
Submitted:
08 April 2025
Posted:
24 April 2025
Read the latest preprint version here
Abstract
Colorectal cancer (CRC) with liver metastases (LM) and peritoneal metastases (PM) presents a formidable challenge, with poor prognosis despite advances in systemic chemotherapy and combined surgical approaches like cytoreductive surgery (CRS) and hyperthermic intraperitoneal chemotherapy (HIPEC). Median overall survival (OS) for unresactable cases ranges from 12–24 months with mod- ern regimens (e.g., FOLFOX/FOLFIRI + targeted therapies), yet conversion to resectable disease remains limited by disease extent and treatment toxicity. This paper proposes that medicinal mush- room extracts, particularly polysaccharopeptides (e.g., PSK and PSP) from Trametes versicolor and bioactive compounds from species like Ganoderma lucidum, could enhance conversion therapy out- comes in CRC with LM and PM. Evidence from preclinical and clinical studies demonstrates that these extracts exert anticancer effects through multiple mechanisms, including suppression of mul- tidrug resistance, immune checkpoint blockade (e.g., PD-1/PD-L1), regulation of oncogenic signaling pathways (e.g., PI3K/AKT, MAPK, NF-κB), and robust immunomodulation. Clinical trials, including meta-analyses of over 8,000 patients, report improved survival and tolerability when combined with chemotherapy, primarily in postoperative settings. Our own meta-analysis involving a total of 2397 patients finds a 10% relative increase in the probability of survival at 5 years compared to the ref- erence group, with a survival risk ratio (RR) of 1.10 (95% CI: 1.04–1.15). The author hypothesizes that integrating these extracts into preoperative regimens could enhance the efficacy of chemother- apy, increase surgical eligibility (e.g., R0 resection rates), and mitigate toxicity, potentially extending OS beyond current benchmarks (e.g., 26–48 months with CRS-HIPEC). While direct evidence in un- resectable CRC with dual metastases is lacking, the biological plausibility and safety profile of mush- room extracts warrant prospective trials to validate their role in conversion therapy.
Keywords:
Colorectal Cancer
; Liver Metastases
; Peritoneal Metastases
; Conversion Therapy
; Medicinal Mushrooms
; Trametes versicolor
; Ganoderma lucidum
; Grifola frondosa
; Lentinula edodes
; Agaricus blazei
; Inonotus obliquus
; Polysaccharopeptide Krestin
; Systemic Chemotherapy
; Cytore-ductive Surgery
; Hyperthermic Intraperitoneal Chemotherapy
; Immunomodulation
; Multidrug Resis-tance
; Surgical Eligibility
; Overall Survival
; Progression-Free Survival
1. Background and Disease Context
Colorectal cancer (CRC) is a leading cause of cancer-related mortality, with metastases significantly impacting prognosis. The peritoneum and liver are common sites of spread, with peritoneal metastases (PM) occurring in 8% to 15% of patients during the first treatment cycle [1] and liver metastases (LM) in up to 15% to 25% at diagnosis [2]. When both sites are involved, the disease is particularly challenging, traditionally associated with poor outcomes due to its extensive nature.
1.1. Assessment of the Efficacy of Systemic Chemotherapy as a Standalone Treatment
Systemic chemotherapy, typically administered intravenously, aims to control cancer spread and prolong survival. For patients with peritoneal carcinomatosis studies indicate a median survival of 6 to 9 months without treatment [3], extending to 12 to 24 months with systemic chemotherapy alone, depending on the regimen and patient characteristics [1,4,5,6,7]. For patients with both PM and LM, the prognosis is likely worse, with median survival potentially under 12 months at the lower end, though specific data for this subgroup is limited. Older studies using 5-fluorouracil (5-FU) and leucovorin showed disappointing results, with survival rarely exceeding 8 months [3]. Modern regimens, such as FOLFOX (5-FU, leucovorin, oxaliplatin) and FOLFIRI (5-FU, leucovorin, irinotecan), combined with targeted therapies like bevacizumab or cetuximab, have improved outcomes, but the response is lower for PM compared to LM [8].
A pooled analysis from the ARCAD CRC database, involving 17,924 patients, showed that compared to patients with LM (including those with additional sites like peritoneum) in the chemotherapy (CT) alone and CT + anti-vascular endothelial growth factor (VEGF) subgroups, non-liver metastases (NLM) patients had better overall survival (OS) and progression-free survival (PFS) within first-line and second-line settings. However, among patients with RAS wild-type status in the CT + anti-epidermal growth factor receptor (EGFR) first-line and second-line subgroups, there was no significant difference in OS and PFS between NLM and LM patients [9].
These findings suggests that while chemotherapy can induce responses depending on regimen and patient characteristics, the presence of multiple metastases, especially including LM and PM, reduces long-term survival. New treatment regimens are being developed to address the challenges of advanced, initially unresectable metastatic colorectal cancer (mCRC), such as the combination of FOLFOXIRI (which includes 5-FU, leucovorin, oxaliplatin, and irinotecan) with bevacizumab. The TRIBE trial, a large phase III clinical study involving 508 patients, compared this regimen to FOLFIRI plus bevacizumab. The results showed a median PFS of 12.1 months for the FOLFOXIRI group compared to 9.7 months for the FOLFIRI group, while the OS was 31.0 months versus 25.8 months, respectively [10]. The inclusion criteria for this treatment require an ECOG performance status score of 2 or less. The TRIBE trial included only patients aged 18 to 75 years, with those over 70 needing an ECOG score of 0. An individual patient data (IDP) meta-analysis conducted in 2020 with data from 5 elegible trials, including the TRIBE trial, concluded, with statistically significant results, that FOLFOXIRI + bevacizumab improves OS when compared with doublets + bevacizumab, with a median OS of 28.9 versus 24.5 months, longer PFS of 12.2 versus 9.9 months, and higher R0 resection rate, 16.4% versus 11.8%, respectively. However, a higher burden of grade 3 and 4 adverse events is also observed, with some events being approximately double the rate compared to the control group. [11].
According to the latest guidelines from the American Society of Clinical Oncology (ASCO) for patients with previously untreated, initially unresectable mCRC, doublet chemotherapy should be offered, while triplet therapy may be considered based on studies involving chemotherapy combined with anti-VEGF antibodies. In the first-line setting, pembrolizumab is recommended for patients with mCRC that has microsatellite instability-high (MSI-H) or deficient mismatch repair (dMMR) tumors. For microsatellite stable (MSS) or proficient mismatch repair (pMMR) left-sided RAS wild-type mCRC, chemotherapy combined with anti-EGFR therapy is recommended, whereas chemotherapy combined with anti-VEGF therapy is recommended for MSS or pMMR right-sided RAS wild-type mCRC. For patients with previously treated BRAF V600E-mutant mCRC that has progressed after at least one line of therapy, encorafenib plus cetuximab is recommended. In cases of colorectal peritoneal metastases, cytoreductive surgery plus systemic chemotherapy may be recommended for selected patients, although the addition of oxaliplatin-based hyperthermic intraperitoneal chemotherapy is not recommended. For patients with liver oligometastases who are not candidates for resection, stereotactic body radiation therapy may be recommended following systemic therapy, while selective internal radiation therapy is not routinely recommended for patients with unilobar or bilobar liver metastases. Additionally, perioperative chemotherapy or surgery alone should be offered to patients with mCRC who are candidates for potentially curative resection of liver metastases. The guidelines emphasize the importance of a multidisciplinary team management approach and shared decision-making to optimize patient care [12].
1.2. Combined Treatment Approaches and Comparative Outcomes
Given the limitations of chemotherapy alone, combined treatments have emerged as a more effective strategy. Cytoreductive surgery (CRS) aims to remove visible tumors, while hyperthermic intraperitoneal chemotherapy (HIPEC) delivers heated chemotherapy directly into the abdominal cavity to target residual disease. For patients with both PM and LM, studies show significant survival benefits when CRS, HIPEC, and liver resection or ablation are used. For instance, a systematic review and meta-analysis reported a median OS of 26.4 months with a 5-year OS rate of 25% for patients treated with CRS-HIPEC plus local liver treatment, compared to 6 to 13 months with systemic chemotherapy alone, according to their own metrics [13]. Another study, focusing on 565 patients, found that preoperative systemic chemotherapy followed by combined surgery and HIPEC resulted in a 48-month median OS, highlighting the potential of multimodal strategies [14]. A total of 491 patients (91.9%) underwent preoperative systemic chemotherapy before surgery to target peritoneal and/or liver metastases prior to CRS with HIPEC and liver resection (LR). The average interval between the diagnosis of liver or peritoneal metastases and the combined surgical intervention was six months, highlighting the urgent need for rapid adjunctive therapies to optimize the effectiveness of chemotherapy.
These outcomes contrast sharply with chemotherapy alone, suggesting that the efficiency of systemic chemotherapy is significantly enhanced when integrated into a multidisciplinary strategy. A clear example of this approach has been presented in a systematic review and pooled analysis of 11 studies regarding the potential of FOLFOXIRI plus bevacizumab as a conversion therapy. The eligibility for surgery after first-line chemotherapy in patients with unresectable mCRC was 39.1% with 28.1% of patients achieving R0 resection [15].
1.3. Patient Selection and Challenges
Not all patients are candidates for combined treatments due to factors like disease extent, performance status, and comorbidities. The peritoneal cancer index (PCI) and completeness of cytoreduction score (CC score), as well as the number of liver lesions, are critical in determining eligibility. A higher PCI (>20), non achievable complete cytoreduction (CC-0), or near-complete cytoreduction with residual tumor <2.5mm (CC-1), as well as the presence of more than two or three liver lesions, often contraindicate CRS [22]. Additionally, signet ring cell histopathology has also been considered a relative contraindication [13]. Systemic chemotherapy may serve as a bridge to surgery in some cases, converting unresectable disease to resectable, but its standalone efficiency remains limited for extensive multi-organ involvement. Since approximately 25% of colorectal cancer cases are diagnosed at stage IV at first presentation [23,24], there is an urgent need for adjunctive therapies that could increase the number of patients eligible for surgery.
1.4. Treatment-Specific Survival Rates with Peritoneal Involvement
Survival rates vary significantly based on the treatment received, highlighting the importance of patient selection and multidisciplinary management. A 2021 review detailed outcomes for different treatment modalities for CRC patiens with PM [1], as summarized in Table 1. This table illustrates that CRS + HIPEC can significantly extend survival in selected patients, with median OS reaching up to 62.7 months in some case-control studies, compared to 12 to 24 months with systemic chemotherapy alone, as we previously indicated. However, the PRODIGE 7 trial (2021) questioned the added value of Oxaliplatin-based HIPEC over CRS alone, showing no significant difference in median OS (41.7 vs. 41.2 months), suggesting the need for a reevaluation of the additional benefit of HIPEC within current practices and methodologies. In contrast, a phase III RCT in 245 ovarian cancer patients showed HIPEC benefits median OS (45.7 vs. 33.9 months); though differences in disease and protocol limit direct comparison [25,26]. PRODIGE 7’s design has also been critiqued [27]. The GECOP-MMC trial, a phase IV, multicenter, randomized, open-label study, aims to address this evidence gap. Initiated in March 2022, it compares CRS plus HIPEC with high-dose Mitomycin-C (35 mg/m2) to CRS alone in patients with limited peritoneal metastases from colon cancer (not rectal), with a focus on preventing peritoneal recurrence [28]. Study completion is estimated for 2029, representing a significant ongoing effort to clarify Mitomycin-C HIPEC’s efficacy.
2. Anticancer Mechanisms of Action in Selected Medicinal Mushrooms
Medicinal mushrooms have garnered attention for their potential anti-cancer properties, with Coriolus versicolor (now classified as Trametes versicolor), commonly known as Turkey Tail, standing out due to its extensive study and clinical use, particularly in Japan and China. Compounds like Polysaccharide-K (PSK, krestin) and Polysaccharide Peptide (PSP) from Coriolus have been approved as adjuvant therapies in certain regions, suggesting their potential efficacy in enhancing treatment outcomes. Here we explore the mechanisms by which a selected number of mushrooms species —Coriolus (Trametes versicolor), Reishi (Ganoderma lucidum), Maitake (Grifola frondosa), Shiitake (Lentinula edodes), Sun Mushroom (Agaricus blazei), and Chaga (Inonotus obliquus)— combat cancer, emphasizing evidence from in vitro, animal, and human studies. While Coriolus is the focal point, findings from other species provide a broader context for mushroom-based therapies. A recent review, published in the International Journal of Molecular Sciences (2022), highlights several anticancer mechanisms, targeting P-gp-mediated multidrug resistance, immune checkpoints (PD-1/PD-L1, CTLA-4/CD80), and signaling pathways (PI3K/AKT, Wnt/-catenin, MAPK, NF-B), while bolstering immunomodulation [29].
2.0.1. Suppression of Multidrug Resistance
P-glycoprotein (P-gp), also known as multidrug resistance protein 1 (MDR1), encoded by the ABCB1 gene, is an ATP-dependent efflux pump that contributes to multidrug resistance (MDR) by expelling chemotherapeutic agents from cancer cells, reducing their intracellular concentration and efficacy. MDR is a major challenge in cancer treatment, and inhibiting P-gp is a strategy to enhance drug effectiveness. Medicinal mushrooms, known for their bioactive compounds, have been studied for various therapeutic properties, including potential effects on cancer and drug resistance. Some medicinal mushrooms can inhibit P-gp to restore drug sensitivity. Extracts of several species of Ganoderma have been shown to induce apoptosis in both drug-sensitive (H69) and multidrug-resistant (VPA) human small-cell lung cancer (SCLC) cells, reducing the for etoposide and doxorubicin [30]. Additionally, polysaccharides from Ganoderma lucidum (GL-PS) supress the persistent activation of nuclear factor kappa-light-chain-enhancer of activated B cells (NF-B), leading to a decrease in the expression of P-gp in cancer cells [29,31]. Two edible mushrooms, Agaricus bisporus and Pleurotus ostreatus, have been studied for their tryptophan derivatives, specifically 5-hydroxy-L-tryptophan (5-HTP) and L-tryptophan (L-Trp). A 2021 BioTechnologia study, demonstrates that these compounds inhibit P-gp, with 5-HTP achieving 82% dye accumulation and L-Trp 47%. Docking reveals serotonin, a 5-HTP metabolite, binds P-gp at -83.93 kcal/mol, while L-Trp scores -64.38 kcal/mol. This suggests their potential as natural adjuvants to enhance chemotherapy by overcoming MDR. However, the study’s in vitro focus and absence of in vivo or clinical cancer data limit immediate applicability, and bioavailability remains untested [32].
2.0.2. Blockade of Immune Checkpoints
Medicinal mushrooms can also enhance immune responses by inhibiting checkpoints that suppress T-cell activity, countering cancer immune evasion. -Glucan, a high-molecular-weight polysaccharide, serves as a significant pathogen-associated molecular pattern (PAMP) present in fungi, bacteria, and other species [33], enhancing both innate and adaptive immune responses. When used alongside programmed cell death protein 1 (PD-1)/PD-ligand 1 (PD-L1) checkpoint-blocking antibodies, whole glucan particle (WGP) -glucan improves immune cell recruitment, balances T cell activation and tolerance, and delays tumor progression. This combination therapy has been shown to increase progression-free survival in advanced cancer patients who previously discontinued anti-PD-1/PD-L1 therapy [34]. This is particularly relevant in MSI-H or dMMR tumors in CRC, where immunotherapy with agents such as Pembrolizumab —an anti-PD-1 antibody that inhibits the PD-1 receptor on T-cells, thereby enhancing the immune response against cancer cells— has demonstrated significant improvements in PFS compared to chemotherapy (median, 16.5 vs. 8.2 months; KEYNOTE-177 trial) [35]. Additionally, Ganoderma lucidum and its bioactive compounds can lower PD-1 protein levels in cultured human B-lymphocytes, indicating their potential for cancer prevention and treatment through immune modulation [36]. PSP from Trametes versicolor inhibits CRC cell proliferation. Using human CRC cell lines (HCT116 and HT29), a 2022 study demonstrates that PSP significantly reduces cell growth by down-regulating the expression of epidermal growth factor receptor (EGFR) and PD-L1, along with key signaling molecules like STAT3 and c-Jun. PSP also enhances T-cell-mediated killing of CRC cells by lowering PD-L1 levels, suggesting its potential as a prophylactic and therapeutic agent against CRC through immune modulation and EGFR pathway inhibition [37]. Inonotus obliquus also blocks the interactions between cytotoxic T-lymphocyte-associated protein 4 (CTLA-4) and CD80 (also known as B7-1), increasing T-cell activity to prevent immune evasion [38].
2.0.3. Regulation of Signaling Pathways
Polysaccharides derived from edible and medicinal mushrooms enhance immune function and interact with various cell signaling pathways, such as NF-B, MAPK, and PI3K/Akt, which are crucial in cancer development. Given the limitations of current cancer treatments, mushroom polysaccharides present a promising alternative due to their natural origin and low toxicity [39]. The phosphoinositide 3-kinase (PI3K)/protein kinase B (AKT) pathway promotes cancer cell survival and resistance; its inhibition induces apoptosis and sensitizes cells to therapy. Ganoderic acid inactivates PI3K/AKT signaling, inducing apoptosis and autophagy in human glioblastoma cells [40]. Dysregulated Wnt/-catenin signaling drives tumor growth and metastasis; inhibition reduces proliferation and enhances immune infiltration. Inonotus obliquus ergosterol peroxide reduces nuclear -catenin in colorectal cancer cells, decreasing the expression of target genes, including c-myc, cyclin D1, CDK-8, and vascular endothelial growth factor (VEGF) [41,42]. The mitogen-activated protein kinase (MAPK) pathway contributes to oncogenesis and resistance to PD-1 blockade; its suppression enhances chemosensitivity and inhibits tumor growth. The -Glucan Lentinan, derived from Lentinula edodes, suppresses cisplatin-induced PD-L1 expression via MAPK inhibition, restoring chemosensitivity in gastric cancer cells [43]. Triterpene extracts, from Ganoderma lucidum, inhibit p38 MAPK phosphorylation, inducing autophagy in colon cancer cells [44]. Small molecules from Trametes versicolor inhibit the production of matrix metalloproteinase-3 (MMP-3), which is an enzyme that can facilitate tumor invasion and metastasis. This inhibition occurs indirectly by inactivating the p38 MAPK pathway [45]. NF-B promotes chemoresistance and tumor survival; its inhibition induces apoptosis and enhances therapy efficacy. As mentioned earlier, Ganoderma lucidum Polysaccharides inhibit NF-B, reducing P-gp expression [31]. Sulfated polysaccharides from Grifola frondosa induce apoptosis in HepG2 liver cancer cells by inhibiting Notch1 expression, degrading IB-, and activating caspases 3 and 8, which are part of a Notch1/NF-B/p65-mediated apoptotic pathway. [46].
2.0.4. Immunomodulation
In relation to immunomodulatory effects, Ganoderma lucidum -glucans and triterpenoids protect normal cells, reduce fatigue, and improve symptoms in patients with lung and breast cancer [47,48]. Extracts from the edible mushrooms Grifola frondosa have been shown to enhance the activity of natural killer (NK) cells and stimulate the production of various cytokines, including interferon (IFN)- and interleukin (IL)-12. A phase I/II clinical trial involving breast cancer survivors demonstrated that oral administration of Maitake extract was well tolerated and resulted in significant immunological changes, with an optimal dose of 5–7 mg/kg per day associated with increased production of tumor necrosis factor (TNF)- and both stimulatory (IL-2, IFN-) and suppressive (IL-10) cytokines. These findings suggest that Maitake extract may modulate immune responses, potentially benefiting cancer patients, although further research is needed to clarify its clinical significance and optimal dosing [49]. Aqueous extracts of Lentinula edodes can inhibit the proliferation of human breast cancer cells while enhancing the proliferation of rat thymocytes, indicating its potential as an immunostimulant [50], with lentinan enhancing cytotoxic T lymphocytes and macrophage proliferation [51]. Agaricus blazei polysaccharides mitigate chemotherapy side effects in gynecological cancer patients receiving chemotherapy [52], and increase dendritic and T-regulatory cells in myeloma patients [53]. Extracts from Trametes versicolor, notably polysaccharopeptides PSP/PSK, exhibit significant immunomodulatory effects, enhancing antitumor immunity. PSP induces a pro-inflammatory cytokine profile, including TNF-, IL-1, IL-12, and IL-6, via pathways involving TLR2, Dectin-1, and partially TLR4, as evidenced by preclinical studies [54]. Notably, PSP increased TNF- secretion >3.5-fold in human PBMCs in vitro [55], demonstrating potent immunostimulation, while in vivo, PSP-treated mice with H238-derived tumors showed elevated TNF- expression in tumor specimens [56], linking cytokine induction to tumor microenvironments and potential tumor necrosis effects. These findings underscore PSP’s capacity to activate NK cells and overcome tolerogenic barriers, supporting its clinical use as an adjunct cancer therapy in Eastern cultures. In contrast, small molecules derived from Trametes versicolor demonstrate significant immunomodulatory properties by inhibiting the production of TNF- induced by lipopolysaccharide (LPS) while enhancing the levels of IFN- induced by polyinosinic:polycytidylic acid (poly I:C) in peripheral blood mononuclear adherent cells (PBMac). These compounds exhibit both indirect anti-cancer effects by reducing MMP-3 production triggered by TNF- in glioblastoma T98G cells and direct effects by impairing the invasive capabilities of various malignant cell lines, including T98G, A549, and MDA-MB-231 [45]. The disruption of pro-inflammatory tumorigenic factors, as well as the anti-migratory effects of Trametes versicolor extract, have also been demonstrated in a wound healing assay, with a reduced production of IL-6, IL-8, and MMP-9 in cells stimulated by LPS, indicating the microenvironment-dependent modulatory capacity of these active compounds [57]. A small clinical trial involving 21 patients with advanced gastric cancer indicates that PSK can enhance overall survival, in part by inhibiting CD57(+) T cells, which are associated with a poor prognosis in this disease [58]. In another clinical trial, 30 rectal adenocarcinoma patients were randomly assigned to receive either standard chemoradiotherapy (CRT) or CRT with concurrent PSK administration. The findings indicated that the PSK group experienced a notable rise in natural killer cell counts in peripheral blood and an increase in cytotoxic T-cell counts in both peri-tumoral and normal mucosa, accompanied by a reduction in serum levels of immunosuppressive acidic protein. These findings suggest that combining PSK with preoperative CRT may enhance immune function and reduce local recurrence, leading to improved survival outcomes [59].
2.0.5. Induction of Cell Cycle Arrest
Regarding cell cycle arrest, a critical mechanism for controlling cancer cell proliferation, research suggests that Trametes versicolor extracts can induce cell cycle arrest at various phases, impacting cancer cell division. PSP isolated from Trametes versicolor has been shown to induce S phase cell arrest in HL-60 leukemia cells, enhancing the cell cycle-dependent activity and apoptotic cell death, when combined with chemotherapy drugs like doxorubicin and etoposide [60]. The Memorial Sloan Kettering Cancer Center reports that a Coriolus medicinal mushroom blend inhibited cell proliferation and induced G2/M cell cycle arrest in an invasive breast cancer cell line, linked to suppression of urokinase plasminogen activator [61,62]. Another study noted that polysaccharides from C. versicolor achieved cell cycle arrest at concentrations as low as 100 µg/mL in vitro; significant given their large molecular weight [63]. These findings indicate that Trametes versicolor extracts likely affect cell cycle regulatory genes, though the exact mechanisms may vary by cancer type and extract formulation. Apoptosis induction, or programmed cell death, is a key strategy for eliminating cancer cells. Evidence leans toward Trametes versicolor extracts promoting apoptosis through multiple pathways. One example has already been highlighted in relation to cell cycle arrest, since these two mechanisms are interrelated [60]. Similarly, water extracts of I’m-Yunity (PSP) have been shown to modulate apoptogenic and anti-apoptotic protein expression, inducing cell cycle changes and apoptosis in human leukemia HL-60 and U-937 cells [64].
2.0.6. Anti-Angiogenic Properties
Anti-angiogenic effects involve inhibiting new blood vessel formation, essential for tumor growth and metastasis. Trametes versicolor extracts can impact angiogenesis by reducing pro-angiogenic factors. An in vitro study found that protein-bound polysaccharides (PBP) from Trametes versicolor decreased VEGF and monocyte chemoattractant protein-1 (MCP-1) secretion by breast cancer cells, disrupting the tumor microenvironment and potentially inhibiting angiogenesis [65]. An in vivo study directly showed that fungal polysaccharopeptide inhibited tumor angiogenesis in mice, reducing blood vessel growth and tumor expansion [66].
2.0.7. Antimetastatic Effects
The protein-bound polysaccharide Krestin (PSK) derived from cultured mycelia of Trametes versicolor, exhibits significant antimetastatic properties, as explored in a 1995 review by Kobayashi and colleagues. Known for its role in thwarting early cancer development, PSK also hinders the spread of established tumors, reducing metastasis in chemically induced sarcomas and human prostate cancer DU145M, as well as lymphatic spread in mouse leukemia P388, while improving survival in spontaneous metastasis scenarios. It further curbs metastatic progression in controlled setups involving rat hepatoma AH60C, mouse colon cancer colon 26, and mouse leukemia RL male 1. PSK achieves this through diverse actions: It hampers tumor entry into blood vessels by limiting invasion and adhesion, disrupts tumor cell binding to vessel walls by reducing platelet clumping, restricts cancer cell movement after exiting circulation by slowing motility, and limits growth at new sites by blocking blood vessel formation, tweaking immune signals, and boosting immune cell activity. Additionally, PSK neutralizes harmful superoxide molecules, slowing tumor aggressiveness in mouse models. These properties highlight PSK’s broad potential to combat metastasis, enhancing its value in cancer therapy [67]. Complementing this, a study conducted in 2014 examined the effects of aqueous extract from Trametes versicolor on metastatic breast cancer using a mouse model (4T1). Administering the extract at a daily dose of 1 g/kg for four weeks led to a 36% decrease in tumor weight and a 70.8% reduction in lung metastasis. Additionally, the extract demonstrated protective effects on bone health, as indicated by increased bone volume observed in micro-CT imaging. In vitro experiments revealed that the extract (at concentrations of 1-2 mg/mL) effectively inhibited the migration and invasion of 4T1 cells, significantly reducing MMP-9 activity. Furthermore, it enhanced immune function by increasing the production of cytokines such as IL-2, IL-6, IL-12, TNF-, and IFN- in spleen lymphocytes [68]. Another study examined the direct effects of PSK on human colorectal adenocarcinoma cells (SW480 and HCT116) using protein microarrays. After 96 hours of PSK exposure, 14 proteins showed significant alterations, with ECA39 identified as a key candidate associated with PSK’s anti-metastatic effects [69]. Together, these findings position Trametes versicolor as a promising agent against metastasis, targeting invasion, migration, angiogenesis, and immune modulation.
2.1. Clinical Evidence and Broader Benefits
In the systematic review and meta-analysis by Zhong et al. (2019) [70], the synergistic potential of Trametes versicolor (Yun Zhi) and Ganoderma lucidum (Ling Zhi) as adjunctive therapies in cancer treatment is rigorously evaluated. This study, encompassing 23 randomized controlled trials and 4,246 cancer patients, demonstrates that natural products derived from these medicinal mushrooms significantly enhance therapeutic outcomes when combined with conventional cancer treatments. The meta-analysis reveals a reduced mortality risk (HR: 0.82; 95% CI: 0.72-0.94) and improved total efficacy (RR: 1.30; 95 % CI: 1.09-1.55) compared to control treatments, alongside immunomodulatory benefits, including elevated CD3 (MD: 9.03%; 95% CI: 2.10-16.50) and CD4 (MD: 9.2%; 95% CI: 1.01-17.39) levels. These effects are attributed to the synergistic action of bioactive compounds, such as polysaccharopeptides (e.g., PSP/PSK) from Trametes versicolor and beta-glucans and triterpenes from Ganoderma lucidum, which collectively enhance immune response and mitigate immunosuppression associated with chemotherapy or radiotherapy. Additionally, this combination therapy improved patients’ quality of life with minimal adverse effects, underscoring its safety profile offering a compelling foundation for integrating medicinal mushrooms into comprehensive cancer care strategies. While these findings position Trametes versicolor and Ganoderma lucidum as promising adjunctive agents across various cancer stages and types, the study highlights the need for further, large sample size, high-quality randomized controlled trials across different continents.
3. Medicinal Mushrooms as Adjunctive Therapy in Cancer Treatment: A Concise Summary
Medicinal mushrooms have emerged as valuable adjunctive therapies in cancer management, particularly due to their diverse bioactive compounds. Notably, Trametes versicolor (Coriolus) and Ganoderma lucidum (Reishi) have been extensively studied for their potential to enhance conventional cancer treatments. These fungi exhibit various mechanisms that contribute to their anticancer effects as potent biological response modifiers (Refer to Table 2 for summary).

Clinical studies have highlighted the synergistic effects of combining these mushrooms with standard cancer therapies, leading to improved survival rates and better therapeutic responses. However, further research is essential to establish standardized treatment protocols and confirm the clinical benefits of these natural products. The integration of medicinal mushrooms into cancer treatment regimens offers a promising strategy for enhancing therapeutic efficacy and patient well-being.
4. Review of Human Studies with a Focus on Medicinal Mushroom Compounds in Cancer Patients
A thorough investigation of the available literature has been conducted to assess the safety and efficacy of medicinal mushroom compounds in cancer patients, specifically focusing on Trametes versicolor and colorectal cancer. This investigation utilized several regularly updated review summaries on the subject, including those from the Memorial Sloan Kettering Cancer Center [61], the Whole Health Library website from the U.S. Department of Veterans Affairs [71], and the Physician Data Query (PDQ) summary provided by the National Cancer Institute (NCI) [72]. These review summaries are comprehensive, evidence-based resources that offer information on various aspects of cancer, including prevention, diagnosis, treatment, and supportive care.
4.1. Reishi (Ganoderma lucidum), Maitake D-Fraction (Grifola frondosa D-Fraction), Lentinan (Lentinula edodes Extract), and AHCC (Active Hexose Correlated Compound, Derived from Various Basidiomycetes)
The use of bioactive compounds derived from Ganoderma lucidum as an adjunctive to chemotherapy has long been suggested [73]. Patients receiving Ganoderma lucidum in combination with chemotherapy and/or radiotherapy were found to have a 1.27 times greater likelihood of responding compared to those receiving conventional treatment alone, according to a systematic review by the Cochrane Library, last updated in 2016 [74,75]. An improvement in quality of life was also observed as well as stimulation of host immune-mediated responses, with a markedly increase in CD3, CD4, and CD8 lymphocytes, and a slight increase in NK cells. Few cases of minor adverse effects, including nausea and insomnia, were reported. There is an ongoing randomized controlled trial (RCT) sponsored by the Second Affiliated Hospital, Zhejiang University [76], investigating the potential of Ganoderma lucidum spore powder as an adjunctive treatment for osteosarcoma, a cancer with a low 5-year survival rate of less than 20%. This Phase II trial evaluates the efficacy of Ganoderma lucidum combined with doxorubicin and cisplatin chemotherapy in a multicenter, double-blind design. Previous research indicates that Ganoderma lucidum may inhibit tumor growth and metastasis without significant toxicity, supporting its use in combination therapy. Japanese researchers investigated a water-soluble extract from the mycelia of Ganoderma lucidum (MAK) in patients with colorectal adenomas. The study involved 123 patients receiving 1.5 g/d of MAK for 12 months, compared to 102 control patients who received no treatment. After 12 months, the treatment group showed a significant reduction in the number of adenomas (-0.42 ± 0.10) and a decrease in total adenoma size (-1.40 ± 0.64 mm), while the control group experienced an increase in both the number of adenomas (+0.66 ± 0.10) and size (+1.73 ± 0.28 mm) (P < .01). These findings suggest that MAK may help suppress the development of premalignant colorectal adenomas [77]. In contrast, a Ganoderma sinense polysaccharide (GSP) tablet ,from a related species, is already approved in China since 2010 by the State Food and Drug Administration (SFDA) as an adjunctive therapy for addressing leukopenia and hematopoietic damage resulting from concurrent chemotherapy and radiation therapy [78].
Grifola frondosa D-fraction, a protein-bound polysaccharide containing beta-glucans and protein, has demonstrated an improved response rate to chemotherapy, increasing from 12% to 28% in a Japanese non-randomized clinical study involving 165 patients suffering from various types of advanced cancers [79,80]. In a non-randomized case series, the effectiveness of a combination of Grifola frondosa D-fraction and whole Grifola frondosa powder was evaluated in cancer patients aged 22 to 57 with stages II-IV cancer. The study found that 58.3% of liver cancer patients, 68.8% of breast cancer patients, and 62.5% of lung cancer patients experienced cancer regression or significant symptom improvement. In contrast, leukemia, stomach cancer, and brain cancer patients showed only a 10-20% improvement. Additionally, the combination of Grifola frondosa with chemotherapy enhanced immune-competent cell activities by 1.2 to 1.4 times compared to chemotherapy alone [81].
Lentinan, a polysaccharide extracted from the Lentinula edodes mushroom, is recognized for its antitumor and immunostimulatory properties and is commonly used in cancer treatment. It has been approved as an adjuvant therapy for cancer treatment in both China and Japan since the 1980s. An extensive review of over 9,474 patients from 135 independent studies in Chinese databases has summarized lentinan-associated cancer treatment cases over the past 12 years (2004-2016) utilizing data from CNKI (China National Knowledge Infrastructure), VIP (Chongqing VIP Chinese Scientific Journals Database), and Wanfang, demonstrating clear improvements in quality of life and enhanced effects of chemotherapy and radiation therapy [82].
AHCC, or Active Hexose Correlated Compound, is a functional food supplement developed at the University of Tokyo Faculty of Pharmaceutical Sciences by Dr. Toshihiko Okamoto, in collaboration with researchers at Amino Up Chemical Co., Ltd. in Japan. The primary component of AHCC is Lentinula edodes, known for their long-standing reputation for healing properties. Additionally, it contains various hybrids from the Basidiomycota phylum of fungi [83]. A small randomized controlled study was conducted with 44 patients who had histologically confirmed advanced liver cancer, all receiving supportive care. Among them, 34 patients received AHCC, while 10 received a placebo. The results indicated that patients treated with AHCC experienced significantly prolonged survival compared to the control group. Additionally, quality of life improved in areas such as mental stability and physical health after three months of treatment. Key clinical parameters, including albumin levels and lymphocyte percentages, also showed significant differences favoring the AHCC group. The study suggests that AHCC may enhance survival and prognosis in advanced liver cancer patients [84]. A pilot study examined the effects of AHCC in 11 patients with advanced cancer, including three each with prostate, breast, or ovarian cancer, and two with multiple myeloma. All patients received conventional therapies alongside 3 grams of AHCC daily. After two weeks, nine of the 11 patients exhibited a 2.5-fold increase in NK cell activity, which was sustained over time. Additionally, the three prostate cancer patients showed a decline in prostate-specific antigen (PSA) levels, indicating reduced malignancy. Normal levels were reached in 1 to 2 months post treatment. Among the breast cancer patients, two experienced a significant decrease in CA-125 levels, with levels returning to normal 3 to 4 months after starting AHCC treatment. This study serves as a preliminary exploration of AHCC’s potential effects in cancer therapy [85]. Very encouraging results were obtained from a prospective cohort study of 269 hepatocellular carcinoma patients. Of these, 113 received oral AHCC after curative surgery, showing a significantly prolonged recurrence-free period (HR = 0.639; 95% CI [0.429–0.952]; P = 0.0277) and improved overall survival (HR = 0.421; 95% CI [0.253–0.701]; P = 0.0009) compared to the control group [86].
4.2. Turkey Tail (Coriolus/Trametes versicolor)
Trametes versicolor is a medicinal fungus with a long history in traditional Chinese medicine, referred to as "Yun Zhi" in China. It is recognized for its immune-modulating properties, primarily through PSK and PSP, which are polysaccharopeptides extracted from its mycelia. These extracts have been extensively researched for their potential as adjunctive cancer therapies, enhancing the efficacy of conventional treatments like chemotherapy and radiotherapy while reducing adverse effects. In Asia, particularly Japan and China, these extracts have been integrated into clinical practice, with PSK approved for use in Japan since 1977 and PSP approved in China since 1987, when PSK’s annual sales in Japan reached $357 million [87,88]. The PSP utilized in China is primarily derived from the COV-1 strain, while the PSP Krestin (PSK) used in Japan comes from the CM-101 strain of Coriolus versicolor. This review notes that PSK and PSP are used as adjuvant therapies, with significant research from Asia focusing on colorectal, gastric, esophageal, lung, liver and various advanced cancers. A review of preclinical and clinical studies conducted in China, extracted from the Chinese VIP, CNKI, and Wanfang databases, concludes that PSP is an effective antitumor agent with minimal side effects, regardless of its administration method. It helps alleviate adverse reactions from chemotherapy, such as bone marrow suppression, and significantly enhances patients’ quality of life. A total of 7 independent clinical studies were analyzed in this review, with one study from Japan, indicating that PSP has curative effects on various advanced cancers, including gastric, non-small cell lung, primary liver, and colorectal cancers. It is commonly used in combination with chemotherapeutic drugs, such as XELOX (Oxaliplatin+Xeloda) for advanced colorectal cancer, to reduce side effects, improve tolerance to treatment, and potentially prolong life [88]. A systematic review and meta-analysis evaluated the efficacy of Yun Zhi (Trametes versicolor) on the survival of cancer patients. Analyzing data from 13 randomized, placebo-controlled trials, the study found that Yun Zhi significantly improved survival rates compared to standard anti-cancer treatments alone, with a 9% absolute reduction in 5-year mortality. The effects on the overall 5-year survival rate were particularly notable in patients with breast, gastric, and colorectal cancers undergoing chemotherapy, while not so evident in esophageal and nasopharyngeal cancers. The analysis suggests that Yun Zhi may enhance survival in certain cancer types, but further prospective studies are needed to optimize treatment protocols [89].
The 2015 systematic review by Heidi Fritz et al. [90] highlights the promising potential of Polysaccharide K (PSK), derived from the Trametes versicolor mushroom, as an adjuvant immunotherapy for lung cancer. Despite its established use in Japan, this review fills a significant gap by synthesizing English-language evidence on PSK’s effects. The analysis included 31 reports from 28 studies, comprising 6 randomized controlled trials (RCTs), 5 nonrandomized controlled trials, and 17 preclinical studies. The majority of preclinical studies (15 out of 17) demonstrated PSK’s anticancer effects through immunomodulation and direct tumor inhibition, while nonrandomized controlled trials showed improvements in various survival metrics. Most RCTs reported beneficial impacts on immune parameters, tumor-related symptoms, and overall survival. Overall, the findings suggest that PSK may enhance immune function, reduce symptoms associated with tumors, and extend survival in lung cancer patients, underscoring the need for larger, more rigorous trials to further validate these encouraging results. This need for further assessment and evaluation of relevant clinical data has also been highlighted in a 2022 systematic review published in the Cochrane Library regarding the use of PSK in colorectal cancer patients [91]. Although the report indicates that there is evidence suggesting a small effect on overall survival at five years, with an absolute risk reduction of 6% (95% CI [1%–11%]), the impact of reduced adverse effects on this outcome could not be determined. Imprecision due to small sample sizes and indirectness related to the unknown relevance to current therapy standards downgraded the quality of evidence to ’low-certainty’, following the guidelines from the GRADE system (Grading of Recommendations Assessment, Development and Evaluation) [92]. Previous attempts to address the uncertainty in the field include a 2006 meta-analysis comprising 8,009 gastric cancer patients, from 8 randomized controlled trials, performed by the Department of Epidemiological and Clinical Research Information Management, at Kyoto University Graduate School of Medicine in order to assess survival benefits [93]. The overall hazard ratio for eligible patients was 0.88 (95% CI [0.79–0.98]; P = 0.018), with no significant heterogeneity observed [(8) for heterogeneity = 11.7; P = 0.16]. These findings from the meta-analysis indicate that adjuvant immunochemotherapy using polysaccharide Krestin enhances the survival of patients following curative resection for gastric cancer. Another meta-analysis from 2006, with a focus on curatively resected colorectal cancer, reassessed the benefits of immunochemotherapy using the biological response modifier PSK. This analysis included data from 1,094 patients enrolled in three clinical trials, all of whom were followed for at least 5 years post-surgery. The study compared outcomes of standard chemotherapy with chemotherapy plus PSK, evaluating overall survival and disease-free survival through intent-to-treat analysis. The results indicated an overall survival risk ratio of 0.71 (95% CI: 0.55–0.90; P=0.006) and a disease-free survival risk ratio of 0.72 (95% CI: 0.58–0.90; P=0.003). These findings suggest that adjuvant immunochemotherapy with PSK can significantly improve both overall and disease-free survival in patients with curatively resected colorectal cancer [94].
In relation to colorectal cancer patients specifically, two observational studies have reported significant results. In a retrospective analysis of 63 patients, where 39 received postoperative UFT alone (control group), and 24 were treated with UFT plus PSK (PSK group), the results showed a significant improvement in the 3-year relapse-free survival rate, with 76.2% in the PSK group compared to 47.8% in the control group (P = 0.041). Additionally, the overall survival rate was notably higher in the PSK group at 80.8%, versus 52.8% in the control group (P = 0.0498). Subset analyses indicated particularly favorable outcomes for patients with colon tumors and those with lower preoperative lymphocyte percentages. Adverse drug reactions were minimal, with all reported reactions being grade 2 or lower [95]. The study by Toshimi Sakai et al. [96] evaluates the long-term survival benefits of combining polysaccharide Kureha (PSK) with oral fluoropyrimidines in patients with curatively resected colorectal cancer. In this retrospective analysis, the 10-year overall survival rate for the PSK group was significantly higher at 81.9%, compared to 50.6% in the control group receiving only fluoropyrimidines. Notably, in Dukes’ C cases, the PSK group also demonstrated superior survival rates. For patients with lymphatic invasion graded ly2-ly3 or venous invasion graded v2-v3, the PSK group achieved a 10-year survival rate of 80.6%, markedly better than the 25.9% in the control group. Cox’s proportional hazard model analysis confirmed a significant difference in prognosis between the two groups. The findings suggest that postoperative adjuvant immunochemotherapy with PSK significantly enhances long-term survival, particularly for patients with advanced disease features, and the authors recommend its use in these cases.
4.3. Exploring the Efficacy of Adjuvant Immunochemotherapy with PSP/PSK: A Meta-Analysis of Selected Randomized Controlled Trials
Several RCTs have reported promising results for the use of polysaccharopeptides derived from Trametes versicolor. In this section, we will review these studies and perform a meta-analysis of selected clinical trials that meet specific criteria: RCTs evaluating PSP/PSK as adjuvant treatment, with overall survival as an endpoint, and a focus on its role as a complementary therapy to the standard of care.
Among the studies excluded from the meta-analyses, K. W. Tsang et al. [97] investigated the effects of PSP on patients with advanced non-small cell lung cancer (NSCLC). Conducted as a double-blind, placebo-controlled trial, it involved 34 patients who had completed conventional treatment. After 28 days of PSP administration, results showed significant improvements in blood leukocyte and neutrophil counts, serum IgG and IgM levels, and body fat percentage in the PSP group compared to the control group. Notably, fewer PSP patients withdrew from the study due to disease progression (5.9% vs. 23.5% in controls). No adverse reactions were reported. The findings suggest that PSP may slow the progression of advanced NSCLC, although it did not improve NSCLC-related symptoms. Miyake et al. [98] in a phase III trial compared oral adjuvant uracil and tegafur plus protein-bound polysaccharide K (UFT/PSK) to uracil and tegafur plus leucovorin (UFT/LV) in patients with stage IIB and III colorectal cancer. The study aimed to demonstrate the non-inferiority of UFT/PSK in terms of 3-year disease-free survival (DFS). A total of 357 patients were randomized, revealing a 3-year DFS of 82.3% for UFT/LV and 72.1% for UFT/PSK, with a difference of -9.06% (90% CI: -17.06% to -1.06%), failing to meet the non-inferiority margin. Overall survival rates were 95.4% for UFT/LV and 90.7% for UFT/PSK. While UFT/PSK was not non-inferior to UFT/LV, the study was not designed to definitively establish superiority of UFT/LV, leaving its statistical superiority unconfirmed in this context.
Among the clinical trials that were selected, Niimoto et al. 1988 [99], Torisu et al. 1990 [100], Mitomi et al. 1992 [101], Nakazato et al. 1994 [102], Ogoshi et al. 1995 [103], Toge et al. 2000 [104], Ito et al. 2004 [105], Ohwada et al. 2004 [106], Akagi et al. 2010 [58], Shichinohe et al. 2013 [107], and Ogawa et al. 2024 [108], only those with a 5-year OS as an endpoint were included in the meta-analysis, for consistency. A summary of all the studies is presented in Table 3. If the specific number of patients in each group could not be obtained (given the limited access to some of the studies’ data) a half and half partition was considered in order to obtain the survival risk ratio and the 95% confidence interval (CI). The assumption of equal groups is reasonable without further data, and the CI’s width reflects the sample size and event rates adequately. In all cases the survival risk ratio is obtained as RR = (Risk in treatment group) / (Risk in control group), considering survival as the event of interest. Equations were derived via the log-transformation method as follows:
Chemotherapy + PSP/PSK () vs. Chemotherapy alone (),
- 95% Confidence Interaval:
(delta method approximation):
Taking the exponential:
In order to perform the meta-analysis to estimate the pooled relative risk (RR) of survival, the following steps were followed [109]:
- Log Relative Risk: The RR for each study, defined as the ratio of event probabilities (), was log-transformed:
- Standard Error (SE) from Confidence Interval: The standard error of was derived from the 95% confidence interval (CI) bounds:
- Variance of Log Relative Risk: The variance was calculated as the square of the SE:
- Fixed-Effect Weight: Each study’s weight () was computed as the inverse of the variance:
- Pooled Log Relative Risk (Fixed-Effect): The pooled estimate was obtained by a weighted average of across studies:
- Heterogeneity Statistic (Cochran’s Q): Heterogeneity was assessed using:
-Between-Study Variance (): The between-study variance was estimated, where k is the number of studies:
(set to 0 if , indicating no additional variance beyond sampling error; with Statistic as ).
- Standard Error of Pooled Estimate: The SE of the pooled estimate was calculated as:
- Pooled Confidence Interval: The 95% CI for was computed as:
These bounds were then exponentiated to yield the pooled RR and its 95% CI on the original scale.
Figure 1.
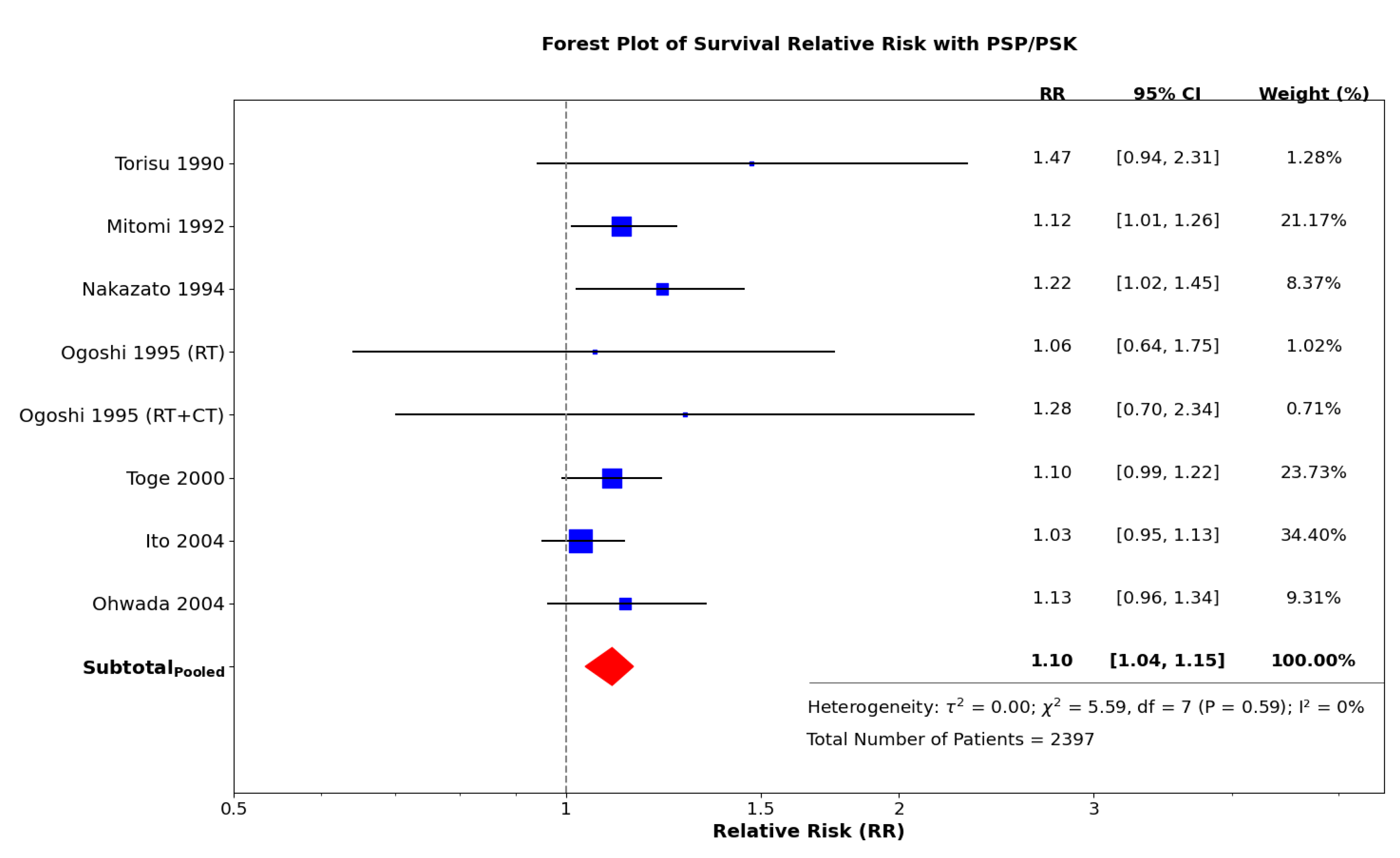
This forest plot illustrates the survival relative risk associated with PSP/PSK across eight studies, encompassing a total of 2,397 patients. Each blue square represents the relative risk (RR) for an individual study, with the size of the square reflecting the study’s weight. The horizontal lines indicate the 95% confidence intervals (CIs). The red diamond represents the pooled RR, which is 1.10 (95% CI: 1.04–1.15). The vertical dashed line at RR = 1 signifies no effect while RR > 1 favors the treatment group (Standard of care + PSP/PSK). Heterogeneity statistics displayed in the plot reveal no significant variability among the studies (P = 0.59, I2 = 0%), indicating a consistent effect of PSP/PSK on survival. Therefore, a random-effects model is unnecessary, as a fixed-effect model adequately represents the data.
Figure 1.
This forest plot illustrates the survival relative risk associated with PSP/PSK across eight studies, encompassing a total of 2,397 patients. Each blue square represents the relative risk (RR) for an individual study, with the size of the square reflecting the study’s weight. The horizontal lines indicate the 95% confidence intervals (CIs). The red diamond represents the pooled RR, which is 1.10 (95% CI: 1.04–1.15). The vertical dashed line at RR = 1 signifies no effect while RR > 1 favors the treatment group (Standard of care + PSP/PSK). Heterogeneity statistics displayed in the plot reveal no significant variability among the studies (P = 0.59, I2 = 0%), indicating a consistent effect of PSP/PSK on survival. Therefore, a random-effects model is unnecessary, as a fixed-effect model adequately represents the data.
5. Extraction Methods and Composition of Polysaccharides and Other Bioactive Compounds Found in Medicinal Mushrooms
Medicinal mushrooms are known to contain a diverse array of bioactive compounds that contribute to their therapeutic potential. Among these, polysaccharides are particularly significant, including -glucans and -glucans, specifically -1,3 and -1,6-D-glucans. Other important polysaccharides found in these fungi include heteroglycans, peptidoglycans (e.g. ganoderan B and C), and polysaccharide peptides (e.g. PSP/PSK). In addition to polysaccharides, terpenes and triterpenoids play a crucial role in the bioactivity of medicinal mushrooms. Notable examples include ganoderic acids, ganodermic acids, ganodermic alcohols, lucidones, and lucinedic acids in the genus Ganoderma.
Proteins and peptides are also essential components, with fungal immunomodulatory proteins (FIPs) recognized for their cytotoxic and immunomodulatory effects, and lectins, which specifically bind to mono- and oligosaccharides, being another important class. Additionally, peptides such as GLP from Ganoderma lucidum, along with glycoproteins like GFG-3a from Grifola frondosa, contribute to the bioactive profile of these mushrooms. Phenolic compounds, known for their antioxidant properties, are present in various species of medicinal mushrooms. Fatty acids, including conjugated linoleic acid (CLA), further enhance the chemical diversity of these fungi. Steroids and their derivatives, including ergosterol and Antcin-A (ATA), are also noteworthy, while ergothioneine, an amino acid derivative, contributes separately to their bioactive spectrum. Diterpenoids, particularly erinacines (A-I), are recognized for their bioactive properties, as are benzyl alcohol derivatives like hericenones (C-H). Finally, other significant compounds include laccases, which are copper-containing oxidases, as well as nucleosides and nucleotides that can influence platelet aggregation. Flavonoids and the -glucosidase inhibitor SKG-3 from Ganoderma lucidum further exemplify the wide range of bioactive compounds found in medicinal mushrooms, highlighting their diverse pharmacological potential [110,111]. In the following we will explore the main bioactive compounds used in clinical research and evaluate their pharmacological equivalence based on extraction methodologies and standardization techniques, with a primary focus on Trametes versicolor.
5.1. Comprehensive Analysis of Medicinal Compounds in Selected Mushrooms
This section, based on the most frequently utilized medicinal mushroom species in human clinical studies, provides a detailed examination of the medicinal compounds found in Reishi (Ganoderma lucidum), Maitake D-fraction (Grifola frondosa D-fraction), Lentinan (Lentinula edodes extract), AHCC (Active Hexose Correlated Compound), and Turkey Tail (Trametes/Coriolus versicolor). The analysis aims to elucidate the chemical nature of these compounds, offering a thorough resource for understanding their pharmacological relevance.
5.1.1. Reishi (Ganoderma lucidum)
Reishi, a widely studied medicinal mushroom, is known for its diverse bioactive compounds, particularly triterpenoids and polysaccharides. Triterpenoids, such as ganoderic acids (including A, C, F, H, T, etc.), lucidenic acids, and ganodermanondiol, are derivatives of lanosterol, a tetracyclic triterpene, and are noted for their antitumor properties. GL-PS polysaccharides, including -glucans (specifically -1,3, and -1,6-D-glucans) and -1,3-D-glucans, as well as peptidoglycans ganoderan B and C, are sugar polymers with glucose as a major component, exhibiting strong immune-strengthening effects. GL-PS can be extracted from Ganoderma lucidum spores, fruiting bodies, mycelium, and fermentation broth using various methods, including hot water extraction, which is commonly empolyed to obtain the soluble polysaccharides. [112,113,114,115].
5.1.2. Maitake D-Fraction (Grifola frondosa D-Fraction)
The protein-bound Maitake D-fraction from Grifola frondosa is characterized as the acid-insoluble, alkali-soluble, and hot water-extractable fraction, identified as containing both a -1,6-D-glucan with -1,3 branches, and a -1,3 main chain having -1,6 branches, forming a heavy proteoglycan with a molecular weight of ∼1000 kDa. This compound is a -glucan conjugated with protein, known for its immune-activating properties, particularly in cancer therapy. It is standardized for oral administration and has been studied for its antitumor effects. This compound’s safety and efficacy are supported by various studies, emphasizing its role as a biological response modifier [79,80,116,117].
5.1.3. Lentinan (Lentinula edodes Extract)
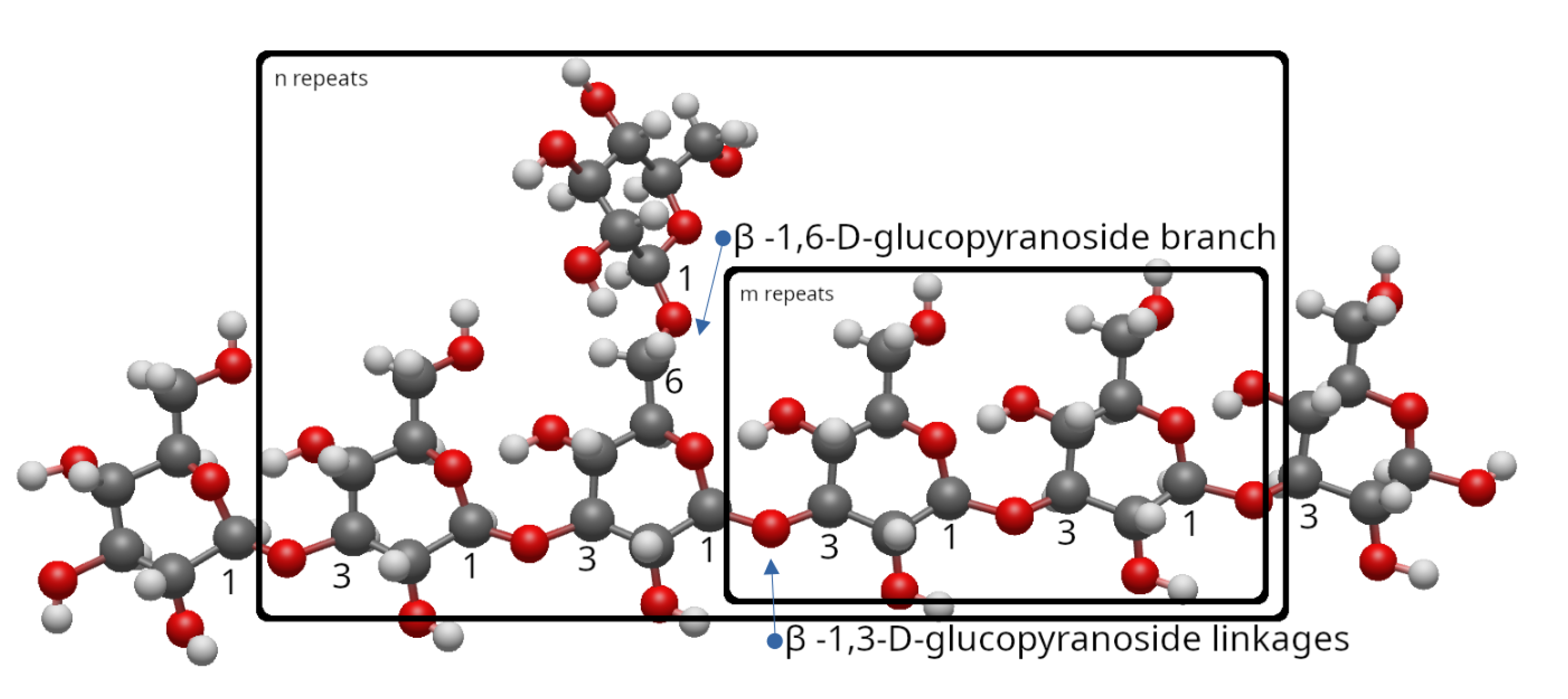
Lentinan, extracted from Lentinula edodes, is a -1,3-D-glucan with two -1,6-glucopyranoside branches for every five -1,3-glucopyranoside linkages, a polysaccharide with a molecular weight of approximately 500 kDa. It is known for its immunomodulatory and antitumor effects, often used as an adjuvant in cancer therapy, particularly in Japan and China. Its chemical structure is detailed in [118,119], which discusses its host-mediated antineoplastic activity via immune stimulation. This compound’s ease of availability and low toxicity make it a significant focus in medicinal mushroom research [82].
5.1.4. AHCC (Active Hexose Correlated Compound)
As we mentioned before, AHCC is a functional food supplement created at the University of Tokyo by Dr. Toshihiko Okamoto and researchers from Amino Up Chemical Co., Ltd. Its main ingredient is Lentinula edodes, recognized for its healing properties, along with various hybrids from the Basidiomycota fungal phylum. AHCC has a composition rich in -1,4-glucans (∼20-30%) with partially acylated sugar moieties. The product also includes various polysaccharides such as -1,3 glucans, along with trace amounts of protein, amino acids, lipids, and minerals, with a mean molecular weight of ∼5 kDa. These components work synergistically to enhance immune responses, particularly natural killer cell and T cell activity. Its production involves a patented culturing process [83,120,121].
5.1.5. Turkey Tail (Trametes/Coriolus versicolor)
Turkey Tail, known scientifically as Trametes versicolor, previously classified as Coriolus versicolor, is rich in polysaccharides, with polysaccharopeptides PSP and PSK being the most commonly known. Both are protein-bound polysaccharides with a molecular weight of ∼100 kDa. Some reports indicate that PSP has a polysaccharide-to-peptide ratio of 90:10, containing mannose, xylose, galactose, fructose, and others, while PSK has a 60:40 ratio, with mannose, xylose, galactose, arabinose, rhamnose, and others. Although these ratios, as well as their monosaccharide compositions, might vary considerably across studies due to differences in extraction methods, fungal strains (e.g., COV-1 for PSP, CM-101 for PSK), and analytical techniques. Structurally diverse, these -glucan-based compounds are recognized for their immunomodulatory and anticancer properties [54,63,87,110,122,123]. Generally, in a broader polysaccharide fraction beyond PSP/PSK, Coriolus versicolor polysaccharides (CVP) have a high molecular weight of ∼500-1000 kDa, with a -1,4/1,3-D-glucan main chain and -1,6 branches. The monosaccharide composition of CVP predominantly contains glucose in the form of beta-D-glucopyranose, along with small amounts of mannose, fructose, rhamnose, fucose, and others. Additionally, as we stated earlier, the variety, processing technology, and extraction method of CVP indeed influence its monosaccharide types, molecular weight, and chemical composition [124]. Further research is needed regarding the pharmacological activities of small molecular weight compounds [45,63].
Polysaccharopeptides from C. versicolor are commercially extracted from mushrooms or mycelia grown on solid substrates, as well as from mycelial biomass produced through submerged fermentation. The primary clinically approved polysaccharopeptide preparations, PSK and PSP, are derived from mycelial biomass cultivated in submerged conditions, processed into dried powder after hot water extraction [124,125]. The extraction and purification of polysaccharides from Coriolus versicolor (CVP) involve several techniques, each employing distinct chemical and physical principles to isolate these bioactive compounds from raw materials like fruiting bodies and mycelium. Following Jing et al. 2022 [124], the most commonly used extraction method for CVP is hot water extraction, with best extraction conditions being a solid-to-liquid ratio of 1:30, and a extraction temperature of 90°C for 120 minutes (twice), followed by ethanol precipitation, resulting in a yield of 5.38%. This yield can be increased to up to 16.7% with mechanical crushing and liquid nitrogen for particles under 200 meshes in size. Other methods include enzyme extraction, operationally more complex, which can achieve yiels of 9.58% at 52°C, enzyme concentration of 2.50%, pH 5.5, and enzymolysis time of 37 minutes, generally using cellulase, proteases and pectinase. Additionally, ultrasonic extraction can be optimized to achieve extraction rates up to 13.6% at 1:45 solid-to-liquid ratio, 30 minutes extraction time, and ultrasonic power of 450 W via the response surface method, although high-intensity shock waves may have some structural impact. The purification process for crude CVP includes the removal of proteins and pigments through methods such as ethanol fractionation, column chromatography, and ion exchange chromatography, resulting in a refined product that is suitable for further pharmacological use. These processes are mirrored in high-quality commercial standardized extracts. It is important to note that although some of these polymers have distinct structures, they cannot be differentiated based on their physiological activity [125].
Figure 2.
Repeat unit of the partial structure of PSP/PSK with m and n repeats, respectively [54]. The -D-glucan molecular structure was generated using Avogadro software. Carbon atoms in black, oxygen in red, and hydrogen in white.
Figure 2.
Repeat unit of the partial structure of PSP/PSK with m and n repeats, respectively [54]. The -D-glucan molecular structure was generated using Avogadro software. Carbon atoms in black, oxygen in red, and hydrogen in white.
6. Enhancing Surgical Eligibility: A Proposal for the Use of Medicinal Mushroom Extracts as an Adjunctive Therapy to Optimize Preoperative Systemic Chemotherapy Outcomes
6.1. Clinical Context, Rationale, and Limitations of Current Therapies
CRC with LM (15–25% at diagnosis) and PM (8–15% during initial treatment) is associated with poor prognosis, with median OS of 6–9 months untreated and 12–24 months with modern systemic chemotherapy alone (e.g., FOLFOX, FOLFIRI), in addition to targeted therapies. Although aggressive regimens such as FOLFOXIRI combined with bevacizumab improve outcomes, with an OS of 31.0 months and a PFS of 12.1 months, as demonstrated in the TRIBE trial involving 508 patients, it is important to note that these results are not limited to patients with LM plus PM, and these statistics only apply to patients who are fit enough to receive this treatment. Nevertheless, conversion to resectable disease within this cohort occurs in only 39.1% of cases, with an R0 resection rate of 28.1%, underscoring the importance of patient selection in optimizing therapeutic strategies. Combined approaches like CRS + HIPEC with liver resection extend OS to 26–48 months in selected patients, but eligibility is restricted by high peritoneal cancer index (PCI >20), multiple liver lesions (>2–3), and incomplete cytoreduction (CC >1). Enhancing preoperative tumor shrinkage is critical to broaden surgical candidacy (Refer to [mysection]Section 1 for citations).
6.2. Medicinal Mushroom Extracts: Mechanisms and Evidence
Medicinal mushroom compounds such as Trametes versicolor PSP/PSK and small molecules, Ganoderma lucidum polysaccharides (GL-PS) and triterpenoids, Grifola frondosa -glucans, Lentinula edodes lentinan, Agaricus blazei polysaccharides, and Inonotus obliquus ergosterol peroxide collectively exhibit potent anticancer effects, as detailed in preclinical and clinical studies. Their activity as biological response modifiers can suppress multidrug resistance (e.g., P-gp inhibition), block immune checkpoints (e.g., PD-L1, CTLA-4), regulate oncogenic pathways (e.g., PI3K/AKT, Wnt/-catenin, MAPK, NF-B), and enhance immunomodulation (e.g., NK cell activation, Th1 cytokine production). Similarly, they can induce apoptosis, inhibit angiogenesis, and reduce metastasis. Clinical trials, including meta-analyses of over 8,000 patients (e.g., Oba 2007 [93], 8,009 gastric cancer patients; Zhong 2019 [70], 4,246 patients across cancers; Sakamoto 2006 [94], 1094 colorectal cancer patients), report improved OS (e.g., our meta-analysis indicates a 5–15% increase in the probability of survival at five years) and tolerability when combined with chemotherapy, primarily in postoperative CRC and other cancers.
6.3. Potential in Conversion Therapy
While most clinical data on mushroom extracts pertain to postoperative settings, their ability to enhance chemotherapy efficacy suggests a preoperative role. For instance, the immune-enhancing effects and chemosensitizing properties of PSP/PSK could amplify tumor responses to FOLFOXIRI + bevacizumab, potentially increasing the 39.1% surgical eligibility rate observed in systematic reviews. In patients with LM and PM, these extracts might counteract liver immunosuppression (e.g., regulatory T-cells) and peritoneal tumor burden, reducing PCI and lesion counts to surgically manageable levels. Synergy with PD-1 inhibitors further suggests compatibility with modern therapies like pembrolizumab in MSI-H mCRC, though this requires separate validation.
6.3.1. Safety and Practical Integration
PSP/PSK (1–3 g/day) and other mushroom extracts (e.g., lentinan, AHCC) are well-tolerated, with mild side effects (e.g., nausea) and extremely rare severe events, as evidenced by extensive use in Japan and China. Their compatibility with chemotherapy supports preoperative integration, though standardization (e.g., hot water extraction, use of fruiting bodies, mycelium or submerged fermentation —where the later is usually preferred in industry in order to increase yield and production—) is essential for consistency. Combining extracts with current regimens could mitigate toxicities (e.g., grade 3–4 events doubled with FOLFOXIRI), improving patient tolerance, and treatment response and duration.
6.3.2. Implementation and Testing
The author agues that a phase II trial in patients with unresectable mCRC with LM and PM would be highly valuable, randomizing participants to receive standard chemotherapy (e.g., FOLFOXIRI + bevacizumab) with or without a mushroom extract cocktail (e.g., PSP/PSK 2-3 g/day, GL-PS 1–2 g/day) for a duration that allows for adequate assessment of treatment response, potentially ranging from 24 to 48 weeks. Primary endpoints would include conversion rate to resectable disease (PCI , ≤ 2–3 liver lesions, CC–0/1), overall response rate (ORR), and PFS. Secondary endpoints would assess OS, toxicity, and quality of life. A cohort of 50–100 patients could detect a 5–10% increase in surgical eligibility (e.g., 39% to 44–49%) and a 2–3 month PFS extension, building on TRIBE trial benchmarks.
6.3.3. Expected Outcomes and Implications
If effective, this adjunctive therapy could elevate R0 resection rates beyond the 28.1% observed with FOLFOXIRI + bevacizumab, potentially aligning OS with CRS-HIPEC outcomes (26–48 months) or surpassing them in a broader population. By enhancing tumor shrinkage and reducing immunosuppression, mushroom extracts could redefine conversion therapy, offering a low-toxicity, biologically plausible adjunct to multidisciplinary care.
6.3.4. Limitations and Future Directions
The absence of direct preoperative trials for mCRC limits current evidence, requiring extrapolation from postoperative data. Variability in extract composition and the unique challenges of dual metastases (e.g., liver vascularity, peritoneal spread) necessitate tailored studies. Future research should explore combinations with targeted therapies (e.g., anti-VEGF, anti-EGFR) and immunotherapies (e.g., pembrolizumab in MSI-H cases), as well as other bioactive compounds (see [myappendix]Appendix A) to maximize efficacy across mCRC subtypes.
Conclusion
This Medical Investigation examines the challenges of managing mCRC with LM and PM, where systemic chemotherapy alone yields median OS of 12–24 months, and conversion to resectable disease remains limited (e.g., 39.1% in patients who are fit enough to undergo FOLFOXIRI + bevacizumab; not limited to LM + PM). Combined approaches like CRS + HIPEC extend OS to 26–48 months in select cases, but eligibility is constrained by disease extent. The author proposes that medicinal mushroom extracts (e.g., PSP/PSK from Trametes versicolor, polysaccharides from Ganoderma lucidum, and others) could enhance preoperative chemotherapy outcomes by increasing tumor response, surgical eligibility, and patient tolerability. This approach is supported by preclinical data on multidrug resistance suppression, immune modulation, and pathway regulation, among others, as well as clinical evidence from meta-analyses (>8,000 patients) showing survival benefits. Our own meta-analysis, involving a total of 2397 patients, indicates a 10% increase risk of survival at 5 years with the inclusion of PSP/PSK compared to the standard of care; RR = 1.10 (95% CI: 1.04–1.15). The investigation suggests a phase II trial to test this approach. While promising, the lack of direct preoperative data and variability in metastatic site responses highlight the need for further research to validate and optimize this strategy in mCRC management.
Figure 3.
Figure 3:Trametes versicolor and Ganoderma lucidum medicinal mushrooms, from left to right. Photographs by @charliewarl and @champsara, respectively, sourced from Unsplash library.
Figure 3.
Figure 3:Trametes versicolor and Ganoderma lucidum medicinal mushrooms, from left to right. Photographs by @charliewarl and @champsara, respectively, sourced from Unsplash library.

Conflicts of Interest
The author declares that there are no conflicts of interest regarding the publication of this paper.
Acronyms
- 5-FU: 5-Fluorouracil
- 5-HTP: 5-Hydroxy-L-Tryptophan
- AHCC: Active Hexose Correlated Compound
- ATA: Anctin-A
- CA125: Cancer Antigen 125
- CC: Completeness of Cytoreduction (e.g., CC-0, CC-1)
- CI: Confidence Interval
- CLA: Conjugated Linoleic Acid
- CNKI: China National Knowledge Infrastructure
- CRC: Colorectal Cancer
- CRS: Cytoreductive Surgery
- CRT: Chemoradiotherapy
- CT: Chemotherapy
- CTLA-4: Cytotoxic T-Lymphocyte-Associated Protein 4
- CVP: Coriolus Versicolor Polysaccharides
- Da: Dalton
- DFS: Disease-Free Survival
- dMMR: Deficient Mismatch Repair
- ECOG: Eastern Cooperative Oncology Group
- EGFR: Epidermal Growth Factor Receptor
- FIP: Fungal Immunomodulatory Protein
- FOLFIRI: 5-Fluorouracil + Leucovorin + Irinotecan
- FOLFOX: 5-Fluorouracil + Leucovorin + Oxaliplatin
- FOLFOXIRI: 5-Fluorouracil + Leucovorin + Oxaliplatin + Irinotecan
- GFG: Grifola Frondosa Glycoprotein
- GLP: Ganoderma Lucidum Peptides
- GL-PS: Ganoderma Lucidum Polysaccharides
- GRADE: Grading of Recommendations Assessment, Development and Evaluation
- GSP: Ganoderma Sinense Polysaccharide
- HIPEC: Hyperthermic Intraperitoneal Chemotherapy
- IgG / IgM: Immunoglobulin G / M
- IL-: Interleukin- (e.g., IL-6, IL-2)
- IFN-: Interferon-gamma
- LM: Liver Metastases
- LPS: Lipopolysaccharide
- LR: Liver Resection
- LV: Leucovorin
- MAPK: Mitogen-Activated Protein Kinase
- mCRC: Metastatic Colorectal Cancer
- MDR: Multidrug Resistance
- MMP-3: Matrix Metalloproteinase-3
- MSI-H: Microsatellite Instability-High
- MSS: Microsatellite Stable
- NCI: National Cancer Institute
- NF-B: Nuclear Factor Kappa-light-chain-enhancer of Activated B Cells
- NK: Natural Killer Cells
- NLM: Non-Liver Metastases
- NSCLC: Non-Small Cell Lung Cancer
- OS: Overall Survival
- PAMP: Pathogen-Associated Molecular Pattern
- PB-Mac: Peripheral Blood Mononuclear Adherent Cells
- PBP: Protein-Bound Polysaccharide
- PCI: Peritoneal Cancer Index
- PD-1: Programmed Cell Death Protein 1
- PD-L1: Programmed Death-Ligand 1
- PDQ: Physician Data Query
- PFS: Progression-Free Survival
- P-gp: P-glycoprotein
- PI3K/AKT: Phospho-Inositide 3-Kinase / Protein Kinase B
- PM: Peritoneal Metastases
- pMMR: Proficient Mismatch Repair
- PSA: Prostate-Specific Antigen
- PSK: Polysaccharide-K (Krestin)
- PSP: Polysaccharide Peptide
- R0: Complete Resection
- RCT: Randomized Controlled Trial
- RR: Risk Ratio
- TNF-: Tumor Necrosis Factor-alpha
- UFT: Tegafur/Uracil
- VEGF: Vascular Endothelial Growth Factor
- VIP: Chongqing VIP Chinese Scientific Journals Database
- WGP: Whole Glucan Particle
- XELOX: Xeloda (Capecitabine) + Oxaliplatin
Appendix A. Analysis of Silymarin’s Potential as a Hepatoprotector and Antimetastatic Agent
Silymarin, a flavonoid derived from milk thistle (Silybum marianum), has been extensively investigated for its therapeutic potential in supporting liver health. This note provides a comprehensive examination of whether silymarin can prevent hepatic metastasis while simultaneously protecting the liver from chemotherapy-induced toxicity in healthy cells, without compromising the chemotherapeutic efficacy against malignant cells. The analysis is grounded in a review of recent literature, encompassing in vitro, in vivo, and clinical studies.
Appendix A.1. Background on Silymarin
Silymarin is a complex of flavonolignans, including silybin, aslo known as silibinin, silidianin, isosilybin, and silychristin, with silybin identified as the most bioactive constituent. Historically, it has been employed to safeguard the liver against conditions such as alcoholic cirrhosis and toxin-induced hepatic damage. Recent research has expanded its scope to include applications in malignant diseases, particularly those affecting the gastrointestinal system, owing to its antiproliferative, anti-inflammatory, and antimetastatic properties [126].
Appendix A.2. Potential to Prevent Hepatic Metastasis
Studies suggest that silymarin exhibits antimetastatic activity by modulating tumor characteristics, including cell cycle arrest, apoptosis, and angiogenesis. For instance, research on malignant colon cell lines (e.g., LoVo and DLD-1) demonstrates that silymarin inhibits cellular proliferation and induces apoptosis, potentially reducing metastatic burden [127]. Furthermore, its antiangiogenic effects —evidenced by the suppression of endothelial cell migration and capillary tube formation— may restrict the vascular support required for metastasis [128]. Although specific studies on the prevention of colorectal-derived hepatic metastasis in animal models remain limited, several investigations highlight silymarin’s broader antimetastatic effects [129].
Appendix A.3. Protection of the Liver Against Chemotherapy-Induced Toxicity in Healthy Cells
Chemotherapy frequently induces hepatotoxicity, impairing liver function. Silymarin’s hepatoprotective properties are well-documented, with preclinical and clinical data indicating its capacity to mitigate oxidative stress and shield hepatocytes from cytotoxic damage. It has been shown to modulate Phase I and Phase II xenobiotic-metabolizing enzymes in a manner that both protects healthy cells from chemotherapy-induced toxicity and fosters chemosensitivity. At the same time the concentrations of silybin following the consumption of milk thistle extract are insufficient to have a significant impact on P450 function [130]. A randomized controlled trial in breast cancer patients demonstrated silymarin’s ability to lower hepatic enzyme levels (e.g., bilirrubin and ALP) during treatment, suggesting potential benefits for individuals with colon cancer [131]. This protective effect is attributed to its antioxidant and anti-inflammatory actions, which may preserve healthy hepatocytes during therapy. In leukemia patients undergoing chemotherapy, silymarin (420 mg/day) combined with diammonium glycyrrhizinate reduced hepatic enzyme levels and exhibited less drug-induced liver injury (DILI) compared to a control group receiving only glycyrrhizinate, indicating its safety and utility in this context [132,133]. Similar findings were observed in breast cancer patients in a randomized, triple blind, placebo-controlled clinical trial of 30 patients who received doxorubicin/cyclophosphamide-paclitaxel chemotherapy. In the silymarin group, the grade of hepatic involvement assessed through ultrasonography significantly decreased following the intervention (P = 0.012) [134,135].
Appendix A.4. Non-Inhibition of Chemotherapy Effects on Metastatic Cells
A critical consideration is ensuring that silymarin does not shield metastatic tumor cells from chemotherapy, which could diminish treatment efficacy. Research suggests that silymarin may enhance, rather than inhibit, chemotherapeutic effects. Studies combining silymarin with doxorubicin or paclitaxel in colon tumor cell lines (e.g., LoVo, LoVo/DX) revealed synergistic antiproliferative activity, particularly in non-multidrug-resistant cells, indicating that it does not confer protection to tumor cells and may, in fact, enhance their sensitivity to chemotherapy [136]. This is supported by evidence that silymarin inhibits ATP-binding cassette transporters, counteracting chemoresistance, and enhances apoptosis in tumor cells [130]. Consequently, silymarin appears likely to protect healthy hepatocytes while maintaining or improving chemotherapy’s effectiveness against metastatic cells. Additionally, at therapeutic doses, it exhibits no significant interactions with CYP450 enzymes, minimizing the risk of drug-herb interference and ensuring compatibility with treatment [133]. It may also enhance chemosensitivity by modulating antiapoptotic pathways [130,134].
Appendix A.5. Conclusion
Based on current research, silymarin demonstrates potential in preventing hepatic metastasis in colon cancer through its antiproliferative, apoptotic, and antiangiogenic effects. It also effectively protects the liver from chemotherapy-induced toxicity in healthy cells, as evidenced by its hepatoprotective properties in clinical trials. Moreover, rather than inhibiting chemotherapy, silymarin may potentiate its effects on metastatic cells, offering a dual strategy in cancer management.
References
- Kim, Y.; Kim, C. Treatment for Peritoneal Metastasis of Patients With Colorectal Cancer. Annals of Coloproctology 2021, 37, 425–433. [Google Scholar] [CrossRef]
- Kow, A. Hepatic metastasis from colorectal cancer. Journal of gastrointestinal oncology 2019, 10, 1274–1298. [Google Scholar] [CrossRef] [PubMed]
- März, L.; Piso, P. Treatment of peritoneal metastases from colorectal cancer. Gastroenterology Report 2015, 3, 298–302. [Google Scholar] [CrossRef]
- Klaver, Y.L.B.; Simkens, L.H.J.; Lemmens, V.E.P.P.; Koopman, M.; Teerenstra, S.; Bleichrodt, R.P.; de Hingh, I.H.J.T.; Punt, C.J.A. Outcomes of colorectal cancer patients with peritoneal carcinomatosis treated with chemotherapy with and without targeted therapy. European Journal of Surgical Oncology (EJSO) 2012, 38, 617–623. [Google Scholar] [CrossRef]
- Nadler, A.; McCart, J.A.; Govindarajan, A. Peritoneal Carcinomatosis from Colon Cancer: A Systematic Review of the Data for Cytoreduction and Intraperitoneal Chemotherapy. Clinics in Colon and Rectal Surgery 2015, 28, 234–246. [Google Scholar] [CrossRef]
- Franko, J.; Shi, Q.; Meyers, J.P.; Maughan, T.S.; Adams, R.A.; Seymour, M.T.; Saltz, L.; Punt, C.J.A.; Koopman, M.; Tournigand, C.; et al. Prognosis of patients with peritoneal metastatic colorectal cancer given systemic therapy: an analysis of individual patient data from prospective randomised trials from the Analysis and Research in Cancers of the Digestive System (ARCAD) database. The Lancet Oncology 2016, 17, 1709–1719. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Moreno, F.; Diez-Alonso, M.; Matías-García, B.; Ovejero-Merino, E.; Gómez-Sanz, R.; Blázquez-Martín, A.; Quiroga-Valcárcel, A.; Vera-Mansilla, C.; Molina, R.; San-Juan, A.; et al. Prognostic Factors of Survival in Patients with Peritoneal Metastasis from Colorectal Cancer. Journal of Clinical Medicine 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Franko, J. Therapeutic efficacy of systemic therapy for colorectal peritoneal carcinomatosis: Surgeon’s perspective. Pleura and peritoneum 2018, 3. [Google Scholar] [CrossRef]
- Cohen, R.; Raeisi, M.; Chibaudel, B.; Shi, Q.; Yoshino, T.; Zalcberg, J.R.; Adams, R.; Cremolini, C.; Cutsem, E.V.; Heinemann, V.; et al. Prognostic value of liver metastases in colorectal cancer treated by systemic therapy: An ARCAD pooled analysis. European Journal of Cancer 2024, 207. [Google Scholar] [CrossRef]
- Loupakis, F.; Cremolini, C.; Masi, G.; Lonardi, S.; Zagonel, V.; Salvatore, L.; Cortesi, E.; Tomasello, G.; Ronzoni, M.; Spadi, R.; et al. Initial Therapy with FOLFOXIRI and Bevacizumab for Metastatic Colorectal Cancer. New England Journal of Medicine 2014, 371, 1609–1618. [Google Scholar] [CrossRef]
- Cremolini, C.; Antoniotti, C.; Stein, A.; Bendell, J.; Gruenberger, T.; Rossini, D.; Masi, G.; Ongaro, E.; Hurwitz, H.; Falcone, A.; et al. Individual Patient Data Meta-Analysis of FOLFOXIRI Plus Bevacizumab Versus Doublets Plus Bevacizumab as Initial Therapy of Unresectable Metastatic Colorectal Cancer. Journal of Clinical Oncology 2020, 38, 3314–3324. [Google Scholar] [CrossRef] [PubMed]
- Morris, V.K.; Kennedy, E.B.; Baxter, N.N.; 3rd, A.B.B.; Cercek, A.; Cho, M.; Ciombor, K.K.; Cremolini, C.; Davis, A.; Deming, D.A.; et al. Treatment of Metastatic Colorectal Cancer: ASCO Guideline. Journal of Clinical Oncology 2022, 41, 678–700. [Google Scholar] [CrossRef] [PubMed]
- Polderdijk, M.C.E.; Brouwer, M.; Haverkamp, L.; Ziesemer, K.A.; Tenhagen, M.; Boerma, D.; Kok, N.F.M.; Versteeg, K.S.; Sommeijer, D.W.; Tanis, P.J.; et al. Outcomes of Combined Peritoneal and Local Treatment for Patients with Peritoneal and Limited Liver Metastases of Colorectal Origin: A Systematic Review and Meta-Analysis. Annals of Surgical Oncology 2022, 29, 1952–1962. [Google Scholar] [CrossRef]
- Dico, R.L.; Faron, M.; Yonemura, Y.; Glehen, O.; Pocard, M.; Sardi, A.; Hübner, M.; Baratti, D.; Liberale, G.; Kartheuser, A.; et al. Combined liver resection and cytoreductive surgery with HIPEC for metastatic colorectal cancer: Results of a worldwide analysis of 565 patients from the Peritoneal Surface Oncology Group International (PSOGI). European Journal of Surgical Oncology 2021, 47, 89–100. [Google Scholar] [CrossRef] [PubMed]
- Tomasello, G.; Petrelli, F.; Ghidini, M.; Russo, A.; Passalacqua, R.; Barni, S. FOLFOXIRI Plus Bevacizumab as Conversion Therapy for Patients With Initially Unresectable Metastatic Colorectal Cancer. A Systematic Review and Pooled Analysis. JAMA Oncology 2017, 3, e170278–e170278. [Google Scholar] [CrossRef]
- Verwaal, V.J.; van Ruth, S.; de Bree, E.; van Slooten, G.W.; van Tinteren, H.; Boot, H.; Zoetmulder, F.A. Randomized trial of cytoreduction and hyperthermic intraperitoneal chemotherapy versus systemic chemotherapy and palliative surgery in patients with peritoneal carcinomatosis of colorectal cancer. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2003, 21, 3737–3743. [Google Scholar] [CrossRef]
- Elias, D.; Lefevre, J.H.; Chevalier, J.; Brouquet, A.; Marchal, F.; Classe, J.M.; Ferron, G.; Guilloit, J.M.; Meeus, P.; Goéré, D.; et al. Complete cytoreductive surgery plus intraperitoneal chemohyperthermia with oxaliplatin for peritoneal carcinomatosis of colorectal origin. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2009, 27, 681–685. [Google Scholar] [CrossRef]
- Franko, J.; Ibrahim, Z.; Gusani, N.J.; Holtzman, M.P.; Bartlett, D.L.; Zeh, H.J. Cytoreductive surgery and hyperthermic intraperitoneal chemoperfusion versus systemic chemotherapy alone for colorectal peritoneal carcinomatosis. Cancer 2010, 116, 3756–3762. [Google Scholar] [CrossRef]
- Cashin, P.H.; Mahteme, H.; Spång, N.; Syk, I.; Frödin, J.E.; Torkzad, M.; Glimelius, B.; Graf, W. Cytoreductive surgery and intraperitoneal chemotherapy versus systemic chemotherapy for colorectal peritoneal metastases: A randomised trial. European journal of cancer (Oxford, England : 1990) 2016, 53, 155–162. [Google Scholar] [CrossRef]
- Quénet, F.; Elias, D.; Roca, L.; Goéré, D.; Ghouti, L.; Pocard, M.; Facy, O.; Arvieux, C.; Lorimier, G.; Pezet, D.; et al. Cytoreductive surgery plus hyperthermic intraperitoneal chemotherapy versus cytoreductive surgery alone for colorectal peritoneal metastases (PRODIGE 7): a multicentre, randomised, open-label, phase 3 trial. he Lancet. Oncology 2021, 22, 256–266. [Google Scholar] [CrossRef]
- Goéré, D.; Glehen, O.; Quenet, F.; Guilloit, J.M.; Bereder, J.M.; Lorimier, G.; Thibaudeau, E.; Ghouti, L.; Pinto, A.; Tuech, J.J.; et al. Second-look surgery plus hyperthermic intraperitoneal chemotherapy versus surveillance in patients at high risk of developing colorectal peritoneal metastases (PROPHYLOCHIP-PRODIGE 15): a randomised, phase 3 study. The Lancet. Oncology 2020, 21, 1147–1154. [Google Scholar] [CrossRef] [PubMed]
- Mo, S.; Cai, G. Multidisciplinary Treatment for Colorectal Peritoneal Metastases: Review of the Literature. Gastroenterology Research and Practice 2016, 2016, 1516259. [Google Scholar] [CrossRef]
- Rodriguez-Bigas, M.A.; Lin, E.H.; Crane, C.H. Stage IV Colorectal Cancer. Holland-Frei Cancer Medicine. 6th edition. BC Decker 2003. https://www.ncbi.nlm.nih.gov/books/NBK13267/.
- Ghiasloo, M.; Pavlenko, D.; Verhaeghe, M.; Langenhove, Z.V.; Uyttebroek, O.; Berardi, G.; Troisi, R.I.; Ceelen, W. Surgical treatment of stage IV colorectal cancer with synchronous liver metastases: A systematic review and network meta-analysis. European Journal of Surgical Oncology 2020, 46, 1203–1213. [Google Scholar] [CrossRef] [PubMed]
- Ströhlein, M.A.; Heiss, M.M. Limitations of the PRODIGE 7 trial. The Lancet Oncology 2021, 22, e178. [Google Scholar] [CrossRef]
- van Driel, W.J.; Koole, S.N.; Sikorska, K.; van Leeuwen, J.H.S.; Schreuder, H.W.; Hermans, R.H.; de Hingh, I.H.; van der Velden, J.; Arts, H.J.; Massuger, L.F.; et al. Hyperthermic Intraperitoneal Chemotherapy in Ovarian Cancer. New England Journal of Medicine 2018, 378, 230–240. [Google Scholar] [CrossRef]
- Sugarbaker, P.H.; der Speeten, K.V. The PRODIGE 7 randomized trial has 4 design flaws and 4 pharmacologic flaws and cannot be used to discredit other HIPEC regimens. Journal of gastrointestinal oncology 2021, 12, S129–S130. [Google Scholar] [CrossRef] [PubMed]
- Pereira, F.; Serrano, A.; Manzanedo, I.; Pérez-Viejo, E.; González-Moreno, S.; González-Bayón, L.; Arjona-Sánchez, A.; Torres, J.; Ramos, I.; Barrios, M.E.; et al. GECOP-MMC: phase IV randomized clinical trial to evaluate the efficacy of hyperthermic intraperitoneal chemotherapy (HIPEC) with mytomicin-C after complete surgical cytoreduction in patients with colon cancer peritoneal metastases. BMC Cancer 2022, 22, 536. [Google Scholar] [CrossRef]
- Park, H.J. Current Uses of Mushrooms in Cancer Treatment and Their Anticancer Mechanisms. International Journal of Molecular Sciences 2022, 23, 10502. [Google Scholar] [CrossRef]
- Sadava, D.; Still, D.W.; Mudry, R.R.; Kane, S.E. Effect of Ganoderma on drug-sensitive and multidrug-resistant small-cell lung carcinoma cells. Cancer Letters 2009, 277, 182–189. [Google Scholar] [CrossRef]
- Sohretoglu, D.; Huang, S. Ganoderma lucidum Polysaccharides as An Anti-cancer Agent. Anti-Cancer Agents in Medicinal Chemistry 2018, 18, 667–674. [Google Scholar] [CrossRef]
- Margret, A.A.; Mareeswari, R.; Kumar, K.A.; Jerley, A.A. Relative profiling of L-tryptophan derivatives from selected edible mushrooms as psychoactive nutraceuticals to inhibit P-glycoprotein: a paradigm to contest blood-brain barrier. BioTechnologia 2021, 102, 55–64. [Google Scholar] [CrossRef] [PubMed]
- Zhong, X.; Wang, G.; Li, F.; Fang, S.; Zhou, S.; Ishiwata, A.; Tonevitsky, A.G.; Shkurnikov, M.; Cai, H.; Ding, F. Immunomodulatory Effect and Biological Significance of β-Glucans. Pharmaceutics 2023, 15, 1615. [Google Scholar] [CrossRef]
- Wang, M.; Bai, Y.; Pei, J.; Li, D.; Pu, X.; Zhu, W.; Xia, L.; Qi, C.; Jiang, H.; Ning, Y. β-Glucan Combined With PD-1/PD-L1 Checkpoint Blockade for Immunotherapy in Patients With Advanced Cancer. Frontiers in pharmacology 2022, 13. [Google Scholar] [CrossRef]
- André, T.; Shiu, K.K.; Kim, T.W.; Jensen, B.V.; Jensen, L.H.; Punt, C.; Smith, D.; Garcia-Carbonero, R.; Benavides, M.; Gibbs, P.; et al. Pembrolizumab in Microsatellite-Instability–High Advanced Colorectal Cancer. The New England journal of medicine 2020, 383, 2207–2218. [Google Scholar] [CrossRef]
- Wang, G.; Wang, L.; Zhou, J.; Xu, X. The Possible Role of PD-1 Protein in Ganoderma lucidum-Mediated Immunomodulation and Cancer Treatment. Integrative cancer therapies 2019, 18. [Google Scholar] [CrossRef] [PubMed]
- Jian, L.; Cheng, H.Z.; Shubai, L. Polysaccharide Peptide Induced Colorectal Cancer Cells Apoptosis by Down-Regulating EGFR and PD-L1 Expression. Iranian journal of pharmaceutical research : IJPR 2022, 21. [Google Scholar] [CrossRef]
- Kim, T.I.; Choi, J.G.; Kim, J.H.; Li, W.; Chung, H.S. Blocking Effect of Chaga Mushroom (/textitInonotus oliquus) Extract for Immune Checkpoint CTLA-4/CD80 Interaction. Applied Sciences 2020, 10, 5774. [Google Scholar] [CrossRef]
- Randeni, N.; Xu, B. New insights into signaling pathways of cancer prevention effects of polysaccharides from edible and medicinal mushrooms. Phytomedicine 2024, 132, 155875. [Google Scholar] [CrossRef]
- Cheng, Y.; Xie, P. Ganoderic acid A holds promising cytotoxicity on human glioblastoma mediated by incurring apoptosis and autophagy and inactivating PI3K/AKT signaling pathway. Journal of Biochemical and Molecular Toxicology 2019, 33, e22392. [Google Scholar] [CrossRef]
- Joseph, T.P.; Chanda, W.; Padhiar, A.A.; Batool, S.; LiQun, S.; Zhong, M.T.; Huang, M. A Preclinical Evaluation of the Antitumor Activities of Edible and Medicinal Mushrooms: A Molecular Insight. Integrative cancer therapies 2018, 17, 200–209. [Google Scholar] [CrossRef]
- Kang, J.H.; Jang, J.E.; Mishra, S.K.; Lee, H.J.; Nho, C.W.; Shin, D.; Jin, M.; Kim, M.K.; Choi, C.; Oh, S.H. Ergosterol peroxide from Chaga mushroom (Inonotus obliquus) exhibits anti-cancer activity by down-regulation of the β-catenin pathway in colorectal cancer. Journal of Ethnopharmacology 2015, 173, 303–312. [Google Scholar] [CrossRef] [PubMed]
- Ina, H.; Yoneda, M.; Kanda, M. Lentinan, A Shiitake Mushroom β-Glucan, Stimulates Tumor-Specific Adaptive Immunity through PD-L1 Down-Regulation in Gastric Cancer Cells. Medicinal chemistry 2016, 6. [Google Scholar] [CrossRef]
- Thyagarajan, A.; Jedinak, A.; Nguyen, H.; Terry, C.; Baldridge, L.A.; Jiang, J.; Sliva, D. Triterpenes From Ganoderma Lucidum Induce Autophagy in Colon Cancer Through the Inhibition of p38 Mitogen-Activated Kinase (p38 MAPK). Nutrition and Cancer 2010, 62, 630–640. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.L.H.; Chik, S.C.C.; Lau, A.S.Y.; Chan, G.C.F. Coriolus versicolor and its bioactive molecule are potential immunomodulators against cancer cell metastasis via inactivation of MAPK pathway. Journal of Ethnopharmacology 2023, 301, 115790. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.L.; Meng, M.; Liu, S.B.; Wang, L.R.; Hou, L.H.; Cao, X.H. A chemically sulfated polysaccharide from Grifola frondos induces HepG2 cell apoptosis by notch1-NF-κB pathway. Carbohydrate polymers 2013, 95, 282–287. [Google Scholar] [CrossRef]
- Gao, Y.; Dai, X.; Chen, G.; Ye, J.; Zhou, S. A Randomized, Placebo-Controlled, Multicenter Study of Ganoderma lucidum (W.Curt.:Fr.) Lloyd (Aphyllophoromycetideae) Polysaccharides (Ganopoly) in Patients with Advanced Lung Cancer. International Journal of Medicinal Mushrooms 2003, 5, 14. [Google Scholar] [CrossRef]
- Zhao, H.; Zhang, Q.; Zhao, L.; Huang, X.; Wang, J.; Kang, X. Spore Powder of Ganoderma lucidum Improves Cancer-Related Fatigue in Breast Cancer Patients Undergoing Endocrine Therapy: A Pilot Clinical Trial. Evidence-based complementary and alternative medicine : eCAM 2012. [CrossRef]
- Deng, G.; Lin, H.; Seidman, A.; Fornier, M.; D’Andrea, G.; Wesa, K.; Yeung, S.; Cunningham-Rundles, S.; Vickers, A.J.; Cassileth, B. A phase I/II trial of a polysaccharide extract from Grifola frondosa (Maitake mushroom) in breast cancer patients: immunological effects. Journal of cancer research and clinical oncology 2009, 135, 1215–1221. [Google Scholar] [CrossRef]
- Israilides, C.; Kletsas, D.; Arapoglou, D.; Philippoussis, A.; Pratsinis, H.; Ebringerová, A.; Hříbalová, V.; Harding, S.E. In vitro cytostatic and immunomodulatory properties of the medicinal mushroom Lentinula edodes. Phytomedicine : international journal of phytotherapy and phytopharmacology 2008, 15, 512–519. [Google Scholar] [CrossRef]
- Wasser, S.P.; Weis, A.L. Medicinal Properties of Substances Occurring in Higher Basidiomycetes Mushrooms: Current Perspectives (Review). International Journal of Medicinal Mushrooms 1999, 1, 31–62. [Google Scholar] [CrossRef]
- Ahn, W.S.; Kim, D.J.; Chae, G.T.; Lee, J.M.; Bae, S.M.; Sin, J.I.; Kim, Y.W.; Namkoong, S.E.; Lee, I.P. Natural killer cell activity and quality of life were improved by consumption of a mushroom extract, Agaricus blazei Murill Kyowa, in gynecological cancer patients undergoing chemotherapy. Int J Gynecol Cancer 2004, 14, 589–594. [Google Scholar] [CrossRef]
- Hetland, G.; Tangen, J.M.; Mahmood, F.; Mirlashari, M.R.; Nissen-Meyer, L.S.H.; Nentwich, I.; Therkelsen, S.P.; Tjønnfjord, G.E.; Johnson, E. Antitumor, Anti-inflammatory and Antiallergic Effects of Agaricus blazei Mushroom Extract and the Related Medicinal Basidiomycetes Mushrooms, Hericium erinaceus and Grifola frondosa: A Review of Preclinical and Clinical Studies. Nutrients 2020, 12, 1339. [Google Scholar] [CrossRef] [PubMed]
- Saleh, M.H.; Rashedi, I.; Keating, A. Immunomodulatory properties of coriolus versicolor: The role of polysaccharopeptide. Frontiers in Immunology 2017, 8. [Google Scholar] [CrossRef]
- Lee, C.L.; Yang, X.; Wan, J.M.F. The culture duration affects the immunomodulatory and anticancer effect of polysaccharopeptide derived from Coriolus versicolor. Enzyme and Microbial Technology 2006, 38, 14–21. [Google Scholar] [CrossRef]
- Mao, X.W.; Archambeau, J.O.; Gridley, D.S. Immunotherapy with Low-dose Interleukin-2 and a Polysaccharopeptide Derived from Coriolus versicolor. https://home.liebertpub.com/cbr 2009, 11, 393–403. [Google Scholar] [CrossRef]
- Jędrzejewski, T.; Sobocińska, J.; Pawlikowska, M.; Dzialuk, A.; Wrotek, S. Extract from the Coriolus versicolor Fungus as an Anti-Inflammatory Agent with Cytotoxic Properties against Endothelial Cells and Breast Cancer Cells. International Journal of Molecular Sciences 2020, 21, 9063. [Google Scholar] [CrossRef] [PubMed]
- Akagi, J.; Baba, H. PSK may suppress CD57(+) T cells to improve survival of advanced gastric cancer patients. International journal of clinical oncology 2010, 15, 145–152. [Google Scholar] [CrossRef]
- Sadahiro, S.; Suzuki, T.; Maeda, Y.; Tanaka, A.; Kamijo, A.; Murayama, C.; Nakayama, Y.; Akiba, T. Effects of preoperative immunochemoradiotherapy and chemoradiotherapy on immune responses in patients with rectal adenocarcinoma. Anticancer Research 2010, 30, 993–999. [Google Scholar] [PubMed]
- Hui, K.P.Y.; Sit, W.H.; Wan, J.M.F. Induction of S phase cell arrest and caspase activation by polysaccharide peptide isolated from Coriolus versicolor enhanced the cell cycle dependent activity and apoptotic cell death of doxorubicin and etoposide, but not cytarabine in HL-60 cells. Oncology Reports 2005, 14, 145–155. [Google Scholar] [CrossRef]
- Coriolus versicolor. Purported Benefits, Side Effects & More 2024. https://www.mskcc.org/cancer-care/integrative-medicine/herbs/coriolus-versicolor.
- J, J.; D, S. Novel medicinal mushroom blend suppresses growth and invasiveness of human breast cancer cells. International journal of oncology 2010, 37. [Google Scholar] [CrossRef]
- Habtemariam, S. Trametes versicolor (Synn. Coriolus versicolor) Polysaccharides in Cancer Therapy: Targets and Efficacy. Biomedicines 2020, 8, 135. [Google Scholar] [CrossRef]
- Hsieh, T.C.; Wu, P.; Park, S.; Wu, J.M. Induction of cell cycle changes and modulation of apoptogenic/anti-apoptotic and extracellular signaling regulatory protein expression by water extracts of I’m-Yunity (PSP). BMC complementary and alternative medicine 2006, 6. [Google Scholar] [CrossRef]
- Jadrzejewski, T.; Pawlikowska, M.; SobociÅska, J.; Wrotek, S. Protein-Bound Polysaccharides from Coriolus Versicolor Fungus Disrupt the Crosstalk Between Breast Cancer Cells and Macrophages through Inhibition of Angiogenic Cytokines Production and Shifting Tumour-Associated Macrophages from the M2 to M1 Subtype. Cellular Physiology & Biochemistry 2020, 54, 615–628. [Google Scholar] [CrossRef]
- Ho, J.C.; Konerding, M.A.; Gaumann, A.; Groth, M.; Liu, W.K. Fungal polysaccharopeptide inhibits tumor angiogenesis and tumor growth in mice. Life Sciences 2004, 75, 1343–1356. [Google Scholar] [CrossRef]
- Kobayashi, H.; Matsunaga, K.; Oguchi, Y. Antimetastatic effects of PSK (Krestin), a protein-bound polysaccharide obtained from basidiomycetes: an overview. Cancer epidemiology, biomarkers & prevention: a publication of the American Association for Cancer Research, cosponsored by the American Society of Preventive Oncology 1995, 4, 275–281. [Google Scholar] [PubMed]
- Luo, K.W.; Yue, G.G.L.; Ko, C.H.; Lee, J.K.M.; Gao, S.; Li, L.F.; Li, G.; Fung, K.P.; Leung, P.C.; Lau, C.B.S. In vivo and in vitro anti-tumor and anti-metastasis effects of Coriolus versicolor aqueous extract on mouse mammary 4T1 carcinoma. Phytomedicine : international journal of phytotherapy and phytopharmacology 2014, 21, 1078–1087. [Google Scholar] [CrossRef] [PubMed]
- Yoshikawa, R.; Yanagi, H.; Noda, M.; Yamamura, T.; Hashimoto-Tamaoki, T. Polysaccharide-K (PSK) inhibits distant metastasis in colorectal cancer dependent on ECA39. American Association for Cancer Research 2005, 65, 1538–7445. [Google Scholar]
- Zhong, L.; Yan, P.; Lam, W.C.; Yao, L.; Bian, Z. Coriolus Versicolor and Ganoderma Lucidum Related Natural Products as an Adjunct Therapy for Cancers: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Frontiers in Pharmacology 2019, 10, 420994. [Google Scholar] [CrossRef]
- Mycomedicinals (Mushrooms) for Cancer. U.S. Department of Veterans Affairs 2024. https://www.va.gov/WHOLEHEALTHLIBRARY/tools/mycomedicinals-mushrooms-for-cancer.asp.
- Medicinal Mushrooms (PDQ®)–Health Professional Version. National Cancer Institute NIH, 2024. https://www.cancer.gov/about-cancer/treatment/cam/hp/mushrooms-pdq.
- Cizmarikova, M. The Efficacy and Toxicity of Using the Lingzhi or Reishi Medicinal Mushroom, Ganoderma lucidum (Agaricomycetes), and Its Products in Chemotherapy (Review). International journal of medicinal mushrooms 2017, 19, 861–877. [Google Scholar] [CrossRef]
- Jin, X.; Beguerie, J.R.; yeun Sze, D.M.; Chan, G.C. Ganoderma lucidum (Reishi mushroom) for cancer treatment. Cochrane Database of Systematic Reviews 2012. [Google Scholar] [CrossRef]
- Jin, X.; Beguerie, J.R.; Sze, D.M.Y.; Chan, G.C. Ganoderma lucidum (Reishi mushroom) for cancer treatment. The Cochrane Database of Systematic Reviews 2016, 2016, CD007731. [Google Scholar] [CrossRef]
- Phase II Clinical Trial Scheme of Ganoderma Lucidum Spore Powder for Postoperative Chemotherapy of Osteosarcoma, (ongoing clinical research). https://clinicaltrials.gov/study/NCT04319874.
- Oka, S.; Tanaka, S.; Yoshida, S.; Hiyama, T.; Ueno, Y.; Ito, M.; Kitadai, Y.; Yoshihara, M.; Chayama, K. A water-soluble extract from culture medium of Ganoderma lucidum mycelia suppresses the development of colorectal adenomas. Hiroshima Journal of Medical Sciences 2010, 59, 1–6. [Google Scholar] [PubMed]
- Zhang, Y.; Jiang, Y.; Zhang, M.; Zhang, L. Ganoderma sinense polysaccharide: An adjunctive drug used for cancer treatment. Progress in molecular biology and translational science 2019, 163, 165–177. [Google Scholar] [CrossRef] [PubMed]
- Konno, S. Synergistic potentiation of D-fraction with vitamin C as possible alternative approach for cancer therapy. International journal of general medicine 2009, 2, 91–108. [Google Scholar] [CrossRef] [PubMed]
- Nanba, H. Maitake D-fraction: Healing and Preventive Potential for Cancer. The Journal of Orthomolecular Medicine 1997, 12, https://orthomolecular.org/library/jom/1997/articles/1997-v12n01–p043shtml. [Google Scholar]
- Kodama, N.; Komuta, K.; Nanba, H. Can maitake MD-fraction aid cancer patients? Alternative Medicine Review 2002, 7, 236–239. [Google Scholar] [PubMed]
- Zhang, M.; Zhang, Y.; Zhang, L.; Tian, Q. Mushroom polysaccharide lentinan for treating different types of cancers: A review of 12 years clinical studies in China. Progress in molecular biology and translational science 2019, 163, 297–328. [Google Scholar] [CrossRef]
- Cheetham, P.; Lifton, D. The Patient’s Guide to AHCC Active Hexose Correlated Compound. The Clinically Proven Nutrient Supported By 25 Clinical Studies 2012. [Google Scholar]
- Cowawintaweewat, S.; Manoromana, S.; Sriplung, H.; Khuhaprema, T.; Tongtawe, P.; Tapchaisri, P.; Chaicumpa, W. Prognostic improvement of patients with advanced liver cancer after active hexose correlated compound (AHCC) treatment. Asian Pacific Journal of Allergy and Immunology 2006, 24, 33–45. [Google Scholar] [PubMed]
- Ghoneum, M.; Wimbley, M.; Salem, F.; Mcklain, A.; Attallah, N.; Gill, G. Immunomodulatory and anticancer effects of active hemicellulose compound (AHCC). International Journal of Immunotherapy 1995, 11, 23–28. [Google Scholar]
- Matsui, Y.; Uhara, J.; Satoi, S.; Kaibori, M.; Yamada, H.; Kitade, H.; Imamura, A.; Takai, S.; Kawaguchi, Y.; Kwon, A.H.; et al. Improved prognosis of postoperative hepatocellular carcinoma patients when treated with functional foods: A prospective cohort study. Journal of Hepatology 2002, 37, 78–86. [Google Scholar] [CrossRef]
- He, Z.; Lin, J.; He, Y.; Liu, S. Polysaccharide-Peptide from Trametes versicolor: The Potential Medicine for Colorectal Cancer Treatment. Biomedicines 2022, 10, 2841. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.; Zhang, M.; Jiang, Y.; Liu, Y.; Luo, H.; Hao, C.; Zeng, P.; Zhang, L. Preclinical and clinical studies of Coriolus versicolor polysaccharopeptide as an immunotherapeutic in China. Discovery Medicine 2017, 23, 207–219. [Google Scholar] [PubMed]
- Eliza, W.L.; Fai, C.K.; Chung, L.P. Efficacy of Yun Zhi (Coriolus versicolor) on survival in cancer patients: systematic review and meta-analysis. Recent patents on inflammation & allergy drug discovery 2012, 6, 78–87. [Google Scholar] [CrossRef]
- Fritz, H.; Kennedy, D.A.; Ishii, M.; Fergusson, D.; Fernandes, R.; Cooley, K.; Seely, D. Polysaccharide K and Coriolus versicolor extracts for lung cancer: a systematic review. Integrative cancer therapies 2015, 14, 201–211. [Google Scholar] [CrossRef]
- Pilkington, K.; Wieland, L.S.; Teng, L.; Jin, X.Y.; Storey, D.; Liu, J.P. Coriolus (Trametes) versicolor mushroom to reduce adverse effects from chemotherapy or radiotherapy in people with colorectal cancer. Cochrane Database of Systematic Reviews 2022. [Google Scholar] [CrossRef]
- Introduction to GRADE (Grading of Recommendations Assessment, Development and Evaluation). https://training.cochrane.org/introduction-grade.
- Oba, K.; Teramukai, S.; Kobayashi, M.; Matsui, T.; Kodera, Y.; Sakamoto, J. Efficacy of adjuvant immunochemotherapy with polysaccharide K for patients with curative resections of gastric cancer. Cancer immunology, immunotherapy : CII 2007, 56, 905–911. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, J.; Morita, S.; Oba, K.; Matsui, T.; Kobayashi, M.; Nakazato, H.; Ohashi, Y. Efficacy of adjuvant immunochemotherapy with polysaccharide K for patients with curatively resected colorectal cancer: a meta-analysis of centrally randomized controlled clinical trials. Cancer immunology, immunotherapy : CII 2006, 55, 404–411. [Google Scholar] [CrossRef]
- Yoshitani, S.I.; Takashima, S. Efficacy of postoperative UFT (Tegafur/Uracil) plus PSK therapies in elderly patients with resected colorectal cancer. Cancer biotherapy & radiopharmaceuticals 2009, 24, 35–40. [Google Scholar] [CrossRef]
- Sakai, T.; Yamashita, Y.; Maekawa, T.; Mikami, K.; Hoshino, S.; Shirakusa, T. Immunochemotherapy with PSK and fluoropyrimidines improves long-term prognosis for curatively resected colorectal cancer. Cancer biotherapy & radiopharmaceuticals 2008, 23, 461–468. [Google Scholar] [CrossRef]
- Tsang, K.W.; Lam, C.L.; Yan, C.; Mak, J.C.; Ooi, G.C.; Ho, J.C.; Lam, B.; Man, R.; Sham, J.S.; Lam, W.K. Coriolus versicolor polysaccharide peptide slows progression of advanced non-small cell lung cancer. Respiratory medicine 2003, 97, 618–624. [Google Scholar] [CrossRef]
- Miyake, Y.; Nishimura, J.; Kato, T.; Ikeda, M.; Tsujie, M.; Hata, T.; Takemasa, I.; Mizushima, T.; Yamamoto, H.; Sekimoto, M.; et al. Phase III trial comparing UFT + PSK to UFT + LV in stage IIB, III colorectal cancer (MCSGO-CCTG). Surgery today 2018, 48, 66–72. [Google Scholar] [CrossRef] [PubMed]
- Niimoto, M.; Hattori, T.; Tamada, R.; Sugimachi, K.; Inokuchi, K.; Ogawa, N. Postoperative adjuvant immunochemotherapy with mitomycin C, futraful and PSK for gastric cancer. An analysis of data on 579 patients followed for five years. The Japanese journal of surgery 1988, 18, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Torisu, M.; Hayashi, Y.; Ishimitsu, T.; Fujimura, T.; Iwasaki, K.; Katano, M.; Yamamoto, H.; Kimura, Y.; Takesue, M.; Kondo, M.; et al. Significant prolongation of disease-free period gained by oral polysaccharide K (PSK) administration after curative surgical operation of colorectal cancer. Cancer immunology, immunotherapy : CII 1990, 31, 261–268. [Google Scholar] [CrossRef]
- Mitomi, T.; Tsuchiya, S.; Iijima, N.; Aso, K.; Suzuki, K.; Nishiyama, K.; Amano, T.; Takahashi, T.; Murayama, N.; Oka, H.; et al. Randomized, controlled study on adjuvant immunochemotherapy with PSK in curatively resected colorectal cancer. The Cooperative Study Group of Surgical Adjuvant Immunochemotherapy for Cancer of Colon and Rectum (Kanagawa). Diseases of the colon and rectum 1992, 35, 123–130. [Google Scholar] [CrossRef] [PubMed]
- Nakazato, H.; Koike, A.; Saji, S.; Ogawa, N.; Sakamoto, J. Efficacy of immunochemotherapy as adjuvant treatment after curative resection of gastric cancer. Study Group of Immunochemotherapy with PSK for Gastric Cancer. Lancet (London, England) 1994, 343, 1122–1126. [Google Scholar] [CrossRef]
- Ogoshi, K.; Satou, H.; Isono, K.; Mitomi, T.; Endoh, M.; Sugita, M. Immunotherapy for esophageal cancer. A randomized trial in combination with radiotherapy and radiochemotherapy. Cooperative Study Group for Esophageal Cancer in Japan. American journal of clinical oncology 1995, 18, 216–222. [Google Scholar] [CrossRef] [PubMed]
- T, T.; Y, Y. Protein-bound polysaccharide increases survival in resected gastric cancer cases stratified with a preoperative granulocyte and lymphocyte count. Oncology reports 2000, 7, 1157–1161. [Google Scholar] [CrossRef]
- Ito, K.; Nakazato, H.; Koike, A.; Takagi, H.; Saji, S.; Baba, S.; Mai, M.; Sakamoto, J.I.; Ohashi, Y. Long-term effect of 5-fluorouracil enhanced by intermittent administration of polysaccharide K after curative resection of colon cancer. A randomized controlled trial for 7-year follow-up. International journal of colorectal disease 2004, 19, 157–164. [Google Scholar] [CrossRef]
- Ohwada, S.; Ikeya, T.; Yokomori, T.; Kusaba, T.; Roppongi, T.; Takahashi, T.; Nakamura, S.; Kakinuma, S.; Iwazaki, S.; Ishikawa, H.; et al. Adjuvant immunochemotherapy with oral Tegafur/Uracil plus PSK in patients with stage II or III colorectal cancer: a randomised controlled study. British journal of cancer 2004, 90, 1003–1010. [Google Scholar] [CrossRef]
- Shichinohe, T.; Komatsu, Y.; Akazawa, K.; Yuki, S.; Fukushima, H.; Ohno, K.; Nakamura, F.; Kusumi, T.; Morita, T.; Senmaru, N.; et al. Randomized phase III clinical study comparing postoperative UFT/LV,UFT+LV/UFT and UFT+LV+PSK/UFT+PSK as adjuvant therapy for curatively resected stage III colorectal cancer HGCSG-CAD study. Journal of Clinical Oncology 2013, 31, 3638–3638. [Google Scholar] [CrossRef]
- Ogawa, H.; Shiraishi, T.; Okada, T.; Miyamae, Y.; Motegi, Y.; Shirabe, K.; Saeki, H. Adjuvant Chemotherapy With UFT/LV Versus UFT/LV Plus PSK in Stage II/III Colorectal Cancer. Anticancer Research 2024, 44, 805–814. [Google Scholar] [CrossRef] [PubMed]
- Veroniki, A.A.; Jackson, D.; Viechtbauer, W.; Bender, R.; Bowden, J.; Knapp, G.; Kuss, O.; Higgins, J.P.; Langan, D.; Salanti, G. Methods to estimate the between-study variance and its uncertainty in meta-analysis. Research synthesis methods 2016, 7, 55–79. [Google Scholar] [CrossRef]
- Venturella, G.; Ferraro, V.; Cirlincione, F.; Gargano, M.L. Medicinal Mushrooms: Bioactive Compounds, Use, and Clinical Trials. International Journal of Molecular Sciences 2021, 22, 634. [Google Scholar] [CrossRef]
- Łysakowska, P.; Sobota, A.; Wirkijowska, A. Medicinal Mushrooms: Their Bioactive Components, Nutritional Value and Application in Functional Food Production—A Review. Molecules 2023, 28, 5393. [Google Scholar] [CrossRef] [PubMed]
- Cadar, E.; Negreanu-Pirjol, T.; Pascale, C.; Sirbu, R.; Prasacu, I.; Negreanu-Pirjol, B.S.; Tomescu, C.L.; Ionescu, A.M. Natural Bio-Compounds from Ganoderma lucidum and Their Beneficial Biological Actions for Anticancer Application: A Review. Antioxidants 2023, 12, 1907. [Google Scholar] [CrossRef]
- Ekiz, E.; Oz, E.; El-Aty, A.M.A.; Proestos, C.; Brennan, C.; Zeng, M.; Tomasevic, I.; Elobeid, T.; Çadırcı, K.; Bayrak, M.; et al. Exploring the Potential Medicinal Benefits of Ganoderma lucidum: From Metabolic Disorders to Coronavirus Infections. Foods 2023, 12, 1512. [Google Scholar] [CrossRef] [PubMed]
- Choong, Y.K.; Ellan, K.; Chen, X.D.; Mohamad, S.A. Extraction and Fractionation of Polysaccharides from a Selected Mushroom Species, Ganoderma lucidum: A Critical Review. Fractionation. IntechOpen 2018. [Google Scholar] [CrossRef]
- Tomoda, M.; Gonda, R.; Kasahara, Y.; Hikino, H. Glycan structures of ganoderans B and C, hypoglycemic glycans of ganoderma lucidum fruit bodies. Phytochemistry 1986, 25, 2817–2820. [Google Scholar] [CrossRef]
- Wu, J.Y.; Siu, K.C.; Geng, P. Bioactive Ingredients and Medicinal Values of Grifola frondosa (Maitake). Foods 2021, 10, 95. [Google Scholar] [CrossRef]
- Kodama, N.; Murata, Y.; Asakawa, A.; Inui, A.; Hayashi, M.; Sakai, N.; Nanba, H. Maitake D-Fraction enhances antitumor effects and reduces immunosuppression by mitomycin-C in tumor-bearing mice. Nutrition 2005, 21, 624–629. [Google Scholar] [CrossRef]
- Zhang, Y.; Li, S.; Wang, X.; Zhang, L.; Cheung, P.C. Advances in lentinan: Isolation, structure, chain conformation and bioactivities. Food Hydrocolloids 2011, 25, 196–206. [Google Scholar] [CrossRef]
- Lentinan - an overview | ScienceDirect Topics 2016. https://www.sciencedirect.com/topics/immunology-and-microbiology/lentinan.
- Fujii, H.; Nishioka, N.; Simon, R.R.; Kaur, R.; Lynch, B.; Roberts, A. Genotoxicity and subchronic toxicity evaluation of Active Hexose Correlated Compound (AHCC). Regulatory Toxicology and Pharmacology 2011, 59, 237–250. [Google Scholar] [CrossRef] [PubMed]
- Shin, M.S.; Park, H.J.; Maeda, T.; Nishioka, H.; Fujii, H.; Kang, I. The Effects of AHCC®, a Standardized Extract of Cultured Lentinura edodes Mycelia, on Natural Killer and T Cells in Health and Disease: Reviews on Human and Animal Studies. Journal of Immunology Research 2019, 2019, 3758576. [Google Scholar] [CrossRef]
- Dou, H.; Chang, Y.; Zhang, L. Coriolus versicolor polysaccharopeptide as an immunotherapeutic in China. Progress in Molecular Biology and Translational Science 2019, 163, 361–381. [Google Scholar] [CrossRef]
- Zhang, X.; Cai, Z.; Mao, H.; Hu, P.; Li, X. Isolation and structure elucidation of polysaccharides from fruiting bodies of mushroom Coriolus versicolor and evaluation of their immunomodulatory effects. International Journal of Biological Macromolecules 2021, 166, 1387–1395. [Google Scholar] [CrossRef]
- Jing, Y.; Zhang, S.; Li, M.; Ma, Y.; Zheng, Y.; Zhang, D.; Wu, L.; Vinson, J.; Jing, Y.; Zhang, S.; et al. Research Progress on the Extraction, Structure, and Bioactivities of Polysaccharides from Coriolus versicolor. Foods 2022, 11, 2126. [Google Scholar] [CrossRef] [PubMed]
- Cui, J.; Chisti, Y. Polysaccharopeptides of Coriolus versicolor: physiological activity, uses, and production. Biotechnology Advances 2003, 21, 109–122. [Google Scholar] [CrossRef]
- Wang, Y.; Yuan, A.J.; Wu, Y.J.; Wu, L.M.; Zhang, L. Silymarin in cancer therapy: Mechanisms of action, protective roles in chemotherapy-induced toxicity, and nanoformulations. Journal of Functional Foods 2023, 100, 105384. [Google Scholar] [CrossRef]
- Montgomery, A.; Adeyeni, T.; San, K.; Heuertz, R.M.; Ezekiel, U.R. Curcumin Sensitizes Silymarin to Exert Synergistic Anticancer Activity in Colon Cancer Cells. Journal of Cancer 2016, 7, 1250–1257. [Google Scholar] [CrossRef]
- Yang, S.H.; Lin, J.K.; Chen, W.S.; Chiu, J.H. Anti-angiogenic effect of silymarin on colon cancer lovo cell line. Journal of Surgical Research 2003, 113, 133–138. [Google Scholar] [CrossRef]
- Fallah, M.; Davoodvandi, A.; Nikmanzar, S.; Aghili, S.; Mirazimi, S.M.A.; Aschner, M.; Rashidian, A.; Hamblin, M.R.; Chamanara, M.; Naghsh, N.; et al. Silymarin (milk thistle extract) as a therapeutic agent in gastrointestinal cancer. Biomedicine & Pharmacotherapy 2021, 142, 112024. [Google Scholar] [CrossRef]
- D, D.; J, X.; A, V.; V, A. Silymarin and Cancer: A Dual Strategy in Both in Chemoprevention and Chemosensitivity. Moluecules 2020, 25, 2009. [Google Scholar] [CrossRef]
- Erfanian, S.S.; Ansari, H.; Javanmard, S.H.; Amini, Z.; Hajigholami, A. The hepatorenal protective effects of silymarin in cancer patients receiving chemotherapy: a randomized, placebo-controlled trial. BMC Complementary Medicine and Therapies 2024, 24, 329. [Google Scholar] [CrossRef]
- Jaffar, H.M.; Al-Asmari, F.; Khan, F.A.; Rahim, M.A.; Zongo, E. Silymarin: Unveiling its pharmacological spectrum and therapeutic potential in liver diseases — A comprehensive narrative review. Food Science & Nutrition 2024, 12, 3097–3111. [Google Scholar] [CrossRef]
- Gillessen, A.; Schmidt, H.H.J. Silymarin as Supportive Treatment in Liver Diseases: A Narrative Review. Adv Ther 2020, 37, 1279–1301. [Google Scholar] [CrossRef] [PubMed]
- Emadi, S.A.; Rahbardar, M.G.; Mehri, S.; Hosseinzadeh, H. A review of therapeutic potentials of milk thistle (Silybum marianum L.) and its main constituent, silymarin, on cancer, and their related patents. Iran J Basic Med Sci 2022, 25, 1166–1176. [Google Scholar] [CrossRef]
- Moezian, G.S.A.; Javadinia, S.A.; Sales, S.S.; Fanipakdel, A.; Elyasi, S.; Karimi, G. Oral silymarin formulation efficacy in management of AC-T protocol induced hepatotoxicity in breast cancer patients: A randomized, triple blind, placebo-controlled clinical trial. J Oncol Pharm Pract 2022, 28, 827–835. [Google Scholar] [CrossRef]
- Colombo, V.; Lupi, M.; Falcetta, F.; Forestieri, D.; D’Incalci, M.; Ubezio, P. Chemotherapeutic activity of silymarin combined with doxorubicin or paclitaxel in sensitive and multidrug-resistant colon cancer cells. Cancer Chemother Pharmacol 2011, 67, 369–379. [Google Scholar] [CrossRef]

Table 1.
Treatment-Specific Survival Rates for PM
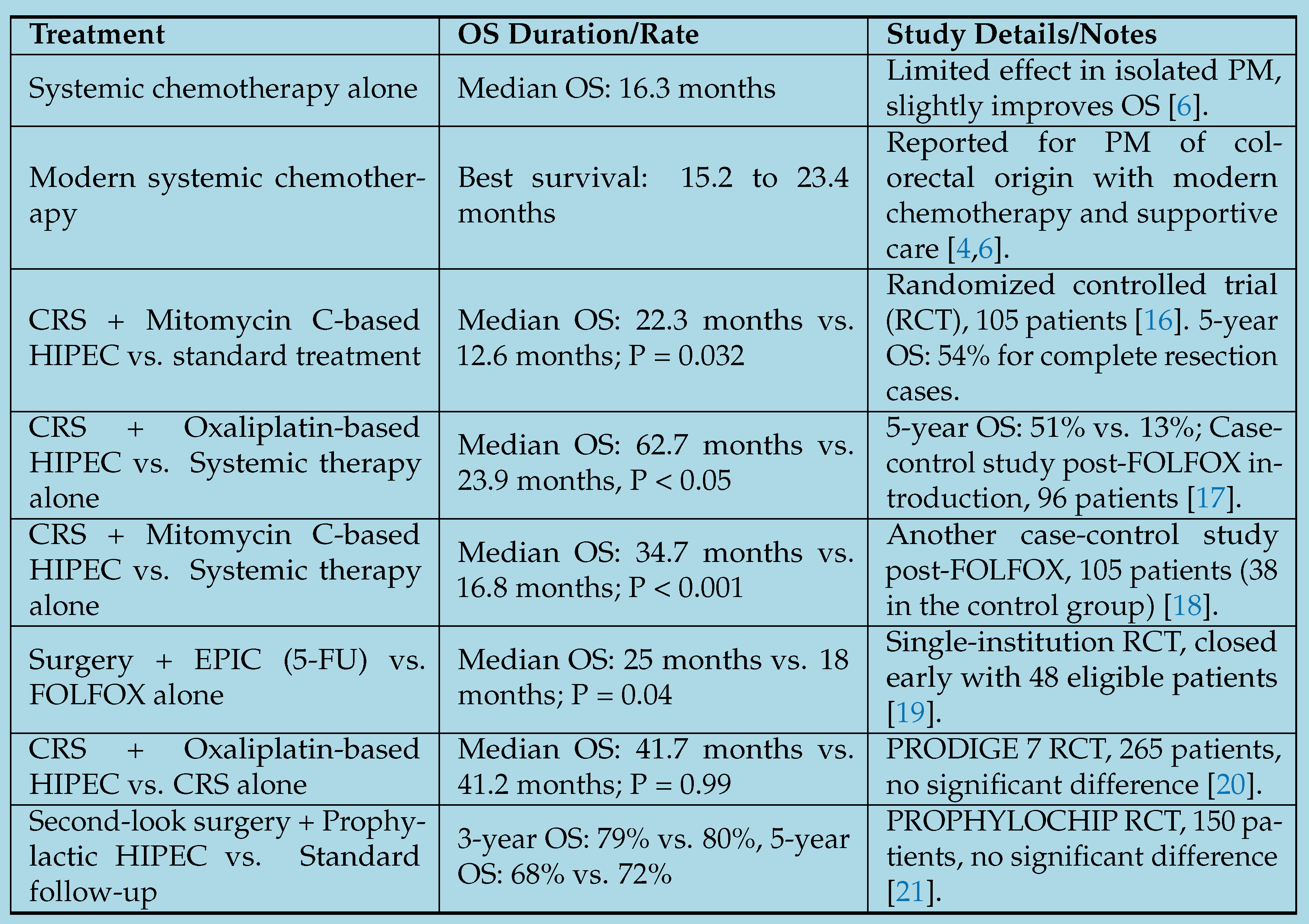
Table 2.
Medicinal Mushrooms and Their Mechanisms of Action.
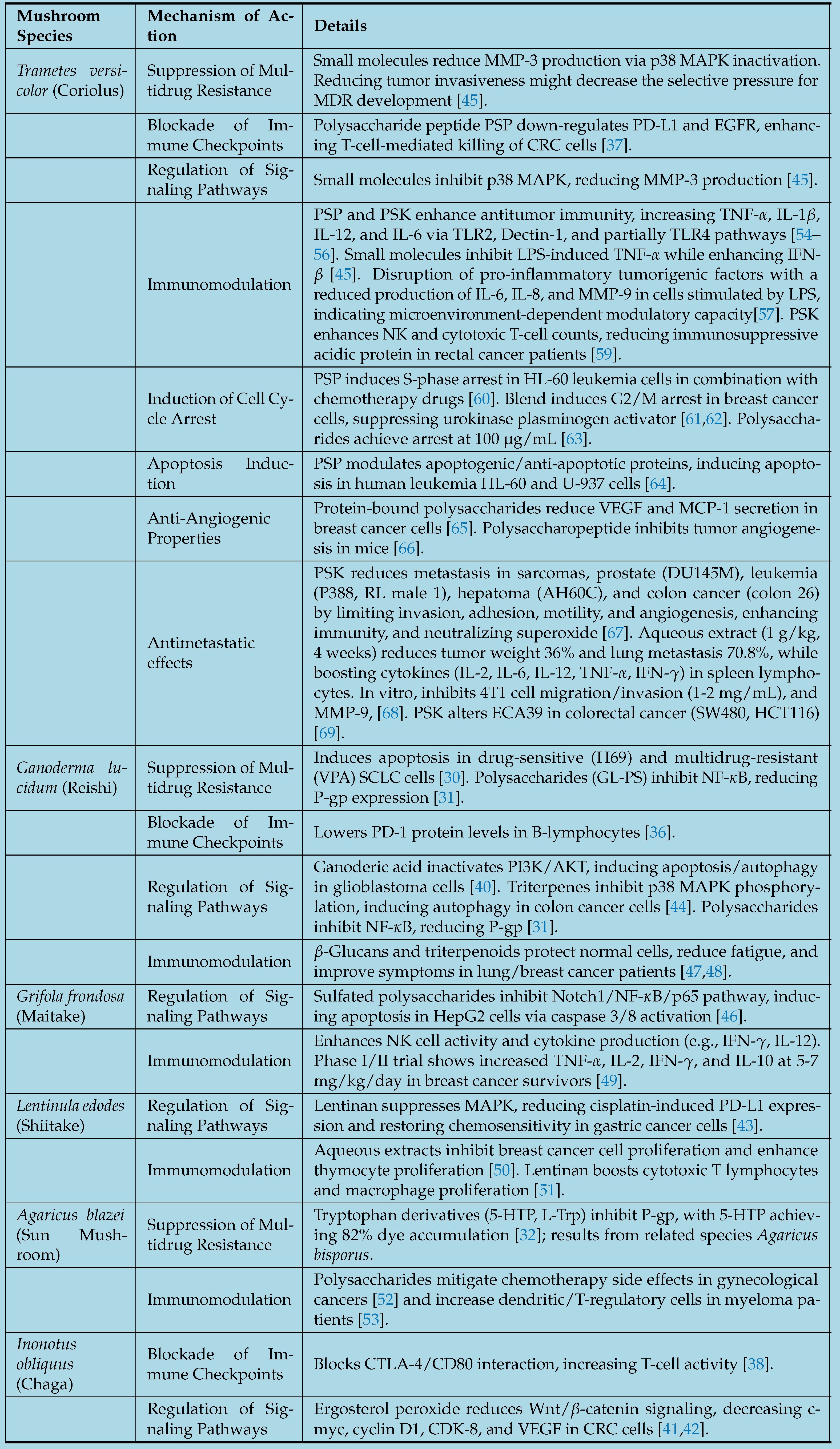
Table 3.
Note: Only the studies marked with an asterisk (*) were included in the meta-analysis.
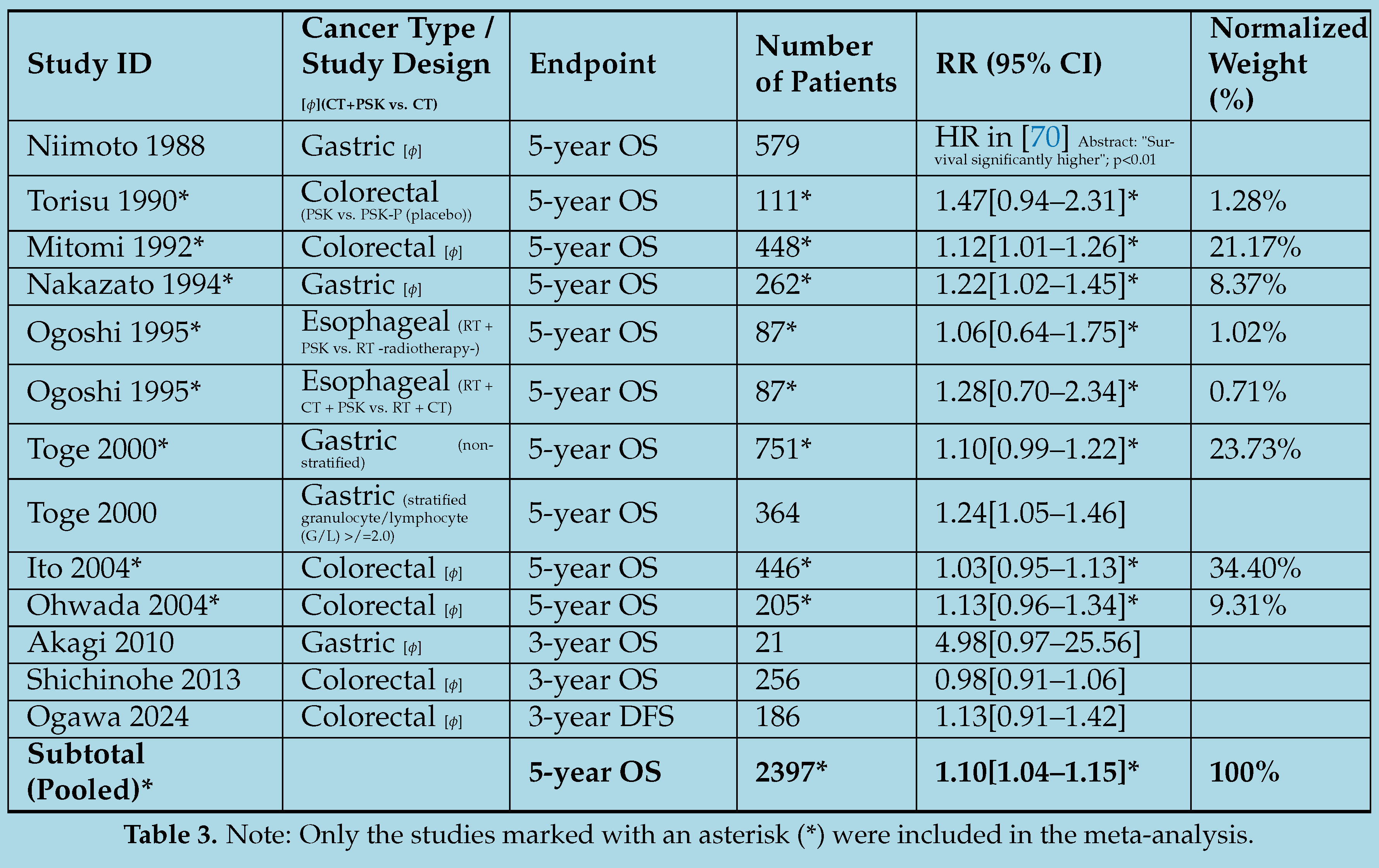
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



