
Submitted:
13 March 2025
Posted:
14 March 2025
You are already at the latest version
Abstract
Background/Objectives: Handgrip strength (HGS) has been used as an important health indicator due to its ability to predict morbidity and mortality risks in various populations. The aim was to investigate the relationship between HGS and health parameters among public sector workers. Methods: A cross-sectional study was carried out, including the participation of 129 workers. The body composition, presence of chronic non-communicable diseases (CNCDs), physical activity level, and physical capacity (flexibility, HGS, and lower limb endurance) of the workers were evaluated. Results: The results showed that most of the employees, regardless of sex, work in the administrative sector, are aged 40 years or older, have chronic non-communicable diseases (CNCDs), and are physically inactive. The majority of women have a body mass index (BMI) within the normal range and are more flexible. On the other hand, men demonstrated greater lower limb endurance. Low HGS was associated with a higher BMI, the presence of a CNCD, and lower limb endurance. A negative correlation was observed between HGS and age, BMI, and body fat. Conversely, a positive correlation was found between HGS and muscle mass as well as with lower limb muscle endurance. Conclusions: It can be concluded that individuals with low HGS are more likely to have a high BMI, develop a CNCD, and present lower muscular endurance. Additionally, HGS was found to be reduced in older individuals and/or those with higher levels of body fat, and to be higher in those with normal physical capacity and body composition.
Keywords:
workplace health promotion
; functional capacity evaluation
; health promotion
1. Introduction
The preservation of workers' health and well-being not only contributes to their personal development but is also a crucial component for optimizing productivity and efficiency at work [1]. However, this population group faces significant challenges related to work overload, high stress levels [2,3], and changes in habits, which directly impact their quality of life [4].
The lack of resources and infrastructure, professional devaluation, limited autonomy, physical overload, lack of cooperation among colleagues, reduced team sizes, and long working hours harm health and work performance [5]. Stressful factors at work can also trigger health conditions, such as gastrointestinal problems, anxiety, depression, alcohol dependency, sleep disorders, increased aggressiveness, and suicidal thoughts [6], that negatively impact workers' health and can result in the onset of chronic non-communicable diseases (CNCDs), affecting productive capacity [7].
CNCDs, which include cardiovascular diseases, cancer, diabetes, and chronic respiratory diseases, constitute the main public health challenges globally [8]. In addition, poor working conditions are among the primary determinants of morbidities in administrative and healthcare sector employees [9,10]. It is recognized in the literature that many cases of morbidity and mortality are associated with unhealthy behaviors, such as physical inactivity [11]. These conditions worsen the disease state, as one morbidity can exacerbate another, due to their intrinsically similar mechanisms [12].
The complexity of CNCDs, combined with musculoskeletal disorders (MSDs), and their relationship with a stressful work environment requires a multifaceted approach for effective occupational health management [1]. MSDs, also referred to as cumulative traumatic disorders, are diseases that affect workers from different occupational sectors. These pathologies can cause inflammation and degeneration, injuries that mainly affect muscles, nerves, tendons, joints, and cartilage, resulting in pain and functional limitations, which are the occupational problems that cause the most harm to workers [13].
Handgrip strength (HGS) is a widely used tool, due to its ability to predict the risk of morbidity and mortality in various populations. This tool is used to evaluate the muscle strength of the upper limbs, specifically the forearm and hand, and is measured using a dynamometer. HGS has been employed in research and clinical evaluations as an indicator of overall muscle strength, muscle health, functional capacity, and nutritional status [14,15].
Furthermore, the importance of measuring HGS as a health indicator is even more evident due to its association with the onset of CNCDs, such as cardiovascular diseases and diabetes mellitus [16]. Studies indicate that a sedentary lifestyle, common among adults in work environments that require long periods of sitting, is associated with a significant decrease in HGS and, consequently, in overall muscle strength [17].
In this way, conducting research on workers' health indicators is essential for the implementation and improvement of institutional policies aimed at maintaining occupational health [18]. Thus, the objective of the present study was to investigate the relationship of HGS with health parameters in public sector workers.
2. Materials and Methods
2.1. Type of Study, Site, and Sample
This is a cross-sectional study with a quantitative approach, carried out with employees in the administrative sector of the Municipal Health Department (MHD) in the city of Jataí, located in the southwest region of the state of Goiás, Brazil.
The sample size was calculated using the G*Power® simulator, version 3.1.9.2 (Institute for Experimental Psychology in Düsseldorf, Germany), with type I and II errors defined as α = 0.05 and β = 0.05, respectively, to achieve an effect size of 0.30 or greater. Based on the sample size calculation, data collection was determined for 115 participants.
The 136 SMS employees were invited to participate in the assessments randomly and voluntarily. These assessments were linked to the extension project “Labor gymnastics for improving workers' health and quality of life”, offered by the Federal University of Jataí (UFJ). In total, 129 employees agreed to participate in the assessments.
The study was conducted in accordance with the Declaration of Helsinki. To authorize the use of the project data, the study was approved by the UFJ Research Ethics Committee (opinion: 6.625.537; CAAE 75454123.2.0000.0187) on January 26, 2024. After approval by the committee, the project was registered with the Brazilian Clinical Trials Registry Platform (ReBEC) under number: RBR-10v25rm5 (https://ensaiosclinicos.gov.br/rg/RBR-10v25rm5). Participants were informed and their verbal consent was obtained.
2.2. Inclusion and Exclusion Criteria
The inclusion criteria were: being an employee of the Jataí MHD, being 18 years of age or older, not having physical limitations and cognitive limitations that prevent the individual from performing the physical tests and answering the questionnaires. The exclusion criteria were: not participating in all stages of the physical assessment and not answering all questionnaires.
2.3. Experimental Design
The experimental design included the following steps: initially, the participants completed questionnaires about the role they perform (administrative sector or healthcare professional), sex, age, presence of CNCD, and physical activity level (PAL). Next, body composition assessments were conducted (body mass, height, body mass index (BMI), triceps skinfolds, percentage of fat, and muscle mass). Finally, the functional tests were performed (HGS, flexibility, and lower limb endurance).
2.4. Procedures
2.4.1. Physical Activity Level (PAL)
PAL was assessed using the International Physical Activity Questionnaire - Short Form (IPAQ-SF). The IPAQ-SF classifies participants as very active, active, insufficiently active, or sedentary [19]. To present the data, in the current study, individuals were classified as active (very active + active) or inactive (insufficiently active + sedentary), as proposed by [20].
2.4.2. Body Mass and Height
Body mass was measured using a calibrated analogue scale (Welmy®), accurate to 100g. Height was measured using a stadiometer attached to the scale, accurate to 0.5 cm. The body mass index (BMI) was calculated by dividing the body mass (kg) by height in meters squared.
2.4.3. Body Composition
Body composition was measured using an Omron bioimpedance scale (HBF-514C), which provided the percentage of fat and muscle mass. Waist and hip circumference were measured using a Sanny® anthropometric tape, and the waist-to-hip ratio was calculated. The right triceps skinfold was measured using a Cescorf® adipometer, accurate to 0.1 mm, and the average of three measurements was used for the results.
2.4.4. Handgrip Strength (HGS)
HGS (dominant limb) was measured using an analogue dynamometer (Saehan®; accuracy of 2 kg), with the forearm in 90º flexion, and the highest value from three attempts (30 seconds interval between attempts) was adopted as the result. The absolute strength values were divided by the body mass to find the relative HGS, as proposed in the study by [15]. The relative HGS classification was considered according to the quartile, that is, the relative HGS values in the 1st quartile (25%) were considered as low HGS, and the relative HGS values in the other quartiles (>25%) as adequate HGS [21].
2.4.5. Flexibility
Flexibility of the hamstring muscles and lower back was measured using the Wells Bench sit and reach test [22]. The test was carried out using a box measuring 30 cm long x 29 cm high x 30 cm wide, with a 27 cm scale at the top. The zero point is at the end closest to the subject and the 27 cm point coincides with the footrest. The subject removed their shoes and, in a sitting position, placed the soles of their feet on the box with their knees extended. With shoulders flexed, elbows extended, and hands supinated, the participant flexed their hips and touched the furthest point possible on the scale with their hands [23].
2.4.6. Lower Limb Endurance
Lower limb endurance was measured using the 30-second sit to stand test (SST). This test consists of sitting down and standing up from a chair as many times as possible in 30 seconds [22].
2.5. Statistical Analysis
Initially, the data were subjected to the Kolmogorov-Smirnov normality test. The associations between HGS and BMI, CNCDs, and SST were evaluated using the Fisher's exact test. The Pearson's r test was used to correlate relative HGS with participants' age, body composition, and SST. The statistical program used was GraphPad Prism 9.5.1 and the minimum significance level adopted was p<0.05.
3. Results
Initially, all 136 employees of the SMS were invited to participate in the study, of whom five declined to participate in the data collection and two were not eligible based on the inclusion criteria. Thus, 129 people were evaluated, 98 females, with an average age of 43.6 ± 10.8 years, and 31 males, with an average age of 43.3 ± 10.0 years. Regarding height, body mass, and BMI, the female participants presented the following average values: 1.60 ± 0.06 meters, 72.1 ± 18.1 kg, and 27.8 ± 6.4 kg/m², respectively, and the male participants: 1.72 ± 0.06 meters, 87.8 ± 15.8 kg, and 29.5 ± 4.7 kg/m², respectively.
Table 1 presents the characteristics of the workers. It was observed that, regardless of sex, most employees work in the administrative sector, are over 40 years of age, have a CNCD, and are physically inactive. On the other hand, when analyzed according to sex, most women showed better BMI levels (<25 kg/m²; 57.1%) and flexibility (≥25 cm; 57.7%), while men demonstrated greater lower limb endurance, as evidenced by the SST (≥25 repetitions in 30 seconds; 64.5%).
Table 2 presents the associations between low and adequate relative strength with BMI, CNCDs, and SST. An odds ratio of 3.2 times was found for people with low strength to have a higher BMI (p=0.01) and a CNCD (p=0.01). Regarding muscle endurance, evaluated by the SST, people with low strength presented a 6.2 times higher odds ratio of having worse lower limb endurance (p=0.001). No associations were found with function, age, PAL, and flexibility (p>0.05), data not shown.
Figure 1 presents the correlations between relative HGS and age, body composition, and muscle endurance of the employees. An inverse correlation was observed between age (Figure 1A), BMI (Figure 1B), fat percentage (Figure 1C), and triceps skinfold (Figure 1D) in relation to relative HGS. On the other hand, there was a positive correlation between relative HGS and muscle mass (Figure 1E) and SST (Figure 1F). Regarding flexibility, no correlation was found with relative HGS (p>0.05), data not shown.
4. Discussion
According to the data obtained in the present study, it was observed that the majority of the SMS workers evaluated, regardless of sex, work in the administrative sector, are over 40 years of age, have a CNCD, and are physically inactive. These findings are consistent with the literature that identified a similar age group profile to that found in the present study [24]. Additionally, among workers in this age group, it is common to find individuals with health patterns similar to those observed in the present research, namely, a high prevalence of CNCDs and low PAL, as indicated by [25] and [26].
Administrative sector workers often lead a physically inactive lifestyle, with short or no breaks during the workday [27]. This hypokinetic behavior leads to low energy expenditure, resulting in obesity, insulin resistance, and chronic inflammation [28]. Studies indicate that long periods of sitting are associated with physical inactivity and/or sedentary behavior [29,30,31] and increase the predisposition to the development of CNCDs [32]. Additionally, factors such as being female, having a dual workload, advanced age, and lower educational levels are also associated with an increase in physical inactivity [33].
In the current study, the BMI values presented by both sexes were greater than 25 kg/m², which characterizes overweight [34]. The main factors that can influence weight gain among professionals who work long hours are hormonal dysregulation, the consumption of ultra-processed foods, and low rates of physical activity [35].
When considering flexibility and muscle endurance, it was observed that women are more flexible, while men demonstrated greater lower limb endurance. These results confirm the differences between sexes in physical abilities, as documented in the literature, where it is commonly observed that women tend to have greater flexibility and men greater strength and muscular endurance, which is multifactorial in nature. These factors may include sex differences in height, body weight, bone and arm length, testosterone levels, muscle mass, agonist muscle voluntary activation, antagonist muscle coactivation, and participation in physical activities during childhood [36]. Higher testosterone levels in males promote an increase in muscle mass, which contributes to strength gain, while women, in turn, have higher levels of estrogen and relaxin compared to men, thus contributing to the elasticity of connective tissues and joint range of motion, resulting in greater flexibility [37].
In the present study, an inverse correlation was also observed between age and relative HGS. As age advances, there is progressive loss of muscle mass and strength, leading to a decline in functional capacity and an increased risk of developing a CNCD. Age-related muscle loss is attributed to a disruption in the regulation of skeletal muscle protein turnover, resulting in an imbalance between muscle protein synthesis and degradation [38]. Muscle strength is necessary for performing daily activities and is considered a marker of overall health [39]. Similarly, in the study by [40], a relationship was observed between HGS and physical capacity in healthy individuals. Thus, HGS may be a factor that contributes to better functionality outcomes in individuals.
The association between low HGS with elevated BMI and the prevalence of individuals with a CNCD found in the present study are consistent with data from the literature. A 22-year longitudinal study conducted in Finland, involving 963 people of both sexes aged 30 to 73, found that physically strenuous work, excess adipose tissue, smoking, cardiovascular disease, hypertension, diabetes mellitus, and asthma were predictors of muscle strength decline in workers [41]. Literature data also point to an association between an inadequate lifestyle (hypercaloric nutrition and sedentary behavior) and obesity, conditions related to the increase in pro-inflammatory mediators [42]. Age-associated adiposity exerts an adverse influence on inflammatory markers, exacerbating the infiltration of adipose tissue into skeletal muscles, which compromises structural integrity and the ability to generate strength [43,44].
In a study involving 1,395 people of both sexes, it was observed that individuals with a CNCD had lower HGS, and higher BMI levels, abdominal circumference, and fat mass compared to the control group. These results were also reflected in the sum of skinfold thickness and the body fat percentage of the group with low HGS [45]. These findings align with the data from the present study. However, the current study did not find an association between relative HGS and variables such as age and flexibility. This suggests that low relative HGS has a more direct impact on body composition, the presence of a CNCD, and lower limb muscle endurance, while other variables may be influenced by factors such as lifestyle, genetics, and individual characteristics [46].
Low HGS has been identified as a marker of musculoskeletal fitness frailty [47,48]. In a study involving 18,708 participants, it was found that factors such as low mobility, the presence of pain, and behavioral disorders were associated with lower HGS in both sexes [49]. Additionally, another study revealed that individuals with low HGS (< 28 kg for men and < 18 kg for women) had lower SST performance [50]. These results reinforce the findings of the present study, where a positive correlation was observed between relative HGS, muscle mass, and performance in the SST.
Although the current study presents some limitations, such as the sample being from a single company and the absence of control over confounding variables like diet and the daily life habits of the participants, these did not compromise the results. A sample size calculation was performed, and the number of people evaluated was representative for the study, which allowed for important inferences about the relationship between HGS and health indicators.
5. Conclusions
It can be concluded that individuals with low HGS are more likely to have a higher BMI, develop a CNCD, and present lower muscular endurance. Additionally, HGS was found to be lower in people who are older and/or have higher levels of body fat, and higher in individuals who present physical capacity and body composition parameters within normal ranges.
These results reinforce the role of HGS as a relevant health indicator among workers, highlighting its usefulness not only in the early detection of risk factors but also in promoting ongoing general monitoring of physical condition. The use of HGS can thus guide more effective preventive interventions, helping in the early identification of physical imbalances and potential health risks, such as obesity, sarcopenia, and cardiovascular diseases. This suggests that incorporating an HGS assessment into occupational exams and workplace wellness programs can contribute to improving the quality of life for workers.
Author Contributions
Conceptualization: RCSB, DMO, MB, AKACS and EVF. Methodology: JCF, RCSB, LFGS and DMO. Validation: LFGS, DMO, MB, AKACS and EVF. Formal analysis: JCF, MB and EVF. Data curation: RCSB, LFGS and MB. Project administration: JCF, DMO and MB. Rriting-original draft preparation: RCSB and JCF. Supervision: MB and EVF. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Funding
This study received financial support from the Federal University of Jataí through PROECE/UFJ notice 02/2023 - institutional support for Extension Activities that can be added to the curriculum - 2023/2024, process number: 23854.004019/2023-84.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki. To au-thorize the use of the project data, the study was approved by the UFJ Research Ethics Committee (opinion: 6.625.537; CAAE 75454123.2.0000.0187) on January 26, 2024. Af-ter approval by the committee, the project was registered with the Brazilian Clinical Trials Registry Platform (ReBEC) under number: RBR-10v25rm5 (https://ensaiosclinicos.gov.br/rg/RBR-10v25rm5). Participants were informed and their verbal consent was obtained.
Informed Consent Statement
All participants provided informed consent prior to enrollment.
Data Availability Statement
Data are available upon reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cassee, F.R.; Bleeker, E.A.J.; Durand, C.; Exner, T.; Falk, A.; Friedrichs, S.; Heunisch, E.; Himly, M.; Hofer, S.; Hofstätter, N.; Hristozov, D.; Nymark, P.; Pohl, A.; Soeteman-Hernández, L.G.; Suarez-Merino, B.; Valsami-Jones, E.; Groenewold, M. Roadmap towards safe and sustainable advanced and innovative materials. Comput Struct Biotechnol J 2024, 2, 105–126. [Google Scholar] [CrossRef]
- Useche, S.A.; Robayo, S.; Orozco-Fontalvo, M. The hidden cost of your 'too fast food': stress-related factors and fatigue predict food delivery riders' occupational crashes. Int J Occup Saf Ergon 2024, 30, 825–834. [Google Scholar] [CrossRef]
- Üngüren, E.; Tekin, Ö.A. The relationship between workplace toxicity, stress, physical activity and emotional eating. Int J Occup Saf Ergon 2024, 30, 215–223. [Google Scholar] [CrossRef]
- Tamers, S.L.; Beresford, S.A.; Cheadle, A.D.; Zheng, Y.; Bishop, S.K.; Thompson, B. The association between worksite social support, diet, physical activity and body mass index. Prev Med 2011, 53, 53–6. [Google Scholar] [CrossRef] [PubMed]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.G.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav Immun 2020, 88, 901–907. [Google Scholar] [CrossRef]
- Larsen, F.B.; Lasgaard, M.; Willert, M.V.; Sørensen, J.B. Estimating the causal effects of work-related and non-work-related stressors on perceived stress level: A fixed effects approach using population-based panel data. PLoS One 2023, 18, e0290410. [Google Scholar] [CrossRef] [PubMed]
- Tazzeo, C.; Zucchelli, A.; Vetrano, D.L.; Demurtas, J.; Smith, L.; Schoene, D.; Sanchez-Rodriguez, D.; Onder, G.; Balci, C.; Bonetti, S.; Grande, G.; Torbahn, G.; Veronese, N.; Marengoni, A. Risk factors for multimorbidity in adulthood: A systematic review. Ageing Res Rev 2023, 91, 102039. [Google Scholar] [CrossRef]
- Martinez, R.; Lloyd-Sherlock, P.; Soliz, P.; Ebrahim, S.; Vega, E.; Ordunez, P.; McKee, M. Trends in premature avertable mortality from non-communicable diseases for 195 countries and territories, 1990-2017: a population-based study. Lancet Glob Health 2020, 8, e511–e523. [Google Scholar] [CrossRef]
- Tchir, D.R.; Szafron, M.L. Occupational Health Needs and Predicted Well-Being in Office Workers Undergoing Web-Based Health Promotion Training: Cross-Sectional Study. J Med Internet Res 2020, 22, e14093. [Google Scholar] [CrossRef]
- Cohen, C.; Pignata, S.; Bezak, E.; Tie, M.; Childs, J. Workplace interventions to improve well-being and reduce burnout for nurses, physicians and allied healthcare professionals: a systematic review. BMJ Open 2023, 13, e071203. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Powell, K.E.; Jakicic, J.M.; Troiano, R.P.; Piercy, K.; Tennant, B. Sedentary Behavior and Health: Update from the 2018 Physical Activity Guidelines Advisory Committee. Med Sci Sports Exerc 2019, 51, 1227–1241. [Google Scholar] [CrossRef]
- Mixter, S.; Mathiassen, S.E.; Bjärntoft, S.; Lindfors, P.; Lyskov, E.; Hallman, D.M. Fatigue, Stress, and Performance during Alternating Physical and Cognitive Tasks-Effects of the Temporal Pattern of Alternations. Ann Work Expo Health 2021, 65, 1107–1122. [Google Scholar] [CrossRef]
- Alavi, S.S.; Abbasi, M.; Mehrdad, R. Risk Factors for Upper Extremity Musculoskeletal Disorders Among Office Workers in Qom Province, Iran. Iran Red Crescent Med J 2016, 18, e29518. [Google Scholar] [CrossRef]
- Wen, Z.; Gu, J.; Chen, R.; Wang, Q.; Ding, N.; Meng, L.; Wang, X.; Liu, H. Sheng, Z.; Zheng, H. Handgrip Strength and Muscle Quality: Results from the National Health and Nutrition Examination Survey Database. J Clin Med 2023, 12, 3184. [CrossRef]
- Gouvêa-E-Silva, L.F.; Brito, E.R.; Sol, N.C.C.; Fernandes, E.V.; Xavier, M.B. Relationship of handgrip strength with health indicators of people living with HIV in west Pará, Brazil. Int J STD AIDS 2023, 34, 932–939. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.Y. Importance of Handgrip Strength as a Health Indicator in the Elderly. Korean J Fam Med 2021, 42, 1. [Google Scholar] [CrossRef] [PubMed]
- Lee, S. Associations Between Dietary Patterns and Handgrip Strength: The Korea National Health and Nutrition Examination Survey 2014-2016. J Am Coll Nutr 2020, 39, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Väisänen, D.; Kallings, L.V.; Andersson, G.; Wallin, P.; Hemmingsson, E.; Ekblom-Bak, E. Lifestyle-associated health risk indicators across a wide range of occupational groups: a cross-sectional analysis in 72,855 workers. BMC Public Health 2020, 20, 1656. [Google Scholar] [CrossRef]
- Lee, P.H.; Macfarlane, D.J.; Lam, T.H.; Stewart, S.M. Validity of the International Physical Activity Questionnaire Short Form (IPAQ-SF): a systematic review. Int J Behav Nutr Phys Act 2011, 8, 115. [Google Scholar] [CrossRef]
- Oliveira, D.M.; Gouvêa-e-Silva, L.F.; da Costa, V.S.; Villela, E.F.M.; Fernandes, E.V. Association between social isolation, level of physical activity, and sedentary behavior in pandemic times. Rev. Bras. Promoç. Saúde 2021, 34, 12280. [CrossRef]
- Basso, G.D.B.; Siqueira, M.A.; Kono, E.M.; Souza, J.D.; Baseggio, L.T.; Fernandes, E.V.; Takanashi, S.Y.L.; Gouvêa-e-Silva, L.F. Relationship between handgrip strength and body composition and laboratory indicators in diabetic and hypertensive patients. Medicina (Ribeirão Preto) 2023, 56, e-210088. [CrossRef]
- Heubel, A.D.; Gimenes, C.; Marques, T.S.; Arca, E.A.; Martinelli, B.; Barrile, S.R. Multicomponent training improves functional fitness and glycemic control in elderly people with type 2 diabetes. J Phys Educ 2018, 29, e2922. [Google Scholar] [CrossRef]
- Ribeiro, C.C.A.; Abad, C.C.C.; Barros, R.V.; Barros Neto, T.L. Flexibility level obtained by the sit-and-reach test from a study conducted in Greater São Paulo. Braz. J. Cineantropon. Hum Perform 2010, 12, 415–421. [Google Scholar] [CrossRef]
- Demissie, B.; Bayih, E.T.; Demmelash, A.A. A systematic review of work-related musculoskeletal disorders and risk factors among computer users. Heliyon 2024, 10, e25075. [Google Scholar] [CrossRef]
- Booth, F.W.; Roberts, C.K.; Thyfault, J.P.; Ruegsegger, G.N.; Toedebusch, R.G. Role of Inactivity in Chronic Diseases: Evolutionary Insight and Pathophysiological Mechanisms. Physiol Rev 2017, 97, 1351–1402. [Google Scholar] [CrossRef]
- Zhao, M.; Wu, Z.; Huang, Y.; Jiang, Z.; Mo, X.; Lowis, H.; Zhao, Y.; Zhang, M. Role of the physical fitness test in risk prediction of diabetes among municipal in-service personnel in Guangxi. Medicine (Baltimore) 2019, 98, e15842. [Google Scholar] [CrossRef] [PubMed]
- Tersa-Miralles, C.; Pastells-Peiró, R.; Rubí-Carnacea, F.; Bellon, F.; Rubinat Arnaldo, E. Effectiveness of workplace exercise interventions in the treatment of musculoskeletal disorders in office workers: a protocol of a systematic review. BMJ Open 2020, 2020 10, e038854. [Google Scholar] [CrossRef]
- Friedenreich, C.; Lynch, B. Can living a less sedentary life decrease breast cancer risk in women? Womens Health (Lond) 2012, 8, 5–7. [Google Scholar] [CrossRef]
- Bácsné, Bába. É.; Müller, A.; Pfau, C.; Balogh, R.; Bartha, É.; Szabados, G.; Bács, Z.; Ráthonyi-Ódor, K., Ráthonyi, G. Sedentary Behavior Patterns of the Hungarian Adult Population. Int J Environ Res Public Health 2023, 20, 2702. [CrossRef]
- Evenson, K.R.; Alhusseini, N.; Moore, C.C.; Hamza, M.M.; Al-Qunaibet, A.; Rakic, S.; Alsukait, R.F.; Herbst, C.H.; AlAhmed, R.; Al-Hazzaa, H.M.; Alqahtani, S.A. Scoping Review of Population-Based Physical Activity and Sedentary Behavior in Saudi Arabia. J Phys Act Health 2023, 20, 471–486. [Google Scholar] [CrossRef]
- Huang, H.C.; Chang, S.H.; Yang, X. Relationship between Sociodemographic and Health-Related Factors and Sedentary Time in Middle-Aged and Older Adults in Taiwan. Medicina (Kaunas) 2024, 60, 444. [Google Scholar] [CrossRef]
- Mclaughlin, M.; Atkin, A.J.; Starr, L.; Hall, A.; Wolfenden, L.; Sutherland, R.; Wiggers, J.; Ramirez, A.; Hallal, P.; Pratt, M.; Lynch, B.M.; Wijndaele, K. Sedentary, Behaviour Council Global Monitoring Initiative Working Group. Worldwide surveillance of self-reported sitting time: a scoping review. Int J Behav Nutr Phys Act 2020, 17, 111. [CrossRef]
- Rocha, S.V.; Barbosa, A.R.; Araújo, T.M. Leisure-time physical inactivity among healthcare workers. Int J Occup Med Environ Health 2018, 31, 251–260. [Google Scholar] [CrossRef] [PubMed]
- Elmaleh-Sachs, A.; Schwartz, J.L.; Bramante, C.T.; Nicklas, J.M.; Gudzune, K.A.; Jay, M. Obesity Management in Adults: A Review. JAMA 2023, 330, 2000–2015. [Google Scholar] [CrossRef]
- Tavares Amaro, M.G.; Conde de Almeida, R.A.; Marques Donalonso, B.; Mazzo, A.; Negrato, C.A. Prevalence of overweight and obesity among health professionals with shift work schedules: A scoping review. Chronobiol Int 2023, 40, 343–352. [Google Scholar] [CrossRef]
- Nuzzo, J.L. Narrative Review of Sex Differences in Muscle Strength, Endurance, Activation, Size, Fiber Type, and Strength Training Participation Rates, Preferences, Motivations, Injuries, and Neuromuscular Adaptations. J Strength Cond Res 2023, 37, 494–536. [Google Scholar] [CrossRef]
- Berger, G.K.; Rockov, Z.A.; Byrne, C.; Trentacosta, N.E.; Stone, M.A. The role of relaxin in anterior cruciate ligament injuries: a systematic review. Eur J Orthop Surg Traumatol 2023, 33, 3319–3326. [Google Scholar] [CrossRef] [PubMed]
- Udo, T.; Grilo, C.M. Physical activity levels and correlates in nationally representative sample of U.S. adults with healthy weight, obesity, and binge-eating disorder. Int J Eat Disord 2020, 53, 85-95. [CrossRef]
- Lima, T.R.D.; Silva, D.A.S.; Kovaleski, D.F.; González-Chica, D.A. The association between muscle strength and sociodemographic and lifestyle factors in adults and the younger segment of the older population in a city in the south of Brazil. Ciencia & saude coletiva 2018, 23, 3811-3820. [CrossRef]
- Seo, H.S.; Lee, H.; Kim, S.; Lee, S.K.; Lee, K.Y.; Kim, N.H.; Shin, C. Paravertebral Muscles as Indexes of Sarcopenia and Sarcopenic Obesity: Comparison With Imaging and Muscle Function Indexes and Impact on Cardiovascular and Metabolic Disorders. AJR Am J Roentgenol 2021, 216, 1596–1606. [Google Scholar] [CrossRef] [PubMed]
- Stenholm, S.; Tiainen, K.; Rantanen, T.; Sainio, P.; Heliövaara, M.; Impivaara, O.; Koskinen, S. Long-term determinants of muscle strength decline: prospective evidence from the 22-year mini-Finland follow-up survey. J Am Geriatr Soc 2012, 60, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Monteiro, R.; Azevedo, I. Chronic inflammation in obesity and the metabolic syndrome. Mediators Inflamm 2010, 2010, 289645. [Google Scholar] [CrossRef]
- Zamboni, M.; Mazzali, G.; Fantin, F.; Rossi, A.; Di Francesco, V. Sarcopenic obesity: a new category of obesity in the elderly. Nutr Metab Cardiovasc Dis 2008, 18, 388–95. [Google Scholar] [CrossRef]
- Choi, S.J.; Files, D.C.; Zhang, T.; Wang, Z.M.; Messi, M.L.; Gregory, H.; Stone, J.; Lyles, M.F.; Dhar, S.; Marsh, A.P.; Nicklas, B.J.; Delbono, O. Intramyocellular Lipid and Impaired Myofiber Contraction in Normal Weight and Obese Older Adults. J Gerontol A Biol Sci Med Sci 2016, 71, 557–64. [Google Scholar] [CrossRef]
- Wan, X.; Ji, Y.; Wang, R.; Yang, H.; Cao, X., Lu, S. Association between systemic immune-inflammation index and sarcopenic obesity in middle-aged and elderly Chinese adults: a cross-sectional study and mediation analysis. Lipids Health Dis 2024, 23, 230. [CrossRef]
- Silva, N.A.; de Menezes, T.N.; de Melo, R.L.P.; Pedraza, D.F. Handgrip strength and flexibility and their association with anthropometric variables in the elderly. Revista da Associação Médica Brasileira 2013, 59, 128-135. [CrossRef]
- Ballarin, G.; Valerio, G.; Alicante, P.; Di Vincenzo, O.; Monfrecola, F.; Scalfi, L. Could BIA-derived phase angle predict health-related musculoskeletal fitness? A cross-sectional study in young adults. Nutrition 2024, 122, 112388. [Google Scholar] [CrossRef]
- Smith, L.; López Sánchez, G.F.; Veronese, N.; Soysal, P.; Kostev, K.; Jacob, L.; Rahmati, M.; Kujawska, A.; Tully, M.A.; Butler, L.; Il Shin, J.; Koyanagi, A. Association Between Pain and Sarcopenia Among Adults Aged ≥65 Years from Low- and Middle-Income Countries. J Gerontol A Biol Sci Med Sci 2023, 78, 1020–1027. [Google Scholar] [CrossRef]
- Jung, H.I.; Gu, K.M.; Park, S.Y.; Baek, M.S., Kim, W.Y.; Choi, J.C.; Shin, J.W.; Kim, J.Y.; Chang, Y.D.; Jung, J.W. Correlation of handgrip strength with quality of life-adjusted pulmonary function in adults. PLoS One 2024, 19, e0300295. [CrossRef]
- Kim, S.H.; Kim, T.; Park, J.C.; Kim, Y.H. Usefulness of hand grip strength to estimate other physical fitness parameters in older adults. Sci Rep 2022, 12, 17496. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Correlations between relative handgrip strength and age (1A), body mass index (1B), body fat (1C), triceps skinfold (1D), muscle mass (1F), and the 30-second sit to stand test (1G).
Figure 1.
Correlations between relative handgrip strength and age (1A), body mass index (1B), body fat (1C), triceps skinfold (1D), muscle mass (1F), and the 30-second sit to stand test (1G).
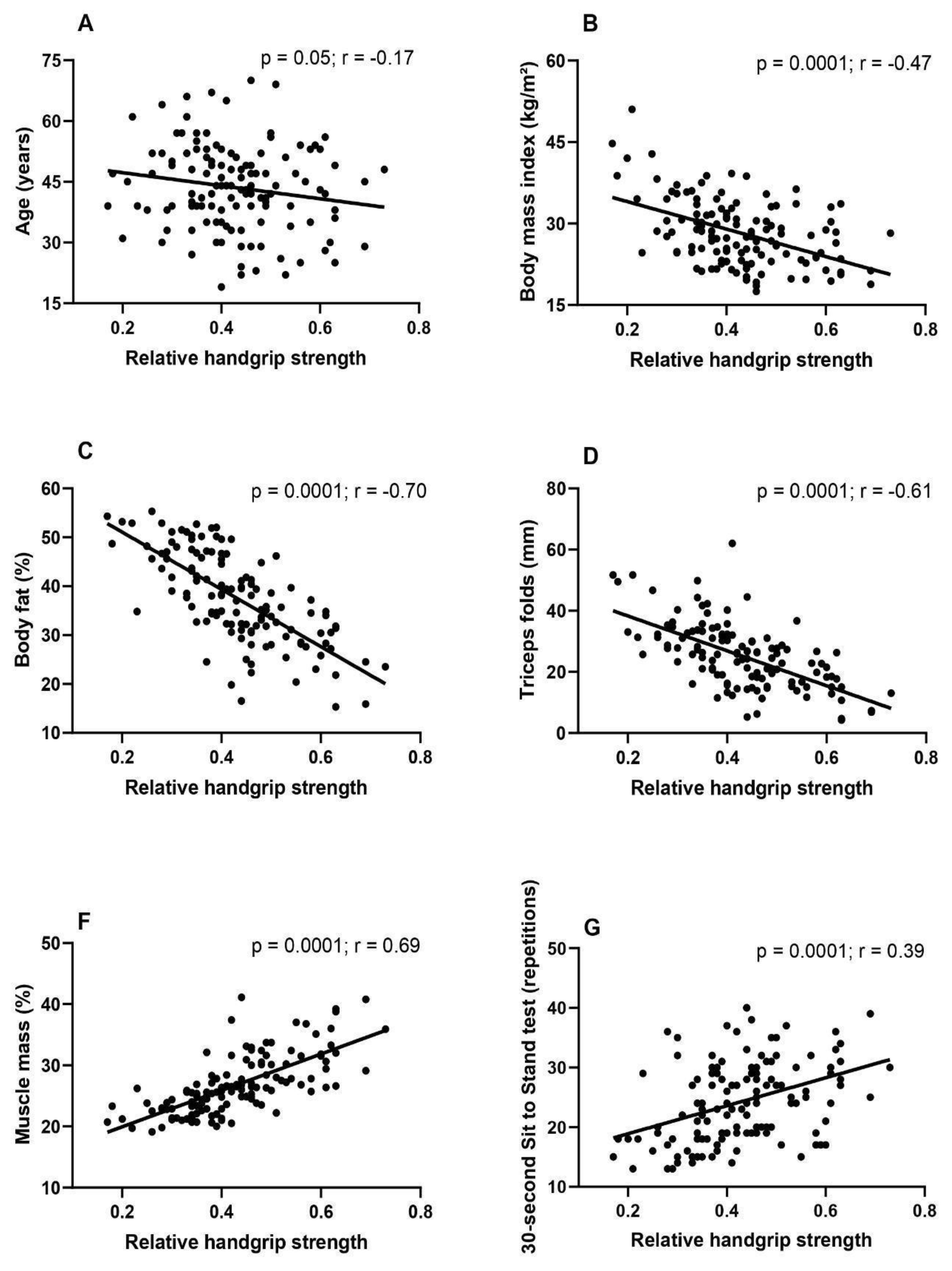

Table 1.
Functional characteristics, age, and body composition of the employees.
| Variables | Male | Female |
|---|---|---|
| n (%) | n (%) | |
| Function | ||
| Administrative sector | 24 (77.4) | 63 (64.3) |
| Healthcare professional | 07 (22.6) | 35 (35.7) |
| Age (years) | ||
| <40 | 11 (35.5) | 36 (36.7) |
| ≥40 | 20 (64.5) | 62 (63.3) |
| CNCD | ||
| Yes | 17 (54.8) | 63 (64.3) |
| No | 14 (45.2) | 35 (35.7) |
| PAL | ||
| Active | 12 (38.7) | 47 (48.0) |
| Inactive | 19 (61.3) | 5 (52.0) |
| BMI (kg/m²) | ||
| <25 | 06 (19.4) | 56 (57.1) |
| ≥25 | 25 (80.6) | 42 (42.9) |
| Flexibility(cm) | ||
| <25 | 18 (56.2) | 41 (42.3) |
| ≥25 | 14 (43.8) | 56 (57.7) |
| SST (repetitions) | ||
| <25 | 11 (35.5) | 58 (59.2) |
| ≥25 | 20 (64.5) | 40 (40.8) |
Legend: CNCD, chronic non-communicable disease; PAL, physical activity level; BMI, body mass index; SST, 30-second sit to stand test. Data expressed in absolute (n) and relative values (%).
Table 2.
Association between relative strength and body composition, presence of chronic non-communicable diseases, and lower limb endurance in employees.
Table 2.
Association between relative strength and body composition, presence of chronic non-communicable diseases, and lower limb endurance in employees.
| Variables | HGS relative | p | OR (95%CI) | |
|---|---|---|---|---|
| Low | Adequate | |||
| n (%) | n (%) | |||
| BMI (kg/m²) | ||||
| ≥25 | 29 (82.9) | 56 (59.6) | 0.01 | 3.2 (1.29 - 8.40) |
| <25 | 06 (17.1) | 38 (40.4) | ||
| CNCD | ||||
| Yes | 28 (80.0) | 52 (55.3) | 0.01 | 3.2 (1.24 - 8.11) |
| No | 07 (20.0) | 42 (44.7) | ||
| SST (repetitions) | ||||
| <25 | 29 (82.9) | 41 (43.6) | 0.001 | 6.2 (2.47 - 15.92) |
| ≥25 | 06 (17.1) | 53 (56.4) | ||
Legend: BMI, body mass index; CNCD, chronic non-communicable disease; SST, 30-second sit to stand test. OR, odds ratio; 95%CI, 95% confidence interval.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



