
Submitted:
18 April 2025
Posted:
21 April 2025
You are already at the latest version
Abstract
Background: Autoimmune hepatitis (AIH) is a chronic liver disease in which the immune system of the body unintentionally targets its own liver cells, resulting in inflammation, liver damage, and, if treatment is not received, cirrhosis. Although the precise origin of AIH is unknown, environmental and genetic factors are believed to play important roles. The clinical, biochemical, and long-term results of patients with autoimmune hepatitis (AIH) at the Science and Technology Hospital in Yemen are described in this paper. Design Retrospective, single-center study. Participants All patients with AIH were diagnosed at the Science and Technology Hospital from 2019 to 2024. Results: The average age of the 25 diagnosed patients was 16 ± 78 years. The majority were male (18 out of 25, 72 %). All patients displayed common signs and symptoms of AIH, including hepatomegaly, vomiting, jaundice, and abdominal distention. In addition to positive anti-nuclear antibodies (ANA) and anti-smooth muscle antibodies (ASMA), the majority of individuals showed increased AST levels. The most prevalent hematological abnormalities were thrombocytopenia (64%) and anemia (56%). Regarding the outcome after admission to the hospital, 60% of cases improved, 12% were discharged against medical advice,8% died, and 20% had unknown outcomes. Conclusion Autoimmune hepatitis affects patients with Yemeni. Jaundice is the most common symptom. Only Type I AIH was observed in this cohort, and mortality reached 8%.
Keywords:
Autoimmune hepatitis
; Liver
; AMA
; ANA
Introduction
All patients displayed common signs and symptoms of Autoimmune Hepatitis, including hepatomegaly, vomiting, jaundice, and abdominal distention. In addition to positive anti-nuclear antibodies (ANA) and anti-smooth muscle antibodies (ASMA), the majority of individuals showed increased AST levels. The most prevalent hematological abnormalities were thrombocytopenia (64%) and anemia (56%) [1]. The (AIH) cause is believed to be caused by a loss of immune tolerance toward liver cells (hepatocytes), triggered by environmental factors in genetically susceptible individuals, possibly through a mechanism known as “molecular mimicry.” [2]. (AIH) is histologically diagnosed based on viral markers (HBV,HAV, HBsAg, and HCV), border hepatitis, elevated serum levels of aspartate aminotransferase (AST), alanine aminotransferase (ALT), and immunoglobulin (IgG), and the presence of autoantibodies [3]. Additionally, autoimmune hepatitis is classified into two subtypes based on serology: type 1, which has antinuclear antibodies (ANA) and/or smooth muscle antibodies (SMA), and type 2, which has anti-liver-kidney microsomal antibody (anti-LKM-1) and/or anti-liver cytosolic antigen type 1 (anti-LC-1) [4]. Children and adolescents have different clinical signs of AIH, and unless treated quickly, they often present with a more aggressive course than adults [5]. The cornerstone of AIH treatment is immunosuppression; corticosteroids alone or in conjunction with azathioprine are the cornerstones of AIH treatment, and novel therapeutic approaches that encompass the full spectrum of immunosuppressive tools, such as biologics and cellular-based therapies, have been suggested [6]. Although prolonged steroid medication has many undesirable side effects, it is generally thought to be the best course of treatment for individuals with moderate-to-severe bouts [7]. An undiagnosed AIH can lead to end-stage liver disease and cirrhosis. Therefore, the differential diagnosis of liver dysfunction should be considered [8]. Liver transplantation (LT) may be a life-saving measure for patients with acute severe autoimmune hepatitis (AS-AIH), decompensated chronic AIH, hepatocellular carcinoma, or acute liver failure (ALF) caused by these conditions. Up to 10% to 50% of patients have been documented to experience recurrent illness following LT, and both pediatric and adult liver transplant recipients have also been known to experience the start of de novo (AIH) [9]. Currently, there are very few reports on autoimmune hepatitis. There has not been much research conducted in Yemen that focused on autoimmune hepatitis titis in Yemenis before this study. Our research started a thorough investigation into autoimmune hepatitis in Yemeni patients, exploring the biochemical, clinical, and long-term effects. All patients with this diagnosis, who were under close observation at the Science and Technology Hospital in Sanaa, Yemen, during the study period, were included.
Methods
Study Design and Participants
The simplified International Autoimmune Hepatitis Group diagnostic score method was used in this retrospective assessment of patients with autoimmune hepatitis diagnoses [10]. Between 2019 and 2024, the Science and Technology Hospital in Sanaa, Yemen. All patients diagnosed with autoimmune hepatitis in different age groups and those with incomplete information at the time of diagnosis were excluded. Laboratory data (immunological markers and elimination of other infectious or metabolic differential diagnoses) were used to diagnose AIH.
Collection of Data
In order to gather a variety of information, including test data such as liver function markers, liver enzyme levels, total and direct bilirubin, and complete blood counts, the patients’ computerized medical records were carefully examined. Immunological markers, such as ASMA, anti-smooth muscle antibody, antinuclear antibody, AMA, and anti-mitochondrial antibody, were also collected. Our study evaluated patient outcomes and found improvements in liver enzymes, synthetic function, and immunological markers. Remission is described as both biochemical and immunological.
Statistical Analysis
Excel was used to enter the data that were gathered and then extracted to Epi-Info version 2.7 for analysis. Univariate analysis was used to describe each variable. Means and ranges were calculated. The data are presented in tables and graphs.
Results
This study included 25 patients with an average age of 38 years (range: 16–78 years). The majority were male (18 out of 25, 72%). All the patients exhibited typical symptoms and signs associated with AIH, such as jaundice, vomiting, abdominal distention, and hepatomegaly. The most common symptoms reported were jaundice (68%), vomiting (52%).
Abdominal distention (48%) and hepatomegaly (42%) (Table 1).
The baseline laboratory data of patients with AIH are summarized in Table 2. Elevated transaminase levels were a consistent finding, with AST) elevation being the most common, observed in 22 patients (88%). The average AST level at presentation was 306 IU/L (range: 18–4367 IU/L). Thrombocytopenia was present in 16 patients (64%), with an average platelet count of 130 × 10⁹/L (range: 37–330). Abnormal alkaline phosphatase levels were detected in 18 patients (72%) (Table 2).
Table 3 details serology results for autoantibodies. ANA positivity was observed in 14 out of 23 tested patients (61%), while ASMA positivity was reported in all 22 patients who underwent testing.
Regarding the outcome after admission to the hospital, 60% of cases improved 12% discharged against medical advice,8% died, and 20% had unknown outcomes. See Figure 1.
After studying these cases, we found that all belonged to the first type and no recorded cases of the second type were found.
Discussion
Autoimmune hepatitis (AIH) is a condition that affects most people in Yemen. However, Yemen’s epidemiological study on the incidence and prevalence of AIH in the Yemeni community is nonexistent. This study is the first to report the clinical features and outcomes of Yemen. Moreover, the worldwide global incidence of Autoimmune Hepatitis affects 28 cases per 100,000 person-years, with a prevalence of 27,91 cases per 100,000 population as of 2022, representing an increase from 9,95 cases per 100,000 in 1970 [11]. Compared to Europe and America, the Asia-Pacific region has a lower prevalence and incidence of AIH [12]. In contrast to Western countries, autoimmune hepatitis is uncommon in Japan. Statistics show a steady rise in the number of diagnosed cases, with an emphasis on older age groups due to the aging population [13]. According to previous research, there are one–two cases per 100,000 people annually. However, most patients are diagnosed between the ages of 40 and 60 years, with women comprising the majority [14]. According to estimates, the prevalence ranges from 17.44 to 27.91 cases per 100,000 individuals, with Northern and Western European nations reporting higher rates than other regions worldwide. Comparable to the global average, the annual incidence rate in Europe is roughly 1.31 cases per 100,000. With a 4:1 female to male ratio, AIH is more frequently observed in women in Europe and can manifest at any time. Genetic predispositions and increased use of sophisticated diagnostic procedures may be the cause of the comparatively higher frequency in Northern Europe [15]. One of the main factors contributing to the high percentage of patients in the UK is the country’s dense population, which is part of the large increase in autoimmune hepatitis [16]. This leads to lack of sun exposure, vitamin D deficiency, and increased exposure to infections or environmental causes. Approximately 10% of the population is typically affected, with a higher frequency in women (13%) than in men (7%) [17]. In 2012, there were 24 cases of autoimmune hepatitis per 100,000 individuals worldwide, with a higher incidence among females in Denmark. The prevalence of AIH has increased over time [18]. An examination of the first five years of data from the Swiss Autoimmune Hepatitis Cohort Study showed that autoimmune hepatitis was treated and that the percentage of patients with primary biliary cholangitis variant syndrome was greater than expected. Additionally, the clinical characteristics of autoimmune hepatitis in Switzerland are similar to those observed in other cohorts [19]. Autoimmune hepatitis is a rare disease that is prevalent among women in the United States. It affects approximately 20 out of every 100,000 individuals worldwide, and the high prevalence of alcoholism and hereditary factors is thought to be the main cause of autoimmune hepatitis in the US [20]. Additionally, autoimmune liver disease is regarded as a rare illness compared with other regions with high rates of human development. However, because many countries on the continent have inadequate infrastructure and healthcare systems, the incidence rates might be less well-documented. The disease occurs in 15–25 cases per 100,000 people worldwide depending on age and sex. Approximately 70% to 80% of cases of autoimmune hepatitis occur in women; this is a global trend that also manifests in Africa [21]. The most prevalent age range for infection is between 30 and 50 years, and the impact of another immunological condition as well as delayed or absent diagnosis are the main causes of disease spread [22]. In Nigeria, autoimmune hepatitis is a lesser-known cause of liver illness than viral diseases, such as hepatitis B and C. Evidence suggests that estimates may be underestimated due to a lack of early detection and routine screening. According to various studies, the prevalence of AIH in Nigeria is estimated to be between 0.5 and 1 case per 100,000 population. Most patients are in severe stages of the disease, with individuals suffering from chronic liver cirrhosis or liver failure. The condition is more typically diagnosed in women than in men, especially throughout middle age [23]. The prevalence of autoimmune hepatitis in the Arab region ranges from 0.7 and 2.0 per 100,000 individuals per year, which is comparable to the global rate of 1–2 per 100,000 people. Most individuals are diagnosed at middle age (40–50 years); however, this condition can present at any age. In Jordan, autoimmune hepatitis (AIH) is a disease with an increasing number of diagnosed cases [5]. Patients with AIH were predominantly female, regardless of ethnicity. Several theories have been proposed to explain the phenomenon. Sex hormones affect innate immunity and gene activation on the X chromosome as well as epigenetic and microbial factors. However, the exact mechanism of action is not completely understood [24]. AIH was more prevalent in men (72%), according to our analysis, which contradicts findings from prior research The reason may possibly because the percentage of men who chew khat is higher than the percentage of women, as some studies have proven that chew khat stimulates autoimmune hepatitis [25]. AIH can manifest as gradual, acute, or fulminant disease. Autoimmune hepatitis may be asymptomatic in 25% of cases. AIH symptoms range from asymptomatic to fulminant. In addition, 25%-75% of patients with AIH have an abrupt onset (lasting less than 30 days) [26].In our study, jaundice was the most commonly reported symptom (68%) Interestingly, none of the individuals in our study were asymptomatic diagnosis elevated transaminase levels. Elevated serum transaminases (AST and ALT) are prominent indicators of autoimmune hepatitis, although an increase in ALP level is less prevalent. Transaminase levels are useful for monitoring disease activity but may not necessarily indicate disease severity in our study, and consistently higher levels of transaminases were found. Detected autoantibodies (ANA or SMA) are a part of the diagnosis of AIH. ANA/SMA is linked to type 1 AIH, whereas LKM-1 antibodies are involved in type 2 AIH [27]. A pediatric study in Jordan reported ANA (approximately 65%), AMA (30.8), and ASMA (56.3%) positivity [5]. This is consistent with our findings (ANA: 61%), AMA: 93%, and ASMA: 100%). Occasionally, idiopathic thrombocytopenic purpura (ITP) coincides with autoimmune hepatitis (AIH) [28]. Remarkably, anemia in our study was 14 (56%), and thrombocytopenia was present in 16 patients (64%), with an average platelet count of 130 × 10⁹/L (range: 37–330). In contrast to the Jordan study, thrombocytopenia was 40%. Moreover, routine lifelong follow-up after the maintenance of remission after treatment is crucial. Research conducted in Egypt, Saudi Arabia, and Jordan has revealed differing relapse tendencies and remission rates [29]. In this study regarding the outcome after admission to the hospital, 60% of cases improved, 12% were discharged against medical advice,8% died, and 20% had unknown outcomes. This study provides insights into the clinical findings, serological markers, and outcomes of this cohort, making it the first to investigate autoimmune hepatitis among Yemeni individuals. However, this study had several limitations. The results of this single-site study might not accurately reflect those of Yemen, even though it was conducted at a significant referral facility in Sana’a. Furthermore, the limited number of patients and rarity of AIH may limit the broad application of these results may be applied. Another significant drawback is the paucity of data, particularly regarding anti-LKM and liver biopsy histological tests.
Conclusion
Our work clarifies the prevalence and key features of autoimmune hepatitis in Yemenis and sheds light on this particular community. In addition, a higher prevalence was observed in male patients. However, the single-center retrospective design of our study has drawbacks such as a small sample size and short follow-up period. Prospective multicenter investigations are required to overcome these limitations. Establishing a specialized liver transplantation program is imperative, as evidenced by the mortality rate in our cohort and the number of patients awaiting liver transplantation. This significant action represents a national investment aimed at alleviating suffering and reducing the high expenses of pursuing comparable interventions.
Declarations
Ethics Approval and Consent to Participate
This analysis was performed in accordance with the local legislation and followed to the Helsinki Declaration. Moreover, the Research Ethics Committees of Faculty of Medicine and Health Science at Ibb University approved the ethical statement for achieving this investigation. Furthermore, an official letter was written to the Science and Technology Hospital in Sana’a Governorate, the Public Health Office of the Ibb Governorate granting permission for using of database data for this purposes. Additionally, due to the retrospective nature of the study, the Article 51 of the Yemeni Public Health Law No. (4) 2009 waived the need for informed consent. Secret codes were used to protect the personal identity of the cases, and all data analysis was conducted as anonymous.
Clinical Trial
Not applicable.
Consent for publication
All authors have read and accepted the final version of the work, and they agree to its publication.
Availability of data and material
All data and materials supporting the final results are presented in the manuscript.
Competing interests
The authors declare no competing interests.
Funding
Funding organizations have not provided the authors with any financial assistance for this work.
Author Contributions
A.R. does the initial draft of the manuscript and writes the manuscript. A.M and K.A edited and co-wrote subsequent versions. A.A. and W.A. finalised the manuscript and coordinated the study. The final has been reviewed and approved by all writers.
Acknowledgments
The authors thank the manager of the the Science and Technology Hospital in Sana’a Governorate for providing the data for this study.
Abbreviations
| AIH | Autoimmune hepatitis |
| ANA | Anti-nuclear antibodies |
| ASMA | Anti-smooth muscle antibodies |
| AST | Aspartate aminotransferase |
| ALT | Alanine aminotransferase |
| SMA | Smooth muscle antibodies |
| anti-LKM-1 | Anti-liver-kidney microsomal antibody |
| anti-LC-1 | Anti-liver cytosolic antigen type 1 |
| ALF | Acute liver failure |
References
- Muratori, L., A.W. Lohse, and M. Lenzi, Diagnosis and management of autoimmune hepatitis. Bmj, 2023. 380: p. e070201.
- Sucher, E., et al., Autoimmune Hepatitis-Immunologically Triggered Liver Pathogenesis-Diagnostic and Therapeutic Strategies. J Immunol Res, 2019. 2019: p. 9437043.
- Mack, C.L., et al., Diagnosis and Management of Autoimmune Hepatitis in Adults and Children: 2019 Practice Guidance and Guidelines From the American Association for the Study of Liver Diseases. Hepatology, 2020. 72(2): p. 671-722.
- Shiffman, M.L., Autoimmune Hepatitis: Epidemiology, Subtypes, and Presentation. Clin Liver Dis, 2024. 28(1): p. 1-14.
- Altamimi, E., et al., Retrospective, single-center analysis of autoimmune hepatitis in Jordanian children: clinical features, treatments, and outcomes. BMC Pediatr, 2024. 24(1): p. 102.
- Tan, C.K., et al., Drug-induced autoimmune hepatitis: A minireview. World J Gastroenterol, 2022. 28(24): p. 2654-2666.
- Mroskowiak, A., et al., Autoimmune Hepatitis-Challenging Diagnosis. Medicina (Kaunas), 2022. 58(7).
- Covelli, C., et al., Pathology of autoimmune hepatitis. Pathologica, 2021. 113(3): p. 185-193.
- Özaslan, E., et al., Diagnosis and Treatment of Autoimmune Hepatitis: Questions, Answers, and Illustrative Cases: Endorsed by Autoimmune Liver Diseases Special Interest Group, Turkish Association for the Study of Liver. Turk J Gastroenterol, 2023. 34(Suppl2): p. S1-s33.
- Hennes, E.M., et al., Simplified criteria for the diagnosis of autoimmune hepatitis. Hepatology, 2008. 48(1): p. 169-76.
- Hahn, J.W., et al., Global incidence and prevalence of autoimmune hepatitis, 1970-2022: a systematic review and meta-analysis. EClinicalMedicine, 2023. 65: p. 102280.
- Yang, F., et al., Autoimmune hepatitis: East meets west. J Gastroenterol Hepatol, 2015. 30(8): p. 1230-6.
- Ohira, H., et al., Autoimmune hepatitis: recent advances in the pathogenesis and new diagnostic guidelines in Japan. Intern Med, 2015. 54(11): p. 1323-8.
- Takahashi, A., et al., Autoimmune hepatitis in Japan: trends in a nationwide survey. J Gastroenterol, 2017. 52(5): p. 631-640.
- van Gerven, N.M., et al., Epidemiology and clinical characteristics of autoimmune hepatitis in the Netherlands. Scand J Gastroenterol, 2014. 49(10): p. 1245-54.
- Gordon, V., et al., Treatment and Outcome of Autoimmune Hepatitis (AIH): Audit of 28 UK centres. Liver Int, 2022.
- Gordon, V., et al., Diagnosis, presentation and initial severity of Autoimmune Hepatitis (AIH) in patients attending 28 hospitals in the UK. Liver Int, 2018. 38(9): p. 1686-1695.
- Gantzel, R.H., et al., The prevalence and disease course of autoimmune liver diseases in Greenland. Int J Circumpolar Health, 2024. 83(1): p. 2327693.
- Ludz, C., et al., Epidemiology, clinical features and management of autoimmune hepatitis in Switzerland: a retrospective and prospective cohort study. Swiss Med Wkly, 2023. 153: p. 40102.
- Bittermann, T., et al., Sociodemographic and geographic differences in the US epidemiology of autoimmune hepatitis with and without cirrhosis. Hepatology, 2023. 77(2): p. 367-378.
- Maharaj, Y. and V.G. Naidoo, Diagnosis and presenting features of autoimmune hepatitis at a central referral hospital in South Africa. S Afr Med J, 2024. 114(4).
- Afaa, T.J., et al., Clinical characteristics of paediatric autoimmune hepatitis at a referral hospital in Sub Saharan Africa. PLoS One, 2020. 15(12): p. e0239964.
- Ugonabo, O. and K. Chudy-Onwugaje, Autoimmune Hepatitis Disguised as Iron Overload Syndrome: Diagnostic Dilemma in a Nigerian Man. J Investig Med High Impact Case Rep, 2023. 11: p. 23247096231175442.
- Invernizzi, F., et al., Gender and Autoimmune Liver Diseases: Relevant Aspects in Clinical Practice. J Pers Med, 2022. 12(6).
- Orlien, S.M.S., et al., High Seroprevalence of Autoantibodies Typical of Autoimmune Liver Disease in Eastern Ethiopia: Is Chewing of Khat (Catha edulis) a Triggering Factor? Can J Gastroenterol Hepatol, 2018. 2018: p. 4980597.
- Schmeltzer, P.A. and M.W. Russo, Clinical narrative: autoimmune hepatitis. Am J Gastroenterol, 2018. 113(7): p. 951-958.
- Xi, D., H. Lin, and A.A. Shah, Overview of autoimmune liver disease: Prevalence, risk factors, and role of autoantibodies. Clin Liver Dis (Hoboken), 2022. 20(4): p. 111-115.
- Fukuda, H., et al., Autoimmune Hepatitis with Concomitant Idiopathic Thrombocytopenic Purpura Diagnosed by Transjugular Liver Biopsy. Case Reports Hepatol, 2018. 2018: p. 5305691.
- Abu Faddan, N.H., et al., Clinico-laboratory study on children with auto-immune hepatitis in Upper Egypt. Arab J Gastroenterol, 2011. 12(4): p. 178-83.
Figure 1.
Outcomes of admission at hospital for patients with autoimmune hepatitis.
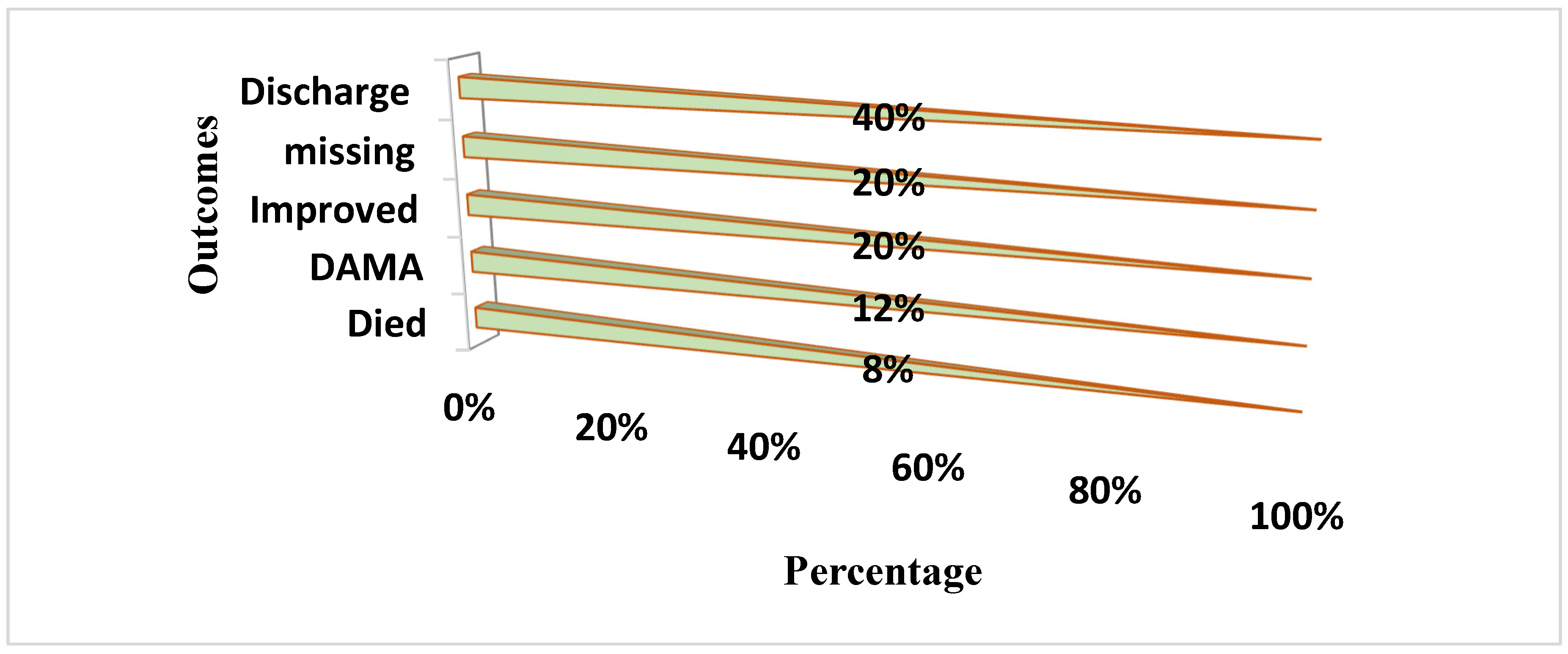

Table 1.
Demographic and clinical features at the presentation.
| Characteristics n=25 | Frequencies |
|---|---|
|
Age at presentation Average ± SD Age range |
38.7 ±15.3 16-78 |
|
Gender Male Female |
18(72%) 7(28%) |
|
Clinical features at presentation: Jaundice Emesis Abdominal distention Edema Hepatomegaly Splenomegaly Excessive itching Bleeding Encephalopathy Acute liver failure |
17(68%) 13(52%) 12(48%) 7(28%) 10(42%) 8(32%) 2(8%) 2(8%) 4(16%) 3(12%) |
Table 2.
Baseline blood examination at presentation.
| Characteristics |
Average (range) | Abnormal results N (%) |
|---|---|---|
|
Hb (g/dl) |
12(8-17) | 14 (56%) |
|
WBC (× 109) |
9.1(2.5-43.7) | 10 (40%) |
| Platelet (× 109) | 130(37-330) | 16 (64%) |
|
ALT (IU/L) |
350(12-6276) | 21(84%) |
|
AST (IU/L) |
306(18-4367) | 22 (88%) |
|
Albumin (g/dl) |
2.9(0.9-4.3) | 19 (76%) |
| Total Bilirubin (mg/dL) | 12(0.5-32) | 23(92%) |
| Alkaline phosphatase (IU/L) | 220(19-918) | 18 (72%) |
Table 3.
Serology rates of Autoantibodies of patients.
| Serology markers | Positivity rates |
|---|---|
| ANA | 14 out of 23 (61%) |
| AMA | 13 out of 14(93%) |
| ASMA | 22 out of 22 (100%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



