
Submitted:
24 April 2025
Posted:
25 April 2025
You are already at the latest version
Abstract
The increasing demand for orthopedic and neurosurgical implants has driven ad-vancements in biomaterials, additive manufacturing, and antimicrobial strategies. With a growing aging population and a high incidence of orthopedic trauma in developing countries, the need for effective, biocompatible, and infection-resistant implants is more critical than ever. This review explores the role of polymers in 3D printing for medical applications, focusing on their use in orthopedic and neurosurgical implants. Polylactic acid (PLA), polycaprolactone (PCL), and polyetheretherketone (PEEK) have gained at-tention due to their biocompatibility, mechanical properties, and potential for antimi-crobial modifications. A major challenge in implantology is the risk of periprosthetic joint infections (PJI) and surgical site infections (SSI). Current strategies, such as antibi-otic-loaded polymethylmethacrylate (PMMA) spacers and bioactive coatings, aim to reduce infection rates, but limitations remain. Additive manufacturing enables the cre-ation of customized implants with tailored porosity for enhanced osseointegration while allowing the incorporation of antimicrobial agents. Future perspectives include the in-tegration of artificial intelligence for implant design, nanotechnology for smart coatings, and bioresorbable scaffolds for improved bone regeneration. Advancing these tech-nologies will lead to more efficient, cost-effective, and patient-specific solutions, ultimately reducing infection rates and improving long-term clinical outcomes.
Keywords:
antimicrobial stewardship
; rapid diagnostic methods
; mHealth
; eHealth
; antimicrobial resistance
; pharmacotherapeutic algorithms
1. Introduction
The global population is following a trend of demographic aging, aligning with worldwide statistics. In other words, life expectancy is increasing, and consequently, the prevalence of degenerative diseases is rising at the same rate. In an effort to restore motor functions and relieve pain, arthroplasties have become increasingly frequent treatment options [1]. At the other extreme, many underdeveloped countries have a large population of young adults, a deficient public transportation system, vast metropolitan areas, and a low level of education [2]. These factors culminate in a rising number of orthopedic traumas and severe polytraumas, such as traumatic brain injuries (TBI) [3]. Arthroplasty is a procedure that aids in mobility, joint discomfort, and pain relief for patients with various musculoskeletal disorders, with advanced age being one of the most common reasons for undergoing the procedure [4].
Among arthroplasties—whether of the hip, knee, or shoulder—it is estimated that between 1% and 3% of procedures will develop acute or late infections, leading to the removal of the prosthesis and its replacement with spacers [5]. In cases of periprosthetic joint infection (PJI), an additional surgical intervention is required, which may involve removing the implant and inserting a temporary antibiotic-loaded spacer. This spacer occupies the space left by the removed prosthesis, maintaining limb stability and alignment while releasing antibiotics to treat the infection. Typically made of polymethylmethacrylate (PMMA), spacers can be commercially available or custom-made by the surgeon. Due to the high cost of commercial spacers, many are handcrafted, which increases surgical time, risk of bleeding, reoperations, spacer breakage, and reduces functionality [6].
In this review, we will discuss aspects of polymers for 3D printing in the context of orthopedic and neurosurgical implants, expanding the focus of these materials to additive manufacturing with antimicrobial agents.
2. Epidemiology of Orthopedical Implant Infections and Cranioplasty
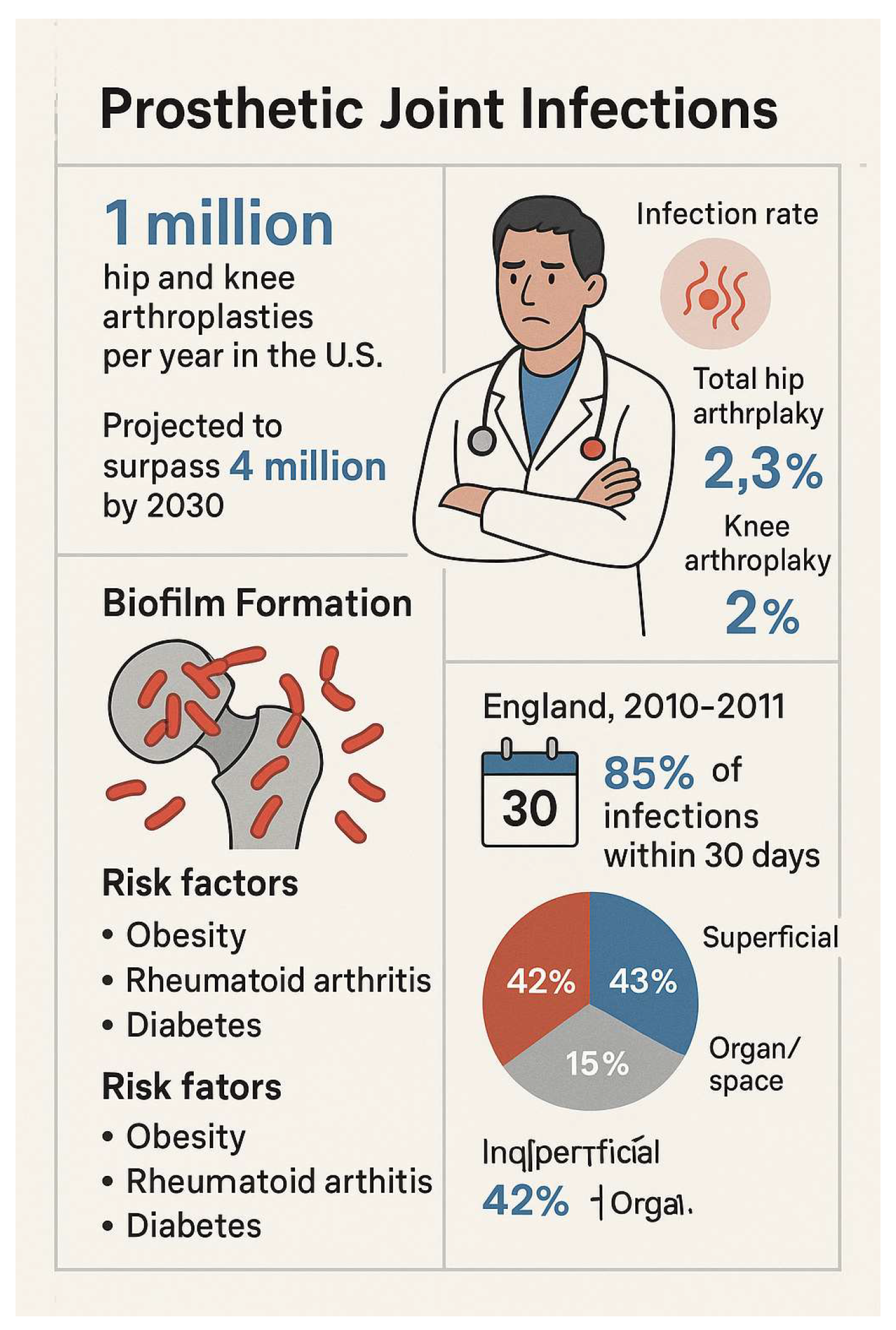
In the United States, approximately 1 million hip and knee arthroplasties are performed annually, with a significant increase in revision surgeries. Between 2005 and 2030, the total number of procedures is expected to surpass 4 million. Despite improvements in aseptic conditions and antibiotic prophylaxis, infection rates following arthroplasties are rising globally. A study conducted in California reported infection rates of 2.3% after total hip arthroplasties and 2% for knee arthroplasties. In Portugal, data from a study at Hospital de Santo António indicated that the average cost of an aseptic revision is more than three times that of a primary arthroplasty without complications and 1.5 times higher than the cost of revisions due to non-infectious causes [7].
Surgical site infections (SSIs) are among the most frequent complications following medical procedures in healthcare facilities. They contribute to prolonged hospital stays, increased hospitalization costs, morbidity, and mortality [8]. The infection rate following knee prosthesis implantation ranges from 0.8% to 1.9%, while for total hip prostheses, it varies between 0.3% and 1.7% [8]. The mortality associated with prosthetic infections in elderly patients is estimated to be between 5% and 10% of cases [9].
Infections are directly linked to prosthetic contamination, which may occur during prosthesis handling in the operating room due to the presence of pathogens resulting from inadequate hygiene, poor asepsis at the surgical site, improperly sterilized equipment, inadequate personal hygiene of the medical team, or incorrect pre-surgical prosthesis cleaning [10]. Contamination results from multiple factors, including bacterial elements, prosthetic material, and host-related factors. Bacterial adhesion to prosthetic surfaces depends on the material used, influenced by smoothness and porosity [10].
Several factors increase the risk of infection in surgical patients, including comorbidities such as obesity, poor nutritional status, rheumatoid arthritis, and diabetes mellitus, in addition to superficial wound complications. Obesity is considered a significant risk factor as it prolongs surgical duration and affects prosthesis longevity. Rheumatoid arthritis patients have a higher infection risk due to immunosuppressive medication use, while diabetes increases susceptibility by promoting biofilm formation due to high glucose levels [7]. In England, data from the National Surveillance Program for Surgical Site Infections (SSI) show that among 72,000 patients undergoing hip and knee replacement surgeries in 2010/11, 1,221 infections were recorded, with 85% occurring within the first 30 days, and an average infection onset time of 14 days [2]. Of these infections, 42% were superficial, 43% were deep incisional, and 15% involved organs or spaces, with superficial infections limited to the initial postoperative period. In contrast, long-term follow-up data from the U.S. indicate that nearly one-fourth of infections occur between two- and ten-years post-surgery, highlighting an ongoing risk beyond the first year [7].
Between 2010 and 2011, 1,221 infections were recorded among 72,000 patients undergoing hip and knee replacement procedures. According to hospital monitoring, readmissions, and post-discharge follow-ups, most infections (85%) occurred within the first 30 days, with an average infection onset of 14 days [4]. Only a portion of post-surgical infections are identified through microbiological sampling, leading to the identification of a specific pathogen. Including non-laboratory-confirmed infections is crucial for providing a comprehensive and comparable measure of incidence, especially given potential variations in sampling practices across hospitals. Understanding pathogen distribution is fundamental for guiding local and national prevention strategies, including selecting appropriate prophylactic antibiotics [4].
Studies analyzing causative organisms indicate that Staphylococcus aureus is the most common pathogen in SSIs among patients undergoing hip and knee arthroplasties. National surveillance data from England in 2010/11 revealed that 44% of microbiologically confirmed SSIs within a year after surgery were attributed to S. aureus, with 20% of cases being methicillin resistant. Coagulase-negative staphylococci were also significant, accounting for 31% of infections, while Enterococcus species caused 12%. The remaining infections were caused by Escherichia coli, Enterobacter spp., Pseudomonas spp., and streptococci (7% each), with 28% of cases being polymicrobial [4].
Monitoring changes in SSI etiology has demonstrated the impact of methicillin-resistant S. aureus (MRSA) screening and decolonization policies introduced in England, initially targeting high-risk groups in 2006 and later expanding to all patients in 2009. Before 2006, between 25% and 30% of hip/knee SSI cases were caused by MRSA; by 2010/11, this proportion had decreased to 8%. These pre-admission screening policies, alongside other interventions, likely contributed to a significant reduction in invasive MRSA infection rates in English hospitals [4]. The primary causes of post-arthroplasty SSIs (periprosthetic joint infections, PJI) are microbial adhesion and biofilm formation, responsible for 60% of hospital-acquired infections. Biofilm-related infections can lead to tissue destruction, systemic pathogen transmission, severe disease, and even death. Bacterial adhesion, a critical factor in implant-associated infections, is influenced by bacterial hydrophobicity and charge, implant surface characteristics, environmental conditions, blood tissue responses, and specific adhesion molecules. A biofilm is an organized microbial colony adhering to surfaces through a polymeric matrix composed of polysaccharides, proteins, and DNA. The biofilm formation process involves several stages: initial cell attachment, adhesion, matrix development, biofilm maturation, and dispersion, which allows new biofilms to form in other areas [4].
Figure 1.
Epidemiological aspects of prosthetic joint infections.
3. Current Landscape of Orthopedic Implants
Over the past decades, orthopedic implants have undergone significant evolution, driven by remarkable advances in software, biomaterials, innovative surface treatment technologies, and increasingly sophisticated manufacturing techniques. The selection of materials for these implants is crucial, as it requires careful consideration of various mechanical and biological properties, friction, and wear. These factors are essential not only for ensuring biocompatibility but also for the long-term durability of the implants, guaranteeing that they can perform effectively and safely throughout their expected service life [11].
Materials commonly used in the fabrication of orthopedic implants encompass a wide range of options. Notably, stainless steel alloys (ASI316L) are recognized for their durability and corrosion resistance; chromium-cobalt-molybdenum (CCM) alloys provide excellent wear resistance; and titanium alloys (Ti6Al4V) are prized for their lightweight nature and biocompatibility. In addition to these metallic alloys, other materials such as ceramics—valued for their high compressive strength and chemical inertness—polyethylene, known for its low-friction properties in joint applications, and polymethylmethacrylate (PMMA) bone cement, widely used for prosthetic fixation due to its gap-filling capability and rapid polymerization, are frequently employed. Each material presents its own set of advantages and disadvantages that must be carefully considered, including factors such as mechanical strength (critical for withstanding bodily loads), chemical stability (which determines durability in the biological environment), and potential toxicity, a key concern for avoiding adverse reactions in surrounding tissues [12].
The surfaces of medical devices play a decisive role in the host’s biological response and in implant performance. These surfaces are reactive and continuously seek to minimize their reactivity through ongoing processes of adsorption, restructuring, and chemical reactions that constantly modify their properties. Such dynamic changes directly influence the interaction between the implant and the surrounding tissues, potentially affecting both bone integration and the risk of infection [12].
Currently, various modifications are being applied to the surfaces of orthopedic devices with the aim of promoting favorable responses to both acute and chronic infections in host tissue, reducing local inflammation at the implant site, enhancing implant integration with bone tissue, and lowering the risk of infection [13]. Emerging technologies, such as 3D printing and nanotechnology, are being explored for the development of personalized implants and for improving osseointegration [11]. Alongside these innovations, the use of synthetic bone substitutes has gained increasing popularity. These substitutes offer several advantages: they can be produced in unlimited quantities, molded to fit bone defects precisely, and, thanks to advances in materials engineering, are now available in forms that mimic the mechanical and biological properties of natural bone. These substitutes feature porous structures, biocompatibility, bio absorbability, and promote both osteoconduction and osseointegration [14,15].
4. CAD Technology
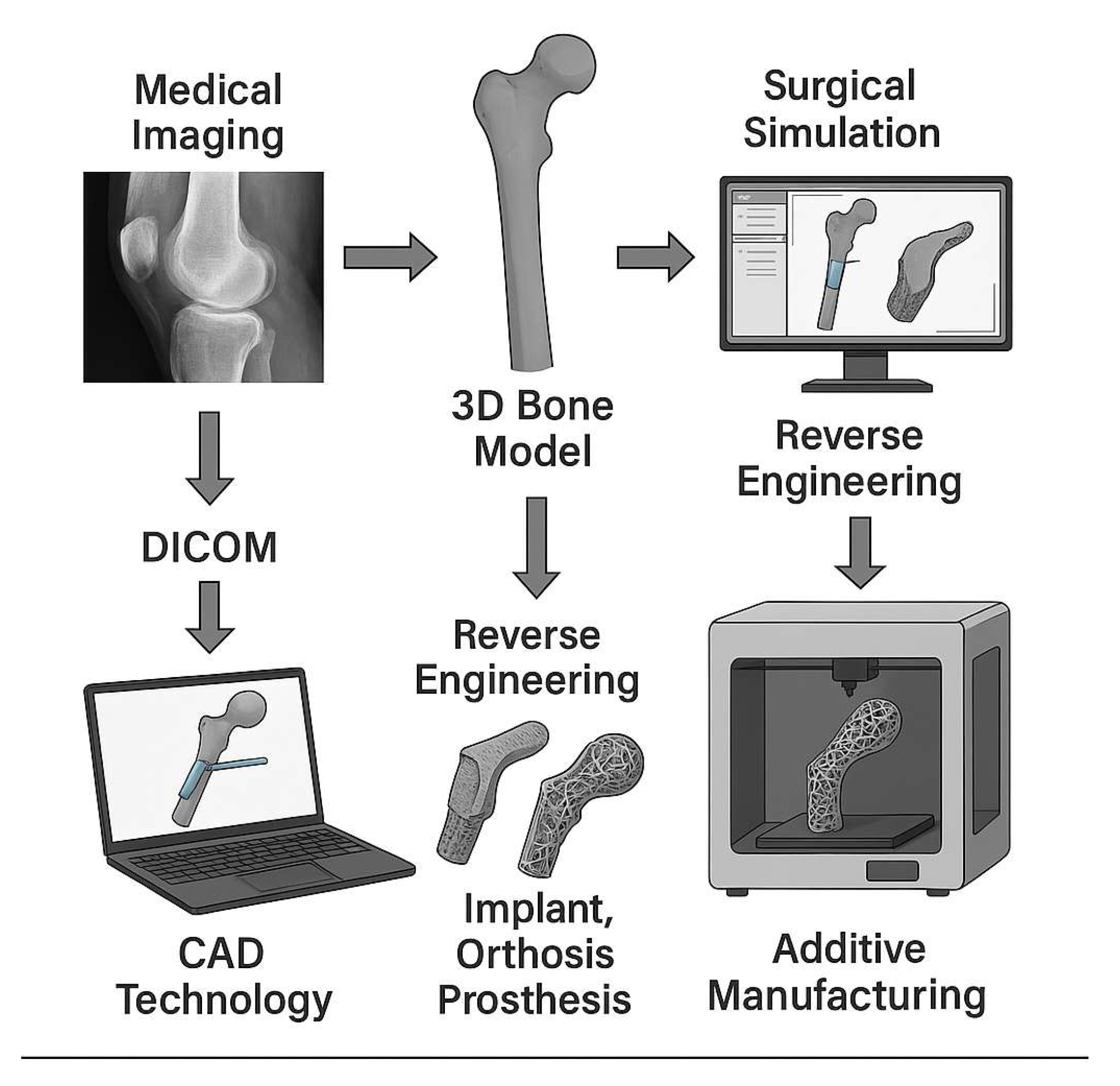
The use of medical imaging in the additive manufacturing (AM) process applied to medicine is directed toward teaching, planning, training, surgical simulation, and the development and manufacturing of instruments and implants. By employing DICOM (Digital Imaging and Communications in Medicine) image exams—such as computed tomography (CT)—it is possible to reproduce the three-dimensional bone structure. Once the 3D bone model is created, surgical simulations can be carried out in a CAD (Computer-Aided Design) environment, accurately modeling instruments and bone implants to adapt to both the surface and interior of bones. This technology enables the development of implant, orthosis, and prosthesis designs with mechanical and topological optimization of prototypes, while reducing the overall time and resources expended in the process.
In the development of orthopedic implants, a particularly useful tool is reverse engineering. This industrial process is employed to improve an object by studying its geometry inside and out, as well as its structure, operation, and characteristics. From this initial examination, a “clone” of the original object is produced to study and enhance it. In medicine, this approach is used to reproduce implants, prostheses, and orthoses with improved adaptation to anatomical details. By integrating reverse engineering with novel medical imaging acquisition technologies, new 3D printing methods, and advanced CAD software, it becomes possible to plan treatments for bone defects that will be reconstructed in the geometric modeling of prostheses and implants [16,17].
5. The Use of Additive Manufacturing for 3D Printing in Medicine
Additive manufacturing (AM) for 3D printing is a technology that enables the creation of three-dimensional objects from a digital model. This manufacturing process does not require molds for production; instead, objects are fabricated layer by layer, reducing material waste and minimizing environmental impact. According to the literature, this process can save up to 70% of raw materials and reduce production time by up to 30%. Compared to traditional subtractive manufacturing, AM offers a faster and more cost-effective method for producing complex shapes. Additionally, it allows for high levels of customization and facilitates on-demand production of replacement parts and custom components, reducing the need for large inventory stocks [18]. This technology has found applications in a wide range of industries, including medicine, architecture, automotive, aerospace, and more. In medicine, for example, 3D printing is used to create personalized prostheses, medical implants, and anatomical models for surgical planning [19].
According to Mendonça (2022), AM technology has been employed to enhance and develop new materials and designs for orthopedic implants, with a growing role in the manufacturing process [20]. Tilton, Lewis, and Manogharan (2018) suggest that AM is a prime candidate to become the next generation of orthopedic implant design and manufacturing [21]. These authors highlight that compared to traditional manufacturing methods, AM provides unique advantages in economically producing small-volume batches of highly complex products. Since AM does not require tool-dependent designs and materials (e.g., jigs and instruments), it enables the production of customized implants with various specifications, making non-conventional implants more economically viable as production scales up. Furthermore, the design freedom offered by AM allows for the easy integration of porous structures, which promote bone growth and biological fixation of implants [22].
6. Thermoplastics Used in the Healthcare Industry
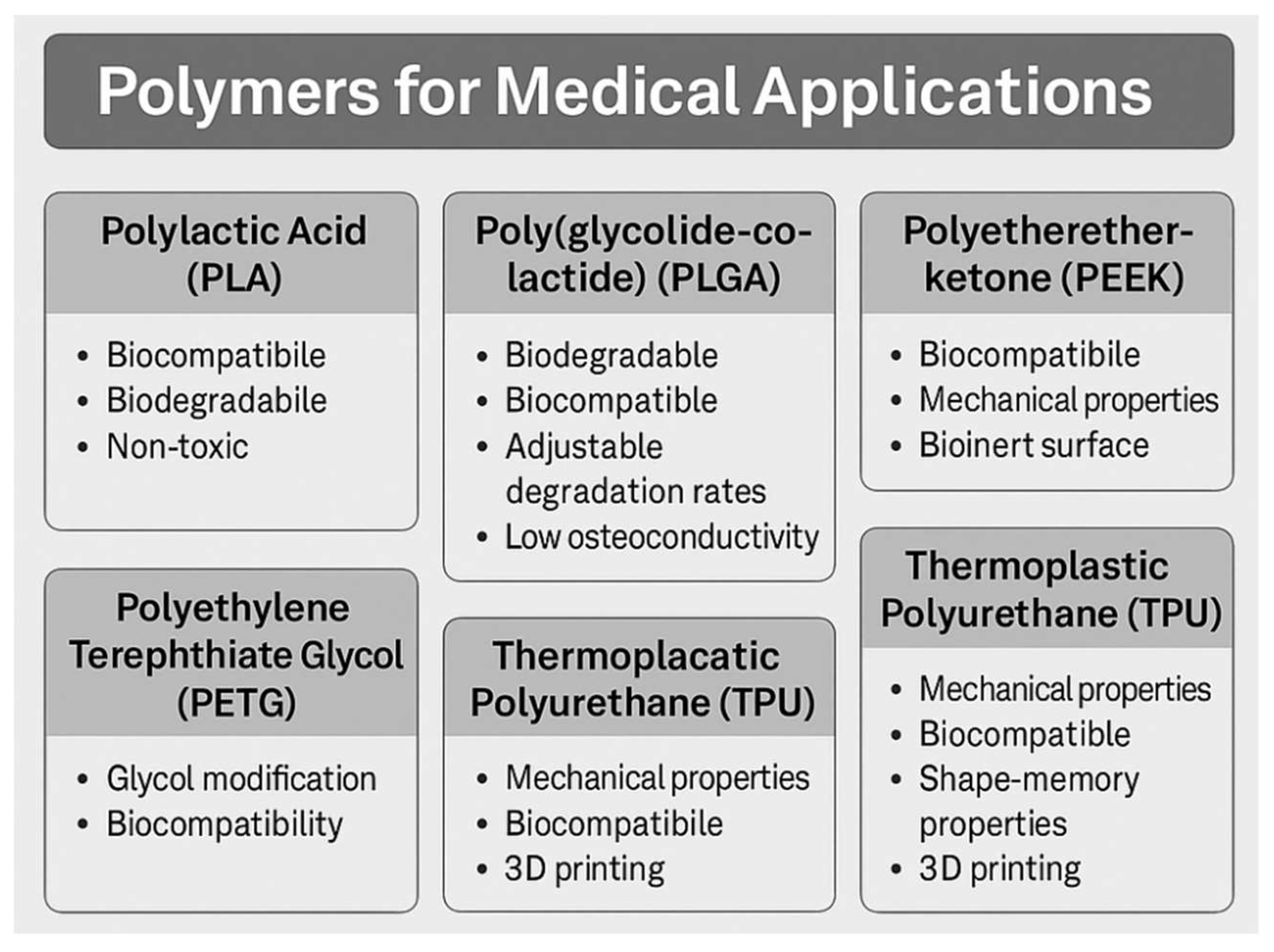
Polylactic acid (PLA) is widely used due to its biocompatibility, allowing for safe contact with living tissues without causing adverse reactions. Its biodegradability is environmentally beneficial, as it decomposes naturally, reducing environmental impact. The mechanical properties of PLA provide strength and durability, making it suitable for various applications, from temporary sutures to permanent orthopedic implants. Additionally, PLA is non-toxic, even in its degraded form, ensuring safety in long-term biomedical applications [23].
Among biodegradable polymers, poly(L-lactic acid) (PLLA) is highly valued for fracture fixation, tissue repair, and tissue engineering due to its high mechanical strength. However, its degradation byproducts create an acidic environment that may lead to inflammatory responses. Moreover, its limited bioactivity often requires the addition of bioactive ceramics, which restricts its clinical applications [24].
Poly(glycolide-co-lactide) (PLGA) is widely employed in orthopedic implants due to its biodegradable and biocompatible properties. This copolymer consists of polylactic acid (PLA) and polyglycolic acid (PGA), with adjustable ratios that allow for control over degradation rates. This characteristic makes PLGA highly versatile for various medical applications. However, despite its biocompatibility, the clinical use of pure PLGA in bone regeneration is limited due to its low osteoconductivity and insufficient mechanical properties for load-bearing applications [25].
PETG is obtained through glycol modification, which reduces the crystallinity of polyethylene terephthalate (PET) while preserving its biological properties. Although PET exhibits good mechanical properties and biocompatibility, its high crystallinity limits its printability. The modification to PETG results in a material with great potential for human tissue engineering applications [26].
Developed in the 1980s, polyetheretherketone (PEEK) gained prominence as a thermoplastic polymer, particularly in orthopedic and trauma applications since the 1990s. PEEK is highly biocompatible and exhibits favorable mechanical properties. However, its inert surface may facilitate bacterial colonization and biofilm formation. It is widely used in bone implants due to its mechanical properties, including an elastic modulus like human bone, biocompatibility, and chemical stability. However, its bioinertness limits its clinical applications, as it does not effectively promote osseointegration [27,28].
Thermoplastic polyurethane (TPU) has multiple applications in orthopedic implants due to its mechanical properties and biocompatibility. TPU is used in biomedical materials designed for low-temperature applications due to its shape-memory properties. Research indicates that TPU with appropriately rigid segments can be molded at low temperatures (36-46°C), enabling the production of customized orthotic devices, such as wrist braces, without causing cytotoxicity. TPU also plays a crucial role in 3D printing for biomedical applications, allowing for the creation of implants with complex geometries and internal architectures that meet precise clinical requirements. TPU produced through 3D printing has demonstrated good cell viability and tissue integration, showing promise for the development of personalized medical implants [29,30].
Polycaprolactone (PCL) is an aliphatic polyester widely used in bone tissue engineering. In vivo studies with PCL scaffolds applied to critical calvarial defect treatment in rats have demonstrated that these scaffolds support new tissue formation. However, PCL has limited bioactivity, a slow degradation rate, and mechanical properties that are insufficient for load-bearing applications [26]. In the Table 1 and Table 2 we compare different filaments used in fused filament fabrication for 3d printing in medical devices.
Figure 2.
Thermoplastic used for prosthetic joint infections with potential use of additive manufacturing with antibiotics.
Figure 2.
Thermoplastic used for prosthetic joint infections with potential use of additive manufacturing with antibiotics.
7. Polymers and Antimicrobial Action in Medicine
The treatment of periprosthetic joint infections (PJI) depends on the onset time and severity of the infection. Early infections can be treated with debridement, antibiotics, and implant retention, while late-stage infections often require implant removal and a two-stage revision arthroplasty, involving complete prosthesis removal, debridement, and placement of a temporary antibiotic-impregnated spacer. After an appropriate course of intravenous and/or oral antibiotic therapy, the implantation of a new prosthesis is planned [31].
In PJI treatment, both mobile and static spacers can be used. The primary material currently utilized for spacers is polymethylmethacrylate (PMMA). Following the removal of infected components, PMMA is prepared intraoperatively with varying types and amounts of antibiotics [32].
Strategies for preventing and controlling implant-related infections include prophylactic antibiotic administration before surgery and the use of antibiotic-loaded PMMA bone cement. The most commonly used antibiotics in this context are gentamicin, rifampicin, vancomycin, and tobramycin. Additionally, biomaterial surface modifications using coatings such as photoactive materials, antibiotic-hydroxyapatite, nanostructured coatings, nanosilver, antiseptics, and antimicrobial-impregnated agents are also crucial approaches. Ensuring that these materials exhibit biocompatibility with the patient is essential [7].
Biocompatibility refers to the ability of biomaterials, whether synthetic or naturally derived, to interact with the human body without causing adverse reactions or harm. It is a crucial prerequisite for the successful use of biomaterials in medical applications. Since these materials are often intended for long-term implants or direct tissue contact, biocompatibility ensures immune system compatibility and promotes healing [33].
A promising alternative for use as an antibiotic carrier and as a spacer material in infected arthroplasties is polylactic acid (PLA). This biomaterial is gaining increasing attention in the clinical field due to its remarkable mechanobiological properties. PLA is widely employed in additive manufacturing (AM) due to its biodegradable and biocompatible nature. Derived from renewable resources such as corn starch and sugarcane, PLA represents a sustainable alternative for biomedical applications. Extensive studies have demonstrated its biocompatibility, highlighting the absence of cytotoxic effects, further reinforcing its potential for safe use in medical devices such as prostheses and implants [34].
The administration of antibiotics through an antibiotic-impregnated medical device is advantageous as it enables localized and effective drug delivery without causing tissue damage, ensuring controlled antibiotic release. This system is also effective against biofilm formation, as bacteria are unable to adhere to the modified surface [35]. The concept of antibiotic-releasing coatings aims to reduce bacterial adhesion and prevent biofilm formation on implants. In this approach, antimicrobial agents are combined with polymeric materials—either biodegradable or non-biodegradable—and applied to the implant surface using various methods such as impregnation or adsorption. The main advantage of this technology is the ability to modulate antibiotic release, controlling the rate and duration of drug delivery [35].
The incorporation of antimicrobial compounds into PLA for medical applications primarily aims to confer antibacterial properties to medical devices and biomaterials, thereby reducing the risk of device-associated infections. A common strategy involves modifying the PLA surface with antimicrobial compounds. A study demonstrated that quaternized poly(2-(dimethylamino)ethyl methacrylate) was used to create PLA surfaces with significant antibacterial activity against both Gram-negative and Gram-positive bacterial strains [36].
Polymeric coatings can be produced using various techniques, including dip coating, spin coating, spray coating, and solvent casting. Among these, dip coating is the most widely used method in both laboratories and industry due to its simplicity, low cost, reliability, and reproducibility. This technique allows researchers to efficiently adjust processing parameters. The thickness of the generated films can be controlled by adjusting immersion duration, withdrawal speed, and the rheological properties of the coating solution. A study demonstrated that vancomycin-impregnated PLLA coatings were capable of reducing bacterial populations by approximately 80–90% [35].
Another technique involves extruding thermoplastic filaments pre-mixed with the antibiotic or treatment compound. When the filament is processed in a 3D printer, the printed object is already impregnated with the active agent. PLA has relatively low crystallinity, which may hinder its processing; however, the insertion of branched structures in its chains can enhance crystallization and improve processing efficiency. A study evaluating the inclusion of additives in PLA modified with maleic anhydride (PLA-g-MA) and lysine (PLA-g-Lys) observed that this combination accelerated crystallization kinetics and improved 3D printability without compromising mechanical properties. The presence of these additives influenced crystal formation, altering the melting temperature and degree of crystallinity, with lysine exhibiting a more pronounced effect due to its branched structure. Additionally, the grafting process reduced molecular weight, increasing chain mobility and promoting crystallization [37]. A recent study applied an ionic silver coating onto PEEK using a hydroxyapatite film. The modified material exhibited strong bactericidal activity in preventing biofilm formation in both in vitro and in vivo models [28].
8. Application in Cranioplasty and Infection Prevent
In developing countries, factors such as a young population, inadequate public transportation systems, densely populated urban centers, and low educational levels contribute to a high incidence of orthopedic and polytrauma injuries, including traumatic brain injuries (TBI). In Brazil, for example, the incidence rate of TBI is estimated at 65.54 per 100,000 inhabitants [3], likely underestimated, considering that in the United States, this rate is 300 per 100,000 inhabitants [38].
In severe cases of TBI, often associated with hematomas and cerebral edema, many patients require a surgical procedure known as decompressive craniectomy, which involves the removal of a portion of the skull bone to normalize intracranial pressure. Elevated intracranial pressures, if untreated, can lead to brain death [24](. After the resolution of intracranial hypertension, bone reimplantation is necessary in a procedure called cranioplasty. When a synthetic implant is used, the cost of the material is extremely high, making its use infeasible in public healthcare systems such as the Brazilian Unified Health System (SUS). As a result, autologous bone reuse is often necessary, despite its higher risk of infection compared to synthetic materials [39]. A recent study have used PLA for cranioplasty impregnated with vancomycin, which is an important perspective to reduce surgical site infections [20]. Nowadays, PMMA is combined with vancomycin during the surgery, but this is not considered as additive manufacture.
Figure 3.
Concept of reverse engineering in prosthetic joint infections with potential use of additive manufacturing with antibiotics.
Figure 3.
Concept of reverse engineering in prosthetic joint infections with potential use of additive manufacturing with antibiotics.
9. Conclusion and Future Perspectives
The continuous advancements in biomaterials, additive manufacturing, and antimicrobial surface modifications offer a promising future for orthopedic and neurosurgical implants. The incorporation of 3D printing technology into the development of patient-specific implants allows for enhanced customization, improved biomechanical performance, and reduced surgical risks. Moreover, the ability to integrate antimicrobial agents directly into polymeric and metallic implant surfaces is expected to mitigate the risk of periprosthetic joint infections and surgical site infections, addressing a critical challenge in orthopedic surgery. However, further clinical trials are necessary to validate the long-term effectiveness and safety of these new technologies in real-world applications.
The use of biodegradable polymers, such as polylactic acid and polycaprolactone, represents an innovative approach in regenerative medicine, particularly in the development of bioresorbable implants. These materials offer an alternative to traditional metal implants by reducing long-term complications, such as stress shielding and implant-related infections. The combination of biodegradable scaffolds with bioactive agents, including antibiotics and growth factors, is a promising strategy for improving osseointegration and bone regeneration. Despite these advantages, challenges such as mechanical stability, controlled degradation rates, and long-term biocompatibility need to be addressed through further research and material optimization.
Looking ahead, the integration of nanotechnology, artificial intelligence, and machine learning into the design and manufacturing of orthopedic implants is expected to revolutionize personalized medicine. AI-driven computational modeling can enhance implant design by optimizing material properties and predicting biomechanical behavior. Additionally, smart implants equipped with biosensors may enable real-time monitoring of infection markers, mechanical loads, and healing progress, improving postoperative outcomes. Future research should focus on developing hybrid implant materials that combine the mechanical strength of metals with the bioactivity of polymers, ultimately advancing the field toward more efficient, cost-effective, and patient-specific solutions for orthopedic and neurosurgical applications.
Author Contributions
G.O., F.Z., L.D., P.S., writing—original draft preparation, J.S., C.M., G.L., M.L., F.T. writing—review and editing..
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are available under request.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest
Abbreviations
The following abbreviations are used in this manuscript:
| LOS | Length of stay |
| ICU | Intensive care unit |
References
- Ferreira, M.C.; Oliveira, J.C.P.; Zidan, F.F.; Franciozi, C.; Luzo, M.V.M.; Abdalla, R.J. Total knee and hip arthroplasty: the reality of assistance in Brazilian public health care. Rev Bras Ortop 2018, 53, 432–440. [Google Scholar] [CrossRef] [PubMed]
- Tande, A.J.; Patel, R. Prosthetic joint infection. Clin Microbiol Rev 2014, 27, 302–345. [Google Scholar] [CrossRef]
- Carteri, R.B.K.; Silva, R.A.D. Traumatic brain injury hospital incidence in Brazil: an analysis of the past 10 years. Rev Bras Ter Intensiva 2021, 33, 282–289. [Google Scholar] [CrossRef] [PubMed]
- Lamagni, T. Epidemiology and burden of prosthetic joint infections. J Antimicrob Chemother 2014, 69 Suppl 1, i5–10. [Google Scholar] [CrossRef]
- Tuon, F.F.; Cieslinski, J.; Ono, A.F.M.; Goto, F.L.; Machinski, J.M.; Mantovani, L.K.; Kosop, L.R.; Namba, M.S.; Rocha, J.L. Microbiological profile and susceptibility pattern of surgical site infections related to orthopaedic trauma. Int Orthop 2019, 43, 1309–1313. [Google Scholar] [CrossRef] [PubMed]
- Rollo, G.; Logroscino, G.; Stomeo, D.; Cioffi, R.; Calvisi, V.; Meccariello, L. Comparing the use of preformed vs hand-made antibiotic spacer cement in two stages revision of hip periprosthetic infection. J Clin Orthop Trauma 2020, 11, S772–S778. [Google Scholar] [CrossRef]
- Costa-Pinto, A.R.; Lemos, A.L.; Tavaria, F.K.; Pintado, M. Chitosan and Hydroxyapatite Based Biomaterials to Circumvent Periprosthetic Joint Infections. Materials (Basel) 2021, 14. [Google Scholar] [CrossRef]
- Shohat, N.; Goh, G.S.; Harrer, S.L.; Brown, S. Dilute Povidone-Iodine Irrigation Reduces the Rate of Periprosthetic Joint Infection Following Hip and Knee Arthroplasty: An Analysis of 31,331 Cases. J Arthroplasty 2022, 37, 226–231 e221. [Google Scholar] [CrossRef]
- Kaye, K.S.; Anderson, D.J.; Sloane, R.; Chen, L.F.; Choi, Y.; Link, K.; Sexton, D.J.; Schmader, K.E. The effect of surgical site infection on older operative patients. J Am Geriatr Soc 2009, 57, 46–54. [Google Scholar] [CrossRef]
- Porretto, M.; Parente, F.; Del Puente, F.; Parisini, A.; Tigano, S.; Nelli, M.; Mazzola, C.; Damiani, G.; Adriano, G.; Sartini, M.; et al. Surveillance of surgical site infections in orthopedic prosthetic surgery: a tool for identifying risk factors and improving clinical practice. J Prev Med Hyg 2024, 65, E273–E277. [Google Scholar] [CrossRef]
- Choi, S.R.; Kwon, J.W.; Suk, K.S.; Kim, H.S.; Moon, S.H.; Park, S.Y.; Lee, B.H. The Clinical Use of Osteobiologic and Metallic Biomaterials in Orthopedic Surgery: The Present and the Future. Materials (Basel) 2023, 16. [Google Scholar] [CrossRef]
- Szczesny, G.; Kopec, M.; Politis, D.J.; Kowalewski, Z.L.; Lazarski, A.; Szolc, T. A Review on Biomaterials for Orthopaedic Surgery and Traumatology: From Past to Present. Materials (Basel) 2022, 15. [Google Scholar] [CrossRef]
- Richards, R.G.; Moriarty, T.F.; Miclau, T.; McClellan, R.T.; Grainger, D.W. Advances in biomaterials and surface technologies. J Orthop Trauma 2012, 26, 703–707. [Google Scholar] [CrossRef] [PubMed]
- Kirkpatrick, J.S.; Cornell, C.N.; Hoang, B.H.; Hsu, W.; Watson, J.T.; Watters, W.C., 3rd; Turkelson, C.M.; Wies, J.L.; Anderson, S. Bone void fillers. J Am Acad Orthop Surg 2010, 18, 576–579. [Google Scholar] [CrossRef] [PubMed]
- Evaniew, N.; Tan, V.; Parasu, N.; Jurriaans, E.; Finlay, K.; Deheshi, B.; Ghert, M. Use of a calcium sulfate-calcium phosphate synthetic bone graft composite in the surgical management of primary bone tumors. Orthopedics 2013, 36, e216-222. [Google Scholar] [CrossRef] [PubMed]
- Marro, A.; Bandukwala, T.; Mak, W. Three-Dimensional Printing and Medical Imaging: A Review of the Methods and Applications. Curr Probl Diagn Radiol 2016, 45, 2–9. [Google Scholar] [CrossRef] [PubMed]
- van Eijnatten, M.; van Dijk, R.; Dobbe, J.; Streekstra, G.; Koivisto, J.; Wolff, J. CT image segmentation methods for bone used in medical additive manufacturing. Med Eng Phys 2018, 51, 6–16. [Google Scholar] [CrossRef] [PubMed]
- Banks, J. Adding value in additive manufacturing: researchers in the United Kingdom and Europe look to 3D printing for customization. IEEE Pulse 2013, 4, 22–26. [Google Scholar] [CrossRef]
- Serra, T.; Mateos-Timoneda, M.A.; Planell, J.A.; Navarro, M. 3D printed PLA-based scaffolds: a versatile tool in regenerative medicine. Organogenesis 2013, 9, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Mendonça, C.J.A.D., L. R.; Soni, J.F. ; Tuon, F.F. Antimicrobial Action of a Biodegradable Thermoplastic Impregnated with Vancomycin for Use in 3D Printing Technology. Brazilian Archives of Biology and Technology 2024, 67, 13. [Google Scholar] [CrossRef]
- Tilton, M.; Lewis, G.S.; Hast, M.W.; Fox, E.; Manogharan, G. Additively manufactured patient-specific prosthesis for tumor reconstruction: Design, process, and properties. PLoS One 2021, 16, e0253786. [Google Scholar] [CrossRef]
- Mendonca, C.J.A.; Guimaraes, R.; Pontim, C.E.; Gasoto, S.C.; Setti, J.A.P.; Soni, J.F.; Schneider, B., Jr. An Overview of 3D Anatomical Model Printing in Orthopedic Trauma Surgery. J Multidiscip Healthc 2023, 16, 875–887. [Google Scholar] [CrossRef] [PubMed]
- Alavi, M.S.; Memarpour, S.; Pazhohan-Nezhad, H.; Salimi Asl, A.; Moghbeli, M.; Shadmanfar, S.; Saburi, E. Applications of poly(lactic acid) in bone tissue engineering: A review article. Artif Organs 2023, 47, 1423–1430. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M.; Kang, I.G.; Cheon, G.H.; Jang, T.S.; Kim, H.E.; Jung, H.D.; Kang, M.H. Enhanced Bioactivity of Micropatterned Hydroxyapatite Embedded Poly(L-lactic) Acid for a Load-Bearing Implant. Polymers (Basel) 2020, 12. [Google Scholar] [CrossRef]
- Gentile, P.; Chiono, V.; Carmagnola, I.; Hatton, P.V. An overview of poly(lactic-co-glycolic) acid (PLGA)-based biomaterials for bone tissue engineering. Int J Mol Sci 2014, 15, 3640–3659. [Google Scholar] [CrossRef] [PubMed]
- Hassan, M.H.; Omar, A.M.; Daskalakis, E.; Hou, Y.; Huang, B.; Strashnov, I.; Grieve, B.D.; Bartolo, P. The Potential of Polyethylene Terephthalate Glycol as Biomaterial for Bone Tissue Engineering. Polymers (Basel) 2020, 12. [Google Scholar] [CrossRef]
- Pu, F.; Yu, Y.; Zhang, Z.; Wu, W.; Shao, Z.; Li, C.; Feng, J.; Xue, L.; Chen, F. Research and Application of Medical Polyetheretherketone as Bone Repair Material. Macromol Biosci 2023, 23, e2300032. [Google Scholar] [CrossRef]
- Ishihama, H.; Ishii, K.; Nagai, S.; Kakinuma, H.; Sasaki, A.; Yoshioka, K.; Kuramoto, T.; Shiono, Y.; Funao, H.; Isogai, N.; et al. An antibacterial coated polymer prevents biofilm formation and implant-associated infection. Sci Rep 2021, 11, 3602. [Google Scholar] [CrossRef] [PubMed]
- Griffin, M.; Castro, N.; Bas, O.; Saifzadeh, S.; Butler, P.; Hutmacher, D.W. The Current Versatility of Polyurethane Three-Dimensional Printing for Biomedical Applications. Tissue Eng Part B Rev 2020, 26, 272–283. [Google Scholar] [CrossRef] [PubMed]
- Meng, Q.; Hu, J.; Zhu, Y. Properties of shape memory polyurethane used as a low-temperature thermoplastic biomedical orthotic material: influence of hard segment content. J Biomater Sci Polym Ed 2008, 19, 1437–1454. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.K.; Yoo, J.H.; Oh, H.C.; Ha, J.W.; Park, S.H. The Incidence Rate, Microbiological Etiology, and Results of Treatments of Prosthetic Joint Infection following Total Knee Arthroplasty. J Clin Med 2023, 12. [Google Scholar] [CrossRef]
- Lachiewicz, P.F.; Wellman, S.S.; Peterson, J.R. Antibiotic Cement Spacers for Infected Total Knee Arthroplasties. J Am Acad Orthop Surg 2020, 28, 180–188. [Google Scholar] [CrossRef]
- Winkler, T.; Sass, F.A.; Duda, G.N.; Schmidt-Bleek, K. A review of biomaterials in bone defect healing, remaining shortcomings and future opportunities for bone tissue engineering: The unsolved challenge. Bone Joint Res 2018, 7, 232–243. [Google Scholar] [CrossRef] [PubMed]
- Kowalczyk, P.; Wojasinski, M.; Jaroszewicz, J.; Kopec, K.; Ciach, T. Controlled formation of highly porous polylactic acid-calcium phosphate granules with defined structure. Biomater Adv 2023, 144, 213195. [Google Scholar] [CrossRef]
- Thamvasupong, P.; Viravaidya-Pasuwat, K. Controlled Release Mechanism of Vancomycin from Double-Layer Poly-L-Lactic Acid-Coated Implants for Prevention of Bacterial Infection. Polymers (Basel) 2022, 14. [Google Scholar] [CrossRef]
- El Habnouni, S.; Lavigne, J.P.; Darcos, V.; Porsio, B.; Garric, X.; Coudane, J.; Nottelet, B. Toward potent antibiofilm degradable medical devices: a generic method for the antibacterial surface modification of polylactide. Acta Biomater 2013, 9, 7709–7718. [Google Scholar] [CrossRef] [PubMed]
- Dorm, B.C.; Bastos, A.C.; Nossa, T.S.; Neto, B.D.; Iemma, M.R.C.; Carvalho, A.J.F.; Trovatti, E. Lysine grafted poly(lactic acid): An intrinsically antimicrobial polymer. Int J Biol Macromol 2024, 273, 133181. [Google Scholar] [CrossRef]
- Thurman, D.J.; Alverson, C.; Dunn, K.A.; Guerrero, J.; Sniezek, J.E. Traumatic brain injury in the United States: A public health perspective. J Head Trauma Rehabil 1999, 14, 602–615. [Google Scholar] [CrossRef] [PubMed]
- Capitelli-McMahon, H.; Kahlar, N.; Rahman, S. Titanium Versus Autologous Bone-Based Cranioplasty: A Systematic Review and Meta-Analysis. Cureus 2023, 15, e39516. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



