Submitted:
28 April 2023
Posted:
04 May 2023
You are already at the latest version
Abstract
: Background: The thymus gland is the first lymphoid organ formed to regulate a newborn's immunity. It reaches its maximum size during puberty, after which it undergoes an atrophic procedure called involution, but its ability to grow again in response to some stresses, such as infections, neoplasia, surgeries, chemotherapy, and radiotherapy is maintained. There is not any comprehensive study on computed tomographic features of thymus gland in dogs. So, the goal of the present study is to achieve some information about thymus gland using computed tomography as a non-invasive method. Methods: One hundred and fifty dogs classified in 5 age groups and 2 breed groups were entered to this study and the thymus gland was evaluated using 2-slice computed tomography machine. The inclusion criteria for the present study were having normal complete blood count, plain and post-contrast CT scan examination of thoracic region and no history of neoplasia, chemotherapy or radiotherapy. The visibility, density, enhancement, grade, size, volume, shape, borders and lateralization of the thymus were evaluated and statistical analysis were performed. The effect of obesity on thymic grade and volume were also investigated. Results: The visibility, density, dorsal length, volume and grade decreased with increasing age. The thymic shape and lateralization were mostly wedge-shaped and left sided respectively. The borders became concave with aging and increasing body fat content caused to increase fatty degeneration of thymus. Conclusions: Declining of thymic density, grade, size and volume with aging was related to thymic involution and fatty degeneration was accelerated by increasing body fat content. Females and Males were different only in thymic shape and small and large breeds were different only in thymic volume. The thymus was visible in some geriatric dogs with no underlying disease. We hope that the present work can be used by radiologists in reading thoracic computed tomography but investigation of thymic characteristics in dogs with neoplasia and history of chemotherapy, radiotherapy and thoracic surgeries can complete this study.
Keywords:
Computed tomography
; Thymus Gland
; Dog
; Age
; Gender
; Breed
; Body Fat
1. Introduction
The thymus gland is the first lymphoid organ formed to regulate a newborn's immunity [1,2,3,4]. It reaches its maximum size during puberty, after which it undergoes an atrophic procedure called involution or degeneration, but its ability to grow again in response to some stresses, such as infections, neoplasia, surgeries, chemotherapy, and radiotherapy, is maintained [2,5]. Anatomically, it is laterally compressed and lies in the cranioventral part of the thoracic cavity in dogs [4]. This organ starts to involute with the changing of the teeth in dogs. Although the process is initially rapid, the tissue usually does not atrophy completely, even in old age. When it decreases in size and loses its lymphoid structure, it is replaced by fat. However, evidence of thymic tissue can be seen in most dogs, regardless of age [4].
There are different conditions with the thymus, like aplasia, hypoplasia, juvenile thymic hematoma, true thymic hyperplasia, rebound hyperplasia, thymic cysts, and thymic tumors like thymoma and lymphoma [3]. Thymoma and lymphoma are the most common mediastinal neoplasia explained in veterinary patients [6,7]. Heart-based tumors, ectopic thyroid or parathyroid tumors, thymic branchial cysts, chemodectomas (aortic or carotid body tumors), metastatic neoplasia, granulomas, abscesses, lipomas, and teratomas must also be considered as differential diagnoses. In humans, there is wide variation in thymic characteristics at different ages making it important for radiologists to reduce unnecessary invasive procedures [2,5]. The recognition of a normal thymus on computed tomography (CT) is easier with knowledge of this normal variation, thereby avoiding false-positive diagnoses of mediastinal neoplasms [9]. So, the present study aims to describe the characteristics of the normal thymus glands in dogs using computed tomography as a non-invasive method and to the best of our knowledge this is the first study that evaluates the normal thymus specifically in dogs.
2. Materials and Methods
This descriptive and prospective study recruited a total of 150 dogs, including 74 females and 76 males entered to the study from February 2022 until February 2023.The criteria for inclusion in the study were having a normal complete blood count (CBC), a plain and post-contrast CT scan examination of the thoracic region, and referring for CT examination with no thymic abnormality, no neoplasia in the thymus or other organs, and metastasis detection. These patients were referred for computed tomography due to traumatic injuries and orthopedic reasons. All medical records and CT scan images were also evaluated to exclude patients with any pathologies that have a possible effect on the thymus, like lung nodules or lesions, sternal, mediastinal, or perihilar lymphadenopathy. The patients were of different breeds (Mix breeds, Pomeranian, German Shepherd, Shih Tzu, Maltese, Yorkshire, Terrier, Rottweiler, Spitz, Dachshund, Lhasa Apso, Jack Russel Terrier, Chihuahua, Grate Dane, Puddle, Border Collie, Pekingese, and Cocker Spaniel). They were divided into five groups, with 30 dogs in each group, according to their ages. Group 1 was a puppy group, including puppies from ages 0–6 months old; group 2 was a juvenile group, including 7–12 months old; group 3 was a young adult, including 1–2-year-old dogs; group 4 was an old adult group, including dogs age 3–7 years old; and group 5 was a geriatric group, including dogs more than 7 years old. They were also divided into two groups based on their size (small breeds: less than 15 Kg, and large breeds: more than 15 Kg).
All CT examinations were performed by a 2-slice Somatom-Spirit CT scan machine (Siemens). The contrast media used for all examinations were Omnipaque (240 mg/ml) with a dosage of 4 ml/kg or Visipaque (320 mg/ml) with a dosage of 2 ml/kg. Standard protocol for thoracic CT scan was used (120 kVp, 60-65 mA, acquisition slice thickness of 1-1.5 mm, and reconstructed slice thickness of 1-3 mm). Dorsal and sagittal images were reconstructed and used for better detection of the thymus. All examinations were stored in the PACS system and then Radiant viewer was used to evaluating the images. The Leonardo system was also used for volumetry. Evaluations were done by a board-certified radiologist in the Osteo window.
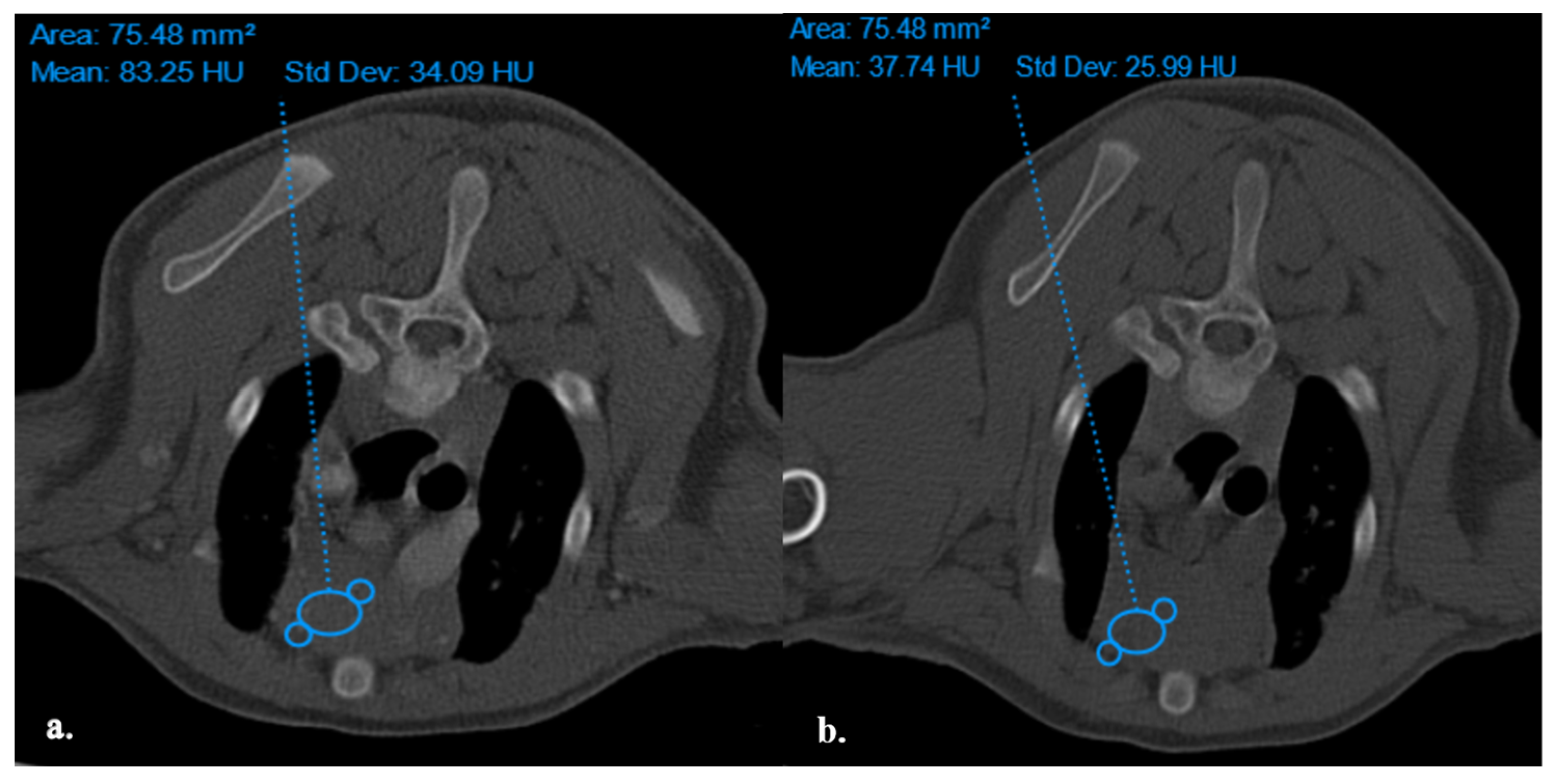
The thymus glands were evaluated in the first step to determine whether they were visible or not. Non-visible thymus glands were those with complete degeneration seen with fat attenuation and not distinguishable from mediastinal fat. After that, a grading system for thymic tissue appearance was used based on its predominant component (grade-0: totally fatty replacement of the thymus (non-visible) and could not differentiate from mediastinal fat; grade-1: more than 50% fatty replacement of the thymus; grade-2: more than 50% soft tissue component in the thymus; grade-3: totally soft tissue component in the thymus (Figure 1). After grading the thymus, the attenuation (CT number) of thymic tissue in plain and contrast-enhanced images was measured. For this purpose, a round-shape region of interest (ROI) with a surface equal to 75 mm2 was considered in the widest part of the organ for large thymus glands (Figure 2) and a smaller ROI for small thymus glands. Then pre- and post-contrast Hounsfield Units (HU) were compared for each patient individually and also between groups for evaluating the pattern of attenuation alteration.
Figure 1.
Demonstration of Post-contrast Transverse CT scan images for Different Grades of Thymus. Picture (a) shows a Visible Grade-3 Wedge-shape Left-sided Thymus in a 4-month-old Male Mixed-breed dog. Picture (b) shows a Visible Grade-3 Rectangular-shape Midline Thymus in a 5-month-old Female Shih Tzu Dog. Picture (c) shows a Visible Grade-2 Wedge-shape midline Thymus in an 8-month-old Male Spitz Dog. Picture (d) shows a Visible Grade-2 Rectangular-shape Midline Thymus in a 3-year-old Female Mixed-breed dog. Picture (e) shows a Visible Grade 1 Wedge-shape Left-sided Thymus in a 6-year-old Female Terrier Dog. Picture (f) shows a Visible Grade-1 Rectangular-shape Midline Thymus in a 7-year-old Female Terrier Dog. Picture (g) shows a non-visible Grade-0 Wedge-shape midline Thymus in an 11-year-old Female Shih Tzu Dog. Picture (h) shows a Non-visible Grade-0 Linear-shaped midline Thymus in a 6-year-old Female Cocker-Spaniel Dog.
Figure 1.
Demonstration of Post-contrast Transverse CT scan images for Different Grades of Thymus. Picture (a) shows a Visible Grade-3 Wedge-shape Left-sided Thymus in a 4-month-old Male Mixed-breed dog. Picture (b) shows a Visible Grade-3 Rectangular-shape Midline Thymus in a 5-month-old Female Shih Tzu Dog. Picture (c) shows a Visible Grade-2 Wedge-shape midline Thymus in an 8-month-old Male Spitz Dog. Picture (d) shows a Visible Grade-2 Rectangular-shape Midline Thymus in a 3-year-old Female Mixed-breed dog. Picture (e) shows a Visible Grade 1 Wedge-shape Left-sided Thymus in a 6-year-old Female Terrier Dog. Picture (f) shows a Visible Grade-1 Rectangular-shape Midline Thymus in a 7-year-old Female Terrier Dog. Picture (g) shows a non-visible Grade-0 Wedge-shape midline Thymus in an 11-year-old Female Shih Tzu Dog. Picture (h) shows a Non-visible Grade-0 Linear-shaped midline Thymus in a 6-year-old Female Cocker-Spaniel Dog.
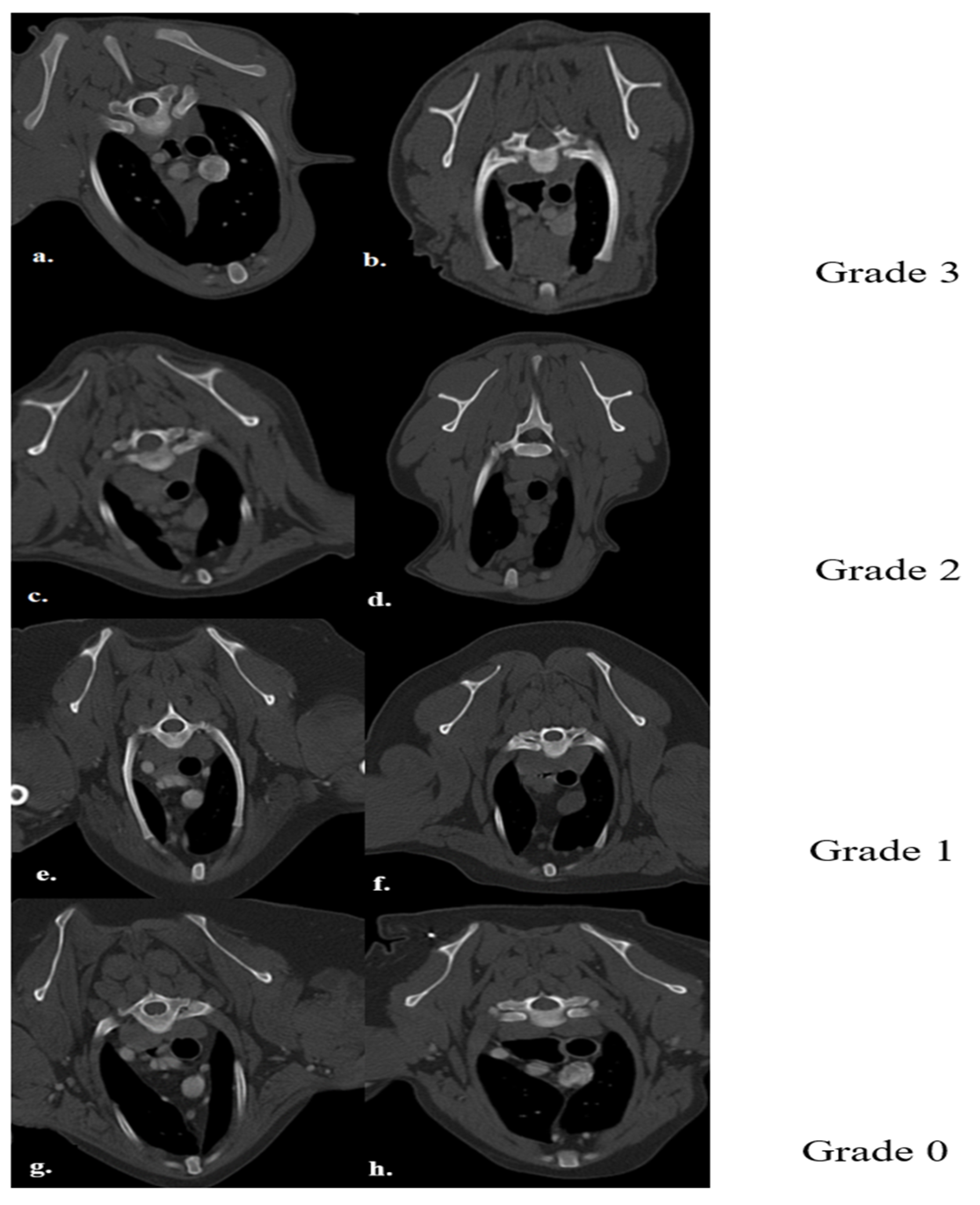
Figure 2.
Density Measurement in ROI equal to 75.48 mm2 in Plain (a) and post-Contrast (b) CT Scan Examinations of a four-month Mixed-Breed Male Dog with a Visible Grade 1 Thymus. The Thymus is Rectangular Shape with one Convex Border and is located in the midline position.
Figure 2.
Density Measurement in ROI equal to 75.48 mm2 in Plain (a) and post-Contrast (b) CT Scan Examinations of a four-month Mixed-Breed Male Dog with a Visible Grade 1 Thymus. The Thymus is Rectangular Shape with one Convex Border and is located in the midline position.
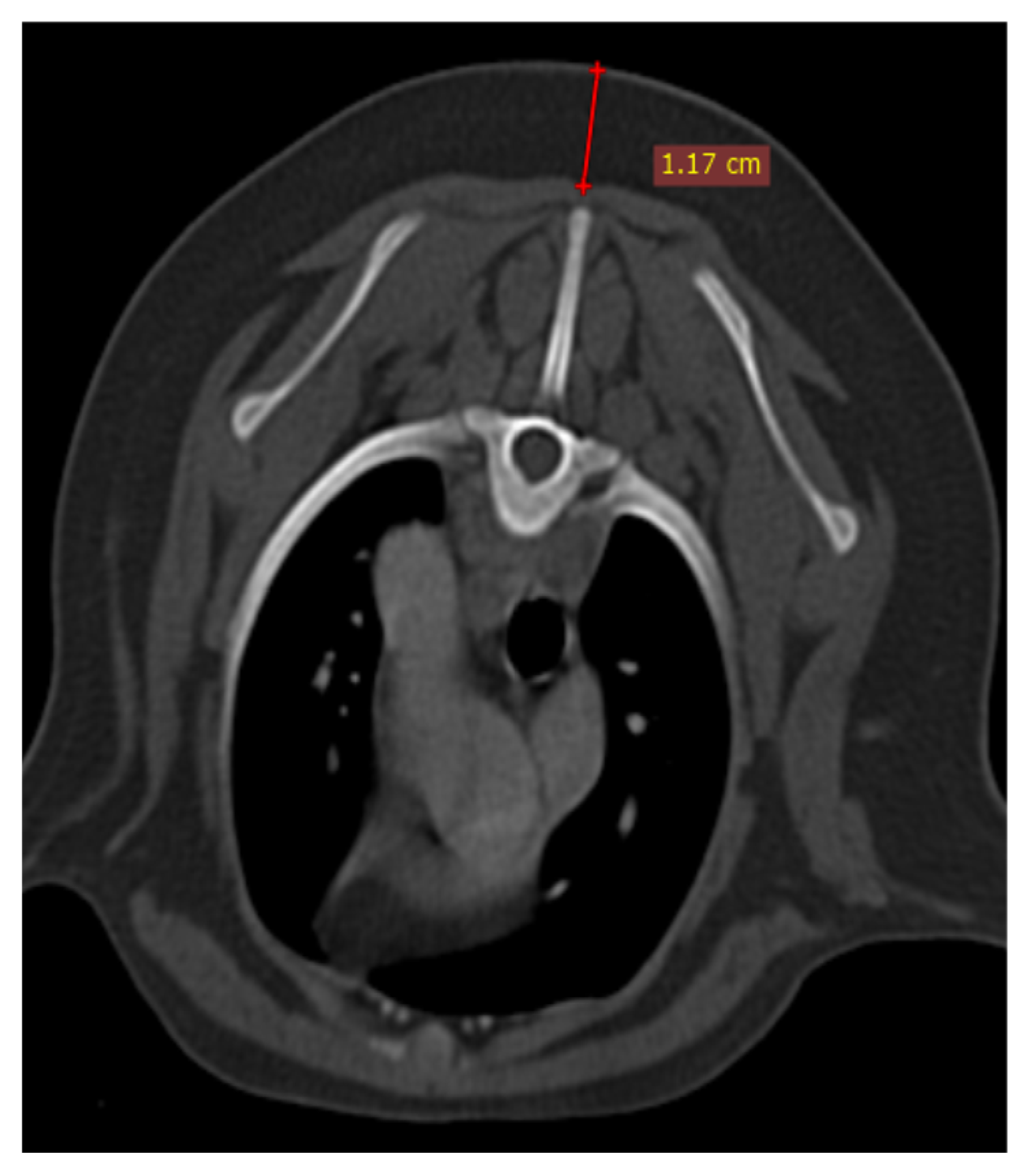
The size of the thymus was also measured in transverse and dorsal images. The maximum height (TH) and diameter (TD) in transverse images and maximum diameter (DD) and length (DL) in the dorsal view were measured (Figure 3 and Figure 4), as well as thymic volume (TV) in all groups. These indices were measured in the area related to mediastinal fat at the normal location of the thymus for patients with a completely fatty replacement of the thymus (grade-0). All measurements were done in contrast-enhanced examinations. To normalize the thickness of the thymus gland in transverse view, the width of the second thoracic vertebra midbody was measured and the ratio was calculated. The correlation between thymic size and grade with the body fat content was evaluated by measuring the thickness of subcutaneous fat in the dorsal aspect of the T4 spinous process (Figure 5). Subjective characteristics such as predominant deviation of the thymus to left or midline position, the thymic shape (wedge-shape, rectangular-shape, or linear-shape), and the thymic contour (convex and concave) were also evaluated. For patients with fatty degeneration, these characteristics were analyzed in mediastinal fat at the location of the previous thymus. Evaluation of thymic size, volume, attenuation, and grade was done twice by a single person within a week, and the mean value of the first and second measurements for numerical data and the second results for thymic grading were reported.
Figure 3.
Measurement of maximum transverse diameter and height in post-contrast CT scan examination. (a): visible grade-3 midline rectangular-shaped thymus in a 4-month-old mixed-breed male dog. (b): visible grade-2 midline rectangular-shaped thymus in a 5-month-old Shih Tzu female dog. (c): visible grade-2 left-sided wedge-shaped thymus in an 8-month mixed-breed male dog. (d): non-visible grade-0 midline wedge-shaped thymus in a 4-year-old mixed-breed female dog.
Figure 3.
Measurement of maximum transverse diameter and height in post-contrast CT scan examination. (a): visible grade-3 midline rectangular-shaped thymus in a 4-month-old mixed-breed male dog. (b): visible grade-2 midline rectangular-shaped thymus in a 5-month-old Shih Tzu female dog. (c): visible grade-2 left-sided wedge-shaped thymus in an 8-month mixed-breed male dog. (d): non-visible grade-0 midline wedge-shaped thymus in a 4-year-old mixed-breed female dog.
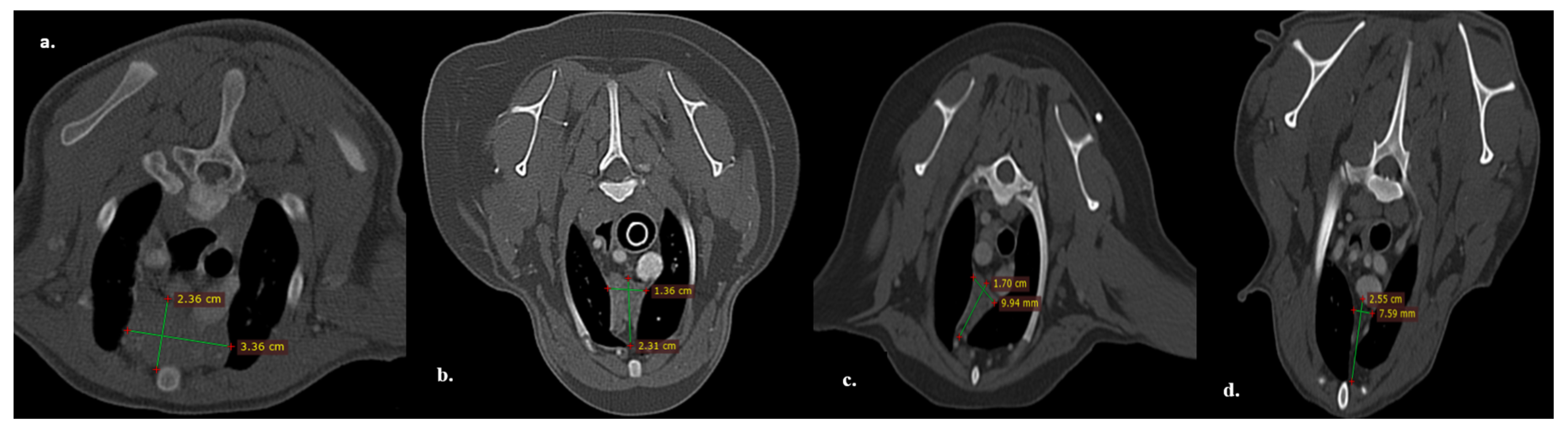
Figure 4.
Measurement of Maximum Dorsal Diameter and Length. Left Image Belongs to the same patient in Figure 3a (Dorsal view, Post-Contrast CT Scan Examination at the Level of Maximum Diameter and Length of Visible Grade-3 Thymus). Right Image Belongs to an 11-year-old Female Shih Tzu Dog, Dorsal View, Post-contrast CT scan Examination at the Level of Maximum Diameter and Length of Non-visible Garde-0 Thymus).
Figure 4.
Measurement of Maximum Dorsal Diameter and Length. Left Image Belongs to the same patient in Figure 3a (Dorsal view, Post-Contrast CT Scan Examination at the Level of Maximum Diameter and Length of Visible Grade-3 Thymus). Right Image Belongs to an 11-year-old Female Shih Tzu Dog, Dorsal View, Post-contrast CT scan Examination at the Level of Maximum Diameter and Length of Non-visible Garde-0 Thymus).
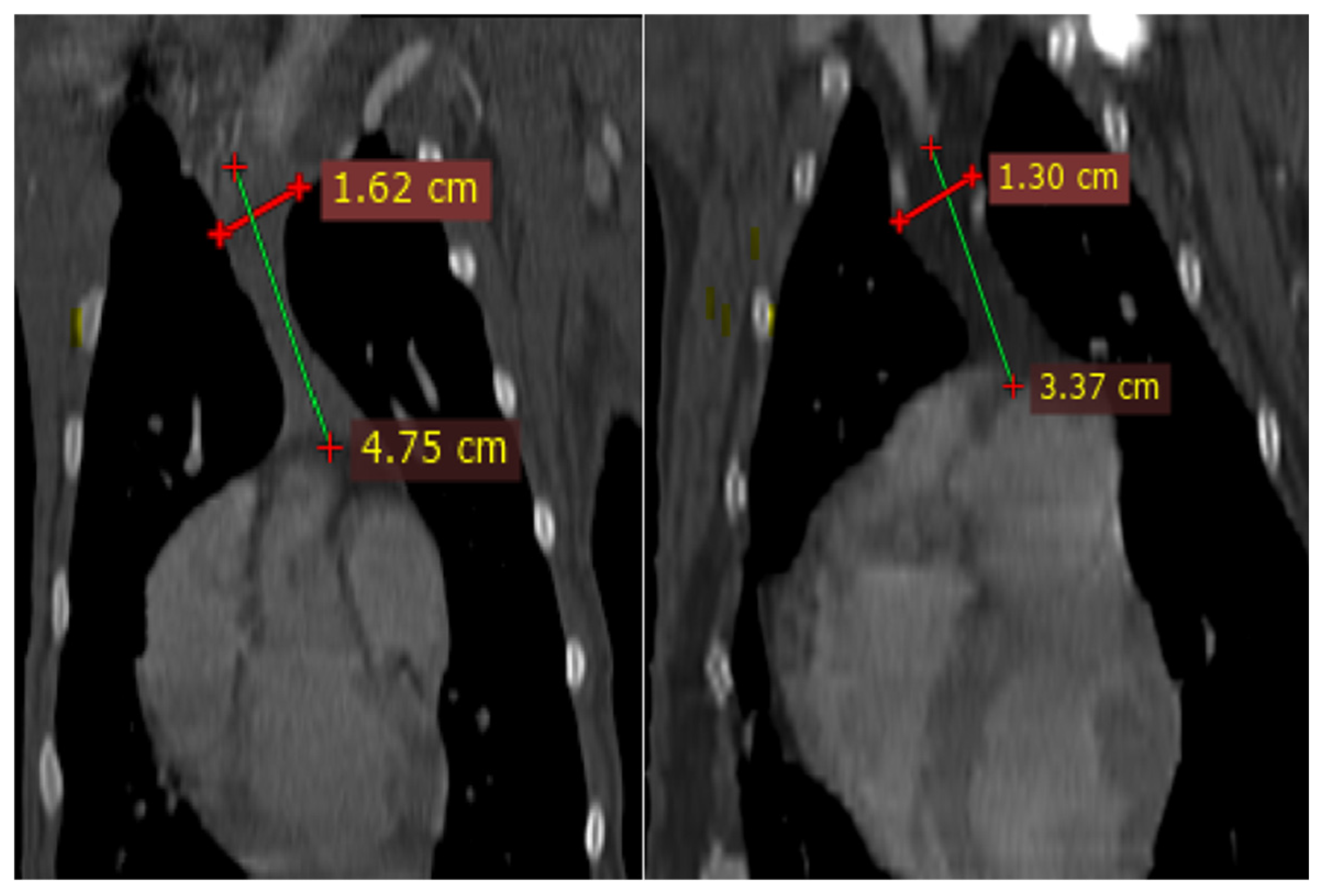
Figure 5.
Demonstration of Measurement of Subcutaneous Fat Content at the Level of T4 in Transverse Section of Post-Contrast CT Examination.
Figure 5.
Demonstration of Measurement of Subcutaneous Fat Content at the Level of T4 in Transverse Section of Post-Contrast CT Examination.
2.1. Statistical Analysis
Categorical data were collected as numbers and presented as a percent value. Continuous data were presented as mean ± SD. Mean density, TD, TH, DD, DL, and TV were compared between groups using one-way ANOVA and the Tukey method; the t-test was used for comparing numerical data between the two groups; and the Pearson Chi-square test was used to analyze the categorical variables like enhancement, shape, predominant side, and grading. The Pearson correlation coefficient (r value) was calculated for the evaluation of the repeatability and reliability of two-stage measurements (intra-observer agreement). All statistical analyses were performed with SPSS software version 16.
3. Results
3.1. Visibility
In the present study, the thymus gland was visible in 104 of 150 cases, but the distinct lobes of the thymus were not distinguishable. The visible thymus glands were noted with soft tissue component and homogenous appearance, a combination of soft tissue and fat component based on the degree of involution with heterogenous (mottled) appearance and only fat component (Figure 1 and Figure 6). We accounted the thymus glands with complete fat degeneration for non-visible thymus glands (Figure 6). The anatomical and topographical location of the thymus is shown in Figure 7. The thymus' dorsal border begins at the ventral aspect of the vessels in the cranial mediastinum and ends at the dorsal aspect of the sternebra. In dorsal and sagittal views, it was extended caudally up to the pericardial region and merged with the pericardium on the left side. The visibility percentage in group 1 was 100%. The minimum and maximum ages in group 1 were three and six months, respectively. In groups 2 and 3, the thymus was visible in 86.7% of cases and it was not notable in 13.3% of cases. The minimum and maximum ages with visible thymus in group 2 were seven and 12 months, respectively. This group includes three 12-month-olds and one 11-month-old case with a non-visible thymus. In group 3, the youngest and oldest cases with a visible thymus were 1.5 and 2 years old. The patients with a non-visible thymus were two years old. In group 4 the visibility percentage was 53.3% and the thymus was not visible in 46.7% of patients. The youngest and oldest patients with visible thymus in group 4 were three and six years old. The visibility percentage of group 5 was 20% and the maximum age with visible thymus was nine years old (Table 4 and Table 6).
Figure 6.
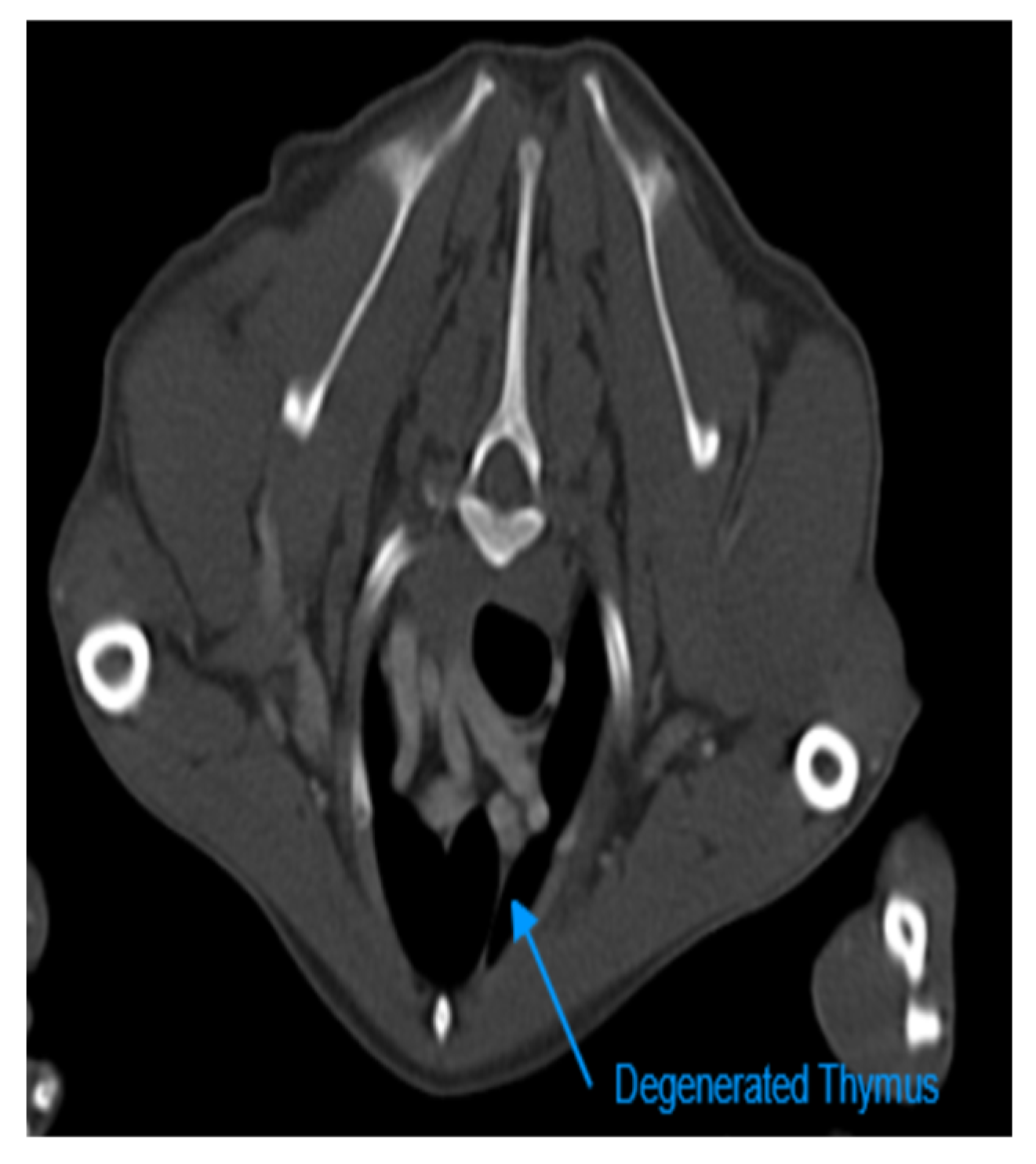
Transverse Section of a Contrast-Enhanced CT scan Examination at the Level of T2 of a 12-year-old Male Terrier Dog. The shorter arrow shows Complete Fatty Degenerated Thymus which is not Distinguishable from Mediastinal fat. LITa: Left Internal Thoracic Artery.
Figure 6.
Transverse Section of a Contrast-Enhanced CT scan Examination at the Level of T2 of a 12-year-old Male Terrier Dog. The shorter arrow shows Complete Fatty Degenerated Thymus which is not Distinguishable from Mediastinal fat. LITa: Left Internal Thoracic Artery.
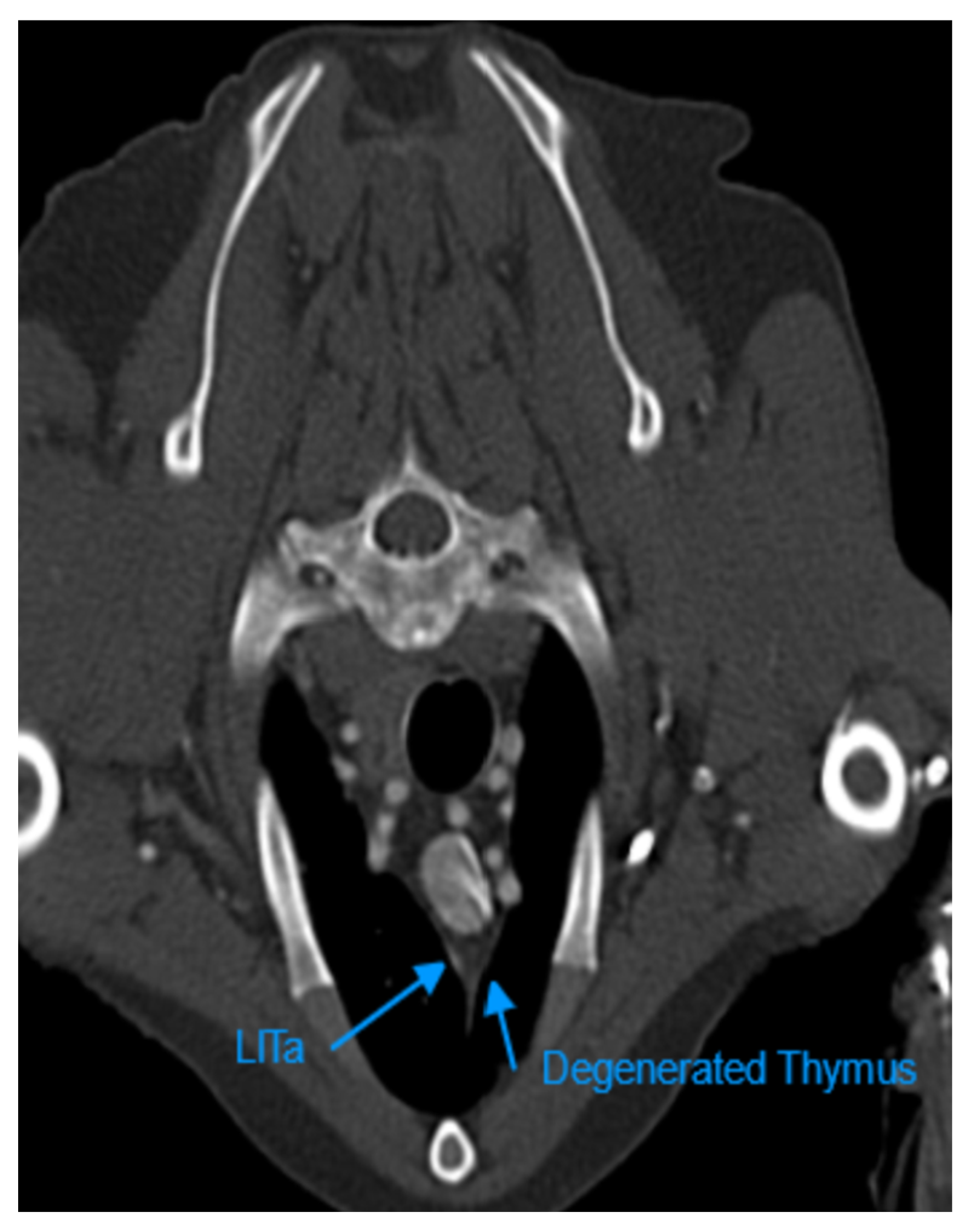
Figure 7.
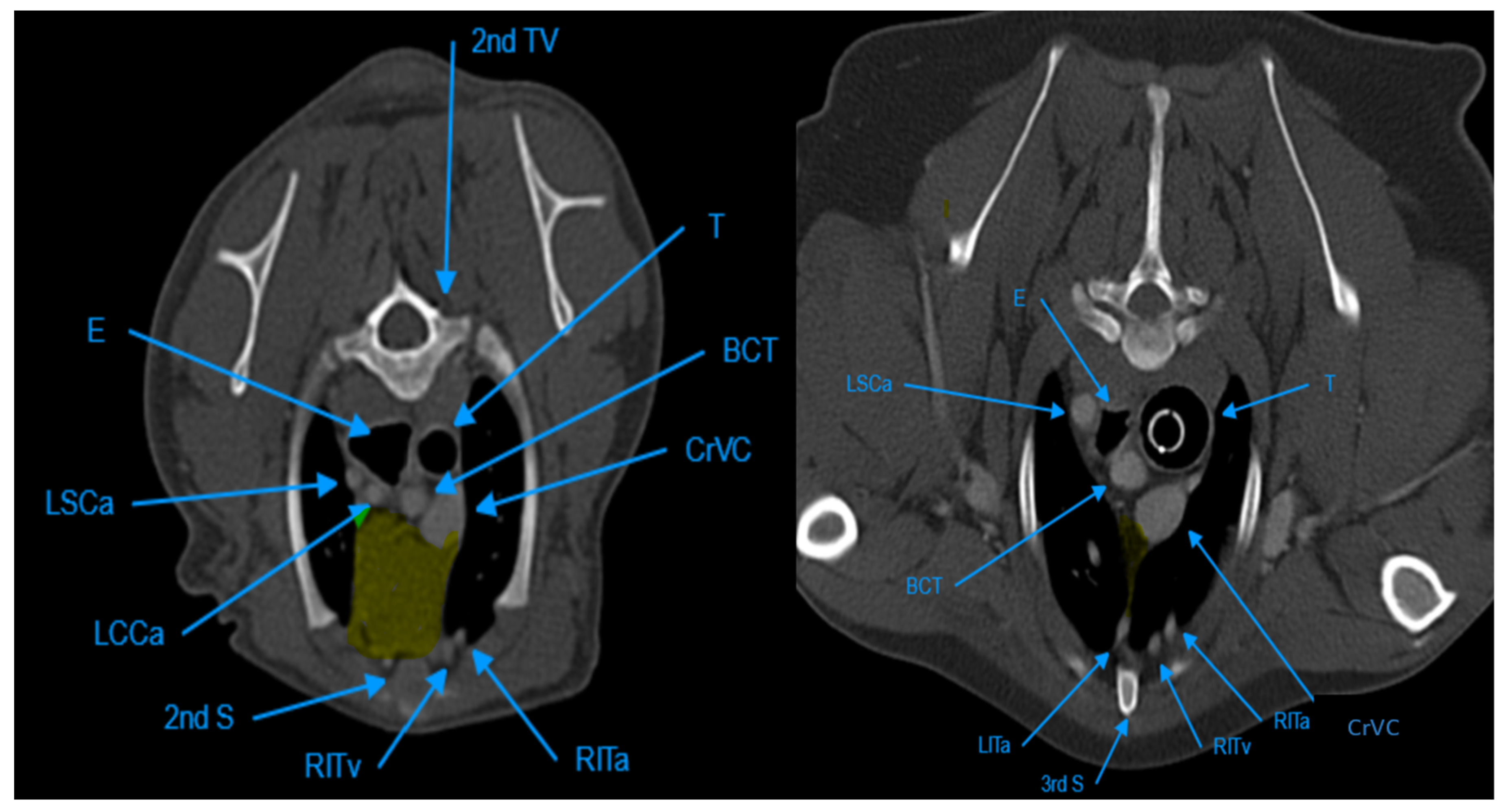
Illustration of Anatomical and Topographical Location of Thymus in Transverse Section of Post-contrast CT Scan Examinations. The Left Image is at the Level of T2 and Belongs to a 3-month-old Male Mixed-breed Dog. The Thymus Highlighted with Yellow Colour is Visible with Complete Soft Tissue Component in this Patient. The Right Image is also at the Level of T2 and Belongs to a 4-year-old Female Dog. In this patient, the Thymus is Completely Degenerated and Highlighted with Yellow Colour. T: Trachea, E: Esophagus, LSCa: Left Subclavian Artery, BCT: Brachiocephalic Trunck, LITa: Left Internal Thoracic artery, S: Sternebra, RITv: Right Internal Thoracic Vein, RITa: Right Internal Thoracic Artery, CrVC: Cranial Vena Cava, TV: Thoracic Vertebra.
Figure 7.
Illustration of Anatomical and Topographical Location of Thymus in Transverse Section of Post-contrast CT Scan Examinations. The Left Image is at the Level of T2 and Belongs to a 3-month-old Male Mixed-breed Dog. The Thymus Highlighted with Yellow Colour is Visible with Complete Soft Tissue Component in this Patient. The Right Image is also at the Level of T2 and Belongs to a 4-year-old Female Dog. In this patient, the Thymus is Completely Degenerated and Highlighted with Yellow Colour. T: Trachea, E: Esophagus, LSCa: Left Subclavian Artery, BCT: Brachiocephalic Trunck, LITa: Left Internal Thoracic artery, S: Sternebra, RITv: Right Internal Thoracic Vein, RITa: Right Internal Thoracic Artery, CrVC: Cranial Vena Cava, TV: Thoracic Vertebra.
3.2. Density
It was found that the mean density of the thymus decreased with increasing age from group 1 to group 5, but there was not the same pattern between the patients in one group with different ages and the distribution of CT numbers in one group was very wide. The mean, minimum, and maximum densities in plain and post-contrast CT scan examinations in each group were summarized in Table 2 and Table 3. The differences in mean density between plain and post-contrast CT scan examination regarding age groups were significant (P-value ≤ 0.05, Table 2 and Table 3). The mean density difference between each group (for example, group 1 with other groups) was evaluated and summarized in Table 4. There was a significant difference between the mean density of group 1 with other groups. Also, there was a significant difference between the mean density of group 2 with groups 1, 4, and 5. The difference in the mean density of group 3 was significant compared to groups 1, 4, and 5, while the difference in the mean density of groups 4 and 5 was not significant. The Pearson correlation coefficient for intra-observer agreement of two-stage measurement of CT numbers was 84.5% and 85% for plain and post-contrast CT scan examinations, respectively (Table 2 and Table 3).
3.3. Enhancement
Ninety-four point seven percent of the thymus glands in this study were enhanced. According to the results, 0.01 percent of the visible thymus was not enhanced (two patients out of 104). The other non-enhanced thymus glands were non-visible (six patients out of 46). The percentage of enhancement in groups 1, 2, and 4 was 100%, and in groups 3 and 5, it was 93.3% and 80%, respectively. The P-value for comparing enhancement showed a significant difference between age groups (Table 1, P-value ≤ 0.05). There was no significant difference between the thymic enhancement of different breeds and genders. The thymus was enhanced in 93% of females and 96% of males. It was also noted that the blood supply of the thymus was mostly by left and right internal thoracic arteries and veins anatomically.
3.4. Shape
Three different shapes of the thymus in the transverse section were noted in the present study: a rectangular shape with convex borders that was visible in younger patients, a wedge-shaped appearance with concave or straight borders in young or adult patients, and a linear shape that was seen predominantly in older patients (Figure 1). The thymic shape in the sagittal view was variable and categorization could not be established for shape in the sagittal and dorsal sections. In the dorsal view, the thymus gland was wider in the cranial and caudal portions and in the mid-part it was narrower and became narrower with aging. The shape of the transverse section of the thymus was wedge-shaped with a concave border at 74.4%, rectangular with a convex border at 22%, and linear at 3.3%. The difference in shape between age groups and different breeds was not significant, but there was a significant difference in the shape of the thymus between genders (P-value = 0.006). The percent values of each kind of shape are summarized in Table 1 and Table 5.
3.5. Predominant Side
The dominant side of the thymus in the cranial portion was evaluated because the thymus deviated to the left side caudally in all patients, resulting in the well-known 'sail sign' in radiographic images. The predominant side of the thymus was left-sided in 46% of cases and mid-line in 53% of cases. There was only one patient with a thymus gland deviated to the right side in the cranial aspect of the mediastinum (Figure 8). The predominant side percentage of each group was summarized in Table 1. The difference in the predominant side was significant between groups 1, 2, and 3. In group 1, the thymus was mostly in the midline and it was deviated to the left side in groups 2 and 3. There was no significant difference between large and small breeds for this variable. There was an equal percentage of this variant in large breeds (50%), 41% of small breeds had a left-sided thymus, and 59% had a mid-line thymus.
Figure 8.
Transverse Section of contrast-enhanced Thoracic CT scan Examination in a 6-year-old Male Puddle Dog. The Blue Arrow Shows a Linear-shaped Degenerated Thymus which is Deviated to the Right side.
Figure 8.
Transverse Section of contrast-enhanced Thoracic CT scan Examination in a 6-year-old Male Puddle Dog. The Blue Arrow Shows a Linear-shaped Degenerated Thymus which is Deviated to the Right side.
3.6. Volume
The mean, maximum, and minimum volumes of each group are summarized in Table 6. The values of volume decreased with aging, and there was a significant difference in the volume of the thymus between age groups (P-value = 0.000). The mean volume of the thymus in females was 2.3 ±2.6 cm3 and 2.5±3.8 cm3 in males, with no significant difference between males and females, but a significant difference in volume between breeds. The mean value of volume in large breeds was 2.99±4.1 cm3, and in small breeds, it was 1.71±1.4 cm3. The Pearson correlation coefficient was high between the 2-stage measurement of thymic volume (97.5%). There was no correlation between thymic volume and subcutaneous fat content (r = 0.053).
3.7. Diameter, Length, and Height
The mean, minimum, and maximum values of the diameter and height in transverse views and the diameter and length in dorsal views are shown in Table 6. There is no significant difference in TD, TH, and DD between age groups, but the difference in DL was significant (P-value ≤ 0.05). The approximate ratio between TD and the diameter of the T2 midbody was 1.2±0.7.
3.8. Grade
The grade of the thymus gland has been declining with increasing age. There was no grade-0 thymus in group 1. There were no grade-3 and 2 thymus glands in group 5. Based on the findings, the correlation between age and grade was significant. The percent value of each grade in each group is summarized in Table 1. Based on the correlation coefficient, there was a reverse correlation between grade and subcutaneous fat content (r: -0.18).

Table 1.
Percent Values of each Categorical Variable of the Thymus Gland in Different Ages and P values.
Table 1.
Percent Values of each Categorical Variable of the Thymus Gland in Different Ages and P values.
| Group (n = 30) | Group 1 | Group2 | Group3 | Group 4 | Group 5 | P value≤0.05 |
|---|---|---|---|---|---|---|
| Visibility (%) | 100 | 86.7 | 86.7 | 53.3 | 20 | |
| Enhanced (%) | 100 | 100 | 93.3 | 100 | 80 | 0.001 |
| Shape | ||||||
| Wedge shape (%) | 63.3 | 76.7 | 86.7 | 66.7 | 80 | |
| Rectangular (%) | 36.7 | 23.3 | 6.7 | 33.3 | 10 | |
| Linear (%) | 0 | 0 | 6.7 | 0 | 10 | |
| Total | ≥0.05 | |||||
| Side predominancy | ||||||
| Left-sided (%) | 43.3 | 50 | 70 | 40 | 26.7 | |
| Mid-line (%) | 56.7 | 50 | 30 | 60 | 73.3 | |
| Total | 0.016 | |||||
| Grade (%) | ||||||
| 3 | 66.7 | 20 | 6.7 | 0 | 0 | |
| 2 | 23.3 | 53.3 | 46.7 | 6.7 | 0 | |
| 1 | 10 | 20 | 36.7 | 53.3 | 20 | |
| 0 | 0 | 6.7 | 10 | 40 | 80 | |
| Total | 0.000 |
Table 2.
Mean, Minimum, and Maximum Densities in Plain CT scan Examination. The P value and r value are also demonstrated.
Table 2.
Mean, Minimum, and Maximum Densities in Plain CT scan Examination. The P value and r value are also demonstrated.
| Age Groups | Mean | Minimum | Maximum | P value (≤0.05) | r value (%) |
|---|---|---|---|---|---|
| Group 1 | 24.3±39 | -40 | 60 | ||
| Group 2 | -2.2±34 | -145 | 63 | ||
| Group 3 | -11.6±39 | -160 | 80 | ||
| Group 4 | -84.1±36 | -180 | -5 | ||
| Group 5 | -100±22 | -140 | -41 | ||
| Total | 0.000 | 84.5 |
Table 3.
Mean, Minimum and Maximum Densities in Contrast-enhanced CT scan Examination. The P value and r value are also demonstrated.
Table 3.
Mean, Minimum and Maximum Densities in Contrast-enhanced CT scan Examination. The P value and r value are also demonstrated.
| Age Groups | Mean | Minimum | Maximum | P value (≤0.05) | r value (%) |
|---|---|---|---|---|---|
| Group 1 | 62.1±29 | -14 | 135 | ||
| Group 2 | 35±41 | -80 | 144 | ||
| Group 3 | 20.06±42 | -109 | 100 | ||
| Group 4 | -45.2±37 | -140 | 2 | ||
| Group 5 | -74.3±34 | -139 | -16 | ||
| Total | 0.000 | 85 |
Table 4.
P values from Comparing Mean Densities between Groups (P value≤ 0.05).
| Age Groups | Group 1 | Group 2 | Group 3 | Group 4 | Group 5 |
|---|---|---|---|---|---|
| Group 1 | - | 0.019 | 0.000 | 0.000 | 0.000 |
| Group 2 | 0.019 | - | 0.8 | 0.000 | 0.000 |
| Group 3 | 0.000 | 0.8 | - | 0.000 | 0.000 |
| Group 4 | 0.000 | 0.000 | 0.000 | - | 0.3 |
| Group 5 | 0.000 | 0.000 | 0.000 | 0.3 | - |
Table 5.
Percent Values of Different Shapes of Thymus based on Gender and Breed.
| Shape of Thymus | Wedge | Rectangular | Linear |
|---|---|---|---|
| Female | 66.2% | 32.4% | 1.4% |
| Male | 82.9% | 11.8% | 5.3% |
| Small Breeds | 66.7% | 28.8% | 4.5% |
| Large Breeds | 81% | 16.7% | 2.4% |
Table 6.
The Mean, Maximum, and Minimum values of Numerical Measurement of the Thymus Gland in Age Groups.
Table 6.
The Mean, Maximum, and Minimum values of Numerical Measurement of the Thymus Gland in Age Groups.
| Groups | Group 1 | Group2 | Group 3 | Group 4 | Group 5 | P value | r value (%) |
|---|---|---|---|---|---|---|---|
| TD (mm) | |||||||
| Mean | 10.5±6.8 | 9.4±4.8 | 7.3±2.6 | 8.3±4.9 | 8.9±3.1 | ||
| Max | 34 | 20.5 | 13 | 30 | 16.5 | ||
| Min | 4.1 | 2 | 3 | 2.8 | 4.5 | ||
| Total | 0.1 | 79 | |||||
| TH (mm) | |||||||
| Mean | 21.3±9.2 | 20.7±7.9 | 18.4±7.3 | 17.1±7.4 | 16.2±9.8 | ||
| Max | 48.5 | 43 | 41.5 | 33 | 43 | ||
| Min | 4.2 | 11.5 | 10 | 2.6 | 5 | ||
| Total | 0.083 | 75 | |||||
| DD (mm) | |||||||
| Mean | 9.1±6.5 | 7.7±3.4 | 5.8±2.8 | 7.4±4.7 | 6.7±3.07 | ||
| Max | 32 | 14.5 | 14.5 | 27 | 14 | ||
| Min | 4.5 | 2.8 | 1 | 1.2 | 1 | ||
| Total | 0.061 | 79 | |||||
| DL (mm) | |||||||
| Mean | 27.6±12.1 | 28.6±13.7 | 25.8±6.9 | 23.8±8.05 | 20.8±8.4 | ||
| Max | 50 | 58 | 40 | 42 | 42.5 | ||
| Min | 9.05 | 7.3 | 15 | 8.5 | 9 | ||
| Total | 0.02 | 72 |
4. Discussion
The thymus gland was visible in all puppies in this study. According to the results, the thymic component started to atrophy and be replaced by fat after six months of age, and the fat content was increasing with aging. According to Evans and de Lahunta, anatomically, in a small dog, the caudal aspect of the left thymic lobe is placed between the thoracic wall and the left ventricle. According to them, the right lobe of the thymus usually touches the cranial surface of the pericardial sac and is extended laterally [4]. According to the present results, the distinct lobes of the thymus were not seen distinctly which can be because of the low accuracy of the 2-slice CT scan machine; anyway, observed the same topographical characteristics as the Evans and de Lahunta study were observed. In one ultrasonographic study of the thoracic region in dogs and cats, the authors concluded that the thymus degenerates after puberty [10].
In humans it was shown that some disorders, such as infection, tumorogenic conditions, and chronic inflammations have been shown in studies to accelerate the fatty involution of the thymus [7,11]. It was also shown that the thymus can regrow after recovery from the stress [2]. This phenomenon which is called ‘rebound hyperplasia’ can happen some month after resolving the stress [2]. In the present study, it was observed that the thymus can be visible in healthy adult dogs. The thymic soft tissue component was preserved in some healthy adult and geriatric dogs but because the mentioned phenomenon has not been confirmed in dogs yet, if the thymus is visible with residual soft tissue component in adult and geriatric ages and there are no clinical signs or suspicion of any neoplasia or infections, it will be a normal variant, but if there are some facts for these problems in the time of examination or related to the past, further investigations should warrant the abnormality of the thymus. The early fatty degeneration of the thymus in juveniles and young adults in this study can also relate to some conditions, such as previously treated infections or inflammations which accelerated the thymic atrophy.
The CT attenuations of thymus glands in the present study were in the range of soft tissue and fat based on the predominant component, but there was a wide spectrum of densities in each group and between individuals. This study also noted that the CT numbers for each patient matched the subjective grade. According to the findings, only in eight patients which were young adults and geriatric, no enhancement was notable. In these patients, the grade of the thymus was also 0, so non-enhancement could be due to severe atrophy of the gland. Another reason can be the very small size of the degenerated thymus, which reduces the accuracy of density measurement. Another theory is that there were insufficient contrast media injected, but when the enhancement of other organs was checked, this theory was ruled out.
The shape of the thymus in the transverse section was variable between dogs, even in the same age and breed group, but a classification was done for the shape. According to the results, it was observed that most of the thymic shapes in the transverse section were wedge-shaped with straight and concave borders, perhaps because most of the patients were adults. Most of the puppies’ thymus were rectangular with a convex border. The thymic shape was also significantly different between genders; females had a more rectangular-shaped thymus than males. Old adult dogs had a more rectangular-shaped thymus than juveniles and young adults; it can be related to the body conformation of dogs in this group. Another reason can be related to the fact that there were more male dogs in the juvenile and young adult groups. The thymic shape was so variable in sagittal and dorsal views that it was impossible to classify it in reconstructed views.
The dominant side of the thymus was also variable, but in all of the samples, the caudal aspect of the thymus extends to the left side, which makes a ‘sail sign’ in ventrodorsal thoracic radiographs. This feature in humans is right-sided and the sail sign is notable on the right side in anterior-posterior radiographs [2]. The dominant side was significantly different between puppies, juveniles, and young adults. The thymus was mostly in the midline in puppies and deviated to the left side with age, but this pattern was not repeated in old adults and geriatrics, and this variable needs more investigation in the future.
In the present study, the transverse view was mostly used to evaluate the characteristics because it is the main non-reconstructed view with better resolution and because of better categorization of features like thymic shape and side predominancy in this view.
In this study population, the volume and thymic length in the dorsal view decreased with aging. The mean values of each measured index of the thymus separately with a high reliability coefficient. Anatomically, in beagles, it is known that when the thymus gland is completely developed it is 12 cm long, 6 cm wide, and 3 cm high [4]. Moarrabi et al. performed radiographic and ultrasonographic examinations of the thymus in five Mongrel puppies every month from birth to five months of age [12]. They reported the thymic width and length at five months of age were about 6.56±0.63 mm and 28.10±2.72 mm, respectively, which were near the reported measurements of this study.
It was observed that the fat replacement of the thymus increases with an increase in subcutaneous fat content, which can be an index of obesity and body condition in the study population. Animal studies also demonstrated that obesity might cause early atrophy and fat accumulation in the thymus, resulting in a decline of naive T-cell production in the thymus gland [13]. The impact of obesity on the thymic attenuation in human patients between 20 and 30 was evaluated in one study that showed overweight patients are more likely to have higher levels of thymic fatty replacement than normal or underweight patients [14]. Obesity has also been shown in murine models to play a role in the induction of thymus gland malfunction, which increases the risk of infection and some types of neoplasia [7,15]. Araki et al. showed that patients with low thymic grades had significantly higher body condition scores. They evaluated the impact of physical characteristics such as body mass index (BMI) and cigarette smoking on thymus shape in CT scans of human patients in middle and old age. They have the same grading and objective description as our study [13]. Their study showed the difference in thymic appearance on CT between males and females in the age range of 40-69. They also demonstrated a variety of normal thymus appearances on CT scans and differences in thymic shape between males and females in the middle and older age groups. Their findings suggested that the start of thymic atrophy in females is delayed by approximately 10 to 20 years in comparison to males. Thymic atrophy is completed before the age of 60 in men and 70 in women, and sexual steroids are considered to affect the thymic shape [13,16].
There is a most recent study evaluated the thymus in adult dogs with non-thymic neoplasia in comparison to thymus in young dogs (under 9 months) using computed tomography. According to this study the thymus was triangular-shaped mostly in both adult and young groups and bilobed thymus was noted only in one patient. The thymus appearance was also lobulated in adults and homogenous in young dogs. Thymus lateralization was mostly left sided in adults and in midline in young dogs. There was just one patient with right-sided thymus according to this study. They also observed that there is a variation in thymic dimensions between different patients with different body weight. They also found that the thymic attenuation was lower in adults because of fatty degeneration. Finally, they concluded that the thymus can be visible in adult dogs with different neoplasia compared to young dogs [17].
Heiberg et al. studied the normal and abnormal thymus using CT scan examinations in 40 human cases under 20 years old. They concluded that there was significant variation in the CT scan appearance of a normal thymus in the preadolescent and adolescent age groups [9]. They reported the thymic characteristics in the CT scan examination and observed smooth and convex thymic contours in the very young and straight and concave thymic contours with increasing age. They also concluded that there is a wide variation in CT attenuation of the thymus gland in plain and contrast-enhanced CT scan examinations [9]. According to their result, the thymus is larger in younger but the thymic size varied widely in all ages. They also noticed the thymic lobes distinctly [9].
In a review of the clinical and radiological features of the thymus gland in the pediatric human group, the mean thickness of the thymus was about 0.5-1.1 cm. In this investigation, the density of the thymus decreased with age in children (from 80 HU to 56 HU) [3]. A human study found that patients younger than 20 years old had a normal thymus thickness of 18 mm, compared to those older than 20 years old who had a thickness of 13 mm. It takes more than 15 years for the thymus to become triangular in shape with straight or concave borders after it has started to develop in the first decade of life. According to this study, the biconvex margins late in the second decade of life or the focal expansion of a lobe or multilobulation at any age are usually indicative of thymic abnormality [18]. An analysis of the side-to-side diameter of a normal thymus was conducted using CT scans in different age groups of humans, according to another study. The mean diameter was three centimeters for children younger than 10 years old, but decreased to 1.5 centimeters for patients over 20 with fatty degeneration after 35 years since it couldn't be seen [19]
Nasseri et al. [2] studied the normal and abnormal thymus by using radiography, ultrasonography, computed tomography, MRI, and PET scan in humans [2]. Their CT scan findings were the same as previous studies. They also explained the regrowing of the thymus after any stress, which is called rebound hyperplasia [2].
Through a retrospective study on human patients that were referred for CT scans due to traumatic injuries over two years, they observed that the thymus was entirely replaced by fat in 138 patients out of 194 (71.1%), and they excluded these patients from their assessments, while the present study did not exclude patients with non-visible thymus to have more accurate results. They found that the shape of the thymus varies widely, even within the same age group. They also found soft tissue components in the thymus of four healthy patients aged 40–54, suggesting that the finding of some soft tissue in an asymptomatic patient was occasional, but could be normal [5]. In their study, the thymus was centered at the midline or showed a left-side predominance in most patients, and an arrowhead-like shape was often seen in patients, although there was wide variation in thymic shape between patients. Simanovsky et al. also found a significant relationship between age and thymic density, and between age and volume. There was no correlation between gender and thymic volume and density in their study [5].
In one study, the thymus in 783 human patients with no underlying disease was evaluated, and it was recognized that the thymus gland was present in 100% of patients under the age of 30, 73% of patients between the ages of 30 and 49, and 17% of patients over 49 years of age. In this study in four patients over 49 years of age, small (0.5 cm or less) irregularly shaped densities were seen in the anterior mediastinum, and because of uncertainties about the nature of these structures, these patients were included in the non-visualized group. The authors explained the size, location, attenuation, and shape of the thymus in their study. They also concluded that thymus attenuation decreases with aging [14].
Ackman et al. [6] described differences in thymic density between the genders in the 20–30 age groups. According to their study in 6% of patients, no thymic tissue was distinguishable, and they showed increased fatty degeneration of the thymus in young males compared to females. According to their results, there was no relationship between thymic morphology and body condition score [7,16].
A study by Hussain et al. investigated how different imaging modalities can be used to assess thymus normality and abnormality to differentiate thymic hyperplasia from thymic malignancy in human patients [19]. According to their study, the CT scan is valuable for primary assessment, providing the morphology and density, and MRI is the imaging modality of choice in diseased thymus because of its ability to provide a functional assessment of the gland [19].
The important limitation in the present study was the 2-slice CT scanner, which causes a loss of some details and a decrease in resolution. Human studies for thymus CT scans were done by different kinds of CT scan machines with different slices [6,7]. Multidetector row CT (MDCT) scanners can image the thymus with more detail because of thinner slices, unceasing images, and multiplanar reconstructions [5]. Another limitation of the present study was lack of histopathologic procedures following CT scan examinations to confirm the thymic tissue.
5. Conclusions
To the best of our knowledge, this is the first study evaluating the normal thymus gland in dogs using computed tomography and performing classification and grading. As a conclusion, variable shapes, sizes, and densities of the thymus gland can be noted in dogs, although some patterns for alteration of these variables with aging are explained through the study. The ratio of thymus thickness in transverse view to the width of the second thoracic vertebral midbody was approximately 1.2±0.7. A grading system for thymic appearance based on predominant thymic components was also established through the study and can be used by radiologists for reading thoracic CT scans. The thymus gland was also visible in adult dogs with no underlying disease, but serial examinations were also indicated if there were some suspicions of infiltrative disease in old dogs with some remnant thymic tissue. According to the results, thymic atrophy was not significantly affecting enhancement. Thymic characteristics were not different significantly between males and females except in the shape of the thymus, which needs more investigation to generalize this finding to other populations. Small and large breed dogs were different only in the volume of the thymus. Also, it can be concluded that increasing body fat content affects thymic fatty degeneration. In conclusion, further investigation of thymic changes in the case of infiltrative disease and some stresses like chemotherapy can complete the present study.
Author Contributions
All authors have been contributed actively in the work and the manuscript has been read and approved by all the authors for submission. Conceptualization, M.M. and S.K.; methodology, S.K.; software, A.B. and S.K.; validation, M.M., S.S., A.B. and S.K.; formal analysis, M.M. and S.K.; investigation, S.K.; resources, S.K.; data curation, S.S., A.B. and S.K.; writing—original draft preparation, S.K.; writing—review and editing, S.S., M.M., A.B. and S.K.; visualization, S.K. and M.M.; supervision, M.M and S.S; project administration, M.M.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was approved by the Institutional Review Board of the Faculty of Veterinary Medicine, University of Tehran, (protocol code of IR28200/6/16).
Informed Consent Statement
Written informed consent has been obtained from the owners of the patients to publish this paper.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Rezzani R, Nardo L, Favero G, Peroni M, Rodella LF. Thymus and aging: Morphological, radiological, and functional overview. Age (Dordr). 2014, 36:313-51. Epub., 2013 Jul 23. PMID: 23877171; PMCID: PMC3889907. [CrossRef]
- Nasseri F, Eftekhari F. Clinical and radiologic review of the normal and abnormal thymus: Pearls and pitfalls. Radiographics. 2010, 30:413-28. PMID: 20228326. [CrossRef]
- Manchanda S, Bhalla AS, Jana M, Gupta AK. Imaging of the pediatric thymus: Clinicoradiologic approach. World J Clin Pediatr. 2017, 6:10-23. PMID: 28224091; PMCID: PMC5296624. [CrossRef]
- Howard E. Evans, Alexander de Lahunta. Miller’s Anatmy of the Dog. Fourth Eddition. Copyright 2013, 1993, 1979, 1964 by Saunders, an imprint of Elsevier Inc., 1:559-560.
- Simanovsky N, Hiller N, Loubashevsky N, Rozovsky K. Normal CT characteristics of the thymus in adults. Eur J Radiol. 2012, 81:3581-6. Epub., 2012 Jan 10. PMID: 22236705. [CrossRef]
- Liggett AD, Thompson LJ, Frazier KS, Styer EL, Sangster LT. Thymic Hematoma in Juvenile Dogs Associated with Anticoagulant Rodenticide Toxicosis. J Veter Diag Inves. 2002, 14:416-419. [CrossRef]
- Harrington KA, Kennedy DS, Tang B, Hickie C, Phelan E, Torreggiani W, Halpenny D. Computed tomographic evaluation of the thymus-does obesity affect thymic fatty involution in a healthy young adult population? Br J Radiol. 2018, 91:20170609. Epub., 2018 Mar 7. PMID: 29356558; PMCID: PMC6223166. [CrossRef]
- Zitz JC, Birchard SJ, Couto GC, Samii VF, Weisbrode SE, Young GS. Results of excision of thymoma in cats and dogs: 20 cases (1984-2005). J Am Vet Med Assoc. 2008, 232:1186-92. PMID: 18412532. [CrossRef]
- Heiberg E, Wolverson MK, Sundaram M, Nouri S. Normal thymus: CT characteristics in subjects under age 20. AJR Am J Roentgenol. 1982, 138:491-4. PMID: 6977998. [CrossRef]
- Reichle JK, Wisner ER. Non-cardiac thoracic ultrasound in 75 feline and canine patients. Vet Radiol Ultrasound. 2000, 41:154-62. PMID: 10779076. [CrossRef]
- Hasson, D., Schiappacase, G., Alegría, J., & Silva, C. Revisiting a forgotten organ: Thymus evaluation in PET-CT. Revista Argentina de Radiologia. 2020, 84: 55-60.
- Moarabi, A., Avizeh, R., Mahabady, M.K., & Badami, M. Radiographic and ultrasonographic evaluation of thymus in mongrel doges. Iranian Vet. J. 2021. 17:59-64. No.1,Spring,2021. [CrossRef]
- Araki T, Nishino M, Gao W, Dupuis J, Hunninghake GM, Murakami T, Washko GR, O'Connor GT, Hatabu H. Normal thymus in adults: Appearance on CT and associations with age, sex, BMI and smoking. Eur Radiol. 2016, 26:15-24. Epub., 2015 Apr 30. PMID: 25925358; PMCID: PMC4847950. [CrossRef]
- Baron RL, Lee JK, Sagel SS, Peterson RR. Computed tomography of the normal thymus. Radiology. 1982, 142(1):121-5. PMID: 7053521. [CrossRef]
- Ackman JB, Kovacina B, Carter BW, Wu CC, Sharma A, Shepard JA, Halpern EF. Sex difference in normal thymic appearance in adults 20-30 years of age. Radiology. 2013, 268:245-53, Epub., 2013 Feb 25. PMID: 23440318. [CrossRef]
- Yang H, Youm YH, Vandanmagsar B, Rood J, Kumar KG, Butler AA, Dixit VD. Obesity accelerates thymic aging. Blood. 2009, 114:3803-12. Epub,2009 Aug 31. PMID: 19721009; PMCID: PMC2773495. [CrossRef]
- Cordella A, Saunders JH, Stock E. CT Characteristics of the Thymus in Adult Dogs with Non-Thymic Neoplasia Compared to Young Dogs. Vet Sci. 2023, 10:192. PMID: 36977231; PMCID: PMC10051521. [CrossRef]
- Sklair-Levy M, Agid R, Sella T, Strauss-Liviatan N, Bar-Ziv J. Age-related changes in CT attenuation of the thymus in children. Pediatr Radiol. 2000, 30:566-9. PMID: 10993542. [CrossRef]
- Hussein SA, Sabri YY, Fouad MA, Zawam H, Mohamed NM. Role of different imaging modalities in the evaluation of normal and diseased thymus. Egypt J Bronchol. 2020, 14, 5. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



