
Submitted:
09 April 2025
Posted:
09 April 2025
You are already at the latest version
Abstract
This study investigated the proportion and trend of transmitted drug resistance (TDR) mutations and human immunodeficiency virus (HIV)-1 subtypes among 487 antiretroviral therapy–naive individuals in Korea from 2021 to 2024 to inform better treatment strategies. Consistent with previous reports, subtype B was the most prevalent among HIV-1 subtypes at 50.7%; however, its proportion has decreased annually. The distribution of circulating recombinant forms has increased, leading to a high genetic diversity. The subtype distributions of Korean and non-Korean patients differed, with subtype B (53.7%) and CRF01_AE (34.4%) being dominant in the former and latter, respectively. TDR across antiretroviral drug classes was approximately 3.5% in Korea. Non-nucleoside reverse transcriptase inhibitors elicited the highest level of drug resistance, which increased from 2021 to 2023, with a slight decrease in 2024. The integrase strand transfer inhibitor drugs, elvitegravir and raltegravir, most frequently exhibited high resistance scores. We provide a comprehensive overview of the HIV genetic distribution and TDR trends in Korea from 2021 to 2024. Within the broader context of HIV epidemiology in Asia and the Pacific, the findings contribute to a comprehensive understanding of the global distribution of HIV resistance and genotypes, enabling the development of effective interventions.
Keywords:
drug resistance
; transmitted drug resistance mutations
; human immunodeficiency virus
; HIV genetic diversity
; antiretroviral therapy
1. Introduction
In 2023, 39.9 million people worldwide (6.7 million in Asia and the Pacific) were living with the human immunodeficiency virus (HIV) [1]. According to the Joint United Nations Programme on HIV/AIDS, 30.7 million people with HIV (PWH) had been treated with antiretroviral (ARV) drugs [1]. The cumulative number of PWH in Korea was 19,745 [2].
PWH need to undergo lifelong antiretroviral therapy (ART) to control their viral load [3]. However, ART can induce drug resistance mutations (DRMs), which cause viral rebound and treatment failure. Drug resistance can be transmitted to treatment-naive individuals, and these transferred drug resistance mutations (TDRMs) spread throughout the population over time [4]. Therefore, understanding the prevalence patterns of TDRMs, as well as the HIV genetic diversity, may inform the selection of ARV drugs [5]. Studies performed on newly diagnosed PWH in Korea have elucidated the pattern of TDRMs and the HIV genetic diversity within the population. Several studies have highlighted the importance of analyzing the TDRMs within HIV subtypes. A study on PWH in Italy from 2004 to 2012 demonstrated the interplay between HIV genetic diversity and TDRMs [6].
Extensive genetic diversity is a major challenge to HIV vaccine development. Although HIV-1 is the most common type of this virus, global diversity has increased owing to changes in country-level distributions of HIV-1 variants [7]. In Korea, subtype B was dominant, accounting for 70.7% of the analyzed samples, between 2018 and 2019 [8]. However, this prevalence sharply decreased to 42.1% in 2023, whereas that of recombinant forms increased to 53.4% [9].
In light of these observations, we analyzed the TDRMs and the genetic distribution among newly diagnosed PWH over the last 4 years. This study was aimed at providing insights into the current status of the HIV epidemic in Korea based on the TDRM patterns, HIV genetic diversity, and differences in subtypes of Korean and non-Korean patients.
2. Materials and Methods
2.1. Study Population and Design
Recently diagnosed PWH who had not been exposed to ART were included. The initial diagnosis for all PWH was made between January 2021 and October 2024. Demographic data were obtained from the Division of HIV/AIDS Prevention and Control at the Korea Disease Control and Prevention Agency (KDCA).
2.2. RNA Extraction, Polymerase Chain Reaction (PCR) Amplification, Sequencing, and Genome Assembly
Viral RNA was extracted from 140 µL of plasma or serum using the QIAcube extraction system (Qiagen, Germany), according to the manufacturer’s instructions. Reverse transcription and nested PCR were performed to amplify the envelope (env), gag protein (gag), and pol protein (pol) for genotyping and the protease, reverse transcriptase, and integrase genes for drug resistance analysis. Genes were reverse-transcribed and amplified using the PrimeScript™ One Step RT-PCR kit (Takara, Japan), and nested PCR was conducted using the AccuPower ProFi Taq PCR PreMix (Bioneer, Republic of Korea). Sanger sequencing was performed using in-house sequencing primers. Sequence quality and generated consensus sequence alignments were assessed using Geneious Prime software (Biomatters Ltd., New Zealand).
2.3. HIV Sequencing and Subtyping
Sequence fragments were edited and assembled using SeqMan Pro 7.1.0 (44.1). HIV was subtyped using the automated HIV DB BLAST tools provided by Los Alamos National Laboratory, USA (https://hiv.lanl.gov/content/sequence/BASIC_BLAST/basic_blast.html). The subtype results were analyzed based on the similarity percentage and frequency count of the partial env, gag, and pol regions.
2.4. HIV Drug Resistance Analysis
Drug resistance regions, specifically protease, reverse transcriptase, or integrase, were targeted for analysis using the Stanford drug resistance database, following the criteria outlined in the analysis guide provided by the World Health Organization (WHO) [10]. Stanford HIVdb drug resistance algorithm version 9.7 was utilized to evaluate the impact of TDRMs on therapeutic responses. This algorithm assigns a specific score to each detected TDRM and categorizes them into one of five susceptibility levels: a total score of less than 10 is considered susceptible (S), 10 to 14 indicates potential low-level resistance (PLR), 15 to 29 indicates low-level resistance (LR), 30 to 59 indicates intermediate resistance (IR), and over 60 indicates high-level resistance (HR). All currently available drugs were included for analysis. Protease inhibitors (PIs): atazanavir (ATV/r), darunavir (DRV/r), fosamprenavir (FPV/r), indinavir (IDV/r), lopinavir (LPV/r), nelfinavir (NFV), saquinavir (SQV/r), and tipranavir (TPV/r); nucleoside reverse transcriptase inhibitors (NRTIs): abacavir (ABC), zidovudine (AZT), stavudine (D4T), didanosine (DDI), emtricitabine (FTC), lamivudine (3TC), and tenofovir (TDF); non-nucleoside reverse transcriptase inhibitors (NNRTIs): doravirine (DOR), efavirenz (EFV), etravirine (ETR), nevirapine (NVP), and rilpivirine (RPV); integrase strand transfer inhibitors (INSTIs): bictegravir (BIC), cabotegravir (CAB), dolutegravir (DTG), elvitegravir (EVG), and raltegravir (RAL). PLR and accessory mutations for PI and INSTI were excluded from the analysis [11]. To evaluate whether drug resistance differed significantly between subtype B and non-B populations, a two-tailed t-test was performed using Microsoft Excel. The resulting p-value was used to determine statistical significance.
2.5. Ethical Approval
All the authors hereby declare that all the experiments were reviewed and granted an exemption from ethical approval by the appropriate ethics committee (the KDCA Institutional Review Board Ethics Committee; approval number: KDCA-2025-01-03-PE-01). The requirement for informed consent from study participants was also waived by the KDCA Institutional Review Board.
3. Results
3.1. Study Population
The study included 487 PWH: 99 from 2021, 143 from 2022, 148 from 2023, and 97 from 2024. According to sex, the study population during this period consisted of an average of 95.5% male, 4.3% female, and 0.2% unknown. Koreans and non-Koreans constituted 87.5% and 12.5%, respectively. The countries of origin for non-Koreans were Asian, American, or unknown. Table 1 summarizes the demographic information for the PWH.
3.2. Genetic Diversity
The genotypes of 487 PWH diagnosed from 2021 to 2024 were analyzed. The most HIV infections were of subtype B. The proportions of subtypes B, circulating recombinant forms (CRFs), A6, and C were 50.7%, 44.4%, 4.5%, and 0.4%, respectively (Figure 1). Among the CRFs, CRF01_AE (24.6%) was the most prevalent, followed by CRF56_cpx (5.1%), CRF_BC (5.1%), CRF_01B (3.7%), CRF_01BC (3.5%), CRF_0263 (1.6%), CRF02_AG (0.4%), and CRF06_cpx (0.2%). The subtype patterns were different for Koreans and non-Koreans (Figure 2). Among the 423 Koreans, subtype B (53.7%) was the most prevalent, followed by CRF01_AE (23.2%), CRF56_cpx (5.9%), CRF_BC (5.0%), CRF_01B (3.5%), CRF_01BC (3.5%), A6 (3.1%), CRF_0263 (1.4%), CRF02_AG (0.5%), and CRF06_cpx (0.2%). In contrast, CRF01_AE (34.4%) was dominant among non-Koreans, followed by B (31.3%), A6 (14.1%), CRF_BC (6.3%), CRF_01B (4.7%), CRF_01BC (3.1%), CRF_0263 (3.1%), and C (3.1%).
3.3. Distribution and Characterization of DRMs
Drug resistance analysis included 417 PWH from 2021 to 2024. The average drug resistance across classes was 1.9%, 4.1%, 4.9%, and 3.3% in 2021, 2022, 2023, and 2024, respectively (Figure 3). The most frequent single-class mutations were against NNRTIs (18/284, 6.3%), followed by INSTIs (14/364, 3.8%), NRTIs (9/284, 3.2%), and PIs (5/281, 1.8%). The DRM proportion for NNRTIs, which was the highest, increased from 2.5% in 2021 to 5.4% in 2022, 7.5% in 2023, and 8.3% in 2024 (Figure 3). Drug resistance according to the population subtype (B and non-B) showed no statistically significant differences (p=0.823) (Table 2). E138A(or G) and E92Q(or V) were the most commonly observed mutations against NNRTIs and INSTIs, respectively (Figure 4). Each drug was independently analyzed. The highest cases of drug resistance were against ATV/r and NFV, D4T, NVP, and RAL among PIs, NRTIs, NNRTIs, and INSTIs, respectively (Figure 5). The analysis of the drug resistance scores for these drugs revealed that drug resistance cases for ATV/r, NFV, and D4T were mostly LR; however, NVP and RAL showed IR or HR drug resistance scores in most cases. NVP elicited five cases of IR and HR and three cases of LR. RAL elicited seven cases of HR, followed by six cases of IR and one case of LR. Detailed information on TDRMs according to drug class is shown in Figure 5.
4. Discussion
This study analyzed the HIV genetic distribution and ARV drug resistance among recently diagnosed PWH in Korea from 2021 to 2024. HIV is a persistent virus that exhibits a high degree of genetic diversity. According to the Los Alamos National Laboratory Database, 158 CRFs have been reported (as of Oct 14, 2024), and this number is continuously increasing [12]. Subtype B was the most prevalent in Korea; however, its prevalence has steadily decreased from 93.1% in 1992–2012 to 70.3% in 2018–2019 [8,13,14]. It was found to be dominant (50.7%) in this study. Among Koreans, subtype B (53.7%) was the most prevalent, followed by CRF01_AE (23.2%). In contrast, CRF01_AE (34.4%) followed by B (31.3%) were the most common subtypes among non-Koreans. The global trend of genetic distribution across continents did not change notably from 2010 to 2021. However, there has been an approximately 8% increase in the proportion of CRFs and unique recombinant forms. CRF01_AE (29%) has been the major subtype among those in Asia and the Pacific [15,16]. Specifically, among the non-Korean individuals in this study, those from Asia and the Pacific have the highest proportion, with the subtype distribution reported as CRF01_AE (29%), B (13%), and C (13%) [15]. The recent changes in the subtype pattern of Koreans appear to have been influenced by the epidemiological trends of neighboring countries. The distribution patterns of subtypes among non-Koreans are mainly associated with the subtypes circulating in their home countries, suggesting that they were likely infected within the country. Notably, since 59.4% of the non-Koreans in this study were of Asian nationality, it is important to continuously monitor the molecular genetics of HIV in neighboring countries.
Consistent with previous results [8,9], NNRTIs elicited the highest level of drug resistance, which increased from 2021 to 2024. This study showed that about 3.6% of treatment-naive PWH were resistant to at least one ARV drug from 2021 to 2024. An analysis of the number of drug resistance cases for a single drug by subtype (B and non-B) showed no significant difference between the groups. According to the clinical treatment guideline for HIV in Korea, a combination including an INSTI is recommended as the first-line treatment for treatment-naive patients, followed by a regimen combining an INSTI and NRTI [17]. Currently, there are no cases of drug resistance to both INSTIs and NRTIs for any subtype (B or non-B), suggesting that dual regimens could be viable starting options.
The most prevalent mutation in the NNRTI class was E138A(or G), which caused LR to RPV. E138A(or G) was identified twice in 2023 and 2024, and all the patients were diagnosed with subtype CRF_0263, suggesting that further analysis of this association is needed. Drug resistance to FTC and TDF was also analyzed because RPV has been co-formulated with these drugs for initial therapy [18]. All four cases showed susceptibility to both drugs. The E138A is known to occur in approximately 2–5% of ART-naive individuals, depending on subtype; however, it is not known whether this mutation selectively occurs in NNRTI-treated individuals [19]. The most prevalent mutation in the INSTI class was E92Q(or V). Four cases showed HR for EVG and IR for RAL. Three exhibited LR and one showed PLR for CAB. The E92Q mutation is known to be the most common cause of resistance to INSTIs such as EVG and RAL. This mutation has been reported as the most common INSTI mutation at the first time point of treatment failure with INSTI-based ART [20]. Therefore, further research is needed to explore the impact of this mutation on ART.
Although generally excluded from the DRM proportion, PLR should also be considered. In this study, the notable mutations causing PLR were V179D (or E or F) (25 cases) for NNRTIs and E157Q (16 cases) for PIs. V179D(or E) is the most common NNRTI-associated mutation in China and is known to significantly regulate the replication capacity of HIV [21,22,23]. E157Q decreases the integrase enzymatic activity promoted by the R263K substitution, and E157Q–R263K could lead to virological failure upon treatment with DTG [24,25]. These mutations were not detected simultaneously in this study. Therefore, they are not currently at a concerning level but have to be continuously monitored.
The distribution of resistance scores by drug revealed that HR was most frequently elicited by EVG and RAL, both INSTIs. RAL and EVG were approved by the FDA in 2007 and 2012, respectively, and have been in use for a long time [26]. Both these drugs have a low to moderate genetic barrier to resistance; cross-resistance to them has also been observed [27]. Therefore, they are of significant concern.
As a result of increased HIVDR to NNRTIs and subsequent cost implications, the WHO has recommended DTG-based first- and second-line ART for PWH since 2018 [28,29]. It also recommends high-priority monitoring of HIVDR to DTG by implementing surveys [30]. Additionally, according to the clinical treatment guidelines for HIV in Korea [17], combinations of antiretroviral drugs such as ABC/3TC/DTG, TAF/FTC/BIC, TAF/FTC+DTG, TAF/FTC+RAL, and 3TC/DTG are recommended. DTG is expected to be commonly prescribed in Korea. Therefore, the number of drug resistance cases for the DTG during the analyzed period revealed that DTG drug resistance increased from zero cases in 2021 to one and five cases in 2022 and 2023, respectively, but decreased to one case in 2024. This study indicates that, although the frequency of DTG resistance is not yet at a concerning level, there is still a need for continuous monitoring.
This study has a few limitations. First, only a limited number of samples were used. This study includes only 10% of newly diagnosed PWH. Therefore, a more comprehensive data analysis is needed to determine trends across the population. Second, epidemiological association was limited owing to a lack of some clinical information such as timing of infection, sexual behaviors and risk factors, immune status, history of sexually transmitted and other infections, and demographic characteristics. Finally, some foreign individuals were uncertain about whether they were taking any ARV drugs.
Notwithstanding these limitations, this study has several important implications. It provides a comprehensive overview of the distribution of HIV subtypes and trends in TDR in Korea from 2021 to 2024. There is no compelling evidence that the HIV subtype needs to be considered when choosing ARV drugs; however, some studies have demonstrated an association between drug resistance and subtypes [31,32,33]. The inclusion criteria ensured that PWH included in this analysis were treatment-naive at the time of diagnosis, which is crucial for accurately reflecting the proportion and impact of TDRMs in treatment-naive individuals. The WHO has established HIVResNET to support global drug resistance research [34]. Within the context of HIV epidemiology in Asia and the Pacific, the findings of this study contribute to an in-depth understanding of the global distribution of HIV resistance and genotypes, which should enable the development of more effective response strategies.
Author Contributions
Conceptualization, J.S.W. and M.G.H.; methodology, G.K., E.J.K. and M.K.; writing—original draft preparation, G.K. and J.S.W.; writing—review and editing, J.S.W. and M.G.H.; visualization, G.K.; Funding acquisition, S.K.; project management, J.S.W., H.M.K. and M.G.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by the Korea Disease Control and Prevention Agency (grant No. 6331-301-210).
Institutional Review Board Statement
Ethical review and approval were waived for this study due to the use of anonymized residual samples. Researchers had no access to donor identification, and the study results are unrelated to individual genetic characteristics.
Informed Consent Statement
Patient consent was waived due to the use of residual samples remaining after diagnosis, which were assigned serial numbers to prevent personal identification.
Data Availability Statement
The data used to support this study are available from the corresponding author upon request.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PWH | People with HIV |
| ARV | Antiretroviral |
| ART | Antiretroviral therapy |
| DRMs | Drug resistance mutations |
| TDRMs | Transferred drug resistance mutations |
| KDCA | Korea Disease Control and Prevention Agency |
| PCR | Polymerase chain reaction |
| WHO | World Health Organization |
| S | Susceptible |
| PLR | Potential low-level resistance |
| LR | Low-level resistance |
| IR | Intermediate resistance |
| HR | High-level resistance |
| PI | Protease inhibitor |
| ATV/r | Atazanavir |
| DRV/r | Darunavir |
| FPV/r | Fosamprenavir |
| IDV/r | Indinavir |
| LPV/r | Lopinavir |
| NFV | Nelfinavir |
| SQV/r | Saquinavir |
| TPV/r | Tipranavir |
| NRTIs | Nucleoside |
| ABC | Abacavir |
| AZT | Zidovudine |
| D4T | Stavudine |
| DDI | Didanosine |
| FTC | Emtricitabine |
| 3TC | Lamivudine |
| TDF | Tenofovir |
| NNRTI | Non-nucleoside reverse transcriptase inhibitor |
| DOR | Doravirine |
| EFV | Efavirenz |
| ETR | Etravirine |
| NVP | Nevirapine |
| RPV | Rilpivirine |
| INSTI | Integrase strand transfer inhibitor |
| BIC | Bictegravir |
| CAB | Cabotegravir |
| DTG | Dolutegravir |
| EVG | Elvitegravir |
| RAL | Raltegravir |
| CRF | Circulating recombinant form |
References
- Joint United Nations Programme on HIV/AIDS. Global HIV Statistics Fact sheet 2024. Available online: https://www.unaids.org/sites/default/files/media_asset/UNAIDS_FactSheet_en.pdf (accessed on 15 Jan 2025).
- Korea Disease Control and Prevention Agency. Annual Report on HIV/AIDS Notifications in Korea, 2023.
- Peter, T.; Ellenberger, D.; Kim, A.A.; Boeras, D.; Messele, T.; Roberts, T.; Stevens, W.; Jani, I.; Abimiku, A.; Ford, N.; et al. Early antiretroviral therapy initiation: access and equity of viral load testing for HIV treatment monitoring. Lancet Infect. Dis. 2017, 17, e26–e29. [Google Scholar] [CrossRef] [PubMed]
- Blassel, L.; Zhukova, A.; Villabona-Arenas, C.J.; Atkins, K.E.; Hué, S.; Gascuel, O. Drug resistance mutations in HIV: new bioinformatics approaches and challenges. Curr. Opin. Virol. 2021, 51, 56–64. [Google Scholar] [CrossRef] [PubMed]
- Geremia, N.; Basso, M.; De Vito, A.; Scaggiante, R.; Giobbia, M.; Battagin, G.; Dal Bello, F.; Giordani, M.T.; Nardi, S.; Malena, M.; et al. Patterns of transmitted drug resistance mutations and HIV-1 subtype dynamics in ART-naïve individuals in Veneto, Italy, from 2017 to 2024. Viruses 2024, 16, 1393. [Google Scholar] [CrossRef]
- Parisi, S.G.; Andreis, S.; Scaggiante, R.; Cruciani, M.; Ferretto, R.; Manfrin, V.; Panese, S.; Rossi, M.C.; Francavilla, E.; Boldrin, C.; et al. Decreasing trends of drug resistance and increase of non-B subtypes amongst subjects recently diagnosed as HIV-infected over the period 2004–2012 in the Veneto Region, Italy. J. Glob. Antimicrob. Resist. 2013, 1, 201–206. [Google Scholar] [CrossRef]
- Nair, M.; Gettins, L.; Fuller, M.; Kirtley, S.; Hemelaar, J. Global and regional genetic diversity of HIV-1 in 2010–21: systematic review and analysis of prevalence. Lancet Microbe. 2024, 5, 100912. [Google Scholar] [CrossRef] [PubMed]
- Park, K.R.; Sim, H.J.; Wang, J.; Han, M. Analysis of genotype and drug resistance of human immunodeficiency virus in Korea from 2018–2019. Public health weekly report (PHWR). 2020, 13, 41. [Google Scholar]
- Kim, G.; Wang, J.; Kim, H.M.; Kim, S.; Kim, E.J.; Han, M. Genetic diversity and drug resistance of human immunodeficiency virus from newly diagnosed human immunodeficiency virus positive in Korean. 2022–2023. Public Health Weekly Report (PHWR) 2024, 17, 44.
- World Health Organization. WHO manual for HIV drug resistance testing using dried blood spot specimens. Available online: https://www.who.int/publications/i/item/9789240009424 (accessed on 3 Febr 2025).
- Stanford University. HIV Drug resistance database. HIVDB User Guide [Internet]. 2024. Available online: https://hivdb.stanford.edu/pages/documentPage/user_guide.pdf (accessed on 20 Jan 2025).
- Los Alamos National Laboratory. HIV circulating recombinant forms (CRFs) [Internet]. 2024. Available online: https://www.hiv.lanl.gov/components/sequence/HIV/crfdb/crfs.comp (accessed on 20 Jan 2025).
- Chung, Y.S.; Choi, J.Y.; Yoo, M.S.; Seong, J.H.; Choi, B.S.; Kang, C. Phylogenetic transmission clusters among newly diagnosed antiretroviral drug-naïve patients with human immunodeficiency virus-1 in Korea: A study from 1999 to 2012. PLOS One 2019, 14, e0217817. [Google Scholar] [CrossRef]
- Kim, J.M.; Kim, N.J.; Choi, J.Y.; Chin, B.S. History of acquired immune deficiency syndrome in Korea. Infect. Chemother. 2020, 52, 234–244. [Google Scholar] [CrossRef]
- Williams, A.; Menon, S.; Crowe, M.; Agarwal, N.; Biccler, J.; Bbosa, N.; Ssemwanga, D.; Adungo, F.; Moecklinghoff, C.; Macartney, M.; et al. Geographic and population distributions of human immunodeficiency virus (HIV)-1 and HIV-2 circulating subtypes: A systematic literature review and meta-analysis (2010–2021). J. Infect. Dis. 2023, 228, 1583–1591. [Google Scholar] [CrossRef]
- Bbosa, N.; Kaleebu, P.; Ssemwanga, D. HIV subtype diversity worldwide. Curr. Opin. HIV AIDS. 2019, 14, 153–160. [Google Scholar] [CrossRef]
- Korean Society for AIDS. Summary of 2021 clinical guidelines for the diagnosis and treatment of HIV/AIDS in HIV-infected Koreans. Infect. Chemother. 2021, 53, 592–616. [Google Scholar] [CrossRef]
- Sluis-Cremer, N.; Jordan, M.R.; Huber, K.; Wallis, C.L.; Bertagnolio, S.; Mellors, J.W.; Parkin, N.T.; Harrigan, P.R. E138A in HIV-1 reverse transcriptase is more common in subtype C than B: implications for rilpivirine use in resource-limited settings. Antiviral Res. 2014, 107, 31–34. [Google Scholar] [CrossRef]
- Stanford University. HIV Drug resistance database. nnrti Resistance Notes. HIVdb version 9.8 [Internet]. Available online: https://hivdb.stanford.edu/dr-summary/resistance-notes/nnrti (accessed on 6 Mar 2025).
- Hatano, H.; Lampiris, H.; Fransen, S.; Gupta, S.; Huang, W.; Hoh, R.; Martin, J.N.; Lalezari, J.; Bangsberg, D.; Petropoulos, C.; et al. Evolution of integrase resistance during failure of integrase inhibitor-based antiretroviral therapy. J. Acquir. Immune Defic. Syndr. 2010, 54, 389–393. [Google Scholar] [CrossRef] [PubMed]
- Jiao, Y.; Li, S.; Li, Z.; Zhang, Z.; Zhao, J.; Li, L.; Wang, L.; Yin, Q.; Wang, Y.; Zeng, Z.; et al. HIV-1 transmitted drug resistance-associated mutations and mutation co-variation in HIV-1 treatment-naïve MSM from 2011 to 2013 in Beijing, China. BMC Infect. Dis. 2014, 14, 689. [Google Scholar] [CrossRef] [PubMed]
- Li, C.L.; Liang, H.Y.; Xiao, J.; Li, R.; Yu, F.T.; Zeng, Y.Q.; Pang, X.L.; Wang, D.; Liu, Y.; Li, B.; et al. The effect of pretreatment potential resistance to NNRTIs on antiviral therapy in patients with HIV/AIDS. J. Acquir. Immune Defic. Syndr. 2022, 91, S27–S34. [Google Scholar] [CrossRef] [PubMed]
- Vink, J.; McFaul, K.; Bradshaw, D.; Nelson, M. Does the presence of a mutation at position V179 impact on virological outcome in patients receiving antiretroviral medication? J. Infect. 2016, 72, 632–633. [Google Scholar] [CrossRef]
- Buzon-Martin, L.; Navarro-San Francisco, C.; Fernandez-Regueras, M.; Sanchez-Gomez, L. Integrase strand transfer inhibitor resistance mediated by R263K plus E157Q in a patient with HIV infection treated with bictegravir/tenofovir alafenamide/emtricitabine: case report and review of the literature. J. Antimicrob. Chemother. 2024, 79, 1153–1156. [Google Scholar] [CrossRef]
- Charpentier, C.; Descamps, D. Resistance to HIV integrase inhibitors: about R263K and E157Q mutations. Viruses. 2018, 10, 41. [Google Scholar] [CrossRef]
- Mbhele, N.; Chimukangara, B.; Gordon, M. HIV-1 integrase strand transfer inhibitors: a review of current drugs, recent advances and drug resistance. Int. J. Antimicrob. Agents. 2021, 57, 106343. [Google Scholar] [CrossRef]
- Wainberg, M.A.; Han, Y.S. HIV-1 resistance to dolutegravir: update and new insights. J. Virus Erad. 2015, 1, 13–16. [Google Scholar] [CrossRef]
- Washaya, T.; Manasa, J.; Kouamou, V. HIV drug resistance monitoring in the era of dolutegravir and injectable long-acting cabotegravir in resource-limited settings. AIDS 2023, 37, 1629–1631. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. New Report Documents Increase in HIV Drug Resistance to Dolutegravir. Available online: https://www.who.int/news/item/05-03-2024-new-report-documents-in-hiv-drug-resistance-to-dolutegravir (accessed on 23 Jan 2025).
- World Health Organization. HIV Drug Resistance: Brief Report, 2024.
- Lessells, R.J.; Katzenstein, D.K.; de Oliveira, T. Are subtype differences important in HIV drug resistance? Curr. Opin. Virol. 2012, 2, 636–643. [Google Scholar] [CrossRef] [PubMed]
- Han, Y.S.; Mesplède, T.; Wainberg, M.A. Differences among HIV-1 subtypes in drug resistance against integrase inhibitors. Infect. Genet. Evol. 2016, 46, 286–291. [Google Scholar] [CrossRef]
- Chaplin, B.; Akanmu, A.S.; Inzaule, S.C.; Samuels, J.O.; Okonkwo, P.; Ilesanmi, O.; Adewole, I.F.A.; Asadu, C.; Khamofu, H.; Mpazanje, R.; et al. Association between HIV-1 subtype and drug resistance in Nigerian infants. J. Antimicrob. Chemother. 2019, 74, 172–176. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. WHO HIVResNet HIV drug resistance laboratory operational framework. 2020. Available online: https://www.who.int/publications/i/item/978-92-4-000987-5 (accessed on 3 Febr 2025).
Figure 1.
Human immunodeficiency virus (HIV) subtypes were identified in 487 people with HIV (PWH). Percentages <1% were not marked. CRF: Circulating recombinant form.
Figure 1.
Human immunodeficiency virus (HIV) subtypes were identified in 487 people with HIV (PWH). Percentages <1% were not marked. CRF: Circulating recombinant form.
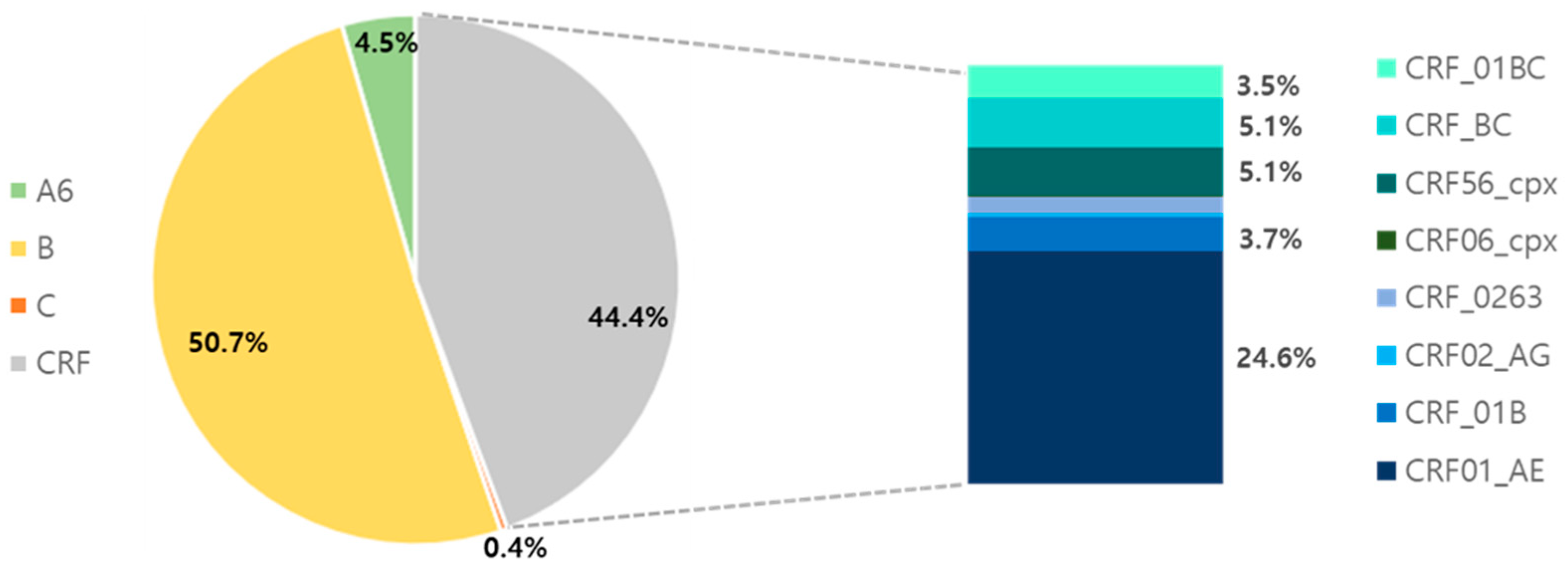
Figure 2.
Distribution of HIV subtypes according to ethnic group: (A) Koreans and (B) non-Koreans.
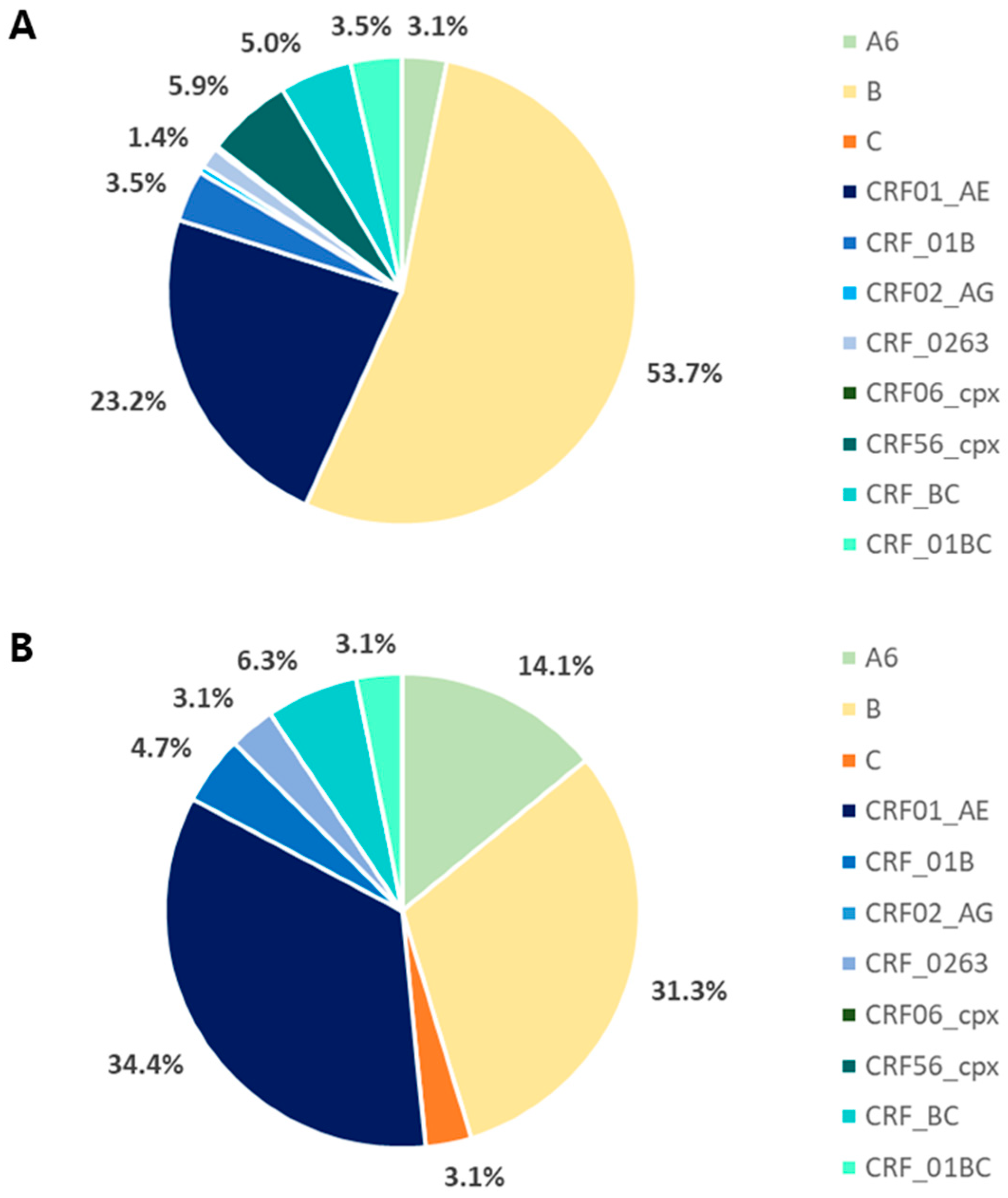
Figure 3.
Proportion of drug resistance mutations (DRMs) according to antiretroviral (ARV) drug classes. PI: protease inhibitor; NRTI: nucleoside reverse transcriptase inhibitor; NNRTI: non-nucleoside reverse transcriptase inhibitor; INSTI: integrase strand transfer inhibitor. The HIVdb program, based on the Stanford University HIV Drug Resistance Database, was used to assess DRMs according to ARV class. Accessory mutations were excluded for PI and INSTI.
Figure 3.
Proportion of drug resistance mutations (DRMs) according to antiretroviral (ARV) drug classes. PI: protease inhibitor; NRTI: nucleoside reverse transcriptase inhibitor; NNRTI: non-nucleoside reverse transcriptase inhibitor; INSTI: integrase strand transfer inhibitor. The HIVdb program, based on the Stanford University HIV Drug Resistance Database, was used to assess DRMs according to ARV class. Accessory mutations were excluded for PI and INSTI.
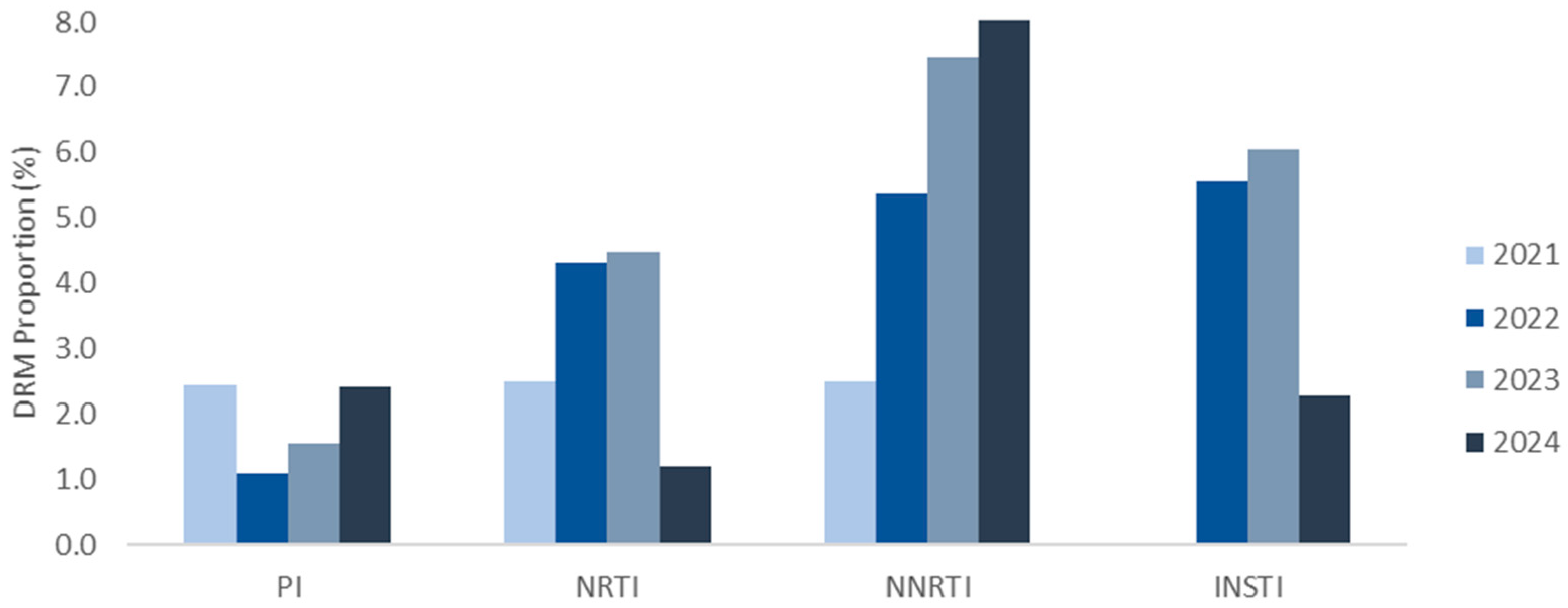
Figure 4.
Frequency of mutations associated with resistance to ARV drugs.
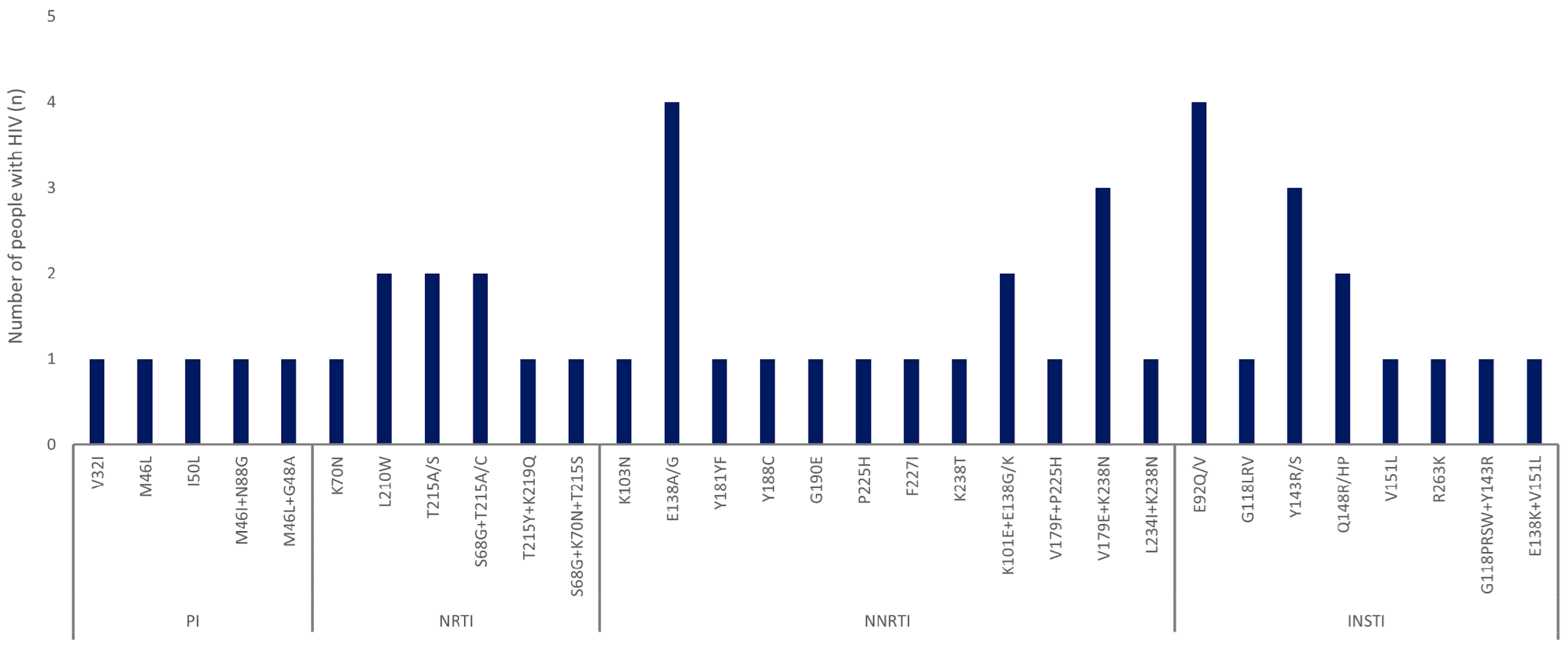
Figure 5.
Predicted resistance to antiretroviral drugs for HIV pol sequences with DRMs in PWH. PIs: atazanavir (ATV/r), darunavir (DRV/r), fosamprenavir (FPV/r), indinavir (IDV/r), lopinavir (LPV/r), nelfinavir (NFV), saquinavir (SQV/r), and tipranavir (TPV/r); NRTIs: abacavir (ABC), zidovudine (AZT), stavudine (D4T), didanosine (DDI), emtricitabine (FTC), lamivudine (3TC), and tenofovir (TDF); NNRTIs: doravirine (DOR), efavirenz (EFV), etravirine (ETR), nevirapine (NVP), and rilpivirine (RPV); INSTIs: bictegravir (BIC), cabotegravir (CAB), dolutegravir (DTG), elvitegravir (EVG), and raltegravir (RAL).
Figure 5.
Predicted resistance to antiretroviral drugs for HIV pol sequences with DRMs in PWH. PIs: atazanavir (ATV/r), darunavir (DRV/r), fosamprenavir (FPV/r), indinavir (IDV/r), lopinavir (LPV/r), nelfinavir (NFV), saquinavir (SQV/r), and tipranavir (TPV/r); NRTIs: abacavir (ABC), zidovudine (AZT), stavudine (D4T), didanosine (DDI), emtricitabine (FTC), lamivudine (3TC), and tenofovir (TDF); NNRTIs: doravirine (DOR), efavirenz (EFV), etravirine (ETR), nevirapine (NVP), and rilpivirine (RPV); INSTIs: bictegravir (BIC), cabotegravir (CAB), dolutegravir (DTG), elvitegravir (EVG), and raltegravir (RAL).
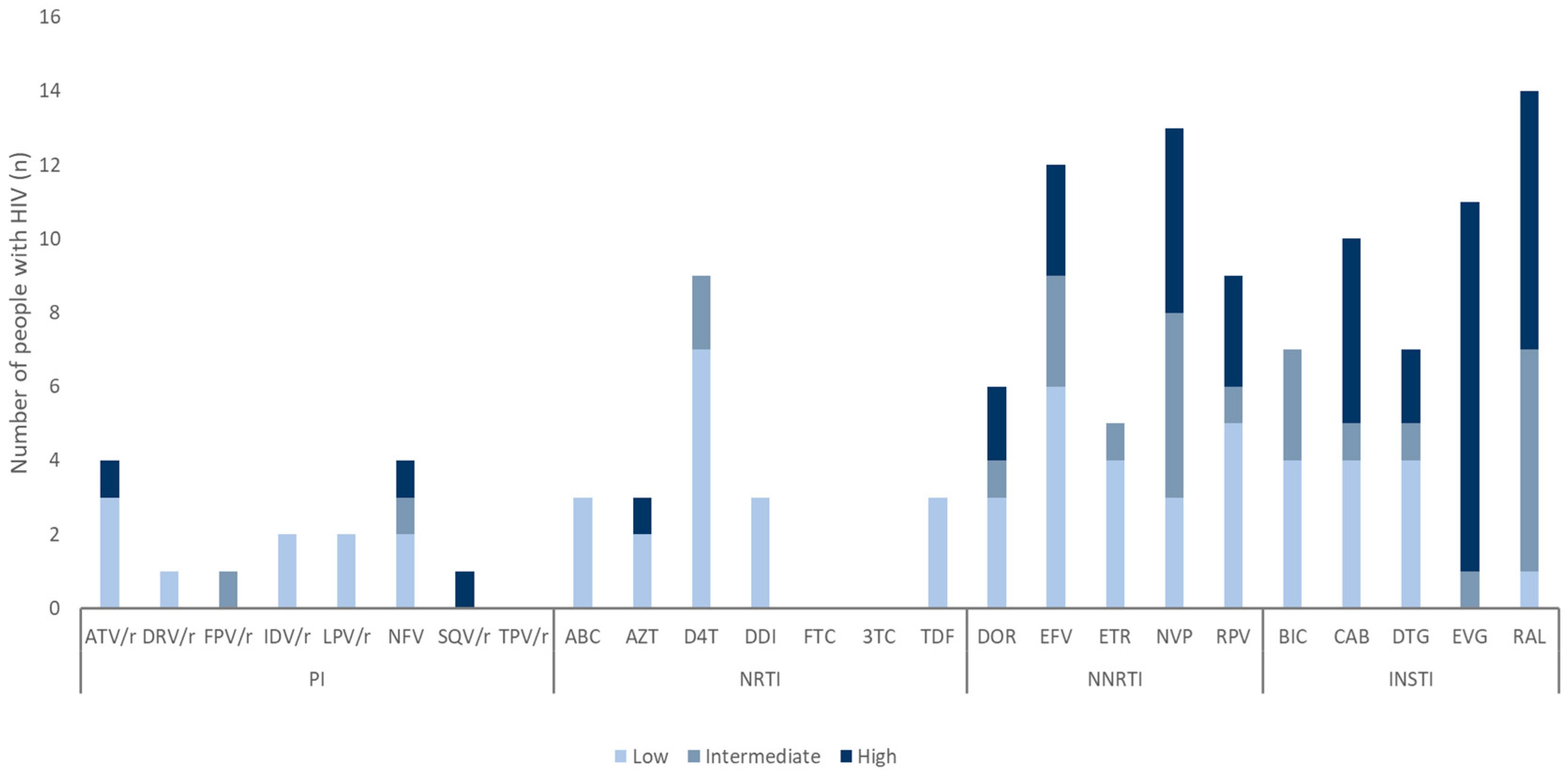

Table 1.
Demographics of study population (2021–2024).
| Variables | n (%) by collection year | ||||
| 2021 | 2022 | 2023 | 2024 | ||
| Sex | Male | 92 (92.9) | 137 (95.8) | 142 (95.9) | 93 (95.9) |
| Female | 7 (7.1) | 5 (3.5) | 6 (4.1) | 4 (4.1) | |
| Unknown | 0 (0.0) | 1 (0.7) | 0 (0.0) | 0 (0.0) | |
| Country of origin | Korean | 83 (83.8) | 121 (84.6) | 133 (89.9) | 86 (88.7) |
| Non-Korean | 16 (16.2) | 22 (15.4) | 15 (10.1) | 11 (11.3) | |
Table 2.
Proportion of DRMs: single and combination classes differentiated by B and non-B subtype from 2021 to 2024.
Table 2.
Proportion of DRMs: single and combination classes differentiated by B and non-B subtype from 2021 to 2024.
| Antiretroviral drug resistance n (%) | |||||||
| PI | NRTI | NNRTI | INSTI |
PI +NRTI |
PI +NNRTI |
NRTI +NNRTI |
|
| Total | 3 (1.1) | 5 (1.8) | 14 (4.9) | 14 (3.8) | 1 (0.4) | 1 (0.4) | 3 (1.1) |
| B | 1 (0.6) | 3 (1.8) | 7 (4.2) | 8 (4.3) | 0 | 0 | 3 (1.8) |
| Non-B | 2 (1.7) | 2 (1.7) | 7 (5.9) | 6 (3.4) | 1 (0.9) | 1 (0.9) | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



