
Submitted:
14 February 2025
Posted:
17 February 2025
You are already at the latest version
Abstract
This article summarizes the case of 30-year-old male diagnosed with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) and its longitudinal follow up that provided a secondary diagnosis of Multiple Sclerosis (MS) eight years after. The most impactful result being his response to rituximab treatment after the systematic failure of prior treatments. Although the expression of endogenous retroviral proteins has been associated with autoimmunity, the patient did not show increased expression of the toxic protein HERV (human endogenous retrovirus)-W ENV, a target of the ongoing clinical trials with temelimab in MS and long COVID-19 cases. However, genome-wide HERV transcriptome analysis by high density microarrays clearly revealed a distinct profile in patient´s blood supportive of an altered immune system. Limitations of the study include MRI imaging follow up to monitor lesion progression and reassessment of HERV profiles after rituximab. As an overall, the coincidence of HERV alterations and the impactful response to rituximab presents the possibility of additional, more specific, therapeutic targets encoded by other HERV elements yet to be discovered.
Keywords:
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS)
; Multiple Sclerosis (MS)
; Human Endogenous Retrovirus (HERV)
; rituximab
; autoimmunity
; Epstein-Barr Virus (EBV)
1. Introduction
Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is defined as a chronic disorder classified by the WHO as postviral fatigue syndrome (ICD-11 8E49 code), while Multiple Sclerosis (MS) (ICD-11 8A40 codes), is known as a chronic, inflammatory demyelinating disease of the central nervous system that includes three categories (relapsing/remitting, secondary progressive and primary progressive) [1].
Diagnosis criteria for ME/CFS relies on clinical symptoms [2,3,4], as no validated biomarker exists, with post-exertional malaise or PEM playing a significant role including fatigue, pain, cognitive, intestinal and sleep disturbances among others, limiting patient´s daily performance in the mildly affected and driving bed confinement in the severe. By contrast, MS is a complex neurological disorder characterized by inflammation in the central nervous system (CNS), leading primarily to demyelinating tissue damage. It affects approximately 2.8 million people worldwide [5]. MS represents a primary chronic, non-traumatic neurological disorder affecting young individuals with a high impact on patients' quality of life [6]. The predominant presentation of MS manifests as relapsing episodes – relapsing MS (RMS) [7]. Clinical relapses lead to acute neurological damage, characterized by varied clinical manifestations and subsequent recovery. Natural history studies indicate that close to 40% of these patients undergo steady neurological deterioration without evident relapses, transitioning into a progressive phase of the disease – progressive MS (PMS) [8,9,10].
While no directional treatment exists for ME/CFS, being often multimedicated to palliate their symptoms [11], there is a wide range of disease-modifying therapies available for MS, spanning from low- to high-efficacy options. These therapies enable neurologists to tailor treatment strategies based on individual prognostic factors [12,13]. In recent years, there has been a shift toward initiating treatment with high-efficacy DMTs early in the disease course, as accumulating evidence suggests superior long-term outcomes [14,15,16,17,18,19,20]. Among these therapies, anti-CD20 monoclonal antibodies have emerged as a key approach, specifically targeting B-cell populations to modulate disease activity [21].
This case report describes the longitudinal follow-up of a patient diagnosed with ME/CFS who developed central nervous system lesions compatible with a diagnosis of MS, the medication received and patient response to treatments. In an effort to understand the potential mechanisms behind patient´s diagnosis and response to rituximab, we evaluated the potential association of his diagnosis with derangement of PBMC human endogenous retrovirus (HERV) expression, using as reference previously reported healthy and ME/CFS HERV profiles [22].
2. Case Description
We present here the case of a male in his 30s diagnosed with ME/CFS and MS, who experienced a significant improvement in his fatigue following initiation of treatment with rituximab.
The patient's symptoms began in 2008, characterized by episodic dizziness, malaise, blurred vision, weakness, and mental fatigue, with no identifiable trigger. Additionally, he had sustained fractures in his right/left 5th metacarpal and his clavicle in 2008, followed by a bimalleolar ankle fracture in 2010. Throughout this period, cognitive fatigue was his predominant symptom, significantly impacting his daily life. He experienced difficulties in concentrating, understanding, or solving problems, which forced him to change his academic pursuits towards less demanding studies. While physical fatigue occasionally led to episodes of being bedridden, he managed to maintain a relatively normal level of physical activity in the periods between extreme fatigue episodes.
Despite evaluations by various specialists in the public health system, including internal medicine, neurology, rheumatology, psychiatry, and digestive medicine, no abnormalities were detected in clinical tests, leading to a referral to mental health services, where depression or anxiety was ruled out. In 2014, his symptoms worsened when he began working in a physically demanding job, leading to new symptoms such as headache, fainting, tinnitus, dyspnea, difficulty speaking, abdominal pain, pain in the hands, neurovegetative crises during sleep, intolerance to temperature changes, and orthostatic intolerance. This resulted in prolonged sick leaves, with the patient living mostly confined to bed.
Further evaluations ruled out autoimmune, thyroid, myasthenia, endocrine, and infectious pathologies, except for Epstein-Barr Virus (EBV) IgG positivity in 2015. Magnetic resonance imaging (MRI) in 2016 revealed a small demyelinating juxtacortical lesion in the left temporal pole, but other investigations were unremarkable, leading to a diagnosis of ME/CFS. Patient met the 2011 International Consensus Criteria [2], as well as Canadian [3] and IOM (Institute of Medicine) 2015 criteria [4]. Prescribed supplements, including magnesium, NADH, D-ribose, L-carnitine, ubiquinol, melatonin, vitamin B1, alpha-lipoic acid, and LDN (Low Dose Naltrexone), failed to improve symptoms.
In June 2017, he decided to stop all treatments, and in July 2017, he experienced sensory loss in his legs with a sensory spinal cord level from C6 to D2, prompting a referral to the Neurology Department. Electromyoneurography (EMG) was normal, and a lumbar puncture revealed intrathecal production of antibodies (oligoclonal bands) not present in serum (IgG and IgM). Evoked sensory potentials were altered on both sides. During the diagnostic panel, anti-Acetylcholine receptor (AchR) antibodies were positive, although this finding was of unknown significance with the normal EMG. Brain and spinal cord MRIs revealed a new demyelinating lesion at the spinal cord level, fulfilling spatial and temporal dissemination criteria for MS diagnosis according to McDonald criteria 2017 [23], with two foci in the medulla and parietal lobe (Figure 1).
He was initially prescribed oral teriflunomide, a low-efficacy disease-modifying therapy (DMT) [12], which was discontinued due to adverse effects, including tachycardia and tiredness. Subsequently, a switch to subcutaneous glatiramer acetate (GA) proved effective for 3 years. To address fatigue symptoms, amantadine, modafinil, and fampidrine [24] were trialed but proved ineffective. Amitriptyline was added for paresthesic symptoms at night, along with lormetazepam to improve sleep disturbances. Although well-tolerated in general, several episodes of immediate post-injection reaction were experienced by the patient, characterized by shortness of breath and palpitations for 15 minutes, which became uncomfortable due to their increased frequency.
Following a new relapse of disease activity for MS with evidence of radiological inflammation in the MRI (Figure 1), rituximab, an anti-CD20 agent aimed at eliminating the B cell population of lymphocytes, was prescribed in December 2021.
The treatment regime consisted of an initial dose of 1 gram on days 1 and 15 of the first month, followed by 9-monthly doses of 1 gram, adjusted based on the repopulation of B cells. This treatment resulted in a significant improvement in fatigue after the third dose, enabling increased mobility and participation in daily activities such as walking and dining out. The patient remains stable of his neurological condition, with fatigue stabilized.
EBV, as well as other viral infections unleashes the otherwise silenced expression of human endogenous retrovirus (HERV) [25], potentially leading to sterile inflammation and additional symptoms that resemble those of acute exogenous infections. In particular, overexpression of the toxic HERV-W ENV protein has been detected in MS patients [26], as well as in ME/CFS and post-COVID condition [27] indicating a relationship of this protein with post-viral disease chronicity.
To determine whether HERV-W ENV is overexpressed in the plasma of this patient, positive for EBV IgGs in 2015, we assessed HERV-W ENV protein levels following the protocol previously described in [27] and compared it to those in other ME/CFS cases and control samples (Figure 2) (Supplementary Table S1) (patient´s archived sample National Registry in Biobanking collection C0006024 obtained in 2016). The results showed that mean HERV-W ENV level of this patient's was 1.36E+05 (AUC), which was below the positivity cutoff value (mean AUC: 2.30E+06), defined as the mean + 2 standard deviations of control samples.
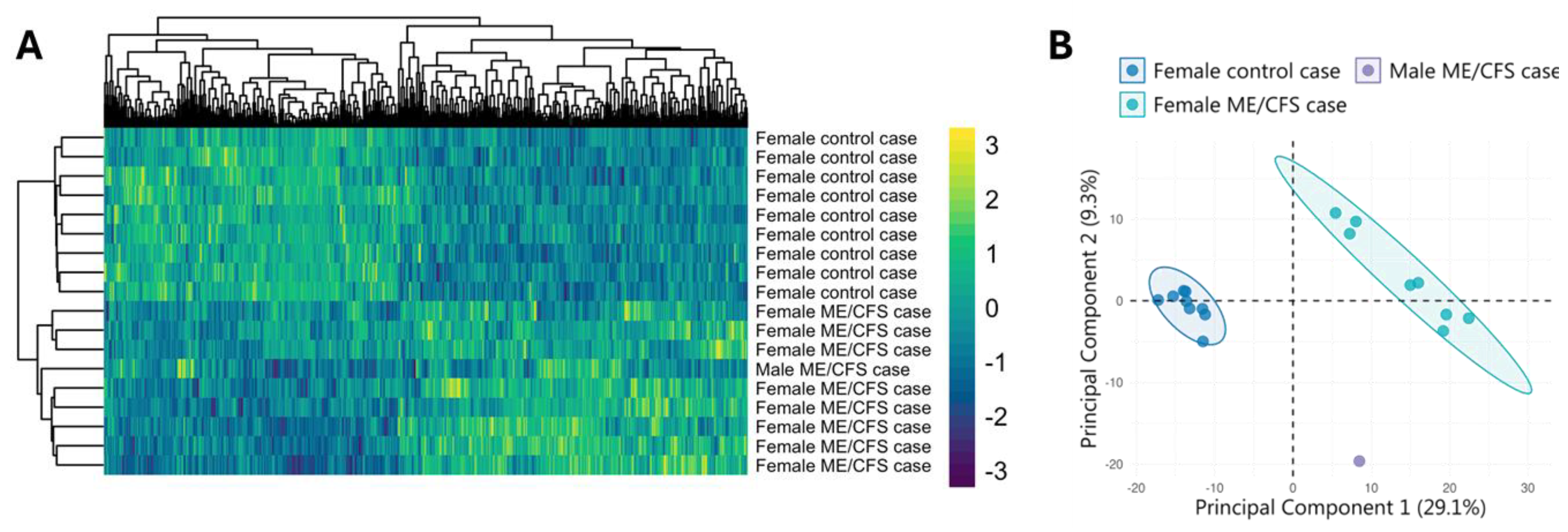
To further explore potential HERV alterations in this patient, we performed a genome-wide analysis using high-density microarrays, as described in [22]. Results of this study case were compared to those of other age- and BMI-matched ME/CFS cases and healthy volunteers. Bioinformatic analysis, conducted with the R "limma" package [22,28], identified 502 differentially expressed HERV probesets between ME/CFS patients and healthy controls (p-value < 0.1 and absolute log2 fold-change > 1) (Supplementary Table S2). Hierarchical clustering of HERV expression profiles revealed that the patient's sample clustered with other ME/CFS cases, despite being from a male subject (Figure 3A). To further investigate the patient’s clustering pattern, we conducted Principal Component Analysis (PCA). This analysis revealed that while the patient’s sample did not perfectly align with female ME/CFS cases, his HERV profile was closer to ME/CFS patients´ than to control´s (Figure 3B), indicating potential epigenetic alterations in his immune cells that despite differing from both comparison groups aligns with that of ME/CFS females.
To understand the potential cell role of top overexpressed HERVs in the study case, we first selected those with highest expression levels in the study case sample with respect to the rest (control or ME/CFS case), which turned out to be 29 out of the 502 differentially expressed (about 6% of them) (Supplementary Table S3), and then searched for their closest annotated genes. Gene names, genomic distances to HERVs with highest expression in the study case and their position within the matched gene were determined using the Goldmine package in RStudio [32] (Supplementary Table S4). The data shows that of the 29 HERV allocated, 10 (34.5%) corresponded with intergenic regions less than 100,000bp away while the remaining 19 (65.5%) seemed to be encoded within genes. From the latter, most (thirteen) were encoded within introns (68.4%), four lied within promoter regions (21%), one within the 3´UTR region and one within a coding exon (5.3% each). In addition to regulatory lncRNAs, novel transcripts, hit genes associated with development, infection, metabolism and neural homeostasis, as for example QKI involved in myelinization and oligodendrocyte differentiation or LINGO2 with a role in the glutamatergic synapse.
3. Discussion
This case report informs of a patient having received an initial diagnosis of ME/CFS (2015) and a later diagnosis of MS (2017), with a lack of response to several treatments for the following three years and striking response to rituximab in 2020, having kept the patient in remission until present. Although MS relapse frequency is highly variable, as it is the case for factors affecting MS-associated fatigue [33], recent meta-analysis reports a reduction in MS relapses with rituximab treatment [34]. Clinical trials assessing the potential benefit of ME/CFS with rituximab are more limited, with an initial partial success in the reduction of symptoms [35] and failure to show benefits by a continuation trial [36]. Discrepancies across trials may be associated with patient heterogeneity, medical regime applied or other. In this case report the patient not only showed clear improvement after only three doses of treatment with rituximab, but also remains stable of his neurological condition, with fatigue stabilized now for some years after the 9-month treatment regime applied. Whether the successful evolution of the patient is due to additional factors is unknown.
The patient displayed auto-antibodies against AchR (AchR-aAbs), a typical finding in myasthenia gravis (MG), an autoimmune disease displaying impaired neuromuscular junction transmission with about 85% of patients presenting AchR-aAbs [37]. Thus, a mechanism mediated by AchR-aAbs contributing to patient improvement by rituximab therapy cannot be discarded [38].
The lack of overexpression of the toxic HERV-W ENV protein, also known as MSRV, frequently reported in MS patients [39], but also reported in some ME/CFS patients [40] was unexpected. Targeting MSRV with the monoclonal antibody temelimab is being studied [41]. On another hand, our mechanistic findings on differential HERV profiles are limited by the lack of comparison of HERV profiles of this case to male ME/CFS and MS cases. In fact, the literature reports molecular differences in the immune systems of male and female ME/CFS patients [42,43,44]. Whether molecular sex-differences in ME/CFS include HERV profiles remains unknown at present. Nevertheless, the results of this patient´s HERV profile seem to align better with other ME/CFS cases, despite the absence of sex-matching, than with profiles of the healthy participants, in support of his ME/CFS diagnosis. In addition, the findings fit with those of previous reports of EBV infections leading to important endogenous retroviral repression in CD19 + B cells [45]. Despite an important downregulation of HERV expression in the PBMCs of our patient, we observed prominent overexpression (overexpressed above all other reference samples; n=17) (Supplementary Table S3), on about 6% of the differentially expressed HERVs. Interestingly associated gene functions match with potential alterations of the patient´s physiology (Supplementary Table S4). Although it is not possible to attribute our findings to CD19+ B cell epigenetic alterations or to any other PBMC subpopulations, the observed response of the patient to rituximab therapy suggests this may be a mechanism for EBV disease triggering worth exploring.
EBV infections seem to constitute a causal factor for developing MS [46] as found for EBNA1-peptide epitope mimicry mechanisms with the central nervous system protein glial cell adhesion molecule (GlialCAM) leading to nervous tissue lesions [47]. Similarly, mechanisms leading to autoimmune encephalitis after herpes simplex infections [48] or to other types of autoimmunity by still unknown mediators (unknown foreign antigens) [49], have been described. Additional auto-antigen-related viral sequences will possibly be discovered in the years to come. In this respect, WHO´s definition of ME/CFS as a post-viral chronic disease, the rich bibliography relating ME/CFS with EBV, herpes or other infectious agents [50,51,52], in addition to the presentation of symptom overlaps between ME/CFS, MS and MG, including muscle weakness, sleep and sensory disturbances, or pain [53,54,55], poses the pertinence of co-exploring the mechanisms underlying these diseases. The case reported here appears singular from the angle that the patient presents with features, to a certain extent, for a triplet disease. Further work towards defining differential markers across these and other symptom related diseases, thus promoting the development of targeted therapeutics, is urgently needed.
4. Conclusions
In summary, we present a male case with a co-diagnosis of ME/CFS and MS, with a positive EBV serology, also expressing AchR-aAbs, and showing multiple symptomatology and lesions in the spine and brain, who positively responded to a 9-month treatment regime of rituximab doses of 1 gram and stayed in remission for at least 3 years after treatment. Despite no evidence of HERV-W ENV overexpression, as expected, patient´s PBMC HERV profile was clearly in closer proximity of other ME/CFS profiles than with those of healthy participants, with potential sex-discrepancies and/or connections to MS and MG, confirmation pending. Derangement of HERV expression in B-cells contained within the explored PBMCs appear as a feasible mechanistic explanation for the response of this patient to rituximab, seemingly worth exploring in future cases. In addition, the possibility of individual responses to viral infections triggering the development of complex chronic states deserves further assessment.
Author Contributions
Conceptualization, E.M-M and E.O.; methodology and data curation, S.G-P; L.B-M; and K.G-O; writing—original draft preparation, E.M-M; S.G-P; K.G-O and E.O; writing—review and editing, ALL authors; funding acquisition, E.O. and K.G-O. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Generalitat Valenciana, grant number CIAICO 2021/103 to E.O. KG-O is supported by the Generalitat Valenciana ACIF2021/179 grant.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Public Health Research Ethics Committee DGSP-CSISP of Valencia, num. 20190301/12 and 20210430/08, Valencia, Spain.
Informed Consent Statement
Informed consent was obtained from the subject involved in the study.
Data Availability Statement
The original contributions presented in this study are included within the article. Further inquiries can be directed to the corresponding author/s.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
Abbreviations
The following abbreviations are used in this manuscript:
| ME/CFS | Myalgic Encephalomyelitis/ Chronic Fatigue Syndrome |
| MS | Multiple Sclerosis |
| MG | Myasthenia Gravis |
| HERV | Human Endogenous Retrovirus |
| HERV-W ENV | Human Endogenous Retrovirus type W (tryptophan), Envelope protein |
| MSRV | Multiple Sclerosis Retrovirus |
| PBMC | Peripheral Blood Mononuclear Cells |
| EBV | Epstein Bar Virus |
| AchR | Acetylcholine Receptor |
| aAb | Autoantibody |
References
- Harrison, J.E.; Weber, S.; Jakob, R.; Chute, C.G. ICD-11: An international classification of diseases for the twenty-first century. BMC Med Inform Decis Mak. 2021, 21 (Suppl. S6), 206. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Carruthers, B.M.; van de Sande, M.I.; De Meirleir, K.L.; Klimas, N.G.; Broderick, G.; Mitchell, T.; et al. Myalgic encephalomyelitis: International consensus criteria. J Intern Med. 2011, 270, 327–338. [Google Scholar] [CrossRef] [PubMed]
- Carruthers, B.M.; Jain, A.K.; De Meirleir, K.L.; Peterson, D.L.; Klimas, N.G.; Lerner, A.; et al. Myalgic encephalomyelitis/chronic fatigue syndrome: Clinical working case definition, diagnostic and treatment protocols. J Chron Fatigue Syndr. 2003, 11, 7–115. [Google Scholar] [CrossRef]
- Clayton, E.W. Beyond myalgic encephalomyelitis/chronic fatigue syndrome: An IOM report on redefining an illness. JAMA. 2015, 313, 1101–1102. [Google Scholar] [CrossRef] [PubMed]
- Walton, C.; King, R.; Rechtman, L.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of, M.S.; third edition. Mult Scler. 2020, 26, 1816–1821. [Google Scholar] [CrossRef]
- Zwibel, H.L.; Smrtka, J. Improving quality of life in multiple sclerosis: An unmet need. Am J Manag Care. 2011, 17 (Suppl. S5), S139. [Google Scholar]
- Lublin, F.D.; Reingold, S.C.; Cohen, J.A.; et al. Defining the clinical course of multiple sclerosis: The 2013 revisions. Neurology 2014, 83, 278–286. [Google Scholar] [CrossRef]
- Scalfari, A.; Neuhaus, A.; Degenhardt, A.; et al. The natural history of multiple sclerosis: A geographically based study 10: Relapses and long-term disability. Brain 2010, 133 Pt 7, 1914–1929. [Google Scholar] [CrossRef] [PubMed]
- Confavreux, C.; Vukusic, S. Natural history of multiple sclerosis: A unifying concept. Brain 2006, 129 Pt 3, 606–616. [Google Scholar] [CrossRef]
- Koch, M.; Kingwell, E.; Rieckmann, P.; et al. The natural history of secondary progressive multiple sclerosis. J Neurol Neurosurg Psychiatry 2010, 81, 1039–1043. [Google Scholar] [CrossRef]
- Almenar-Pérez, E.; Sánchez-Fito, T.; Ovejero, T.; Nathanson, L.; Oltra, E. Impact of Polypharmacy on Candidate Biomarker miRNomes for the Diagnosis of Fibromyalgia and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: Striking Back on Treatments. Pharmaceutics. 2019, 11, 126. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Montalban, X.; Gold, R.; Thompson, A.J.; Otero-Romero, S.; Amato, M.P.; Chandraratna, D.; et al. ECTRIMS/EAN guideline on the pharmacological treatment of people with multiple sclerosis. Mult Scler. 2018, 24, 96–120. [Google Scholar] [CrossRef]
- Rae-Grant, A.; Day, G.S.; Marrie, R.A.; Rabinstein, A.; Cree, B.A.C.; Gronseth, G.S.; et al. Practice guideline recommendations summary: Disease-modifying therapies for adults with multiple sclerosis: Report of the guideline development, dissemination, and implementation subcommittee of the American Academy of Neurology. Neurology. 2018, 90, 777–788. [Google Scholar] [CrossRef] [PubMed]
- Harding, K.; Williams, O.; Willis, M.; Hrastelj, J.; Rimmer, A.; Joseph, F.; et al. Clinical outcomes of escalation vs early intensive disease-modifying therapy in patients with multiple sclerosis. JAMA Neurol. 2019, 76, 536–541. [Google Scholar] [CrossRef]
- Brown, J.W.L.; Coles, A.; Horakova, D.; Havrdova, E.; Izquierdo, G.; Prat, A.; et al. Association of initial disease-modifying therapy with later conversion to secondary progressive multiple sclerosis. JAMA. 2019, 321, 175–187. [Google Scholar] [CrossRef] [PubMed]
- He, A.; Merkel, B.; Brown, J.W.L.; Zhovits Ryerson, L.; Kister, I.; Malpas, C.B.; et al. Timing of high-efficacy therapy for multiple sclerosis: A retrospective observational cohort study. Lancet Neurol. 2020, 19, 307–316. [Google Scholar] [CrossRef]
- Buron, M.D.; Chalmer, T.A.; Sellebjerg, F.; Barzinji, I.; Christensen, J.R.; Christensen, M.K.; et al. Initial high-efficacy disease-modifying therapy in multiple sclerosis: A nationwide cohort study. Neurology. 2020, 95, e1041–e1051. [Google Scholar] [CrossRef]
- Spelman, T.; Magyari, M.; Piehl, F.; Svenningsson, A.; Rasmussen, P.V.; Kant, M.; et al. Treatment escalation vs immediate initiation of highly effective treatment for patients with relapsing-remitting multiple sclerosis: Data from 2 different national strategies. JAMA Neurol. 2021, 78, 1197–1204. [Google Scholar] [CrossRef]
- Uher, T.; Krasensky, J.; Malpas, C.; Bergsland, N.; Dwyer, M.G.; Kubala Havrdova, E.; et al. Evolution of brain volume loss rates in early stages of multiple sclerosis. Neurol Neuroimmunol Neuroinflamm. 2021, 8, e979. [Google Scholar] [CrossRef]
- Hanninen, K.; Viitala, M.; Atula, S.; Laakso, S.M.; Kuusisto, H.; Soilu-Hanninen, M. Initial treatment strategy and clinical outcomes in Finnish MS patients: A propensity-matched study. J Neurol. 2022, 269, 913–922. [Google Scholar] [CrossRef]
- Carlson, A.K.; Amin, M.; Cohen, J.A. Drugs Targeting CD20 in Multiple Sclerosis: Pharmacology, Efficacy, Safety, and Tolerability. Drugs 2024, 84, 285–304. [Google Scholar] [CrossRef] [PubMed]
- Giménez-Orenga, K.; Martín-Martínez, E.; Nathanson, L.; Oltra, E. HERV activation segregates ME/CFS from fibromyalgia while defining a novel nosologic entity. eLife 2025, 14, RP104441. [Google Scholar] [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; Fujihara, K.; Galetta, S.L.; Hartung, H.P.; Kappos, L.; Lublin, F.D.; Marrie, R.A.; Miller, A.E.; Miller, D.H.; Montalban, X.; Mowry, E.M.; Sorensen, P.S.; Tintoré, M.; Traboulsee, A.L.; Trojano, M.; Uitdehaag, B.M.J.; Vukusic, S.; Waubant, E.; Weinshenker, B.G.; Reingold, S.C.; Cohen, J.A. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [Google Scholar] [CrossRef]
- Yang, T.T.; Wang, L.; Deng, X.Y.; Yu, G. Pharmacological treatments for fatigue in patients with multiple sclerosis: A sys-tematic review and meta-analysis. J Neurol Sci. 2017, 380, 256–261. [Google Scholar] [CrossRef] [PubMed]
- Giménez-Orenga, K.; Oltra, E. Human Endogenous Retrovirus as Therapeutic Targets in Neurologic Disease. Pharmaceuticals 2021, 14, 495. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Perron, H.; Lazarini, F.; Ruprecht, K.; Péchoux-Longin, C.; Seilhean, D.; Sazdovitch, V.; Créange, A.; Battail-Poirot, N.; Sibaï, G.; Santoro, L.; Jolivet, M.; Darlix, J.L.; Rieckmann, P.; Arzberger, T.; Hauw, J.J.; Lassmann, H. Human endogenous retrovirus (HERV)-W ENV and GAG proteins: Physiological expression in human brain and pathophysiological modulation in multiple sclerosis lesions. J Neurovirol. 2005, 11, 23–33. [Google Scholar] [CrossRef] [PubMed]
- Giménez-Orenga, K.; Pierquin, J.; Brunel, J.; Charvet, B.; Martín-Martínez, E.; Perron, H.; Oltra, E. HERV-W ENV antigenemia and correlation of increased anti-SARS-CoV-2 immunoglobulin levels with post-COVID-19 symptoms. Front Immunol. 2022, 13, 1020064. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ritchie, M.E.; Phipson, B.; Wu, D.; Hu, Y.; Law, C.W.; Shi, W.; Smyth, G.K. limma powers differential expression analyses for RNA-sequencing and microarray studies. Nucleic Acids Res. 2015, 43, e47. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Becker, J.; Pérot, P.; Cheynet, V.; Oriol, G.; Mugnier, N.; Mommert, M.; Tabone, O.; Textoris, J.; Veyrieras, J.B.; Mallet, F. A comprehensive hybridization model allows whole HERV transcriptome profiling using high density microarray. BMC Genomics. 2017, 18, 286. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kolde RLizee AMetsalu T.2018Pheatmap: Pretty heatmapsGitHub. Available online: https://github.com/raivokolde/pheatmap.
- Kassambara AMundt F.2019F actoextra: Extract and Visualize the Results of Multivariate Data AnalysesR package. Available online: https://rpkgs.datanovia.com/factoextra/index.html.
- Bhasin, J.M.; Ting, A.H. Goldmine integrates information placing genomic ranges into meaningful biological contexts. Nucleic Acids Res. 2016, 44, 5550–5556. [Google Scholar] [CrossRef]
- Machtoub, D.; Fares, C.; Sinan, H.; Al Hariri, M.; Nehme, R.; Chami, J.; Joukhdar, R.; Tcheroyan, R.; Adib, S.; Khoury, S.J. Factors affecting fatigue progression in multiple sclerosis patients. Sci Rep. 2024, 14, 31682. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ridley, B.; Minozzi, S.; Gonzalez-Lorenzo, M.; Del Giovane, C.; Piggott, T.; Filippini, G.; Peryer, G.; Foschi, M.; Tramacere, I.; Baldin, E.; Nonino, F. Immunomodulators and immunosuppressants for progressive multiple sclerosis: A network meta-analysis. Cochrane Database Syst Rev. 2024, 9, CD015443. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fluge, Ø.; Risa, K.; Lunde, S.; Alme, K.; Rekeland, I.G.; Sapkota, D.; Kristoffersen, E.K.; Sørland, K.; Bruland, O.; Dahl, O.; Mella, O. B-Lymphocyte Depletion in Myalgic Encephalopathy/ Chronic Fatigue Syndrome. An Open-Label Phase II Study with Rituximab Maintenance Treatment. PLoS ONE. 2015, 10, e0129898. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fluge, Ø.; Rekeland, I.G.; Lien, K.; Thürmer, H.; Borchgrevink, P.C.; Schäfer, C.; Sørland, K.; Aßmus, J.; Ktoridou-Valen, I.; Herder, I.; Gotaas, M.E.; Kvammen, Ø.; Baranowska, K.A.; Bohnen, L.M.L.J.; Martinsen, S.S.; Lonar, A.E.; Solvang, A.H.; Gya, A.E.S.; Bruland, O.; Risa, K.; Alme, K.; Dahl, O.; Mella, O. B-Lymphocyte Depletion in Patients With Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Randomized, Double-Blind, Placebo-Controlled Trial. Ann Intern Med. 2019, 170, 585–593. [Google Scholar] [CrossRef] [PubMed]
- Lazaridis, K.; Tzartos, S.J. Myasthenia Gravis: Autoantibody Specificities and Their Role in MG Management. Front Neurol. 2020, 11, 596981. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gilhus, N.E.; Andersen, H.; Andersen, L.K.; Boldingh, M.; Laakso, S.; Leopoldsdottir, M.O.; Madsen, S.; Piehl, F.; Popperud, T.H.; Punga, A.R.; Schirakow, L.; Vissing, J. Generalized myasthenia gravis with acetylcholine receptor antibodies: A guidance for treatment. Eur J Neurol. 2024, 31, e16229. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- van Horssen, J.; van der Pol, S.; Nijland, P.; Amor, S.; Perron, H. Human endogenous retrovirus W in brain lesions: Rationale for targeted therapy in multiple sclerosis. Mult Scler Relat Disord. 2016, 8, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Giménez-Orenga, K.; Pierquin, J.; Brunel, J.; Charvet, B.; Martín-Martínez, E.; Perron, H.; Oltra, E. HERV-W ENV antigenemia and correlation of increased anti-SARS-CoV-2 immunoglobulin levels with post-COVID-19 symptoms. Front Immunol. 2022, 13, 1020064. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Madeira, A.; Burgelin, I.; Perron, H.; Curtin, F.; Lang, A.B.; Faucard, R. MSRV envelope protein is a potent, endogenous and pathogenic agonist of human toll-like receptor 4: Relevance of GNbAC1 in multiple sclerosis treatment. J Neuroimmunol. 2016, 291, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Gamer, J.; Van Booven, D.J.; Zarnowski, O.; Arango, S.; Elias, M.; Kurian, A.; Joseph, A.; Perez, M.; Collado, F.; Klimas, N.; Oltra, E.; Nathanson, L. Sex-Dependent Transcriptional Changes in Response to Stress in Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Pilot Project. Int J Mol Sci. 2023, 24, 10255. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Germain, A.; Giloteaux, L.; Moore, G.E.; Levine, S.M.; Chia, J.K.; Keller, B.A.; Stevens, J.; Franconi, C.J.; Mao, X.; Shungu, D.C.; Grimson, A.; Hanson, M.R. Plasma metabolomics reveals disrupted response and recovery following maximal exercise in myalgic encephalomyelitis/chronic fatigue syndrome. JCI Insight. 2022, 7, e157621. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cheema, A.K.; Sarria, L.; Bekheit, M.; Collado, F.; Almenar-Pérez, E.; Martín-Martínez, E.; Alegre, J.; Castro-Marrero, J.; Fletcher, M.A.; Klimas, N.G.; Oltra, E.; Nathanson, L. Unravelling myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): Gender-specific changes in the microRNA expression profiling in ME/CFS. J Cell Mol Med. 2020, 24, 5865–5877. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Macchietto, M.G.; Langlois, R.A.; Shen, S.S. Virus-induced transposable element expression up-regulation in human and mouse host cells. Life Sci Alliance. 2020, 3, e201900536. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bjornevik, K.; Cortese, M.; Healy, B.C.; Kuhle, J.; Mina, M.J.; Leng, Y.; Elledge, S.J.; Niebuhr, D.W.; Scher, A.I.; Munger, K.L.; Ascherio, A. Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Science. 2022, 375, 296–301. [Google Scholar] [CrossRef] [PubMed]
- Lanz, T.V.; Brewer, R.C.; Ho, P.P.; Moon, J.S.; Jude, K.M.; Fernandez, D.; Fernandes, R.A.; Gomez, A.M.; Nadj, G.S.; Bartley, C.M.; Schubert, R.D.; Hawes, I.A.; Vazquez, S.E.; Iyer, M.; Zuchero, J.B.; Teegen, B.; Dunn, J.E.; Lock, C.B.; Kipp, L.B.; Cotham, V.C.; Ueberheide, B.M.; Aftab, B.T.; Anderson, M.S.; DeRisi, J.L.; Wilson, M.R.; Bashford-Rogers, R.J.M.; Platten, M.; Garcia, K.C.; Steinman, L.; Robinson, W.H. Clonally expanded B cells in multiple sclerosis bind EBV EBNA1 and GlialCAM. Nature 2022, 603, 321–327. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Armangue, T.; Spatola, M.; Vlagea, A.; Mattozzi, S.; Cárceles-Cordon, M.; Martinez-Heras, E.; Llufriu, S.; Muchart, J.; Erro, M.E.; Abraira, L.; Moris, G.; Monros-Giménez, L.; Corral-Corral, Í.; Montejo, C.; Toledo, M.; Bataller, L.; Secondi, G.; Ariño, H.; Martínez-Hernández, E.; Juan, M.; Marcos, M.A.; Alsina, L.; Saiz, A.; Rosenfeld, M.R.; Graus, F.; Dalmau, J.; Spanish Herpes Simplex Encephalitis Study Group. Frequency, symptoms, risk factors, and outcomes of autoimmune encephalitis after herpes simplex encephalitis: A prospective observational study and retrospective analysis. Lancet Neurol. 2018, 17, 760–772. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Iversen, R.; Sollid, L.M. Dissecting autoimmune encephalitis through the lens of intrathecal B cells. Proc Natl Acad Sci U S A. 2024, 121, e2401337121. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ruiz-Pablos, M.; Paiva, B.; Zabaleta, A. Epstein-Barr virus-acquired immunodeficiency in myalgic encephalomyelitis-Is it present in long COVID? J Transl Med. 2023, 21, 633. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kasimir, F.; Toomey, D.; Liu, Z.; Kaiping, A.C.; Ariza, M.E.; Prusty, B.K. Tissue specific signature of HHV-6 infection in ME/CFS. Front Mol Biosci. 2022, 9, 1044964. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- O'Neal, A.J.; Hanson, M.R. The Enterovirus Theory of Disease Etiology in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome: A Critical Review. Front Med (Lausanne). 2021, 8, 688486. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Morris, G.; Maes, M. Myalgic encephalomyelitis/chronic fatigue syndrome and encephalomyelitis disseminata/multiple sclerosis show remarkable levels of similarity in phenomenology and neuroimmune characteristics. BMC Med. 2013, 11, 205. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Danikowski, K.M.; Jayaraman, S.; Prabhakar, B.S. Regulatory T cells in multiple sclerosis and myasthenia gravis. J Neuroinflammation. 2017, 14, 117. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pérez-Carbonell, L.; Iranzo, A. Sleep Disturbances in Autoimmune Neurological Diseases. Curr Neurol Neurosci Rep. 2023, 23, 617–625. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Magnetic resonance imaging (MRI) of the brain and spinal cord of the patient described in the clinical case. Two subtle lesions can be observed in T2 sequences of the cervical spinal cord at the level of C3 (A) and in the white matter (WM) of the brain at the level of the temporal horn of the left lateral ventricle (B). Image obtained in FLAIR sequence, which enhances the lesions in WM (C). The images were obtained in a 3-Tesla MRI (General Electric, Signa HDx, Boston, MA, USA).
Figure 1.
Magnetic resonance imaging (MRI) of the brain and spinal cord of the patient described in the clinical case. Two subtle lesions can be observed in T2 sequences of the cervical spinal cord at the level of C3 (A) and in the white matter (WM) of the brain at the level of the temporal horn of the left lateral ventricle (B). Image obtained in FLAIR sequence, which enhances the lesions in WM (C). The images were obtained in a 3-Tesla MRI (General Electric, Signa HDx, Boston, MA, USA).
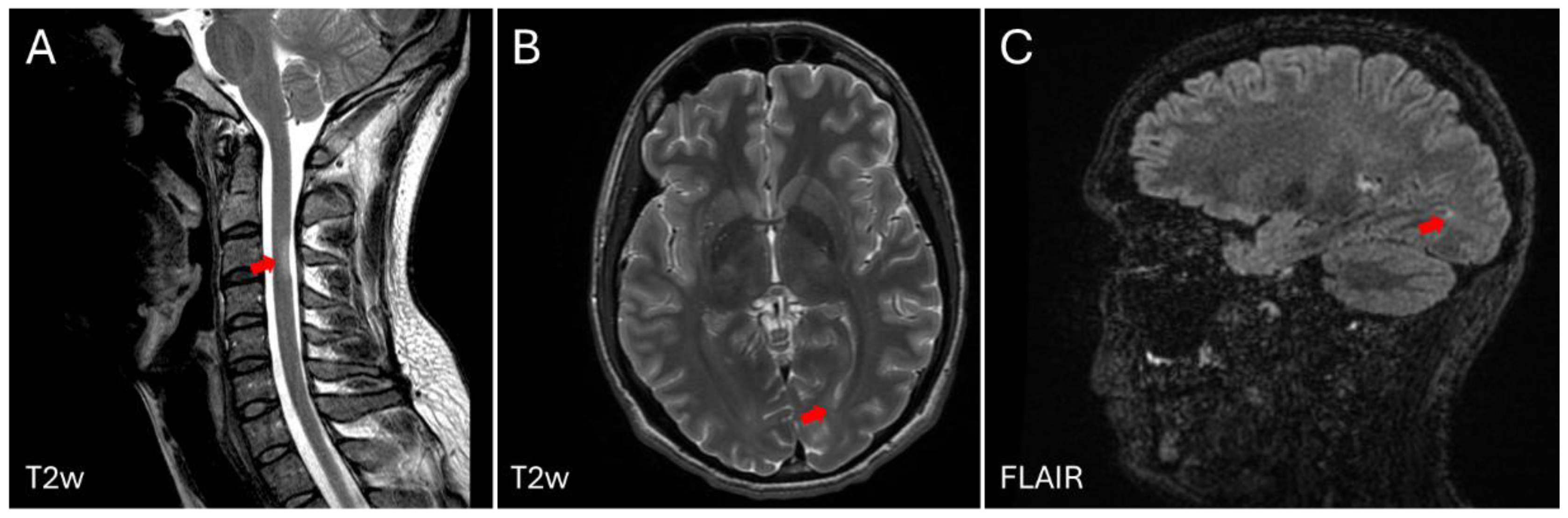
Figure 2.
HERV-W envelope (ENV) antigenemia in control cases (n=10), ME/CFS (n=15) and post-COVID-19 condition subjects (n=26). Levels of HERV-W ENV protein in plasma are shown as mean area under the curve (AUC). HERV-W ENV protein level in plasma is highlighted in blue for the study case. Cutoff line shows the minimum value to be considered positive.
Figure 2.
HERV-W envelope (ENV) antigenemia in control cases (n=10), ME/CFS (n=15) and post-COVID-19 condition subjects (n=26). Levels of HERV-W ENV protein in plasma are shown as mean area under the curve (AUC). HERV-W ENV protein level in plasma is highlighted in blue for the study case. Cutoff line shows the minimum value to be considered positive.
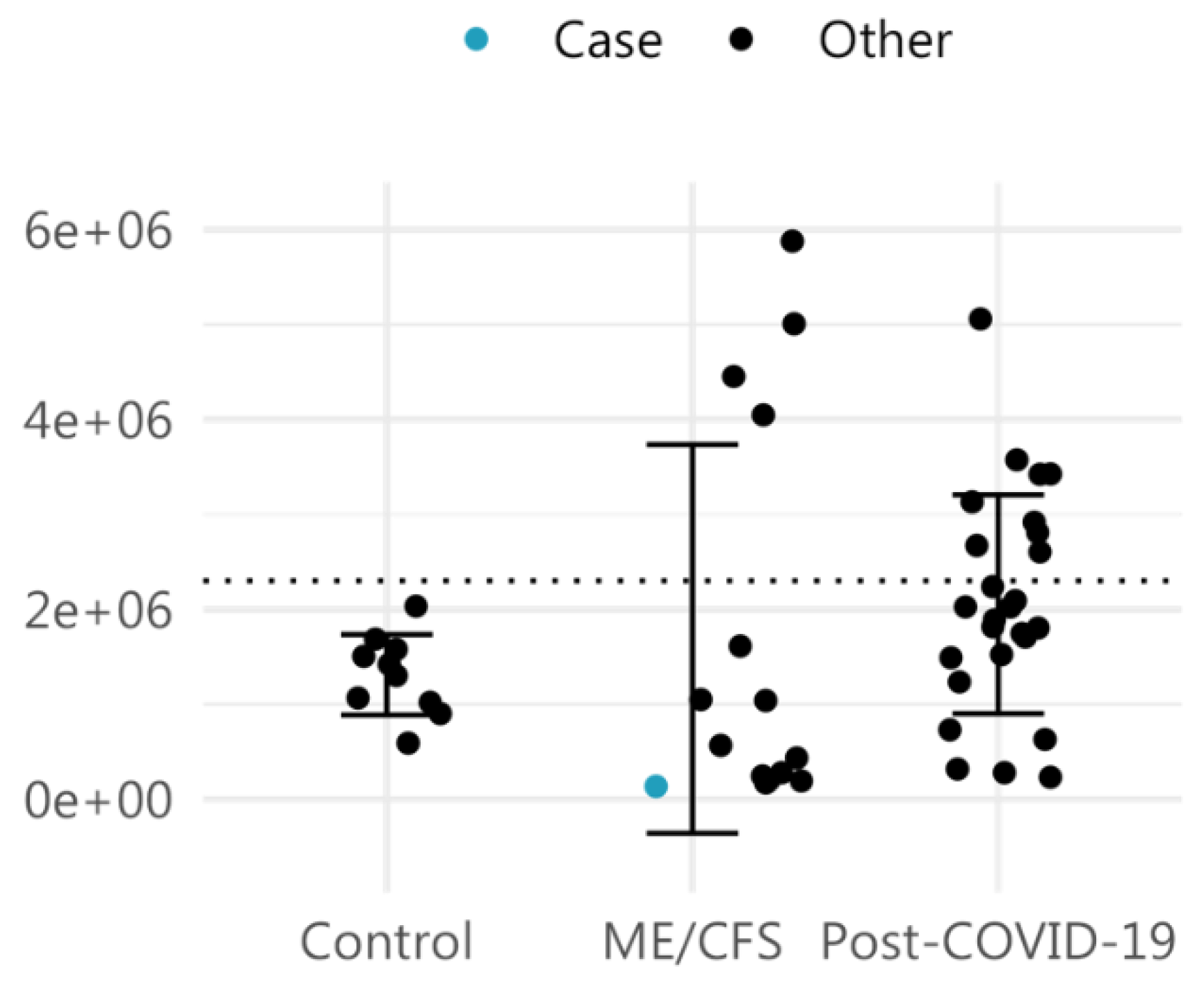
Figure 3.
HERV clustering (A) and principal component analysis (B) of the ME/CFS male case reported in this study along with 8 female ME/CFS cases and 9 healthy volunteer samples. Analysis includes all HERV probes of custom HERV-V3 arrays [29], displaying significant differential expression between ME/CFS and healthy control groups (FDR<0.1 and |log2FC|>1). Clustering heatmap was built with pheatmap [30] and PCA with FactoMineR package [31].
Figure 3.
HERV clustering (A) and principal component analysis (B) of the ME/CFS male case reported in this study along with 8 female ME/CFS cases and 9 healthy volunteer samples. Analysis includes all HERV probes of custom HERV-V3 arrays [29], displaying significant differential expression between ME/CFS and healthy control groups (FDR<0.1 and |log2FC|>1). Clustering heatmap was built with pheatmap [30] and PCA with FactoMineR package [31].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



