Submitted:
04 February 2026
Posted:
05 February 2026
You are already at the latest version
Abstract
Background: Radiologically isolated syndrome (RIS) is defined by MRI findings suggestive of multiple sclerosis (MS) in the absence of prior clinical demyelinating events. We aimed to compare health-related quality of life (HRQoL) between RIS and relapsing–remitting MS (RRMS) after adjusting for fatigue, cognition, and psychological distress, and to contextualize generic HRQoL relative to healthy controls. Methods: Data from 30 RIS, 29 RRMS, and 30 healthy controls were analyzed. MS-specific HRQoL (patients only) was assessed with the Functional Assessment of Multiple Sclerosis (FAMS), and generic HRQoL (all participants) was assessed with the EuroQol-5D (EQ-5D) visual analogue scale and utility index. Multivariable linear regression with robust (HC3) standard errors adjusted for demographics, fatigue impact, cognitive performance, and psychological distress. Results: FAMS totals were similar in RIS vs RRMS (median 167.50 vs 164.0; p=0.694) and remained non-different after adjustment (β=−2.37, 95% CI −10.18 to 5.44; p=0.544). EQ-5D outcomes showed an unadjusted gradient across groups, but adjusted differences relative to RIS were not statistically significant. Greater fatigue impact was associated with poorer HRQoL across all models (all p < 0.001). Psychological distress was associated with lower FAMS (β = -14.53; p < 0.001) but not with EQ-5D outcomes. Conclusion: HRQoL in RIS was comparable to RRMS; fatigue impact was the most consistent correlate of poorer HRQoL.
Keywords:
radiologically isolated syndrome
; multiple sclerosis
; quality of life
; fatigue
; EuroQol
; FAMS
Introduction
Radiologically isolated syndrome (RIS) describes individuals with incidental magnetic resonance imaging (MRI) abnormalities typical of multiple sclerosis (MS) in the absence of prior clinical demyelinating events,[1] Since its original description, RIS has been viewed as the earliest point on the MS spectrum and has raised practical questions regarding prognosis, monitoring, and the appropriateness and timing of disease-modifying therapy (DMT).[2,3,4,5]
Large observational cohorts show that a substantial proportion of patients with RIS develop a first clinical event or meet MS diagnostic criteria over time, with risk influenced by age, sex, spinal cord or infratentorial lesions, and cerebrospinal fluid oligoclonal bands.[4,6,7,8] Proposed revisions to RIS criteria seek to improve specificity and better align RIS with contemporary MS imaging concepts.[9] At the same time, randomized trials of early treatment in RIS (e.g., teriflunomide) have further intensified debate about whether RIS should be managed as a preclinical stage of MS.[10]
Beyond clinical conversion, the patient-reported burden of RIS may be clinically meaningful. RIS is often identified during evaluation for headaches or nonspecific symptoms, and disclosure of an uncertain, potentially progressive diagnosis may affect psychological well-being.[5] Subclinical inflammatory and neurodegenerative processes may also contribute to fatigue, cognitive dysfunction, and emotional symptoms—key determinants of health-related quality of life (HRQoL) in MS.[11,12,13,14,15,16]
Although HRQoL data in RIS remain limited, available evidence suggests a non-trivial impact. In a longitudinal cohort of non-converting RIS, Lebrun et al [17] reported HRQoL at diagnosis comparable to controls, but fatigue was already present, and mental HRQoL declined over follow-up, Labiano-Fontcuberta et al.[14] described frequent clinically significant depression, greater somatic symptom burden, and worse generic HRQoL (EuroQol 5-Dimension questionnaire [EQ-5D]) in RIS versus controls, with strong links between depressive symptoms, fatigue, and HRQoL. Socio-emotional factors may contribute, as noted by Joly et al.[16], who found that pathological alexithymia in approximately one-third of RIS participants was associated with depression, cognitive fatigue, and poorer mental quality of life. Consistent with these reports, large cohort data show higher depression/anxiety symptom burden and worse generic HRQoL in combined RIS/MS groups compared with healthy controls, and minimal differences between RIS and early relapsing–remitting MS (RRMS) on mood and HRQoL measures. [18]
Prior studies have used heterogeneous HRQoL instruments and have often relied on unadjusted comparisons or bivariate associations rather than integrated multivariable models that account simultaneously for fatigue, mood, cognition, and personality-related factors.[14,16,17,18] Thus, despite growing evidence that RIS is not uniformly benign, comprehensive analyses directly contrasting RIS with RRMS while jointly modeling major determinants of HRQoL remain scarce.
The primary aim of this study was to test whether HRQoL in RIS is comparable to HRQoL in RRMS after adjustment for demographics (age, sex, and education), fatigue impact (Daily Fatigue Impact Scale for Daily Use; D-FIS), cognitive performance, and psychological distress. As a secondary aim, we contextualized generic HRQoL in RIS and RRMS against a healthy control group.
HRQoL is increasingly recognized as a core outcome in MS research and clinical practice, complementing traditional measures such as relapse rate and disability.[11,13] Patient-reported outcomes capture fatigue, pain, mood, cognition, and social participation—domains that may not be fully reflected by neurological examination—and fatigue and depression are consistently among the strongest predictors of poor HRQoL, often exceeding the influence of physical disability in early disease.[11,13] Defining HRQoL in RIS therefore has practical implications for counseling, identifying modifiable targets (notably fatigue and psychological distress), and informing RIS trials that incorporate patient-centered endpoints.
Methods
Standard Protocol Approvals, Registrations, and Patient Consents
All participants provided written informed consent, and the study was approved by the ethics committee of 12 de Octubre University Hospital (Madrid, Spain).
Participants
Consecutive participants were recruited from MS units in Madrid, Spain. RIS was defined as MRI anomalies highly suggestive of demyelination in individuals without prior clinical demyelinating events, according to the criteria in use at the time the cohort was initiated. [1] In 53.3% of RIS cases, the index MRI was obtained for headache. MS participants met the 2017 McDonald criteria.[19] Healthy controls were recruited from the community and hospital environment and had no history of neurological disease.
Key exclusion criteria for RIS and MS included substance abuse, major acute comorbidities, or serious chronic illness (stable chronic conditions were permitted). Healthy controls and MS participants were group-matched to the RIS group by age, sex, and years of education; the same exclusion criteria were applied to healthy controls. All participants underwent baseline clinical evaluation and completed patient-reported outcomes and neuropsychological testing; only baseline data were analyzed.
Clinical and Demographic Variables
Age, sex, and years of formal education were recorded. Disability in RRMS was assessed using the Expanded Disability Status Scale (EDSS).[20]
Health-Related Quality of Life
MS-specific HRQoL was assessed in RIS and RRMS using the Spanish version of the Functional Assessment of Multiple Sclerosis (FAMS) questionnaire.[21,22,23,24] Items are rated on a 5-point Likert scale (0–4). The Spanish FAMS includes 52 items covering six core domains—Mobility (0–28), Symptoms (0–56), Emotional Well-Being (0–32), General Contentment (0–28), Thinking/Fatigue (0–36), and Family/Social Well-Being (0–28)—plus an Additional Concerns subscale (0–28).[21,22,23,24] The Spanish FAMS has demonstrated high internal consistency across subscales and for the total score (α = 0.78–0.96). [21,25] Higher scores indicate better HRQoL.[21,22,23,24] The FAMS total score was computed as the sum of the six core domains (excluding Additional Concerns).
Generic HRQoL was assessed in all participants with the EQ-5D descriptive system and visual analogue scale (VAS).[26] The EQ-5D assesses mobility, self-care, usual activities, pain/discomfort, and anxiety/depression, which are combined into a utility index (1.0 indicates full health).[26] The EQ-5D VAS ranges from 0 (worst imaginable health) to 100 (best imaginable health).[26]
Fatigue, Mood, and Personality/Psychological Variables
Fatigue impact was assessed using the D-FIS, an eight-item instrument designed to quantify the daily impact of fatigue in MS (Benito-León et al., 2007). Total scores range from 0 to 32, with higher scores indicating greater fatigue impact.
Neuropsychological Assessment
Cognition was assessed using the Brief Repeatable Battery of Neuropsychological Tests (BRB-N).[30] Verbal learning and memory were evaluated with the Selective Reminding Test (SRT).[31,32,33] Visuospatial learning and delayed recall were assessed with the 10/36 Spatial Recall Test (SPART).[31,33] Attention and processing speed were assessed using the Symbol Digit Modalities Test (SDMT) and the Paced Auditory Serial Addition Test (PASAT).[30] Phonemic verbal fluency was assessed using the Word List Generation (WLG) test. [33] Executive functioning was further assessed using the Stroop Color-Word Test [34,35] and the Controlled Oral Word Association Test (FAS).[36]
Statistical Analyses
Analyses were performed using Python (version 3.11) with the pandas, statsmodels, and scikit-learn libraries. Continuous variables are presented as mean ± SD when approximately symmetric and as median [Q1–Q3] when skewed or bounded; categorical variables are summarized as n (%). Missing data were handled using complete-case analysis within each model.
-Unadjusted group comparisons
Between-group comparisons across RIS, RRMS, and healthy controls were performed using one-way analysis of variance (ANOVA) for approximately normally distributed continuous variables, Kruskal–Wallis tests for non-normally distributed variables, and χ2 tests for categorical variables. Patient-only comparisons (RIS vs. RRMS) used Mann–Whitney U tests for non-normally distributed outcomes. Because several EQ-5D dimension cross-tabulations had expected cell counts <5, EQ-5D dimensions were compared using Fisher–Freeman–Halton exact tests after dichotomization (no problems vs. any problems).
Unadjusted HRQoL analyses were conducted separately for MS-specific and generic instruments. FAMS outcomes (RIS and RRMS only) and EQ-5D outcomes (all participants) are reported as median [Q1–Q3] and compared using the Mann–Whitney U test and the Kruskal–Wallis test, respectively.
-Principal component analysis (PCA)
To reduce dimensionality and limit multicollinearity among correlated predictors, PCA was performed separately for cognitive and psychological variables using the correlation matrix. The number of retained components was determined based on scree plots, eigenvalues, and interpretability. Component scores were derived using regression, standardized to z-scores (mean 0, SD 1), and scaled for interpretability.
The cognitive PCA included all neuropsychological measures administered: verbal learning and memory (SRT), visuospatial learning and delayed recall (10/36 SPART), attention and processing speed (SDMT and PASAT), phonemic verbal fluency (WLG and FAS), and executive functioning/inhibitory control (Stroop Color and Word Test). Higher scores indicate better cognitive performance.
The psychological PCA included depressive symptoms (BDI-II), state anxiety (STAI), and selected PAI scales (Somatic Complaints, Anxiety, Anxiety-Related Disorders, Depression, Stress, and Suicidal Ideation). The first component was retained and interpreted as psychological distress, with higher scores indicating greater distress.
- Multivariable regression models
Separate ordinary least squares (OLS) linear regression models were fitted for each HRQoL outcome: (i) FAMS total score (RIS+RRMS), (ii) EQ-5D visual analogue scale (RIS+RRMS+healthy controls), and (iii) EQ-5D utility index (RIS+RRMS+healthy controls). The diagnostic group was modeled using indicator variables, with RIS as the reference category. All models were adjusted for age, sex (female as the reference group), years of education, fatigue impact (Daily Fatigue Impact Scale), cognitive performance (z-score), and psychological distress (z-score).
Model diagnostics included visual inspection of residual and Q–Q plots. Inference was based on heteroskedasticity-consistent (HC3) robust standard errors, with results reported as β coefficients, 95% confidence intervals, and two-sided p-values. Multicollinearity was assessed using variance inflation factors (VIF), and model fit was summarized using R2. Statistical significance was defined as p < 0.05.
Results
The sample comprised 89 participants: 30 with RIS, 29 with RRMS, and 30 healthy controls (Table 1). Groups were comparable in age, sex distribution, and education (all p > 0.05). Disability in RRMS was low (EDSS 2.0 [1.0, 3.0]). Fatigue impact (D-FIS) showed a borderline difference across groups (p=0.051), whereas cognitive performance and psychological distress differed significantly (p=0.013 and p=0.014, respectively). Full characteristics are shown in Table 1.
FAMS total scores were similar in RIS and RRMS (167.5 [135.2–185.0] vs. 164.0 [136.2–181.0]; p=0.694), with no significant differences across domains or the Additional Concerns subscale (all p>0.05), although Family/Social Well-Being showed a non-significant trend (p=0.093) (Table 2; Figure 1A).
Panel A shows MS-specific HRQoL, measured with the Functional Assessment of Multiple Sclerosis (FAMS) total score (six domains) and subscales, in radiologically isolated syndrome (RIS) and relapsing–remitting multiple sclerosis (RRMS). Panel B shows generic HRQoL measured with the EuroQol-5D (EQ-5D) utility index and EQ-5D visual analogue scale (VAS) in RIS, RRMS, and healthy controls (HC). For each outcome, points represent the median, and vertical bars represent the interquartile range (Q1–Q3). P values correspond to Mann–Whitney U tests for FAMS comparisons (RIS vs. RRMS) and Kruskal–Wallis tests for EQ-5D comparisons (three-group). Higher values indicate better HRQoL for all outcomes.
EQ-5D VAS and utility index showed a descriptive gradient (lowest in RIS, highest in controls) without statistically significant overall differences (VAS p=0.058; utility p=0.087) (Table 2; Figure 1B).
Anxiety/depression and pain/discomfort were the most frequently affected dimensions, particularly in RIS. Any anxiety/depression was reported by 37.0% of RIS, 18.5% of RRMS, and 6.7% of controls (p=0.017), whereas pain/discomfort did not differ significantly (p=0.580). Other dimensions were infrequently endorsed and did not differ between groups (mobility: p=0.733; self-care: p=0.535; usual activities: p=0.088).
After adjustment, RRMS did not differ from RIS (β=−2.37, 95% CI −10.18 to 5.44; p=0.544). Higher fatigue impact (β=−2.04 per D-FIS point; p<0.001) and greater psychological distress (β=−14.53 per SD; p<0.001) were independently associated with lower FAMS, and older age was also associated with lower FAMS (β=−0.60 per year; p=0.020). Cognitive performance and education were not independently associated, and sex showed a non-significant trend (p=0.091) (Table 3; Figure 2).
Forest plot of adjusted regression coefficients (β) with 95% confidence intervals for independent variables (left) in models of multiple sclerosis (MS)-specific HRQoL (FAMS total), EQ-5D VAS, and EQ-5D utility index. The vertical dashed line indicates no association (β=0). P values are shown to the right of each panel. Reference categories were radiologically isolated syndrome (RIS) for the diagnostic group and female for sex; cognitive performance and psychological distress were standardized component scores (z).
Adjusted group differences were not significant (RRMS vs. RIS p=0.787; controls vs. RIS p=0.719). Higher fatigue impact remained independently associated with lower VAS (β = -1.21 per D-FIS point; p < 0.001), whereas psychological distress and cognitive performance were not (Table 3; Figure 2).
Adjusted group differences were again non-significant (RRMS vs. RIS p=0.143; controls vs. RIS p=0.363). Fatigue impact was independently associated with a lower utility index (β = -0.011 per D-FIS point; p < 0.001), whereas psychological distress and cognitive performance were not (Table 3).
All inferences used HC3 robust standard errors. Model fit was high for FAMS (R2=0.867) and moderate for EQ-5D outcomes (VAS R2=0.491; utility R2=0.397). Multicollinearity was low (maximum VIF ≤2.13).
Discussion
In this cross-sectional baseline analysis, patients with RIS reported MS-specific HRQoL comparable to that of participants with RRMS even after adjustment for demographics, fatigue impact, cognitive performance, and psychological distress. Generic HRQoL, assessed with the EQ-5D, showed a descriptive gradient in unadjusted analyses (lowest in RIS and highest in healthy controls), but adjusted group differences were not statistically significant for either EQ-5D VAS or the EQ-5D utility index. Across outcomes, fatigue impact emerged as the most consistent independent correlate of worse HRQoL, whereas psychological distress was independently associated with MS-specific HRQoL (FAMS) but did not remain independently associated with EQ-5D outcomes in adjusted models.
The absence of significant differences between RIS and healthy controls on the generic EQ-5D likely reflects the limited sensitivity of generic HRQoL instruments to capture early, non-motor disease burden.[11,13] The EQ-5D places substantial weight on mobility, self-care, and usual activities—domains that were infrequently affected in RIS and showed no between-group differences—thereby constraining its ability to detect impairments driven primarily by fatigue and psychological distress.[11,13] In addition, the EQ-5D utility index is subject to a ceiling effect, as evidenced by the high proportion of maximum scores among healthy controls and RRMS participants, which further reduces discrimination at higher levels of perceived health. In contrast, MS-specific instruments such as the FAMS are designed to capture symptoms particularly relevant to demyelinating disease, including cognitive dysfunction, fatigue, and emotional well-being, and may therefore reveal clinically meaningful burden in RIS that is not reflected in generic measures.[21,22,23,24] Taken together, these considerations suggest that the apparent similarity between RIS and healthy controls on EQ-5D does not imply the absence of patient-reported burden in RIS, but rather highlights the importance of disease-specific tools for assessing HRQoL at early stages of the MS spectrum.
Our findings add to a growing body of evidence indicating that RIS can be associated with clinically relevant symptom burden and psychosocial impact.[14,16,17] Taken together, these data suggest that characterizing RIS as a “benign” incidental imaging finding may be misleading when patient-reported outcomes—particularly fatigue, mood symptoms, and HRQoL—are considered.
Notably, our MS-specific findings relied on the FAMS instrument. While FAMS has been validated in MS populations [21]–[23], it is not routinely used in RIS. Nevertheless, the overlap between RIS and RRMS scores on an MS-specific HRQoL measure is clinically meaningful. It indicates that patient-reported domains such as thinking/fatigue, symptoms, and emotional well-being may already be compromised in RIS, as reflected by their similarity to RRMS in this cohort. The absence of statistically significant differences between RIS and RRMS does not imply identical mechanisms; rather, it may reflect the low disability burden in the RRMS group (median EDSS 2.0 [1.0–3.0]) and the predominance of non-motor determinants—particularly fatigue impact (and psychological distress for MS-specific HRQoL)—in shaping perceived health status.
Several mechanisms may explain impaired or MS-like HRQoL in RIS. First, subclinical central nervous system demyelination and network dysfunction may contribute to fatigue, cognitive inefficiency, and mood symptoms even in the absence of focal neurological deficits.[37] Prior work has reported cognitive deficits in RIS compared with healthy controls and, in some settings, compared with clinically isolated syndrome, [15] supporting the notion of functional impact at this stage.[12] Second, the psychological impact of receiving an uncertain diagnosis and living with the risk of MS could directly reduce HRQoL, increase anxiety, and amplify symptom perception. Our models suggest that once fatigue impact and psychological distress are considered, the diagnostic group per se explains little additional variance in generic HRQoL.
The current findings have practical implications for clinical care and research. Clinicians should avoid assuming that RIS is asymptomatic or benign from the patient’s perspective and should proactively assess fatigue, mood symptoms, and psychosocial stressors. Fatigue and psychological distress are potentially modifiable through patient education, sleep optimization, management of comorbidities, structured exercise, and evidence-based psychological interventions.[38,39] Moreover, as treatment trials in RIS emerge, incorporation of patient-reported outcomes alongside conversion and MRI endpoints may help quantify benefits that matter to patients.
Our results also inform the broader debate regarding RIS management. While risk stratification for conversion remains central to decisions about monitoring and early disease-modifying therapy, [9,10] patient-reported burden may justify supportive interventions regardless of conversion risk and may influence shared decision-making about initiating therapy. Recent discussions and trials have moved RIS from an incidental imaging descriptor toward a potential preclinical phase of MS. [9,10] Patient-centered outcomes provide an additional dimension to this evolving framework.
Several research priorities follow. Longitudinal studies stratified by conversion status and established imaging or cerebrospinal fluid risk markers are needed to define HRQoL trajectories in RIS. Future cohorts should also integrate MRI measures of lesion burden and brain atrophy, together with biomarkers of neuroaxonal injury, to determine whether fatigue and psychological distress track biological disease activity. Interventional studies are warranted to test whether targeted non-pharmacological approaches (e.g., fatigue management, cognitive-behavioral therapy, exercise) improve HRQoL in RIS. As disease-modifying therapy trials advance, incorporating patient-reported outcomes may capture benefits or harms not reflected by conversion rates alone.[40]
Strengths of this study include the inclusion of three well-characterized groups, the use of both a disease-specific and a generic HRQoL measure, and the availability of detailed assessments of fatigue, neuropsychological functioning, and psychological functioning. To limit model complexity with a modest sample size, we reduced high-dimensional cognitive and psychological measures using principal component analysis and included prespecified covariates in multivariable models.
Several limitations should be acknowledged. First, the analysis is cross-sectional; causal interpretations and temporal sequencing (e.g., whether fatigue precedes HRQoL impairment) cannot be established. Second, the cohort was recruited from specialized centers and may not generalize to all patients with RIS. Third, FAMS has not been formally validated in RIS, and some degree of measurement non-equivalence is possible; future work could incorporate alternative MS-specific instruments and qualitative research.
In closing, in a baseline cohort spanning RIS, RRMS, and healthy controls, HRQoL in RIS was comparable to that in RRMS on an MS-specific measure and tended to be lower than that in healthy controls on generic EQ-5D measures. Fatigue was the most consistent independent correlate of poorer HRQoL across outcomes, whereas psychological distress was independently associated with MS-specific HRQoL. These findings suggest that RIS is not necessarily benign from the patient’s perspective and support routine screening and management of fatigue and psychological distress in patients with RIS.
Author Contributions
All authors meet the ICMJE criteria for authorship.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request and subject to approval by the local ethics committee. The data are not publicly available due to restrictions related to patient confidentiality and informed consent.
Acknowledgments
Julián Benito-León is supported by the National Institutes of Health (NINDS R01 NS39422 and R01 NS094607) and by Spain’s Ministry of Science and Innovation through the Recovery, Transformation, and Resilience Plan (grants TED2021-130174B-C33, NETremor, and PID2022-138585OB-C33, Resonate. Maria Díez-Cirarda is supported by the Instituto de Salud Carlos III (ISCIII) through the “Miguel Servet” program (Grant No. CP25/00085) and co-funded by the European Union. The Instituto de Salud Carlos III also supports Jordi A. Matias-Guiu through the projects INT20/00079 and INT23/00017 (co-funded by European Regional Development Fund “A way to make Europe”).
References
- Okuda, DT; Mowry, EM; Beheshtian, A. Incidental MRI anomalies suggestive of multiple sclerosis: the radiologically isolated syndrome. Neurology 2009. Available online: https://pubmed.ncbi.nlm.nih.gov/19073949/. [CrossRef]
- Bourdette, D; Simon, J. The radiologically isolated syndrome: is it very early multiple sclerosis? Neurology 2009. Available online: https://pubmed.ncbi.nlm.nih.gov/19073944/. [CrossRef] [PubMed]
- Granberg, T; Martola, J; Bergendal, G. Radiologically isolated syndrome—incidental MRI findings suggestive of multiple sclerosis: a systematic review. Multiple Sclerosis 2013. Available online: https://pubmed.ncbi.nlm.nih.gov/22760099/. [CrossRef] [PubMed]
- Okuda, DT; Siva, A; Kantarci, O; Inglese, M; Katz, I; Tutuncu, M. Radiologically isolated syndrome: 5-year risk for an initial clinical event. PLoS One 2014. Available online: https://pubmed.ncbi.nlm.nih.gov/24598783/. [CrossRef]
- Labiano-Fontcuberta, J. Benito-León, Radiologically isolated syndrome: An update on a rare entity. Mult Scler 2016. [Google Scholar] [CrossRef] [PubMed]
- Lebrun-Frenay; Kantarci, O.; Siva, A.; Sormani, M.P.; Pelletier, D.; Okuda, D.T. 10-year RISC study group on behalf of SFSEP, OFSEP. Radiologically Isolated Syndrome: 10-Year Risk Estimate of a Clinical Event. Ann Neurol 2020. [Google Scholar] [CrossRef]
- Kantarci, O; Lebrun-Frénay, C. Radiologically isolated syndrome: 10-year risk estimate of a clinical event. Annals of Neurology 2020. Available online: https://pubmed.ncbi.nlm.nih.gov/32500967/.
- Lebrun-Frénay, C; Rollot, F; Mondot, L. Risk factors and time to clinical symptoms of multiple sclerosis among patients with radiologically isolated syndrome. JAMA Network Open 2021. Available online: https://pubmed.ncbi.nlm.nih.gov/34698934/. [CrossRef]
- Lebrun-Frénay, C; Kantarci, O; Siva, A. The radiologically isolated syndrome: revised diagnostic criteria. The Lancet Neurology 2023. Available online: https://pubmed.ncbi.nlm.nih.gov/36864688/. [CrossRef]
- Lebrun-Frénay, C. Teriflunomide and time to clinical multiple sclerosis in radiologically isolated syndrome (TERIS). JAMA Neurology 2023. Available online: https://pubmed.ncbi.nlm.nih.gov/37466238/. [CrossRef]
- Benito-León, J.; Morales, J.M.; Rivera-Navarro, J.; Mitchell, A. A review about the impact of multiple sclerosis on health-related quality of life. Disabil Rehabil 2003, 25, 1291–1303. [Google Scholar] [CrossRef]
- Morales-Gonzáles, J.M.; Benito-León, J.; Rivera-Navarro, J.; Mitchell, A.J. GEDMA Study Group, A systematic approach to analyse health-related quality of life in multiple sclerosis: the GEDMA study. Mult Scler 2004, 10, 47–54. [Google Scholar] [CrossRef]
- Mitchell, A.J.; Benito-León, J.; González, J.-M.M.; Rivera-Navarro, J. Quality of life and its assessment in multiple sclerosis: integrating physical and psychological components of wellbeing. Lancet Neurol 2005, 4, 556–566. [Google Scholar] [CrossRef] [PubMed]
- Labiano-Fontcuberta; Aladro, Y.; Martínez-Ginés, M.L.; Ayuso, L.; Mitchell, A.J.; Puertas, V.; Cerezo, M.; Higueras, Y.; Benito-León, J. Psychiatric disturbances in radiologically isolated syndrome. J Psychiatr Res 2015. [Google Scholar] [CrossRef] [PubMed]
- Labiano-Fontcuberta, A. Cognitive deficits in radiologically isolated syndrome compared with multiple sclerosis and healthy controls. Multiple Sclerosis 2016. Available online: https://pubmed.ncbi.nlm.nih.gov/26084350/. [CrossRef] [PubMed]
- Joly J, Alexithymia and quality of life in radiologically isolated syndrome. Brain and Behavior 2024. Available online: https://pubmed.ncbi.nlm.nih.gov/39341200/.
- Lebrun, C. Evaluation of quality of life and fatigue in radiologically isolated syndrome. Revue Neurologique (Paris) 2016. Available online: https://pubmed.ncbi.nlm.nih.gov/27158044/. [CrossRef]
- Oh, J.; Arbour, N.; Giuliani, F.; Guenette, M.; Kolind, S.; Lynd, L.; Marrie, R.A.; Metz, L.M.; Prat, A.; Schabas, A.; Smyth, P.; Tam, R.; Traboulsee, A.; Yong, V.W.; Patten, S.B. The Canadian Prospective Cohort Study to understand progression in multiple sclerosis: baseline characteristics. Ther Adv Neurol Disord 2024, 17, 17562864241273045. [Google Scholar] [CrossRef]
- Thompson, AJ; Banwell, BL; Barkhof, F. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. The Lancet Neurology 2018. Available online: https://pubmed.ncbi.nlm.nih.gov/29275977/. [CrossRef]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale. Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef]
- Rivera-Navarro, J.; Benito-León, J.; Morales-González, J.M. Searching for more specific dimensions for the measurement of quality of life in multiple sclerosis. Rev Neurol 2001, 32, 705–713. [Google Scholar]
- Morales-Gonzáles, J.M.; Benito-León, J.; Rivera-Navarro, J.; Mitchell, A.J. GEDMA Study Group, A systematic approach to analyse health-related quality of life in multiple sclerosis: the GEDMA study. Mult Scler 2004, 10, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Benito-León, J.; Mitchell, A.J.; Rivera-Navarro, J.; Morales-González, J.M. Impaired health-related quality of life predicts progression of disability in multiple sclerosis. Euro J of Neurology 2013, 20, 79–86. [Google Scholar] [CrossRef]
- Labiano-Fontcuberta; Mitchell, A.J.; Moreno-García, S.; Puertas-Martín, V.; Benito-León, J. Impact of anger on the health-related quality of life of multiple sclerosis patients. Mult Scler 2015, 21, 630–641. [Google Scholar] [CrossRef] [PubMed]
- Cella, DF; Dineen, K; Arnason, B. Validation of the functional assessment of multiple sclerosis quality of life instrument. Neurology 1996. Available online: https://pubmed.ncbi.nlm.nih.gov/8710066/. [CrossRef] [PubMed]
- EuroQol - a new facility for the measurement of health-related quality of life. Health Policy 1990, 16, 199–208. [CrossRef]
- Beck, A.T.; Steer, R.A.; Brown, G. Beck Depression Inventory–II; 2011. [Google Scholar] [CrossRef]
- Spielberger, C.D.; Gonzalez-Reigosa, F.; Martinez-Urrutia, A.; Natalicio, L.F.; Natalicio, D.S. The State-Trait Anxiety Inventory. Revista Interamericana de Psicología/Interamerican Journal of Psychology 2017, 5. [Google Scholar] [CrossRef]
- Busse, M.; Whiteside, D.; Waters, D.; Hellings, J.; Ji, P. Exploring the reliability and component structure of the personality assessment inventory in a neuropsychological sample. Clin Neuropsychol 2014, 28, 237–251. [Google Scholar] [CrossRef]
- Rao, S.M. A manual for the brief repeatable battery of neuropsychological tests in multiple sclerosis; Medical College of Wisconsin: Milwaukee, 1990; p. 1696. [Google Scholar]
- Lebrun, C.; Blanc, F.; Brassat, D.; Zephir, H.; de Seze, J. behalf of CFSEP, Cognitive function in radiologically isolated syndrome. Mult Scler 2010, 16, 919–925. [Google Scholar] [CrossRef]
- Buschke, H.; Fuld, P.A. Evaluating storage, retention, and retrieval in disordered memory and learning. Neurology 1974, 24, 1019–1025. [Google Scholar] [CrossRef]
- Portaccio, E.; Goretti, B.; Zipoli, V.; Siracusa, G.; Sorbi, S.; Amato, M.P. A short version of Rao’s Brief Repeatable Battery as a screening tool for cognitive impairment in multiple sclerosis. The Clinical Neuropsychologist 2009, 23, 268–275. [Google Scholar] [CrossRef]
- Scarpina, F.; Tagini, S. The Stroop Color and Word Test. Front. Psychol. 2017, 8. [Google Scholar] [CrossRef] [PubMed]
- Peña-Casanova, J.; Casals-Coll, M.; Quintana, M.; Sánchez-Benavides, G.; Rognoni, T.; Calvo, L.; Palomo, R.; Aranciva, F.; Tamayo, F.; Manero, R.M. Estudios normativos españoles en población adulta joven (Proyecto NEURONORMA jóvenes): métodos y características de la muestra. Neurología 2012, 27, 253–260. [Google Scholar] [CrossRef]
- Bauer, K.; Malek-Ahmadi, M. Meta-analysis of Controlled Oral Word Association Test (COWAT) FAS performance in amnestic mild cognitive impairment and cognitively unimpaired older adults. Applied Neuropsychology: Adult 2021, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Benito-León, J.; Del Pino, A.B.; Aladro, Y.; Cuevas, C.; Domingo-Santos, Á.; Galán Sánchez-Seco, V.; Labiano-Fontcuberta, A.; Gómez-López, A.; Salgado-Cámara, P.; Costa-Frossard, L.; Monreal, E.; Sainz De La Maza, S.; Matías-Guiu, J.A.; Matías-Guiu, J.; Delgado-Álvarez, A.; Montero-Escribano, P.; Martínez-Ginés, M.L.; Higueras, Y.; Ayuso-Peralta, L.; Malpica, N.; Melero, H. Abnormal functional connectivity in radiologically isolated syndrome: A resting-state fMRI study. Mult Scler 2023, 29, 1393–1405. [Google Scholar] [CrossRef]
- Harrison, A.M.; Safari, R.; Mercer, T.; Picariello, F.; Van Der Linden, M.L.; White, C.; Moss-Morris, R.; Norton, S. Which exercise and behavioural interventions show most promise for treating fatigue in multiple sclerosis? A network meta-analysis. Mult Scler 2021, 27, 1657–1678. [Google Scholar] [CrossRef] [PubMed]
- Boda, M.R.; Rees, A.E.; Goldsworthy, M.R.; Evangelou, N.; Sidhu, S.K.; Smith, A.E. Scoping review: The effects of diet, physical activity and sleep on motor and physical fatigue in people with multiple sclerosis. Neuroscience 2025, 568, 166–194. [Google Scholar] [CrossRef]
- Cruz Rivera, S.; Buxhoeveden, S.; Aiyegbusi, O.L.; Bozinov, N.; Kamudoni, P.; McBurney, R.; Calvert, M. The importance of patient-reported outcomes: A call for their integration in the routine care of patients with multiple sclerosis. Mult Scler 2025, 31, 1518–1530. [Google Scholar] [CrossRef]
Figure 1.
Unadjusted health-related quality of life outcomes in radiologically isolated syndrome (RIS), relapsing–remitting multiple sclerosis (RRMS), and healthy controls.
Figure 1.
Unadjusted health-related quality of life outcomes in radiologically isolated syndrome (RIS), relapsing–remitting multiple sclerosis (RRMS), and healthy controls.
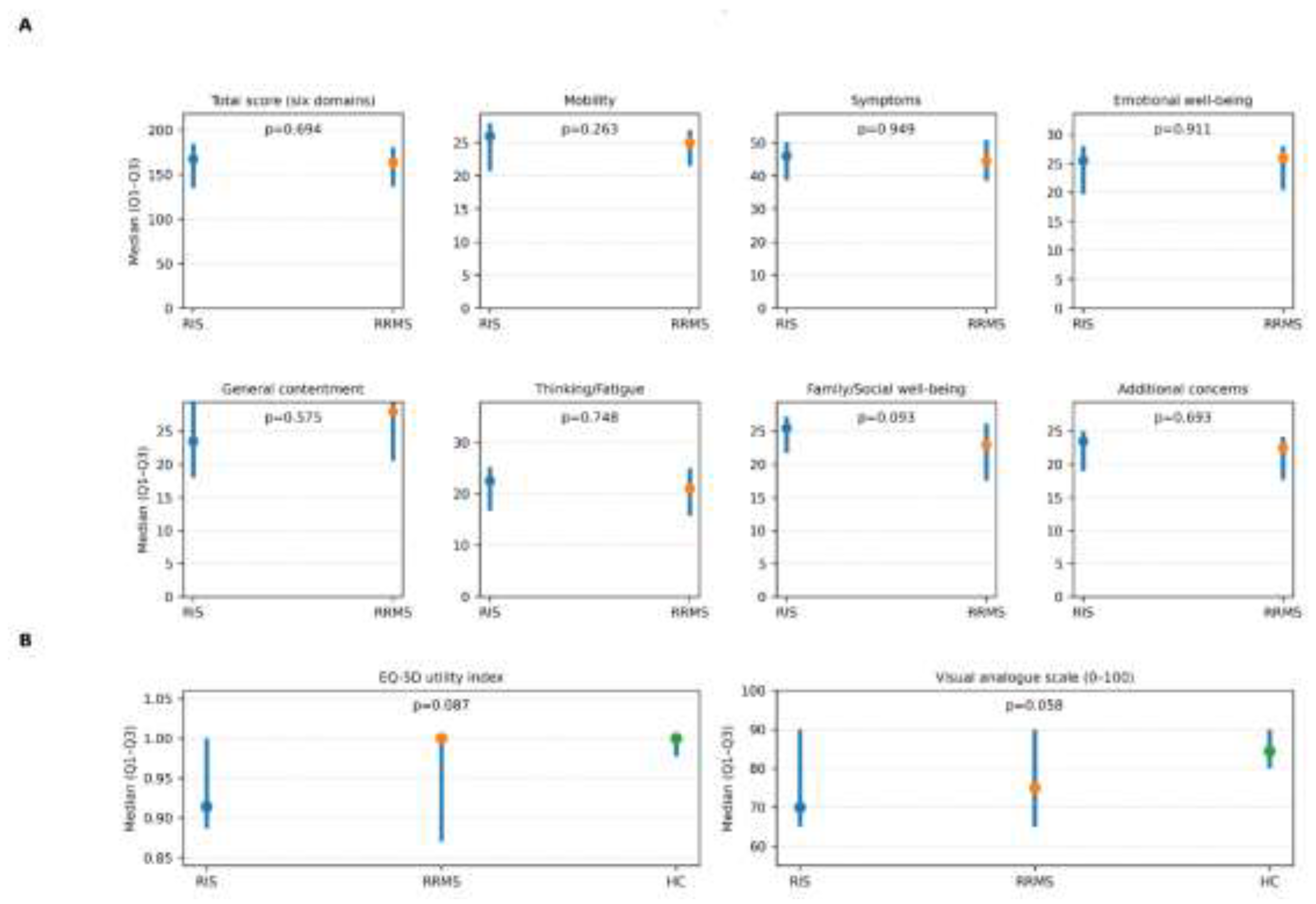
Figure 2.
Multivariable models for health-related quality of life outcomes.
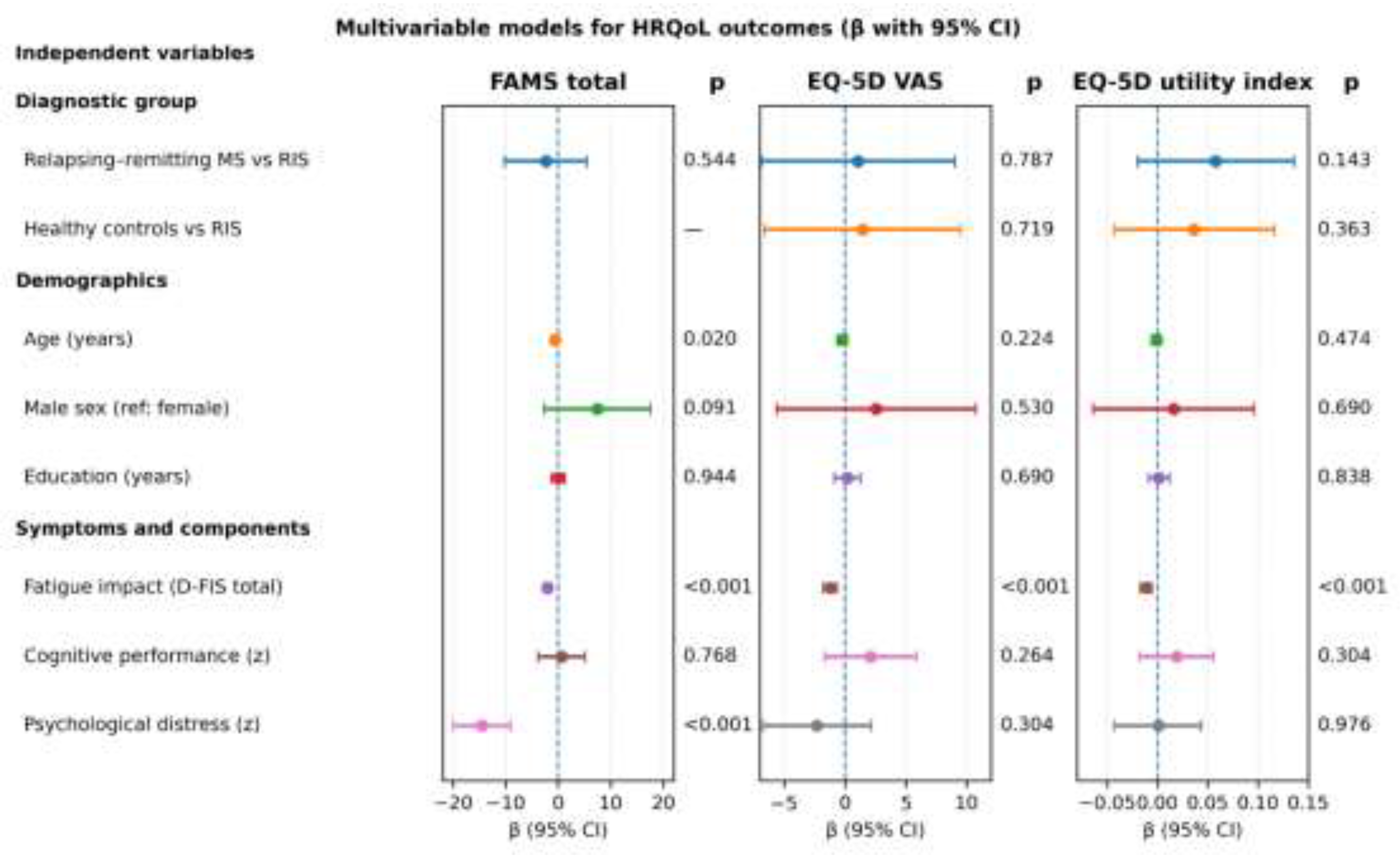

Table 1.
Baseline demographic, clinical, fatigue, cognitive, and psychological characteristics.
| Variable | Radiologically isolated syndrome (n=30) | Relapsing–remitting multiple sclerosis (n=29) | Healthy controls (n=30) | p value |
| Age (years), mean ± SD | 41.7 ± 8.1 | 41.4 ± 7.2 | 40.9 ± 7.8 | 0.925* |
| Female sex, n (%) | 26 (86.7%) | 20 (69.0%) | 24 (80.0%) | 0.247† |
| Education (years),median[Q1, Q3] | 15 [12–17.2] | 15 [11.5–17.5] | 15 [13-7–17.0] | 0.662‡ |
| Time since diagnosis (years), median[Q1, Q3] | 2.5 [1.0–8.7] | 4.0 [2.0–10.5] | — | 0.399** |
| Disability (Expanded Disability Status Scale), median [Q1, Q3] | — | 2.0 [1.0–3.0] | — | — |
| Fatigue impact (Daily Fatigue Impact Scale total score), median [Q1, Q3] | 3.0 [0.0, 13.0] | 7.0 [2.0, 15.0] | 2.0 [0.0, 8.2] | 0.051‡ |
| Depressive symptoms (Beck Depression Inventory total score), median [Q1, Q3] | 6.5 [3.0, 13.5] | 7.0 [2.7, 15.2] | 6.0 [1.5, 8.0] | 0.257‡ |
| State anxiety (State-Trait Anxiety Inventory-State total score), median [Q1, Q3] | 15.0 [8.0, 22.5] | 14.0 [5.0, 20.0] | 11.5 [5.7, 17.0] | 0.240‡ |
| Cognitive performance (component score; z), mean ± SD | -0.37 ± 1.12 | -0.04 ± 0.93 | 0.39 ± 0.81 | 0.013* |
| Psychological distress (component score; z), median [Q1, Q3] | -0.12 [-0.55, 0.96] | -0.10 [-0.59, 0.91] | -0.54 [-0.86, -0.14] | 0.014‡ |
* one-way analysis of variance (ANOVA); ** Mann-Whitney U test; †chi-square test; ‡ Kruskal–Wallis test.
Table 2.
Unadjusted health-related quality of life outcomes.
| Outcome | Radiologically isolated syndrome | Relapsing–remitting multiple sclerosis | Healthy controls | p value† |
| Functional Assessment of Multiple Sclerosis) | ||||
| Total score (six domains), median [Q1, Q3] | 167.5 [135.2, 185.0] | 164.0 [136.2, 181.0] | 0.694 | |
| Mobility, median [Q1, Q3] | 26.0 [20.7, 28.0] | 25.0 [21.5, 27.0] | — | 0.263 |
| Symptoms, median [Q1, Q3] | 46.0 [38.7, 50.2] | 44.5 [38.5, 51.0] | — | 0.949 |
| Emotional well-being, median [Q1, Q3] | 25.5 [19.7, 28.0] | 26.0 [20.5, 28.0] | — | 0.911 |
| General contentment, median [Q1, Q3] | 23.5 [18.0, 30.2] | 28.0 [20.5, 30.2] | — | 0.575 |
| Thinking/Fatigue, median [Q1, Q3] | 22.5 [16.7, 25.2] | 21.0 [15.7, 25.0] | — | 0.748 |
| Family/Social well-being, median [Q1, Q3] | 25.5 [21.7, 27.2] | 23.0 [17.5, 26.2] | — | 0.093 |
| Additional concerns, median [Q1, Q3] | 23.5 [19.0, 25.0] | 22.5 [17.7–24.2] | — | 0.693 |
| Generic HRQoL (EuroQol-5D) | ||||
| EQ-5D utility index, median [Q1–Q3] | 0.914 [0.887, 1.000] | 1.000 [0.870, 1.000] | 1.000 [0.978, 1.000] | 0.087 |
| Visual analogue scale (0–100), median [Q1–Q3] | 70.0 [65.0, 90.0] | 75.0 [65.0, 90.0] | 84.5 [80.0, 90.0] | 0.058 |
Higher scores indicate better health-related quality of life for all outcomes. † Mann-Whitney U test (radiologically isolated syndrome vs. multiple sclerosis); Kruskal–Wallis test (three-group comparison).
Table 3.
Multivariable models for health-related quality of life outcomes.
| Predictor | Functional Assessment of Multiple Sclerosis total β (95% CI) | p value | EuroQol-5D visual analogue scale β (95% CI) | p value | EQ-5D utility index β (95% CI) | p value |
| Relapsing–remitting multiple sclerosis vs. radiologically isolated syndrome | -2.37 (-10.18, 5.44) | 0.544 | 1.08 (-6.86, 9.01) | 0.787 | 0.058 (-0.020, 0.136) | 0.143 |
| Healthy controls vs. radiologically isolated syndrome | — | — | 1.46 (-6.60, 9.52) | 0.719 | 0.036 (-0.043, 0.116) | 0.363 |
| Age (years) | -0.60 (-1.09, -0.10) | 0.020 | -0.26 (-0.68, 0.16) | 0.224 | -0.001 (-0.006, 0.003) | 0.474 |
| Male sex (reference: female) | 7.44 (-2.71, 17.59) | 0.091 | 2.58 (-5.58, 10.75) | 0.530 | 0.016 (-0.064, 0.096) | 0.690 |
| Education (years) | 0.04 (-1.17, 1.25) | 0.944 | 0.22 (-0.86, 1.29) | 0.690 | 0.001 (-0.009, 0.012) | 0.838 |
| Fatigue impact (Daily Fatigue Impact Scale total score) | -2.04 (-2.66, -1.43) | <0.001 | -1.21 (-1.76, -0.67) | <0.001 | -0.011 (-0.017, -0.006) | <0.001 |
| Cognitive performance (component score; z) | 0.66 (-3.82, 5.13) | 0.768 | 2.12 (-1.64, 5.88) | 0.264 | 0.019 (-0.018, 0.056) | 0.304 |
| Psychological distress (component score; z) | -14.53 (-19.98, -9.08) | <0.001 | -2.30 (-6.75, 2.14) | 0.304 | 0.001 (-0.043, 0.044) | 0.976 |
β coefficients (95% CI) were estimated using multivariable ordinary least squares linear regression with heteroskedasticity-robust (HC3) standard errors. For categorical predictors, β represents the adjusted mean difference relative to the reference category; for continuous predictors, β represents the adjusted change in outcome per 1-unit increase in the predictor. Reference categories were RIS for the diagnostic group and female for sex. Cognitive and psychological predictors were standardized component scores (z; mean 0, SD 1). For the FAMS model (patients only), component scores were derived within the RIS/RRMS sample; for EQ-5D models (all participants), component scores were derived within the total sample. Model fit: FAMS R2=0.867; EQ-5D VAS R2=0.491; EQ-5D utility index R2=0.397. Multicollinearity was low (maximum VIF ≤2.13).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2026 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



