
Submitted:
29 April 2025
Posted:
30 April 2025
You are already at the latest version
Abstract
The COVID-19 pandemic and recent viral outbreaks have underscored the urgent need for diagnostics that combine accuracy with widespread accessibility. While laboratory-based methods remain essential, point-of-care (POC) solutions are critical for quick, decentralized testing. Significant advancements in viral biosensors, from innovative technologies to enhancements of existing platforms, demonstrate the growing potential of new sensing technologies for clinical applications. However, a gap remains between academic proof-of-concept studies and viable, clinically deployable diagnostic tools. This review examines how recent advancements in sensing methodologies, including innovative analyte detection, simplified assay administration, and enhanced performance in complex media such as serum, collectively address barriers to adoption, including cost, usability, and scalability. We also explore broader trends, such as open-source hardware, modular assay design, and standardized reporting practices, that collectively work to reduce barriers to clinical implementation. By analyzing these converging innovations, we emphasize how interdisciplinary progress is transforming the landscape of viral diagnostics, bringing the field closer to practical, equitable, and scalable solutions for real-world settings through novel biosensing advancements.
Keywords:
Viral Diagnostics
; Point-of-care
; Biosensors
Introduction
In recent years, viral diagnostic technologies have evolved significantly, rapidly improving to meet the demand for quick, accurate, and accessible testing capabilities. Given the emergence of large-scale viral infections such as avian influenza (H5N1), Ebola, and the Zika virus, the need for advancements in diagnostic technologies remains pressing. These crises have underscored the critical necessity for diagnostic tools to deliver timely results, especially in the early stages of infection. The ongoing COVID-19 pandemic, caused by SARS-CoV-2, illustrates the severe consequences of failing to control localized endemic events before the pathogen spreads through global markets and travel systems. Widespread infections like COVID-19 also highlight the demand for effective diagnostics to extend beyond the laboratory, with population-level testing pushing diagnostics toward at-home and point-of-care (POC) settings. The pandemic has also seen development efforts expand focus in this area, with enhancements in sensitivity and accuracy balanced with cost reduction, miniaturization, scalability for mass production, and simplified sampling and data processing. These advancements address the challenges posed by emerging and ongoing infectious diseases, aiming to democratize access to diagnostics, both in their administration and in interpreting their results.
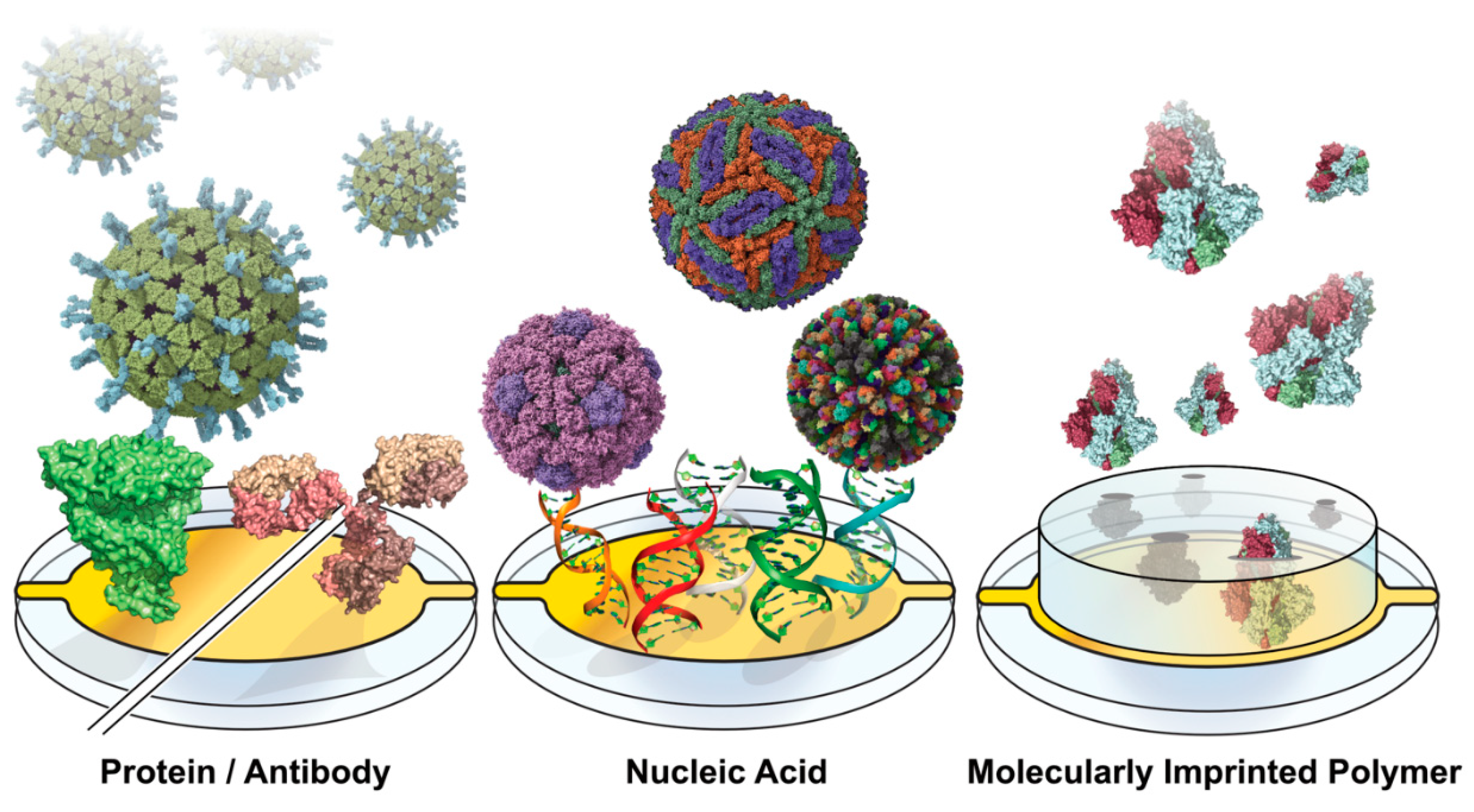
At its core, a biosensor typically includes a biorecognition element designed to capture diagnostic targets selectively. These targets include nucleic acids, viral proteins, antibodies, and entire virions. The capture elements for these biomarkers can take various forms, such as antibodies (both whole and functional fragments), proteins, or nucleic acids like DNA, RNA, or aptamers. Accompanying the biorecognition element is a form of signal transduction that translates the capture of the biomarker into a measurable readout. Optical signaling methods rely on changes in light properties, including refractive index, fluorescence, color changes, absorbance, or light interference [1]. Electrochemical signal transduction can appear in several forms, including amperometric readouts that measure current, potentiometric readouts of voltage, and changes in impedance [2]. Biosensors can also integrate mechanical signal transduction, exemplified by quartz crystal microbalance (QCM) and microcantilever sensors [3,4].
Furthermore, signal transduction may involve thermal or magnetic methods. Signal amplification techniques often lower detection limits and enhance the readout of weak signals. Nanomaterials such as colloidal gold, quantum dots, and graphene nanotubes can be combined with biorecognition elements to improve the quality and strength of faint signals. While some diagnostics, like lateral flow assays (LFAs), provide a simple binary readout that users can interpret directly, other diagnostic methods require post-processing to convert the signal into a comprehensible output. Various post-processing methods are employed, from software interfaces and smartphone apps that interpret results to more complex machine learning (ML) models designed to handle increasingly intricate datasets. Moreover, viral diagnostics often utilize microfluidic sample delivery systems, which assist users by reducing sample volumes, directing the specimen to the sensing region, and minimizing the risk of human error associated with manual sample processing.
Multiple approaches to viral diagnostics can be taken, depending on the nature of the viral recognition target. The detection of viral genomes has become particularly ubiquitous due to the COVID-19 pandemic, and methods such as real-time reverse transcription polymerase chain reaction (RT-PCR), next-generation sequencing (NGS), and reverse-transcription loop-mediated isothermal amplification (RT-LAMP) have all undergone significant development in recent years. While RT-PCR serves as the gold standard for viral detection due to its rapid time-to-result, high specificity, and low copy number requirements, it requires specialized instrumentation, trained personnel, and the production and storage of reagents such as polymerases and primers. RT-LAMP does improve accessibility by eliminating the need for a thermal cycler, but it has also seen limited adoption in the clinic [5]. Other diagnostic methods target viral proteins or antibodies raised against them rather than genomic information. Methods like ELISA are the standard for protein-based diagnostics, but they also suffer from limitations in personnel, sample handling, and costly reagents like antibodies. At the same time, demonstrably effective point-of-care implementation is not ideal. Lateral flow assays and CRPSIR-based diagnostics offer greater accessibility by requiring minimal instrumentation, often providing simple, binary colorimetric readouts that can be interpreted by physicians and patients alike without requiring a fundamental understanding of their underlying mechanisms.
Across the scientific community, there is no shortage of promising publications effectively demonstrating advancements in viral detection from the standpoint of instrumentation and methodology. However, seeing such technologies finalized into a feasible, cost-effective clinical product is far less common. Factors like the need to control local outbreaks, expand accessibility to disenfranchised communities, and conduct population-scale testing mean diagnostics must expand beyond central laboratories, regardless of how technically effective lab-oriented methods may be. In addition to logistical constraints like manufacturing costs and scalability, an underlying cause is prioritization dominating the research world. Given the cyclical nature of research funding, shifting to novel assay developments rather than focusing on maturing previously demonstrated technology is far more viable intellectually and financially. Until this approach shifts, this cycle of seeking new research areas rather than continuing to hone existing methodologies for clinical adoption will likely continue.
These diagnostic products are also frequently neglected because contagious diseases prevalent in low-income countries do not yield substantial economic returns for biotech companies—this lack of profitability results in insufficient investment in their development. One potential solution to this issue is establishing partnerships between academic institutions, industry, regulatory agencies, and government. In this model, the most promising diagnostic products developed in academic laboratories would receive targeted financial incentives from the government and be manufactured by the industrial partners with approval from the regulators. This collaboration could significantly advance the development of vital diagnostic products for infectious diseases.
We must recognize the urgent need for solutions to infectious diseases. Access to effective diagnostics and treatments is crucial for the health and well-being of millions. By prioritizing this partnership, we can drive meaningful progress and tackle the critical health challenges that underserved populations face. In today's interconnected world, no geographical barrier can prevent infectious diseases from crossing borders. The rapid globalization of trade and travel has facilitated the movement of people and goods around the globe, increasing the likelihood of pathogens being transmitted from one location to another. In this environment, outbreaks can escalate quickly, as seen in the case of diseases like COVID-19, which spread swiftly from one country to another. This highlights the vulnerabilities of public health systems worldwide.
Figure 1.
Capture Motif-Functionalized Biosensor Surfaces. Sensing surfaces are functionalized across the various viral diagnostic approaches with motifs for capturing proteins and whole virions. Capture moieties can range from proteins and antibodies to nucleic acids, aptamers, and molecularly imprinted polymers.
Figure 1.
Capture Motif-Functionalized Biosensor Surfaces. Sensing surfaces are functionalized across the various viral diagnostic approaches with motifs for capturing proteins and whole virions. Capture moieties can range from proteins and antibodies to nucleic acids, aptamers, and molecularly imprinted polymers.
The World Health Organization (WHO) broadly characterizes ideal POC diagnostics through real-time connectivity, ease of specimen collection, affordability, sensitivity, specificity, user-friendliness, rapidness, and robustness [6]. In this review, we discuss a variety of advancements in viral diagnostics, which aim to make improvements within these criteria. While many of the advancements discussed have not yet been implemented in POC settings, they demonstrate the ever-moving push to bridge the gap between POC accessibility and laboratory diagnostic technology. Further, we discuss production processes that improve the feasibility of pushing state-of-the-art diagnostics into POC settings by lowering costs, enabling local component manufacturing, and simplifying diagnostic administration and reporting with pre-functionalized sensors and out-of-the-box software tools.
Optical Methods
Surface Plasmon Resonance
Surface Plasmon Resonance (SPR) is a label-free optical technique that utilizes photon-electron interactions with plasmonic materials. The method operates through the phenomenon of light under ideal matching conditions, undergoing total internal reflection at the interface of a thin metal film and a dielectric. Tracking the angle of light at which the total internal reflection occurs enables real-time analysis of binding events since changes in the refractive index will shift the angle of incidence [7]. SPR biosensing is commonplace in pharmaceutical research due to its ability to study binding affinities between biomolecules. It is well-suited for screening drugs at on and off-rates and affinities. Still, it can also detect the presence of antibodies and viral antigens. The absence of labels means that the interactions being studied are closer to their native interactive states, and the method is exceptionally sensitive [8]. The technique is not without flaws, however. Typical commercial instrumentation is often expensive, and costs per run are high due to plasmonic metals (like gold and silver) in chip production. Still, instruments frequently costing hundreds of thousands of dollars cannot be feasibly implemented in clinics. Further, while SPR is straightforward to train, it requires additional considerations of buffer preparation and system design to minimize bulk refractive index shifts and non-specific surface binding [9], which makes adoption in clinics difficult. Further, multiplexed sensing is limited by the number of fluidic channels.
Viral SPR biosensing is by no means a novel technique, however. For instance, Riedel et al. demonstrated an SPR biosensor for detecting the Epstein-Barr virus in patient sera in 2014 [10]. Similarly, Florschütz et al. used surface-immobilized nucleotides to capture the barley stripe mosaic virus RNA (BSMV), in 2013 [11]. More recently, Yano et al. demonstrated a SARS-CoV-2 SPR biosensor, which detected the nucleocapsid, claiming a LOD as low as 85 fM, in which surface-immobilized anti-nucleocapsid antibodies were used for capture. In contrast, secondary antibody-conjugated AuNPs were used for amplification [12]. Surface-immobilized aptamers have also been used for viral detection, with sensors for the HIV-1 Tat protein [13] and the SARS CoV-2 N-protein in complex media [14], which have been shown using commercial instrumentation.
While these studies demonstrate the method’s ability to detect viral analytes, recent work has aimed to push SPR closer to clinical relevance. Recently, a portable SPR system has been demonstrated for analyzing nasopharyngeal COVID-19 tests, using covalently linked, RBD-binding nanobodies to the chip surface. The studies utilized an SPR spectrometer [15], which is a fraction of the size of other commercial SPR instruments, and machine learning was incorporated to help identify positive signal shifts. In another SARS-CoV-2 assay, a four-channel SPR chip was immobilized with the spike protein and the human ACE2 receptor to detect antibodies and viral particles in serum samples [16].
The size reduction of SPR instruments is gradually progressing, with instruments from the likes of OpenSPR [17], NanoSPR [18], and Plasmetrix [19] demonstrating how SPR instruments can easily find a place in a clinic. In addition to their physical footprint, sensor surface advancements have also been made to improve the clinical adoptability of SPR. Wallace et al. showed the development of disposable, multiplexed plasmonic chip surfaces with multiple discrete sensing regions that could detect SARS-CoV-2, Norovirus, and Zika [20]. The pre-functionalized surface allowed them to be produced and shipped to clinics, ready to use out of the box, which compounds with the size improvements of recent instrumentation. While this system was centered around hyperspectral polarimetry, the plasmonic nature of the chip design means it could be implemented in SPR systems, and more importantly, pre-functionalized surfaces reduce the complexity of running assays in a clinic. While SPR systems are already sufficiently sensitive to detect viral biomarkers in patient samples, there is still work regarding miniaturization, adaptable chip surfaces, and multiplexed sensing methodologies to push them closer to clinical adoption. There is an unavoidable cost regarding sensor chips, but reusable surfaces and multiplexed sensing can help get more diagnoses per chip investment.
Biolayer Interferometry
Biolayer interferometry is gaining traction as another versatile tool for detecting viral infections. BLI systems characterize binding interactions through a recognition ligand coupled to a sensor tip. Interactions with analytes in solution occur at the tip, creating a thin layer that causes interference in light passing through the length of the sensor [21]. Light bouncing off a ligand-binding and a stationary reference surface causes an interference pattern, which induces a measurable wavelength shift. Since the wavelength shift is proportional to the thickness of the layer, active measurement enables real-time binding analysis [22], which can elucidate kinetic parameters. Measuring biomolecular interactions of analytes directly in solution and minimizing sample workup procedures can make it well suited for point-of-care applications. Like SPR, biolayer interferometry carries the benefits of sensitive, real-time, and label-free biosensing. Still, careful surface design and considerations like non-specific binding and surface regeneration are required. BLI avoids the time-consuming steps of washing and visualization necessary for ELISA diagnostics, making it more consistent in the hands of clinicians. BLI has been used to develop viral inhibitors, such as therapeutic antibody epitope mapping [23] and characterizing inhibitors for viral infections [24,25]. Still, its applicability extends into diagnostics as well. In addition to simplified sensor preparation, BLI’s applicability in the clinic can be further bolstered with more robust capture probes on the sensor surface. Poolsup et al. demonstrated a BLI aptasensor to detect SARS-CoV-2 anti-nucleocapsid antibodies in human saliva [26]. By using aptamers rather than protein-based capture ligands, the sensor can be made far more robust, which is especially conducive for sensors that will be mass-manufactured and distributed to clinics [27].
Numerous studies have utilized BLI to characterize virus-ligand interactions, and several have tried to democratize novel viral diagnostics for clinical use. For instance, Dzimianski et al. demonstrated a single-use BLI assay for detecting antibodies against the SARS-CoV-2 spike protein while achieving isotype detection [28]. By producing sensors pre-functionalized with capture ligands, their approach demonstrates how simplification can reduce costs and quicken the time-to-result for BLI diagnostics. Additionally, this assay was used on a BLI instrument compatible with 96-well plates, offering markedly greater throughput.
Further, single-particle interferometric resonance imaging sensors (IRIS) utilize sensor chips arrayed with viral capture probes to count and size viral particles by capturing transmitted light from an LED imaging system [29]. This approach has proven versatile in viral detection, with studies utilizing SP-IRIS to detect VSV [30], H1N1 [31], and filamentous ebolaviruses [29]. In terms of accessibility, this method simplifies the diagnostic process by eliminating purification steps and reducing sample volumes. Recent improvements in this methodology have further improved its operational simplicity by utilizing multi-wavelength sensing, eliminating the need to capture and process Z-stacked images [32]. Minimizing the need for trained personnel, this instrument could outcompete ELISA methods in detecting the monkeypox virus (MPXV) in 20 minutes. Still fitting on a benchtop, the improvements in simplicity and time-to-result make this instrument well-suited for clinical use.
The recent developments in BLI have shown how well-fitting this method can be for clinical viral diagnostic applications. The continued iterative improvements in BLI sensing show how the development of novel diagnostic technologies does not end at demonstrating their efficacy but rather how continued refinement helps push proof-of-concept techniques into practical implementation in the clinic. While the quirks of novel biosensors can be worked around more easily in academic labs, where personnel are highly specialized and intimately involved in the development process, honing the technology for simplified use opens the door for untrained personnel to make use of the technology in the field.
Colorimetric & Fluorescent Sensors
Colorimetric sensors represent a class of highly accessible diagnostic tools already commonly used in clinical viral diagnostics. Unlike methods such as PCR, which relies on complex instrumentation and specialized training, colorimetric sensors translate the presence of viral biomarkers, such as antibodies, proteins, or nucleic acids, into visible color changes. This readout mechanism pairs target-specific capture motifs like antibodies or oligonucleotides with chemical or nanomaterial-based signal amplifiers, such as gold nanoparticle aggregation or enzymatic chromogenic reactions. The resulting signals are detectable by the naked eye or with basic spectrophotometric devices. They represent a rapid, affordable, simple-to-administer testing strategy that retains strong accuracy. These tests are relatively simple and conducive to widespread field testing, evidenced by the widespread adoption of lateral flow assays (LFA) [33]. Unlike the more complex optical or electrochemical sensing methods, colorimetric sensors have already established a strong presence in clinical and at-home testing.
In contrast, fluorescent systems can offer improved sensitivity and quantitative abilities by coupling biomarker capture with a light-emissive signal. However, this can come with a reduction in simplicity compared to a simple colorimetric lateral flow assay, as instrumentation would be needed for precise quantification. Current clinical advancements in colorimetric and fluorescent platforms focus on refining sensitivity and usability, with CRISPR-Cas systems emerging as an approach for extremely accurate yet simple diagnostic systems. CRISPR-Cas systems' strong specificity and programmability enable significantly more sensitive sensing and the ability to tune existing diagnostics for new viruses and mutated variants.
The specificity of CRISPR-Cas-based colorimetric reporter systems has been utilized to make highly multiplexed diagnostics for multiple viruses and subtypes, simplifying the administration of multi-virus testing by requiring only one substrate [34]. Further, this strong specificity can help reduce sample workup and purification steps by enabling consistent viral sensing directly in serum [35]. With the time sensitivity accompanying viral infections, improvements in the administration and time-to-result of tests make them much more conducive for rapid field testing. Beyond CRISPR systems, other novel colorimetric reporting systems have also been demonstrated. Weerathunge et al. demonstrated a Murine Norovirus (MNV) colorimetric sensor, which utilized a gold ‘nanozyme’ that produces a blue color when the virus displaces color-suppressing aptamers [36]. Offering speed, sensitivity, and simplicity in administration, this example shows how alternatives to established capture and readout mechanisms in colorimetric tests can improve upon an already accessible diagnostic approach.
Despite their simplicity, colorimetric sensors have still exemplified how further refinements can help simplify the interpretation of assay results. Visual readouts are well-suited for simple, binary detection of an infection, but granularity can be added to colorimetric readouts by coupling computational analysis to the assay. For instance, in a plasmonic nanoparticle-based LFA for SARS-CoV-2 detection, a bimodal detection approach was used to provide an initial visual readout followed by a quantifiable fluorometric reporter [37]. Two-step readouts like this could benefit clinical testing since the first reporter can enable quick responses like isolation and contact tracing. In contrast, the more accurate secondary readout can help clinicians plan treatment regimens. Quantifiable colorimetric readouts would previously require dedicated detection hardware, but recent work has aimed to democratize this process by using hardware that clinics will already have. Since the requirements for processing a colorimetric readout are essentially a light source, a camera, and a means of processing a signal, smartphones, and computers can replace a dedicated detector, using their screens as a light source and their built-in cameras for detection [38]. For example, Kim et al. demonstrated a SARS-CoV-2 CRISPR-Cas12 trans-cleavage assay using a smartphone app to quantify the colorimetric readouts of N-protein detection [39]. Using a common dye for the reporting system, the assay was both cheap to produce and able to be run by anyone with a smartphone. Incorporating easy-to-use interfaces in such readout programs makes an additional dimension of viral diagnosis accessible to clinicians and patients without modification to assay administration. Such assays could also be implemented using commodity hardware in clinics with a low financial barrier.
Colorimetric diagnostics' simplicity, mainly when administered in a lateral flow assay, has already achieved the accessibility that other diagnostics seek to attain. However, there is always room for refinement. The binary nature of colorimetric readouts leaves much to be desired regarding quantification, and shifts towards more granular readouts offer improvements in this area. Further, the development of multiplexed tests can improve the number of viruses being screened within a single assay, improving the efficiency of each assay.
Non-Optical Methods
While both optical and colorimetric biosensing technologies have seen significant improvements, which improve their clinical viability, electrochemical sensing methods have presented themselves as another viral diagnostic approach, which has also seen recent democratization efforts. These methods, including impedance spectroscopy, voltammetry, and amperometry, offer sensitive and quantitative diagnostic readouts packaged into small, cheap, and simple systems. Impedance spectroscopy monitors changes in electrical resistance resulting from a binding event of an analyte, such as a viral antigen, to a capturing surface. Voltammetry measures binding by analyzing current as a function of applied potential, which can enable viral detection directly through analyte oxidation or reduction and redox-active labels. Voltammetric sensors boast strong sensitivity, rapid measurement, and relative portability, and their sensitivity can be maximized by incorporating specific capture elements like antibodies [40]. Amperometry biosensors achieve detection by measuring current at a fixed potential, where analyte binding results in a proportional, measurable redox reaction at the electrode. The simplicity of amperometric biosensors makes them well-suited for compact and portable biosensing devices, such as those that could be used in clinical and field testing [41]. Nonetheless, there are still practical barriers to seeing electrochemical viral biosensing developments through to the stage of full clinical implementation. Often, electrochemical sensors require a means of additional amplification to improve the sensitivity. Further, surface biofouling becomes particularly prevalent when sensing complex media, as the absorption of proximal proteins, nucleic acids, and lipids to the sensor surface can reduce the long-term stability of the sensing system [42]. Several recent advancements in electrochemical viral biosensors have been made in their simplicity, ease of use, and robustness, bringing them closer to feasible implementation in the clinic.
Alongside the accessibility and cost improvements in optical biosensing, electrochemical viral sensors have also trended towards cheaper and more robust sensing surfaces. These improvements can be tailored to clinical adoption through reusable or disposable, single-use sensing surfaces. It was recently demonstrated that gold leaf electrodes - made of extremely thin gold sheets - can be engineered into electrochemical viral biosensors by immobilizing oligonucleotides conjugated with redox-mediating compounds like methylene blue [43]. Since the electrodes could be assembled with gold leaf sheets, a razor, stencils, and simple adhesives, they lack the costly cleanroom equipment and labor often required to manufacture gold electrodes. Further, incorporating isothermal amplification into the assay protocol enabled the detection of HIV and HPV without even a thermal cycler. This approach to electrode manufacturing is strongly conducive to both mass manufacturing and self-assembly in grassroots testing environments. Advances in electrode materials have also pushed the democratization of electrochemical-based viral diagnostics. Electrodes utilizing graphene have also proven effective for viral biosensing due to their high surface area, conductivity, and compatibility with functionalization. For example, Huang et al. demonstrated a graphene-based Hepatitis B surface antigen sensor, which also touted simple, cleanroom-free manufacturing, that could detect the antigen in human serum [44]. Although the electrode was primarily described as an alternative for lab-based testing, this sensor's simple manufacturing and disposability could also make it well suited for the clinic as a cheap, pre-manufactured product. The benefits of graphene-based electrodes have been demonstrated more widely in the field, with graphene being incorporated into nanocomposite inks [45] and even bacterially derived cellulose [46]. Incorporating recognition elements into matrices like cellulose and inks enables deposition through screen printing for cheaper and simpler electrode fabrication as an alternative to simple metal electrodes. Screen printing can mass-produce graphene electrodes, as their surfaces can be engineered to immobilize virus-recognizing moieties like antibodies [47]. While antibody-immobilized electrodes are less affordable and robust than capture moieties like nucleic acids, their specificity is strongly conducive to directly testing patient samples in media such as saliva or serum. Further, the automated nature of printing heads could be combined with multiple inks containing different capture elements to give way to a scalable means of producing multiplexed-capable electrochemical sensors against multiple viral targets.
Electrode technology is one area where electrochemical sensing has advanced, with significant progress in improving sensing hardware for clinical adoption. While academic researchers may find traditional electrochemical setups straightforward to assemble, clinical labs require hardware tailored to their needs—prioritizing speed, throughput, and ease of use. Compact, user-friendly designs are far more practical in clinical settings, and recent studies have demonstrated such solutions for viral sensing. For example, during the COVID-19 pandemic, multiple compact and affordable sensors were developed using accessible electronics and simple readouts. Salahandish et al. created a multiplexed EIS sensor with commercially available hardware [45], enabling binary detection of SARS-CoV-2 and variant-specific identification. Similarly, another study demonstrated an amplification-free immunosensor targeting viral RNA using a portable, smartphone-operated electrochemical workstation [48]. This plug-and-play system required just two copies of SARS-CoV-2 per assay, proving that compact hardware can maintain high sensitivity. Further streamlining clinical viral sensing, wireless data transmission allows at-home testing with real-time results sent directly to clinics. One example used laser-engraved graphene electrodes in a SARS-CoV-2 diagnostic device that wirelessly transmitted multiplexed results [49]. Each sensor detected viral proteins or IgG/IgM antibodies, enabling high-sensitivity, multi-target testing. Importantly, these sensing surfaces are also disposable, making them promising candidates for pre-packaged and sterile single-use assays. Such devices could enhance telemedicine by bridging the gap between home and clinic. Moreover, integrating wireless sensors into IoT ecosystems and population monitoring platforms could significantly improve large-scale infection surveillance.
Electrochemical viral biosensing has emerged as a versatile and democratized diagnostic tool, combining sensitivity, portability, and cost-effectiveness to bridge gaps between research and clinical implementation. Advances in impedance spectroscopy, voltammetry, and amperometry have enabled compact, quantitative systems. At the same time, innovations in electrode materials, such as affordable gold leaf and graphene surfaces, have simplified manufacturing and improved accessibility. Coupled with user-friendly hardware designs, including smartphone-compatible workstations and wireless telemedicine integration, these systems offer multiplexed, high-sensitivity detection without sacrificing practicality. However, barriers to clinical translation persist. Protein-based capture motifs like antibodies still face shelf-life stability and batch-to-batch variability challenges. At the same time, temperature sensitivity during storage and operation can compromise performance in resource-limited settings. Biofouling in complex matrices like blood or saliva remains a critical limitation, often requiring surface passivation or frequent recalibration [50].
Additionally, many systems still rely on amplification steps or redox labels to achieve clinically relevant sensitivities, adding complexity to workflows. Despite these hurdles, disposable sensing surfaces and scalable production methods (like screen-printed graphene electrodes [51]) underscore the potential for widespread adoption. As electrochemical sensors continue to evolve - addressing stability, standardization, and environmental robustness - their integration into Internet of Things (IoT) ecosystems and clinical workflows shows promise to transform both point-of-care diagnostics and population-scale surveillance, bringing precision medicine closer to patients and clinicians.
QCM
Gravimetric sensing provides another potential avenue for the clinical detection of viruses, offering operational simplicity by not requiring labeling steps, which may be present in optical sensing methods. Quartz crystal microbalance (QCM) instruments utilize the piezoelectric effect, passing an electric potential through a transducer surface to induce a vibrational oscillation through contraction and expansion of the quartz crystal lattice [52]. The addition of mass to the surface can be tracked through changes in the transducer's resonant frequency [53]. If a viscoelastic material is added to the surface, like biological materials, then the dissipation of the oscillations can also be tracked [52]. Like other surface-based sensing methods, QCM can be adapted for viral diagnostics by immobilizing viral capture ligands to the surface. While QCM has generally seen less use in clinical diagnostics, it presents a promising alternative to traditional sensing methods. This is mainly due to the instruments' low cost, compact size, and operational simplicity.
Like other surface-based methods such as SPR and BLI, it is possible to immobilize capture ligands like antigens and antibodies on the surface for viral detection. The antigen-capture approach has been used for various viruses, including SARS-CoV-2 [54] and African swine fever (ASF) [53]. Antibodies have also been used for viral antigen capture, with studies using this QCM approach to detect HIV-1 [55], bovine leukemia virus [56], and influenza-A [57]. While these approaches were practical, they are not directly conducive for clinical use. The immobilization of proteins or antibodies for capture would need to be done in the clinic, adding costly and fragile reagents, more complicated assay administration, and more opportunities for procedural error. An alternative approach is likely required to bring QCM into the clinic.
Molecularly imprinted polymers (MIPS) have been shown as a potential alternative for protein-based capture on QCM systems. They offer the ability to cheaply functionalize surfaces without the complications of temperature stability that protein capture ligands incur. This means that surfaces can be premade and sent to clinics without storage concerns, and sensor surfaces would be ready to accept diagnostic samples with no additional workup. MIP surfaces are often washable as well, which makes these surfaces more affordable for clinics by lowering the cost per run [58]. However, molecularly imprinted polymer QCM sensors are not a recent approach in viral diagnostics. For instance, in 2012, Jenik et al. reported an assay to bind different picornaviruses, such as human rhinovirus (HRV) and foot-and-mouth disease virus (FMDV), using stamp imprinting with template viruses [59]. Being able to differentiate between different viral serotypes with signals multiple orders of magnitude stronger than non-specific binding, the process shows how a multi-virus sensor could be built on a QCM platform using MIPs for capture. In 2005, Tai et al. demonstrated a similar molecularly imprinted polymer process, demonstrating that smaller peptides from the linear epitope of the Dengue virus NS1 protein could also be used for detecting viral samples. They achieved quantitative detection of the NS1 protein in crude and purified samples [60]. Despite these studies not being relatively recent, we have yet to see a mass-produced, readily available MIP solution for clinical adoption. For this QCM approach to reach the clinic, extra development work will need to be done to bridge this gap.
Generally, QCM presents itself as a promising potential technique for clinical biosensing. It offers high sensitivity and real-time sensing while maintaining a relatively simple operation. Although standard QCM can run into limitations with non-rigid analytes being added to the surface, this can be addressed through QCM-D sensing. QCM, like other methods such as SPR, BLI, and electrochemical processes, requires a capture ligand for viral sensing. However, the ability to use more straightforward, more durable capture methods like molecularly imprinted polymers can improve accessibility by simplifying the viral sensor system and by reducing the number of steps to be done in the clinic itself. While multi-region QCM sensors exist [61], the more affordable instrumentation will likely be limited to individual channels, limiting its throughput.
Comparing Approaches
Optical biosensing methods carry several advantages that could make them well-suited for clinical use. They are often extremely sensitive, which is beneficial in detecting low viral loads in the early stages of infection. Further, many optical methods like SPR and BLI do not rely on labeling for detection, which reduces the complexity of assay preparation and the possible interfering effects that labels may have on the native interaction being measured for detection. The real-time capabilities of optical methods can also enable rapid detection. When combined with high throughput and multiplexed detection strategies, optical biosensors hold the potential for high throughput mass testing. This does not mean optical detection is a silver bullet approach to viral detection, though. Often, optical instruments can be costly, and the bulky nature of many optical instruments can make them challenging to deploy in small clinics and field testing.
Some instruments, such as SPR chips and single-use BLI probes, can have high running costs. Further, additional considerations must be taken when using optical instrumentation, such as the effects of temperature, buffer mismatches, and pH. While these factors can be accounted for in a research setting, they add further complexity and training for clinicians. Assay interpretation and false positives can also be a risk for the point-of-care deployment of these instruments since non-specific binding could be interpreted as a detected infection in untrained hands. Conversely, colorimetric sensors offer far greater simplicity regarding administration and result interpretation but sacrifice some sensitivity and granularity.
Similarly, non-optical methods also balance several benefits and drawbacks. Often, instruments like electrochemical sensors are more accessible to clinics than their optical counterparts due to their relatively low cost. Their compact nature makes them more feasible for various situations, from smaller clinics to field testing. This is further bolstered by advancements in manufacturing capabilities, like printable electrodes and pre-functionalized surfaces, which can provide out-of-the-box functionality for rapid test administration. Their portability means they can also be scaled with less of a need for multiplexed testing, and the simplicity of electrochemical sensors means they could be integrated into portable solutions for community-level testing in the field. While these forms of biosensors are less susceptible to environmental factors like refractive index mismatches, electrochemical sensors can suffer from strong biofouling effects, particularly when sensing in complex matrices like serum. Further, signal interference can be possible in electrochemical sensors due to other materials in the sample that may be, for instance, redox-reactive. While QCM and electrochemical sensing hardware can be designed with reusability in mind, there is still a cost associated with using the instrumentation, as components like electrodes can degrade over time.
When directly comparing these approaches, none is explicitly a perfect technique that is the most ideal for clinical deployment. While the portability and lower cost of electrochemical sensors may seem appealing, the sensitivity of optical sensors can also make a strong case. This has meant that clinics must weigh the benefits and drawbacks of each diagnostic method, determining which concessions are acceptable while meeting their needs. The innovations we see in recent diagnostic publications - both in the realms of optical and non-optical viral biosensing - have aimed to minimize the drawbacks of their respective approaches and minimize the concessions clinics would have to make. Logistics can also play a significant role in the feasibility of applying novel diagnostics to the point-of-care; as such, the development and production of biosensing surfaces, sensing hardware, and software also significantly determine whether a clinic could feasibly adopt new technologies.
Diagnostic Development - Hardware and Software
Advancements in viral biosensor technology are essential, but ensuring ease of use and accessibility is crucial for widespread adoption at the point of care. Developing more straightforward instruments and protocols reduces the training required for operators, and lowering the costs of these instruments allows more clinics to utilize state-of-the-art sensing technologies.
Improvements in accessibility for viral diagnostics can be achieved in various ways, including providing pre-made sensing surfaces that offer out-of-the-box functionality, designing instruments that can be easily assembled within the clinic, and creating software that simplifies readouts for healthcare providers and patients. Reducing the number of preparation steps simplifies the administration of diagnostics and minimizes the risk of human error.
Additionally, pre-manufacturing essential diagnostic components, such as microfluidics and functionalized sensor chips, increases reliability and practicality in the field. For instance, mass-producing chips with pre-immobilized capture ligands streamlines the setup process, reduces user error, and requires less skilled labor. Simplifying manufacturing processes can also lower costs through economies of scale, making innovative viral diagnostics more accessible.
3D Printing
3D printing has emerged as a pivotal tool in improving the accessibility of diagnostic technology. With the costs of 3D printers falling and the library of open-source designs growing, it is now possible to repair, modify, or even outright assemble instruments by printing parts. In conjunction with the previously discussed improvements in biosensing technology, it is more feasible than ever to build diagnostic systems.
Several studies have demonstrated the ability of 3D printers to be used to make components of diagnostic systems, including microfluidic systems, at high resolutions. Standard methods like extrusion, stereolithography, and material jetting-based 3D printing have demonstrated microfluidic feature resolutions as high as single micrometers, with processes like direct laser writing coupled with photoresists even reaching the nanometer scale [62]. These processes can also be connected with biocompatible materials like polyethylene glycol diacrylate (PEGda) [63] and silicone [64] (among others [65]) to minimize the leaching of material and even enable wearable diagnostic technology. In a more indirect sense, low-cost printers can make molds to cast microfluidics from materials like PDMS [66]. Fluidics are not the only diagnostic components that 3D printing aims to democratize; materials like liquid silica resins and germanate glass have been successfully used to print optical components like prisms and lenses [67], as well as supporting mounts for hardware like smartphones [68] in DIY detectors.
3D-printed components have already significantly impacted the realm of viral diagnostics. For instance, aerosol-jet 3D printing was used by Ali et al. to print 3-dimensional micropillar arrays that were coated in graphene and functionalized with viral antigens. These 3D-printed sensors were used as electrodes to detect SARS-CoV-2 spike protein and nucleocapsid-specific antibodies in patient sera [69]. Similarly, 3D-printed electrode cassettes were recently developed by Sharma et al., which were combined with paper electrodes to detect dengue and chikungunya antigens in serum through cyclic voltammetry [70]. Krejcova et al. developed a 3D-printable, bead-based microfluidic chip system that isolated paramagnetic beads, followed by voltammetry-based detection [71]. Printed fluidic systems have even been designed to automate ELISA reagent delivery, as demonstrated by Karamzadeh et al., which successfully detects the SARS-CoV-2 N-protein in a largely automated format [72]. Extending beyond sensing interfaces themselves, the COVID-19 pandemic saw widespread use of 3D printing for manufacturing face shields [73]; plastic supports for lateral flow assays [74], nasopharyngeal swabs [75], housings for respirator filters [76], and pumps [77]. While some 3D-printable technologies have been directly demonstrated in viral diagnostics, numerous other 3D-printed instruments have been published that could be adapted for detecting viral infections, demonstrating the continued progress in this field. Examples include microspectroscopy imaging devices [78], PCR thermal cyclers [79,80], photosensitive drug delivery systems [81], quartz crystal microbalances, and electrochemical sensors [82,83].
While the capabilities of 3D printing have been shown across many methods of viral biosensing, continued development will still be needed to lower the barrier of technical knowledge to utilize these tools properly. This is partly aided by the tendency for 3D-printed, open-sourced electronic devices to be made with off-the-shelf components. This aspect is critical in bringing novel diagnostic technology to logistically constrained and underfunded areas. Utilizing generic components helps eliminate the need for niche or proprietary parts, a common hurdle regarding traditional laboratory equipment. Further, the upkeep of these instruments designed with this approach can be far more manageable as replacement parts and instrument schematics will be more accessible to the end user than what may be seen for commercial biosensing technologies. While publications touting novel sensing methodologies initially seem accessible to clinics, they have little use if the instrumentation required to adopt the methods is prohibitively expensive. Further refinements beyond these initial studies need to be done to design easy-to-assemble, printable components to minimize hardware limitations that clinics may often face.
Sensor Surface Fabrication
Another aspect of bringing more advanced bioanalytical techniques into the clinic for viral biosensing is the ability to produce highly consistent, functionalized, and ready-to-use sensing surfaces. Functionalizing sensing substrates in manufacturing reduces the potential for human error before being sent to a clinic, providing a more ‘plug and play’ process in diagnostics. Further, chip robustness and reusability reduce the cost per run, helping clinics digest the cost of expensive analytical techniques. Pre-functionalizations can range from self-assembled monolayers to polymer and nanomaterial coatings to surfaces pre-functionalized with viral capture motifs [84]. Metallic sensor surfaces, such as those used in SPR, QCM, and electrochemical diagnostics, can be manufactured in bulk in a clean room using physical deposition methods [85]. This extends beyond metallic surfaces, and thermally grown silicon chips have also been used in viral biosensing [31,32]. Specific surface designs like microarrays, wells, and layered materials can be achieved by coupling physical deposition with photolithography [86,87]. These chips can then be connected to capture elements by carefully selecting surface chemistry. Generic capture methods are also appealing for clinical use since a single capture protocol could be applied for the simple production of a multi-readout sensor. For instance, gold-thiol chemistry can immobilize thiol-modified capture motifs such as antigen-specific nucleic acids [88]. Materials like paper have even been shown as an affordable diagnostic substrate. For example, freeze-dried, toehold switch-containing paper substrates have been combined with isothermal amplification and colorimetric readouts to detect the Zika virus [89].
In electrochemical sensing, screen printing offers a more accessible alternative to deposition-based electrode fabrication. Generally, screen-printed electrodes are cheaper and more disposable, and their compatibility with bulk production is conducive to scaled manufacturing [90]. Further, they lack the requirement for a high vacuum and a cleanroom environment for manufacturing, eliminating a lot of training required for cleanroom manufacturing. They can enable printing on flexible materials like paper and plastic, whereas other sensor surfaces are constrained to glass or metal substrates [91]. A range of printable electrode materials, such as conductive inks containing graphene, polymers like PEDOT: PSS, and nanoparticle-based solutions [92,93,94], are available. Screen-printed electrodes have already been used in viral diagnostics, including detecting Dengue, HBV, HCV, Zika virus, H1N1, and even in variant-specific SARS CoV-2 detection [47,95]. Due to the production cost of metallic surfaces like electrodes, screen printing presents an affordable, scalable alternative. Further, quickly disposable electrodes develop single-use, ready-to-run sensing surfaces.
While cheap, single-use sensing surfaces represent one approach to lowering the cost of viral diagnostics, regenerable functionalized surfaces offer another approach to sustainability. The ability to cleanly strip analytes from a surface enables the reuse of sensing surfaces, which lowers the per-run cost of costly sensing surfaces that cannot be improved by cheaper alternatives (such as gold-coated chips in SPR and QCM). This has been shown using molecularly imprinted polymers [96] and surface-exposed NTA groups to capture histidine-tagged proteins [26,97,98]. Because approaches such as these also lack functional proteins for capture, they benefit from avoiding sensitive storage conditions. This holds the potential of cheaper running costs and more straightforward manufacturing scalability, which could further lower costs.
Software
Coupled with the development of accessible diagnostic hardware, novel software packages have also been developed to streamline the process of viral diagnostics. The overall goal of pushing new technology into the clinic can be aided by software in several ways. From broad-scale infection reporting and tracking software to smartphone apps coupled with DIY hardware or even machine learning algorithms built to process complex samples, software advancements go hand in hand with improving the adoption of new diagnostic technology. By streamlining result delivery, simplifying wide-scale testing, and automating the processing of diagnostic data, software tools reduce the administrative burden on clinics, making it easier and more cost-effective to incorporate innovative diagnostics into routine care.
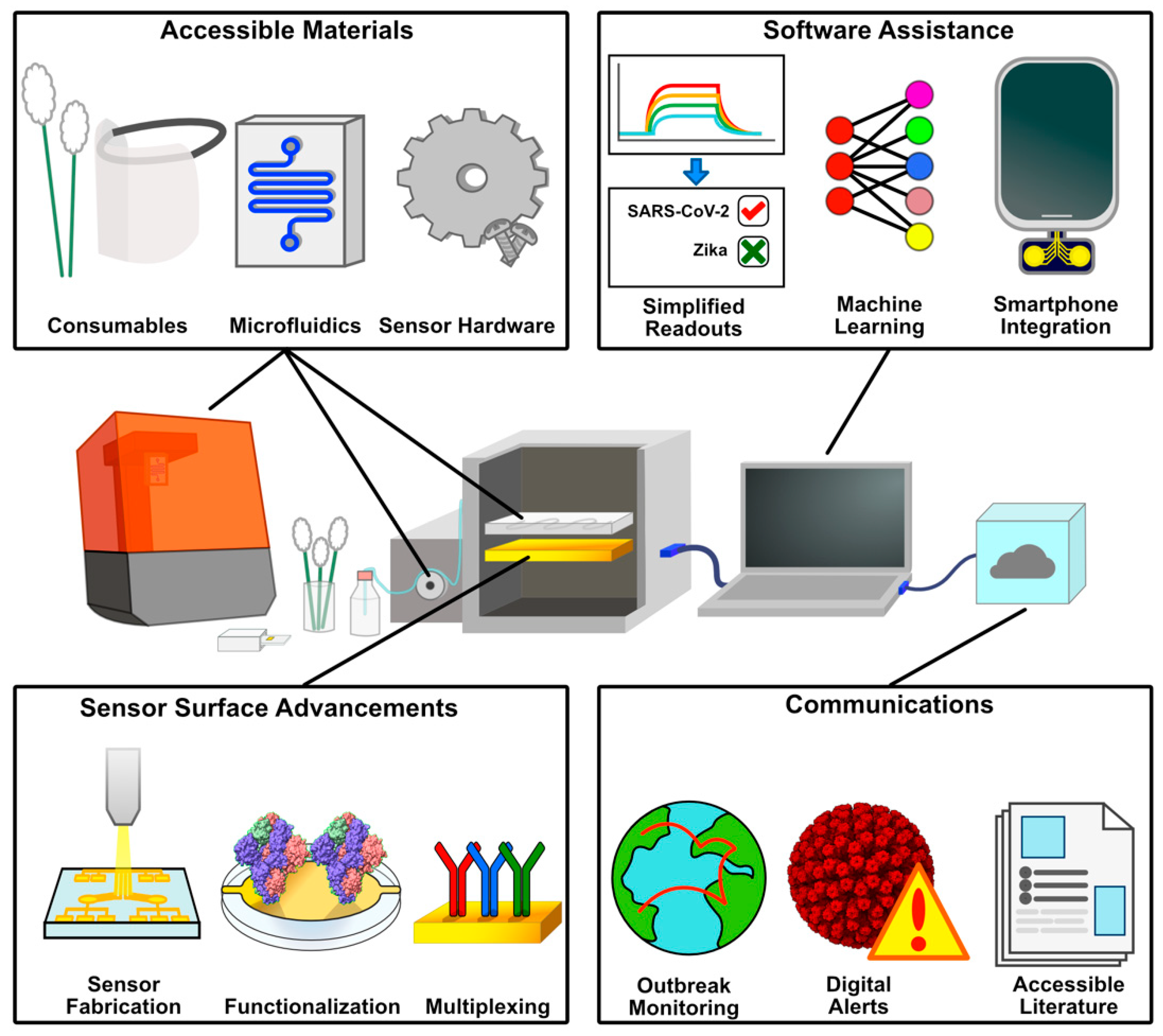
Figure 2.
Aspects of POC Accessibility to Novel Diagnostics. 3D printing enables self-production of consumables, protective equipment, sensor hardware, and microfluidic systems. Sensor surface advancements improve accessibility and cost through scalable, mass manufacturing, and pre-functionalized sensing surfaces. These hardware solutions benefit from software, simplifying test administration and analyzing complex data sets. Communication of these results helps spread information and track infection events on a broader scale.
Figure 2.
Aspects of POC Accessibility to Novel Diagnostics. 3D printing enables self-production of consumables, protective equipment, sensor hardware, and microfluidic systems. Sensor surface advancements improve accessibility and cost through scalable, mass manufacturing, and pre-functionalized sensing surfaces. These hardware solutions benefit from software, simplifying test administration and analyzing complex data sets. Communication of these results helps spread information and track infection events on a broader scale.
Machine learning is drastically changing the scientific world, and while we find ourselves in the early stages of its advancement into clinical settings, its potential can already be seen. Since machine learning and artificial intelligence tools are well-suited for processing enormous amounts of data, information sources like viral sequences, patient symptoms, and epidemiological trends could all be used to achieve higher-level analysis that individual diagnostic assays cannot attain. Often, machine learning tools are associated with the underlying analysis backing diagnostic development, such as high-throughput screening of diagnostic-target pairs [99]. However, recent advancements in machine learning extend beyond academic labs, with the benefits of their computational power now reaching the clinic. For instance, Khan et al. proposed a tunicate swarm machine learning algorithm for efficient data processing and transmission of biosensor data between patients and clinicians [100]. The development of such data pipelines is vital for active symptom monitoring and testing recommendations, as it allows for integrating a range of Internet of Things (IoT) sensors, including those for ECG, body temperature, glucose, and EMG. Beyond backend data management, machine learning has also been deployed for clinician and patient use. Machine learning tools can be used to track multiple parameters like symptoms, CD4 counts, and adherence to treatment regimens, which could provide clinicians with strong tools to predict infections and follow through with treatments [101]. Further, broad-scale infection predictions can be made through mass surveillance and publicly available information like search engine trends, where increases in searches related to symptoms could help anticipate waves of infections [102]. Such tools could drastically help in preemptively stocking assay reagents rather than chasing strong demand like what was seen in the COVID-19 pandemic.
With the mass implementation of artificial intelligence tools into every science and technology realm, it is hard not to see its promise in viral diagnostics. Particularly following the COVID-19 pandemic, we have seen the strong need for infrastructure that can handle diagnostics en masse. The mass data processing capabilities and ease of use of machine learning tools present a novel intersection between accessibility and technical strength, which could show substantial benefits in viral diagnostics. Nonetheless, there still needs to be a gradual, intentional implementation of such tools into clinical testing to ensure proper use and an understanding of how these tools operate. The tendency for AI tools to ‘hallucinate,’ confidently giving incorrect results, carries much more dire consequences when lives are at stake [103]. In this regard, machine learning tools must be implemented cautiously to ensure their convenience does not enable blind trust in the readouts given by the diagnostics they may use.
Smartphone Apps
Mainly due to isolation protocols from the COVID-19 pandemic, the coupling of viral diagnostics and smartphone apps became highly prevalent. Depending on the app, the purpose can range from symptom monitoring to contact tracing or even utilizing a smartphone in a home-built diagnostic device. Many apps have been published that ask users to answer symptom questionnaires regularly and alert patients and healthcare providers when symptoms warrant testing [104,105]. The pandemic also saw telemedicine's widespread adoption and expansion, which gave patients and clinicians a more convenient option [106]. Such styles of apps can also be coupled with methods to improve diagnostic throughput - like sample barcoding and automated alert systems - to rapidly diagnose and alert patients of positive results without additional visits to the clinic [107,108]. Alongside symptom monitoring apps, the pandemic also saw the broad adoption of contact tracing apps, which use proximity monitoring of other signed-up users to anonymously alert potentially exposed individuals. These apps were mainly popularized due to their adoption by both Apple and Google, as well as through state-sponsored solutions like TraceTogether and COVIDSafe (from Singapore and Australia, respectively) [107]. Other apps have been developed to use smartphones as key components of assays, serving as detectors. For instance, smartphones have been used in bioluminescent RT-LAMP to detect the Zika virus in urine and saliva and HIV in blood [109]. Similarly, numerous colorimetric COVID-19 tests have utilized smartphones for test readouts in colorimetric and fluorescent tests, taking advantage of the high-quality cameras present in modern smartphones [16,110,111]. Smartphone apps add another angle of usability improvements for modern diagnostics by avoiding the reliance on proprietary or complex systems for diagnostic readouts. Given the commonality of smartphones today, a well-designed smartphone app can eliminate the requirement for a clinician to process a readout, leaving them freer to run the assays themselves.
Pre-built diagnostic solutions are appealing to clinics due to the simplicity of their setup and learning processes. Still, the increase in home-built alternatives has also presented a more grassroots approach. Publicly available hardware and software have proven that significant cost and logistical benefits can be had from the end user taking the burden of assembly upon themselves. With the barrier to entry for processes like 3D printing continuing to become more accessible, it is becoming far more feasible to take this approach to bring new diagnostic technologies into the clinic. An ideal home-built clinical solution for viral diagnostics could incorporate every aspect of these recent democratization efforts, coupling freely available hardware to open-sourced software packages and using regenerable sensing surfaces to maximize the number of assays per purchase.
Democratizing Scientific Communications
When discussing advancements that enable clinics to adopt new diagnostic technologies, it is also essential to acknowledge the role of scientific journals in disseminating information to clinicians. In the same way that new technologies have accessibility concerns, particularly in cost and training requirements, there is often a perceived gap between the academic community and the general public. This disparity is mainly present in the sciences that drive diagnostic development, like chemistry, material sciences, and informatics [112]. In recent years, and particularly following the broad reach of the COVID-19 pandemic on the public, many journals have made significant moves to improve the accessibility of their publications. New pilot programs have been adopted, such as translating abstracts from English to other languages like Japanese, Danish, Thai, and Arabic [113]. Recent years have also seen movements that promote disability accessibility in articles. Font sizes, acronym use, and design choices like color and contrast in figures are some considerations that can help open scientific literature to more readers [114,115].
Regarding greater public access, journals have increasingly adopted plain-language summaries of their published papers [116,117]. For example, replacing the term ‘hypoxia’ with ‘lack of oxygen’ construes the same idea in a format that a wider audience can understand. There have also been additions like definitions of terms, lists of acronyms, bulleted key points, and video or audio abstracts to accompany paper graphics [118,119,120]. This is a subtle but important aspect in adopting new diagnostics since accessible scientific literature equips clinicians with the knowledge necessary to administer and understand the diagnostics they may be adopting into their workflows. Improving patient access to scientific literature also helps them understand the procedures they may undergo in a clinic. There is no doubt that in the coming years, artificial intelligence will also see increasing use by clinicians and the public to summarize scientific information. With these tools often being trained by scrubbing vast amounts of data from online sources, it is even more relevant to make scientific details digestible, succinct, and easily accessible to ensure that their responses are grounded in truth.
The push for greater accessibility in scientific publishing mirrors the broader goal of democratizing viral diagnostics. By adopting plain-language summaries, multilingual abstracts, and inclusive design, journals are bridging the gap between academic researchers and clinicians by equipping them with the necessary information to adopt and administer state-of-the-art diagnostic techniques. These efforts also extend to patients whose understanding and receptivity of new diagnostic procedures are enhanced through digestible formats like bulleted key points or audio abstracts. As AI-driven tools increasingly facilitate access to scientific knowledge, ensuring clarity and standardization in publications will grow even more critical to prevent misinformation and align innovation with real-world needs. Accessible literature is supplemental to diagnostic advancement and a foundational step toward equitable adoption across diverse clinical and public health settings.
Conclusion
The drive to develop faster, more sensitive, and accessible viral diagnostics underscores the clinical world's commitment to early disease detection. While the COVID-19 pandemic focused on this need, emerging threats like avian flu and monkeypox reinforce the strong demand for innovation. Significant progress has been made in biosensing technologies, enhancing sensitivity, reproducibility, and the detection of novel analytes. However, transitioning from promising research to practical, point-of-care diagnostics still requires overcoming cost, scalability, and ease-of-use challenges. Techniques such as SPR, BLI, and electrochemical sensing offer remarkable sensitivity. However, their adoption in clinical settings hinges on reducing instrument cost, minimizing device footprint, and simplifying operation and data interpretation. Multi-faceted improvements have been seen recently, with democratization efforts in both sensing surface chemistry and production, greater accessibility in the instrumentation hardware and software, and the dissemination of both assay results and scientific information. In effect, accessibility improvements in diagnostics don’t just lie in the sciences developing the assays. It requires a multidisciplinary effort between scientists, engineers, and even journalists to not only create new sensing technologies but to put them in clinicians' hands and equip them with the knowledge needed to utilize them effectively.
References
- Damborský, P.; Švitel, J.; Katrlík, J. Optical Biosensors. Essays Biochem 2016, 60, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Grieshaber, D.; MacKenzie, R.; Vörös, J.; Reimhult, E. Electrochemical Biosensors - Sensor Principles and Architectures. Sensors (Basel) 2008, 8, 1400–1458. [Google Scholar] [CrossRef] [PubMed]
- Marx, K. A. Quartz Crystal Microbalance: A Useful Tool for Studying Thin Polymer Films and Complex Biomolecular Systems at the Solution−Surface Interface. Biomacromolecules 2003, 4, 1099–1120. [Google Scholar] [CrossRef]
- Mouro, J.; Pinto, R.; Paoletti, P.; Tiribilli, B. Microcantilever: Dynamical Response for Mass Sensing and Fluid Characterization. Sensors (Basel) 2020, 21, 115. [Google Scholar] [CrossRef]
- Fowler, V. L.; Armson, B.; Gonzales, J. L.; Wise, E. L.; Howson, E. L. A.; Vincent-Mistiaen, Z.; Fouch, S.; Maltby, C. J.; Grippon, S.; Munro, S.; et al. A Highly Effective Reverse-Transcription Loop-Mediated Isothermal Amplification (RT-LAMP) Assay for the Rapid Detection of SARS-CoV-2 Infection. Journal of Infection 2021, 82, 117–125. [Google Scholar] [CrossRef]
- Otoo, J. A.; Schlappi, T. S. REASSURED Multiplex Diagnostics: A Critical Review and Forecast. Biosensors (Basel) 2022, 12, 124. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, H. H.; Park, J.; Kang, S.; Kim, M. Surface Plasmon Resonance: A Versatile Technique for Biosensor Applications. Sensors (Basel) 2015, 15, 10481–10510. [Google Scholar] [CrossRef]
- Abbas, A.; Linman, M. J.; Cheng, Q. Sensitivity Comparison of Surface Plasmon Resonance and Plasmon-Waveguide Resonance Biosensors. Sens Actuators B Chem 2011, 156, 169–175. [Google Scholar] [CrossRef]
- Liu, B.; Liu, X.; Shi, S.; Huang, R.; Su, R.; Qi, W.; He, Z. Design and Mechanisms of Antifouling Materials for Surface Plasmon Resonance Sensors. Acta Biomaterialia 2016, 40, 100–118. [Google Scholar] [CrossRef]
- Riedel, T.; Rodriguez-Emmenegger, C.; de los Santos Pereira, A.; Bědajánková, A.; Jinoch, P.; Boltovets, P. M.; Brynda, E. Diagnosis of Epstein–Barr Virus Infection in Clinical Serum Samples by an SPR Biosensor Assay. Biosensors and Bioelectronics 2014, 55, 278–284. [Google Scholar] [CrossRef]
- Florschütz, K.; Schröter, A.; Schmieder, S.; Chen, W.; Schweizer, P.; Sonntag, F.; Danz, N.; Baronian, K.; Kunze, G. ‘Phytochip’: On-Chip Detection of Phytopathogenic RNA Viruses by a New Surface Plasmon Resonance Platform. Journal of Virological Methods 2013, 189, 80–86. [Google Scholar] [CrossRef]
- Yano, T.; Kajisa, T.; Ono, M.; Miyasaka, Y.; Hasegawa, Y.; Saito, A.; Otsuka, K.; Sakane, A.; Sasaki, T.; Yasutomo, K.; Hamajima, R.; Kanai, Y.; Kobayashi, T.; Matsuura, Y.; Itonaga, M.; Yasui, T. Ultrasensitive Detection of SARS-CoV-2 Nucleocapsid Protein Using Large Gold Nanoparticle-Enhanced Surface Plasmon Resonance. Sci Rep 2022, 12, 1060. [Google Scholar] [CrossRef]
- Tombelli, S.; Minunni, M.; Luzi, E.; Mascini, M. Aptamer-Based Biosensors for the Detection of HIV-1 Tat Protein. Bioelectrochemistry 2005, 67, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Chen, R.; Kan, L.; Duan, F.; He, L.; Wang, M.; Cui, J.; Zhang, Z.; Zhang, Z. Surface Plasmon Resonance Aptasensor Based on Niobium Carbide MXene Quantum Dots for Nucleocapsid of SARS-CoV-2 Detection. Microchim Acta 2021, 188, 316. [Google Scholar] [CrossRef] [PubMed]
- P4SPR 2.0. Affinite Instruments. https://www.affiniteinstruments.com/p4spr-2-0 (accessed 2025-04-22).
- Dong, T.; Han, C.; Jiang, M.; Zhang, T.; Kang, Q.; Wang, P.; Zhou, F. A Four-Channel Surface Plasmon Resonance Sensor Functionalized Online for Simultaneous Detections of Anti-SARS-CoV-2 Antibody, Free Viral Particles, and Neutralized Viral Particles. ACS Sens. 2022, 7, 3560–3570. [Google Scholar] [CrossRef]
- Meet OpenSPR | Benchtop SPR Instrument | Nicoya. https://nicoyalife.com/products/spr-instruments/openspr/ (accessed 2025-04-22).
- NanoSPR - Devices and glass plates for surface plasmon resonance. https://nanospr.com/ (accessed 2025-04-22).
- Choudhary, S.; Altintas, Z. Development of a Point-of-Care SPR Sensor for the Diagnosis of Acute Myocardial Infarction. Biosensors (Basel) 2023, 13, 229. [Google Scholar] [CrossRef]
- Wallace, S.; Kartau, M.; Kakkar, T.; Davis, C.; Szemiel, A.; Samardzhieva, I.; Vijayakrishnan, S.; Cole, S.; De Lorenzo, G.; Maillart, E.; Gautier, K.; Lapthorn, A. J.; Patel, A. H.; Gadegaard, N.; Kadodwala, M.; Hutchinson, E.; Karimullah, A. S. Multiplexed Biosensing of Proteins and Virions with Disposable Plasmonic Assays. ACS Sens. 2023, 8, 3338–3348. [Google Scholar] [CrossRef] [PubMed]
- Murali, S.; Rustandi, R. R.; Zheng, X.; Payne, A.; Shang, L. Applications of Surface Plasmon Resonance and Biolayer Interferometry for Virus–Ligand Binding. Viruses 2022, 14, 717. [Google Scholar] [CrossRef]
- Jug, A.; Bratkovič, T.; Ilaš, J. Biolayer Interferometry and Its Applications in Drug Discovery and Development. TrAC Trends in Analytical Chemistry 2024, 176, 117741. [Google Scholar] [CrossRef]
- Guo, Z.; Wilson, J. R.; York, I. A.; Stevens, J. Biosensor-Based Epitope Mapping of Antibodies Targeting the Hemagglutinin and Neuraminidase of Influenza A Virus. Journal of Immunological Methods 2018, 461, 23–29. [Google Scholar] [CrossRef]
- Enhanced Inhibition of Influenza A Virus Adhesion by Di- and Trivalent Hemagglutinin Inhibitors. Journal of Medicinal Chemistry 2019, 62, 6398–6404. [CrossRef] [PubMed]
- Preventing Influenza A Virus Infection by Mixed Inhibition of Neuraminidase and Hemagglutinin by Divalent Inhibitors. Journal of Medicinal Chemistry 2022, 65, 7312–7323. [CrossRef] [PubMed]
- Poolsup, S.; Zaripov, E.; Hüttmann, N.; Minic, Z.; Artyushenko, P. V.; Shchugoreva, I. A.; Tomilin, F. N.; Kichkailo, A. S.; Berezovski, M. V. Discovery of DNA Aptamers Targeting SARS-CoV-2 Nucleocapsid Protein and Protein-Binding Epitopes for Label-Free COVID-19 Diagnostics. Molecular Therapy - Nucleic Acids 2023, 31, 731–743. [Google Scholar] [CrossRef] [PubMed]
- Thiviyanathan, V.; Gorenstein, D. G. Aptamers and the Next Generation of Diagnostic Reagents. Proteomics Clin Appl 2012, 6, 563–573. [Google Scholar] [CrossRef]
- Dzimianski, J. V.; Lorig-Roach, N.; O’Rourke, S. M.; Alexander, D. L.; Kimmey, J. M.; DuBois, R. M. Rapid and Sensitive Detection of SARS-CoV-2 Antibodies by Biolayer Interferometry. Sci Rep 2020, 10, 21738. [Google Scholar] [CrossRef]
- Daaboul, G. G.; Freedman, D. S.; Scherr, S. M.; Carter, E.; Rosca, A.; Bernstein, D.; Mire, C. E.; Agans, K. N.; Hoenen, T.; Geisbert, T. W.; Ünlü, M. S.; Connor, J. H. Enhanced Light Microscopy Visualization of Virus Particles from Zika Virus to Filamentous Ebolaviruses. PLOS ONE 2017, 12, e0179728. [Google Scholar] [CrossRef]
- Daaboul, G. G.; Lopez, C. A.; Chinnala, J.; Goldberg, B. B.; Connor, J. H.; Ünlü, M. S. Digital Sensing and Sizing of Vesicular Stomatitis Virus Pseudotypes in Complex Media: A Model for Ebola and Marburg Detection. ACS Nano 2014, 8, 6047–6055. [Google Scholar] [CrossRef]
- Daaboul, G. G.; Yurt, A.; Zhang, X.; Hwang, G. M.; Goldberg, B. B.; Ünlü, M. S. High-Throughput Detection and Sizing of Individual Low-Index Nanoparticles and Viruses for Pathogen Identification. Nano Lett. 2010, 10, 4727–4731. [Google Scholar] [CrossRef]
- Aslan, M.; Seymour, E.; Brickner, H.; Clark, A. E.; Celebi, I.; Townsend, M. B.; Satheshkumar, P. S.; Riley, M.; Carlin, A. F.; Ünlü, M. S.; Ray, P. A Label-Free Optical Biosensor-Based Point-of-Care Test for the Rapid Detection of Monkeypox Virus. Biosensors and Bioelectronics 2025, 269, 116932. [Google Scholar] [CrossRef]
- Wang, X.; Shang ,Xiaoyun; and Huang, X. Next-Generation Pathogen Diagnosis with CRISPR/Cas-Based Detection Methods. Emerging Microbes & Infections 2020, 9, 1682–1691. [CrossRef]
- Kaminski, M. M.; Abudayyeh, O. O.; Gootenberg, J. S.; Zhang, F.; Collins, J. J. CRISPR-Based Diagnostics. Nat Biomed Eng 2021, 5, 643–656. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Xiong, E.; Tian, T.; Cheng, M.; Lin, W.; Wang, H.; Zhang, G.; Sun, J.; Zhou, X. Clustered Regularly Interspaced Short Palindromic Repeats/Cas9-Mediated Lateral Flow Nucleic Acid Assay. ACS Nano 2020. [Google Scholar] [CrossRef]
- Weerathunge, P.; Ramanathan, R.; Torok, V. A.; Hodgson, K.; Xu, Y.; Goodacre, R.; Behera, B. K.; Bansal, V. Ultrasensitive Colorimetric Detection of Murine Norovirus Using NanoZyme Aptasensor. Anal. Chem. 2019, 91, 3270–3276. [Google Scholar] [CrossRef] [PubMed]
- Gupta, R.; Gupta, P.; Wang, S.; Melnykov, A.; Jiang, Q.; Seth, A.; Wang, Z.; Morrissey, J. J.; George, I.; Gandra, S.; Sinha, P.; Storch, G. A.; Parikh, B. A.; Genin, G. M.; Singamaneni, S. Ultrasensitive Lateral-Flow Assays via Plasmonically Active Antibody-Conjugated Fluorescent Nanoparticles. Nat. Biomed. Eng 2023, 7, 1556–1570. [Google Scholar] [CrossRef] [PubMed]
- Gugliandolo, G.; Pilato, G.; Donato, N. Compact System for Colorimetric Sensor Arrays Characterization Based on Computer Screen Photo-Assisted Technology. Electronics 2021, 10, 2587. [Google Scholar] [CrossRef]
- Kim, H.; Jang, H.; Song, J.; Lee, S. M.; Lee, S.; Kwon, H.-J.; Kim, S.; Kang, T.; Park, H. G. A CRISPR/Cas12 Trans-Cleavage Reporter Enabling Label-Free Colorimetric Detection of SARS-CoV-2 and Its Variants. Biosensors and Bioelectronics 2024, 251, 116102. [Google Scholar] [CrossRef]
- Lopez-Tellez, J.; Ramirez-Montes, S.; Ferreira, T. A.; Santos, E. M.; Rodriguez, J. A. Application of Voltammetric Sensors for Pathogen Bacteria Detection: A Review. Chemosensors 2022, 10, 424. [Google Scholar] [CrossRef]
- Hammond, J. L.; Formisano, N.; Estrela, P.; Carrara, S.; Tkac, J. Electrochemical Biosensors and Nanobiosensors. Essays Biochem 2016, 60, 69–80. [Google Scholar] [CrossRef]
- Jarosińska, E.; Zambrowska, Z.; Witkowska Nery, E. Methods of Protection of Electrochemical Sensors against Biofouling in Cell Culture Applications. ACS Omega 2024, 9, 4572–4580. [Google Scholar] [CrossRef]
- Zamani, M.; Robson, J. M.; Fan, A.; Bono, M. S. Jr.; Furst, A. L.; Klapperich, C. M. Electrochemical Strategy for Low-Cost Viral Detection. ACS Cent. Sci. 2021, 7, 963–972. [Google Scholar] [CrossRef]
- Huang, K.-J.; Li, J.; Liu, Y.-M.; Cao, X.; Yu, S.; Yu, M. Disposable Immunoassay for Hepatitis B Surface Antigen Based on a Graphene Paste Electrode Functionalized with Gold Nanoparticles and a Nafion-Cysteine Conjugate. Microchim Acta 2012, 177, 419–426. [Google Scholar] [CrossRef]
- Salahandish, R.; Jalali, P.; Tabrizi, H. O.; Hyun, J. E.; Haghayegh, F.; Khalghollah, M.; Zare, A.; Berenger, B. M.; Niu, Y. D.; Ghafar-Zadeh, E.; Sanati-Nezhad, A. A Compact, Low-Cost, and Binary Sensing (BiSense) Platform for Noise-Free and Self-Validated Impedimetric Detection of COVID-19 Infected Patients. Biosensors and Bioelectronics 2022, 213, 114459. [Google Scholar] [CrossRef]
- de Lima, L. F.; Ferreira, A. L.; Ranjan, I.; Collman, R. G.; de Araujo, W. R.; de la Fuente-Nunez, C. A Bacterial Cellulose-Based and Low-Cost Electrochemical Biosensor for Ultrasensitive Detection of SARS-CoV-2. Cell Reports Physical Science 2023, 4, 101476. [Google Scholar] [CrossRef] [PubMed]
- Szydlowska, B. M.; Pola, C. C.; Cai, Z.; Chaney, L. E.; Hui, J.; Sheets, R.; Carpenter, J.; Dean, D.; Claussen, J. C.; Gomes, C. L.; Hersam, M. C. Biolayer-Interferometry-Guided Functionalization of Screen-Printed Graphene for Label-Free Electrochemical Virus Detection. ACS Appl. Mater. Interfaces 2024, 16, 25169–25180. [Google Scholar] [CrossRef]
- Zhao, H.; Liu, F.; Xie, W.; Zhou, T.-C.; OuYang, J.; Jin, L.; Li, H.; Zhao, C.-Y.; Zhang, L.; Wei, J.; Zhang, Y.-P.; Li, C.-P. Ultrasensitive Supersandwich-Type Electrochemical Sensor for SARS-CoV-2 from the Infected COVID-19 Patients Using a Smartphone. Sensors and Actuators B: Chemical 2021, 327, 128899. [Google Scholar] [CrossRef] [PubMed]
- Torrente-Rodríguez, R. M.; Lukas, H.; Tu, J.; Min, J.; Yang, Y.; Xu, C.; Rossiter, H. B.; Gao, W. SARS-CoV-2 RapidPlex: A Graphene-Based Multiplexed Telemedicine Platform for Rapid and Low-Cost COVID-19 Diagnosis and Monitoring. Matter 2020, 3, 1981–1998. [Google Scholar] [CrossRef]
- Russo, M. J.; Han, M.; Desroches, P. E.; Manasa, C. S.; Dennaoui, J.; Quigley, A. F.; Kapsa, R. M. I.; Moulton, S. E.; Guijt, R. M.; Greene, G. W.; Silva, S. M. Antifouling Strategies for Electrochemical Biosensing: Mechanisms and Performance toward Point of Care Based Diagnostic Applications. ACS Sens. 2021, 6, 1482–1507. [Google Scholar] [CrossRef]
- Kamsong, W.; Primpray, V.; Pasakon, P.; Sriprachuabwong, C.; Pakapongpan, S.; Mensing, J. P.; Wisitsoraat, A.; Tuantranont, A.; Karuwan, C. Highly Sensitive and Disposable Screen-Printed Ionic Liquid/Graphene Based Electrochemical Sensors. Electrochemistry Communications 2022, 135, 107209. [Google Scholar] [CrossRef]
- Dixon, M. C. Quartz Crystal Microbalance with Dissipation Monitoring: Enabling Real-Time Characterization of Biological Materials and Their Interactions. J Biomol Tech 2008, 19, 151–158. [Google Scholar]
- Uttenthaler, E.; Kößlinger, C.; Drost, S. Quartz Crystal Biosensor for Detection of the African Swine Fever Disease. Analytica Chimica Acta 1998, 362, 91–100. [Google Scholar] [CrossRef]
- Nilsson, P. H.; Al-Majdoub, M.; Ibrahim, A.; Aseel, O.; Suriyanarayanan, S.; Andersson, L.; Fostock, S.; Aastrup, T.; Tjernberg, I.; Rydén, I.; Nicholls, I. A. Quartz Crystal Microbalance Platform for SARS-CoV-2 Immuno-Diagnostics. Int J Mol Sci 2023, 24, 16705. [Google Scholar] [CrossRef] [PubMed]
- Ly, T. N.; Park, S.; Park, S. J. Detection of HIV-1 Antigen by Quartz Crystal Microbalance Using Gold Nanoparticles. Sensors and Actuators B: Chemical 2016, 237, 452–458. [Google Scholar] [CrossRef]
- Makaraviciute, A.; Ruzgas, T.; Ramanavicius, A.; Ramanaviciene, A. A QCM-D Study of Reduced Antibody Fragments Immobilized on Planar Gold and Gold Nanoparticle Modified Sensor Surfaces. Key Engineering Materials 2014, 605, 340–343. [Google Scholar] [CrossRef]
- Owen, T. W.; Al-Kaysi, R. O.; Bardeen, C. J.; Cheng, Q. Microgravimetric Immunosensor for Direct Detection of Aerosolized Influenza A Virus Particles. Sens Actuators B Chem 2007, 126, 691–699. [Google Scholar] [CrossRef]
- Sajini, T.; Mathew, B. A Brief Overview of Molecularly Imprinted Polymers: Highlighting Computational Design, Nano and Photo-Responsive Imprinting. Talanta Open 2021, 4, 100072. [Google Scholar] [CrossRef]
- Jenik, M.; Schirhagl, R.; Schirk, C.; Hayden, O.; Lieberzeit, P.; Blaas, D.; Paul, G.; Dickert, F. L. Sensing Picornaviruses Using Molecular Imprinting Techniques on a Quartz Crystal Microbalance. Anal. Chem. 2009, 81, 5320–5326. [Google Scholar] [CrossRef]
- Tai, D.-F.; Lin, C.-Y.; Wu, T.-Z.; Chen, L.-K. Recognition of Dengue Virus Protein Using Epitope-Mediated Molecularly Imprinted Film. Anal. Chem. 2005, 77, 5140–5143. [Google Scholar] [CrossRef] [PubMed]
- Shen, H.; Zhou, T.; Hu, J. A High-Throughput QCM Chip Configuration for the Study of Living Cells and Cell-Drug Interactions. Anal Bioanal Chem 2017, 409, 6463–6473. [Google Scholar] [CrossRef]
- Su, R.; Wang, F.; McAlpine, M. C. 3D Printed Microfluidics: Advances in Strategies, Integration, and Applications. Lab Chip 2023, 23, 1279–1299. [Google Scholar] [CrossRef]
- Three-Dimensional Direct Laser Writing of PEGda Hydrogel Microstructures with Low Threshold Power using a Green Laser Beam. https://www.light-am.com/en/article/doi/10.37188/lam.2021.003 (accessed 2025-04-22).
- Jin, Y.; Xiong, P.; Xu, T.; Wang, J. Time-Efficient Fabrication Method for 3D-Printed Microfluidic Devices. Sci Rep 2022, 12, 1233. [Google Scholar] [CrossRef]
- Guttridge, C.; Shannon, A.; O’Sullivan, A.; O’Sullivan, K. J.; O’Sullivan, L. W. Biocompatible 3D Printing Resins for Medical Applications: A Review of Marketed Intended Use, Biocompatibility Certification, and Post-Processing Guidance. Annals of 3D Printed Medicine 2022, 5, 100044. [Google Scholar] [CrossRef]
- Poskus, M. D.; Wang, T.; Deng, Y.; Borcherding, S.; Atkinson, J.; Zervantonakis, I. K. Fabrication of 3D-Printed Molds for Polydimethylsiloxane-Based Microfluidic Devices Using a Liquid Crystal Display-Based Vat Photopolymerization Process: Printing Quality, Drug Response and 3D Invasion Cell Culture Assays. Microsyst Nanoeng 2023, 9, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Vaidya, N.; Solgaard, O. 3D Printed Optics with Nanometer Scale Surface Roughness. Microsyst Nanoeng 2018, 4, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Shanmugam, A.; Usmani, M.; Mayberry, A.; Perkins, D. L.; Holcomb, D. E. Imaging Systems and Algorithms to Analyze Biological Samples in Real-Time Using Mobile Phone Microscopy. PLOS ONE 2018, 13, e0193797. [Google Scholar] [CrossRef]
- Ali, M. A.; Zhang, G. F.; Hu, C.; Yuan, B.; Jahan, S.; Kitsios, G. D.; Morris, A.; Gao, S.-J.; Panat, R. Ultrarapid and Ultrasensitive Detection of SARS-CoV-2 Antibodies in COVID-19 Patients via a 3D-printed Nanomaterial-based Biosensing Platform. [CrossRef]
- Sharma, P.; Hasan, Mohd. R.; Yardim, A.; Celik, E. G.; Timur, S.; Abdin, M. Z.; Narang, J. Next-Generation Point-of-Care Diagnostics: Silver Nanoparticle-Enhanced 3D-Printed Multiplex Electrochemical Biosensor for Detecting Dengue and Chikungunya Viruses. ACS Appl. Bio Mater. 2025, 8, 1251–1260. [CrossRef]
- Krejcova, L.; Nejdl, L.; Rodrigo, M. A. M.; Zurek, M.; Matousek, M.; Hynek, D.; Zitka, O.; Kopel, P.; Adam, V.; Kizek, R. 3D Printed Chip for Electrochemical Detection of Influenza Virus Labeled with CdS Quantum Dots. Biosens Bioelectron 2014, 54, 421–427. [Google Scholar] [CrossRef]
- Karamzadeh, V.; Sohrabi-Kashani, A.; Shen, M.; Juncker, D. Digital Manufacturing of Functional Ready-to-Use Microfluidic Systems. Advanced Materials 2023, 35, 2303867. [Google Scholar] [CrossRef]
- Armijo, P. R.; Markin, N. W.; Nguyen, S.; Ho, D. H.; Horseman, T. S.; Lisco, S. J.; Schiller, A. M. 3D Printing of Face Shields to Meet the Immediate Need for PPE in an Anesthesiology Department during the COVID-19 Pandemic. Am J Infect Control 2021, 49, 302–308. [Google Scholar] [CrossRef]
- Prototyping Rapid Diagnostics for COVID-19 With 3D Printing. Formlabs. https://formlabs.com/covid-19-response/covid-19-rapid-diagnostics/?srsltid=AfmBOoq2JMJEfdWqop-UvUqu4hrgqFwz8Ngiu-GrmlGGl162dFemATCz (accessed 2025-04-23).
- Ford, J.; Goldstein, T.; Trahan, S.; Neuwirth, A.; Tatoris, K.; Decker, S. A 3D-Printed Nasopharyngeal Swab for COVID-19 Diagnostic Testing. 3D Printing in Medicine 2020, 6, 21. [Google Scholar] [CrossRef]
- Goswami, M.; Yadav, A. K.; Chauhan, V.; Singh, N.; Kumar, S.; Das, A.; Yadav, V.; Mandal, A.; Tiwari, J. K.; Siddiqui, H.; Ashiq, M.; Sathish, N.; Kumar, S.; Biswas, D.; Srivastava, A. K. Facile Development of Graphene-Based Air Filters Mounted on a 3D Printed Mask for COVID-19. Journal of Science: Advanced Materials and Devices 2021, 6, 407–414. [Google Scholar] [CrossRef]
- Naz, S. A.; Huynh, V. T.; Doeven, E. H.; Adams, S.; Kouzani, A.; Guijt, R. M. Closed-Loop Control Systems for Pumps Used in Portable Analytical Systems. Journal of Chromatography A 2023, 1695, 463931. [Google Scholar] [CrossRef] [PubMed]
- Moya Muñoz, G. G.; Brix, O.; Klocke, P.; Harris, P. D.; Luna Piedra, J. R.; Wendler, N. D.; Lerner, E.; Zijlstra, N.; Cordes, T. Single-Molecule Detection and Super-Resolution Imaging with a Portable and Adaptable 3D-Printed Microscopy Platform (Brick-MIC). Science Advances 2024, 10, eado3427. [Google Scholar] [CrossRef]
- Mendoza-Gallegos, R. A.; Rios, A.; Garcia-Cordero, J. L. An Affordable and Portable Thermocycler for Real-Time PCR Made of 3D-Printed Parts and Off-the-Shelf Electronics. Anal. Chem. 2018, 90, 5563–5568. [Google Scholar] [CrossRef]
- Sheu, S. C.; Kijamnajsuk, P.; Chan, C. K.; Chen, J. J. A 3D-Printed Oscillatory Polymerase Chain Reaction System Using a Single Heater. Applied Thermal Engineering 2024, 239, 122201. [Google Scholar] [CrossRef]
- Torres Fredes, I. P.; Cortés-Adasme, E. N.; Barrientos, B. A.; Real, J. P.; Gomez, C. G.; Palma, S. D.; Kogan, M. J.; Real, D. A. 3D-Printed Plasmonic Nanocomposites: VAT Photopolymerization for Photothermal-Controlled Drug Release. Pharmaceuticals 2024, 17, 1453. [Google Scholar] [CrossRef] [PubMed]
- Horst, R. J.; Katzourakis, A.; Mei, B. T.; de Beer, S. Design and Validation of a Low-Cost Open-Source Impedance Based Quartz Crystal Microbalance for Electrochemical Research. HardwareX 2022, 12, e00374. [Google Scholar] [CrossRef] [PubMed]
- Glasco, D. L.; Elhassan, M. M.; McLeod, W. T.; Bell, J. G. Nonenzymatic Detection of Glucose Using 3D Printed Carbon Electrodes in Human Saliva. ECS Sens. Plus 2024, 3, 020602. [Google Scholar] [CrossRef]
- Lee, J. W.; Sim, S. J.; Cho, S. M.; Lee, J. Characterization of a Self-Assembled Monolayer of Thiol on a Gold Surface and the Fabrication of a Biosensor Chip Based on Surface Plasmon Resonance for Detecting Anti-GAD Antibody. Biosensors and Bioelectronics 2005, 20, 1422–1427. [Google Scholar] [CrossRef]
- Nakamoto, K.; Kurita, R.; Niwa, O.; Fujii, T.; Nishida, M. Development of a Mass-Producible on-Chip Plasmonic Nanohole Array Biosensor. Nanoscale 2011, 3, 5067–5075. [Google Scholar] [CrossRef]
- Wang, Z.; Wilkop, T.; Han, J. H.; Dong, Y.; Linman, M. J.; Cheng, Q. Development of Air-Stable, Supported Membrane Arrays with Photolithography for Study of Phosphoinositide−Protein Interactions Using Surface Plasmon Resonance Imaging. Anal. Chem. 2008, 80, 6397–6404. [Google Scholar] [CrossRef]
- Liu, Y.; Zhang, X. Microfluidics-Based Plasmonic Biosensing System Based on Patterned Plasmonic Nanostructure Arrays. Micromachines 2021, 12, 826. [Google Scholar] [CrossRef] [PubMed]
- Sun, S.; Zhao, Y.; Hao, Y.; Xue, P.; Guo, X.; Zhang, W.; Zhang, C.; Zhang, Q.; Zhou, W.; Ong, H. C.; Yu, X.; Li, Z.; Li, J.; Yao, J. Rapid, Sensitive and Multiplexed Detection of SARS-CoV-2 Viral Nucleic Acids Enabled by Phase-Based Surface Plasmon Resonance of Metallic Gratings. Biomed Opt Express 2024, 15, 5215–5226. [Google Scholar] [CrossRef]
- Pardee, K.; Green, A. A.; Takahashi, M. K.; Braff, D.; Lambert, G.; Lee, J. W.; Ferrante, T.; Ma, D.; Donghia, N.; Fan, M.; Daringer, N. M.; Bosch, I.; Dudley, D. M.; O’Connor, D. H.; Gehrke, L.; Collins, J. J. Rapid, Low-Cost Detection of Zika Virus Using Programmable Biomolecular Components. Cell 2016, 165, 1255–1266. [Google Scholar] [CrossRef] [PubMed]
- Crapnell, R. D.; Banks, C. E. Electroanalytical Overview: Screen-Printed Electrochemical Sensing Platforms. ChemElectroChem 2024, 11, e202400370. [Google Scholar] [CrossRef]
- Inam, A. K. M. S.; Costa Angeli, M. A.; Shkodra, B.; Douaki, A.; Avancini, E.; Magagnin, L.; Petti, L.; Lugli, P. Flexible Screen-Printed Electrochemical Sensors Functionalized with Electrodeposited Copper for Nitrate Detection in Water. ACS Omega 2021, 6, 33523–33532. [Google Scholar] [CrossRef]
- He, P.; Cao, J.; Ding, H.; Liu, C.; Neilson, J.; Li, Z.; Kinloch, I. A.; Derby, B. Screen-Printing of a Highly Conductive Graphene Ink for Flexible Printed Electronics. ACS Appl. Mater. Interfaces 2019, 11, 32225–32234. [Google Scholar] [CrossRef]
- Wu, K.; Kim, K.-W.; Kwon, J. H.; Kim, J. K.; Kim, S. H.; Moon, H. C. Direct Ink Writing of PEDOT:PSS Inks for Flexible Micro-Supercapacitors. Journal of Industrial and Engineering Chemistry 2023, 123, 272–277. [Google Scholar] [CrossRef]
- Fernandes, I. J.; Aroche, A. F.; Schuck, A.; Lamberty, P.; Peter, C. R.; Hasenkamp, W.; Rocha, T. L. A. C. Silver Nanoparticle Conductive Inks: Synthesis, Characterization, and Fabrication of Inkjet-Printed Flexible Electrodes. Sci Rep 2020, 10, 8878. [Google Scholar] [CrossRef] [PubMed]
- Sher, M.; Faheem, A.; Asghar, W.; Cinti, S. Nano-Engineered Screen-Printed Electrodes: A Dynamic Tool for Detection of Viruses. TrAC Trends in Analytical Chemistry 2021, 143, 116374. [Google Scholar] [CrossRef]
- Sestaioni, D.; Giurlani, W.; Ciacci, G.; Camagni, V.; Palladino, P.; Barucci, A.; Scarano, S. Sustainable and Effective Reconditioning of SPR Gold Chips Functionalized with Molecularly Imprinted Polynorepinephrine. Analytica Chimica Acta 2024, 1321, 343037. [Google Scholar] [CrossRef]
- Kimple, A. J.; Muller, R. E.; Siderovski, D. P.; Willard, F. S. A Capture Coupling Method for the Covalent Immobilization of Hexahistidine Tagged Proteins for Surface Plasmon Resonance. Methods Mol Biol 2010, 627, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Auer, S.; Azizi, L.; Faschinger, F.; Blazevic, V.; Vesikari, T.; Gruber, H. J.; Hytönen, V. P. Stable Immobilisation of His-Tagged Proteins on BLI Biosensor Surface Using Cobalt. Sensors and Actuators B: Chemical 2017, 243, 104–113. [Google Scholar] [CrossRef]
- Mantena, S.; Pillai, P. P.; Petros, B. A.; Welch, N. L.; Myhrvold, C.; Sabeti, P. C.; Metsky, H. C. Model-Directed Generation of Artificial CRISPR–Cas13a Guide RNA Sequences Improves Nucleic Acid Detection. Nat Biotechnol 2024, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Khan, S.; Singh, Y. V.; Singh, P.; Singh, R. S. An Optimized Artificial Intelligence System Using IoT Biosensors Networking for Healthcare Problems. Computational Intelligence and Neuroscience 2022, 2022, 2206573. [Google Scholar] [CrossRef]
- Padhi, A.; Agarwal, A.; Saxena, S. K.; Katoch, C. D. S. Transforming Clinical Virology with AI, Machine Learning and Deep Learning: A Comprehensive Review and Outlook. Virusdisease 2023, 34, 345–355. [Google Scholar] [CrossRef]
- Ginsberg, J.; Mohebbi, M. H.; Patel, R. S.; Brammer, L.; Smolinski, M. S.; Brilliant, L. Detecting Influenza Epidemics Using Search Engine Query Data. Nature 2009, 457, 1012–1014. [Google Scholar] [CrossRef]
- Sun, Y.; Sheng, D.; Zhou, Z.; Wu, Y. AI Hallucination: Towards a Comprehensive Classification of Distorted Information in Artificial Intelligence-Generated Content. Humanit Soc Sci Commun 2024, 11, 1–14. [Google Scholar] [CrossRef]
- Zens, M.; Brammertz, A.; Herpich, J.; Südkamp, N.; Hinterseer, M. App-Based Tracking of Self-Reported COVID-19 Symptoms: Analysis of Questionnaire Data. Journal of Medical Internet Research 2020, 22, e21956. [Google Scholar] [CrossRef]
- Çelik Ertuğrul, D.; Çelik Ulusoy, D. A Knowledge-Based Self-Pre-Diagnosis System to Predict Covid-19 in Smartphone Users Using Personal Data and Observed Symptoms. Expert Syst 2022, 39, e12716. [Google Scholar] [CrossRef]
- Aborode, A. T.; Adesola, R. O.; Scott, G. Y.; Arthur-Hayford, E.; Otorkpa, O. J.; Kwaku, S. D.; Elebesunu, E. E.; Nibokun, E. O.; Aruorivwooghene, I. J.; Bakre, A. A.; Ogundijo, O. A.; Banwo, O. G.; Ige, O.; Adelakun, I. O.; Onifade, I. A.; Ogungbemi, S. E.; Dosunmu, B. T.; Ayando, O. D.; Idowu, N.; Adegoye, G. A.; Jimoh, O. O. Bringing Lab to the Field: Exploring Innovations in Point-of-Care Diagnostics for the Rapid Detection and Management of Tropical Diseases in Resource-Limited Settings. Advances in Biomarker Sciences and Technology 2025, 7, 28–43. [Google Scholar] [CrossRef]
- Chen, H.-C. A Systematic Review of the Barcoding Strategy That Contributes to COVID-19 Diagnostics at a Population Level. Front Mol Biosci 2023, 10, 1141534. [Google Scholar] [CrossRef] [PubMed]
- Farrell, L. Automated Digital Notification of COVID-19 Diagnoses Through Text and Email Messaging — North Carolina, December 2020–January 2021. MMWR Morb Mortal Wkly Rep 2021, 70. [Google Scholar] [CrossRef]
- Song, J.; Pandian, V.; Mauk, M. G.; Bau, H. H.; Cherry, S.; Tisi, L. C.; Liu, C. Smartphone-Based Mobile Detection Platform for Molecular Diagnostics and Spatiotemporal Disease Mapping. Anal Chem 2018, 90, 4823–4831. [Google Scholar] [CrossRef]
- Ding, X.; Yin, K.; Li, Z.; Lalla, R. V.; Ballesteros, E.; Sfeir, M. M.; Liu, C. Ultrasensitive and Visual Detection of SARS-CoV-2 Using All-in-One Dual CRISPR-Cas12a Assay. Nat Commun 2020, 11, 4711. [Google Scholar] [CrossRef] [PubMed]
- Martín-Sierra, C.; Chavez, M. T.; Escobedo, P.; García-Cabrera, V.; López-Delgado, F. J.; Guardia-Monteagudo, J. J.; Ruiz-García, I.; Erenas, M. M.; Sanchez-Martin, R. M.; Capitán-Vallvey, L. F.; Palma, A. J.; Pernagallo, S.; Diaz-Mochon, J. J. SARS-CoV-2 Viral RNA Detection Using the Novel CoVradar Device Associated with the CoVreader Smartphone App. Biosensors and Bioelectronics 2023, 230, 115268. [Google Scholar] [CrossRef] [PubMed]
- Peters, H. P. Gap between Science and Media Revisited: Scientists as Public Communicators. Proc Natl Acad Sci U S A 2013, 110 (Suppl 3), 14102–14109. [Google Scholar] [CrossRef]
- Dankel, M.; Lambert, M. Abstracts for a Wider Audience: Promoting Linguistic Diversity in JBI Evidence Synthesis. JBI Evidence Synthesis 2023, 21, 833. [Google Scholar] [CrossRef]
- How to make your research accessible. Author Services. https://authorservices.taylorandfrancis.com/publishing-your-research/writing-your-paper/how-to-make-your-research-accessible/ (accessed 2025-04-23).
- Stack Whitney, K.; Perrone, J.; Bahlai, C. A. Open Access Journals Lack Image Accessibility Guidelines. Quantitative Science Studies 2025, 6, 46–62. [Google Scholar] [CrossRef]
- Shailes, S. Plain-Language Summaries of Research: Something for Everyone. eLife 2017, 6, e25411. [Google Scholar] [CrossRef]
- Sedgwick, C.; Belmonte, L.; Margolis, A.; Shafer, P. O.; Pitterle, J.; Gidal, B. E. Extending the Reach of Science – Talk in Plain Language. Epilepsy Behav Rep 2021, 16, 100493. [Google Scholar] [CrossRef]
- Viruses: Instructions for Authors. https://www.mdpi.com/journal/viruses/instructions (accessed 2025-04-23).
- Highlights of journal articles | Elsevier. www.elsevier.com. https://www.elsevier.com/researcher/author/tools-and-resources/highlights (accessed 2025-04-23).
- Bredbenner, K.; Simon, S. M. Video Abstracts and Plain Language Summaries Are More Effective than Graphical Abstracts and Published Abstracts. PLOS ONE 2019, 14, e0224697. [Google Scholar] [CrossRef] [PubMed]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



