
Submitted:
23 December 2024
Posted:
24 December 2024
You are already at the latest version
Abstract
In recent years, the interest in the comprehension of the fasciae has significantly grown, together with the necessity to find a consensus for a terminology of the fasciae in the research and clinical fields. Furthermore, it is becoming necessary to categorize the various types of fascia (superficial, deep, visceral, neural) since they possess different anatomical characteristics, and are implicated in different pathophysiological pathways. While in the past we have described the deep/muscular fascia, the aim of this work is to summarize and catalogue the information relating to the superficial fascia (thickness, cellular end extracellular matrix component, innervation, vascularization).
Keywords:
fascia
; superficial fascia
; hypodermis
; matrix
; autonomic innervation
; blood vessels
; lymphatic
1. Introduction
Anatomists, academics and professionals in different health-oriented fields, increasingly use the term fascia but there is still absence of a clear consensus on the definition and significance of this term, thus making impossible to compare results and descriptions among different Authors or papers [1,2,3]. Moreover, most of the Authors are focused on the comprehension of the deep/muscular fascia, in its role in force transmission and proprioception, and in its implication in movement and muscular force, together with its alterations in pathological processes. However, the superficial fascia in recent years was recognized as a key element that organize the hypodermis. It is a thin fibrous layer mainly formed by collagen and elastic fibers, but also, containing fat lobules, vessels and nerves.
The superficial fasciae that have been first discovered and studied are those of Scarpa (1801), at the level of the abdomen, and of Colles (1819), at the level of the pelvic and inguinal area [4]. For a long time it was thought that the superficial fascia was present only at the level of these districts but more recently it has been recognized that it runs across the entire surface of the body [5,6,7,8,9,10,11], together with the dermis, presenting differences based on the location and function of the area it covers.
Anatomically, the superficial fascia separates two parts of the hypodermis: the superficial adipose tissue (SAT) and deep adipose tissue (DAT) [12,13,14] (Figure 1-A). These two layers present different features and functions: the SAT is strongly connected with the skin and share with it the innervation, probably collaborating in the the exteroception, whereas the DAT is a less organized layer, rich in hyaluronan and water with few adipose cells and collagen fibers, with the main function to separate both physically and functionally the superficial fascia from the deep one, allowing them to respond independently to different external and internal stimuli [15]. Passing between these two layers and dividing them, the superficial fascia permits to separate the skin form the musculoskeletal system, allowing an independent and normal sliding of these two components. Moreover, the superficial fascia splits to surround vessels and nerves, ensuring their patency, and form the so-called retinacula cutis, which have the function of connecting the superficial fascia to the skin (retinacula cutis superficialis, or skin ligaments) and to the deep fascia (retinacula cutis profundis), to provide a dynamic and flexible anchor of the skin to underlying tissues [12,16]. The deep septa are rare, thin, oblique and with an apparent lesser organization, allowing great autonomy between superficial and deep fascia. In contrast, the superficial septa are short, vertically oriented and dense, and connect the superficial fascia to the skin with a different orientation depending on the region [12,17,18]. The presence of retinacula in the SAT determines the formation of polygonal-oval lobes of fat cells with a mean circularity factor of 0.856 (±0.113) to 1, while in the DAT retinacula define large, flat and polygonal lobes of fat cells (circularity factor: mean 0.473 to 1, SD: 0.07) [19].
At the level of the sole of the foot and the palm of the hand the superficial fascia is apparently absent because it fuses with the underlying deep fascia, forming the so-called palmar fascia and plantar fascia [12]. Even at the facial level, points of adhesion between the superficial and deep fascia have been identified, with the function of separating adjacent adipose compartments, or adipose compartments and anatomical spaces [20]. Besides, in the face the superficial fascia envelopes all the mimical muscles, and it is also called SMAS (superficial musculo-aponeurotic system) of the face. In the skull, it becomes very fibrotic, and it is called galea capitis. In the gluteal region, the superficial fascia was clearly observed in the upper region, but becomes more difficult to describe in the lower gluteal region, which appears to be made up entirely of fat lobules with honeycomb septal walls [14].
The superficial fascia presents the typical characteristics of a fibrous connective tissue formed by cells, fibers and extracellular matrix (Figure 1-B): the loosely packed interwoven collagen fibres are mixed with a high content of elastic fibres. Moreover, it is populated by immune cells, and pervaded by a thin and huge network of blood and lymphatic vessels. Each component of the tissue defines specific functional characteristics of the fascia, which are below described and further explained.
2. Results
2.1. Thickness of the Superficial Fascia
The thickness of the superficial fascia can vary depending on its anatomical location, on the individual’s body mass index (BMI), age, gender and physiopathologic condition. By ultrasound imaging the superficial fascia appears as an hyperechoic tissue that presents a good contrast with the surrounding tissues [21,22], but the variability caused by the instrument, the probe and patient position, and intra- and interpersonal variation has to be taken into account. As demonstrated by Hammoudeh et al. and Pirri et al. [21,23], different regions of the body show marked differences in the thickness of the superficial fascia and in the number of layers it is composed of, appearing linear, laminate, bi-laminate or tri-laminate. Moreover, the thickness of the subcutaneous tissue is significantly and positively correlated with the total thickness of the superficial fascia and the mean thickness of the various layers that form it [23]. In general, in the posterior region of the body the superficial fascia appears less defined, but thicker, especially in the posterior part of the trunk, thigh and arm [24]. It is also thicker in the region of the trunk and thighs, compared to the peripheral regions of the body [25]. Gender differences are also observable: Abu-Hijleh observed major thicknesses at the level of the same areas in females with respect to males [26], whereas other Authors analyzed that the thickness is greater in the lower abdomen of the male (mean 528.336 ± 38.48 µm) than that in females (mean 390.822 ± 36.24 µm) [27,28].
Moreover, wide discrepancy between the thicknesses of the fasciae measured according to histological sections and US images were noted, probably due to tissue dehydration and shrinkage during the histological protocols. This evidence highlights the difficulty of comparing studies carried out with different protocols and techniques. In any case, the patterns measured by US and histology were similar, with a correlation (r = 0.918) highly significant (p < 0.01) [21]. In detail, Pirri et al. have demonstrated that, at thigh level, the average thickness of the SF measured by US imaging is equal to 490 ± 140 µm (anterior portion), 520 ± 100 µm (medially), 420 ± 120 µm (laterally) and 500 ± 110 µm (posterior portion). The measurements performed by histology give a mean thickness of 146.6±31.5 µm, but it does not appear uniform: the mean thicknesses were 153.2 ± 39.3 µm anteriorly, 128.4 ± 24.7 µm medially, 154.0 ± 28.8 µm laterally, 148.8 ± 33.2 µm posteriorly [22].
At the level of the abdomen, the SF is multilayered (3 to 7) in the midline, with a reduction in the number of layers as one proceeds towards the lateral portion, due to the progressive fusion between them. The thickness of the superficial fascia is greater in the lower portion of the abdomen than in the upper one, with a mean thickness respectively of 528.336 ± SE38.48µm and 364.165 ± SE 22.49µm in the male; 390.822 ± SE36.21 µm and 315.822 ± SE56.93 µm in the female [28].
The dorsal trunk has the thickest superficial fascia with a mean thickness of 600 µm (0.6 to 0.7 mm), followed by the lumbar region (similar thickness, but slightly thinner on average) [23].
At the nipple-areolar complex (NAC) there is a hyperdense line of superficial fascia, with an average thickness of 309 ± 171 µm, visible immediately below the skin in the sagittal sections [29]. This line turned under the NAC and at this point, the line became very thick. This measurement is important for infra-alveolar mammoplasty [30]. However, the thickness of the mammary fascia tends to change in different stages of life, especially in women [31].
The SF of the upper limb shows a mean thickness of 450 ± 100 µm and is thicker in the posterior region of the arm (530 ± 100 µm) than in the anterior one (400 ± 100 µm), while no statistically different values were noted between the anterior (400 µm) and posterior (410 µm) region of the forearm [24].
All the main mean values of SF evaluated by US imaging are summarized in Table 1.
2.2. The Cellular Population
Like in the deep fascia [32], the predominant cell population of the superficial fascial tissue are fibroblasts [33], randomly distributed, with the function of maintaining the structural integrity of the tissue, and of producing precursors of the extracellular matrix, such as collagen and elastic fibers, contributing to the organization and remodeling of the matrix. Numerous adipocytes are found in the midst of the collagen fibres, in small clusters. Some studies demonstrated that some preadipocytes are found in the superficial fascia, which gives origin to the retinacula cutis in superficial and deeper adipose layers [34].
Moreover, a density of 20.4 ± 9.4/mm2 of mast cells was observed in the superficial fascia of subumbilical area, between the collagen fibers, near the wall of the blood vessels and near the nerve fibers [35]. These cells are able to intervene together with other inflammatory transient cells, in early inflammatory stages, in tissue healing and regeneration process, confirming the involvement in these processes of the subcutaneous tissue and the superficial fascia [36].
Moreover, the superficial fascia, having ancestral origin from the panniculus carnosus present in animals, can present in some regions also muscle fibers, such as in the neck (indicated as the platysma muscle), in the face (the SMAS or superficial muscular aponeurotic system) [37,38], in the anal region (external anal sphincter) and in the scrotum (the dartos fascia) [39]. Really, in all the regions muscular fibers were found inside the superficial fascia.
2.3. Fibrous Component of the Superficial Fascia
The superficial fascia is composed of fibro-fatty layers interconnected and made of loosely packed collagen fibres (Figure 1-B), intertwined with abundant elastic fibres, both vertically and horizontally arranged, crossed by blood vessels and nerves along all three axes [26,40]. The thickness and the number of sub-layers of superficial fascia in the different regions of the body are probably proportional to the daily stress experienced in that site, confirming that the specific composition of the tissue can have direct implications in its mechanical properties and functionality [23].
Collagen fibers have great tensile strength: they can withstand considerable tensile forces without a significant increase in their length, but at the same time they are flexible.
The superficial fascia contains an high amount of elastic fibres forming a 3D network, with a prevalence of fibers in the transversal axis [41]. They form a lacework pattern, in some areas perforating the collagen bundles at different levels, and permitting to protect the nerves, and at the same time enabling the proper functioning of blood and lymph vessels. Some Authors evaluated that the ratio between collagen and elastic fibres is equal to 1:1: at the level of the lower abdomen, for instance, Pandey and coauthors quantified the collagen fibres equal to 13.455±3.960% and the elastic fibres equal to 14.602±5.244% [27]. This percentage of elastic fibres corresponds also with the data published by Pirri et al [41], that found 13.5% of elastic fibres in the superficial fascia of the thigh, ten times more than the fascia lata (deep fascia of the thigh). Really, this amount can physiologically change with the aging: in young people the superficial fascia is more elastic, allowing the hypodermis to respond adequately to stress stimuli coming from all dimensions without being damaged, and therefore returning to its initial state [12]. Elastic fibers in superficial fascia do not form bundles, but they are visible as a web with many branches and anastomose with other fibers. The elastic fibres are thinner than collagen ones and stretch easily with a high capacity to return to their original length [12].
The mechanical tests, performed in the thoracic and abdomen regions, observed that the superficial fascia is anisotropic, with a more rigid and tenacious nature along the lateral-medial direction, compared to the cranio-caudal one [42]. Furthermore, the thoracic region exhibited significantly greater strength and resultant Young's modulus compared to the abdomen (with greater results along the latero-medial direction), but the deformation at break was in both the regions almost independent of the direction of load, thanks to the high content of elastic fibers. Stress-relaxation tests highlighted the viscous behavior of the superficial fascia, with no significant differences in stress decay between different directions: most of the stress reduction occurred in the first minute of rest, reaching on average 37% of residual stress after 300 s [42].
In pathological conditions, such as in presence of a scar, the load-bearing capacity of the tissue is reduced by 30% and persists for several years after the formation of the scar [43].
2.4. Innervation
Although the superficial fascia has been reported as the second most innervated tissue after the skin (Fede et al. 2020), its innervation is still little studied. It has been shown that its innervation rate is higher than the deep fascia: the skin presented an innervated area equal to 0.73% ± 0.37%, the superficial fascia 0.22% ± 0.06%, and the deep one 0.17% ± 0.17% [44]. The nerve fibers in the superficial fascia showed a density of 33.0 ± 2.5/cm2: some nerve bundles are larger (mean diameter of 21.1 ± 12.2 µm), but the majority of the nerves pervading the tissue are very thin (average diameter of 4.8 ± 2.6 µm), showing a huge network of small nerve fibers supplying the tissue [45]. The nerve fibers are found around the blood vessels, close to the adipocytes and in the connective tissue itself [45]. The innervation in the midst of the collagen bundles confirms the sensorial role of the superficial fascia and its possible implications in nociception, although no Pacinian corpuscles and/or Ruffini corpuscles were found in the abdominal and hip region, contrary to what has been observed at the level of the plantar fascia [12].
The positivity to the immuno-staining for tyrosine hydroxylase (TH) marker confirmed the presence of a sympathetic autonomic nervous system in the superficial fascia, with a relative percentage of 33.82% and a S100/TH positivity ratio equal to 2.96, suggesting its possible role as vasoconstrictors and regulators of the vascularization in the superficial fascia [45]. However, some of these sympathetic endings do not terminate on the vessels, so their function is still a matter of debate: they may have a trophic activity [46], a role as pain modulator, mediating mechanical allodynia evoked by touch [47], or may have a role in the control of fascial tone and fascial stiffness [48,49].
The specific innervation of the superficial fascia and its strong relationship with the skin suggest that this innervation is part of the dermatomeric perception [15]. Moreover, the huge presence of TH-positive fibers permit to demonstrate that stress, temperature and trauma may affect the sympathetic activity not only in the skin, but also in the superficial fascia, with a consequent definition of its function as fundamental for thermoregulation, exteroception and pain modulation.
2.5. Blood Supply and Limphatyc Net of the Superficial Fascia
The superficial fascia is richly vascularized by a dense and thin network of blood vessels, composed of arteries, veins, capillaries and lymphatic segments that "run" inside the superficial fascia, both longitudinally and transversally, and which cross it at full thickness, as demonstrated in the Scarpa’s fascia. The surface is occupied by arterial vessels (6.20 ± 2.10%) and venous vessels (2.93 ± 1.80%) in the superficial fascia of the abdomen [50], but seems that there are regional differences. Indeed Tao et al. found at the level of the forearm a smaller quantity of blood vessels, equal to 2.7 ± 2.1% [51]. The vessels present a diameter between 13 and 65 μm, which had an average of 54.24 ± 15.80 µm for arteries, 60.10 ± 1.04 µm for veins, and 17.28 ± 3.84 µm for smaller vessels [50]. All these vessels connect to each other, creating a rete mirabile and extend along straight and curved paths in close contact with the cellular and extracellular component of the fascia matrix. They are well branched with a density of crossing points equal to 3.40 ± 1.90 per mm2 and with an optimal homogeneity of spatial distribution, confirming that the entire space of the superficial fascia is pervaded by vessels.
Tao and colleagues, analyzing the full-thickness area of forearm, from skin to muscle, showed that the branches of the intermuscular space and the septal cutaneous arteries join together to form longitudinal arterial chains at the level of the superficial fascia, repeatedly ramified [51]. Also the cadaveric studies of Wang et al. in the lower limb demonstrated that the perforators had three main branches: two cutaneous (vertical and oblique, which enter the subdermal layer) and one superficial fascial branch, which traveles in the superficial fascia and connects with the nearby perforators [52]. The superficial fascial network sends branches into adipose lobules to form the capillary networks, permitting to the superficial and deep fascial networks to communicate with each other.
Recently, Albertin et al. demonstrated a lymphatic plexus inside the superficial fascia. The lymphatic vessels appeared as flattened channels with an average diameter of 19.5 ± 4.77 µm [53]. The lymphatic vessels also head towards the dermis, crossing the SAT and flanking the retinacula cutis, until they reach the vicinity of the hair follicles, sebaceous and sweat glands, forming a coiled tubular structure. This network of lymphatic vessels accompanies adjacent veins and arteries, branching out in different directions, both longitudinally and transversally, following the orientation of the collagen and elastic fibres. Also Friedman and coauthors observed the lymphatic vessels in the dermis, superficial fascia (Scarpa fascia), and loose areolar tissue but not in deep or superficial fat, in the human anterior abdominal wall. They reported that the highest concentration was in the dermis (mean of 82.6%), whereas the Scarpa fascia contained 9.4% of lymphatics [54]. Albertin and coauthors, on the contrary, evaluated the positive area% (with the endothelium positive to factor D2-40) from the ratio between the total immunoreactive area and the total sampled area, showing that in the dermis was equal to 0.095 ± 0.018%, not significantly different with respect to the SF layer (0.122 ± 0.029%; p > 0.05) [53].
Thanks to the injection of dye at the subareolar level and in the glandular tissue of the upper lateral quadrant of the mammary gland, Wuringer et al. demonstrated the presence of lymphatic vessels embedded into the superficial fascia also at the level of the breast, showing how some lymphatic vessels isolated within the superficial fascia, drain toward the axillary lymph nodes [55].
2.6. Pathological Implications
The comprehension of the macroscopic and microscopic characteristics of the superficial fascia can allow to better understand the specific alterations that occur in fascial dysfunctions, facilitating a more targeted approach to treatment and therapies. As happened with the deep fascia, which was initially considered only as an inert collagen layer, also the superficial fascia has long been ignored. Instead, it has its own specific characteristics, it is richly innervated and vascularized, and hosts a lymphatic plexus, and consequently can be altered in various pathological situations.
First of all, being strongly connected to the subcutaneous adipose tissue, it is involved in cellulite.
Cellulite is a common aesthetic condition, which affects the majority of women, characterized by the heterogeneous appearance mainly of the skin that covers the gluteal and posterior thigh regions [56]. By studying the diseased tissue in full thickness, it has been seen how the heterogeneity at the skin level is caused by an imbalance between the forces of tissue containment (especially determined by the retinacula cutis) and the forces that push outward (determined by the increase in the volume of adipose cells following an increase in BMI or dysregulation of fluids [57]. Fibrosis of the subcutaneous connective tissue, shortening the septa and altering the skin surface, is therefore linked to the interaction between containment and extrusion forces, which increase interstitial pressure [58]. The involvement of the superficial fascia in this pathological pathway has been proven by the presence of short and oblique septa associated with cellulite dimples, which for 93.4% originate from this structure (the remaining septa originate from the deep fascia) [56] and a thickening of the superficial fascia already present at non-severe cellulite levels [59].
Besides, the superficial fascia is thicker in obese people respect to control ones [19]. The alterations seems not uniform, but according to Pandey et al. [27] the superficial fascia of the lower abdomen has a relatively lower content of elastic support, collagen and hydroxyproline compared to the upper one, and this could be one of the reasons why in obesity there is a greater flexion of the skin in the lower part of the abdomen compared to the upper part.
Regarding the wound healing process, it is proven that the superficial fascia is fundamental, intervening by mobilizing its extracellular matrix, acting as a temporary matrix in the wound bed [35]. Once mobilized, the fascial matrix loses its elastic properties and dehydrates becoming a rigid fibrotic scar [60]. However, this reorganization of the tissue, especially when it causes thickening of the fascia and retinacula, triggers inflammation and stiffening of the region adjacent to the scar [61]. Since there are differences in the thickness of the superficial fascia, age and gender dependent, as already reported, a different involvement of the tissue in the wound healing processes has also been observed: the combination of thinner skin with thicker superficial fascia, a common condition in women, can cause an easier violation of the fascial compartment by a skin lesion. This would mobilize the matrix more often in women and inflicting larger and pathological scars. Older patients, on the other hand, have a lower risk of extreme scarring as the superficial fascia becomes thinner with age [62].
Knowing the strong interaction between the superficial fascia and the lymphatic vessels, it can be postulated that these two factors can influence each other, and in both directions, in case of problems such as lymphedema. This theory is supported by works which observed a significant increase in the thickness of the superficial fascia and retinacula cutis in swollen legs compared to normal limbs. The mean relative increase in the thickness of the superficial fascia was 206.0% more than control group, while no significant difference was demonstrated between the thickness of the fascia in primary versus secondary lymphedema [63]. Really, this data are not confirmed by Pirri et al [64], which did not found alteration in superficial fascia thickness in the limbs with lymphedema compared with the contralateral side. Really, it is possible that the lymphedema leads to the alteration of the fascia, and its consequent and eventual damage, but at the same time, the alteration of the superficial fascia can compromise the lymphatic drainage present within it, as the collagen and elastic fibers guide the lymphatic flow also determining a low resistance path, facilitating the movement of the interstitial fluid [65].
The superficial fascia can also be used in reconstructive surgery for the creation of fascial flap, such as the parascapular fascio-cutaneous free flap or cutaneous flaps [66], thanks to the high vascularization and capacity of adherence to underlying tissues, or can be employed in the cosmetic surgery to lift layers of the lateral midface soft tissues, obtaining a significant and long-lasting lateral midface rejuvenation [67].
It can also act as a barrier against tumors that develop in the subcutaneous level: benign lesions in fact remain separated from the fascia, while malignant lesions adapt to its presence even penetrating its margins. These characteristics allow the superficial fascia to be used to facilitate the categorization of soft tissue tumors as benign or malignant [68].
Moreover, the huge amount of blood vessels and the autonomic innervation which regulate their action, can help to understand how alterations in thermoregulation, lymphatic flow and venous circulation are related to the superficial fascia. Caggiati et al (1999) highlighted how the superficial fascia represents an excellent support for the wall of the saphenous veins, supporting the adventitia from the outside through numerous fibrous septa which act like the spokes of a bicycle [69] (Figure 3-A). Consequently, if the superficial fascia is altered, it can stretch the venous wall in an anomalous way, causing a deformation of the vein and consequently an incontinence of the venous valves (Figure 3-B).
The recent demonstration of the huge sympathetic innervation of the superficial fascia suggests that it could be also influenced by state of chronic stress [70,71]. The changes caused by the chronic stress can also influence the immune system by the axis TGF-β1/Smad2/3/Foxp3, causing lymphocyte apoptosis and immunosuppression [72]. These aspects can suggest a possible involvement of the superficial fascia also in the mechanism of fibromyalgia, in which patients show a reduced dermal fiber length of fibers with vessel contact, suggesting a possible relationship between sympathetic neurons and impaired thermal tolerance commonly reported by fibromyalgic patients [73].
3. Materials and Methods
Our search was conducted on Web of Science (WOS), PubMed, and Cochrane databases, covering publications from their inception until November 2024. The MeSH keyword employed was “Superficial fascia”, following the string PubMed: (superficial fascia [Title/Abstract]); WOS: (superficial fascia [title]); Cochrane: (superficial fascia [Title Abstract Keyword]). The inclusion criteria were studies about superficial fascia in humans, in English language. The exclusion criteria were studies related in general to ‘fasciae’ but referred to the deep one without specifying it; not written in English; studies on animals; and duplicates.
The literature search was conducted by one reviewer (C.C) and verified by a senior researcher (C.F.). Any discrepancies were resolved through consensus among the authors. Our screening process involved reviewing title and abstracts, followed by a full-text review of eligible studies. Additionally, we meticulously examined the references of the included studies to identify any further relevant publications. In total, 1056 papers were identified (PubMed: 582, WOS: 147, Cochrane: 327). After removing 23 articles as duplicates, the screening was conducted according to the inclusion and exclusion criteria. Subsequently, the textual content of the remaining 220 potentially eligible papers was meticulously reviewed, removing papers that did not align with our predefined inclusion criteria. Ultimately, 60 articles remained available, and 4 more papers were added by hand-search to identify other potentially eligible studies for inclusion in the analysis. Finally, 64 studies met the inclusion criteria and were considered eligible for the comparative analysis for the review (Figure 2).
4. Conclusions
The superficial fascia is recognized as a specific anatomical structure with distinctive cellular, innervation and vascularization properties. It is a thin, fibrous membrane in the hypodermis that extends continuously throughout the body, and is composed of irregularly arranged collagen fibers interspersed with numerous elastic fibers. It works as a scaffold for supporting adipose lobules, providing structural integrity to the surrounding tissues and guarantying autonomy between the skin and the muscle/deep fascia. However, the more superficial fascia is studied, the more it is discovered that it encompasses multiple functions. It is implicated in tissue assemblage and mobilization, opening new perspectives for wound repair. It can be involved in reconstructive surgery and pain management of clinical manifestations caused by altered lymphatic transport (like lymphedema). Lastly, the rich thin autonomic innervation supplying the tissue can be influenced by a stress condition or a sudden change in temperature.
All this evidences highlight the complex and fascinating role of the superficial fascia that should be considered in clinical practice. Indeed, a better understanding of its dynamics will help a good comprehension of some fascial dysfunctions.
Author Contributions
Conceptualization, C.F. and C.S.; methodology, C.F., C.C.; formal analysis, C.F., C.C; C.P., Y.S., X.Z.; writing—original draft preparation, C.F. and C.C.; writing—review and editing, C.S., C.P., L.P. and V.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Stecco, C.; Adstrum, S.; Hedley, G.; Schleip, R.; Yucesoy, C.A. Update on fascial nomenclature. J Bodyw Mov Ther. 2018;22(2):354. [CrossRef]
- Adstrum, S.; Hedley, G.; Schleip, R.; Stecco, C.; Yucesoy, C.A. Defining the fascial system. J Bodyw Mov Ther. 2017;21(1):173-177. [CrossRef]
- Stecco, C.; Schleip, R. A fascia and the fascial system. J Bodyw Mov Ther. 2016;20(1):139-140. [CrossRef]
- Joshi, R.; Duong, H. Anatomy, Abdomen and Pelvis, Scarpa Fascia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; August 7, 2023.
- Bordoni, B.; Mahabadi, N.; Varacallo, M. Anatomy, Fascia. In: StatPearls. Treasure Island (FL): StatPearls Publishing; July 17, 2023.
- Ullah, S.M.; Grant, R.C.; Johnson, M.; McAlister, V.C. Scarpa's fascia and clinical signs: the role of the membranous superficial fascia in the eponymous clinical signs of retroperitoneal catastrophe. Ann R Coll Surg Engl. 2013;95(7):519-522. [CrossRef]
- Chopra, J.; Rani, A.; Rani, A.; Srivastava, A.K.; Sharma, P.K. Re-evaluation of superficial fascia of anterior abdominal wall: a computed tomographic study. Surg Radiol Anat. 2011;33(10):843-849. [CrossRef]
- Putterman, A.M. Deep and superficial eyelid fascia. Plast Reconstr Surg. 2012;129(4):721e-723e. [CrossRef]
- Graca Neto, L.; Graf, R.M. Anatomy of the Superficial Fascia System of the Breast: A Comprehensive Theory of Breast Fascial Anatomy. Plast Reconstr Surg. 2020;145(1):193e-194e. [CrossRef]
- Rehnke, R.D.; Groening, R.M.; Van Buskirk, E.R.; Clarke, J.M. Anatomy of the Superficial Fascia System of the Breast: A Comprehensive Theory of Breast Fascial Anatomy. Plast Reconstr Surg. 2018;142(5):1135-1144. [CrossRef]
- Yaghan, R.J.; Heis, H.A.; Lataifeh, I.M.; Al-Khazaaleh, O.A. Herniation of part of the breast through a congenital defect of the superficial fascia of the anterior thoracic wall. Aesthetic Plast Surg. 2008;32(3):566-568. [CrossRef]
- Stecco, C. Functional atlas of the human fascial system, 1st ed.; 2015, Churchill Linvingston, Elsevier: London, UK, 2015. ISBN 978-070-204-430-4.
- Rohrich, R.J.; Pessa, J.E. The retaining system of the face: histologic evaluation of the septal boundaries of the subcutaneous fat compartments. Plast Reconstr Surg. 2008 May;121(5):1804-1809. [CrossRef]
- Han, A.; Inoue, E.; Kikuchi, K.; Haikata, Y.; Tabira, Y.; Iwanaga, J.; Saga, T.; Kiyokawa, K.; Watanabe, K. Gross anatomical study of the subcutaneous structures that create the three-dimensional shape of the buttocks. Clin Anat. 2023 Mar;36(2):297-307. [CrossRef]
- Stecco, C.; Pirri, C.; Fede, C.; Fan, C.; Giordani, F.; Stecco, L.; Foti, C.; De Caro, R. Dermatome and fasciatome. Clin Anat. 2019;32(7):896-902. [CrossRef]
- Wilke, J.; Tenberg, S. Semimembranosus muscle displacement is associated with movement of the superficial fascia: An in vivo ultrasound investigation. J Anat. 2020;237(6):1026-1031. [CrossRef]
- Di Taranto, G.; Cicione, C.; Visconti, G.; Isgrò, M.A.; Barba, M.; Di Stasio, E.; Stigliano, E.; Bernadini, C.; Michetti, F.; Salgarello, M.; et al. Qualitative and quantitative differences of adipose-derived stromal cells from superficial and deep subcutaneous lipoaspirates: a matter of fat. Cytotherapy. 2015;17(8):1076-1089. [CrossRef]
- Si, L.; Li, H.; Li, Z.; Zhang, M.; Chen, X.; Yu, L.; Wang, H.C.; Wang, Y. The Superficial Fascia System: Anatomical Guideline for Zoning in Liposuction-Assisted Back Contouring. Plast Reconstr Surg. 2023 May 1;151(5):989-998. [CrossRef]
- Lancerotto, L.; Stecco, C.; Macchi, V.; Porzionato, A.; Stecco, A.; De Caro, R. Layers of the abdominal wall: anatomical investigation of subcutaneous tissue and superficial fascia. Surg Radiol Anat. 2011 Dec;33(10):835-42. [CrossRef]
- Pessa, J.E. SMAS Fusion Zones Determine the Subfascial and Subcutaneous Anatomy of the Human Face: Fascial Spaces, Fat Compartments, and Models of Facial Aging. Aesthet Surg J. 2016 May;36(5):515-26. [CrossRef]
- Pirri, C.; Fede, C.; Petrelli, L.; Guidolin, D.; Fan, C.; De Caro, R.; Stecco, C. An anatomical comparison of the fasciae of the thigh: A macroscopic, microscopic and ultrasound imaging study. J Anat. 2021 Apr;238(4):999-1009. [CrossRef]
- Pirri, C.; Stecco, C.; Petrelli, L.; De Caro, R.; Özçakar, L. Reappraisal on the Superficial Fascia in the Subcutaneous Tissue: Ultrasound and Histological Images Speaking Louder Than Words. Plast Reconstr Surg. 2022 Jul 1;150(1):244e-245e. [CrossRef]
- Hammoudeh, D.S.N.; Dohi, T.; Cho, H.; Ogawa, R. In Vivo Analysis of the Superficial and Deep Fascia. Plast Reconstr Surg. 2022 Nov 1;150(5):1035-1044. [CrossRef]
- Pirri, C.; Pirri, N.; Guidolin, D.; Macchi, V.; De Caro, R.; Stecco, C. Ultrasound Imaging of the Superficial Fascia in the Upper Limb: Arm and Forearm. Diagnostics (Basel). 2022 Aug 4;12(8):1884. [CrossRef]
- Gatt, A.; Agarwal, S.; Zito, P.M. Anatomy, Fascia Layers. In: StatPearls. Treasure Island (FL): StatPearls Publishing; July 24, 2023.
- Abu-Hijleh, M.F.; Roshier, A.L.; Al-Shboul, Q.; Dharap, A.S.; Harris, P.F. The membranous layer of superficial fascia: evidence for its widespread distribution in the body. Surg Radiol Anat. 2006 Dec;28(6):606-19. [CrossRef]
- Pandey, A.K.; Kumar, P.; Aithal, S.K.; Kotian, S.R.; Thittamaranahalli, H.; Bangera, H.; Prasad, K.; Souza, A.D. Histological and biochemical study of the superficial abdominal fascia and its implication in obesity. Anat Cell Biol. 2016 Sep;49(3):184-188. [CrossRef]
- Kumar, P.; Pandey, A.K.; Kumar, B.; Aithal, S.K. Anatomical study of superficial fascia and localized fat deposits of abdomen. Indian J Plast Surg. 2011 Sep;44(3):478-83. [CrossRef]
- Matousek, S.A.; Corlett, R.J.; Ashton, M.W. Understanding the fascial supporting network of the breast: key ligamentous structures in breast augmentation and a proposed system of nomenclature. Plast Reconstr Surg. 2014 Feb;133(2):273-281. [CrossRef]
- Komiya, T.; Ito, N.; Imai, R.; Itoh, M.; Naito, M.; Matsubayashi, J.; Matsumura, H. Anatomy of the superficial layer of superficial fascia around the nipple-areola complex. Aesthetic Plast Surg. 2015 Apr;39(2):209-13. [CrossRef]
- Nava, M.; Quattrone, P.; Riggio, E. Focus on the breast fascial system: a new approach for inframammary fold reconstruction. Plast Reconstr Surg. 1998 Sep;102(4):1034-45. [CrossRef]
- Fede, C.; Pirri, C.; Fan, C.; Petrelli, L.; Guidolin, D.; De Caro, R.; Stecco, C. A Closer Look at the Cellular and Molecular Components of the Deep/Muscular Fasciae. Int J Mol Sci. 2021;22(3):1411. Published 2021 Jan 30. [CrossRef]
- Langevin, H.M.; Cornbrooks, C.J.; Taatjes, D.J. Fibroblasts form a body-wide cellular network. Histochem Cell Biol. 2004;122(1):7-15. [CrossRef]
- Baptista, L.S.; Côrtes, I.; Montenegro, B.; Claudio-da-Silva, C.; Bouschbacher, M.; Jobeili, L.; Auxenfans, C.; Sigaudo-Roussel, D. A novel conjunctive microenvironment derived from human subcutaneous adipose tissue contributes to physiology of its superficial layer. Stem Cell Res Ther. 2021 Aug 28;12(1):480. [CrossRef]
- Fede, C.; Petrelli, L.; Pirri, C.; Tiengo, C.; De Caro, R.; Stecco, C. Detection of Mast Cells in Human Superficial Fascia. Int J Mol Sci. 2023 Jul 18;24(14):11599. [CrossRef]
- Soliman, A.M.; Barreda, D.R. Acute Inflammation in Tissue Healing. Int. J. Mol. Sci. 2022, 24, 641.
- Watanabe, K.; Han, A.; Inoue, E.; Iwanaga, J.; Tabira, Y.; Yamashita, A.; Kikuchi, K.; Haikata, Y.; Nooma, K.; Saga, T. The Key Structure of the Facial Soft Tissue: The Superficial Musculoaponeurotic System. Kurume Med J. 2023 Jul 3;68(2):53-61. [CrossRef]
- Ferreira, L.M.; Hochman, B.; Locali, R.F.; Rosa-Oliveira L.M. A stratigraphic approach to the superficial musculoaponeurotic system and its anatomic correlation with the superficial fascia. Aesthetic Plast Surg. 2006 Sep-Oct;30(5):549-52. [CrossRef]
- Stecco, C.; Macchi, V.; Porzionato, A.; Duparc, F.; De Caro, R. The fascia: the forgotten structure. Ital J Anat Embryol. 2011;116(3):127-38.
- Hwang, K.; Kim, H.; Kim, D.J.; Kim, Y.J.; Kang, Y.H. Superficial Fascia (SF) in the Cheek and Parotid Area: Histology and Magnetic Resonance Image (MRI). Aesthetic Plast Surg. 2016 Aug;40(4):566-77. [CrossRef]
- Pirri, C.; Fede, C.; Petrelli, L.; Guidolin, D.; Fan, C.; De Caro, R.; Stecco, C. Elastic Fibres in the subcutaneous tissue: Is there a difference between superficial and muscular fascia? A cadaver study. Skin Res Technol. 2022 Jan;28(1):21-27. [CrossRef]
- Berardo, A.; Bonaldi, L.; Stecco, C.; Fontanella, C.G. Biomechanical properties of the human superficial fascia: Site-specific variability and anisotropy of abdominal and thoracic regions. J Mech Behav Biomed Mater. 2024 Sep;157:106637. [CrossRef]
- Hollinsky, C.; Sandberg, S. Measurement of the tensile strength of the ventral abdominal wall in comparison with scar tissue. Clin Biomech (Bristol, Avon). 2007 Jan;22(1):88-92. [CrossRef]
- Fede, C.; Porzionato, A.; Petrelli, L.; Fan, C.; Pirri, C.; Biz, C.; De Caro, R.; Stecco, C. Fascia and soft tissues innervation in the human hip and their possible role in post-surgical pain. J Orthop Res. 2020 Jul;38(7):1646-1654. [CrossRef]
- Fede, C.; Petrelli, L.; Pirri, C.; Neuhuber, W.; Tiengo, C.; Biz, C.; De Caro, R.; Schleip, R.; Stecco, C. Innervation of human superficial fascia. Front Neuroanat. 2022 Aug 29;16:981426. [CrossRef]
- Neuhuber, W.; and Jänig, W. Fascia in the Osteopathic Field, eds T. Liem, P. Tozzi, A. Chila. Scotland: Handspring Publishing Limited. 2017. ISBN 978-882-144-729-7.
- Larsson, M.; Nagi, S.S. Role of C-tactile fibers in pain modulation: animal and human perspectives. Curr. Opin. Behav. Sci. 43, 2022, 138–144. [CrossRef]
- Staubesand, J.; Li, Y. (1996). Zum Feinbau der Fascia cruris mit besonderer Beruücksichtigung epi- und intrafaszialer Nerven. Manuelle Medizin 34, 1996, 196–200.
- Schleip, R.; Gabbiani, G.; Wilke, J.; Naylor, I.; Hinz, B.; Zorn, A.; Jäger, H.; Breul, R.; Schreiner, S.; Klingler, W. Fascia Is Able to Actively Contract and May Thereby Influence Musculoskeletal Dynamics: A Histochemical and Mechanographic Investigation. Front Physiol. 2019;10:336. [CrossRef]
- Pirri, C.; Petrelli, L.; Fede, C.; Guidolin, D.; Tiengo, C.; De Caro, R.; Stecco, C. Blood supply to the superficial fascia of the abdomen: An anatomical study. Clin Anat. 2023 May;36(4):570-580. [CrossRef]
- Tao, K.Z.; Chen, E.Y.; Ji, R.M.; Dang, R.S. Anatomical study on arteries of fasciae in the forearm fasciocutaneous flap. Clin Anat. 2000;13(1):1-5. [CrossRef]
- Wang, X.; He, Z.P.; Sun, Y.; Li, L.C.; Liu, Y.Q.; Yang, Y.R.; Qi, L.N.; Yang, J.H.; Shi, Y.T.; Qin, X.Z. More potential uses of specific perforator flaps in the calf - A cadaveric study on the subdermal vascular structure of the lower leg. Ann Anat. 2024 Jun;254:152262. [CrossRef]
- Albertin, G.; Astolfi, L.; Fede, C.; Simoni, E.; Contran, M.; Petrelli, L.; Tiengo, C.; Guidolin, D.; De Caro, R.; Stecco, C. Detection of Lymphatic Vessels in the Superficial Fascia of the Abdomen. Life (Basel). 2023 Mar 20;13(3):836. [CrossRef]
- Friedman, T.; Coon, D.; Kanbour-Shakir, A.; Michaels, J.5th; Rubin, J.P. Defining the lymphatic system of the anterior abdominal wall: an anatomical study. Plast Reconstr Surg. 2015 Apr;135(4):1027-1032. [CrossRef]
- Würinger, E. Localization of Central Breast Lymphatics and Predefined Separation of Lobes along the Horizontal Septum. Plast Reconstr Surg Glob Open. 2023 Dec 7;11(12):e5446. [CrossRef]
- Whipple, L.A.; Fournier, C.T.; Heiman, A.J.; Awad, A.A.; Roth, M.Z.; Cotofana, S.; Ricci, J.A. The Anatomical Basis of Cellulite Dimple Formation: An Ultrasound-Based Examination. Plast Reconstr Surg. 2021 Sep 1;148(3):375e-381e. [CrossRef]
- Rudolph, C.; Hladik, C.; Hamade, H.; Frank, K.; Kaminer, M.S.; Hexsel, D.; Gotkin, R.H.; Sadick, N.S.; Green, J.B.; Cotofana, S. Structural Gender Dimorphism and the Biomechanics of the Gluteal Subcutaneous Tissue: Implications for the Pathophysiology of Cellulite. Plast Reconstr Surg. 2019 Apr;143(4):1077-1086. [CrossRef]
- Cotofana, S.; Kaminer, M.S. Anatomic update on the 3-dimensionality of the subdermal septum and its relevance for the pathophysiology of cellulite. J Cosmet Dermatol. 2022 Aug;21(8):3232-3239. [CrossRef]
- Révelon, G.; Rahmouni, A.; Jazaerli, N.; Godeau, B.; Chosidow, O.; Authier, J.; Mathieu, D.; Roujeau, J.C.; Vasile, N. Acute swelling of the limbs: magnetic resonance pictorial review of fascial and muscle signal changes. Eur J Radiol. 1999 Apr;30(1):11-21. [CrossRef]
- Correa-Gallegos, D.; Rinkevich, Y. Cutting into wound repair. FEBS J. 2022 Sep;289(17):5034-5048. [CrossRef]
- Pirri, C.; Stecco, C.; Pirri, N.; De Caro, R.; Özçakar, L. Ultrasound examination for a heel scar: seeing/treating the painful superficial fascia. Med Ultrason. 2022 May 25;24(2):255-256. [CrossRef]
- Jiang, D.; Rinkevich, Y. Furnishing Wound Repair by the Subcutaneous Fascia. Int J Mol Sci. 2021 Aug 20;22(16):9006. [CrossRef]
- Idy-Peretti, I.; Bittoun, J.; Alliot, F.A.; Richard, S.B.; Querleux, B.G.; Cluzan, R.V. Lymphedematous skin and subcutis: in vivo high resolution magnetic resonance imaging evaluation. J Invest Dermatol. 1998 May;110(5):782-7. [CrossRef]
- Pirri, C.; Pirri, N.; Ferraretto, C.; Bonaldo, L.; De Caro, R.; Masiero, S.; Stecco, C. Ultrasound Imaging of the Superficial and Deep Fasciae Thickness of Upper Limbs in Lymphedema Patients Versus Healthy Subjects. Diagnostics (Basel). 2024;14(23):2697. [CrossRef]
- Stecco, A.; Stern, R.; Fantoni, I.; De Caro, R.; Stecco, C. Fascial Disorders: Implications for Treatment. PM R. 2016 Feb;8(2):161-8. [CrossRef]
- Stecco, C.; Tiengo, C.; Stecco, A.; Porzionato, A.; Macchi, V.; Stern, R.; De Caro, R. Fascia redefined: anatomical features and technical relevance in fascial flap surgery. Surg Radiol Anat. 2013 Jul;35(5):369-76. [CrossRef]
- Byun, J.S.; Hwang, K.; Lee, S.Y.; Song, J.M.; Kim, H. Forces Required to Pull the Superficial Fascia in Facelifts. Plast Surg (Oakv). 2018 Feb;26(1):40-45. [CrossRef]
- Galant, J.; Martí-Bonmatí, L.; Soler, R.; Saez, F.; Lafuente, J.; Bonmatí, C.; Gonzalez, I. Grading of subcutaneous soft tissue tumors by means of their relationship with the superficial fascia on MR imaging. Skeletal Radiol. 1998 Dec;27(12):657-63. [CrossRef]
- Caggiati, A. Fascial relationships of the long saphenous vein. Circulation. 1999;100(25):2547-2549. [CrossRef]
- Won, E.; Kim, Y.K. Stress, the Autonomic Nervous System, and the Immune-kynurenine Pathway in the Etiology of Depression. Curr Neuropharmacol. 2016;14(7):665-73. [CrossRef]
- Lowrance, S.A.; Ionadi, A.; McKay, E.; Douglas, X.; Johnson, J.D. Sympathetic nervous system contributes to enhanced corticosterone levels following chronic stress. Psychoneuroendocrinology 2016;68:163-70. [CrossRef]
- Zhang, H.; Caudle, Y.; Wheeler, C.; Zhou, Y.; Stuart, C.; Yao, B.; Yin, D. TGF-β1/Smad2/3/Foxp3 signaling is required for chronic stress-induced immune suppression. J Neuroimmunol. 2018;314:30-41. [CrossRef]
- Evdokimov, D.; Dinkel, P.; Frank, J.; Sommer, C.; Üçeyler, N. Characterization of dermal skin innervation in fibromyalgia syndrome. PLoS One. 2020;15(1):e0227674. [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, n71.
Figure 1.
Scheme representing the anatomy from skin to the muscle (A) and histological detail (Hematoxylin and Eosin staining) of the superficial fascial layer (B). .
Figure 1.
Scheme representing the anatomy from skin to the muscle (A) and histological detail (Hematoxylin and Eosin staining) of the superficial fascial layer (B). .
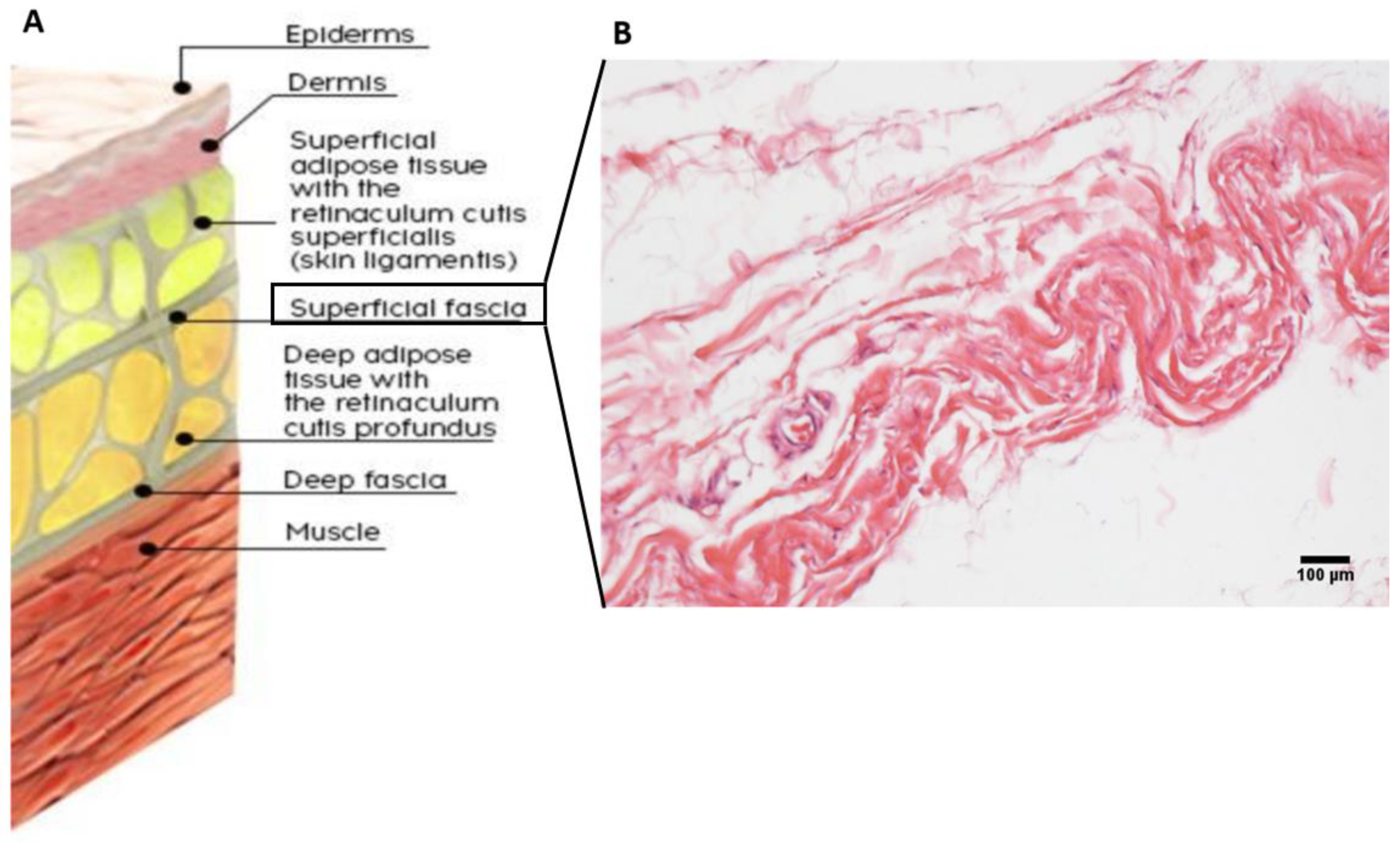
Figure 2.
PRISMA flow diagram of articles selection. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews [74].
Figure 2.
PRISMA flow diagram of articles selection. From: Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews [74].
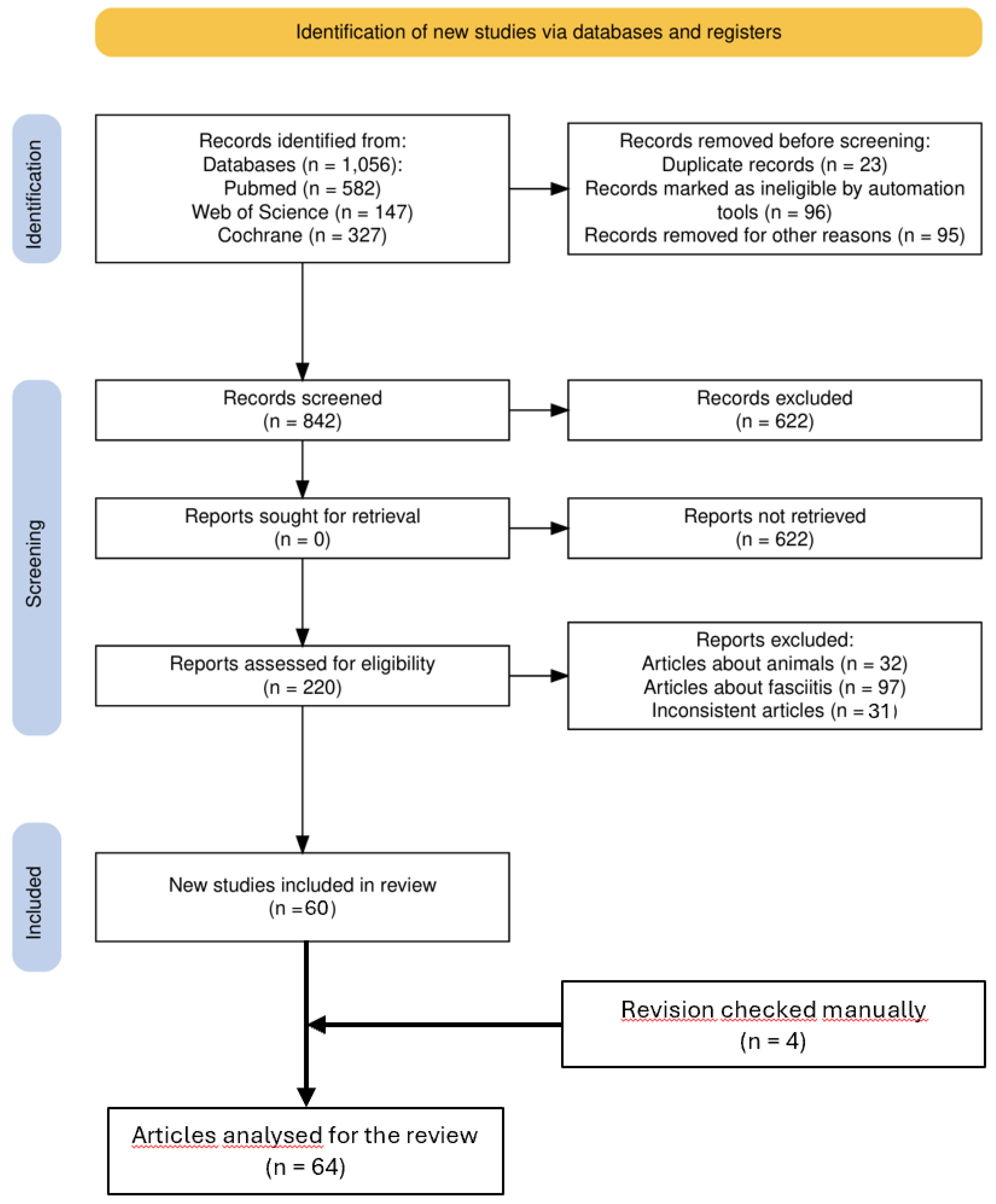
Figure 3.
Schematic representation of the saphenous vein (in blue) and its relationship with the superficial fascia. A: as described by Caggiati [69], the superficial fascia splits around the saphenous vein and sends some fibrous septa to the adventitia, supporting from outside the patent of the vein. B: when superficial fascia is overstretched due to a scar or a fascial fibrosis (red arrow), the anomalous tension is transmitted to the support system of the saphenous vein, causing a deformation of the vessel and consequently incontinence of the valves (in yellow).
Figure 3.
Schematic representation of the saphenous vein (in blue) and its relationship with the superficial fascia. A: as described by Caggiati [69], the superficial fascia splits around the saphenous vein and sends some fibrous septa to the adventitia, supporting from outside the patent of the vein. B: when superficial fascia is overstretched due to a scar or a fascial fibrosis (red arrow), the anomalous tension is transmitted to the support system of the saphenous vein, causing a deformation of the vessel and consequently incontinence of the valves (in yellow).
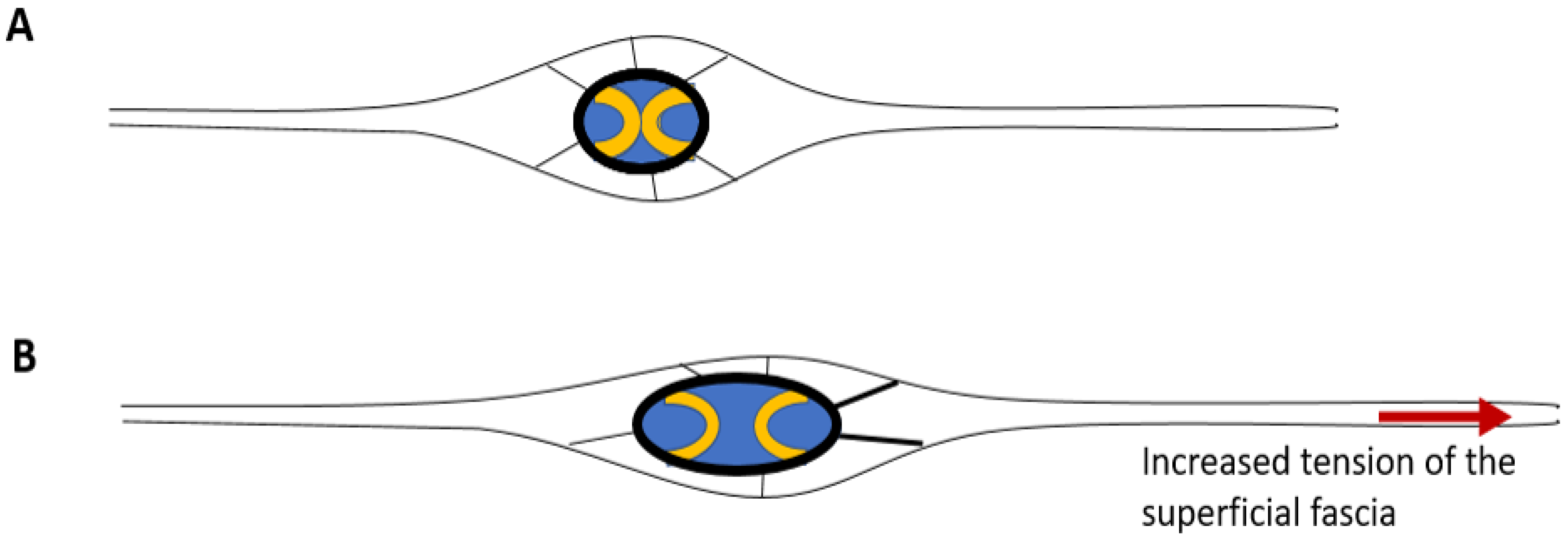

Table 1.
Values of SF thicknesses (in µm,) measured using US imaging.
| Region | Mean value | |
|---|---|---|
| Upper limb | Anterior | 400 ± 100 |
| Posterior | 530 ± 100 | |
| Dorsal Trunk | Cranial | 600 to 700 |
| Caudal | 500 to 600 | |
| Abdomen | Cranial | 360 ± 22 ♂ 315 ± 56 ♀ |
| Caudal | 528 ± 38 ♂ 390 ± 36 ♀ |
|
| NAC | 309 ± 171 | |
| Thigh | Anterior | 490 ± 140 |
| Posterior | 500 ± 110 | |
| Medially | 520 ± 100 | |
| Laterally | 420 ± 120 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



