
Submitted:
13 April 2025
Posted:
15 April 2025
Read the latest preprint version here
Abstract
It is not widely known that the human genome retains ancestral emergency programs that can be activated in response to germline stress and irreparable DNA damage, freeing affected cells from the constraints of multicellularity. The reactivation of unicellular genome modules—via a process known as the multicellular-to-unicellular transition (MUT)—represents an ancient mechanism rooted in the gradual back-and-forth transition to multicellularity. MUT modules are preserved in a reactivatable state within the genomes of all metazoans and are activated in approximately 50% of humans, particularly at advanced stages of life. This inversion to a unicellular genome state gives rise to a subpopulation of precancerous cells that proliferate through defective symmetric cell division (DSCD). Once DSCD progeny acquire fusibility, they form hyperpolyploid genome repair syncytia (MGRS), which work to eliminate genomic defects and establish a unicellular cancer stemgermline capable of producing committed, non-proliferative cancer stem cells. Similar to the Ur-germline of unicellular ancestors, the cancer stemgermline, along with its clones and sublines, is hypoxic and becomes dysfunctional in tissues with oxygen levels above 6.0% O₂, a condition referred to as germline hyperoxia. Together with a somatic helper lineage that does not generate cancer stem cells, the stem-germline forms an autonomous cellular system that functions according to the principles of unicellular life. The stem-germline and its somatic counterpart work in concert to maintain and expand a stable, unicellularized stemgermline genome
Keywords:
cancer
; Entamoeba
; stemgermline
; committed CSCs
; multicellular-unicellular transition
; genome evolution and stability
1.0. Introduction
Most cancer researchers today still view cancer cells as deregulated, diseased multicellular entities that give rise to a chaotic population of plastic successors—both stem cells and non-stem cells—all of which are genomically unstable and have lost their genomic integrity. Despite numerous indications over the past two decades suggesting that cancer cells may share an ancestral relationship with protists, particularly amoebae, or that they rely on ancestral genes, these insights have largely been overlooked or unrecognized. Molecular biologists continue to search for the driver genes responsible for transforming normal multicellular cells into abnormal multicellular entities—cancer cells [1]. As evident, cancer research remains centered around Dollo’s law of evolutionary irreversibility, a paradigm established 135 years ago.
In 1893, Louis Dollo[2] postulated that evolution cannot return to earlier states or to a previously realized state in an ancestral lineage [3]. According to this dogma, once a more or less complex trait has been lost, it remains lost forever. However, recent studies in phylogenomics and functional genomics have shown that this is not the case; evolution can, in fact, revert to conserved genetic and developmental ancestral programs [4,5].
As recently noted by Elmer and Clobertz [6], comprehensive evolutionary reconstructions and comparative studies of multiple lineages provide evidence of both loss and regain of traits through Ancestral State Reconstruction (ASR) [7,8,9]. Several compelling cases of „breaking Dollo’s law” have been reported in the recent literature, spanning diverse taxa, from bacteria to plants to animals.
Cancer is undoubtedly one such case [10,11,12,13]. In the post-genomic era, cancer exemplifies a reversal in the evolutionary history of a clade, occurring on a functional genomic basis [6]. Ancestral State Reconstruction (ASR) in cancer is not a transient phenomenon, nor is it merely a result of cellular plasticity [14,15,16]. Cancer demonstrates that ASR enables not only the reversion of individual traits and marker expression but also the transformation of entire cellular systems, from multicellularity to unicellularity. In this regained ancestral state, intermediate genomic losses and gains occur that were absent in the original multicellular system. Further molecular studies are required to classify losses and recoveries functionally, genomically, and post-genomically [6].
Unfortunately, many cancer researchers still adhere to the outdated theory that viewis cancer solely as a disease within the multicellular cell system, rather than recognizing the coexistence of two fundamentally different cell systems competing against each other: (1) the unicellularized cancer cell system, which arises from irreparably stress-damaged stemgemline cells, and (2) the multicellular host cell system. Unicellularization precedes carcinogenesis. It originates from senescent or apoptotic stemgermline cells and occurs during a prolonged phase of restorative senescence [13] through an evolutionary process of multicellular-to- unicellular transition (MUT).
MUT is a process of genome inversion that evolved approximately 1000–900 million years ago (Mya) during the Tonian period in early multicellular living forms with genomic deficiencies. It emerged as a counterpart to the unicellular-to-multicellular transition (UMT) processes. Through the reciprocal MUT process, stable unicellular genome networks replace unstable multicellular genome networks, allowing non-viable early metazoans to revert to stable unicellular life forms. Additionally, MUT facilitated renewed and more successful attempts at multicellularity. MUT mechanisms have been evolutionarily conserved in the genomes of all metazoans.
In this way, dysfunctional stemgermline cells of non-cancerous individuals can restrict their genome by downregulating and suppressing multicellular genome repair genes that have been damaged by stress factors and have become dysfunctional. MUT mechanisms and genome inversion programs persists in all metazoans and can be reactivated when dysfunctional multicellular stemgermline cells encounter restorative senescent niches along with appropriate inducers of unicellularization [13]. Within these niches, such cells can initiate evolutionarily MUT and repair processes, transitioning toward an autonomous unicellular life cycle characterized by the alternating ACD and DSCD phenotypes, with and without stemness potential.
The unicellular system of cancer is neither unstable nor chaotic. Instead, it develops and evolves according to the principles of complex unicellular life systems derived from the common AMF.
Recent advancements by the evolutionary cancer cell biology ECCB [10,11,12,13] highlight the deep homology between cancer cells and parasitic amoebae, drawing parallels with the common AMF ancestor of amoebozoans, metazoans and fungi. This perspective places ancestral state reconstruction at a higher explanatory level than mutational genetic changes, which alone have not satisfactorily clarified the origin, genome and function of cancer.
Furthermore, the ECCB has demonstrated that the primary driver of both unicellular cell systems - cancer and its Entamoeba model - is the stemgermline, previously referred to as the non-gametogenic (NG) germline. Stemgermlines are phylogenetically related to the hypoxic Ur-germline of the AMF ancestor. Ancestral stem- germlines give rise to non-proliferative committed stem cells and cancer stem cells (CSCs). In host tissues and the bloodstream, oxygen levels typically range from 0.1% to 13% (oxygen gradient), but the unicellular cell systems of cancer and amoebae function normoxically (physioxically) only below 6.0% oxygen. Oxygen levels exceeding this threshold create a hyperoxic environment for the stemgermline (germline hyperoxia), leading to irreversible genome damage. However, both cell systems possess unicellular repair mechanisms, such as hyperpolyploidization, to restore functional genomic states.
According to evolutionary cancer cell biology (ECCB), gaining deeper insight into the evolutionary history of the stemgermline, which drives cancer evolution is paramount to understanding cancer [13]. In recent years, significant progress in amoeba cell biology has provided a fortunate parallel [17,18,19,20,21,22,23,24,25], revealing the deep evolutionary homology between these unicellular parasites and the cancer cell system. Currently, Entamoeba represents the most evolutionarily relevant model for cancer, demonstrating that cancer exploits ancient unicellular mechanisms established by the common ancestor of amoebozoans, metazoans, and fungi (AMF).
Numerous studies in evolutionary cancer cell biology (ECCB) over the last decade have demonstrated the deep homology between the native cancer cell system and the life cycle of Entamoeba, both of each share a common AMF ancestor. These cell systems possess a unicellular oxygen-sensitive stemgermline with two distinct phenotypes. One is the asymmetric cell division (ACD) phenotype, which produces committed stem cells. The other is the dysfunctional symmetric cell division (DSCD) phenotype, which have lost its stemness potential and proliferates by defective DSCDs. Additionally, there is a somatic oxygen-resistant cell lineage consisting of numerous subtypes and clones, which play an essential role in maintaining and expanding the genome.
Both cancer and Entamoeba stemgermlines share many characteristics of unicellular life cycle, including (1) sensitivity to oxygen levels exceding 6.0% O₂ ß (germline hyperoxia), (2) the presence of committed stem cells, (3) stemness loss and recovery, (4) hyperpolyploidy, multinucleated giant cells (MGRS, PGCC), and other features. These homologies strongly support the unicellular nature ty of both cell systems and their shared AMF origin.
The two autonomous cell systems - cancer and its evolutionarely model, the parasitic Entamoeba [10,11,12,13] –retain full functionality and stemness in hypoxic niches and tissues with oxygen levels below 5.7–6.0% O₂ but are severely compromised in environments where oxygen levels exceed germline normoxia, (≥ 6.0% O₂). Such hyperoxic germline conditions in tissue and blood flow lead to the loss of DNA repair capabilities via homologous recombination (HR), resulting in irreparable double-strand break (DSB). Both the cancer and protist stemgermlines are vulnerable to oxygen excess, but hyperoxic damage can be mitigated through hyperpolyploidy—a specialized repair mechanism of unicellular cell systems. During this repair process, DSCD cells fuse to form specific unicellular giant repair structures known as multinucleated giant repair structures (MGRS) or, polyploid giant cancer cells (PGCC).
From an evolutionary perspective, committed non-proliferative human stem cells, such as adult stem cells (ASCs), originate from a proliferative stemgermline closely related to the Ur-germline of the common AMF ancestor. Understanding the evolutionary roadmap of cancer is essential to guide future molecular research toward solving long-standing questions in cancer biology.
2.0. Stemgermline Vulnerability to Stress
2.1. Stemgermlines Give Rise to Committed Stem Cells and CSCs
It has long been known that stem cells are in fact germline cells or germline stem cells (GSC) and that the hidden, little-known non-gametogenic NG stemgermline functions as a „proliferative stem cell line” in tissues and organs, giving rise to self –renewing cells and committed non-proliferative stem cells (CSCs) capable of differentiation [10]. Even today, this stemgermline is mistakenly referred to as a proliferating stem cell line, although it is clear that stem cells - committed stem cells - cannot proliferate. The stemness potential is manifested by the functional ACD phenotype, which proliferates through asymmetric cell division (ACD), producing self- renewing and committed sister cells. Cells in G0 are not committed stem cells; rather, they are non-committed quiescent cells capable of re-entering the cell cycle. Committed stem cells, which are primed for differentiation, lack the ability to proliferate. However, they can accumulate additional copy cells through polyploidization and hyperpolyploidyzation [10,11,12,13].
2.2. Oxygen Sensitivity of Cancerous and Non-Cancerous Stemgermlines
Stemgermline cells exposed to oxygenic stress switch undergo a shift to defective symmetric cell division (DSCD), which lacks stemness. Some cancer researchers interpret the transition from ACD to DSCD as a shift from stem cell to non-stem cells; however, this is not the case. Notably, true committed stem cells and CSCs do not proliferate. Both ACD (stemness positive) and DSCD (stemness negative) phenotypes are germline phenotypes. Understanding this differentiation within stemgermline cells is crucial for unraveling the evolutionary processes underlying cancer.
Stemgermlines capable of producing stem cells in humans, vertebrates, invertebrates and protists, are all related and can be traced back to AMF Urgermline. They all contain the genes and modules of the ancestral genome, or at least significant parts of it. In the course of evolution, primitive germlines have evolved, but these have often been misclassified as proliferative stem cell lines without taking into account the lack of proliferative capacity of true committed stem cells. [10]
2.3. Aging Stemgermlines; Mitotic Arrest (Senescence) and Apoptosis
In metazoans and humans, stemgermlines, sublines, and clones tend to undergo apoptotic death because the multicellular life has introduced numerous barriers to the restoration of divergent genomes. Unlike protists, they cannot survive or proliferate indefinitely.
Protists do not face such barriers, and surprisingly, some genomically damaged stemgermline cells of multicellular organisms can overcome these constraints and adopt a unicelular fate. What are these cells, and why does this happen? This phenomenon most often occurs in old age when „spent” adult stemgermline cells experience physiological stress, such as germline hyperoxia, which damages their repair genes and impairs their functionality. As a result, these cells arrest the cell cycle, enter mitotic arrest (senescence) and usually undergo apoptotic cell death.
Multicellular organisms lack the mechanisms required for genomically damaged stem cells to repair DNA DSB (double-strand breaks), whereas unicellular systems, such as protist parasites, possess efficient genome repair mechanisms, including hyperpolyploidy. In a recent study, the author of this article [13]. demonstrated that irreparable replicative DSB defects in multicellular stemgermlines can be repaired through an extended DNA damage response (DDR) process, which includes unicellularization and genomic repair via MGRS mechanisms, ultimately restoring a functional genomic architecture within unicellular entities.
2.4. Stressed Stemgermline Cells Capable of MUT and Genome Inversion
How do individual stemgermline cells find the key to MUT rescue after genomic insults? And for what reason?
Following mitotic arrest, some DNA-damaged stem germline cells may find restorative senescence niches and favorable environmental conditions that enable them to bypass apoptotic barriers and prepare for the MUT process. But why do these nearly apoptotic cells overcome the constraints of multicellularity and revert to a unicellular state?
First, the intrinsic cellular drive for survival—an ancient, evolutionarily conserved trait—compels life-threatening cells to seek repair mechanisms and survival opportunities. In this context, the transition from multicellularity to unicellularity represents an escape strategy, allowing cells to circumvent the structural and functional constraints imposed by a multicellular system and adopt an alternative state better suited for repairing severe genomic damage. This shift can be seen as the triumph of cellular autonomy over cooperative multicellularity—an individual’s liberation from the „planned economy” of multicellular regulation and restrictions.
But what are the consequences? A fundamental redefinition of „self” and „non-self” emerges. The newly formed cellular entity, now distinct from its original tissue community, behaves as a separate and autonomous system, potentially acting against the host organism. This mirrors the behavior of parasitic amoebae, illustrating a survival strategy that prioritizes individual persistence over collective homeostasis.
In restorative senescence niches, genomically damaged stemgermline cells encounter hyperoxic conditions similar to those experienced by mitotically arrested Entamoeba in well-oxygenated host tissues. For both multicellular and unicellular stemgermline cells, oxygen levels above 6.0% O₂ are considered hyperoxic (germline hyperoxia) [10,11,12,13]. Restorative senescence niches activate unicellularity-associated genes that drive senescence exit, induce the DSCD phenotype, promote aberrant SCD proliferation, and initiate hyperpolyploidization.
Through these evolutionary mechanisms, dysfunctional genomes could revert to a unicellular genome state (genome inversion). However, this process of Ancestral State Reconstruction ASR repair process. Multicellular genome damage caused by stressors cannot be repaired by genome inversion or subsequent DSCD proliferation. Instead, repair can be achieved through cell fusion and the formation of hyperpolyploid MGRS structures [10,11,12,13].
The author of this work suggests that the MUT overcoming process is the desperate struggle of individual cells driven to death by the barriers and programs of multicellularity. However, some cells take up the fight for survival against the control and free themselves through a kind of „Faust-Mephisto pact”. They are allowed to return to unicellularity, but this fountain of youth is directed against the relatives they betray and expose to carcinogenesis
3.0. Multicellular to Unicellular Transition and Post-MUT Stages - Where Do They Occur?
3.1. Hyperplasia and Dysplasia Are Stages After Unicellularization
Current cancer knowledge fails to recognize that processes such as prolonged metaplasia, hyperplasia, dysplasia, and carcinoma in situ (Figure 1) are stages of an obligatory genome repair pathway. In this process, unicellularized dysfunctional hyperplastic DSCD cells undergo genome reconstruction, restore stemness, and ultimately give rise to CSCs through productive ACD phenotypes. According to current opinion:
Metaplasia is an adaptive, reversible process in which one well-differentiated cell type is replaced by another well-differentiated cell type in response to external stimuli. In most cases, metaplasia can revert to its normal state once the stimulus is removed. However, certain metaplastic conditions may be precancerous. Additionally, if metaplasia persists for a prolonged period without resolution, it can progress to dysplasia, ultimately leading to cancer.
Hyperplasia. In contrast to metaplasia, hyperplasia is an irreversible cell statehallmark of precancerous cellular changes. Pathological hyperplasia often arises from dysregulated cellular processes and can increase the risk of certain cancers. For instance, atypical ductal hyperplasia in the breast is a known risk factor for breast cancer development. The term ’hyperplasia’ broadly refers to the abnormal proliferation of cells within otherwise healthy tissues or organs, such as breast hyperplasia, endometrial hyperplasia, or prostate hyperplasia. However, hyperplasia is not always indicative of malignancy.
Dysplasia. In contrast, anatomic pathologists define dysplasia as epithelial disordered growth characterized by the loss of cellular uniformity and architectural organization, particularly in epithelial tissues. In the past, it was considered a delay in tissue maturation, resulting in the expansion of immature cells while reducing the number and proper localization of mature cells within the tissue. Consequently, dysplasia is regarded as the earliest form of a precancerous lesion, potentially progressing to carcinoma in situ and neoplasia. Neoplasia occurs when the entire epithelium becomes dysplastic.
Carcinoma in situ. Ductal carcinoma in situ (DCIS) as occurring in the lumen of mammary ducts is defined as a premalignant proliferation of neoplastic epithelial cells [26] DCIS are lined by an outer layer of myoepithelial cells and surrounded by an intact basement membrane [27]. DCIS were considered non-malignant lesions and precursors of invasive breast cancer. Numerous older papers have shown their genetic similarity and likely common origin [28,29,30,31].
A common theory of progression is that the normal myoepithelium acts as a ‘gatekeeper’, exerting tumor-suppressive effects on the in-situ lesion, and that it is the loss of this suppressive environment that triggers progression to invasive disease [32,33,34,35]. In addition to forming a physical barrier to invasion, myoepithelial cells also secrete “various ECM components and protease inhibitors, such as maspin, which have been proposed to inhibit the invasive capacity of DCIS in a paracrine manner.“
In contrast, the ECCB framework interprets precancerous conditions such as hyperplasia (the proliferation of a dysfunctional, unicellularized non-hypoxic DSCD cells) and dysplasia (the expansion of a hypoxic stemgermline population) as stages that follow genomic inversion. According to ECCB, hyperplastic overgrowth occurs through defective symmetric proliferation (DSCD phenotype). In contrast, dysplastic subpopulations occurs through progenitors and nascent cancer stemgermline cells, which proliferate asymmetrically (ACD phenotype), ultimately leading to the formation of primary pCSCs and somatic cancer cells within the protective hyperplastic structure.
There is substantial evidence suggesting that the “green“cells in the Figure 1 represent DSCD cells capable of proliferating under conditions of germline hyperoxia, while the “brown“ cells develop hypoxically, giving rise to a transformed unicellular cancer cell system. Both hyperplastic and dysplastic cells represent irreversible phenotypes driven by stress and genetic alterations.

3.2. Dysplasia and Adenocarcinoma Arising from the Gastric Stemgermline
In a recent paper 2022 study, Min et al. [37] reported that both cellular plasticity and the regulatory mechanisms involved in the neoplastic transformation and dysplasia remain largely unknown and poorly understood. According to the authors, gastric dysplasia is the focal neoplastic lesion with the highest risk of developing into intestinal-type gastric cancer [38,39]. It is widely recognized as the initiating event in the neoplastic transformation of precancerous cells into cancer [40].
The researchers identified several populations of dysplastic stem cells (DSCs), such as DP-DSCs and TP-DSCs, which exhibit highly similar molecular profiles. However, only the DP-DSC population demonstrated high dynamic activity and survival capacity, maintaining dysplastic cell lineages. This DP-DSC subpopulation clonally evolves into multiple types of gastric adenocarcinomas. In other words, it is now recognized that de novo stem cells act as the initial triggers of cancer evolution. However, their origin remains unclear to proponents of the multicellular cancer concept and is a widely debated topic within the research community.

Most cancer researchers have not yet recognized that these “de novo stem cells“ are in fact proliferative stemgermline cells. They arise when genomically damaged adult stem cells (ASCs) bypass apoptosis and the constraints of multicellularity. According to the ECCB, they undergo unicellularization (MUT) in restorative senescence niches. After unicellularization, they exit senescence, proliferate as a DSCD phenotype, undergo genomic repair by hyperpolyploidization and finally form the nascent cancer stemline. The stemgermline in turn gives rise to committed primary non-proliferative pCSCs, which are exclusively capable of differentiation [10,13].
4.0. ECCB Opens New Perspectives in Cancer Research
Cancer research today stands at a crossroads between traditional molecular oncology and the emerging field of evolutionary oncology [10,11,12,13,21]. As Arun Upadhay noted in 2020 [41] „Cancer today is still an unknown territory that requires rethinking before moving forward.” This rethinking is increasingly driven by evolutionary ECCB [10,11,12,13], which offers a fresh perspective beyond the molecular oncology framework.
Molecular and evolutionary oncology differ fundamentally in their understanding of the nature and origin of cancer cells. Molecular oncology views cancer cells as divergent multicellular entities that retain their multicellular hallmarks. In the absence of a comprehensive biological model to explain the initial steps and causes of cancer, molecular oncology adopts a retrospective strategy, drawing molecular inferences from final tumors to determine the causes and onset of cancer. In recent years, extensive tumor screenings have been conducted to identify specific common genes, known as driver genes, under the assumption that these genes are responsible for carcinogenic transformation. However, the results, remained modest.
In contrast, evolutionary cancer cell biology ECCB has found a evolutionarely model that essentially corresponds to the cancer cell system. This model comes from parasitic amoebae (Entamoeba), which (i) share the same ancient unicellular cell system as cancer and (ii) similarly to the cancer cell system, exploit the entire range of the oxygen gradients of the host tissues from 0.1% (gut) to approximately 13% O₂ (bloodstream). Both systems utilize oxygen levels as triggers, stressors, and effectors to regulate their behavior.
Cancer and Entamoeba are both autonomous parasitic cell systems [21] and share a deep homology with the unicellular common ancestor of amoebozoans, metazoans and fungi (AMF). They follow the rules of the unicellular cell system, not those of the multicellular host organism. Only the ECCB can truly explain how cancer arises and what it is. This new evolutionary concept will drive cancer research in the future.
Key discoveries in evolutionary oncology and ECCB include (i) the multicellular-to-unicellular transition (MUT) that precedes cancer and (ii) the identification of a low-incidence, stemgermline as the driving force of the cancer cell system. This proliferative, self-renewing germline, which gives rise to cancer stem cells (CSCs) and is also referred to as the cancer germline, was previously misidentified as a proliferating CSC line [10]. The NG germline undergoes transient genomic disruption and phenotypic changes in response to stressors; however, it retains the ability to restore its functional genomic architecture and integrity through evolutionary mechanisms inherent to unicellular life. These repair mechanisms, lost in multicellular systems, remain preserved and reactivatable within the ancestral genome compartment of all metazoans, including humans.
4.1. Hallmarks of Cancer Stemgermlines
The hallmarks of the stemgermline are summarized as follows:
Stemness - ability to generate committed (non-proliferative) CSCs under hypoxic growth conditions (<5.7–6.0% O₂);
Sensitivity to Hyperoxia - vulnerability to oxygen levels above 6.0%, resulting in loss of asymmetric cell division (ACD) and stemness;
Stemness cycles: alternation between hypoxic periods of stemness and hyperoxic periods of stemness loss;
Genomic Stability: ability to repair genomic damage via unicellular, cell cycle-independent repair mechanisms;
DSCD Proliferation: capacity for unrestricted proliferation followed by homotypic cell fusion and repair hyperpolyploidy represent major risk for cancer
MGRS/PGCC genome repair pathway: restoration (reconstruction) of genomic architecture and function.
Phenotype changing: functional transition from ACD- phenotypes to dysfunctional DSCD phenotypes and from GST/MET to SGT/EMT;
4.2. ECCB and the Unicellular Centric View of Cancer
The most relevant difference between classical molecular oncology and the more recent evolutionary ECCB is their mutual perspective: the molecular cancer research adheres to the multicellular-centric view of cancer, while the latter embraces a unicellular-centric paradigm.
This unicellular-focused framework allows oncology to explain cancer not merely as a genetic or molecular aberration through mutations but as the reactivation of ancient unicellular survival strategies embedded within the genome of metazoans. Cancer is a biological anomaly and disease in which an archaic unicellular cell system develops within a multicellular organism and becomes active according to its own rules. It is not subject to regulation by the host organism and cannot be effectively combated by it.
5.0. Cancer Multicellularity Concept Left Many Questions Unanswered
Until now, cancer has been interpreted as an aberrant multicellular system that bypasses multicellular regulatory constraints. The unicellular nature of the cancer cell system, along with its genomically stable stem-germlines and clones, has received little attention and has been largely overlooked in modern cancer research. The perceived genomic chaos and loss of genomic integrity in cancer are consequences of this oversight. Here are some examples of inconsistencies that arise as a result:
5.1. Current Research Does Not Doubt the Multicellularity of the Cancer Cell System
Just a decade ago, the prevailing view was that there is no fixed cancer genome. Instead, cancer was thought to involve a progressive reorganization of multicellularity genes (MGs), which determines and defines the genetic network structure of cancer through a process of genome remodeling. Horne in 2015 [42] noted that the early theories of cancer genome remodeling arose on assumpsions from dedifferentiation and deprogramming processes [42,43,44,45].
Such theories suggested that the genome acts as an „instruction manual,” guiding the assembly of new biological systems. According to this perspective, the genome serves as a blueprint that determines how genes and their encoded products combine to form the structure of new genetic and protein networks
Despite similar gene content, changes in genomic topology could drastically alter gene interaction networks, with significant consequences for cellular function and phenotype. Changes to individual genes could disrupt this organisation, leading to genomic instability and chaos.
Comparison of sequencing data from primary and metastatic tumors with somatic mutation catalogs [46,47] supported an earlier alternative hypothesis that the cancer cell genome is the results from multiple genomic aberrations accumulated throughout the tumor’s developmental history and even earlier [48,49,50,51,52,53]. Additionally, a proposed timeline for tumor development suggests that significant carcinogenic events may occur decades before diagnosis. Overall, it was suggested, that cancer genomes are shaped by a lifelong process of somatic evolution, which blurs the distinction between normal aging processes [54,55] and precanceros evolution.
The evolutionary perspective (ECCB) does not deny that significant carcinogenic events may occur long before diagnosis. However, it interprets these events in terms of DSCD risk following unicellularization. DSCD cells may remain in a quiescent state within specific niches or slowly proliferate over extended periods through defective symmetric proliferation. This process may continue until DSCD proliferation is halted by homotypic agglutination and hyperpolyploidization.
5.2. Current Views on Genome Reprogramming
But how important are dedifferentiation, reprogramming and redifferentiation of multicellularity cells for the development of cancer?
According to Hanahan [56] dedifferentiation converts adult somatic cells into a pluripotent ground state whereas reprogramming or redifferentiation involve the conversion of pluripotent cells into a differentiated cell state. In vitro, dedifferentiation is achieved through the overexpression of four key reprogramming factors: OCT4, SOX2, KLF4, and C-MYC. These factors induce the transformation of a differentiated somatic cell into an induced pluripotent stem cell (iPSC). The subsequent step in reprogramming involves re-differentiating these iPSCs into the desired cell type.
All these processes normally take place within the multicellular cell system and its development. Do they also occur during carcinogenesis? Can iPSCs differentiate into true CSCs? And vice versa? The results were discouraging.
Sveral researchers consider that cancer stem cells (CSCs) share many molecular features with iPSCs. Malignant cells could be successfully reprogrammed into iPSC-like cancer cells (cancer iPSCs) [57] but also normal iPSCs could be transformed into CSC-like cells by genetic manipulation involving tumor microenvironment factors. Some cancer-derived iPSCs have been shown to exhibit reduced malignancy and can differentiate into benign cancer lineages [58,59,60,61,62].
Shamsian et al. in 2022 [63] underline that cancer cells are however, largely resistant to reprogramming due to several biological barriers, including mutations, accumulated DNA damage, epigenetic changes, and the activation of cancer-related genes. Consequently, the reprogramming of cancer cells has been largely unsuccessful in regenerative medicine. While the aforementioned barriers typically permit only partial reprogramming into cancer- iPSCs, even fully reprogrammed iPSCs often revert to the original cancer cell traits over time [64,65].
In short, the outcomes of such studies have not very promising, despite researchers’ hopes of gaining valuable insights into various oncogenic processes to facilitate their modulation.
Attempts at transdifferentiation have also been largely unsuccessful. Transdifferentiation is the process by which differentiated adult somatic cells are directly converted into cells of a different lineage without reverting to a pluripotent state. However, natural transdifferentiation is rare in mammals but it is more common in cancer and protists, where germlines undergo transdifferentiation through GST processes to form somatic cell lines [10,11,12]. According to Graham and Sottoriva [66], transdifferentiation have a lower risk for carcinogenesis compared to reprogramming as it bypasses the intermediate pluripotent state, which is a significant source of tumorigenic potential in iPS cells. Consequently, autologous cells obtained through transdifferentiation do not inherently acquire the ability to self-renew and proliferate uncontrollably as in reprogramming. Nevertheless, the risk of carcinogenesis cannot be entirely ruled out due to potential genetic and epigenetic changes that may occur during the transdifferentiation process.
5.3. Current Opinions on Tumor Suppressors and Oncogenes (Caretakers, Gatekeepers, and Landscapers)
In the absence of solid evolutionary insights and a suitable cell biological model to explain cancer and the cancer stemgermline, the question of what causes uncontrolled somatic outgrowth in multicellular organisms has been debated for years. It was concluded that tumor suppressor genes, often referred to as caretaker genes, must play a critical role in preventing somatic outgrowth and, by extension, tumor development. These genes were believed to produce specific proteins responsible for maintaining genomic stability.
If these genes became defective due to replication errors („mutations”) and lost their functional control, it was thought that the uncontrolled multicellular cell growth would lead to tumor formation. There was a strong belief that mutations in tumor suppressor genes were the primary drivers of cancer. [67].
The distinction between „caretakers” and „gatekeepers” was introduced by Kinzler and Vogelstein [68]. Unlike caretaker genes, which would maintain genomic integrity, gatekeeper genes encode products that actively prevent the growth of potential cancer cells and suppress the accumulation of mutations that directly lead to increased cellular proliferation [69,70]. Gatekeeper genes would directly regulate tumor growth by encoding dual-function proteins that either stimulate or inhibit proliferation, differentiation, or apoptosis in a dose-dependent manner. Key gatekeeper and caretaker genes of significant interest include APC, RB1, CDKN2A, TP53, BRCA genes.
Additionally, Michor et al. [71] introduced the term „landscaper” genes. According to the researchers, landscaper genes encode products that, when “mutated“, would contribute to the neoplastic growth of cells by fostering a stromal environment that is conducive to unregulated cell proliferation.
Caretaker genes would ensure genomic stability by preventing the accumulation and transmission of replication defects (mutations). According to this dogma, the loss of function of mutant caretaker genes allows mutations in other genes to arise and persist, potentially driving the conversion of a normal cell into a neoplastic one. In this concept, caretaker genes do not directly regulate cell proliferation. Instead, they function by slowing the cell division process to allow DNA repair to be completed or by initiating apoptosis to eliminate damaged cells.
This concept also has its limits. Notably, the restoration of a caretaker gene from its mutated form to the wild-type version does not appear to significantly limit tumorigenesis, raising questions about its role in halting or reversing cancer progression.
More recently, oncogenes and tumor suppressor genes are considered genes whose alterations, including intragenic mutations, chromosomal deletions and loss of expression, are involved in tumor processes, including cell cycle progression, differentiation, maintenance of genomic integrity, DNA (deoxyribonucleic acid) damage repair, and even apoptosis. According to Fanale et al. (2017) [72] “inactivation of both genes contributes directly to cancer development and progression.
5.4. Current Views on Genomic Alterations and the Ineffective DNA Damage Response (DDR)
As early as 1976, Nowell [73] proposed that tumor initiation and progression might result from acquired genomic changes within the „original normal cells,” triggered by exogenous DNA damage. These changes, and the accumulation and transmission of replication defects, were later interpreted as evidence of genomic instability, with tumor cell populations appearing to be genetically more unstable and more heterogenous (chaotic) than normal cell populations [74]. From this perspective, it was concluded that cancer cells evade the regulatory control of the multicellular organism. Additionally, their outgrowth proliferation through shorter cell cycles was considered a significant growth advantage. These factors contributed to the development of the concept of genomic instability in cancer and tumors, contrasting with the stable genome of normal multicellular cells. This discrepancy is considered one of the biggest problems in cancer. but is the assumption of cancer genome instability correct?
DNA damage, if left unchecked, is associated with an increased risk of tumor development. To counteract this, cells have evolved several conserved pathways that respond to such errors by initiating DNA repair processes or apoptosis. The process of DNA repair is tightly linked to the DNA damage response (DDR), which involves the recruitment and localization of DNA damage sensors, mediators, transducers, and effector proteins to distinct nuclear foci. [75]
There is still confusion about the genomic stability and instability of the cancer stemgermline (proliferative CSC line). However, several older hypotheses explain the driving force behind tumour initiation and progression through the emergence of a “mutator phenotype“. These phenotypes would result from the loss of gene function due to DNA replication stress [76,77,78]. Mutator phenotypes have been observed in the early stages of tumour progression and are the result of changes in genes that normally maintain genomic stability in multicellular organisms. The ECCB finds such earlier considerations enlightening.
Overall, current cancer research indicates that the transformation of a normal cell into a malignant one is driven by genetic, epigenetic, transcriptomic, and metabolic alterations. However, the predominant focus on genetic, genomic, and mutational studies - along with the century-old dogma of cancer as a purely multicellular phenomenon - has yielded limited success. This approach has often led to disappointing statements, leaving many aspects unclear or unresolved, which remains a significant challenge.
5.5. The Dogma of Reversible Cancer Cell Plasticity
A recent study by Warrier et al. in 2023 [79] provides a compelling illustration of this issue. The researchers outline three models of tumor heterogeneity: the clonal evolution model, the cancer stem cell (CSC) model, and the reversible cellular plasticity model. The first two models aim to explain tumor initiation, maintenance, progression, and origin [80], while the plasticity model proposes a unified framework that integrates elements of both other proposals.
The reversible cellular plasticity model focuses on the reversibility of cancer stem cells, which, according to ECCB, are irreversible committed CSCs that can not proliferate mitotically or transform back a proliferative self-renewing stemgermline cell. According to the ECCB, only stemgermline cells exhibit proliferative ACD capacities. Furthermore, the reversible cellular plasticity model does not acknowledge that similar processes — including the formation, maintenance, and progression of intra-tumoral stem cells (stemgermlines/clones) — also apply to pre-carcinogenic stages and arise from MUT and unicellular genome inversion.
The cancer cell hallmarks - including „CSC and non-CSC, differentiated and stem-like, asymmetrically and symmetrically divided, quiescent and proliferative cells, and epithelial and mesenchymal reversible transition”- are presented by Warrier et al. [79] in an almost tabular format, without addressing the contextual and environmental conditions in which they occur. The specific purposes of these transitions are not individually discussed, nor is it acknowledged that not all plasticity processes are directly reversible. However, according to the modern ECCB, most reversibilities are systemic, follow complex pathways, and involve multiple indirect reversibility pathways (cycles) For example:
(1) According to the ECCB, the reversible conversion of committed CSCs into self-renewing stemgermline cells (Warrier’s “CSC plasticity“) does not occur. Only quiescent, mitotically arrested stemgermline cells (non-committed CSCs) have this capacity. Furthermore, when the ACD phenotype converts into the DSCD phenotype, the functional stemgermline cell, which is capable of producing committed CSCs, loses its functionality. This transition is irreversible: the dysfunctional DSCD phenotype (“non-CSC“) represents an intermediate cell state devoid of stemness capacity. It is part of a unidirectional, long-lasting stemness recovery cycle and cannot revert into a functional stem-germline cell (contrary to Warrier’s “non-stem cell plasticity” concept).
(2) The epithelial-mesenchymal transition (EMT) is an irreversible soma-to-germ transition (SGT). Its primary function is to compensate for the loss of functional ACD stemgermline phenotypes and CSC within short-term recovery cycles. Newly formed functional stemgermline clones can subsequently generate somatic cell lineages through germ-to-soma transition GST. While these somatic lineages cannot produce CSCs, they can generate new functional ACD clones, which, in turn, can give rise to new CSCs.
5.6. Calling for Non-Genetic Research
Numerous mutations found in healthy tissues exposed to carcinogens challenge the interpretation that cancer often arises solely from premalignant clonal outgrowths. As recently reviewed by Nam et al. in 2022 [81], somatic mutations observed in clonal outgrowths sometimes regress or overlap with recurrent cancer driver mutations [82,83,84,85,86,87]. This suggests that genetic mechanisms alone may not be sufficient to induce malignant transformation [88].
According to Nam et al. [81] as malignant populations expand, cells undergo further genetic diversification, driving tumour progression, relapse and resistance to therapy [89]. This concept led to the assumption that integrating multiple layers of information from individual cancer cells using single-cell multi-omics would be essential for a comprehensive understanding of cancer evolution. However, clear genetic factors associated with cancer progression, metastasis and therapy resistance have been identified in only a limited number of tumors, further suggesting the significant involvement of non-genetic factors. Genetic mechanisms alone may not fully capture the complexity of intratumoural heterogeneity.
6.0. Early Findings About the Unicellular Nature of Cancer
The first consequential evolutionary concepts emerged at the end of the first decade of the present century when Pepper et al. in 2009 [90] thought that cancer involves complex evolutionary processes. He regards neoplastic progression as a process of somatic evolution through cell cycle arrest and senescence.
Regarding CSCs, the researcher adopted the prevailing view—still widely accepted today—that CSCs are proliferative, a notion contradicted by the ECCB. Moreover, the claim that CSC proliferation serves “to produce more CSCs“ is doubly incorrect. According to the ECCB, more daughter cells can only be produced through accumulative SCD cycling, and only by the stemgermline. However, the SCD progeny of the stem-germline is dysfunctional and consists of DSCD cells, which lack stemness potential and cannot generate additional stem cells.
In 2010, Mark D. Vincent [91] published a paper on cancer speciation, a topic that was becoming fashionable at the time. Vincent addresses the somewhat older „“cancer as species“ thesis. He refers to Huxley 1956 [92] supposition, which proposed teht “once the neoplastic process has crossed the threshold of autonomy, the resultant tumor can be logically regarded as a new biologic species” a view largely shared by Greaves [93], Swanton [94] and Duesberg and Rasnick [95]. In contrast, Vincent considers tumor cell heterogeneity a real obstacle to the cancer species concept and also questions how much certainty exists that cancer cells are indeed genetically heterogeneous.
For the time, it was unconventional; Vincent [91] mentions cancer as a separate cell system that lives off the host in a manner smilar to destructive parasites, as described by Merlo et al. (2006) [96]. They view cancer cells as a colony of loosely cooperating yet often competing and independently evolving individual cells - or, at worst, a collection of unicellular eukaryotic organisms that are fully capable of existing independently of each other.
Notably, as early as 2004 Gray et al. [97] and Rivera and Lake [98] saw cancer cells as exhibiting colonial attributes, with host organisms “literally being eaten inside out by a very primitive type of animal“, primitive in the sense of being minimized due to secondary losses of characteristics.
Very bold for this time - when no suitable evolutionarily development and the evolution of multicellularity are not just opposite processes, but rather the result of bidirectional traffic on the same two-way street. One prediction would be that a similar set of genes may be involved, and that elucidating one of these phenomena may automatically provide mechanistic insights into the other. Vincent believed that the correspondence between the cellular mediators of multicellularity and those that “fail” during carcinogenesis strongly supports the notion that these two apparently disparate phenomena are actually on the same continuum.
In 2011, Vincent [99] believed that cancer represents the de-repression of a default survival program inherent to all eukaryotic cells. He suggests that cancer arises from the reactivation of an ancestral program that prioritizes cellular survival above all else. To describe this phenomenon, he introduced the term „adaptive resilience,” referring to an „any-cost cellular survivalism” that is independent of identity and cell origin. The author characterizes cancer cells as a protozoan-like population with evolutionary roots in the Precambrian era. He argues that through the deconstruction of the metazoan phenotype, these cells acquire autonomous, parasitic traits, ultimately becoming entities that, while residing within the body, are no longer truly part of it.
Nevertheless, when molecular cancer research was gaining momentum, such evolutionary perspectives were met with little enthusiasm in the cancer research community and were often regarded as unconventional. However, over the past three to four years, the ECCB has thoroughly validated Vincent’s earlier position, confirming its accuracy.
In the second decade of this century, evolutionary researchers such as Domazet-Lošo and Tautz [100,101], Trigos [102,103,104] and Lineweaver and Davis [105] extend these ideas and find evidence that in cancer, young multicellular genes (MGs) are downregulated and older unicellular genes (UGs) are upregulated. They proposed that tumor growth follows a branching evolutionary pattern, tracing back to a common ancestor from which cancer cell subclones with different fitness diverge and proliferate, supporting the idea that key features of cancer arise from the disruption of molecular networks that originally evolved during the transition to multicellularity.
In a recent review article, Rebolleda-Gomez and Travisano in 2018 [106] investigated whether ancestral unicellular wild forms capable of developing multicellular phenotypes could revert from multicellularity to unicellularity. They found that environmental changes and constant agitation of Saccaromyces cerevisiae cultures could induce multicellular structures really to revert to a unicellular state and demonstrate that the reversible switch from unicellularity to multicellularity and vice versa is still possible today.
Although the transition to multicellularity is believed to be evolutionarily stabilized by traits that prevent unicellular reversion [107,108,109,110] – this is not the case. MUT events provided a clear survival advantage in the evolutionary past and in cancer. Reverting cells evolved into independent populations with evident reproductive benefits. The ability to undergo genomic inversion was a key determinant of UMT/MUT reversibility [111].
The aforementioned researchers recognized that the unicellularized cancer cell system exists within the host body but is no longer an integrated part of it. They provided valuable insights, particularly the idea that this system resembles a protozoan-like population with evolutionary roots in the Precambrian, capable of mimicking processes associated with the transition to multicellularity (UMT).
However, only ECCB research - leveraging the deep homology between the unicellular cancer cell system and the Entamoeba model - has been able to clarify the organization and development of the cancer cell system [10,11,12,13]. ECCB studies have demonstrated that MUT processes begin even in non-cancerous individuals, specifically in dysfunctional stem cells with severe DNA DSB that cannot be repaired by multicellular mechanisms. The primary function of MUT is to eliminate irreparable DSB damage, which can no longer be resolved within a multicellular framework. Evolutionary genome inversion facilitates hyperpolyploid MGRS repair.
MUT processes occur within restorative senescence niches. However, neither MUT nor subsequent DSCD proliferation restores genomic- integrity. Furthermore, MUT-derived DSCD cells are not yet cancerous. This transformation occurs only when DSCD cells fuse into hyperpolyploid MGRS/PGCC structures, characterized by giant nuclei with multiple genome copies. These hyperpolyploid giant nuclei eliminate the DSB-damage reduce the nuclear mass into numerous haploid buds. These buds serve as precursors genomic integrity and stemness, forming the nascent stem-germline and establishing the autonomous unicellular cancer cell system.
7.0. ECCB Insights into Tumor Development: Oxygen Gradients and the Effect of Hypo- and Hyperoxia
7.1. Genome Dysfunctionality and Genome Reconstruction
Unicellular cell systems, such as parasitic amoebae and unicellular cancer cell populations, possess the ability to survive across the full oxygen gradient within their host organisms. They can thrive in both hypoxic conditions (≤ 6.0% O₂) and hyperoxic environments (> 6.0% O₂), the latter of which exerts a damaging effect on the stemgermline. The normoxic-physiological range consists of mild, decreasing degrees of hypoxia, within which the stemgermline develops its ACD phenotype, giving rise to committed CSCs.
In hyperoxic regions, the germline genome sustains DNA DSB and damage to repair genes, leading to a shift from the ACD phenotype to a dysfunctional DSCD phenotype, which no longer produces committed CSCs. However, unicellular cell systems possess intrinsic repair mechanisms that recover genomic integrity. These mechanisms include homotypic cell fusion, hyperploidization and giant MGRSs/PGCCs, which can restore the ACD phenotype and generate primary pCSCs.
Additionally, new productive stemgermlines can emerge through soma-to-germ transition (SGT/EMT pathway). This process can originate from either homotypic somatic cancer cell lines or syncytia formed with non-cancerous cells. All repair and quiescence processes are regulated by specific stimuli and inducers from the tumor microenvironment, particularly oxygen supply, which governs the unicellular life cycles of both cancer and amoebae.
As illustrated in Figure 1, dysplastic structures progressively consume oxygen from the periphery toward the center. At the periphery, a discontinuous layer of epithelial cells, proliferating under germline hyperoxia (≥6.0% O₂), permits hyperplastic DSCD expansion. These cells consume oxygen, creating hypoxic conditions in the inner tumor regions, which in turn support dysplastic transition and ACD-driven growth. Both tumor layers grow simultaneously, influenced by varying oxygen levels and microenvironmental stimuli.
7.2. The Duality of Angiogenesis: Contradictory Effects, Stemness Cycles and Negative CSC Periods
On the other hand, hypoxic ACD proliferation reduces the intra-tumoral oxygen level. The resulting state of intra-tumoral hypoxia— which slows ACD growth to the point of quiescence and temporarily halts pCSC production—creates a demand for additional oxygen. In response, angiogenic signals emanate from the tumor core, reaching the blood vessels and initiating the directed growth of angiogenic blood vessels toward the tumor [112] (Figure 2).
The supply, consumption, and depletion of oxygen within the tumor maintains a continuous intra-tumoral stemness cycle, facilitating transitions between DSCD and ACD phenotypes, stemness recovery and CSC regeneration.
Some oxygen-sensitive, stemness (+) ACD cells near these blood vessels receive excessive oxygen exposure. As a result, they experience DNA DSB defects and repair gene malfunctions, leading to a shift toward the dysfunctional, oxygen-resistant, stemness (-) DSCD phenotype, which no longer produces pCSCs. To counteract the CSC loss, these cells activate the MGRS/PGCC reconstruction pathway to generate new functional stemgermlines, sublines, or clones that continue pCSC production (Figure 3). A second pathway for germline genome regeneration is the SGT/EMT transition process initiated from homotypic somatic cancer cells that are oxygen resistant and preserve the integrity and functionality of the germline genome.
7.3. The UMT-like Evolution of Cancer: Lateral Gene Transfer and Genome Expansion
The molecular processes driving to genomic expansion are based on ancient gene hijacking mechanisms (lateral gene transfer) dating back to the transition period to multicellularity. It can be assumed that during the early UMT period, the common AMF ancestor expanded its genome through heterotypic cell fusions with genomically distinct competitors. Functionally advantageous genes were retained, while non-beneficial ones were eliminated or repurposed.
Foreign gene hijacking serves as a mechanism for expanding genomic expression and functionality within the cancer cell system. This process likely enhances invasiveness and pathogenicity in evolutionarily related parasitic amoebae while also contributing to the emergence of new strains.
7.3.1. The Hijacked Genes Are Multicellularity Genes
Through conserved mechanisms from the transition period, a large number of hybrid genomes can be formed in primary tumors. Such heterosyncytia arise from the heterotypic fusion of unicellular somatic cancer cells with multicellular somatic host cells. Notably, many host macrophages undergo heterotypic fusions with cancer cells. It is hypothesized that some of these UG/MG hybrids remain non-proliferative, while others become proliferative and accumulate DNA replication defects (mutations).
As previously described, when stemgermlines lose their stemness and cease producing pCSCs, they send distress signals to their environment. These signals reach not only homotypic somatic cancer cells - genomically identical to the dysfunctional stemgermline - but also proliferative and non-proliferative hybrid UG/MG cells that arise from heterotypic fusion with multicellular host cells and also contain multicellular host genes (MGs). In response to loss-of-stemness signaling, hybrid cells are also integrated into SGT/EMT processes, leading to the formation of secondary stemgermlines clones, and secondary sCSCs.
7.3.2. Intratumoral Heterogeneity (ITH) Is Due to the Phenotypic and Genomic Heterogeneity of the Stemgermline Population
Each newly formed secondary germline clone differs genomically and phenotypically previous formed clones, which arise through fractal or non-fractal SGT/EMT processes [12,13]. Functional clones and sublines derived from heterosyncytia exhibit distinct proliferative capacities, forming secondary sCSC pools of varying sizes and potency. Additionally, their genomes may contain genes or gene modules associated with tissue-specific and teratoma-like profiles.
Each new ACD clone and subline arising from heterotypic syncytia is oxygen-sensitive and susceptible to intra-tumoral oxygen fluctuations. In response to elevated oxygen levels, these cells cease sCSC production and transition into sDSCD cells, which can either activate the MGRS/PGCC repair program or stimulate further SGT/EMT processes with other heterosyncytia. Through numerous lateral gene transfer events, both the MGRS/PGCC and SGT/EMT processes give rise to new stem-germline clones and sublines with expanded genomes and enhanced invasive potential. This explains how the primary tumor generates secondary stemgermline clones capable of invading additional hypoxic niches and forming metastases (Figure 4, B).
The cancer-specific genomic expansions described here are rooted in evolutionary mechanisms, during transitional periods. Historically, similar genomic acquisitions occurred when the common AMF ancestor repeatedly accessed genes from genomically distinct competitors, facilitating its evolution toward multicellularity.
It is conceivable that ITH, following fractal SGT/EMT processes, generates both to functional M-cell fractions —incorporating multicellular genes—and E-fractions, which remain dysfunctional and fail to establish new productive stemgermline clones [12,13].
All functional secondary clones responsible for sCSC production maintain genomic stability and preserve their integrity. If one were to refer to genomic chaos or instability, it would apply solely to the numerous somatic cancer cell lines and sublines, which accumulate irreparable replication defects (mutations), rather than to the bouquet of stable stem-germline clones.
At the end of the primary tumor evolution, multiple stemgermline cells of varying invasive potential (different sublines and clones) leave the primary tumor structure (Figure 4) and are exposed to unfavorable environmental conditions (germline hyperoxia). These stemgermline cells exhibit optimal survival when migrating in clusters with oxygen-resistant cells, which enhance their viability and functionality under hypoxic conditions. The most favorable hypoxic niches for metastatic colonization are found in the bones, where metastases preferentially develop.
8.0. ECCB Statements on Migrating Tumor Cells; Metastasis and Bone Metastasis
The ECCB framework provides explanations for several unresolved aspects of metastasis, including the properties, origin, physiology, and fate of metastatic cells. These can all be explained by evolutionary processes that can be traced back to the common ancestor of amoebae, metazoans, and fungi (AMF ancestor). This perspective challenges many assumptions of the current mutation theory of metastasis.
In primary tumor sites, cancer cells typically adhere closely to one another and to the extracellular matrix. When these cells detach from the primary tumor, they can enter the peripheral blood system as circulating tumor cells (CTCs). However, only a subset of these CTCs possesses the ability to adapt to new environments, enabling them to survive, spread, and establish pre-metastasis sites or metastases [113,114].
8.1. CTCs Are Cells of Stemgermline Origin
Circulating tumor cells (CTCs) is a collective term first introduced by Ashworth in 1869 [115]. It refers to all types of cancer cells that leave the primary tumor and migrate through peripheral blood vessels and the bloodstream to secondary sites in various organs [116,117,118,119].
CTCs can exhibit epithelial, mesenchymal, or hybrid phenotypes. Although the majority of CTCs are eliminated by the host immune system, a subset possesses high metastatic potential and can evade immune surveillance, leading to the formation of microscopic cancer foci, tumor recurrence, and metastasis. Notably, these immune-resistant cancer cells often exhibit stem-like properties and are sensitive to the hyperoxic germline values (≥6.0% O₂) found in the bloodstream and peripheral tissues [120].
8.1. Intrinsic Properties of CTCs
According to Gao et al. [121], only a limited number of disseminated tumor cells are capable of forming metastatic tumors. This capacity depends on both the intrinsic properties of CTCs and external regulatory factors. Previous studies by Lambert et al. [122] and Liu and Cao [123] highlighted genotypic and phenotypic characteristics as key determinants of CTC survival, invasion and metastatic efficiency. Gao et al. [121] also refer to the “temporal/spatial secrets” of metastatic tumor cells, proposing that “transient and bidirectional CSC differentiation occurs, which is strongly influenced by microenvironmental factors”. In other words, it is the plasticity of CSCs and their dynamic phenotypic transitions that fundamentally shape tumor progression and metastasis. Intermediate phenotypes have been described, though only in the context of fractal SGT/EMT processes.
In the authors’ view, “metastatic cells inherit critical driver mutations from their parental tumors allowing the persistence of tumorigenic ability and on the other hand, metastatic cells develop new mutations to adapt to emerging challenges during metastasis”. However, this perspective, formulated several years ago, does not take into account the current ECCB understanding that transient and bidirectional CTC evolution actually involves cycles of stem cell loss and recovery. CTC and metastasis processes involve a switch from the functional state of asymmetric cell division (ACD phenotype) to the dysfunctional, CSC-negative DSCD phenotype under oxygen stress. Furthermore, the restoration of stemgermline functionality and genomic integrity occurs exclusively through the MGRS/PGCC repair pathway. In contrast, SGT/EMT processes aim to replace the damaged, CSC-deficient stem germline with new, functional stem germline clones that can resume ACD-driven proliferation and generate committed CSCs.
Additionally, this statement—as with many others concerning the multicellularity of cancer—suffers from a conceptual conflation of the stemgermline, its clones, and sublines with a non-existent, proliferative CSC lineage and the notion of CSC plasticity. According to the ECCB, CSCs are committed stem cells that neither proliferate mitotically nor exhibit plasticity. Only undifferentiated, self-renewing stem cells possess these capacities. The ECCB further posits that the explanation involving inherited driver mutations and newly acquired metastatic mutations is superfluous. It argues that only the ancestral mechanisms of the unicellular cancer cell cycle govern CTC behavior during migration, invasion, and metastasis.

8.2. Migrating CTC Cluster Escapes Hyperoxic Damage
Cancer cells can detach from the primary tumor either as multicellular aggregates or as single cells that subsequently form heterotypic clusters within the peripheral blood circulation [124]. These CTC clusters arise through the aggregation of varying numbers of cells mediated by intercellular adhesion molecules [125]. Both the size and number of CTC clusters have been shown to correlate significantly with metastatic potential and clinical outcomes [126,127].
CTCs clusters that survive in the bloodstream are capable of initiating metastases. The prevailing view is that clustered CTCs exhibit a higher metastatic potential compared to single CTCs. Upon entering the circulation, tumor cells lose the protective hypoxic microenvironment of the primary tumor. Consequently, only those CTCs that can adapt to the hyperoxic conditions of the circulatory system are able to survive, disseminate to distant tissues, and ultimately form metastases [113]. According to Chen et al. [114] additional challenges in peripheral blood further threaten CTC survival. These include attacks by the host immune system and exposure to apoptotic signals, both of which limit the ability of migrating cancer cells to persist and colonize secondary sites.
Metastasis is a multistage process involving several intermediate steps. During this progression, CTC and must adapt to the unfamiliar hyperoxic environment of the bloodstream and distant tissues in order to survive, colonize, and ultimately form secondary tumor lesions. Aggregation and clustering is the response of stemgermline cells and CTCs to an oxygen gradient ranges above 6.0%.
8.3. The Advantage of Collective Migration
As revealed by Chen et al. [114], only those CTCs capable of adapting to the new microenvironment are able to successfully disseminate and establish metastatic lesions. Notably, CTC clusters are 50–100 times more likely to facilitate metastasis than individual CTCs [128,129,130]. As cancer progresses, the number of detectable CTC clusters increases, suggesting a strong association between cluster formation and metastatic progression [131]. This implies that CTC clusters possess significant advantages over single CTCs during migration and invasion.
This advantage lies in the formation of hypoxic–normoxic gradients within the CTC cluster, along with a protective outer layer of surface cells that shields the oxygen-sensitive stem germline cells at the core. This protective architecture enables the stemgermline to maintain and recover stemness and ACD potential, thereby allowing the generation of sufficient numbers of non-proliferative, committed CSCs. The oxygen-buffering and immunosuppressive microenvironment within the cluster [132] facilitates the continued progression of the unicellular cancer cell system by preserving the genomic integrity and functionality of the stemgermline, clones and subclones.
8.4. Homotypic and Heterotypic CTC Clusters
As cancer cells travel through the bloodstream, they are exposed to a variety of external stresses until they reach distant organs [133]. The collective migration of hyperoxia-protected clusters has been identified as a key mechanism of invasion, whereas the migration of single, unprotected cancer cells appears to be largely ineffective or absent [134].
In recent years, it was observed that CTCs can also aggregate heterotypically with non-tumor cells, including neutrophils, platelets, myeloid cells, cancer-associated fibroblasts (CAFs), and tumor-associated macrophages (TAMs) [120]. These heterotypic associations are widely believed to provide CTCs with enhanced protection against the hostile conditions of the circulatory system, enabling them to evade immune attack, resist shear stress, and survive transit. Ultimately, such interactions facilitate the successful establishment of metastatic lesions at distant sites. Heterotypic clusters show greater metastatic capability compared to homotypic clusters [135].
Gu et al. [120] discussed recently the role of adhesion proteins in homotypic clustering and showed that tumor hypoxia can upregulate genes that produce such adhesion proteins [136] and improve overexpression of stem-like traits [137,138], survival and self-renewal ability.
The ECCB suggests that homotypic clustering may be an ancient evolutionary adhesion mechanism, also observed in amoebae. In Entamoeba, homotypic cell clustering leads to cluster hypoxia, a condition essential for initiating the generation of replacement stemgermlines, through processes such as soma-to-genome transition and polyploidization/depolyploidization cycles [24]. Ultimately, this sequence gives rise to progenitor cells capable of producing new stemgermline, sublines and clones. In this way, the unicellular cell system resolves DSCD dysfunction and recovers new ACD clones and sublines capable of generating new committed, non-proliferative stem cells.
8.5. Fractal EMT Phenotypes and Polyclonal Dissemination
Recent studies reveal that the progression of cancer from the primary tumor to metastasis involves polyclonal dissemination and polyclonal transfer, characterized by individual traits related to growth [139]. Fractal EMT/SGT phenotypes play an important role in this process. Studies have shown that weakly migrating subsets tend to be more epithelial (E) [140], and thus more somatic in nature, whereas strongly migrating subsets are more mesenchymal (M) and exhibit more stemness-like characteristics. Many CTC clusters display a partial EMT phenotype [141], with some cells within the cluster acting as “leaders” (initiating migration) and others as “followers.” The alternation between mesenchymal “M-leader” phenotypes and epithelial E-followers is considered particularly advantageous for tumor progression [142,143]. This phenotypic M- and E-clonal diversity enables cells to more effectively adapt to changes in the tumor microenvironment cancer, thereby promoting tumor progression [144].
8.6. Bone Metastases
Nearly all types of cancer have the potential to spread (metastasize) to the bones. However, certain cancers, such as breast and prostate cancer, are particularly prone to bone metastasis. Among various metastatic sites, bone is the most frequent target for tumors originating in the breast and prostate. Tumor cells can escape from the primary site and colonize hypoxic bone niches [145].
Depending on the degree of hypoxia within the bone niche, disseminated tumor cells—including those associated with multiple myeloma—may enter a state of dormancy, remaining quiescent for years before reactivating. Upon resuming proliferation, these cells contribute to overt metastasis, leading to bone destruction through osteoclast-mediated osteolysis [146].
9.0. The Genomic Stability (GS) of Stemgermlineages vs. The Dogma of Genomic Instability (GI)
The concept of genomic instability (GI) stems from the dogma that cancer are purely multicellular. Current cancer research often compares the multicellular genome of non-cancerous host cells genome with the unicellular genome of cancer cells, revealing significant differences—which are not surprising from an ECCB perspective. Secondly, GI was introduced as hallmark of the entire cancer population without distinguishing between stem and non-stem cells. According to the researcher, GI refers to an increased tendency for genomic alterations during the cell cycle. It was then defined as an abnormally high frequency of errors that may occur in one or both symmetric daughter cells.
In 2011, Zhiyuan Shen [147] identified GI as the main driving force of tumorigenesis. According to this concept, the accumulation of genomic alterations - through mutations at specific genes, amplifications, deletions or rearrangements of chromosome segments - can lead to dysregulated cell division and imbalanced growth, eventually resulting in cancer. In contrast, non-cancerous cells are characterized by genomic stability (GS) which is maintained through high fidelity DNA replication in S phase, error-free repair of sporadic DNA, and tightly regulated cell cycle progression with checkpoint control.
This view remained dominant and has expanded year by year. In 1991, Loeb [76,77] proposed that an early step in tumor progression is the emergence of a mutator phenotype resulting from mutations in genes normally responsible for maintaining genetic stability. At that time, it was believed that the loss of such genes could lead to GI and thus promote cancer development. Consequently, the prevailing assumption was that the functional differences between healthy multicellularity and dysfunctional cancer multicellularity could only be explained by mutations, genomic instability, and chaos.
Many researchers supported this perspective. Yao and Dai in 2014 [73] recognized a heightened tendency for genome alteration during cancer cell division, attributing this to defects in surveillance mechanisms such as DNA damage checkpoints, repair systems, and mitotic checkpoints. They concluded that the malfunction these multicellular regulatory mechanisms predisposes cells to malignant transformation. Unfortunately, the authors do not acknowledge that the transformation of the dysfunctional multicellular unit is actually a MUT process.
In this vein, Salmaninejad et al. (2021) [148] linked aberrations in DNA repair mechanisms with GI and mutation, identifying the activation of oncogenes and/or inactivation of tumor suppressor genes as major consequences of this instability. This is why GI genomic instability is frequently considered a critical factor in carcinogenesis and a defining feature of many human malignancies.
Chen et al. (2022) [149] pointed out that GI results from various genomic alterations, including germline or somatic defects in DNA repair [130], oncogene-induced replication stress [150], defective mitotic chromosome segregation [151], and other genomic impairments [152]. They emphasize that cancer-associated GI is driven by multiple processes that regulate DNA replication and repair, including the formation of micronuclei due to defective DNA repair [153].
8.1. Genomic Stability and GS Maintenance in the Nascent Stemgermline
Today, however, thanks to ECCB, we understand that the unicellular cancer cell system—like all other related unicellular cell systems—has two mechanisms for generating genomically identical sublines and clones, with the nascent (primary) stemgermline. One is the MGRS/PGCC genome repair pathway; the other is the homotypic SGT/EMT pathway, which ensues the formation of additional clones and sublines of the same genomic identitiy. Both mechanisms restore the previously intact genomic state that was lost in the irreversible affected stemgermline due to stress and hyperoxia. The newly formed replacement stemgermline has the same genome—this time fully intact. The system is therefore highly stable, not chaotic.
Thus, the previous assumption of instability and loss of genomic integrity is incorrect—at least for the overweight stemgermline (1–2% of tumor cells), which regulates cell fate in the remaining tumor cell population. Nevertheless, this new and still emerging understanding of ECCB has not yet been widely recognized. We continue to speak of genomic instability, loss of integrity, and chaos
8.2. Heterotypic SGT/EMTs, Expanded Cancer Genome, and Genomic Stability (GS) in Multiple Secondary Stemgermlineage
According to the ECCB, the cancer and tumor cell system operates as a dual unicellular system, comprising two distinct lineages: (i) genomically stable stemgermlines, which include multiple sublines and clones (stemgermlineage) capable of repairing genomic defects and maintaining GS in all stemgermlines formed through heterotypic SGT from hybrid UG/MG cells, and (ii) secondary somatic cell lineages derived from these stemgermlines, which accumulate replicative DNA damage (mutations) due to their higher proliferative activity. Secondary and primary (nascent) cancer stemgermlines are both repaired by the same MGRS/PGCCs repair pathway
8.3. The Genomic Integrity of Committed pCSCs and sCSCs and Accumulation of Progenitor Cells
For years, the stemgermline has been mistakenly viewed as a proliferative CSC lineage. In reality, „proliferative CSCs” are self-renewing stem cells, while „committed CSCs” are differentiated and non-proliferative. As long as the two synergistic cell types were not analyzed separately, a comprehensive understanding of cancer plasticity, carcinogenesis, and tumorigenesis remained elusive.
Due to this confusion, conventional multicellular cancer research has failed to resolve key questions about the origin of CSCs. Their definition remains ambiguous and is still based on the foundational assumption by Bonnet and Dick in 1997 [154], who proposed that CSCs are both proliferative and capable of differentiation. CSCs were also believed to exhibit phenotypic plasticity, enabling them to adapt to the tumor microenvironment and contribute to the genetic heterogeneity of tumors [155,156,157].
According to the ECCB, committed pCSCs and sCSCs are non-proliferative and only capable of differentiation. Only the stemgermline is proliferative, giving rise to committed CSCs. pCSCs and sCSCs are genomically identical to their corresponding primary and secondary stemgermlines that generated them. The heterogeny observed in the CSC population reflects the heterogeny within in the stemgermlineage of cancer, which include various genomically stable stemgermlines, sublines and clones. CSC evolution is essentially the evolution of the genomically expanding stemgermlines.
Non proliferative CSC populations can accumulate stemgermline progenitors with identical genome structure through a unicellular process of cyst- like differentiation and polyploidization-depolyploidization (non-mitotic accumulation), thereby forming homotypic stemgermline clones and sublines. This represents the third mechanism by which the unicellular tumor cell system expands its homotypic stemgermlineages [10].
Conclusions
Despite the significant efforts devoted to cancer research in recent years, many researchers argue that substantial gaps in knowledge persist, and fundamental questions regarding cancer and the origin of cancer stem cells remain unanswered. A striking contradiction exists between the vast amount of detailed molecular data available and the unresolved fundamental questions to cancer development. The emerging field of evolutionary cancer cell biology (ECCB) aims to bridge this gap and provide greater clarity.
For years, cancer research has lacked a suitable model to explain the complexity of the cancer cell system. Such an evolutionary model can be found in the protist world—specifically, parasitic amoebae that infect humans and other vertebrates. Parasitic amoebae inhabit similar microenvironments as cancer cells, thriving in hypoxic niches where they evade excess oxygen (germline hyperoxia) in the bloodstream and tissues.
The challenges and confusion in cancer research to date stem from a fundamental misinterpretation of cancer. The vast majority of cancer researchers have assumed—and continue to assume—that the cancer cell system is a multicellular system that, upon the disruption of control and surveillance genes, descends into organizational chaos. This disruption is believed to ultimately result in genomic instability and the loss of multicellular genome integrity.
This view has persisted for years, largely due to the lack of evolutionary perspectives in cancer cell research. It was only with the emergence of Evolutionary Cancer Cell Biology (ECCB) that it became clear the cancer cell system does not function as a multicellular system.
According to ECCB, when multicellular cells experience DNA double-strand breaks—whether from intrinsic or extrinsic factors—they are unable to fully reverse the damage. Instead, they resort to an evolutionary mechanism from the transition to multicellularity, known as the unicellular genome inversion or multicellular-to-unicellular transition (MUT). This mechanism rescues and reconstitutes a stable, functional unicellular genome architecture, equipping the cell to make more effective attempts at re-establishing a primitive multicellularity.
The lack of understanding genome inversion has led molecular cancer researchers to compare the characteristics of the unicellularized cancer genome with those of the original (healthy) multicellular genome. Such comparisons inevitably reveal a variety of divergences that are, however, not mutations.
Evolutionary Cancer Cell Biology (ECCB) reveals that cancer follows a lineage duality of ancestral origin. This includes an oxygen-sensitive stemgermline capable of generating committed cancer stem cells (CSCs) and a somatic, oxygen-resistant line that does not generate CSCs but maintains genomic integrity under germline hyperoxia. Somatic cell lines can also transform into new functional stemgermlines (clones), replace the damaged stemgermline, and resume the production of much-needed CSCs. In addition, stemgermline clones undergo continuous transitions between a proliferative ACD phenotype, which maintains stemness and produces committed non-proliferative CSCs, and a stress-damaged DSCD phenotype, which loses stemness potential and CSC-generating capacity. These aspects have not yet been recognized in the previous cancer research. CSCs have traditionally been viewed as both proliferative and differentiating, a perspective that diminishes the dominant role of the stemgermline along with its sublines and clones.
ACD-DSCD cycles are stemness loss and recovery cycles. Mechanisms such as the MGRS/PGCC genome repair pathway compensate for the frequent stemness lost. These frequently recurring stemness cycles have long been misinterpreted as evidence of cancer cell plasticity and genomic instability.
The contributions of polyploidy and hyperpolyploidy to the accumulation of cancer stem cells (CSCs) and the role of MGRS/PGCC as a genome repair pathway have only recently been elucidated with the help of ECCB, as has the expansion of the unicellularized genome through the integration of multicellular host genes. On the other hand, one can assume that Entamoeba not only serves as an optimal model for cancer but also that cancer cells provide the best evolutionarely model for understanding the processes underlying the early transition to multicellularity.
Finally, this work expresses the hope that ECCB findings will contribute to both theoretical and practical oncology, expanding the field and improving prospects for vaccines targeting the early risk of carcinogenesis, especially the MUT moment. While remarkable therapeutic advances have been developed and implemented over the past decades, extending patients’ lives by 20–25 years, the cost of these treatments remains immense, posing significant challenges for both healthcare systems and patients. Moreover, these therapies often come with numerous adverse effects. A vaccine capable of preventing unicellularization and blocking the senescence exit of DNA-DSB-damaged cells would represent a major breakthrough for all.
Abbreviations
ACD, asymmetric cell division; AMF, amoebozoans, metazoans and fungi;
CSC, cancer stem cells; pCSCs, primary CSCs; CTC, circulating tumor cells; DSCD, dysfunctional symmetric cell division; ECCB, evolutionary cancer cell biology; GI, genome instability; GS, genome stability; GST/MET, germ-to soma transition/mesenchymal-epithelial-transition; ITH, intra-tumoral heterogeneity; MGRS/PGCC, multinucleated genome repair structures/ polyploid giant cancer cells; MUT, multicellular to unicellular transition; SCD, symmetric cell division; SGT/EMT, soma to germ transition; UMT, unicellular to multicellular transition; UG/MG, hybrid unicellular cancer cell containing hijacked multicellular genes MGs (lateral gene transition)
References
- Bodmer WF. The evolutionary progression of cancers. Academia Oncology 2024; 1(2). [CrossRef]
- Dollo, L. Les lois de l’évolution/ The Laws of Evolution (translated by M. Carrano). Bull. Soc. Belge Geol. Paleontol. Hydrol. 1893, VII, 164–166. [Google Scholar]
- Gould, SJ. Dollo on Dollo’s law: irreversibility and the status of evolutionary laws. J. Hist. Biol 1970, 3, 189–212. [Google Scholar] [CrossRef] [PubMed]
- Collin R, Miglietta MP. Reversing opinions on Dollo’s Law. Trends Ecol. Evol. 2008; 23, 602–609.
- Hall BK. Dollo’s Law. In Encyclopedia of Evolution (Pagel, M., ed.), 2002, pp. 287–288, Oxford Univ Press.
- Elmer KR, Clobert J. Dollo’s law of irreversibility in the post-genomic age. Trends Ecol Evol. 2025; 40(2):136-146. [CrossRef]
- Forni G, Martelossi J, Valero P, Hennemann F, Conle O et al. (2022) Macroevolutionary analyses provide new evidence of phasmid wings evolution as a reversible process. Syst. Biol. 2022; 71, 1471–1486.
- Sadier A, Sears KE, Womack M. Unraveling the heritage of lost traits. J Exp Zool B Mol Dev Evol. 2022; 338[1–2]:107-118. [CrossRef]
- Paluh DJ, Dillard WA, Stanley EL, Fraser GJ, Blackburn DC. (2021) Re-evaluating the morphological evidence for the re-evolution of lost mandibular teeth in frogs. Evolution 2021; 75, 3203–3213.
- Niculescu VF (3). Reevaluating cancer stem cells and polyploid giant cancer cells from the evolutionary cancer cell biology perspective. Cancer Plus 2024, 6(4), 3970. [CrossRef]
- Niculescu VF. Understanding cancer from an evolutionarymperspective: High-risk reprogramming of genome-damaged stem cells. Acad Med. 2024;2.
- Niculescu VF, Niculescu ER. The enigma of cancer polyploidy as deciphered by evolutionary cancer cell biology (ECCB). Acad Med. 2024;1(2).
- Niculescu VF. Cancer Genomics: Restorative Senescence, Transition to Unicellularity, DDR Circuits and the Status Quo Ante, 2025. [CrossRef]
- Bank S, Bradler S. A second view on the evolution of flight in stick and leaf insects (Phasmatodea). BMC Ecol. Evol. 2022; 22, 62.
- Visser B, Alborn HT, Rondeaux S, Haillot M, Hance T, Reba D. (2021) Phenotypic plasticity explains apparent reverse evolution of fat synthesis in parasitic wasps. Sci. Rep. 2021, 11, 7751. [CrossRef]
- Lynch VJ. Is there a loophole in Dollo’s law? A DevoEvo perspective on irreversibility (of felid dentition). J. Exp. Zool. B Mol. Dev. Evol. 2023: 340, 509–517.
- Mukherjee C, Clark CG, Lohia A. Entamoeba shows reversible variation in ploidy under different growth conditions and between life cycle phases. PLoS Negl Trop Dis 2008; 2:e281.
- Mukherjee C, Majumder S, Lohia A. Inter-cellular variation in DNA content of Entamoeba histolytica originates from temporal and spatial uncoupling of cytokinesis from the nuclear cycle. PLoS Negl Trop Dis 2009; 3(4):e409.
- Niculescu VF. Growth of Entamoeba invadens in sediments with metabolically repressed bacteria leads to multicellularity and redefinition of the amoebic cell system. Roum Arch Microbiol Immunol 2013; 72(2):25–48.
- Niculescu, VF. The stem cell biology of the protist pathogen Entamoeba invadens in the context of eukaryotic stem cell evolution. Stem Cell Biol Res 2015. [Google Scholar] [CrossRef]
- Niculescu VF. aCLS cancers: Genomic and epigenetic changes transform the cell of origin of cancer into a tumorigenic pathogen of unicellular organization and lifestyle. Gene. 2020; 726:144174.
- Niculescu VF. Developmental and Non- Developmental Polyploidy in Xenic and Axenic Cultured Stem Cell Lines of Entamoeba invadens and E. histolytica. Insights Stem Cells. 2016; 2:1.
- Niculescu VF. Development, cell line differentiation and virulence in the primitive stem-/progenitor cell lineage of Entamoeba. J Stem Cell Res Med. 2017; 2(1):8.
- Krishnan D, Ghosh SK. Cellular events of multinucleated giant cell formation during the encystation of Entamoeba invadens. Front Cell Infect Microbiol 2018; 31(8):262.
- Hazra S, Kalyan Dinda S, Kumar Mondal N, Hossain SR, Datta P et al. Giant cells: Multiple cells unite to survive. Front Cell Infect Microbiol. 2023; 13:1220589. [CrossRef]
- Cowell CF, Weigelt B, Sakr RA, Ng CK, Hicks J, King TA, Reis-Filho JS. Progression from ductal carcinoma in situ to invasive breast cancer: revisited. Mol Oncol. 2013 Oct;7(5):859-69. [CrossRef]
- Lopez-Garcia MA, Geyer FC, Lacroix-Triki M, Marchio C, Reis-Filho JS. Breast cancer precursors revisited: molecular features and progression pathways. Histopathology 2010; 57, 171e192.
- Buerger H, Otterbach F, Simon R, Poremba C, Diallo, et al. Comparative genomic hybridization of ductal carcinoma in situ of the breastevidence of multiple genetic pathways. The Journal of Pathology 1999; 187, 396e402.
- Buerger H, Otterbach F, Simon R, Schafer KL, Poremba C et al. Different genetic pathways in the evolution of invasive breast cancer are associated with distinct morphological subtypes. The Journal of Pathology 1999; 189, 521e526.
- Burkhardt L, Grob TJ, Hermann I, Burandt E, Choschzick M et al. Gene amplification in ductal carcinoma in situ of the breast. Breast Cancer Research and Treatment 2010; 123, 757e765.
- O’Connell P, Pekkel V, Fuqua SA, Osborne CK, Clark GM, Allred D. Analysis of loss of heterozygosity in 399 premalignant breast lesions at 15 genetic loci. Journal of the National Cancer Institute 1998; 90, 697e703.
- Barsky SH, Karlin NJ. Myoepithelial cells: autocrine and paracrine suppressors of breast cancer progression. Journal of Mammary Gland Biology and Neoplasia 2005; 10, 249e260.
- Gudjonsson T, Adriance MC, Sternlicht MD, Petersen OW, Bissell MJ. 2005. Myoepithelial cells: their origin and function in breast morphogenesis and neoplasia. Journal of Mammary Gland Biology and Neoplasia. 2005; 10, 261e272.
- Place AE, Jin Huh S, Polyak K. The microenvironment in breast cancer progression: biology and implications for treatment. Breast Cancer Research: BCR 2011; 13, 227.
- Polyak K, HuM. Do myoepithelial cells hold the key for breast tumor progression? J Mammary Gland Biol Neoplasia. 2005;10(3):231-47. [CrossRef]
- Canval S. Effect of O-GlcNAcylation on tamoxifen sensitivity in breast cancer derived MCF-7 cells. Agricultural sciences. Universit’e Ren’e Descartes - Paris V, 2013.
- Min J, Zhang C, Bliton RJ, Caldwell B, Caplan L, et al. Dysplastic Stem Cell Plasticity Functions as a Driving Force for Neoplastic Transformation of Precancerous Gastric Mucosa. Gastroenterology. 2022;163(4):875-890. [CrossRef]
- Correa P. A human model of gastric carcinogenesis. Cancer Res. 1988; 48:3554-3560.
- Tan P, Yeoh KG. Genetics and molecular pathogenesis of gastric adenocarcinoma. Gastroenterology. 2015; 149:1153-1162.e3.
- de Vries AC, van Grieken NC, Looman CW. Gastric cancer risk in patients with premalignant gastric lesions: a nationwide cohort study in the Netherlands. Gastroenterology. 2008; 134:945-952.
- Upadhyay A. Cancer: An unknown territory; rethinking before going ahead. Genes Dis. 2020;8(5):655-661. [CrossRef]
- Horne SD, Ye CJ, Abdallah BY, Liu G, Heng HH. Cancer genome evolution. Transl Cancer Res 2015;4(3):303-313. [CrossRef]
- Heng HH. The genome-centric concept: resynthesis of evolutionary theory. Bioessays 2009; 31:512-25.
- Heng HH. Bio-complexity: challenging reductionism. In: Sturmberg JP, Martin CM, editors. Handbook on Systems and Complexity in Health. New York: Springer 2013:193-208.
- Heng HH, Liu G, Stevens JB, Bremer SW, Ye KJ et al. Decoding the genome beyond sequencing: the new phase of genomic research. Genomics 2011; 98:242-52.
- Gerstung M, Jolly C, Leshchiner I, Dentro SC, Gonzalez S et al.The evolutionary history of 2,658 cancers. Nature. 2020;578(7793):122-128. 7793. [CrossRef]
- Danovi S. The evolving cancer genome. Nat Genet 2023; 55; 1082. [CrossRef]
- Jolly, C. & Van Loo, P. Timing somatic events in the evolution of cancer. Genome Biol. 2018; 19, 95.
- Mitchell TJ, Turajlic S, Rowan A, Nicol D, Farmery JHR, et al. TRACERx Renal Consortium. Timing the Landmark Events in the Evolution of Clear Cell Renal Cell Cancer: TRACERx Renal. Cell. 2018;173(3):611-623.e17. [CrossRef]
- Gundem G, Van Loo P, Kremeyer B, Alexandrov LB, Tubio JMC et al. The evolutionary history of lethal metastatic prostate cancer. Nature. 2015;520(7547):353-357. [CrossRef]
- Yates LR, Gerstung M, Knappskog S, Desmedt C, Gundem G et al. Subclonal diversification of primary breast cancer revealed by multiregion sequencing. Nat Med. 2015;21(7):751-9. [CrossRef]
- Brastianos PK, Carter SL, Santagata S, Cahill DP, Taylor-Weiner A et al. Genomic Characterization of Brain Metastases Reveals Branched Evolution and Potential Therapeutic Targets. Cancer Discov. 2015 Nov;5(11):1164-1177. [CrossRef]
- Landau DA, Tausch E, Taylor-Weiner AN, Stewart C, Reiter JG et al. Mutations driving CLL and their evolution in progression and relapse. Nature. 2015;526(7574):525-30. [CrossRef]
- European Molecular Biology Laboratory. Cancer mutations occur decades before diagnosis. Science Daily, 6 February 2020. www.sciencedaily.com/releases/2020/02/200206080451.htm.
- Cheek DM, Naxerova K. Mapping the long road to cancer. Cell. 2022;185(6):939-940. [CrossRef]
- Hanahan D. Hallmarks of Cancer: New Dimensions. Cancer Discov. 2022;12(1):31-46. [CrossRef]
- Sarker DB, Xue Y, Mahmud F, Jocelyn JA, Sang QA. Interconversion of Cancer Cells and Induced Pluripotent Stem Cells. Cells. 2024; 13(2):125. [CrossRef]
- Gandre-Babbe S, Paluru P, Aribeana C, Chou ST, Bresolin S et al. Patient-derived induced pluripotent stem cells recapitulate hematopoietic abnormalities of juvenile myelomonocytic leukemia. Blood J. Am. Soc. Hematol. 2013; 121, 4925–4929.
- Oshima N, Yamada Y, Nagayama S, Kawada K, Hasegawa S et al. Induction of cancer stem cell properties in colon cancer cells by defined factors. PLoS ONE 2014; 9, e101735.
- Yu Z, Pestell TG, Lisanti MP, Pestell RG. Cancer stem cells. Int. J. Biochem. Cell Biol. 2012; 44, 2144–2151.
- Miyoshi N, Ishii H, Nagai K, Hoshino H, Mimori K. et al. Defined factors induce reprogramming of gastrointestinal cancer cells. Proc. Natl. Acad. Sci. USA 2010, 107, 40–45.
- Utikal J, Maherali N Kulalert W, Hochedlinger K. Sox2 is dispensable for the reprogramming of melanocytes and melanoma cells into induced pluripotent stem cells. J. Cell Sci. 2009; 122, 3502–3510.
- Shamsian A, Sahebnasagh R, Norouzy A, Hussein SH, Ghahremani MH, Azizi Z. Cancer cells as a new source of induced pluripotent stem cells. Stem Cell Res Ther. 2022;13(1):459. [CrossRef]
- Kim HJ, Jeong J, Park S, Jin YW, Lee SS et al. Establishment of Hepatocellular Cancer Induced Pluripotent Stem Cells Using a Reprogramming Technique. Gut Liver. 2017 Mar 15;11(2):261-269. [CrossRef]
- Mahalingam D, Kong CM, Lai J, Tay LL, Yang H, Wang X. (2012). Reversal of aberrant cancer methylome and transcriptome upon direct reprogramming of lung cancer cells. Scientific Reports, 2012; 2. [CrossRef]
- Trevor A Graham TA, Sottoriva A. Measuring cancer evolution from the genome: Measuring cancer evolution. Journal of Pathology 2016. [CrossRef]
- Levitt NC, Hickson ID. Caretaker tumour suppressor genes that defend genome integrity”. Trends in Mol. Medicine. 2002; 8 (4): 179–86. [CrossRef]
- Kinzler KW, Vogelstein B. Cancer-susceptibility genes. Gatekeepers and caretakers. Nature. 1997;386(6627):761, 763. [CrossRef]
- Frank SA. Somatic mutation: Early cancer steps depend on tissue architecture. Current Biology. 2003; 13 (7): R261–3. [CrossRef]
- Campisi J. Aging, tumor suppression and cancer: High wire-act! Mechanisms of Ageing and Development. 2005:126 (1): 51-58. [CrossRef]
- Michor F, Iwasa Y, Nowak M. Dynamics of cancer progression. Nat Rev Cancer 2004;4:197–205. [CrossRef]
- Fanale D, Maragliano R, Bazan V, Russo A. Caretakers and Gatekeepers. Genetics & Disease. 2017. [CrossRef]
- Nowell PC. The clonal evolution of tumor cell populations. Science. 1976; 194:23–28.
- Yao Y, Dai W. Genomic Instability and Cancer. J Carcinog Mutagen. 2014;5:1000165. [CrossRef]
- Polo SE, Jackson SP. Dynamics of DNA damage response proteins at DNA breaks: a focus on protein modifications. Genes Dev. 2011; 25:409–433.
- Loeb LA. Mutator phenotype may be required for multistage carcinogenesis. Cancer Res. 1991; 51:3075–3079.
- Loeb LA. A mutator phenotype in cancer. Cancer Res. 2001; 61:3230–3239.
- Negrini S, Gorgoulis VG, Halazonetis TD. Genomic instability-an evolving hallmark of cancer. Nat Rev Mol Cell Biol. 2010; 11:220–228.
- Warrier NM, Kelkar N, Johnson CT, Govindarajan T, Prabhu V, Kumar P. Understanding cancer stem cells and plasticity: Towards better therapeutics. Eur J Cell Biol. 2023;102(2):151321. [CrossRef]
- Plaks V, Kong N, Werb Z. The cancer stem cell niche: how essential is the niche in regulating stemness of tumor cells. Cell Stem Cell, 2015; 16, 225-238. [CrossRef]
- Nam AS, Chaligne R, Landau DA. Integrating Genetic and Non-Genetic Determinants of Cancer Evolution by Single-Cell Multi-Omics. Nat. Rev. Genet. 2021, 22, 3–18.
- Martincorena I, Fowler JC, Wabik A, Lawson ARJ, Abascal F et al. Somatic mutant clones colonize the human esophagus with age. Science. 2018;362(6417) 911-917. [CrossRef]
- Yizhak K, Aguet F, Kim J, Hess JM, Kübler K et al. RNA sequence analysis reveals macroscopic somatic clonal expansion across normal tissues. Science. 2019;7;364(6444):eaaw0726. [CrossRef]
- Yokoyama A, Kakiuchi N, Yoshizato T, Nannya Y, Suzuki H et al. Age-related remodelling of oesophageal epithelia by mutated cancer drivers. Nature. 2019 Jan;565(7739):312-317. [CrossRef]
- Martincorena I, Roshan A, Gerstung M, Ellis P, Van Loo P et al. Tumor evolution. High burden and pervasive positive selection of somatic mutations in normal human skin. Science. 2015;348(6237):880-6. [CrossRef]
- Yoshida K, Gowers KHC, Lee-Six H, Chandrasekharan DP, Coorens T et al. Tobacco smoking and somatic mutations in human bronchial epithelium. Nature. 2020;578(7794):266-272. [CrossRef]
- Teixeira VH, Pipinikas CP, Pennycuick A, Lee-Six H, Chandrasekharan D et al. Deciphering the genomic, epigenomic, and transcriptomic landscapes of pre-invasive lung cancer lesions. Nat Med. 2019;25(3):517-525. [CrossRef]
- Kaufman CK, Mosimann C, Fan ZP, Yang S, Thomas AJ et al. A zebrafish melanoma model reveals emergence of neural crest identity during melanoma initiation. Science. 2016;351(6272):aad2197. [CrossRef]
- Turajlic S, Sottoriva A, Graham T, Swanton C. Resolving genetic heterogeneity in cancer. Nat. Rev. Genet 2019: 20, 404–416 (2019). [CrossRef]
- Pepper JW, Scott Findlay C, Kassen R, Spencer SL, Maley CC. Cancer research meets evolutionary biology. Evol Appl. 2009;2(1):62-70. [CrossRef]
- Vincent MD. The animal within: carcinogenesis and the clonal evolution of cancer cells are speciation events sensu stricto. Evolution. 2010;64(4):1173-83. [CrossRef]
- Huxley, J. 1956. Cancer biology: comparative and genetic. Biol. Rev. 31:474–514.
- Greaves M, Maley CC. Clonal Evolution in Cancer. Nature 2012, 481, 306–313.
- Swanto, C. Intratumor Heterogeneity: Evolution through Space and Time. Cancer Res. 2012;72, 4875–4882.
- Duesberg P, Rasnick D. Aneuploidy, the somatic mutation that makes cancer a species of its own. Cell Motil. Cytoskeleton 2000; 47:81–107.
- Merlo LMF, Pepper JW, Reid BJ, Maley CC. Cancer as an evolutionary and ecological process. Nat. Rev. Cancer 2006; 6:924–935.
- Gray MW, Lang BF, Burger G. Mitochondria of protists. Ann. Rev. Genet. 2004; 38:477–524.
- Rivera M, Lake J. The ring of life provides evidence for a genome fusion origin of eukaryotes. Nature 2004; 431:152–155.
- Vincent, M. Vincent M. Cancer: a de-repression of a default survival program common to all cells? a life-history perspective on the nature of cancer. Bioessays. 2012; 34(1):72-82. [CrossRef]
- Domazet-Lošo T, Tautz D. An ancient evolutionary origin of genes associated with human genetic diseases. Mol Biol Evol. 2008; 25:2699-2707. [CrossRef]
- Domazet-Loso T, Tautz D. Phylostratigraphic tracking of cancer genes suggests a link to the emergence of multicellularity in metazoa. BMC Biol. 2010; 8:66. [CrossRef]
- Trigos AS, Pearson RB, Papenfuss AT, Goode DL. Altered interactions between unicellular and multicellular genes drive hallmarks of transformation in a diverse range of solid tumors. Proc Natl Acad Sci U S A. 2017; 114:6406–6411. [CrossRef]
- Trigos AS, Pearson RB, Papenfuss AT, Goode DL. How the evolution of multicellularity set the stage for cancer. Br J Cancer. 2018; 118:145-152. [CrossRef]
- Trigos AS, Pearson RB, Papenfuss AT, Goode DL. Somatic mutations in early metazoan genes disrupt regulatory links between unicellular and multicellular genes in cancer. Elife. 2019; 8:e40947. [CrossRef]
- Lineweaver CH, Davies P. Comparison of the atavistic model of cancer to somatic mutation theory: Phylostratigraphic analyses support the atavistic model. In: Gerstman BS, editor. The Physics of Cancer: Research Advances. Singapore: World Scientific; 2020. p. 243-261. [CrossRef]
- Rebolleda-Gomez M, Travisano M. The cost of being big: local competition, importance of dispersal and experimental evolution of reversal to unicellularity. Am.Nat. 2018; 192,731–744. [CrossRef]
- Libby E, Ratcliff WC. 2014. Ratcheting the evolution of multicellularity. Science 2014; ce 346 (6208), 426–427. [CrossRef]
- Michod RE, Viossat Y, Solari CA, Hurand M, Nedelcu AM. Life-history evolution and the origin of multicellularity. J Theor Biol. 2006;239(2):257-72. [CrossRef]
- Michod RE. Evolution of individuality during the transition from unicellular to multicellular life. Proc Natl Acad Sci U S A. 2007 May 15;104 Suppl 1(Suppl 1):8613-8. [CrossRef]
- Folse HJ, Roughgarden J. What is an individual organism? A multilevel selection perspective. Q. Rev. Biol. 2010, 85 (4), 447–472. [PubMed]
- Rebolleda-Gómez M, Travisano M. Adaptation, chance, and history in experimental evolution reversals to unicellularity. Evolution. 2019 Jan;73(1):73-83. [CrossRef]
- Liu, ZL., Chen, HH., Zheng, LL. et al. Angiogenic signaling pathways and anti-angiogenic therapy for cancer. Sig Transduct Target Ther 8, 198 (2023). [CrossRef]
- K. Schlacher, N. Christ, N. Siaud, A. Egashira, H. Wu, M. Jasin, Double-strand break repair-independent role for BRCA2 in blocking stalled replication fork degradation by MRE11, Cell 2011;145, 529–542.
- Chen Q, Zou J, He Y, Pan Y, Yang G, et al. A narrative review of circulating tumor cells clusters: A key morphology of cancer cells in circulation promote hematogenous metastasis. Front. Oncol. 2022; 12:944487. [CrossRef]
- Ashworth TR. A case of cancer in which similar cells similar to those in the tumour were seen in the blood after death. Australian Medical Journal. 1969; 146-149.
- Gwark S, Kim J, Kwon NJ, Kim KY, Kim Y, Lee CH et al. Publisher Correction: Analysis of the serial circulating tumor cell count during neoadjuvant chemotherapy in breast cancer patients. Sci Rep. 2021;11(1):6148. doi: 10.1038/s41598-021-85731-3. Erratum for: Sci Rep. 2020 Oct 15;10(1):17466. doi: 10.1038/s41598-020-74577-w. [CrossRef]
- Tellez-Gabriel M, Knutsen E, Perander, M. Current status of circulating tumor cells, circulating tumor DNA, and exosomes in breast cancer liquid biopsies. Int. J. Mol. Sci. 2020; 21, 9457.
- Vismara M, Reduzzi C, Daidone, MG, CappellettiV. Circulating tumor cells (CTCs) heterogeneity in metastatic breast cancer: different approaches for different needs. Adv. Exp. Med. Biol. 2020;1220, 81–91.
- Pinheiro R, Martínez-Pena I, López-López R. Relevance of CTC clusters in breast cancer metastasis. Adv. Exp. Med. Biol. 2020; 1220, 93–115.
- Gu X, Wei S, Lv X. Circulating tumor cells: from new biological insights to clinical practice. Signal Transduct Target Ther. 2024 Sep 2;9(1):226. [CrossRef]
- Gao D, Mittal V, Ban Y, Lourenco AR, Yomtoubian S, Lee S. Metastatic tumor cells - genotypes and phenotypes. Front Biol (Beijing). 2018;13(4):277-286. [CrossRef]
- Lambert A W, Pattabiraman D R, Weinberg R A (2017). Emerging Biological Principles of Metastasis. Cell 2017;168:670–691.
- Liu H, Patel MR, Prescher JA, Patsialou A, Qian D, Lin J et al. Cancer stem cells from human breast tumors are involved in spontaneous metastases in orthotopic mouse models. Proc Natl Acad Sci U S A 2010;107:18115–18120.
- Comaills V, Kabeche L, Morris R, Buisson R, Yu M et al. Genomic instability is induced by persistent proliferation of cells undergoing epithelial-to-mesenchymal transition, Cell Rep. 2016; 17, 2632–2647.
- Levine MS, A.J. Holland AJ. The impact of mitotic errors on cell proliferation and tumorigenesis. Genes Dev. 2018;32,620–638.
- Davoli T, Uno H, Wooten EC, Elledge SJ. Tumor aneuploidy correlates with markers of immune evasion and with reduced response to immunotherapy, Science 2017;355.
- Germano G, Lamba S, Rospo G, Barault L, Magrì A, et al. Inactivation of DNA repair triggers neoantigen generation and impairs tumour growth, Nature. 2017; 552, 116–120.
- Christensen S, Van der Roest B, Besselink N, Janssen R, Boymans RS et al. 5-fluorouracil treatment induces characteristic T>G mutations in human cancer, Nat. Commun. 2019; 10, 4571.
- Schuster E, Taftaf R, Reduzzi C, Albert MK, Romero-Calvo I, Liu H. Better together: circulating tumor cell clustering in metastatic cancer. Trends Cancer. 2021;7(11):1020-1032. [CrossRef]
- Aguilera A, García-Muse T. Causes of genome instability, Annu. Rev. Genet. 2013;47, 1–32.
- Schlacher K, Wu H, Jasin M. A distinct replication fork protection pathway connects fanconi anemia tumor suppressors to RAD51-BRCA1/2, Cancer cell. 2012; 22, 106–116.
- Nassour J, Radford R, Correia A, Fust’e JM, Schoell B, Jauch A. Autophagic cell death restricts chromosomal instability during replicative crisis, Nature. 2019;565, 659–663.
- Ira G, Pellicioli A, Balijja A, Wang X, Fiorani S et al. DNA end resection, homologous recombination and DNA damage checkpoint activation require CDK1. Nature. 2004;431(7011):1011-7. [CrossRef]
- Wyman C, Ristic D, Kanaar K. Homologous recombination-mediated doublestrand break repair, DNA repair. 2004; 3, 827–833.
- Piazza A, HeyeWD. Homologous recombination and the formation of complex genomic rearrangements. Trends Cell Biol. 2019; 29,135–149.
- Liu X, Taftaf R, Kawaguchi M, Chang YF, Chen W et al. Homophilic CD44 Interactions Mediate Tumor Cell Aggregation and Polyclonal Metastasis in Patient-Derived Breast Cancer Models. Cancer Discov. 2019;9(1):96-113. [CrossRef]
- Taftaf R, Liu X, Singh S, Jia Y, Dashzeveg NK et al. ICAM1 initiates CTC cluster formation and trans-endothelial migration in lung metastasis of breast cancer. Nat Commun. 2021;12(1):4867. [CrossRef]
- Chimonidou M, Strati A, Tzitzira A, Sotiropoulou G, Malamos N et al. DNA methylation of tumor suppressor and metastasis suppressor genes in circulating tumor cells. Clin Chem. 2011;57(8):1169-77. [CrossRef]
- Chen DS, Mellman I. Elements of cancer immunity and the cancer-immune set point. Nature. 2017;541,321–330.
- Lara-Gonzalez P, Westhorpe FG, Taylor SS. The spindle assembly checkpoint, Current Biol. 2012;22, R966–R980.
- McClintock B. The production of homozygous deficient tissues with mutant characteristics by means of the aberrant mitotic behavior of ring-shaped chromosomes. Genetics. 1938; 23, 315–376.
- Drost J, van Jaarsveld RH, Ponsioen B, Zimberlin C, van Boxtel R, et al. Sequential cancer mutations in cultured human intestinal stem cells. Nature. 2015;7;521(7550):43-7. [CrossRef]
- Davies AA, Masson JY, McIlwraith MJ, Stasiak AZ, Stasiak, A et al. Role of BRCA2 in control of the RAD51 recombination and DNA repair protein, Mol. Cell. 2001;7, 273–282.
- Petros JA, Baumann AK, Ruiz-Pesini E, Amin MB, Sun CQ et al. mtDNA mutations increase tumorigenicity in prostate cancer, Proc. Natl. Acad.Sci. U. S. A. 2005; 102, 719–724.
- Coleman RE, Croucher PI, Padhani AR, Clézardin P, Chow E et al. Bone metastases. Nat Rev Dis Primers. 2020;6(1):83. [CrossRef]
- Croucher P, McDonald M, Martin, T. Bone metastasis: the importance of the neighbourhood. Nat Rev Cancer 2016; 16, 373–386 (2016). [CrossRef]
- Shen Z. Genomic instability and cancer: an introduction. J Mol Cell Biol. 2011; 3(1):1-3. [CrossRef]
- Salmaninejad A, Ilkhani K, Marzban H, Navashenaq JG, Rahimirad S et al.. Genomic Instability in Cancer: Molecular Mechanisms and Therapeutic Potentials. Curr Pharm Des. 2021;27(28):3161-3169. [CrossRef]
- Chen M, Linstra R, van Vugt. Genomic instability, inflammatory signaling and response to cancer immunotherapy. Biochim Biophys Acta Rev Cancer. 2022;1877(1):188661. [CrossRef]
- Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144, 646–674.
- Lawrence KS, Chau T, Engebrecht J. DNA damage response and spindle assembly checkpoint function throughout the cell cycle to ensure genomic integrity.PLoS Genet. 2015;11, e1005150.
- Hatch EM, Fischer AH, Deerinck TJ, Hetzer MW., Catastrophic nuclear envelope collapse in cancer cell micronuclei. Cell 2013; 154, 47–60.
- Chu X, Tian W, Ning J et al. Cancer stem cells: advances in knowledge and implications for cancer therapy. Sig Transduct Target Ther. 2024; 9, 170. [CrossRef]
- Bonnet D, Dick JE. Human acute myeloid leukemia is organized as a hierarchythat originates from a primitive hematopoietic cell. Nat. Med. 1997;3, 730–737.
- Mani SA, Guo W, Liao MJ, Eaton EN, Ayyanan A et al. The epithelial-mesenchymal transition generates cells with properties of stem cells. Cell. 2008 May 16;133(4):704-15. [CrossRef]
- Thiery JP, Acloque H, Huang RY, Nieto MA. Epithelial-mesenchymaltransitions in development and disease. Cell. 2009;139, 871–890.
- Wellner U, Schubert J, Burk UC, Schmalhofer O, Zhu F et al. The EMT-activator ZEB1 promotes tumorigenicity by repressing stemness-inhibiting microRNAs. Nat Cell Biol. 2009 Dec;11(12):1487-95. [CrossRef]
Figure 1.
From genetical altered epithelial cells to metastases - original legend [36]: Tumors development takes place in different steps. (A) Hyperplasia is the stage where genetically altered or abnormal cells show uncontrolled and rapid growth. (B) Dysplasia, stage of tumor development where overgrowing cells changes their original form. It consists of more immature cells than mature. (C) In situ cancer represent neoplastic lesion where cells do not go into the process of maturation, have lost their tissue identity and grow without regulation. (D) With malignant tumor, overgrowing cells invade other areas by rupturing basal membrane (E.) Metastases occur when cancer cells reach to the distant parts through lymphatic system and blood circulation. This figure is uploaded from the HAL archive for the deposit and dissemination of scientific research documents. These documents come from teaching and research institutions in France orabroad, or from public or private research centers. It was uploaded by Shahzina Kanwal (see: 36. Effect of O-GlcNAcylation on tamoxifen sensitivity in breast cancer derived MCF-7 cells. Agricultural sciences. Universit’e Ren’e Descartes - Paris V, 2013).
Figure 1.
From genetical altered epithelial cells to metastases - original legend [36]: Tumors development takes place in different steps. (A) Hyperplasia is the stage where genetically altered or abnormal cells show uncontrolled and rapid growth. (B) Dysplasia, stage of tumor development where overgrowing cells changes their original form. It consists of more immature cells than mature. (C) In situ cancer represent neoplastic lesion where cells do not go into the process of maturation, have lost their tissue identity and grow without regulation. (D) With malignant tumor, overgrowing cells invade other areas by rupturing basal membrane (E.) Metastases occur when cancer cells reach to the distant parts through lymphatic system and blood circulation. This figure is uploaded from the HAL archive for the deposit and dissemination of scientific research documents. These documents come from teaching and research institutions in France orabroad, or from public or private research centers. It was uploaded by Shahzina Kanwal (see: 36. Effect of O-GlcNAcylation on tamoxifen sensitivity in breast cancer derived MCF-7 cells. Agricultural sciences. Universit’e Ren’e Descartes - Paris V, 2013).
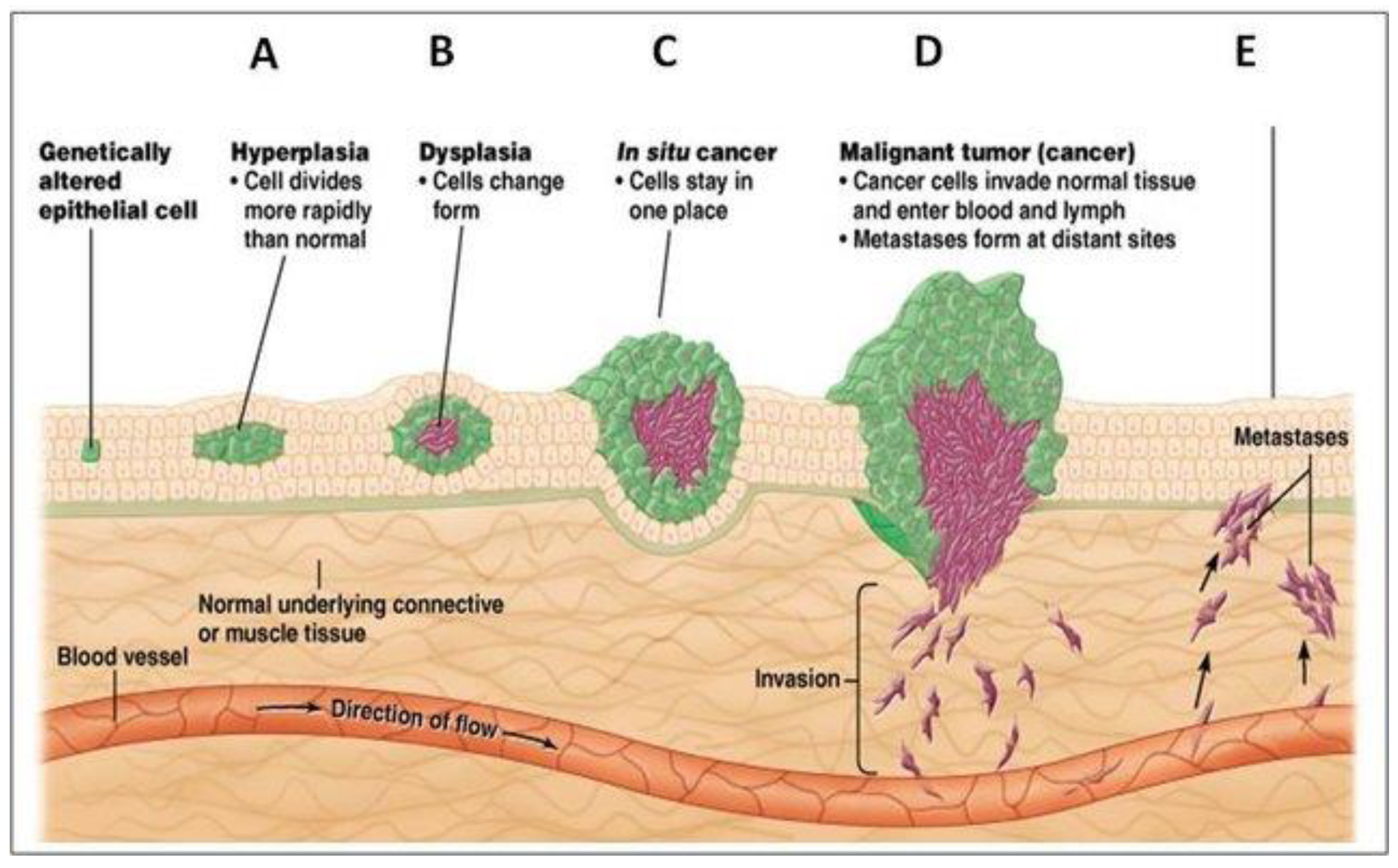
Figure 2.
The progression of the canceration through growth and angiogenesis. The rapid expansion of tumor results in a reduction in the oxygen supply. The consequent hypoxic tumor microenvironment stimulates excessive angiogenesis via increasing various angiogenic pro-factors including VEGF, PDGF, FGF, and angiopoietin. Later, new blood vessels facilitate the transportation of oxygen and nutrients to further support the survival, growth and proliferation of tumor cells. When tumor cells develop a more aggressive phenotype, they continue to proliferate, spread and induce angiogenesis, with the invasion and metastasis of tumor cells into distant tissues through blood circulation. Original caption of Liu et al.[123].
Figure 2.
The progression of the canceration through growth and angiogenesis. The rapid expansion of tumor results in a reduction in the oxygen supply. The consequent hypoxic tumor microenvironment stimulates excessive angiogenesis via increasing various angiogenic pro-factors including VEGF, PDGF, FGF, and angiopoietin. Later, new blood vessels facilitate the transportation of oxygen and nutrients to further support the survival, growth and proliferation of tumor cells. When tumor cells develop a more aggressive phenotype, they continue to proliferate, spread and induce angiogenesis, with the invasion and metastasis of tumor cells into distant tissues through blood circulation. Original caption of Liu et al.[123].
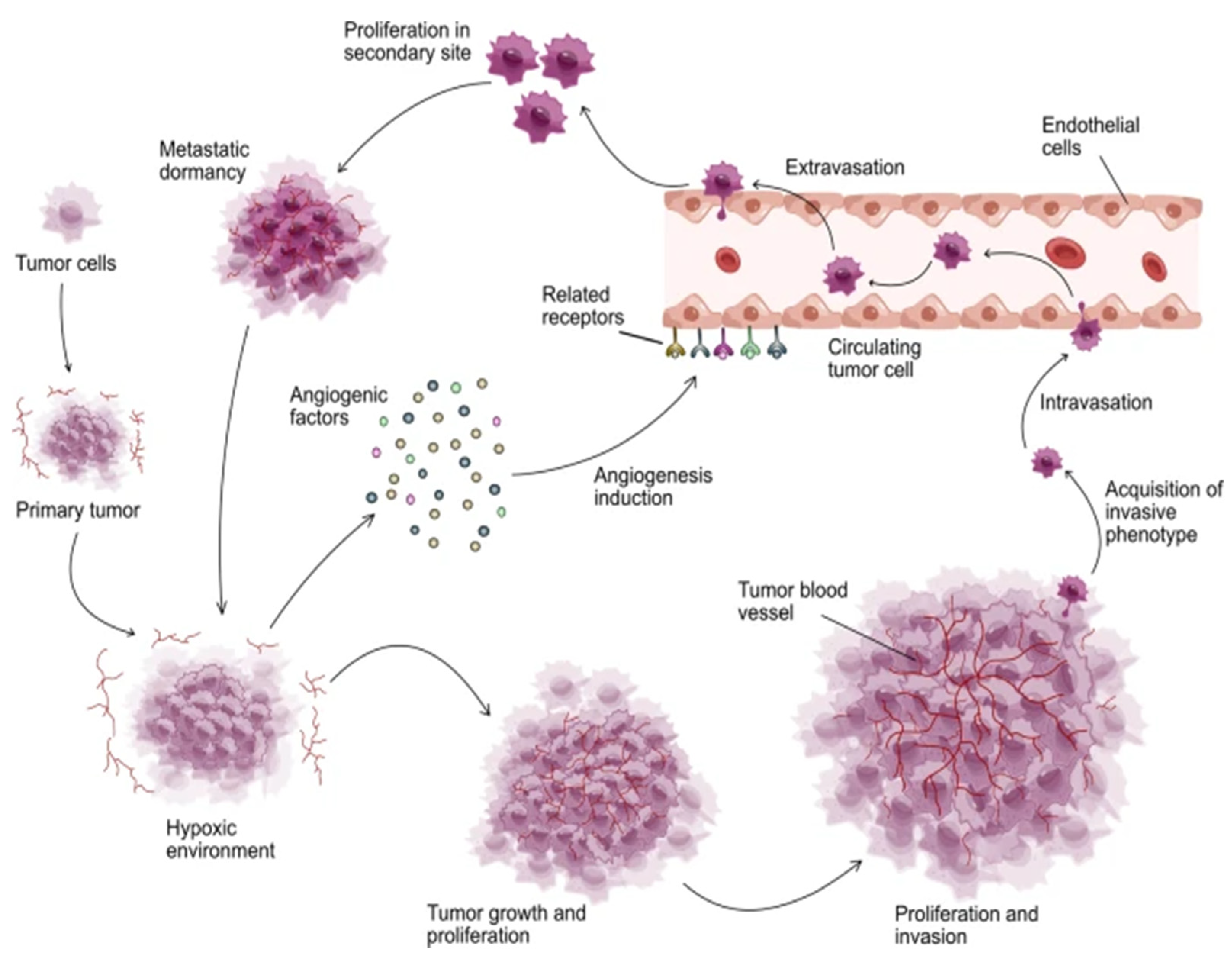
Figure 3.
The life cycle of stemness (stemness cycle) in cancer and protists: alternation of ACD and DSCD phenotypes and repair through the MGRS/PGCC pathway; from Niculescu, 2024 [10].
Figure 3.
The life cycle of stemness (stemness cycle) in cancer and protists: alternation of ACD and DSCD phenotypes and repair through the MGRS/PGCC pathway; from Niculescu, 2024 [10].
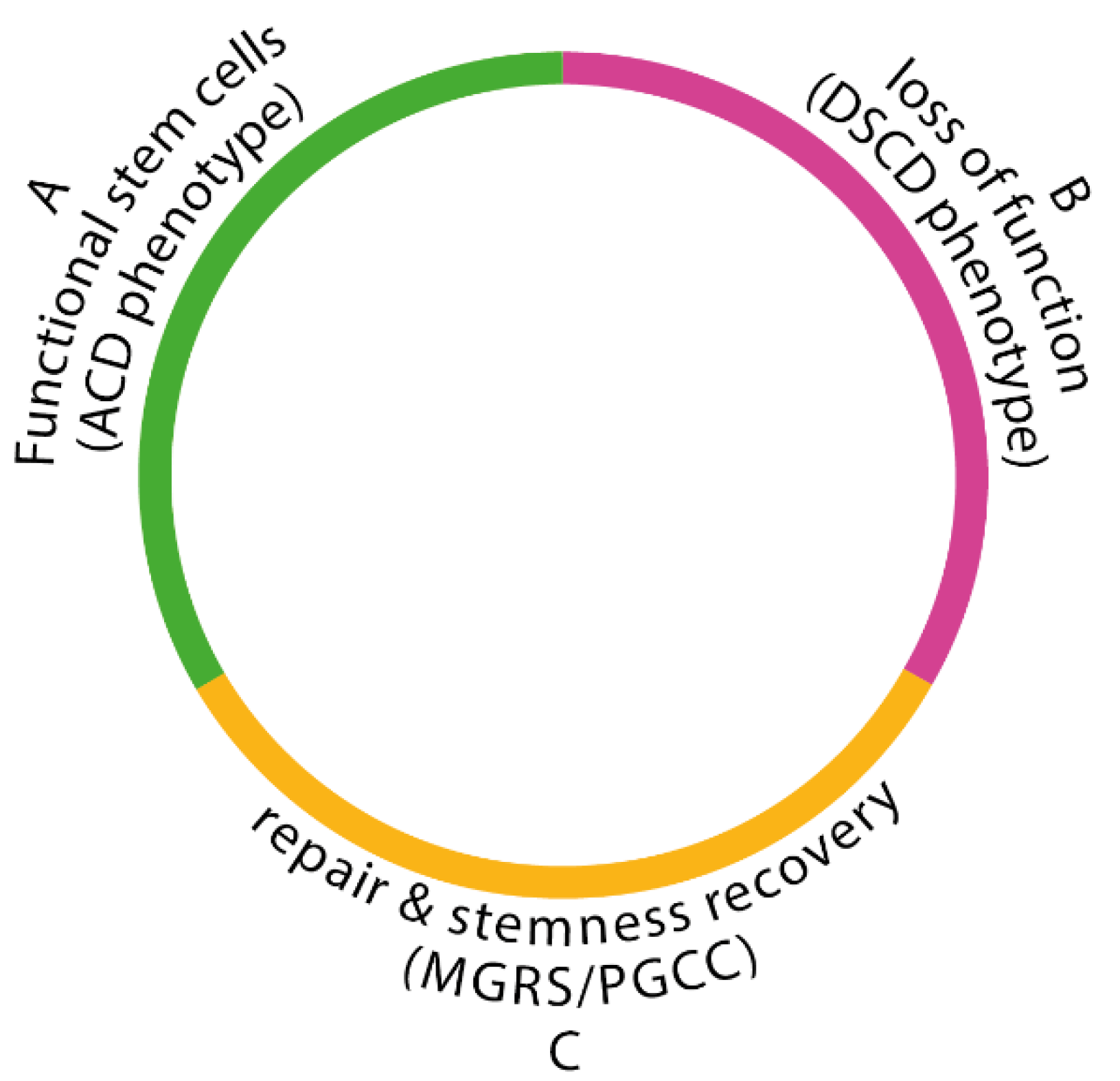
Figure 4.
Hypothetical models of progression from in situ to invasive breast cancer. (A) Progression from DCIS to IBC as a convergent phenotype, where several combinations of somatic genetic and/or epigenetic aberrations result in the acquisition of the biological properties required for cancer cells to progress from in situ to invasive disease (i.e. the genetic/epigenetic aberrations selected for are distinct between patients but all result in the progression to invasive disease). (B) Progression from DCIS to IBC as an evolutionary bottleneck. As DCIS develops, cells accumulate somatic mutations and copy number aberrations (depicted by color) to generate a heterogeneous lesion with distinct subclones harboring private mutations in addition to the founder genetic aberrations present in all neoplastic cells. Only subclones harboring a specific repertoire of genetic aberrations are selected and pass through the evolutionary bottleneck of progression to IBC. DCIS: ductal carcinoma in situ; IBC: invasive breast cancer; Original Legend. From Cowell [26] with the permission of Wiley and FEBS (CC By).
Figure 4.
Hypothetical models of progression from in situ to invasive breast cancer. (A) Progression from DCIS to IBC as a convergent phenotype, where several combinations of somatic genetic and/or epigenetic aberrations result in the acquisition of the biological properties required for cancer cells to progress from in situ to invasive disease (i.e. the genetic/epigenetic aberrations selected for are distinct between patients but all result in the progression to invasive disease). (B) Progression from DCIS to IBC as an evolutionary bottleneck. As DCIS develops, cells accumulate somatic mutations and copy number aberrations (depicted by color) to generate a heterogeneous lesion with distinct subclones harboring private mutations in addition to the founder genetic aberrations present in all neoplastic cells. Only subclones harboring a specific repertoire of genetic aberrations are selected and pass through the evolutionary bottleneck of progression to IBC. DCIS: ductal carcinoma in situ; IBC: invasive breast cancer; Original Legend. From Cowell [26] with the permission of Wiley and FEBS (CC By).
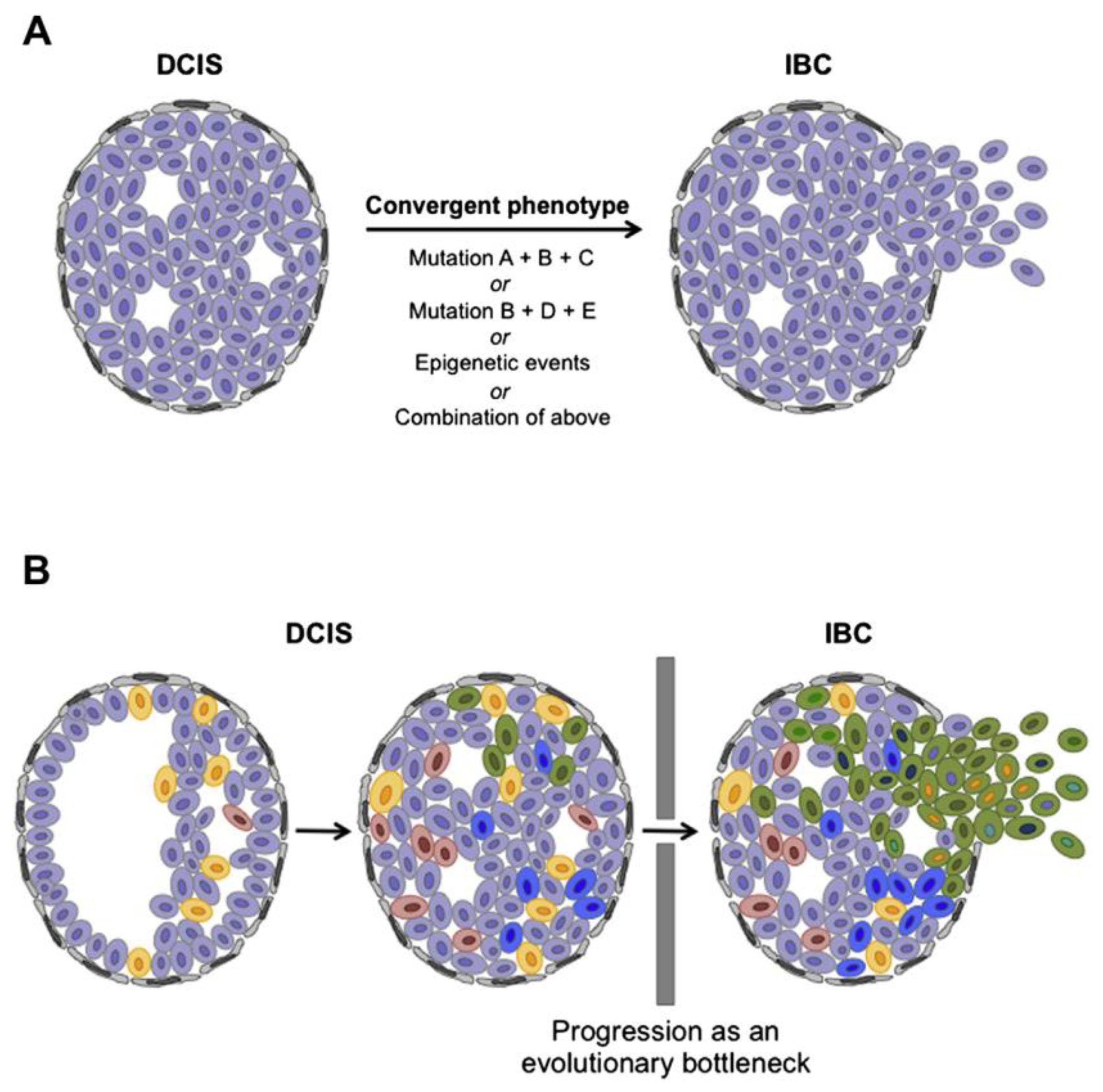
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



