
Submitted:
06 April 2025
Posted:
07 April 2025
Read the latest preprint version here
Abstract
Background/Objectives: Major depressive disorder (MDD), a debilitating psychiatric condition, is intricately linked to neuroinflammation, oxidative stress, mitochondrial dysfunction, disrupted tryptophan–kynurenine pathways, and an urgent need for novel, plant-based therapeutics such as curcumin and other natural antidepressants. Emerging evidence further highlights altered brain-derived neurotrophic factor (BDNF) signaling in MDD, making the search for integrative, phytomedicine-oriented interventions more critical than ever. Methods: This systematic review critically analyzed 62 articles initially retrieved from PubMed, Cochrane, EMBASE, and Google Scholar databases, with 19 studies deemed eligible for comprehensive synthesis. Results: The included investigations spanned diverse populations and examined the therapeutic potential of phytochemicals to modulate neuroimmune interactions, reduce oxidative injury, and enhance mood-related biomarkers. Among the promising candidates, curcumin, polyphenols, and flavonoid-rich extracts consistently demonstrated improvements in depressive symptoms, often by targeting pro-inflammatory mediators and promoting neuroplasticity. These findings reinforce the notion that bioactive compounds from plants may serve as effective adjunctive or standalone strategies in MDD management, particularly for individuals who experience limited benefit from conventional approaches. Conclusions: This study demonstrates the growing feasibility of phytomedicine as a powerful complement to existing treatment paradigms. Future work should focus on standardized dosing, long-term safety, and mechanistic studies that clarify how plant-derived compounds can be leveraged for more robust, personalized depression care. Such integrative approaches promise to broaden therapeutic horizons and spark novel research pathways in translational neuroscience.
Keywords:
major depressive disorder (MDD)
; plant-based therapeutics
; neuroinflammation
; oxidative stress
; natural antidepressants
; tryptophan
; kynurenine
; brain-derived neurotrophic factor(BDNF)
; mitochondrial dysfunction
; curcumin
1. Introduction
Major depressive disorder (MDD) is a highly prevalent and disabling psychiatric condition, characterized by pervasive low mood, anhedonia, cognitive dysfunction, and significant impairments in occupational, social, and interpersonal functioning [1]. Beyond its impact on quality of life, MDD remains the leading psychiatric contributor to global suicide mortality, with core symptoms including diminished self-worth, excessive guilt, psychomotor changes, and sleep disturbances—factors that collectively contribute to increased all-cause mortality rates [2]. Patients with MDD often exhibit persistent negative cognitive biases, social withdrawal, and disrupted emotional regulation [3]. Epidemiological data indicate a growing global burden, currently affecting over 350 million individuals, with projections by the World Health Organization suggesting that MDD will become the leading cause of disability worldwide by 2030 [4]. Vulnerable populations—including pregnant women, the elderly, and children—exhibit disproportionately high incidence rates, underscoring the role of psychosocial stressors, genetic susceptibility, and environmental adversity in its etiology [5,6,7,8]. Chronic stress, in particular, has been implicated in the pathophysiology of MDD through its capacity to disrupt neuroplastic processes, inducing neuronal atrophy, synaptic loss, and volumetric changes in key brain regions such as the hippocampus and prefrontal cortex, ultimately driving the affective, cognitive, and behavioral symptoms characteristic of the disorder [9,10,11]. Figure 1 summarizes the primary neurobiological mechanisms involved in MDD pathogenesis.
Emerging evidence underscores the critical role of neuroinflammatory processes in the pathogenesis of MDD, positioning central nervous system (CNS) inflammation as a key mechanistic driver in a subset of patients [12]. A growing body of research implicates dysregulation within the kynurenine pathway of tryptophan metabolism—a principal biosynthetic route for serotonin—in contributing to both decreased serotonergic tone and increased production of neurotoxic metabolites [13]. These metabolic shifts not only compromise neurotransmitter homeostasis but also enhance susceptibility to mood dysregulation and cognitive impairment, hallmarks of depressive pathology [14,15,16,17]. Moreover, metabolomic profiling studies in individuals with MDD consistently report aberrations in a range of circulating metabolites, including tryptophan, tyrosine, methionine, valine, phenylalanine, pyruvate, kynurenic acid, and deoxycholic acid [18]. These metabolic disruptions are closely associated with impaired neuroprotective mechanisms, increased oxidative burden, dysregulated apoptotic signaling, and chronic low-grade inflammation [19,20,21]. Collectively, these pathophysiological alterations foster a neurobiological environment conducive to the initiation and persistence of depressive symptoms, particularly through the destabilization of neuronal resilience and synaptic integrity [22].
While conventional pharmacological treatments—particularly tricyclic antidepressants (TCAs) such as imipramine, amitriptyline, clomipramine, desipramine, and doxepin—remain foundational in the management of MDD, their therapeutic efficacy is primarily mediated through modulation of monoaminergic neurotransmission, specifically by increasing synaptic concentrations of serotonin and norepinephrine [4]. Despite their clinical utility, accumulating evidence indicates that antidepressants, though considered first-line interventions, do not represent the only effective modality for managing MDD [2]. Notably, in pediatric and adolescent populations, non-pharmacological strategies—including psychosocial support, structured physical activity, and nutritional optimization—have demonstrated clinically relevant preventive and therapeutic effects [23]. Nonetheless, a significant proportion of individuals exhibit partial or complete resistance to these interventions, highlighting the need for adjunctive or alternative therapeutic strategies [24]. In this context, phytotherapeutics have gained renewed scientific interest due to their historical use, biological plausibility, cost-effectiveness, and favorable side-effect profiles. Medicinal plants have long served as a source of bioactive compounds with neuroprotective, anti-inflammatory, and neuromodulatory properties [25]. These natural products continue to inform the discovery and development of novel pharmacological agents, offering a potentially valuable adjuvant approach for individuals with treatment-resistant or recurrent depression [26,27].
Phytochemicals are naturally occurring bioactive compounds found in a wide array of plants and dietary sources, contributing to their pigmentation, aroma, and flavor profiles [28]. These compounds span diverse chemical classes—including alkaloids, flavonoids, steroids, coumarins, and terpenoids such as eucalyptol—and have been increasingly recognized for their therapeutic properties, particularly in conditions driven by oxidative stress and chronic inflammation [29]. Beyond their well-established antioxidant and anti-inflammatory actions, phytochemicals also exhibit vasoprotective and cardiometabolic benefits, positioning them as promising agents in the prevention and management of complex, multifactorial disorders [30]. Within the field of neuropsychiatry, phytocompounds have garnered substantial attention for their potential roles in modulating key neurobiological processes implicated in neurodegenerative and mood disorders. Compounds derived from plants such as Aizoaceae, Acorus, Korthalsella, Astragalus membranaceus, Sophora flavescens, and Ononis spinosa have long been employed in traditional medicine systems for their psychotropic and neuromodulatory effects [31,32,33]. Preclinical studies and emerging clinical trials suggest that several of these botanicals exert antidepressant-like effects through mechanisms involving monoaminergic modulation, neurotrophic signaling, and suppression of neuroinflammatory cascades [34]. As such, the integration of phytocompounds into therapeutic frameworks for MDD is increasingly being explored, both as standalone treatments and as adjuncts to conventional pharmacotherapy [35]. Their potential to target multiple pathological domains simultaneously renders them particularly relevant in the context of MDD, a disorder characterized by complex and heterogeneous neurobiological underpinnings [36].
It is well established that neurodevelopment intricately shapes emotional regulation and cognitive function, both of which are highly susceptible to disruption by psychiatric and neurological disorders [37]. In recent decades, the global burden of neuropsychiatric conditions—particularly those with complex, multifactorial etiologies such as MDD—has escalated significantly, placing substantial pressure on healthcare systems and highlighting the urgent need for innovative, accessible, and well-tolerated therapeutic strategies [38,39,40]. Although conventional antidepressants remain central to current treatment paradigms, their limitations—namely delayed onset of action, treatment resistance, and undesirable side effect profiles—have driven the search for alternative and adjunctive interventions that can engage broader neurobiological targets with improved safety margins [41,42].
In this context, phytocompounds have emerged as promising candidates due to their pleiotropic mechanisms of action, encompassing anti-inflammatory, antioxidant, and neuromodulatory properties [43]. However, despite mounting preclinical evidence and isolated clinical investigations suggesting their potential benefit, no prior systematic review has comprehensively synthesized the clinical trial literature evaluating the efficacy of general phytocompounds in MDD [44]. Addressing this gap, the present review aims to critically evaluate and consolidate available interventional evidence from human studies, with a specific focus on the therapeutic effects, mechanistic underpinnings, and translational relevance of phytochemicals in the treatment of depression. By doing so, we aim to provide a scientifically rigorous and clinically informative resource for guiding future research and potential integration of phytotherapeutics into evidence-based psychiatric care.
2. Materials and Methods
2.1. Focused Question
This systematic review intended to answer the question: Can phytocompounds consumption benefit patients with MDD? is the targeted therapeutic intervention capable of yielding a measurable improvement in symptom progression compared to standard care alone? We started by surveying existing literature to identify gaps in current understanding and zeroed in on this specific inquiry because it addresses a major clinical hurdle. By doing so, we aimed to ensure that every step of our methodology—from patient selection to data collection—stayed aligned with the single, most critical issue at hand: quantifying whether our proposed treatment truly moves the needle for patients in a meaningful way.
2.2. Language
This study exclusively employed clinical trials in the English language for literature searches, data collection, and participant interactions. We did not rely on any foreign-language sources, believing that an English-only focus would simplify our review process and minimize translational discrepancies. By narrowing our scope to the most widely accessible corpus of medical literature, we aimed to ensure comprehensive coverage without introducing linguistic ambiguities. This uniform approach kept every phase of the project consistent and transparent.
2.3. Literature Search and Databases
A comprehensive literature search was conducted across four major biomedical databases—Google Scholar, Cochrane Library, EMBASE, and MEDLINE/PubMed—to identify studies investigating the therapeutic relevance of phytocompounds in the context of MDD. The search strategy employed Boolean combinations of the following terms: “Major Depressive Disorder” OR “depression” AND “phytocompounds” OR “phytochemicals” OR “plant-derived compounds.” Study selection was independently performed by two reviewers (A.C.F.G. and F.F.F.) to ensure methodological rigor and minimize bias. In instances where inclusion decisions were incongruent, a third reviewer (L.P.A.) served as an adjudicator to reach consensus. This dual-reviewer model with conflict resolution ensured consistency in study eligibility, aligning with PRISMA guidelines and reinforcing the integrity of the evidence synthesis. The methodological emphasis remained on studies with clearly defined endpoints related to symptom progression, treatment response, and neurobiological mechanisms, with the aim of elucidating how phytocompounds may modulate core processes implicated in the onset, maintenance, and treatment resistance of MDD.
2.4. Study Selection
This review was designed to synthesize interventional studies investigating the therapeutic potential of phytocompounds in the treatment of MDD. Inclusion criteria were restricted to experimental studies that employed well-characterized phytochemicals as the primary treatment modality in populations formally diagnosed with MDD. Eligible studies were required to assess outcomes relevant to depressive symptomatology and, where applicable, include mechanistic endpoints related to neurotransmission, neurotrophic signaling, inflammation, or oxidative stress.
To ensure methodological consistency and reduce interpretive variability, we applied stringent exclusion criteria. Studies were excluded if they (i) involved heterogeneous or unstandardized mixtures of phytocompounds without compound-specific analysis; (ii) were published in languages other than English; or (iii) fell outside the scope of primary research, including editorials, commentaries, conference proceedings, poster abstracts, case reports, and gray literature. This rigorous selection process ensured that the synthesized evidence was derived exclusively from high-quality interventional designs capable of supporting mechanistic inference and clinical translation. The goal was to distill a coherent and actionable understanding of how phytochemicals may modulate core neurobiological processes implicated in the onset, maintenance, and treatment resistance of MDD.
2.5. Data Extraction
This review focused exclusively on the synthesis of interventional studies evaluating the efficacy of phytocompounds in the treatment of MDD. No temporal restrictions were applied in the literature search, thereby enabling a comprehensive inclusion of both foundational and recent studies relevant to the evolving understanding of phytochemical interventions in depression. To standardize data extraction and facilitate consistent interpretation across heterogeneous trial designs, we employed the PICO (Population, Intervention, Comparison, and Outcomes) framework.
The Population component included individuals diagnosed with MDD according to standardized diagnostic criteria (DSM-IV, DSM-5, or ICD-10). The Intervention was defined as the administration of isolated or standardized phytocompounds, either as monotherapy or as adjunctive treatment to conventional antidepressants. Comparisons included placebo, standard pharmacotherapy, or other active comparators. Outcomes were limited to clinically validated measures of depressive symptom severity (e.g., HAM-D, MADRS, BDI), along with secondary outcomes such as remission rates, response rates, and tolerability profiles when available.
By anchoring our methodological framework to the PICO structure, we ensured a high level of analytical precision in synthesizing data on the therapeutic relevance of phytochemicals, particularly in relation to their potential neuromodulatory roles in the pathophysiology and treatment resistance of depression.
2.6. Search and Selection of the Relevant Articles
The selection of studies for this review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, ensuring methodological transparency, reproducibility, and rigor throughout the screening and inclusion process [45,46]. All retrieved records underwent a two-tiered selection protocol: an initial title and abstract screening followed by full-text evaluation based on predefined eligibility criteria. This approach facilitated a systematic appraisal of interventional studies investigating the efficacy of phytocompounds in the treatment of MDD.
The application of PRISMA methodology allowed for the consistent identification and extraction of relevant clinical trials that met the inclusion parameters—namely, the use of well-characterized phytochemicals as therapeutic agents and the assessment of depression-related outcomes in formally diagnosed MDD populations. Discrepancies during the selection process were resolved through consensus or consultation with a third reviewer to uphold methodological consistency. This framework ensured that only high-quality interventional evidence was synthesized, enabling robust interpretation of the neuromodulatory and therapeutic potential of phytocompounds in the context of depression onset, chronicity, and treatment resistance.
2.7. Quality Assessment
To ensure the methodological quality and internal validity of the included interventional studies, we adhered to the evaluative criteria outlined in the Cochrane Handbook for Systematic Reviews of Interventions [47]. This framework was employed to systematically assess the risk of bias across multiple domains, including random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, completeness of outcome data, selective reporting, and other potential sources of bias.
Each domain was independently evaluated by two reviewers using the Cochrane Risk of Bias tool (RoB 2.0), with discrepancies resolved through discussion or adjudication by a third reviewer when necessary. The use of this standardized tool ensured that bias assessment was both transparent and reproducible, thereby strengthening the interpretive reliability of the synthesized findings. This quality appraisal process was critical to distinguishing high-confidence evidence from studies with methodological limitations and enabled a more nuanced understanding of the extent to which phytocompounds may exert clinically meaningful effects on depressive symptomatology through neuromodulatory mechanisms.
3. Results
3.1. Literature Search and Study Selection
A total of 62 records were initially retrieved through systematic searches of major biomedical databases using predefined search terms related to phytocompounds and MDD. Following the removal of 30 articles—due to duplication, non-English language, unpublished manuscripts, poster presentations, conference abstracts, and gray literature—32 articles remained for preliminary screening. After title and abstract evaluation, 22 full-text articles were selected for comprehensive eligibility assessment. These studies were further appraised for their methodological rigor, relevance to the research question, and the clarity of outcome reporting. Of the 22, three were excluded due to methodological limitations, insufficient alignment with predefined inclusion criteria, or incomplete outcome data. Ultimately, 19 interventional studies—predominantly randomized controlled trials and open-label interventions—met the eligibility requirements and were included in the final qualitative synthesis (Figure 2). These studies represent a diverse range of phytochemical agents evaluated for their antidepressant efficacy across varied populations and clinical settings, providing a rich foundation for further analysis (Table 1).
*Consider, if feasible to do so, reporting the number of records identified from each database or register searched (rather than the total number across all databases/registers).
**If automation tools were used, indicate how many records were excluded by a human and how many were excluded by automation tools.

Table 1.
Summary of Interventional Studies Evaluating the Therapeutic Effects of Phytocompounds in Major Depressive Disorder (MDD). This table presents a structured synthesis of the 19 clinical trials included in the systematic review, selected according to PRISMA guidelines. Each study is characterized by its design, geographic location, sample demographics, intervention type, control conditions, outcome measures, and reported adverse events. The interventions include a range of phytocompounds—such as curcumin, flavonoids, anthocyanins, and isoflavones—administered in monotherapy or adjunctive formats. Outcomes were assessed via validated psychometric scales and, where applicable, supported by biochemical and neurotrophic markers. This compilation provides a comparative overview of study quality, efficacy, and safety in the clinical application of phytochemicals for MDD.
Table 1.
Summary of Interventional Studies Evaluating the Therapeutic Effects of Phytocompounds in Major Depressive Disorder (MDD). This table presents a structured synthesis of the 19 clinical trials included in the systematic review, selected according to PRISMA guidelines. Each study is characterized by its design, geographic location, sample demographics, intervention type, control conditions, outcome measures, and reported adverse events. The interventions include a range of phytocompounds—such as curcumin, flavonoids, anthocyanins, and isoflavones—administered in monotherapy or adjunctive formats. Outcomes were assessed via validated psychometric scales and, where applicable, supported by biochemical and neurotrophic markers. This compilation provides a comparative overview of study quality, efficacy, and safety in the clinical application of phytochemicals for MDD.
| REFERENCE | MODEL/COUNTRY | POPULATION | INTERVENTION/ COMPARISON | OUTCOMES | SIDE EFFECTS | |
|---|---|---|---|---|---|---|
| [48] | Randomized double-blind placebo-controlled clinical trial/ Iran |
42 patients with CSFP; 35–70 y, 25 ≤ body mass index < 40 kg/m2) | Participants received 80 mg/day nano-curcumin or placebo for 12 weeks. | Mental component summary scores significantly improved in the treated group; more patients with lower degrees of depression were found in the intervention group (p = 0.046). | Nausea, headache, diarrhea. | |
| [49] [50] https://pubmed.ncbi.nlm.nih.gov/35745176/ (Não conseguimos citar, mas encontramos no endnote) [51] [52] [53] [54] [55] [56] |
Randomized, double-blind, placebo-controlled / Iran. Randomized, simple blind, controlled/ South Korea. Randomized, double- blind, placebo-controlled / Japan. Randomized, simple-blind, controlled / South Korea. Randomized, parallel and open/ Slovakia. Randomized, double-blind, placebo-controlled/ United Kingdom. Randomized, double- blind, placebo-controlled / Italy Randomized, double-blind, placebo-controlled/ Japan. Randomized, double-blind, placebo-controlled/ Japan. |
76 individuals – all ♂ - 35 to 65 y. Study 40 young ♂ and ♀ with MDD – Age: 18 to 29 y. Study with 15 individuals – 4 (♂) and 11 (♀) – Age: 50–70 y. Study with 40 individuals – 16 (♂) and 24 (♀) – Age: 20-30 y. Study with 67 individuals of both sexes with MDD -20 (♂) and 47 (♀) -Age: 18-65 y. Study 1 with 21 individuals – 2 (♂) and 19 (♀) – Age: 18 - 21 y; Study 2 with 52 children – 23 (♂) and 29 (♀) – Age: 7 - 10 y. Study with 60 (♂) recently menopausal - 50 - 55 y. Study 87 women's who presented at least one symptom of menopause in MSS – Age: 40 - 60 y. Study with 91 women with at least one symptom of menopause – Age: 40 – 60 years. |
G1: quercetin, 500 mg/day; G2: placebo, 500 mg/day; for 8 weeks. G1: FR ou FL; They consumed FR or FL three times a day (30–60 minutes before breakfast, lunch, and dinner; 190 mL per bottle); for 8 weeks. G1: Potatoes – SQ - Naturally contains anthocyanins - containing 45 mg of anthocyanin; G2: Potatoes – Haruka; Subjects ate potatoes (75 g) cooked - microwaved for 2 min once a day / for 8 weeks, evaluated MSC counts and various stress responses. G1: FR or FL - 190 mL, twice daily (30–60 min before breakfast and dinner); for 8 weeks. G1: ESC + PYC (34 individuals – 11♂ and 23♀ - 10 to 20 mg/day of ESC+ 50 mg/day of PYC) or ESC no additional supplementation (33 individuals – 9♂ and 24♀ - 10 to 20 mg/day of ESC), for 12 weeks. G1: Flavonoid-rich WBB, with 253 mg of anthocyanins + 30 g of freeze-dried WBB with 30 mL of low-flavonoid Rocks Orange Squash and 220 mL of water; G2: vitamin C (4 mg), sugars (8.90 g fructose, 7.99 g glucose), 30 mL Rocks Orange Squash and 220 mL water; Study 2 content identical to study 1, but with 170 ml of water. Não achamos o tempo do estudo. G1: food supplement with 200 mg of fermented soy (with 10 mg of equol + 80 mg of isoflavone aglycones) + 25 mg of resveratrol (1 tablet/day) G2: placebo; for 12 weeks. G1: ultra-low dose (12.5 mg/day) or low dose (25 mg/day) isoflavone aglycone tablets; G2: placebo; for 8 weeks G1: low dose (100 mg/day – 25 mg of GSPE - 33 women) or high dose (200 mg/day – 50 mg of GSPE - 32 women) – GSPE tablets; G2: Placebo – 0 mg of GSPE - 38 women In both groups, women were instructed to take 4 tablets per day at any time of the day; For 8 weeks. |
G1: depression rates decreased significantly in the quercetin group post-intervention [median (IQR): −1.00 (6.00); P = 0.04) but not compared with the placebo group. Orange flavonoid interventions significantly improved HAMD-17, BDI, and CES-D scores in patients with MDD. In addition to having probiotics potential in the treatment of depression. Intake of SQ significantly improved the response to psychological stress, irritability and depression in BJSQ compared to "Haruka". The health benefits of anthocyanins are established, especially in preventing diseases related to oxidative stress. After the intervention, the mean CES-D scores in the FR and FL groups decreased to <20 points; Flavonoids exhibit a neuroprotective effect by counteracting inflammatory reactions Treatment with ESC reduced the MADRS score and extra administration of PYC did not bring about changes. In both studies, an increase in PA was observed 2 h after consumption of the WBB drink rich in flavonoids, but it had no effect on NA. The effect of flavonoids on mood was consistent across both populations. Treatment significantly reduced the number of individuals affected by depressive symptoms assessed by HAM-D. These significant improvements occurred at week 12 and were observed in work and activities (-94.1%) (p<0.001). G1 low dose: A significant improvement in the HADS score was obtained; AIS; MSS somatic symptoms after 4 to 8 weeks of treatment; In the ultra-low dose and placebo groups, there was no significant change in HADS and AIS. In the HADS-depression subscale, the score was not significantly changed in any of the groups, whereas in the HADS-anxiety subscale, the score in the low and high dose groups improved after 4 weeks of treatment. Furthermore, the change in the anxiety subscale score was substantially greater in the high-dose group than in the placebo group. |
G1: headache, joint pain, tingling in extremities, abdominal discomfort. No significant AD. No significant AD. No significant AD? No significant AD. No significant AD.? The most common adverse events associated with the use of resveratrol is mild diarrhea. No significant AD. No significant AD. |
|
| [57] | Block randomized, triple-blind, placebo-controlled clinical trial / Iran (multicenter). | 50 patients with MS and Depression - 12% (♂) and 88% (♀); 18-55 y. | G1: 180 mg of ellagic acid - 90mg/2x day; G2: Placebo /12 weeks. |
Ellagic acid significantly reduced serum levels of IFN-γ, NO, and cortisol. It significantly increased serum levels of serotonin and BDNF and promoted a favorable effect in reducing BDI-II and EDSS scores. | No significant AD. | |
| [50] |
Randomized, simple blind, controlled/ South Korea. |
40 young ♂ and ♀ with MDD; 18 to 29 y. |
G1: FR or FL; Participants consumed FR or FL three times a day (30–60 minutes before breakfast, lunch, and dinner; 190 mL per bottle); for 8 weeks. | Orange flavonoid interventions significantly improved HAMD-17, BDI, and CES-D scores in patients with MDD. In addition to having probiotics potential in the treatment of depression. | No significant AD. |
|
| [58] |
Randomized, double- blind, placebo-controlled / Japan. |
15 individuals – 4 (♂) and 11 (♀); 50–70 y. |
G1: Potatoes – SQ (contains anthocyanins 45 mg; G2: Potatoes – Haruka. Subjects ate potatoes (75 g) cooked - microwaved for 2 min once a day / for 8 weeks | Intake of SQ significantly improved the response to psychological stress, irritability, and depression in BJSQ compared to "Haruka". Anthocyanins can help preventing diseases related to oxidative stress. | No significant AD. |
|
| [59] | Randomized, controlled, exploratory study, clinical trial / United Kingdom. |
38 mothers who had babies under 12 months (baby age ranged from 5 to 48 weeks). | G1: 21 mothers (consumption of an average of 15.45 items with a high flavonoid content); G2: changes in their diet/ for 2 weeks. | Mothers who ate a high level of flavonoids had significantly lower state anxiety after the intervention. The quality of perceived physical health, perceived psychological health, and the quality of social relationships were significantly higher after the intervention | No significant AD. | |
| [60] |
Randomized, single-blinded, placebo-controlled, crossover, parallel clinical trial / Spain. | 63 healthy young, middle-aged adults with overweight; 19♂) 44♀; 18-33 y. | G1: 2 groups, namely: 25g of SRP, and 32 g/day of PB; G2: 32g/day of CB /for 6 months or 7 months in some cases (pandemic). | The SRP groups; PB and CB showed a significant decrease in depression, with the P-value: (p= 0.007, p= 0.026 and p= 0.032, respectively). | n=5 in the SRP group: digestive symptoms; 3 who consumed PB or CB: softening of stool and reduced constipation. | |
| [61] | Multi-center, randomized, Open-Label with 4 parallel groups Intervention / France, Italy, Germany. | 125 participants (67 ♀, 70.4 y). | Participants of treated group received a diet rich in antioxidants (vitamin E, C, carotenoid, polyphenols), | In 2-month there was a reduction of depressive symptoms according to Center for Epidemiologic Studies Depression Scale in the four arms | No serious AE. | |
| [62] | Randomized, controlled, parallel-group, single-blinded trial, /United Kingdom | 99 mildly hypertensive participants; 40–65 y | Patients were enrolled in a 4-week low polyphenol diet washout period and then randomized to an low polyphenol diet or an high polyphenol diet / 8 weeks. | High Polyphenol Diest group showed reduction in depressive symptoms (Beck Depression Inventory-II), and an amelioration of mental health component scores | Not reported. | |
| [51] |
Randomized, simple-blind, controlled / South Korea. |
40 individuals – 16 (♂) and 24 (♀) –20-30 y. |
G1: FR or FL - 190 mL, twice daily (30–60 min before breakfast and dinner); 8 weeks. | After the intervention, the mean CES-D scores in the FR and FL groups decreased to <20 points; Flavonoids exhibit a neuroprotective effect by counteracting inflammatory reactions. | No significant AD |
|
| [52] |
Randomized, parallel, and open/ Slovakia. | 67 individuals of both sexes with MDD -20 (♂) and 47 (♀) - 18-65 y. |
G1: ESC + PYC (34 individuals – 11♂ and 23♀ - 10 to 20 mg/day of ESC+ 50 mg/day of PYC) or ESC no additional supplementation (33 individuals – 9♂ and 24♀ - 10 to 20 mg/day of ESC), for 12 weeks. | Treatment with ESC reduced the MADRS score, and extra administration of PYC did not bring about changes. |
No significant AD. |
|
| [63] | Randomized, multicenter, double-blind, placebo-controlled clinical trial / Thailand, Brazil, Bulgaria, and Australia. | 61 patients who had at least 1 episode of MDD (♂/♀); 18-63 y. | G1: curcumin 500 - 1500 mg/day orally; G2: placebo /for 1 week; then 1 dose each week and after 4 weeks (1500 mg of curcumin/placebo); 12 to 16 weeks. | No significant difference in blood parameters, heart rate, and PR and QRS intervals between G1 and G2 curcumin improved MADRS score. | G1: dizziness; nausea/vomiting; insomnia; diarrhea; G2: dizziness; nausea/vomiting; insomnia. | |
| [54] | Randomized, double- blind, placebo-controlled / Italy. | 60 (♂) recently menopausal; 50 - 55 y. |
G1: food supplement (200 mg of fermented soy/ 10 mg of equol + 80 mg of isoflavone aglycones) + 25 mg of resveratrol (1 tablet/day); G2: placebo; for 12 weeks. | Treatment significantly reduced the number of individuals affected by depressive symptoms assessed by HAM-D. These significant improvements occurred in week 12 and were observed in work and activities (-94.1%) (p<0.001). | The most common adverse event associated with the use of resveratrol is mild diarrhea. |
|
| [53] | Randomized, double-blind, placebo-controlled/ United Kingdom. |
Study 1 with 21 individuals – 2 (♂) and 19 (♀); 18 - 21 y; Study 2 with 52 children – 23 (♂) and 29 (♀); 7-10 y. |
G1: Flavonoid-rich WBB, with 253 mg of anthocyanins + 30 g of freeze-dried WBB with 30 mL of low-flavonoid Rocks Orange Squash (OS) and 220 mL of water; G2: vitamin C (4 mg), 30 mL Rocks OS, and 220 mL water; Study 2 content same as study 1, but with 170 ml of water. | In both studies, an increase in PA was observed 2 h after consumption of the WBB drink rich in flavonoids, but it had no effect on NA. The effect of flavonoids on mood was consistent across both populations. |
No significant AE |
|
| [55] |
Randomized, double-blind, placebo-controlled/ Japan. |
87 women who presented at least one symptom of menopause in MSS;40 - 60 y. |
G1: ultra-low dose (12.5 mg/day) or low dose (25 mg/day) isoflavone aglycone tablets or G2: placebo/ 8 weeks |
G1 low dose: A significant improvement in the HADS score was obtained; AIS; MSS somatic symptoms after 4 to 8 weeks of treatment. There was no significant change in HADS and AIS in the ultra-low dose and placebo groups. | No significant AE |
|
| [64] |
Randomized, double-blind, placebo-controlled, crossover, clinical trial / Iran and the United Kingdom. | 30 obese individuals - 83% (♀) and 17% (♂); mean age: 38.37 ± 11.51 y. | G1: curcumin, 1 g/day; G2: placebo/ 30 days; after that, inversion of the groups and perform the same intervention. |
G1: presented a significantly reduced mean BAI score; however, no significant impact on BDI scores. Therefore, curcumin has a potential anxiolytic effect on obese people. | No significant AE. |
|
| [56] | Randomized, double-blind, placebo-controlled/ Japan. | 91 women with at least one symptom of menopause; 40 – 60 years. | G1: low dose (100 mg/day – 25 mg of GSPE or high dose (200 mg/day – 50 mg of GSPE) – GSPE tablets; G2: Placebo – 0 mg of GSPE. In both groups, women were instructed to take 4 tablets per day at any time of the day for 8 weeks. | In the HADS-depression subscale, the score did not change significantly in any of the groups, whereas in the HADS-anxiety subscale, the score in the low and high-dose groups improved after 4 weeks. The change in the anxiety subscale score was substantially greater in the high-dose group than in the placebo group. | No significant AE. |
|
| [10] | Double-blind parallel trial / Australia | Participants: 39% ♂; 40–65 years | Participants consumed dark chocolate drink with 500 mg, 250 mg or 0 mg of polyphenols (placebo)/ once day / 30days. | The high dose polyphenols diet significantly increased self-rated calmness and contentedness compared to placebo. Mood scale and cognition was unchanged. | No AE | |
| [65] | Double blinded, randomised, clinical pilot crossover study/ United Kingdon |
10 participants | Comparison of a high polyphenol chocolate with iso-calorific chocolate (cocoa liquor free/low polyphenols). | The Hospital Anxiety and Depression score showed improvement after the consumption of olyphenol rich chocolate but deteriorated after isocaloric diet. | No AE | |
AE: Adverse events; AIS: Athens Insomnia Scale; BAI: Beck Anxiety Inventory; BDI: Beck Depression Inventory; BDI-II: Beck Depression Inventory-II; BDNF: Brain-derived neurotrophic fator; CB: control butter; CES-D: Center for Epidemiological Studies Depression Scale; EDSS: expanded disability status scales; ESC: Escitalopram; FL: low flavonoid orange cordial group; FR: group of orange juice rich in flavonoids; GSPE: grape seed proanthocyanidin extract; HADS: Hospital Anxiety and Depression Scale; HAMD/ HAMD -17: Hamilton Depression Rating Scale; IFN-γ: gamma interferon; IQR: range between quartiles; MADRS: Montgomery - Asberg Depression Rating Scale; MDD: major depressive disorder; MSC: mesenchymal stem cells; MSS: Menopause Symptom Scale; MS: multiple sclerosis; NO: nitric oxide; PA: Positive Affect; PB: peanut butter; PR: time interval between the beginning of atrial depolarization and the beginning of ventricular depolarization; PYC: Pycnogenol; QRS: depolarization of the ventricles, consisting of Q, R and S waves; SQ: Shadow Queen; SRP: roasted peanuts in shell; WBB: The wild blueberry drink; y: years.
3.2. Risk of Bias Assessment
All 19 included studies underwent systematic quality appraisal using the Cochrane Handbook for Systematic Reviews of Interventions as the guiding framework. Each trial was independently evaluated across multiple bias domains: random sequence generation, allocation concealment, blinding of participants and personnel, blinding of outcome assessment, completeness of outcome data, and risk of selective reporting. Most studies were found to have implemented adequate randomization procedures and maintained low attrition rates, enhancing internal validity. However, several trials, particularly open-label designs, lacked transparency in allocation concealment and participant blinding, introducing potential performance bias. In a minority of studies, outcome assessors were not blinded, raising the risk of detection bias. Despite these limitations, selective reporting was largely absent, and outcome data were generally reported comprehensively. Discrepancies in the quality ratings were resolved through consensus among reviewers. Overall, the collective evidence demonstrated moderate to high methodological quality, providing a solid foundation for interpreting the clinical relevance of phytocompound-based interventions in MDD.
Table 2.
Risk of Bias Assessment for Included Interventional Studies Evaluating Phytocompounds in Major Depressive Disorder (MDD). This table presents the methodological appraisal of the 19 clinical trials included in the synthesis, based on Cochrane risk of bias domains. Key dimensions assessed include randomization procedures, blinding of participants and personnel, allocation concealment, attrition rates, baseline demographic comparability, outcome measurement, and intention-to-treat (ITT) analysis. While most studies demonstrated adequate randomization and outcome reporting, variability was observed in blinding strategies and ITT implementation. This assessment informs the interpretive reliability and translational value of the synthesized findings on phytocompound efficacy in MDD.
Table 2.
Risk of Bias Assessment for Included Interventional Studies Evaluating Phytocompounds in Major Depressive Disorder (MDD). This table presents the methodological appraisal of the 19 clinical trials included in the synthesis, based on Cochrane risk of bias domains. Key dimensions assessed include randomization procedures, blinding of participants and personnel, allocation concealment, attrition rates, baseline demographic comparability, outcome measurement, and intention-to-treat (ITT) analysis. While most studies demonstrated adequate randomization and outcome reporting, variability was observed in blinding strategies and ITT implementation. This assessment informs the interpretive reliability and translational value of the synthesized findings on phytocompound efficacy in MDD.
| STUDY | QUESTION FOCUS | APPROPRIATE RANDOMIZATION | ALLOCATION BLINDING - | DOUBLE-BLIND | LOSSES (<20%) | PROGNOSTICS DEMOGRAPHIC CHARACTERISTICS | OUTCOMES | ITT |
| [48] | Yes | Yes | Yes | Yes | No | Yes | Yes | No |
| [49] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No |
| [57] | Yes | Yes | Triple-blinded | No | Yes | Yes | Yes | Yes |
| [50] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes |
| [58] | Yes | Yes | Ye | No | No | Yes | Yes | No |
| [59] | Yes | Yes | Yes | No | No | Yes | Yes | No? |
| [60] | Yes | Yes | No | No | No | Yes | Yes | No |
| [51] | Yes | Yes | No | No | No | Yes | Yes | Yes? |
| [62] | Yes | Yes | No | No | Yes | Yes | Yes | No |
| [61] | Yes | Yes | No | No | Yes | Yes | Yes | No |
| [52] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| [63] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | Yes |
| [54] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes |
| [53] | Yes | Yes | Yes | Yes | No | Yes | Yes | No |
| [55] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No |
| [64] | Yes | Yes | Yes | Yes | No | Yes | Yes | Yes |
| [56] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No |
| [10] | Yes | Yes | Yes | Yes | Yes | Yes | Yes | No |
| [65] | Yes | Yes | Yes | Yes | Yes | No | Yes | Yes |
ITT: Intention to treat analysis
3.3. Summary of Findings
The qualitative synthesis of the 19 interventional studies revealed consistent evidence supporting the therapeutic efficacy of phytocompounds in alleviating depressive symptoms. These compounds, administered as either monotherapy or adjunctive treatments, demonstrated clinically meaningful improvements across diverse MDD populations. Notable agents included curcumin, hypericin (from Hypericum perforatum), saffron extract, rosmarinic acid, and epigallocatechin gallate (EGCG). Across trials, statistically significant reductions in depression severity were observed using validated psychometric scales such as the Hamilton depression rating scale (HAM-D), Montgomery–Åsberg Depression Rating Scale (MADRS), and Beck Depression Inventory (BDI). The mechanistic actions of these compounds frequently involved enhancement of monoaminergic signaling, suppression of neuroinflammation via cytokine modulation, upregulation of brain-derived neurotrophic factor (BDNF), and attenuation of oxidative stress. While study heterogeneity in dosage, treatment duration, and formulation limits direct comparison, the collective findings support a biologically plausible and clinically relevant role for phytochemicals in MDD. These data justify further large-scale, placebo-controlled trials to optimize clinical application and assess long-term safety.
4. Synthesis
The 19 clinical trials synthesized in this review reveal a promising, though heterogeneous, body of evidence regarding the therapeutic potential of phytocompounds in MDD. These trials examined a wide range of phytochemicals, including curcumin, quercetin, polyphenols, anthocyanins, isoflavones, proanthocyanidins, and flavonoid-rich extracts, often administered in monotherapy or adjunctive formats. Although sample sizes, duration, and design quality varied, most studies used validated depression scales and biochemical endpoints, supporting a neurobiological rationale for clinical translation.
In a well-structured randomized controlled trial, Soltani et al. [25] evaluated the impact of nanocurcumin supplementation in individuals with coronary slow flow phenomenon (CSFP). The intervention led to improvements in depressive symptoms, physical and psychological health-related quality of life, and cardiometabolic parameters, with biochemical assays confirming anti-inflammatory and antioxidant effects [48]. Conversely, the double-blind, placebo-controlled study by Jalili et al. (2020) examining quercetin failed to find significant antidepressant effects. Moreover, the intervention group reported notable adverse effects—abdominal discomfort, paresthesia, and headaches—raising concerns about tolerability in psychiatric populations [49].
Methodological strengths such as stratified randomization and biomarker analysis were evident in the study by Hajiluian et al. [34], which demonstrated reduced depressive symptoms in individuals with Multiple Sclerosis following polyphenol-rich interventions. However, its narrow population limits generalizability to broader MDD cohorts [57]. In a similarly well-structured clinical trial, Choi et al. [27] examined the effects of flavonoid-enriched orange juice in healthy adults. Improvements in depressive symptoms were paralleled by increased serum BDNF and reduced zonulin levels, indicating neuromodulatory and gut-brain axis effects. Despite robust biochemical correlates, the sample size of 40 reduced statistical power [27].
Maeda-Yamamoto et al. [35] assessed the impact of anthocyanin-rich Solanum tuberosum L. on stress and mesenchymal stem cell proliferation. Although qualitative outcomes were positive, the trial was limited by its very small sample (n=15) and short duration (8 weeks), which precluded long-term conclusions. Similarly, Barfoot et al. [36] conducted a randomized study during the COVID-19 pandemic, which introduced significant confounding related to global psychological stress. While randomization via software strengthened validity, high dropout rates impaired data reliability.
Parilli-Moser et al. [37] explored the effects of botanical cognitive enhancers on depressive symptoms. Although standardized cognitive assessments were used, low group sizes and a lack of blinding limited interpretive strength, and COVID-19-related disruptions likely impacted outcome validit. In contrast, the RISTOMED study by Bourdel-Marchasson et al. [38] assessed a dietary protocol rich in antioxidants and polyphenols. After 2 months, reductions in depressive symptoms were observed, but these were found to be independent of inflammatory biomarker changes, suggesting mechanisms beyond systemic inflammation.
Kontogianni et al. [62] investigated high versus low polyphenol diets in the PPhIT trial, noting improved psychological wellbeing in the high-polyphenol group using standardized lifestyle and mood assessments. Park, Choi, and Lee [62] similarly conducted a placebo-controlled flavonoid study using orange juice and observed improvements in depression alongside increased serum serotonin, BDNF, and reduced CRP—though the small sample again limits external validity.
Smetanka et al. [62] focused on the potential for Pycnogenol to mitigate selective serotonin reuptake inhibitor (SSRI)-induced sexual dysfunction in patients taking escitalopram. However, the open-label design and simultaneous pharmacologic interventions created confounding that weakens causal inference. In the curcumin trial by Kanchanatawan et al. [40],methodological strengths included matched placebo capsules and double-blinding, although prior treatments continued during the trial, potentially masking true curcumin effects.
The study by Esmaily et al. [41] observed only marginal reductions in anxiety and depressive symptoms in response to saffron extract, with effects limited to a single outcome measure—suggesting potential underpowering or scale insensitivity. In a postmenopausal population, Terauchi et al. [33] demonstrated that grape seed proanthocyanidins reduced depressive symptoms in a dose-dependent manner, using validated questionnaires. However, the short duration (8 weeks) and modest sample size limit generalizability.
Equol and resveratrol were evaluated in a longitudinal 12-week study on menopausal women aged 50–55, where supplementation improved mood as assessed by the HAM-D [54]. Hirose et al. [55] explored low-dose isoflavone aglycone for postmenopausal symptoms, including depression and anxiety, using HADS and AIS. Despite positive outcomes, lack of adverse event documentation and small sample size limit clinical confidence.
Cognitive-affective benefits of blueberry-derived flavonoids were tested in a crossover design by Khalid et al. [55], involving both children and young adults. Stratified analysis revealed reductions in depressogenic cognitive patterns two hours post-consumption, supporting the acute neuromodulatory potential of these compounds.
Lastly, Sathyapalan et al. [55] evaluated chocolate rich in cocoa liquor and polyphenols versus low-polyphenol control chocolate in patients with chronic fatigue syndrome. Participants in the high-cocoa group reported improvements in depressive and fatigue symptoms, supporting flavonoid efficacy in neuropsychological syndromes. Pase et al. [10] reported mood-enhancing effects of cocoa polyphenols but no cognitive improvements after 30 days of supplementation.
Overall, the 19 studies reviewed underscore the emerging promise of phytocompounds as adjunctive or standalone interventions for MDD. While most trials reported clinically meaningful reductions in depressive symptoms, variability in methodological rigor, sample size, and treatment duration limited the generalizability of these findings. Notably, studies incorporating double-blind, placebo-controlled designs and objective biomarkers (e.g., inflammatory mediators, neurotrophic factors) provided stronger evidence for neuromodulatory and neuroprotective mechanisms. Nevertheless, several investigations reported inconclusive or modest effects, indicating the necessity of improved trial designs and larger, more diverse samples. Given the heterogeneous nature of depression, a multi-targeted approach—such as that offered by phytochemicals—holds particular relevance. Future research efforts should focus on optimizing dosage regimens, exploring synergistic effects with standard antidepressants, and elucidating long-term safety profiles to solidify phytocompounds’ place in evidence-based psychiatric care.
5. Discussion
The findings of this systematic review illuminate the multifaceted nature of MDD and the potential utility of phytocompounds in its management. Recent evidence reveals that MDD involves not only monoaminergic dysregulation but also neuroinflammatory processes, oxidative stress, and mitochondrial dysfunction, implicating diverse pathophysiological pathways [66]. By evaluating interventional studies centered on phytochemicals—including polyphenols, flavonoids, and alkaloids—this review highlights their potential neuroprotective, anti-inflammatory, and antioxidant properties [21]. These effects align with emerging translational research suggesting that multi-targeted strategies may offer enhanced therapeutic outcomes in complex mood disorders [67,68]. Nevertheless, the heterogeneity of study designs, phytocompound formulations, and patient populations underscores the need for more robust trials with standardized protocols [69,70,71]. This discussion aims to synthesize the mechanistic underpinnings and clinical implications of phytocompound use in MDD, situating these findings within broader neuropsychiatric research and outlining key directions for future investigation.
Neuroinflammation, driven by heightened immune responses in the CNS, is intricately linked to depression through elevated production of pro-inflammatory cytokines and activation of microglia in key brain regions such as the prefrontal cortex, anterior cingulate cortex, and insula [72,73,74,75,76,77]. Approximately 30% of individuals with MDD exhibit marked CNS inflammation, correlating with more severe and treatment-resistant symptoms [78,79]. Inflammation has been identified as a central factor in MDD pathogenesis, with mechanisms involving elevated levels of the nucleotide-binding oligomerization domain, leucine rich repeat and pyrin domain containing (NLRP) 3 inflammasome, which stimulates pro-inflammatory cytokines (interleukin (IL)-1β, IL-18) implicated in depressive symptoms [80,81,82]. These inflammatory cascades appear in chronic infections, neurodegenerative disorders (e.g., multiple sclerosis), and perinatal depression, further underscoring their pervasive role [68,83,84,85,86,87,88]. Research indicates that both immune dysregulation and metabolic disturbances—encompassing neuroendocrine dysfunction, dysbiosis, and mitochondrial abnormalities—can exacerbate depression [89,90,91,92]. Notably, phytochemical interventions, including polyphenols, may confer neuroprotective effects by suppressing pro-inflammatory mediators and neuronal apoptosis, thus offering a compelling adjunctive avenue for managing MDD [83,84].
Oxidative stress arises when reactive oxygen species (ROS) and other free radicals overwhelm the body’s antioxidant defenses, causing cellular damage through protein, lipid, and nucleic acid injury [93,94]. In depressed individuals, lower concentrations of antioxidants such as zinc, vitamin E, and coenzyme Q10 compound this vulnerability, promoting neurodegeneration and aggravating pathophysiological processes in MDD [95,96]. Tryptophan metabolism contributes further to oxidative stress, as its depletion can intensify free-radical formation and neurotoxic metabolite production, correlating with depressive severity [18,97,98]. Mitochondrial dysfunction—including altered morphology and impaired energy balance—amplifies ROS generation, triggering neuroinflammation and cognitive deficits [99,100,101,102], while an accumulation of damaged mitochondria fuels neuronal injury [103,104]. Obesity-related inflammation also exacerbates oxidative stress by producing adipokines (IL-6, IL-1, tumor necrosis factor-alpha) and disrupting insulin regulation, potentially leading to type 2 diabetes and depression [105,106,107]. Lifestyle factors, such as high-fat diets and sedentary behavior, can aggravate ROS production via mitochondrial β-oxidation and nuclear factor kappa B (NF-κB) pathways, underscoring the importance of dietary antioxidants and physical exercise in mitigating MDD risk [108,109,110,111,112].
Mitochondria serve not only as cellular powerhouses but also as central regulators of neuroinflammatory processes, rendering them critical to both the onset and progression of MDD [92]. In MDD, mitochondrial abnormalities—such as structural damage, deoxyribonucleic acid (DNA) disruptions, and respiratory chain dysfunction—elevate ROS production, disrupting neurotransmitter balance and worsening depressive symptoms [100,113,114,115]. While psychosocial factors contribute to MDD, biochemical markers like methylmalonic acid (MMA) further implicate mitochondrial dysfunction [116]. Elevated MMA interferes with succinate dehydrogenase, enhancing ROS formation and neuronal injury, compounded by deficiencies in vitamin B12 and folate [117,118,119,120]. Recent studies highlight potential therapeutic avenues, including mitochondrial transplantation—replacing damaged mitochondria or introducing mtDNA and related proteins—to restore function. Additionally, inhibiting the renin-angiotensin system via angiotensin receptor blockers may attenuate neuroinflammation and oxidative stress, mitigating depressive pathology [121,122]. Ultimately, targeting mitochondrial health through phytochemicals and other multimodal strategies could significantly advance MDD management by reducing oxidative damage and bolstering neuronal resilience [99].
Food intake is a continuous part of daily life, yet psychological factors can significantly shape dietary patterns, thereby influencing obesity risk and depressive symptoms [123,124,125]. Evidence suggests that inadequate consumption of essential nutrients—such as vitamin B12, zinc, magnesium, folic acid, and vitamin B6—heightens susceptibility to MDD [14]. Unhealthy dietary choices, often dominated by high-fat convenience foods, correlate with lower intakes of fruits, vegetables, lean proteins, and whole grains, ultimately fostering systemic inflammation and oxidative stress that exacerbate depressive pathology [126,127,128]. Obesity is likewise implicated, as elevated adiposity undermines mental health by increasing pro-inflammatory markers and metabolic dysregulation [85,86]. Beyond poor nutritional profiles, behaviors such as smoking, sedentarism, and insufficient sleep are commonly observed among individuals with severe depression, compounding their vulnerability [129,130]. Conversely, emerging research indicates that adopting healthier diets, coupled with lifestyle modifications like regular physical activity and stress management, may mitigate both depressive symptomatology and comorbid metabolic disorders, thereby improving overall wellbeing [125,131,132].
Pharmacological and non-pharmacological therapies for MDD are increasingly delivered through multidisciplinary care teams, involving psychiatrists, psychologists, and other specialists [133,134]. Among pharmacological options, SSRIs frequently serve as first-line agents, whereas TCAs, serotonin–norepinephrine reuptake inhibitors (SNRIs), and other drug classes—such as monoamine oxidase inhibitors (MAOIs) and N-methyl-D-aspartate (NMDA) antagonists—offer alternative pathways [9,135,136,137]. Despite established efficacy, these medications can elicit adverse effects, including gastrointestinal disturbances (nausea, dyspepsia), hepatic toxicity, sleep disruptions driven by 5-HT2 receptor activation, and cardiovascular changes such as QTc prolongation or orthostatic hypotension [138,139,140,141,142]. Furthermore, hyponatremia poses an additional concern, particularly in older adults and those on diuretics [143,144]. Such limitations of standard antidepressants have prompted research into safer, more tolerable interventions. In this context, herbal medicines are emerging as promising adjunctive or complementary treatments, potentially minimizing side effects and improving patient adherence, thus contributing to a more holistic approach to MDD management [145,146,147].
Phytochemicals, naturally derived from plants, have gained considerable attention for their capacity to modulate neurobiological pathways implicated in MDD [36,148]. Among these, polyphenols, notable for crossing the blood-brain barrier, display neuroprotective, antioxidant, and anti-inflammatory properties, attenuating cytokine activity and neuronal apoptosis [84,149]. Within this class, flavonoids such as luteolin effectively neutralize free radicals and mitigate inflammation [149,150,151], whereas carotenoids also confer antidepressant benefits via similar mechanisms [152,153,154,155]. These actions align with evidence that upregulating BDNF can enhance synaptic resilience, as demonstrated by curcumin and resveratrol, which bolster BDNF in animal models [156,157,158]. Additional phytochemicals found in Panax ginseng, Mitragyna speciosa, Astragalus membraneceus, and Acorus genus plants similarly reduce depressive behaviors through anti-inflammatory and antioxidant pathways [31,33,159,160,161]. Although these interventions present fewer side effects than conventional antidepressants, further research is essential to optimize dosage, elucidate mechanisms, and confirm safety profiles [162,163]. The emerging evidence underscores the value of phytotherapies as promising, integrative approaches to addressing MDD’s multifactorial etiology [164]. Collectively, these findings reinforce the importance of clinical exploration of phytotherapeutics for the management of mood disorders [165]. Figure 3 shows some phytochemicals and their effects in brain metabolism and function.
This review aims to situate the current findings within the broader context of psychiatric research, specifically addressing the study’s primary objective of assessing how phytocompounds might influence MDD outcomes. By evaluating multiple clinical trials of phytochemicals (e.g., curcumin, flavonoids, anthocyanins), our review highlights evidence of neuromodulatory, anti-inflammatory, and antioxidant benefits that align with the multifactorial pathophysiology of MDD. These observations not only build upon prior studies suggesting phytocompounds’ capacity to target oxidative stress and neuroinflammation but also offer novel insights into their potential for synergistic use alongside standard antidepressants [166]. The theoretical implications of these findings underscore the importance of broad-spectrum therapeutic strategies for MDD, challenging the traditional monoamine-centric paradigm and prompting a more integrative view of depression biology [167]. Practically, adopting phytocompounds could address current treatment limitations—such as adverse effects and partial response rates—while enhancing patient adherence due to their favorable safety profiles [168]. Nonetheless, key challenges remain, including the heterogeneity of formulations, variable methodologies, and small sample sizes [169]. Robust, large-scale, randomized controlled trials featuring standardized phytochemical preparations and validated biomarkers would strengthen evidence quality [170]. Finally, this data have significant clinical relevance, as safer, more accessible adjunctive treatments could broaden therapeutic options, reduce polypharmacy, and ultimately improve functional outcomes for individuals with MDD.
6. Conclusions
This systematic review highlights the promising yet heterogeneous landscape of phytocompounds in managing MDD. By synthesizing 19 interventional studies involving a variety of phytochemicals—such as curcumin, flavonoids, and anthocyanins—this review underscores their potential neuroprotective, anti-inflammatory, and antioxidant roles, which appear crucial given the multifactorial pathophysiology of MDD. Notably, the ability of these compounds to target inflammation, oxidative stress, and mitochondrial dysfunction expands on the traditional monoamine-focused paradigm, offering a broader therapeutic scope. While several trials reported significant symptom improvement and few adverse events, methodological limitations—particularly small sample sizes, varying treatment regimens, and inconsistent outcome measures—restrain definitive conclusions. Future studies should prioritize standardized compound formulations, larger cohorts, and robust mechanistic endpoints to bolster evidence on long-term safety and synergistic efficacy with conventional antidepressants. Overall, these findings illuminate the value of phytocompounds as integrative adjuvants for MDD, bridging novel mechanistic insights with tangible clinical applications, and emphasizing the need for continued exploration and innovation in this evolving research domain.
Author Contributions
Conceptualization, S.M.B., M.T., and L.F.L.; methodology, A.C.F.G.; investigation, F.F.F., V.E.V., L.P.A., C.R.P.D., and F.C.C., and L.F.L.; writing—original draft preparation, S.M.B., L.F.L., L.P.A., and M.T.; writing—review and editing, S.M.B., F.F.F., V.E.L., C.M.G., E.S.B.M.P., and R.S.A.H.; visualization, S.M.B., M.T., and F.F.F.; supervision, S.M.B. and M.T.; project administration, S.M.B.; funding acquisition, S.M.B. and M.T. All authors agreed to the final version of this manuscript.
Funding
This work was supported by the HUN-REN Hungarian Research Network to M.T.
Acknowledgments
Images were built with biorender, fripik.com, canva, and pixabay.com
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BDNF | brain-derived neurotrophic factor |
| CNS | central nervous system |
| DNA | deoxyribonucleic acid |
| HAM-D | Hamilton depression rating scale |
| IL | Interleukin |
| MMA | methylmalonic acid |
| MDD | major depressive disorder |
| ROS | reactive oxygen species |
| SSRI | selective serotonin reuptake inhibitor |
| TCA | tricyclic antidepressant |
References
- Manosso, L.M.; Arent, C.O.; Borba, L.A.; Abelaira, H.M.; Réus, G.Z. Natural Phytochemicals for the Treatment of Major Depressive Disorder: A Mini-Review of Pre- and Clinical Studies. CNS Neurol Disord Drug Targets 2023, 22, 237–254. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Suzuki, K.; Kavalali, E.T.; Monteggia, L.M. Ketamine: Mechanisms and Relevance to Treatment of Depression. Annu Rev Med 2024, 75, 129–143. [Google Scholar] [CrossRef]
- Schoeller, F.; Jain, A.; Adrien, V.; Maes, P.; Reggente, N. Aesthetic chills mitigate maladaptive cognition in depression. BMC Psychiatry 2024, 24, 40. [Google Scholar] [CrossRef] [PubMed]
- Averina, O.V.; Poluektova, E.U.; Zorkina, Y.A.; Kovtun, A.S.; Danilenko, V.N. Human Gut Microbiota for Diagnosis and Treatment of Depression. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef]
- Bagby, S.P.; Martin, D.; Chung, S.T.; Rajapakse, N. From the outside in: biological mechanisms linking social and environmental exposures to chronic disease and to health disparities. American journal of public health 2019, 109, S56–S63. [Google Scholar] [CrossRef] [PubMed]
- Fusar-Poli, P.; Tantardini, M.; De Simone, S.; Ramella-Cravaro, V.; Oliver, D.; Kingdon, J.; Kotlicka-Antczak, M.; Valmaggia, L.; Lee, J.; Millan, M. Deconstructing vulnerability for psychosis: meta-analysis of environmental risk factors for psychosis in subjects at ultra high-risk. European Psychiatry 2017, 40, 65–75. [Google Scholar] [CrossRef]
- Lesch, K.-P. When the serotonin transporter gene meets adversity: the contribution of animal models to understanding epigenetic mechanisms in affective disorders and resilience. Molecular and functional models in neuropsychiatry 2011, 251–280. [Google Scholar]
- Simons, R.L.; Lei, M.K.; Stewart, E.A.; Beach, S.R.; Brody, G.H.; Philibert, R.A.; Gibbons, F.X. Social adversity, genetic variation, street code, and aggression: A genetically informed model of violent behavior. Youth violence and juvenile justice 2012, 10, 3–24. [Google Scholar] [CrossRef]
- Cui, L.; Li, S.; Wang, S.; Wu, X.; Liu, Y.; Yu, W.; Wang, Y.; Tang, Y.; Xia, M.; Li, B. Major depressive disorder: hypothesis, mechanism, prevention and treatment. Signal Transduct Target Ther 2024, 9, 30. [Google Scholar] [CrossRef]
- Pase, M.P.; Scholey, A.B.; Pipingas, A.; Kras, M.; Nolidin, K.; Gibbs, A.; Wesnes, K.; Stough, C. Cocoa polyphenols enhance positive mood states but not cognitive performance: a randomized, placebo-controlled trial. Journal of psychopharmacology (Oxford, England) 2013, 27, 451–458. [Google Scholar] [CrossRef]
- Jia, S.; Hou, Y.; Wang, D.; Zhao, X. Flavonoids for depression and anxiety: a systematic review and meta-analysis. Critical reviews in food science and nutrition 2023, 63, 8839–8849. [Google Scholar] [CrossRef]
- Tang, M.; Liu, T.; Jiang, P.; Dang, R. The interaction between autophagy and neuroinflammation in major depressive disorder: from pathophysiology to therapeutic implications. Pharmacological research 2021, 168, 105586. [Google Scholar] [CrossRef]
- Bertollo, A.G.; Mingoti, M.E.D.; Ignácio, Z.M. Neurobiological mechanisms in the kynurenine pathway and major depressive disorder. Reviews in the Neurosciences 2025, 36, 169–187. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Cai, X.; Ma, Y.; Yang, Y.; Pan, C.W.; Zhu, X.; Ke, C. Metabolomics on depression: A comparison of clinical and animal research. J Affect Disord 2024, 349, 559–568. [Google Scholar] [CrossRef] [PubMed]
- Barbalho, S.M.; Leme Boaro, B.; da Silva Camarinha Oliveira, J.; Patočka, J.; Barbalho Lamas, C.; Tanaka, M.; Laurindo, L.F. Molecular Mechanisms Underlying Neuroinflammation Intervention with Medicinal Plants: A Critical and Narrative Review of the Current Literature. Pharmaceuticals (Basel) 2025, 18. [Google Scholar] [CrossRef]
- de Lima, E.P.; Laurindo, L.F.; Catharin, V.C.S.; Direito, R.; Tanaka, M.; Jasmin Santos German, I.; Lamas, C.B.; Guiguer, E.L.; Araújo, A.C.; Fiorini, A.M.R.; et al. Polyphenols, Alkaloids, and Terpenoids Against Neurodegeneration: Evaluating the Neuroprotective Effects of Phytocompounds Through a Comprehensive Review of the Current Evidence. Metabolites 2025, 15. [Google Scholar] [CrossRef]
- de Lima, E.P.; Tanaka, M.; Lamas, C.B.; Quesada, K.; Detregiachi, C.R.P.; Araújo, A.C.; Guiguer, E.L.; Catharin, V.; de Castro, M.V.M.; Junior, E.B.; et al. Vascular Impairment, Muscle Atrophy, and Cognitive Decline: Critical Age-Related Conditions. Biomedicines 2024, 12. [Google Scholar] [CrossRef] [PubMed]
- Pearson, K.; Beier, K.; Mardis, T.; Munoz, B.; Zaidi, A. The Neurochemistry of Depression: The Good, The Bad and The Ugly. Mo Med 2024, 121, 68–75. [Google Scholar]
- Ullah, R.; Khan, M.; Shah, S.A.; Saeed, K.; Kim, M.O. Natural antioxidant anthocyanins—A hidden therapeutic candidate in metabolic disorders with major focus in neurodegeneration. Nutrients 2019, 11, 1195. [Google Scholar] [CrossRef]
- Jin, W.; Xu, X.; Chen, X.; Qi, W.; Lu, J.; Yan, X.; Zhao, D.; Cong, D.; Li, X.; Sun, L. Protective effect of pig brain polypeptides against corticosterone-induced oxidative stress, inflammatory response, and apoptosis in PC12 cells. Biomedicine & Pharmacotherapy 2019, 115, 108890. [Google Scholar]
- Wang, J.; Song, Y.; Chen, Z.; Leng, S.X. Connection between systemic inflammation and neuroinflammation underlies neuroprotective mechanism of several phytochemicals in neurodegenerative diseases. Oxidative medicine and cellular longevity 2018, 2018, 1972714. [Google Scholar] [CrossRef]
- Battaglia, S.; Avenanti, A.; Vécsei, L.; Tanaka, M. Neural correlates and molecular mechanisms of memory and learning. 2024, 25, 2724.
- Yoder, R.; Michaud, A.; Feagans, A.; Hinton-Froese, K.E.; Meyer, A.; Powers, V.A.; Stalnaker, L.; Hord, M.K. Family-Based Treatment for Anxiety, Depression, and ADHD for a Parent and Child. Int J Environ Res Public Health 2024, 21. [Google Scholar] [CrossRef]
- Moreira, J.; Machado, M.; Dias-Teixeira, M.; Ferraz, R.; Delerue-Matos, C.; Grosso, C. The neuroprotective effect of traditional Chinese medicinal plants—A critical review. Acta Pharmaceutica Sinica B 2023, 13, 3208–3237. [Google Scholar] [CrossRef] [PubMed]
- Ajao, A.A.-n.; Sabiu, S.; Balogun, F.O.; Adekomi, D.A.; Saheed, S.A. The Ambit of Phytotherapy in Psychotic Care. In Psychosis-Biopsychosocial and Relational Perspectives; IntechOpen: 2018.
- Rajpal, V.R.; Koul, H.K.; Raina, S.N.; Kumar, H.M.S.; Qazi, G.N. Phytochemicals for Human Health: The Emerging Trends and Prospects. Curr Top Med Chem 2024, 24, v–vi. [Google Scholar] [CrossRef]
- Kumar, H.M.S.; Rajpal, V.R.; Koul, H.K.; Raina, S.N.; Qazi, G.N. Phytochemicals for Human Health: The Emerging Trends and Prospects, Part-3. Curr Top Med Chem 2024, 24, 1011–1012. [Google Scholar] [CrossRef]
- Xiao, J.; Bai, W. Bioactive phytochemicals. Critical reviews in food science and nutrition 2019, 59, 827–829. [Google Scholar] [CrossRef] [PubMed]
- Fais, A.; Era, B. Phytochemical Composition and Biological Activity. Plants (Basel) 2024, 13. [Google Scholar] [CrossRef] [PubMed]
- Muscolo, A.; Mariateresa, O.; Giulio, T.; Mariateresa, R. Oxidative Stress: The Role of Antioxidant Phytochemicals in the Prevention and Treatment of Diseases. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef]
- Zhao, Y.; Li, J.; Cao, G.; Zhao, D.; Li, G.; Zhang, H.; Yan, M. Ethnic, Botanic, Phytochemistry and Pharmacology of the. Molecules 2023, 28. [Google Scholar] [CrossRef]
- Reddy, K.; Stafford, G.I.; Makunga, N.P. Skeletons in the closet? Using a bibliometric lens to visualise phytochemical and pharmacological activities linked to. Front Plant Sci 2024, 15, 1268101. [Google Scholar] [CrossRef]
- Gong, G.; Ganesan, K.; Wang, Y.; Zhang, Z.; Liu, Y.; Wang, J.; Yang, F.; Zheng, Y. Ononin ameliorates depression-like behaviors by regulating BDNF-TrkB-CREB signaling in vitro and in vivo. J Ethnopharmacol 2024, 320, 117375. [Google Scholar] [CrossRef]
- Tanaka, M.; Vécsei, L. From Lab to Life: Exploring Cutting-Edge Models for Neurological and Psychiatric Disorders. Biomedicines 2024, 12, 613. [Google Scholar] [CrossRef] [PubMed]
- Seung, H.-B.; Kwon, H.-J.; Kwon, C.-Y.; Kim, S.-H. Neuroendocrine Biomarkers of Herbal Medicine for Major Depressive Disorder: A Systematic Review and Meta-Analysis. Pharmaceuticals 2023, 16, 1176. [Google Scholar] [CrossRef] [PubMed]
- Jaberi, K.R.; Alamdari-Palangi, V.; Savardashtaki, A.; Vatankhah, P.; Jamialahmadi, T.; Tajbakhsh, A.; Sahebkar, A. Modulatory Effects of Phytochemicals on Gut-Brain Axis: Therapeutic Implication. Curr Dev Nutr 2024, 8, 103785. [Google Scholar] [CrossRef] [PubMed]
- Liloia, D.; Zamfira, D.A.; Tanaka, M.; Manuello, J.; Crocetta, A.; Keller, R.; Cozzolino, M.; Duca, S.; Cauda, F.; Costa, T. Disentangling the role of gray matter volume and concentration in autism spectrum disorder: A meta-analytic investigation of 25 years of voxel-based morphometry research. Neuroscience & Biobehavioral Reviews 2024, 105791. [Google Scholar]
- Davis, C.C.; Choisy, P. Medicinal plants meet modern biodiversity science. Curr Biol 2024, 34, R158–R173. [Google Scholar] [CrossRef]
- Kakarla, R.; Karuturi, P.; Siakabinga, Q.; Kasi Viswanath, M.; Dumala, N.; Guntupalli, C.; Nalluri, B.N.; Venkateswarlu, K.; Prasanna, V.S.; Gutti, G.; et al. Current understanding and future directions of cruciferous vegetables and their phytochemicals to combat neurological diseases. Phytother Res 2024, 38, 1381–1399. [Google Scholar] [CrossRef]
- Chandel, P.; Thapa, K.; Kanojia, N.; Rani, L.; Singh, T.G.; Rohilla, P. Exploring Therapeutic Potential of Phytoconstituents as a Gut Microbiota Modulator in the Management of Neurological and Psychological Disorders. Neuroscience 2024, 551, 69–78. [Google Scholar] [CrossRef]
- Tanaka, M. From Serendipity to Precision: Integrating AI, Multi-Omics, and Human-Specific Models for Personalized Neuropsychiatric Care. Biomedicines 2025, 13, 167. [Google Scholar] [CrossRef]
- Tanaka, M. Beyond the boundaries: Transitioning from categorical to dimensional paradigms in mental health diagnostics. Advances in Clinical and Experimental Medicine 2024, 33, 1295–1301. [Google Scholar] [CrossRef]
- Cordeiro, M.L.d.S.; Martins, V.G.d.Q.A.; Silva, A.P.d.; Rocha, H.A.O.; Rachetti, V.d.P.S.; Scortecci, K.C. Phenolic acids as antidepressant agents. Nutrients 2022, 14, 4309. [Google Scholar] [CrossRef]
- Fazilat, S.; Tahmasbi, F.; Mirzaei, M.R.; Sanaie, S.; Yousefi, Z.; Asnaashari, S.; Yaqoubi, S.; Mohammadi, A.B.; Araj-khodaei, M. A systematic review on the use of phytotherapy in managing clinical depression. BioImpacts 2024, 15, 30532–30532. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ (Clinical research ed.) 2021, 372, n71. [Google Scholar] [CrossRef]
- Moher, D.J.A.I.M. Liberat i A, Tetzlaff J, et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. 2009, 151, 264–269. [Google Scholar]
- Cumpston, M.; Li, T.; Page, M.J.; Chandler, J.; Welch, V.A.; Higgins, J.P.; Thomas, J.J.T.C.d.o.s.r. Updated guidance for trusted systematic reviews: a new edition of the Cochrane Handbook for Systematic Reviews of Interventions. 2019, 2019.
- Soltani, M.; Hosseinzadeh-Attar, M.J.; Rezaei, M.; Alipoor, E.; Vasheghani-Farahani, A.; Yaseri, M.; Rezayat, S.M. Effect of nano-curcumin supplementation on cardiometabolic risk factors, physical and psychological quality of life, and depression in patients with coronary slow flow phenomenon: a randomized double-blind clinical trial. Trials 2024, 25, 515. [Google Scholar] [CrossRef] [PubMed]
- Dehghani, F.; Vafa, M.; Ebrahimkhani, A.; Găman, M.A.; Sezavar Seyedi Jandaghi, S.H. Effects of quercetin supplementation on endothelial dysfunction biomarkers and depression in post-myocardial infarction patients: A double-blind, placebo-controlled, randomized clinical trial. Clin Nutr ESPEN 2023, 56, 73–80. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.; Kim, J.H.; Park, M.; Lee, H.J. Effects of Flavonoid-Rich Orange Juice Intervention on Major Depressive Disorder in Young Adults: A Randomized Controlled Trial. Nutrients 2022, 15. [Google Scholar] [CrossRef]
- Park, M.; Choi, J.; Lee, H.J. Flavonoid-Rich Orange Juice Intake and Altered Gut Microbiome in Young Adults with Depressive Symptom: A Randomized Controlled Study. Nutrients 2020, 12. [Google Scholar] [CrossRef]
- Smetanka, A.; Stara, V.; Farsky, I.; Tonhajzerova, I.; Ondrejka, I. Pycnogenol supplementation as an adjunct treatment for antidepressant-induced sexual dysfunction. Physiol Int 2019, 106, 59–69. [Google Scholar] [CrossRef]
- Khalid, S.; Barfoot, K.L.; May, G.; Lamport, D.J.; Reynolds, S.A.; Williams, C.M. Effects of Acute Blueberry Flavonoids on Mood in Children and Young Adults. Nutrients 2017, 9. [Google Scholar] [CrossRef]
- Davinelli, S.; Scapagnini, G.; Marzatico, F.; Nobile, V.; Ferrara, N.; Corbi, G. Influence of equol and resveratrol supplementation on health-related quality of life in menopausal women: A randomized, placebo-controlled study. Maturitas 2017, 96, 77–83. [Google Scholar] [CrossRef] [PubMed]
- Hirose, A.; Terauchi, M.; Akiyoshi, M.; Owa, Y.; Kato, K.; Kubota, T. Low-dose isoflavone aglycone alleviates psychological symptoms of menopause in Japanese women: a randomized, double-blind, placebo-controlled study. Arch Gynecol Obstet 2016, 293, 609–615. [Google Scholar] [CrossRef] [PubMed]
- Terauchi, M.; Horiguchi, N.; Kajiyama, A.; Akiyoshi, M.; Owa, Y.; Kato, K.; Kubota, T. Effects of grape seed proanthocyanidin extract on menopausal symptoms, body composition, and cardiovascular parameters in middle-aged women: a randomized, double-blind, placebo-controlled pilot study. Menopause 2014, 21, 990–996. [Google Scholar] [CrossRef] [PubMed]
- Hajiluian, G.; Karegar, S.J.; Shidfar, F.; Aryaeian, N.; Salehi, M.; Lotfi, T.; Farhangnia, P.; Heshmati, J.; Delbandi, A.A. The effects of Ellagic acid supplementation on neurotrophic, inflammation, and oxidative stress factors, and indoleamine 2, 3-dioxygenase gene expression in multiple sclerosis patients with mild to moderate depressive symptoms: A randomized, triple-blind, placebo-controlled trial. Phytomedicine 2023, 121, 155094. [Google Scholar] [CrossRef]
- Maeda-Yamamoto, M.; Honmou, O.; Sasaki, M.; Haseda, A.; Kagami-Katsuyama, H.; Shoji, T.; Namioka, A.; Namioka, T.; Magota, H.; Oka, S.; et al. The Impact of Purple-Flesh Potato (Nutrients 2022, 14. [CrossRef]
- Barfoot, K.L.; Forster, R.; Lamport, D.J. Mental Health in New Mothers: A Randomised Controlled Study into the Effects of Dietary Flavonoids on Mood and Perceived Quality of Life. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Parilli-Moser, I.; Domínguez-López, I.; Trius-Soler, M.; Castellví, M.; Bosch, B.; Castro-Barquero, S.; Estruch, R.; Hurtado-Barroso, S.; Lamuela-Raventós, R.M. Consumption of peanut products improves memory and stress response in healthy adults from the ARISTOTLE study: A 6-month randomized controlled trial. Clinical nutrition (Edinburgh, Scotland) 2021, 40, 5556–5567. [Google Scholar] [CrossRef]
- Bourdel-Marchasson, I.; Ostan, R.; Regueme, S.C.; Pinto, A.; Pryen, F.; Charrouf, Z.; d'Alessio, P.; Baudron, C.R.; Guerville, F.; Durrieu, J.; et al. Quality of Life: Psychological Symptoms-Effects of a 2-Month Healthy Diet and Nutraceutical Intervention; A Randomized, Open-Label Intervention Trial (RISTOMED). Nutrients 2020, 12. [Google Scholar] [CrossRef]
- Kontogianni, M.D.; Vijayakumar, A.; Rooney, C.; Noad, R.L.; Appleton, K.M.; McCarthy, D.; Donnelly, M.; Young, I.S.; McKinley, M.C.; McKeown, P.P.; et al. A High Polyphenol Diet Improves Psychological Well-Being: The Polyphenol Intervention Trial (PPhIT). Nutrients 2020, 12. [Google Scholar] [CrossRef]
- Kanchanatawan, B.; Tangwongchai, S.; Sughondhabhirom, A.; Suppapitiporn, S.; Hemrunrojn, S.; Carvalho, A.F.; Maes, M. Add-on Treatment with Curcumin Has Antidepressive Effects in Thai Patients with Major Depression: Results of a Randomized Double-Blind Placebo-Controlled Study. Neurotox Res 2018, 33, 621–633. [Google Scholar] [CrossRef]
- Esmaily, H.; Sahebkar, A.; Iranshahi, M.; Ganjali, S.; Mohammadi, A.; Ferns, G.; Ghayour-Mobarhan, M. An investigation of the effects of curcumin on anxiety and depression in obese individuals: A randomized controlled trial. Chin J Integr Med 2015, 21, 332–338. [Google Scholar] [CrossRef]
- Sathyapalan, T.; Beckett, S.; Rigby, A.S.; Mellor, D.D.; Atkin, S.L. High cocoa polyphenol rich chocolate may reduce the burden of the symptoms in chronic fatigue syndrome. Nutrition journal 2010, 9, 55. [Google Scholar] [CrossRef]
- Singh, N.; Garg, M.; Prajapati, P.; Singh, P.K.; Chopra, R.; Kumari, A.; Mittal, A. Adaptogenic property of Asparagus racemosus: Future trends and prospects. Heliyon 2023, 9. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, M.; Szabó, Á.; Vécsei, L.; Giménez-Llort, L. Emerging translational research in neurological and psychiatric diseases: from in vitro to in vivo models. 2023, 24, 15739.
- Tanaka, M.; Vécsei, L. A decade of dedication: pioneering perspectives on neurological diseases and mental illnesses. 2024, 12, 1083.
- Kessler, R.C.; van Loo, H.M.; Wardenaar, K.J.; Bossarte, R.M.; Brenner, L.; Ebert, D.; De Jonge, P.; Nierenberg, A.; Rosellini, A.; Sampson, N. Using patient self-reports to study heterogeneity of treatment effects in major depressive disorder. Epidemiology and psychiatric sciences 2017, 26, 22–36. [Google Scholar] [CrossRef] [PubMed]
- Malgaroli, M.; Calderon, A.; Bonanno, G.A. Networks of major depressive disorder: A systematic review. Clinical Psychology Review 2021, 85, 102000. [Google Scholar] [CrossRef] [PubMed]
- Mew, E.J.; Monsour, A.; Saeed, L.; Santos, L.; Patel, S.; Courtney, D.B.; Watson, P.N.; Szatmari, P.; Offringa, M.; Monga, S. Systematic scoping review identifies heterogeneity in outcomes measured in adolescent depression clinical trials. Journal of Clinical Epidemiology 2020, 126, 71–79. [Google Scholar] [CrossRef]
- Wu, A.; Zhang, J. Neuroinflammation, memory, and depression: new approaches to hippocampal neurogenesis. J Neuroinflammation 2023, 20, 283. [Google Scholar] [CrossRef]
- Jurcau, A.; Simion, A. Neuroinflammation in Cerebral Ischemia and Ischemia/Reperfusion Injuries: From Pathophysiology to Therapeutic Strategies. Int J Mol Sci 2021, 23. [Google Scholar] [CrossRef]
- Fornari Laurindo, L.; Aparecido Dias, J.; Cressoni Araújo, A.; Torres Pomini, K.; Machado Galhardi, C.; Rucco Penteado Detregiachi, C.; Santos de Argollo Haber, L.; Donizeti Roque, D.; Dib Bechara, M.; Vialogo Marques de Castro, M.; et al. Immunological dimensions of neuroinflammation and microglial activation: exploring innovative immunomodulatory approaches to mitigate neuroinflammatory progression. Front Immunol 2023, 14, 1305933. [Google Scholar] [CrossRef]
- Laurindo, L.F.; Barbalho, S.M.; Araújo, A.C.; Guiguer, E.L.; Mondal, A.; Bachtel, G.; Bishayee, A. Açaí (Euterpe oleracea Mart.) in Health and Disease: A Critical Review. Nutrients 2023, 15. [Google Scholar] [CrossRef]
- Laurindo, L.F.; Simili, O.A.G.; Araújo, A.C.; Guiguer, E.L.; Direito, R.; Valenti, V.E.; de Oliveira, V.; de Oliveira, J.S.; Yanaguizawa Junior, J.L.; Dias, J.A.; et al. Melatonin from Plants: Going Beyond Traditional Central Nervous System Targeting-A Comprehensive Review of Its Unusual Health Benefits. Biology (Basel) 2025, 14. [Google Scholar] [CrossRef]
- Tanaka, M.; Tuka, B.; Vécsei, L. Navigating the Neurobiology of Migraine: From pathways to potential therapies. 2024, 13, 1098.
- Zanella, I. Neuroinflammation: From Molecular Basis to Therapy. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef] [PubMed]
- Hassamal, S. Chronic stress, neuroinflammation, and depression: an overview of pathophysiological mechanisms and emerging anti-inflammatories. Front Psychiatry 2023, 14, 1130989. [Google Scholar] [CrossRef]
- Poletti, S.; Mazza, M.G.; Benedetti, F. Inflammatory mediators in major depression and bipolar disorder. Transl Psychiatry 2024, 14, 247. [Google Scholar] [CrossRef]
- Xia, C.Y.; Guo, Y.X.; Lian, W.W.; Yan, Y.; Ma, B.Z.; Cheng, Y.C.; Xu, J.K.; He, J.; Zhang, W.K. The NLRP3 inflammasome in depression: Potential mechanisms and therapies. Pharmacol Res 2023, 187, 106625. [Google Scholar] [CrossRef] [PubMed]
- Han, Q.; Li, W.; Chen, P.; Wang, L.; Bao, X.; Huang, R.; Liu, G.; Chen, X. Microglial NLRP3 inflammasome-mediated neuroinflammation and therapeutic strategies in depression. Neural Regen Res 2024, 19, 1890–1898. [Google Scholar] [CrossRef]
- Wakasugi, D.; Kondo, S.; Ferdousi, F.; Mizuno, S.; Yada, A.; Tominaga, K.; Takahashi, S.; Isoda, H. A rare olive compound oleacein functions as a TrkB agonist and mitigates neuroinflammation both in vitro and in vivo. Cell Commun Signal 2024, 22, 309. [Google Scholar] [CrossRef]
- Guo, Y.; Yang, Y. Progress of plant polyphenol extracts in treating depression by anti-neuroinflammatory mechanism: A review. Medicine (Baltimore) 2024, 103, e37151. [Google Scholar] [CrossRef] [PubMed]
- Bruno, A.; Dolcetti, E.; Rizzo, F.R.; Fresegna, D.; Musella, A.; Gentile, A.; De Vito, F.; Caioli, S.; Guadalupi, L.; Bullitta, S.; et al. Corrigendum: Inflammation-Associated Synaptic Alterations as Shared Threads in Depression and Multiple Sclerosis. Front Cell Neurosci 2020, 14, 647259. [Google Scholar] [CrossRef]
- Sha, Q.; Escobar Galvis, M.L.; Madaj, Z.B.; Keaton, S.A.; Smart, L.; Edgerly, Y.M.; Anis, E.; Leach, R.; Osborne, L.M.; Achtyes, E.; et al. Dysregulated placental expression of kynurenine pathway enzymes is associated with inflammation and depression in pregnancy. Brain Behav Immun 2024, 119, 146–153. [Google Scholar] [CrossRef]
- Achtyes, E.; Keaton, S.A.; Smart, L.; Burmeister, A.R.; Heilman, P.L.; Krzyzanowski, S.; Nagalla, M.; Guillemin, G.J.; Escobar Galvis, M.L.; Lim, C.K.; et al. Inflammation and kynurenine pathway dysregulation in post-partum women with severe and suicidal depression. Brain Behav Immun 2020, 83, 239–247. [Google Scholar] [CrossRef]
- Tanaka, M.; Vécsei, L. Revolutionizing our understanding of Parkinson’s disease: Dr. Heinz Reichmann’s pioneering research and future research direction. Journal of Neural Transmission 2024, 1-21.
- Pontillo, G.; Cepas, M.B.; Broeders, T.A.A.; Koubiyr, I.; Schoonheim, M.M. Network Analysis in Multiple Sclerosis and Related Disorders. Neuroimaging Clin N Am 2024, 34, 375–384. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.; Liu, Z.; Wang, J.; Gao, M.; Zhang, Y.; Yang, C.; Zhang, A.; Li, G.; Li, X.; Liu, S.; et al. Immunoregulatory role of the gut microbiota in inflammatory depression. Nat Commun 2024, 15, 3003. [Google Scholar] [CrossRef]
- Molina Galindo, L.S.; Gonzalez-Escamilla, G.; Fleischer, V.; Grotegerd, D.; Meinert, S.; Ciolac, D.; Person, M.; Stein, F.; Brosch, K.; Nenadić, I.; et al. Concurrent inflammation-related brain reorganization in multiple sclerosis and depression. Brain Behav Immun 2024, 119, 978–988. [Google Scholar] [CrossRef] [PubMed]
- Qin, P.; Sun, Y.; Li, L. Mitochondrial dysfunction in chronic neuroinflammatory diseases (Review). Int J Mol Med 2024, 53. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, T.; You, F. Oxidative Stress and Bio-Regulation. Int J Mol Sci 2024, 25. [Google Scholar] [CrossRef]
- Bhatt, S.; Nagappa, A.N.; Patil, C.R. Role of oxidative stress in depression. Drug Discov Today 2020, 25, 1270–1276. [Google Scholar] [CrossRef]
- Li, K.; Deng, Z.; Lei, C.; Ding, X.; Li, J.; Wang, C. The Role of Oxidative Stress in Tumorigenesis and Progression. Cells 2024, 13. [Google Scholar] [CrossRef]
- Correia, A.S.; Cardoso, A.; Vale, N. Oxidative Stress in Depression: The Link with the Stress Response, Neuroinflammation, Serotonin, Neurogenesis and Synaptic Plasticity. Antioxidants (Basel) 2023, 12. [Google Scholar] [CrossRef]
- Ilavská, L.; Morvová, M.; Paduchová, Z.; Muchová, J.; Garaiova, I.; Ďuračková, Z.; Šikurová, L.; Trebatická, J. The kynurenine and serotonin pathway, neopterin and biopterin in depressed children and adolescents: an impact of omega-3 fatty acids, and association with markers related to depressive disorder. A randomized, blinded, prospective study. Front Psychiatry 2024, 15, 1347178. [Google Scholar] [CrossRef]
- Szabó, Á.; Galla, Z.; Spekker, E.; Szűcs, M.; Martos, D.; Takeda, K.; Ozaki, K.; Inoue, H.; Yamamoto, S.; Toldi, J. Oxidative and Excitatory Neurotoxic Stresses in CRISPR/Cas9-Induced Kynurenine Aminotransferase Knock-out Mice: A Novel Model for Experience-Based Depression and Post-Traumatic Stress Disorder. 2024.
- Larrea, A.; Sánchez-Sánchez, L.; Diez-Martin, E.; Elexpe, A.; Torrecilla, M.; Astigarraga, E.; Barreda-Gómez, G. Mitochondrial Metabolism in Major Depressive Disorder: From Early Diagnosis to Emerging Treatment Options. J Clin Med 2024, 13. [Google Scholar] [CrossRef]
- Chen, H.; Lu, M.; Lyu, Q.; Shi, L.; Zhou, C.; Li, M.; Feng, S.; Liang, X.; Zhou, X.; Ren, L. Mitochondrial dynamics dysfunction: Unraveling the hidden link to depression. Biomed Pharmacother 2024, 175, 116656. [Google Scholar] [CrossRef] [PubMed]
- Martos, D.; Lőrinczi, B.; Szatmári, I.; Vécsei, L.; Tanaka, M. The impact of C-3 side chain modifications on Kynurenic Acid: a behavioral analysis of its analogs in the Motor Domain. International journal of molecular sciences 2024, 25, 3394. [Google Scholar] [CrossRef] [PubMed]
- Battaglia, S.; Avenanti, A.; Vécsei, L.; Tanaka, M. Neurodegeneration in cognitive impairment and mood disorders for experimental, clinical and translational neuropsychiatry. 2024, 12, 574.
- Cao, Y.; Chen, H.; Tan, Y.; Yu, X.D.; Xiao, C.; Li, Y.; Reilly, J.; He, Z.; Shu, X. Protection of p-Coumaric acid against chronic stress-induced neurobehavioral deficits in mice via activating the PKA-CREB-BDNF pathway. Physiol Behav 2024, 273, 114415. [Google Scholar] [CrossRef]
- Song, Y.; Cao, H.; Zuo, C.; Gu, Z.; Huang, Y.; Miao, J.; Fu, Y.; Guo, Y.; Jiang, Y.; Wang, F. Mitochondrial dysfunction: A fatal blow in depression. Biomed Pharmacother 2023, 167, 115652. [Google Scholar] [CrossRef] [PubMed]
- Masenga, S.K.; Kabwe, L.S.; Chakulya, M.; Kirabo, A. Mechanisms of Oxidative Stress in Metabolic Syndrome. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Li, H.; Ren, J.; Li, Y.; Wu, Q.; Wei, J. Oxidative stress: The nexus of obesity and cognitive dysfunction in diabetes. Front Endocrinol (Lausanne) 2023, 14, 1134025. [Google Scholar] [CrossRef]
- Ramírez-Garza, S.L.; Laveriano-Santos, E.P.; Moreno, J.J.; Bodega, P.; de Cos-Gandoy, A.; de Miguel, M.; Santos-Beneit, G.; Fernández-Alvira, J.M.; Fernández-Jiménez, R.; Martínez-Gómez, J.; et al. Metabolic syndrome, adiposity, diet, and emotional eating are associated with oxidative stress in adolescents. Front Nutr 2023, 10, 1216445. [Google Scholar] [CrossRef]
- Li, H.; Song, L.; Cen, M.; Fu, X.; Gao, X.; Zuo, Q.; Wu, J. Oxidative balance scores and depressive symptoms: Mediating effects of oxidative stress and inflammatory factors. J Affect Disord 2023, 334, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Tan, B.L.; Norhaizan, M.E. Effect of High-Fat Diets on Oxidative Stress, Cellular Inflammatory Response and Cognitive Function. Nutrients 2019, 11. [Google Scholar] [CrossRef]
- Nunes, Y.C.; Mendes, N.M.; Pereira de Lima, E.; Chehadi, A.C.; Lamas, C.B.; Haber, J.F.S.; Dos Santos Bueno, M.; Araújo, A.C.; Catharin, V.C.S.; Detregiachi, C.R.P.; et al. Curcumin: A Golden Approach to Healthy Aging: A Systematic Review of the Evidence. Nutrients 2024, 16. [Google Scholar] [CrossRef]
- Pagotto, G.L.O.; Santos, L.; Osman, N.; Lamas, C.B.; Laurindo, L.F.; Pomini, K.T.; Guissoni, L.M.; Lima, E.P.; Goulart, R.A.; Catharin, V.; et al. Ginkgo biloba: A Leaf of Hope in the Fight against Alzheimer's Dementia: Clinical Trial Systematic Review. Antioxidants (Basel) 2024, 13. [Google Scholar] [CrossRef] [PubMed]
- Takeda, L.N.; Omine, A.; Laurindo, L.F.; Araújo, A.C.; Machado, N.M.; Dias, J.A.; Kavalakatt, J.; Banerjee, S.; de Alvares Goulart, R.; Atanasov, A.G.; et al. Brazil nut (Bertholletia excelsa Bonpl.) in health and disease: A narrative review. Food Chem 2025, 477, 143425. [Google Scholar] [CrossRef]
- Li, W.; Zhu, L.; Chen, Y.; Zhuo, Y.; Wan, S.; Guo, R. Association between mitochondrial DNA levels and depression: a systematic review and meta-analysis. BMC Psychiatry 2023, 23, 866. [Google Scholar] [CrossRef] [PubMed]
- Jiang, M.; Wang, L.; Sheng, H. Mitochondria in depression: The dysfunction of mitochondrial energy metabolism and quality control systems. CNS Neurosci Ther 2024, 30, e14576. [Google Scholar] [CrossRef] [PubMed]
- Valotto Neto, L.J.; Reverete de Araujo, M.; Moretti Junior, R.C.; Mendes Machado, N.; Joshi, R.K.; Dos Santos Buglio, D.; Barbalho Lamas, C.; Direito, R.; Fornari Laurindo, L.; Tanaka, M.; et al. Investigating the Neuroprotective and Cognitive-Enhancing Effects of Bacopa monnieri: A Systematic Review Focused on Inflammation, Oxidative Stress, Mitochondrial Dysfunction, and Apoptosis. Antioxidants (Basel) 2024, 13. [Google Scholar] [CrossRef]
- Scaini, G.; Mason, B.L.; Diaz, A.P.; Jha, M.K.; Soares, J.C.; Trivedi, M.H.; Quevedo, J. Dysregulation of mitochondrial dynamics, mitophagy and apoptosis in major depressive disorder: Does inflammation play a role? Molecular psychiatry 2022, 27, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Zhan, F.; Lin, G.; Su, L.; Xue, L.; Duan, K.; Chen, L.; Ni, J. The association between methylmalonic acid, a biomarker of mitochondrial dysfunction, and cause-specific mortality in Alzheimer's disease and Parkinson's disease. Heliyon 2024, 10, e29357. [Google Scholar] [CrossRef]
- Guo, J.; Wang, S.; Wan, X.; Liu, X.; Wang, Z.; Liang, C.; Zhang, Z.; Wang, Y.; Yan, M.; Wu, P.; et al. Mitochondria-derived methylmalonic acid aggravates ischemia-reperfusion injury by activating reactive oxygen species-dependent ferroptosis. Cell Commun Signal 2024, 22, 53. [Google Scholar] [CrossRef]
- Cao, B.; Xiao, Y.; Liu, D. Associations of methylmalonic acid and depressive symptoms with mortality: a population-based study. Transl Psychiatry 2024, 14, 297. [Google Scholar] [CrossRef]
- Huang, Q.N.; Watanabe, F.; Koseki, K.; He, R.E.; Lee, H.L.; Chiu, T.H.T. Effect of roasted purple laver (nori) on vitamin B(12) nutritional status of vegetarians: a dose-response trial. European journal of nutrition 2024, 63, 3269–3279. [Google Scholar] [CrossRef]
- Zong, Y.; Li, H.; Liao, P.; Chen, L.; Pan, Y.; Zheng, Y.; Zhang, C.; Liu, D.; Zheng, M.; Gao, J. Mitochondrial dysfunction: mechanisms and advances in therapy. Signal Transduct Target Ther 2024, 9, 124. [Google Scholar] [CrossRef]
- Ali, N.H.; Al-Kuraishy, H.M.; Al-Gareeb, A.I.; Albuhadily, A.K.; Hamad, R.S.; Alexiou, A.; Papadakis, M.; Saad, H.M.; Batiha, G.E. Role of brain renin-angiotensin system in depression: A new perspective. CNS Neurosci Ther 2024, 30, e14525. [Google Scholar] [CrossRef]
- Muha, J.; Schumacher, A.; Campisi, S.C.; Korczak, D.J. Depression and emotional eating in children and adolescents: A systematic review and meta-analysis. Appetite 2024, 200, 107511. [Google Scholar] [CrossRef] [PubMed]
- Ekinci, G.N.; Sanlier, N. The relationship between nutrition and depression in the life process: A mini-review. Exp Gerontol 2023, 172, 112072. [Google Scholar] [CrossRef] [PubMed]
- Chrzastek, Z.; Guligowska, A.; Sobczuk, P.; Kostka, T. Dietary factors, risk of developing depression, and severity of its symptoms in older adults-A narrative review of current knowledge. Nutrition 2023, 106, 111892. [Google Scholar] [CrossRef]
- Lane, M.M.; Gamage, E.; Travica, N.; Dissanayaka, T.; Ashtree, D.N.; Gauci, S.; Lotfaliany, M.; O'Neil, A.; Jacka, F.N.; Marx, W. Ultra-Processed Food Consumption and Mental Health: A Systematic Review and Meta-Analysis of Observational Studies. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Ejtahed, H.S.; Mardi, P.; Hejrani, B.; Mahdavi, F.S.; Ghoreshi, B.; Gohari, K.; Heidari-Beni, M.; Qorbani, M. Association between junk food consumption and mental health problems in adults: a systematic review and meta-analysis. BMC Psychiatry 2024, 24, 438. [Google Scholar] [CrossRef] [PubMed]
- Malmir, H.; Mahdavi, F.S.; Ejtahed, H.S.; Kazemian, E.; Chaharrahi, A.; Mohammadian Khonsari, N.; Mahdavi-Gorabi, A.; Qorbani, M. Junk food consumption and psychological distress in children and adolescents: a systematic review and meta-analysis. Nutr Neurosci 2023, 26, 807–827. [Google Scholar] [CrossRef]
- Selvaraj, R.; Selvamani, T.Y.; Zahra, A.; Malla, J.; Dhanoa, R.K.; Venugopal, S.; Shoukrie, S.I.; Hamouda, R.K.; Hamid, P. Association Between Dietary Habits and Depression: A Systematic Review. Cureus 2022, 14, e32359. [Google Scholar] [CrossRef]
- Gorbachev, D.; Markina, E.; Chigareva, O.; Gradinar, A.; Borisova, N.; Syunyakov, T. Dietary Patterns as Modifiable Risk Factors for Depression: a Narrative Review. Psychiatr Danub 2023, 35, 423–431. [Google Scholar]
- Magzal, F.; Turroni, S.; Fabbrini, M.; Barone, M.; Vitman Schorr, A.; Ofran, A.; Tamir, S. A personalized diet intervention improves depression symptoms and changes microbiota and metabolite profiles among community-dwelling older adults. Front Nutr 2023, 10, 1234549. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Zhou, W.; Zhu, X.; Hu, Z.; Li, S.; Zheng, B.; Xu, H.; Long, W.; Xiong, X. Association between dietary intake and symptoms of depression and anxiety in pregnant women: Evidence from a community-based observational study. Food Sci Nutr 2023, 11, 7555–7564. [Google Scholar] [CrossRef]
- Qaseem, A.; Owens, D.K.; Etxeandia-Ikobaltzeta, I.; Tufte, J.E.; Cross, J.T.; Wilt, T.J.; Physicians, C.G.C.f.t.A.C.o. Nonpharmacologic and Pharmacologic Treatments of Adults in the Acute Phase of Major Depressive Disorder: A Living Clinical Guideline From the American College of Physicians (Version 1, Update Alert 2). Ann Intern Med 2024. [Google Scholar] [CrossRef]
- Direito, R.; Barbalho, S.M.; Sepodes, B.; Figueira, M.E. Plant-Derived Bioactive Compounds: Exploring Neuroprotective, Metabolic, and Hepatoprotective Effects for Health Promotion and Disease Prevention. Pharmaceutics 2024, 16. [Google Scholar] [CrossRef] [PubMed]
- Bayes, A.; Parker, G. How to choose an antidepressant medication. Acta Psychiatr Scand 2019, 139, 280–291. [Google Scholar] [CrossRef]
- Gillman, P.K. Tricyclic antidepressant pharmacology and therapeutic drug interactions updated. Br J Pharmacol 2007, 151, 737–748. [Google Scholar] [CrossRef]
- Arakawa, R.; Stenkrona, P.; Takano, A.; Svensson, J.; Andersson, M.; Nag, S.; Asami, Y.; Hirano, Y.; Halldin, C.; Lundberg, J. Venlafaxine ER Blocks the Norepinephrine Transporter in the Brain of Patients with Major Depressive Disorder: a PET Study Using [18F]FMeNER-D2. Int J Neuropsychopharmacol 2019, 22, 278–285. [Google Scholar] [CrossRef] [PubMed]
- Carvalho, A.F.; Sharma, M.S.; Brunoni, A.R.; Vieta, E.; Fava, G.A. The Safety, Tolerability and Risks Associated with the Use of Newer Generation Antidepressant Drugs: A Critical Review of the Literature. Psychother Psychosom 2016, 85, 270–288. [Google Scholar] [CrossRef]
- Kishi, T.; Ikuta, T.; Sakuma, K.; Okuya, M.; Hatano, M.; Matsuda, Y.; Iwata, N. Antidepressants for the treatment of adults with major depressive disorder in the maintenance phase: a systematic review and network meta-analysis. Mol Psychiatry 2023, 28, 402–409. [Google Scholar] [CrossRef]
- Wichniak, A.; Wierzbicka, A.; Walęcka, M.; Jernajczyk, W. Effects of Antidepressants on Sleep. Curr Psychiatry Rep 2017, 19, 63. [Google Scholar] [CrossRef]
- Zhou, S.; Li, P.; Lv, X.; Lai, X.; Liu, Z.; Zhou, J.; Liu, F.; Tao, Y.; Zhang, M.; Yu, X.; et al. Adverse effects of 21 antidepressants on sleep during acute-phase treatment in major depressive disorder: a systemic review and dose-effect network meta-analysis. Sleep 2023, 46. [Google Scholar] [CrossRef] [PubMed]
- Beach, S.R.; Kostis, W.J.; Celano, C.M.; Januzzi, J.L.; Ruskin, J.N.; Noseworthy, P.A.; Huffman, J.C. Meta-analysis of selective serotonin reuptake inhibitor-associated QTc prolongation. J Clin Psychiatry 2014, 75, e441–449. [Google Scholar] [CrossRef] [PubMed]
- Gheysens, T.; Van Den Eede, F.; De Picker, L. The risk of antidepressant-induced hyponatremia: A meta-analysis of antidepressant classes and compounds. Eur Psychiatry 2024, 67, e20. [Google Scholar] [CrossRef]
- Wu, X.; Zhang, W. Reminiscence therapy-based care program alleviates anxiety and depression, as well as improves the quality of life in recurrent gastric cancer patients. Front Psychol 2023, 14, 1133470. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, C.; Fornai, M.; Antonioli, L.; Blandizzi, C.; Calderone, V. Phytochemicals as Novel Therapeutic Strategies for NLRP3 Inflammasome-Related Neurological, Metabolic, and Inflammatory Diseases. Int J Mol Sci 2019, 20. [Google Scholar] [CrossRef]
- Laurindo, L.F.; de Carvalho, G.M.; de Oliveira Zanuso, B.; Figueira, M.E.; Direito, R.; de Alvares Goulart, R.; Buglio, D.S.; Barbalho, S.M. Curcumin-Based Nanomedicines in the Treatment of Inflammatory and Immunomodulated Diseases: An Evidence-Based Comprehensive Review. Pharmaceutics 2023, 15. [Google Scholar] [CrossRef]
- Nishikito, D.F.; Borges, A.C.A.; Laurindo, L.F.; Otoboni, A.; Direito, R.; Goulart, R.A.; Nicolau, C.C.T.; Fiorini, A.M.R.; Sinatora, R.V.; Barbalho, S.M. Anti-Inflammatory, Antioxidant, and Other Health Effects of Dragon Fruit and Potential Delivery Systems for Its Bioactive Compounds. Pharmaceutics 2023, 15. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.; Iqbal, H.; Kim, S.M.; Jin, M. Phytochemicals That Act on Synaptic Plasticity as Potential Prophylaxis against Stress-Induced Depressive Disorder. Biomol Ther (Seoul) 2023, 31, 148–160. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Zhou, Y.; Xi, Y.; Zhou, H.; Tang, Z.; Xiong, L.; Qin, D. Polyphenols: Natural Food-Grade Biomolecules for the Treatment of Nervous System Diseases from a Multi-Target Perspective. Pharmaceuticals (Basel) 2024, 17. [Google Scholar] [CrossRef]
- Wang, T.; Yang, C.; Li, Z.; Li, T.; Zhang, R.; Zhao, Y.; Cheng, T.; Zong, Z.; Ma, Y.; Zhang, D.; et al. Flavonoid 4,4'-dimethoxychalcone selectively eliminates senescent cells via activating ferritinophagy. Redox Biol 2024, 69, 103017. [Google Scholar] [CrossRef]
- Zhu, M.; Sun, Y.; Su, Y.; Guan, W.; Wang, Y.; Han, J.; Wang, S.; Yang, B.; Wang, Q.; Kuang, H. Luteolin: A promising multifunctional natural flavonoid for human diseases. Phytother Res 2024, 38, 3417–3443. [Google Scholar] [CrossRef]
- Rasmus, P.; Kozłowska, E. Antioxidant and Anti-Inflammatory Effects of Carotenoids in Mood Disorders: An Overview. Antioxidants (Basel) 2023, 12. [Google Scholar] [CrossRef]
- Barbalho, S.M.; Direito, R.; Laurindo, L.F.; Marton, L.T.; Guiguer, E.L.; Goulart, R.A.; Tofano, R.J.; Carvalho, A.C.A.; Flato, U.A.P.; Capelluppi Tofano, V.A.; et al. Ginkgo biloba in the Aging Process: A Narrative Review. Antioxidants (Basel) 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Barbalho, S.M.; Laurindo, L.F.; de Oliveira Zanuso, B.; da Silva, R.M.S.; Gallerani Caglioni, L.; Nunes Junqueira de Moraes, V.B.F.; Fornari Laurindo, L.; Dogani Rodrigues, V.; da Silva Camarinha Oliveira, J.; Beluce, M.E.; et al. AdipoRon's Impact on Alzheimer's Disease-A Systematic Review and Meta-Analysis. Int J Mol Sci 2025, 26. [Google Scholar] [CrossRef] [PubMed]
- Buglio, D.S.; Marton, L.T.; Laurindo, L.F.; Guiguer, E.L.; Araújo, A.C.; Buchaim, R.L.; Goulart, R.A.; Rubira, C.J.; Barbalho, S.M. The Role of Resveratrol in Mild Cognitive Impairment and Alzheimer's Disease: A Systematic Review. J Med Food 2022, 25, 797–806. [Google Scholar] [CrossRef] [PubMed]
- Costa, R.O.; Martins, L.F.; Tahiri, E.; Duarte, C.B. Brain-derived neurotrophic factor-induced regulation of RNA metabolism in neuronal development and synaptic plasticity. Wiley Interdiscip Rev RNA 2022, 13, e1713. [Google Scholar] [CrossRef]
- Gadad, B.S.; Vargas-Medrano, J.; Ramos, E.I.; Najera, K.; Fagan, M.; Forero, A.; Thompson, P.M. Altered levels of interleukins and neurotrophic growth factors in mood disorders and suicidality: an analysis from periphery to central nervous system. Transl Psychiatry 2021, 11, 341. [Google Scholar] [CrossRef]
- Afzal, A.; Batool, Z.; Sadir, S.; Liaquat, L.; Shahzad, S.; Tabassum, S.; Ahmad, S.; Kamil, N.; Perveen, T.; Haider, S. Therapeutic Potential of Curcumin in Reversing the Depression and Associated Pseudodementia via Modulating Stress Hormone, Hippocampal Neurotransmitters, and BDNF Levels in Rats. Neurochem Res 2021, 46, 3273–3285. [Google Scholar] [CrossRef]
- Idayu, N.F.; Hidayat, M.T.; Moklas, M.A.; Sharida, F.; Raudzah, A.R.; Shamima, A.R.; Apryani, E. Antidepressant-like effect of mitragynine isolated from Mitragyna speciosa Korth in mice model of depression. Phytomedicine 2011, 18, 402–407. [Google Scholar] [CrossRef]
- Ahmad, I.; Prabowo, W.C.; Arifuddin, M.; Fadraersada, J.; Indriyanti, N.; Herman, H.; Purwoko, R.Y.; Nainu, F.; Rahmadi, A.; Paramita, S.; et al. Species as Pharmacological Agents: From Abuse to Promising Pharmaceutical Products. Life (Basel) 2022, 12. [Google Scholar] [CrossRef]
- Chen, L.; Fei, S.; Olatunji, O.J. LC/ESI/TOF-MS Characterization, Anxiolytic and Antidepressant-like Effects of. Molecules 2022, 27. [Google Scholar] [CrossRef] [PubMed]
- Fathinezhad, Z.; Sewell, R.D.E.; Lorigooini, Z.; Rafieian-Kopaei, M. Depression and Treatment with Effective Herbs. Curr Pharm Des 2019, 25, 738–745. [Google Scholar] [CrossRef] [PubMed]
- Lee, G.; Bae, H. Therapeutic Effects of Phytochemicals and Medicinal Herbs on Depression. Biomed Res Int 2017, 2017, 6596241. [Google Scholar] [CrossRef] [PubMed]
- Manosso, L.M.; Arent, C.O.; Borba, L.A.; Abelaira, H.M.; Réus, G.Z. Natural Phytochemicals for the Treatment of Major Depressive Disorder: A Mini-Review of Pre-and Clinical Studies. CNS & Neurological Disorders-Drug Targets-CNS & Neurological Disorders) 2023, 22, 237–254. [Google Scholar]
- Picheta, N.; Piekarz, J.; Daniłowska, K.; Mazur, K.; Piecewicz-Szczęsna, H.; Smoleń, A. Phytochemicals in the treatment of patients with depression: a systemic review. Frontiers in Psychiatry 2024, 15, 1509109. [Google Scholar] [CrossRef]
- Wang, J.; Behl, T.; Rana, T.; Sehgal, A.; Wal, P.; Saxena, B.; Yadav, S.; Mohan, S.; Anwer, M.K.; Chigurupati, S. Exploring the pathophysiological influence of heme oxygenase-1 on neuroinflammation and depression: A study of phytotherapeutic-based modulation. Phytomedicine 2024, 155466. [Google Scholar] [CrossRef]
- Mariani, N.; Everson, J.; Pariante, C.M.; Borsini, A. Modulation of microglial activation by antidepressants. Journal of psychopharmacology (Oxford, England) 2022, 36, 131–150. [Google Scholar] [CrossRef]
- Khan, A.; Siddiqui, S.; Husain, S.A.; Mazurek, S.; Iqbal, M.A. Phytocompounds Targeting Metabolic Reprogramming in Cancer: An Assessment of Role, Mechanisms, Pathways, and Therapeutic Relevance. J Agric Food Chem 2021. [Google Scholar] [CrossRef]
- Bozzuto, G.; Calcabrini, A.; Colone, M.; Condello, M.; Dupuis, M.L.; Pellegrini, E.; Stringaro, A. Phytocompounds and Nanoformulations for Anticancer Therapy: A Review. Molecules 2024, 29. [Google Scholar] [CrossRef]
- Majchrzak-Celińska, A.; Studzińska-Sroka, E. New Avenues and Major Achievements in Phytocompounds Research for Glioblastoma Therapy. Molecules 2024, 29. [Google Scholar] [CrossRef]
Figure 1.
Neurobiological contributors to the onset and progression of major depressive disorder (MDD). Multiple interacting systems—including genetic predisposition, chronic psychosocial stress, systemic comorbidities, and immune dysregulation—converge to disrupt neuroimmune homeostasis. Central to this pathophysiology are oxidative stress, liver dysfunction, intestinal dysbiosis, and neuroinflammation, driven by activated microglia and astrocytes. These cells increase reactive nitrogen and oxygen species (NO, ROS), impair mitochondrial function, and alter kynurenine (KYN) pathway dynamics, reducing kynurenic acid (KYNA) and promoting neurotoxicity. Dysregulated serotonin and gamma-aminobutyric acid (GABA) signaling, alongside diminished brain-derived.
Figure 1.
Neurobiological contributors to the onset and progression of major depressive disorder (MDD). Multiple interacting systems—including genetic predisposition, chronic psychosocial stress, systemic comorbidities, and immune dysregulation—converge to disrupt neuroimmune homeostasis. Central to this pathophysiology are oxidative stress, liver dysfunction, intestinal dysbiosis, and neuroinflammation, driven by activated microglia and astrocytes. These cells increase reactive nitrogen and oxygen species (NO, ROS), impair mitochondrial function, and alter kynurenine (KYN) pathway dynamics, reducing kynurenic acid (KYNA) and promoting neurotoxicity. Dysregulated serotonin and gamma-aminobutyric acid (GABA) signaling, alongside diminished brain-derived.
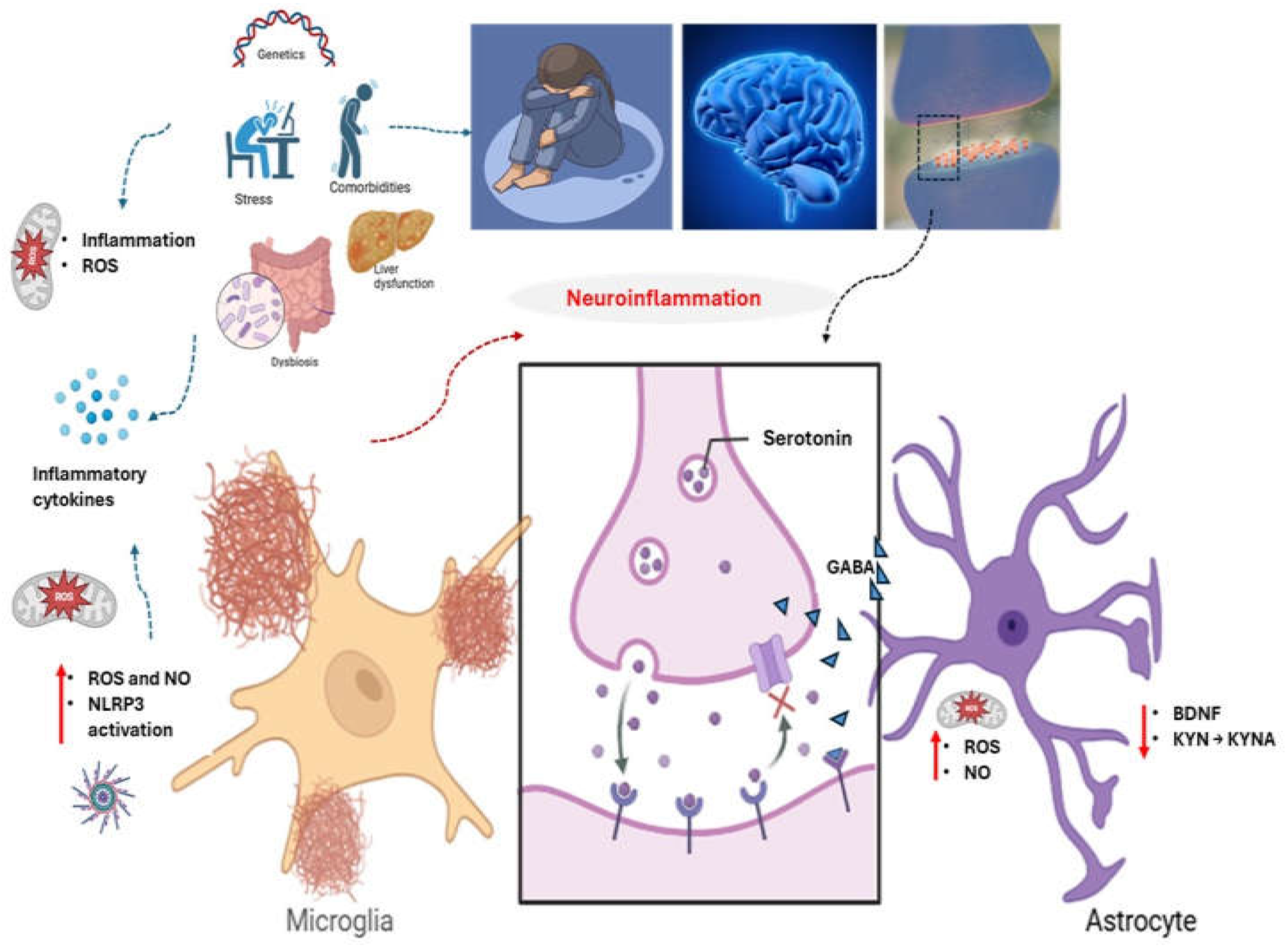
Figure 2.
PRISMA flow diagram illustrates the systematic selection process of clinical trials evaluating phytocompounds in Major Depressive Disorder (MDD). Of the 98 initially identified records, 42 were excluded due to duplication, non-English language, unpublished or non-peer-reviewed formats. Of the remaining 56, 21 full-text articles underwent eligibility assessment. Three were excluded for methodological limitations or insufficient relevance. Ultimately, 19 rigorously appraised interventional studies were included in the final synthesis, forming the evidence base for this review.
Figure 2.
PRISMA flow diagram illustrates the systematic selection process of clinical trials evaluating phytocompounds in Major Depressive Disorder (MDD). Of the 98 initially identified records, 42 were excluded due to duplication, non-English language, unpublished or non-peer-reviewed formats. Of the remaining 56, 21 full-text articles underwent eligibility assessment. Three were excluded for methodological limitations or insufficient relevance. Ultimately, 19 rigorously appraised interventional studies were included in the final synthesis, forming the evidence base for this review.
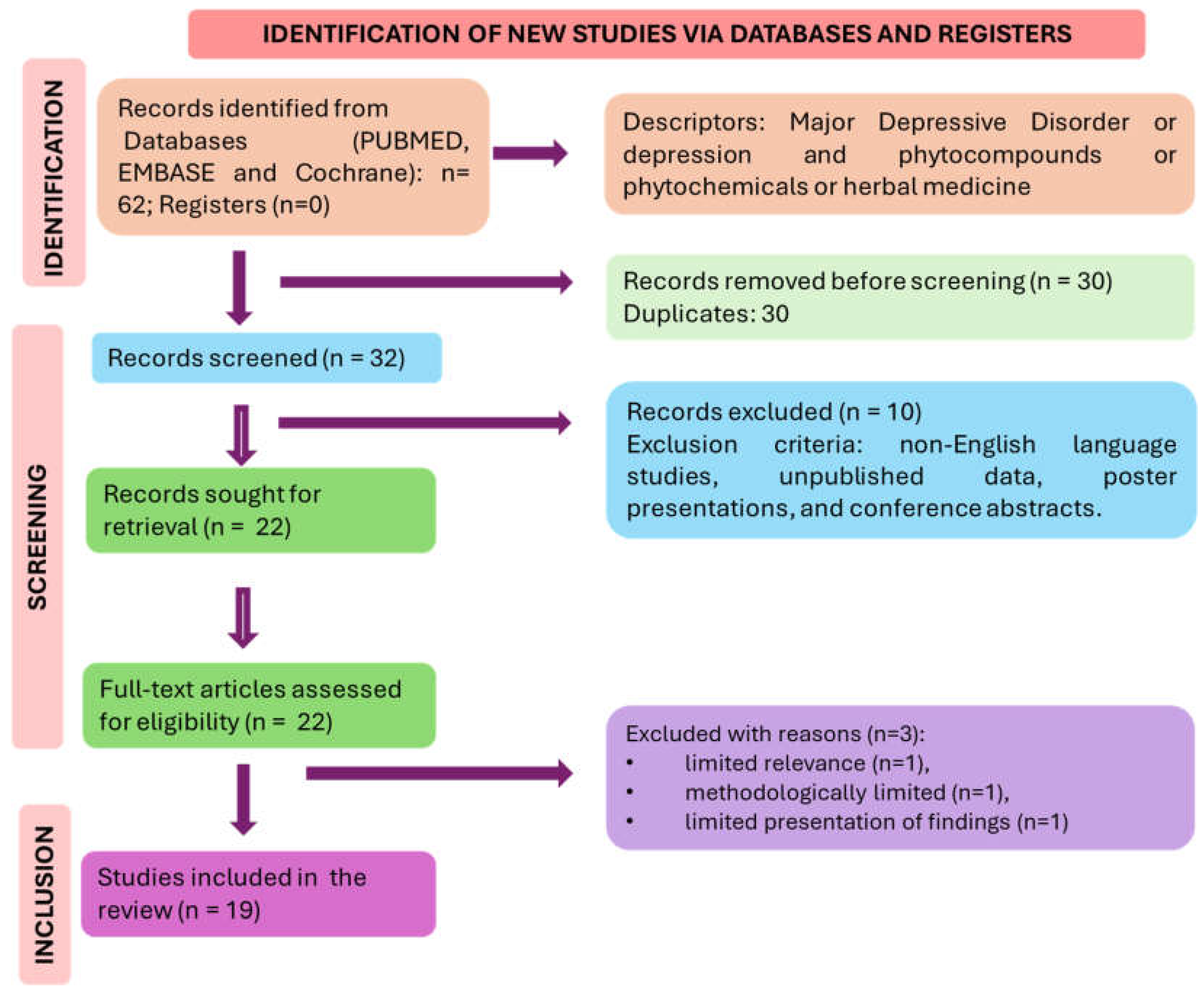
Figure 3.
Phytochemicals and the role in brain health and reduction of depression. HPA: hypothalamic-pituitary-adrenal; BDNF: Brain-derived neurotrophic factor. a: hypericin; b: coumarin; c: eucalyptol; d: resveratrol; e: curcumin; f: gallic acid; g: epicathechin.
Figure 3.
Phytochemicals and the role in brain health and reduction of depression. HPA: hypothalamic-pituitary-adrenal; BDNF: Brain-derived neurotrophic factor. a: hypericin; b: coumarin; c: eucalyptol; d: resveratrol; e: curcumin; f: gallic acid; g: epicathechin.
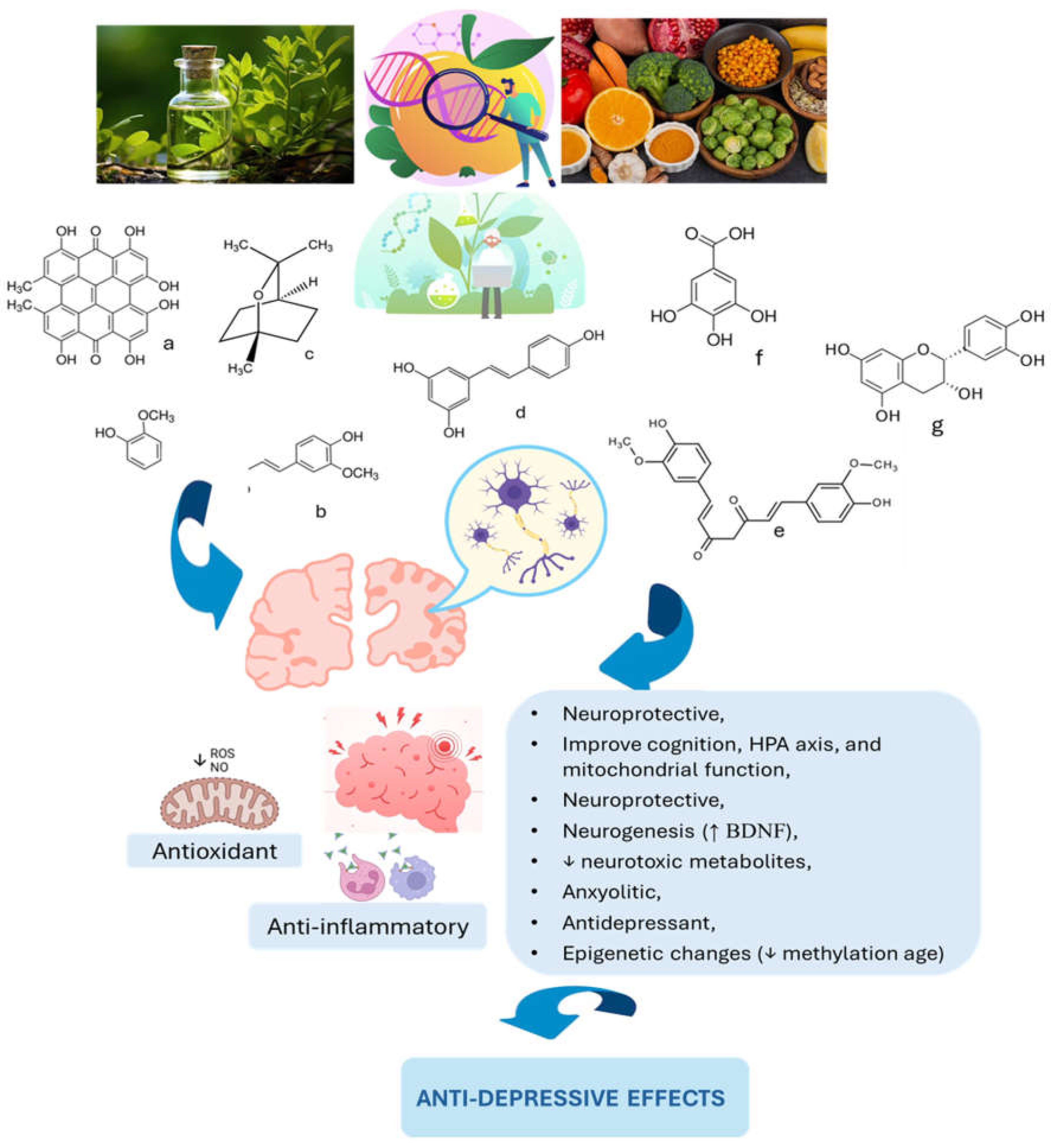
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



