapid Decline in Odor Identification than in Odor Threshold or Dementia Rating Scale Scores. Brain Cogn 2005, 58, 178–182. [Google Scholar] [CrossRef] [PubMed]
- Devanand, D.P.; Lee, S.; Luchsinger, J.A.; Knopman, D.; Vassilaki, M.; Motter, J.N. Comparison of Brief Olfactory and Cognitive Assessments to Neuroimaging Biomarkers in the Prediction of Cognitive Decline and Dementia in the MCSA Cohort. Alzheimers Dement 2024, 20, 8346–8358. [Google Scholar] [CrossRef]
- Palta, P.; Chen, H.; Deal, J.A.; Sharrett, A.R.; Gross, A.; Knopman, D.; Griswold, M.; Heiss, G.; Mosley, T.H. Olfactory Function and Neurocognitive Outcomes in Old Age: The Atherosclerosis Risk in Communities Neurocognitive Study. Alzheimer’s and Dementia 2018, 14, 1015–1021. [Google Scholar] [CrossRef]
- Roberts, R.O.; Christianson, T.J.H.; Kremers, W.K.; Mielke, M.M.; Machulda, M.M.; Vassilaki, M.; Alhurani, R.E.; Geda, Y.E.; Knopman, D.S.; Petersen, R.C. Association Between Olfactory Dysfunction and Amnestic Mild Cognitive Impairment and Alzheimer Disease Dementia. JAMA Neurol 2016, 73, 93–101. [Google Scholar] [CrossRef] [PubMed]
- Laukka, E.J.; Ekström, I.; Larsson, M.; Grande, G.; Fratiglioni, L.; Rizzuto, D. Markers of Olfactory Dysfunction and Progression to Dementia: A 12-Year Population-Based Study. Alzheimer’s and Dementia 2023, 19, 3019–3027. [Google Scholar] [CrossRef]
- Guo, J.; Dove, A.; Wang, J.; Laukka, E.J.; Ekström, I.; Dunk, M.M.; Bennett, D.A.; Xu, W. Trajectories of Olfactory Identification Preceding Incident Mild Cognitive Impairment and Dementia: A Longitudinal Study. EBioMedicine 2023, 98, 104862. [Google Scholar] [CrossRef] [PubMed]
- Tu, L.; Lv, X.; Fan, Z.; Zhang, M.; Wang, H.; Yu, X. Association of Odor Identification Ability With Amyloid-β and Tau Burden: A Systematic Review and Meta-Analysis. Front Neurosci 2020, 14, 586330. [Google Scholar] [CrossRef] [PubMed]
- Bothwell, A.R.; Resnick, S.M.; Ferrucci, L.; Tian, Q. Associations of Olfactory Function with Brain Structural and Functional Outcomes. A Systematic Review. Ageing Res Rev 2023, 92, 102095. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Li, Y.; Liu, K.; Han, X.; Liu, R.; Ren, Y.; Cong, L.; Zhang, Q.; Hou, T.; Song, L.; et al. Anosmia, Mild Cognitive Impairment, and Biomarkers of Brain Aging in Older Adults. Alzheimers Dement 2023, 19, 589–601. [Google Scholar] [CrossRef]
- Iranzo, A.; Molinuevo, J.L.; Santamaría, J.; Serradell, M.; Martí, M.J.; Valldeoriola, F.; Tolosa, E. Rapid-Eye-Movement Sleep Behaviour Disorder as an Early Marker for a Neurodegenerative Disorder: A Descriptive Study. Lancet Neurology 2006, 5, 572–577. [Google Scholar] [CrossRef] [PubMed]
- Iranzo, A.; Tolosa, E.; Gelpi, E.; Molinuevo, J.L.; Valldeoriola, F.; Serradell, M.; Sanchez-Valle, R.; Vilaseca, I.; Lomeña, F.; Vilas, D.; et al. Neurodegenerative Disease Status and Post-Mortem Pathology in Idiopathic Rapid-Eye-Movement Sleep Behaviour Disorder: An Observational Cohort Study. Lancet Neurol 2013, 12, 443–453. [Google Scholar] [CrossRef]
- Schenck, C.H.; Boeve, B.F.; Mahowald, M.W. Delayed Emergence of a Parkinsonian Disorder or Dementia in 81% of Older Men Initially Diagnosed with Idiopathic Rapid Eye Movement Sleep Behavior Disorder: A 16-Year Update on a Previously Reported Series. Sleep Med 2013, 14, 744–748. [Google Scholar] [CrossRef]
- Mahlknecht, P.; Iranzo, A.; Högl, B.; Frauscher, B.; Müller, C.; Santamaría, J.; Tolosa, E.; Serradell, M.; Mitterling, T.; Gschliesser, V.; et al. Olfactory Dysfunction Predicts Early Transition to a Lewy Body Disease in Idiopathic RBD. Neurology 2015, 84, 654–658. [Google Scholar] [CrossRef]
- Iranzo, A.; Marrero-González, P.; Serradell, M.; Gaig, C.; Santamaria, J.; Vilaseca, I. Significance of Hyposmia in Isolated REM Sleep Behavior Disorder. J Neurol 2021, 268, 963–966. [Google Scholar] [CrossRef] [PubMed]
- Postuma, R.B.; Iranzo, A.; Hu, M.; Högl, B.; Boeve, B.F.; Manni, R.; Oertel, W.H.; Arnulf, I.; Ferini-Strambi, L.; Puligheddu, M.; et al. Risk and Predictors of Dementia and Parkinsonism in Idiopathic REM Sleep Behaviour Disorder: A Multicentre Study. Brain 2019, 142, 744–759. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; Del Tredici, K.; Rüb, U.; de Vos, R.A.I.; Jansen Steur, E.N.H.; Braak, E. Staging of Brain Pathology Related to Sporadic Parkinson’s Disease. Neurobiol Aging 2003, 24, 197–211. [Google Scholar] [CrossRef] [PubMed]
- Hawkes, C.H.; Del Tredici, K.; Braak, H. Parkinson’s Disease: A Dual-hit Hypothesis. Neuropathol Appl Neurobiol 2007, 33, 599–614. [Google Scholar] [CrossRef] [PubMed]
- Braak, H.; Rüb, U.; Gai, W.P.; Del Tredici, K. Idiopathic Parkinson’s Disease: Possible Routes by Which Vulnerable Neuronal Types May Be Subject to Neuroinvasion by an Unknown Pathogen. J Neural Transm 2003, 110, 517–536. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Ferro, Á.; Rábano, A.; Catalán, M.J.; Rodríguez-Valcárcel, F.C.; Díez, S.F.; Herreros-Rodríguez, J.; García-Cobos, E.; Álvarez-Santullano, M.M.; López-Manzanares, L.; Mosqueira, A.J.; et al. In Vivo Gastric Detection of A-synuclein Inclusions in Parkinson’s Disease. Movement Disorders 2015, 30, 517–524. [Google Scholar] [CrossRef]
- Kim, C.; Lv, G.; Lee, J.S.; Jung, B.C.; Masuda-Suzukake, M.; Hong, C.-S.; Valera, E.; Lee, H.-J.; Paik, S.R.; Hasegawa, M.; et al. Exposure to Bacterial Endotoxin Generates a Distinct Strain of α-Synuclein Fibril. Sci Rep 2016, 6, 30891. [Google Scholar] [CrossRef] [PubMed]
- Forsyth, C.B.; Shannon, K.M.; Kordower, J.H.; Voigt, R.M.; Shaikh, M.; Jaglin, J.A.; Estes, J.D.; Dodiya, H.B.; Keshavarzian, A. Increased Intestinal Permeability Correlates with Sigmoid Mucosa Alpha-Synuclein Staining and Endotoxin Exposure Markers in Early Parkinson’s Disease. PLoS One 2011, 6, e28032. [Google Scholar] [CrossRef] [PubMed]
- Knudsen, K.; Fedorova, T.D.; Hansen, A.K.; Sommerauer, M.; Otto, M.; Svendsen, K.B.; Nahimi, A.; Stokholm, M.G.; Pavese, N.; Beier, C.P.; et al. In-Vivo Staging of Pathology in REM Sleep Behaviour Disorder: A Multimodality Imaging Case-Control Study. Lancet Neurol 2018, 17, 618–628. [Google Scholar] [CrossRef]
- Buongiorno, M.; Marzal, C.; Fernandez, M.; Cullell, N.; de Mena, L.; Sánchez-Benavides, G.; de la Sierra, A.; Krupinski, J.; Compta, Y. Altered Sleep and Neurovascular Dysfunction in Alpha-Synucleinopathies: The Perfect Storm for Glymphatic Failure. Front Aging Neurosci 2023, 15, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen, M.K.; Mestre, H.; Nedergaard, M. Fluid Transport in the Brain. Physiol Rev 2022, 102, 1025–1151. [Google Scholar] [CrossRef]
- Mestre, H.; Hablitz, L.M.; Xavier, A.L.; Feng, W.; Zou, W.; Pu, T.; Monai, H.; Murlidharan, G.; Castellanos Rivera, R.M.; Simon, M.J.; et al. Aquaporin-4-Dependent Glymphatic Solute Transport in the Rodent Brain. Elife 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Nedergaard, M. Neuroscience. Garbage Truck of the Brain. Science 2013, 340, 1529–1530. [Google Scholar] [CrossRef]
- Koundal, S.; Elkin, R.; Nadeem, S.; Xue, Y.; Constantinou, S.; Sanggaard, S.; Liu, X.; Monte, B.; Xu, F.; Van Nostrand, W.; et al. Optimal Mass Transport with Lagrangian Workflow Reveals Advective and Diffusion Driven Solute Transport in the Glymphatic System. Sci Rep 2020, 10, 1990. [Google Scholar] [CrossRef] [PubMed]
- Iliff, J.J.; Wang, M.; Zeppenfeld, D.M.; Venkataraman, A.; Plog, B.A.; Liao, Y.; Deane, R.; Nedergaard, M. Cerebral Arterial Pulsation Drives Paravascular CSF-Interstitial Fluid Exchange in the Murine Brain. J Neurosci 2013, 33, 18190–18199. [Google Scholar] [CrossRef] [PubMed]
- Mestre, H.; Tithof, J.; Du, T.; Song, W.; Peng, W.; Sweeney, A.M.; Olveda, G.; Thomas, J.H.; Nedergaard, M.; Kelley, D.H. Flow of Cerebrospinal Fluid Is Driven by Arterial Pulsations and Is Reduced in Hypertension. Nat Commun 2018, 9, 4878. [Google Scholar] [CrossRef] [PubMed]
- Xie, L.; Kang, H.; Xu, Q.; Chen, M.J.; Liao, Y.; Thiyagarajan, M.; O’Donnell, J.; Christensen, D.J.; Nicholson, C.; Iliff, J.J.; et al. Sleep Drives Metabolite Clearance from the Adult Brain. Science 2013, 342, 373–377. [Google Scholar] [CrossRef] [PubMed]
- Louveau, A.; Smirnov, I.; Keyes, T.J.; Eccles, J.D.; Rouhani, S.J.; Peske, J.D.; Derecki, N.C.; Castle, D.; Mandell, J.W.; Lee, K.S.; et al. Structural and Functional Features of Central Nervous System Lymphatic Vessels. Nature 2015, 523, 337–341. [Google Scholar] [CrossRef]
- Henderson, M.X.; Cornblath, E.J.; Darwich, A.; Zhang, B.; Brown, H.; Gathagan, R.J.; Sandler, R.M.; Bassett, D.S.; Trojanowski, J.Q.; Lee, V.M.Y. Spread of α-Synuclein Pathology through the Brain Connectome Is Modulated by Selective Vulnerability and Predicted by Network Analysis. Nat Neurosci 2019, 22, 1248–1257. [Google Scholar] [CrossRef] [PubMed]
- Ossenkoppele, R.; Smith, R.; Mattsson-Carlgren, N.; Groot, C.; Leuzy, A.; Strandberg, O.; Palmqvist, S.; Olsson, T.; Jögi, J.; Stormrud, E.; et al. Accuracy of Tau Positron Emission Tomography as a Prognostic Marker in Preclinical and Prodromal Alzheimer Disease: A Head-to-Head Comparison Against Amyloid Positron Emission Tomography and Magnetic Resonance Imaging. JAMA Neurol 2021, 78, 961–971. [Google Scholar] [CrossRef]
- Ringstad, G.; Vatnehol, S.A.S.; Eide, P.K. Glymphatic MRI in Idiopathic Normal Pressure Hydrocephalus. Brain 2017, 140, 2691–2705. [Google Scholar] [CrossRef]
- Ringstad, G.; Valnes, L.M.; Dale, A.M.; Pripp, A.H.; Vatnehol, S.-A.S.; Emblem, K.E.; Mardal, K.-A.; Eide, P.K. Brain-Wide Glymphatic Enhancement and Clearance in Humans Assessed with MRI. JCI Insight 2018, 3. [Google Scholar] [CrossRef] [PubMed]
- Hablitz, L.M.; Vinitsky, H.S.; Sun, Q.; Stæger, F.F.; Sigurdsson, B.; Mortensen, K.N.; Lilius, T.O.; Nedergaard, M. Increased Glymphatic Influx Is Correlated with High EEG Delta Power and Low Heart Rate in Mice under Anesthesia. Sci Adv 2019, 5. [Google Scholar] [CrossRef] [PubMed]
- Malhotra, R.K. Neurodegenerative Disorders and Sleep. Sleep Med Clin 2018, 13, 63–70. [Google Scholar] [CrossRef]
- Mielke, M.M.; Teresa Ferretti, M.; Florencia Iulita, M.; Hayden, K.; Khachaturian, A.S. Sex and Gender in Alzheimer’s Disease - Does It Matter? 2018. [CrossRef]
- Luckey, A.M.; Robertson, I.H.; Lawlor, B.; Mohan, A.; Vanneste, S. Sex Differences in Locus Coeruleus: A Heuristic Approach That May Explain the Increased Risk of Alzheimer’s Disease in Females. Journal of Alzheimer’s Disease 2021, 83, 505–522. [Google Scholar] [CrossRef]
- Cui, J.; Shen, Y.; Li, R. Estrogen Synthesis and Signaling Pathways during Aging: From Periphery to Brain. Trends Mol Med 2013, 19, 197–209. [Google Scholar] [CrossRef] [PubMed]
- Giorgi, F.S.; Galgani, A.; Puglisi-Allegra, S.; Limanaqi, F.; Busceti, C.L.; Fornai, F. Locus Coeruleus and Neurovascular Unit: From Its Role in Physiology to Its Potential Role in Alzheimer’s Disease Pathogenesis. J Neurosci Res 2020, 98, 2406–2434. [Google Scholar] [CrossRef]
- Peter-Derex, L.; Yammine, P.; Bastuji, H.; Croisile, B. Sleep and Alzheimer’s Disease. Sleep Med Rev 2015, 19, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Chen, S.-J.; Ma, M.-Y.; Bao, Y.-P.; Han, Y.; Wang, Y.-M.; Shi, J.; Vitiello, M. V.; Lu, L. Sleep Disturbances Increase the Risk of Dementia: A Systematic Review and Meta-Analysis. Sleep Med Rev 2018, 40, 4–16. [Google Scholar] [CrossRef] [PubMed]
- Geiger, P.J.; Eisenlohr-Moul, T.; Gordon, J.L.; Rubinow, D.R.; Girdler, S.S. Effects of Perimenopausal Transdermal Estradiol on Self-Reported Sleep, Independent of Its Effect on Vasomotor Symptom Bother and Depressive Symptoms. Menopause 2019, 26, 1318–1323. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Choi, I.H.; Lee, S.H.; Kim, T.H. Association between Subjective Olfactory Dysfunction and Female Hormone-Related Factors in South Korea. Sci Rep 2019, 9, 20007. [Google Scholar] [CrossRef] [PubMed]
- Doty, R.L.; Tourbier, I.; Ng, V.; Neff, J.; Armstrong, D.; Battistini, M.; Sammel, M.D.; Gettes, D.; Evans, D.L.; Mirza, N.; et al. Influences of Hormone Replacement Therapy on Olfactory and Cognitive Function in Postmenopausal Women. Neurobiol Aging 2015, 36, 2053–2059. [Google Scholar] [CrossRef] [PubMed]
- Bernal-Mondragón, C.; Rivas-Arancibia, S.; Kendrick, K.M.; Guevara-Guzmán, R. Estradiol Prevents Olfactory Dysfunction Induced by A-β 25–35 Injection in Hippocampus. BMC Neurosci 2013, 14, 104. [Google Scholar] [CrossRef] [PubMed]
- Martinez, B.; Karunanayaka, P.; Wang, J.; Tobia, M.J.; Vasavada, M.; Eslinger, P.J.; Yang, Q.X. Different Patterns of Age-Related Central Olfactory Decline in Men and Women as Quantified by Olfactory FMRI. Oncotarget 2017, 8, 79212–79222. [Google Scholar] [CrossRef] [PubMed]
- Ekanayake, A.; Peiris, S.; Ahmed, B.; Kanekar, S.; Grove, C.; Kalra, D.; Eslinger, P.; Yang, Q.; Karunanayaka, P. A Review of the Role of Estrogens in Olfaction, Sleep and Glymphatic Functionality in Relation to Sex Disparity in Alzheimer’s Disease. Am J Alzheimers Dis Other Demen 2024, 39. [Google Scholar] [CrossRef]
- Wali, M.A.; Raparelli, V.; Pilote, L.; Daskalopoulou, S.S. Blood Pressure Variability in Normotensive Perimenopausal Women: Non-Dipping Status, Maximum Blood Pressure and Arterial Stiffness. Int J Cardiol 2021, 325, 149–154. [Google Scholar] [CrossRef] [PubMed]
- Gavriilaki, M.; Anyfanti, P.; Mastrogiannis, K.; Gavriilaki, E.; Lazaridis, A.; Kimiskidis, V.; Gkaliagkousi, E. Association between Ambulatory Blood Pressure Monitoring Patterns with Cognitive Function and Risk of Dementia: A Systematic Review and Meta-Analysis. Aging Clin Exp Res 2023, 35, 745–761. [Google Scholar] [CrossRef]
- Tarumi, T.; Harris, T.S.; Hill, C.; German, Z.; Riley, J.; Turner, M.; Womack, K.B.; Kerwin, D.R.; Monson, N.L.; Stowe, A.M.; et al. Amyloid Burden and Sleep Blood Pressure in Amnestic Mild Cognitive Impairment. Neurology 2015, 85, 1922–1929. [Google Scholar] [CrossRef] [PubMed]
- Dorsey, E.R.; Elbaz, A.; Nichols, E.; Abbasi, N.; Abd-Allah, F.; Abdelalim, A.; Adsuar, J.C.; Ansha, M.G.; Brayne, C.; Choi, J.-Y.J.; et al. Global, Regional, and National Burden of Parkinson’s Disease, 1990–2016: A Systematic Analysis for the Global Burden of Disease Study 2016. Lancet Neurol 2018, 17, 939–953. [Google Scholar] [CrossRef] [PubMed]
- Zirra, A.; Rao, S.C.; Bestwick, J.; Rajalingam, R.; Marras, C.; Blauwendraat, C.; Mata, I.F.; Noyce, A.J. Gender Differences in the Prevalence of Parkinson’s Disease. Mov Disord Clin Pract 2023, 10, 86–93. [Google Scholar] [CrossRef]
- Pringsheim, T.; Jette, N.; Frolkis, A.; Steeves, T.D.L. The Prevalence of Parkinson’s Disease: A Systematic Review and Meta-Analysis. Movement Disorders 2014, 29, 1583–1590. [Google Scholar] [CrossRef]
- Bathini, P.; Mottas, A.; Jaquet, M.; Brai, E.; Alberi, L. Progressive Signaling Changes in the Olfactory Nerve of Patients with Alzheimer’s Disease. Neurobiol Aging 2019, 76, 80–95. [Google Scholar] [CrossRef] [PubMed]
- Arnold, S.E.; Lee, E.B.; Moberg, P.J.; Stutzbach, L.; Kazi, H.; Han, L.-Y.; Lee, V.M.Y.; Trojanowski, J.Q. Olfactory Epithelium Amyloid-Beta and Paired Helical Filament-Tau Pathology in Alzheimer Disease. Ann Neurol 2010, 67, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Saiz-Sanchez, D.; De la Rosa-Prieto, C.; Ubeda-Banon, I.; Martinez-Marcos, A. Interneurons, Tau and Amyloid-β in the Piriform Cortex in Alzheimer’s Disease. Brain Struct Funct 2015, 220, 2011–2025. [Google Scholar] [CrossRef] [PubMed]
- Christen-Zaech, S.; Kraftsik, R.; Pillevuit, O.; Kiraly, M.; Martins, R.; Khalili, K.; Miklossy, J. Early Olfactory Involvement in Alzheimer’s Disease. Can J Neurol Sci 2003, 30, 20–25. [Google Scholar] [CrossRef] [PubMed]
- Attems, J.; Jellinger, K.A. Olfactory Tau Pathology in Alzheimer Disease and Mild Cognitive Impairment. Clin Neuropathol 2006, 25, 265–271. [Google Scholar] [PubMed]
- Wuestefeld, A.; Pichet Binette, A.; Berron, D.; Spotorno, N.; van Westen, D.; Stomrud, E.; Mattsson-Carlgren, N.; Strandberg, O.; Smith, R.; Palmqvist, S.; et al. Age-Related and Amyloid-Beta-Independent Tau Deposition and Its Downstream Effects. Brain 2023, 146, 3192–3205. [Google Scholar] [CrossRef]
- Crary, J.F.; Trojanowski, J.Q.; Schneider, J.A.; Abisambra, J.F.; Abner, E.L.; Alafuzoff, I.; Arnold, S.E.; Attems, J.; Beach, T.G.; Bigio, E.H.; et al. Primary Age-Related Tauopathy (PART): A Common Pathology Associated with Human Aging. Acta Neuropathol 2014, 128, 755–766. [Google Scholar] [CrossRef]
- Chae, J.; Choi, M.; Choi, J.; Yoo, S.-J. The Nasal Lymphatic Route of CSF Outflow: Implications for Neurodegenerative Disease Diagnosis and Monitoring. Anim Cells Syst (Seoul) 2024, 28, 45–54. [Google Scholar] [CrossRef]
- de Leon, M.J.; Li, Y.; Okamura, N.; Tsui, W.H.; Saint-Louis, L.A.; Glodzik, L.; Osorio, R.S.; Fortea, J.; Butler, T.; Pirraglia, E.; et al. Cerebrospinal Fluid Clearance in Alzheimer Disease Measured with Dynamic PET. J Nucl Med 2017, 58, 1471–1476. [Google Scholar] [CrossRef] [PubMed]
- Huang, S.-Y.; Zhang, Y.-R.; Guo, Y.; Du, J.; Ren, P.; Wu, B.-S.; Feng, J.-F.; Alzheimer’s Disease Neuroimaging Initiative; Cheng, W. ; Yu, J.-T. Glymphatic System Dysfunction Predicts Amyloid Deposition, Neurodegeneration, and Clinical Progression in Alzheimer’s Disease. Alzheimers Dement 2024, 20, 3251–3269. [Google Scholar] [CrossRef]
- Li, Y.; Wang, L.; Zhong, J.; Xu, H.; Han, Y.; Alzheimer’s Disease Neuroimaging Initiative; Zuo, C. ; Jiang, J. Impaired Glymphatic Function as a Biomarker for Subjective Cognitive Decline: An Exploratory Dual Cohort Study. Alzheimers Dement 2024, 20, 6542–6555. [Google Scholar] [CrossRef]
- Bae, Y.J.; Kim, J.-M.; Choi, B.S.; Ryoo, N.; Song, Y.S.; Nam, Y.; Yoon, I.-Y.; Cho, S.J.; Kim, J.H. Altered Brain Glymphatic Flow at Diffusion-Tensor MRI in Rapid Eye Movement Sleep Behavior Disorder. Radiology 2023, 307, e221848. [Google Scholar] [CrossRef]
- Ethell, D.W. Disruption of Cerebrospinal Fluid Flow through the Olfactory System May Contribute to Alzheimer’s Disease Pathogenesis. J Alzheimers Dis 2014, 41, 1021–1030. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



